
Abstract
A higher extent of resection (EOR) in WHO grade II gliomas (GIIG) is correlated with longer survival. However, the molecular markers also feature prognostic relevance. Here, we examined whether maximal EOR was related to the genetic profile. We retrospectively investigated the predictive value of 1p19q, IDH1, 53 expression and Ki67 index for the EOR in 200 consecutive GIIGs (2007–2013). Data were modeled in a linear model. The analysis was performed with two statistical methods (arcsin-sqrt and Beta-regression model with logit link). There was no deletion 1p19q in 118 cases, codeletion 1p19q (57 cases), single deletion 1p (4 cases) or19q (16 cases). 155 patients had a mutation of IDH1. p53 was graded in 4 degrees (0:92 cases, 1:52 cases, 2:31 cases, 3:8 cases). Mean Ki67 index was 5.2 % (range 1–20 %). Mean preoperative tumor volume was 60.8 cm3 (range 3.3–250 cm3) and mean EOR was 0.917 (range 0.574–1). The statistical analysis was significant for a lower EOR in patients with codeletion 1p19q (OR 0.738, p = 0.0463) and with a single deletion 19q (OR 0.641, p = 0.0168). There was no significant correlation between IDH1 or p53 and the EOR. Higher Ki67 was marginally associated with higher EOR (p = 0.0603). The study demonstrates in a large cohort of GIIG that a higher EOR is not attributable to favorable genetic markers. This original result supports maximal surgical resection as an important therapeutic factor per se to optimize prognosis, independently of the molecular pattern.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The prognosis of WHO grade II glioma (GIIG) is essentially related to the inevitable progression to a high grade glioma (WHO III and WHO IV). Patients with GIIG are usually young and often enjoy a good quality of life due to absent or only minor neurological deficits [1], which can be explained by neuroplasticity induced by these slow growing neoplasms [2, 3].
There are several molecular genetic tumor markers in GIIG which have been shown be prognostically relevant [4]. The loss of genetic information (loss of heterozygosity, LOH) of the chromosomal regions 1p and 19q (1p19q-LOH) is generally regarded as a marker of oligodendroglioma, associated with a better prognosis [5, 6]. Mutations of the IDH1 gene are considered an early event in the development of a GIIG and reduce the formation of α-ketoglutarate in favor of 2-hydroxyglutarate. IDH1 mutations have been correlated with an improved prognosis [7–9]. Mutations of the tumor suppressor gene TP53 are predominantly prevalent in astrocytomas and are often associated with a worsened prognosis [10]. The Ki67 index describes the proliferative activity of a glioma and is commonly used as a marker to evaluate a tumor’s growth rate but also features prognostic significance [11–13].
It has been extensively demonstrated in the recent literature with objective measurement of the extent of resection (EOR) on T2/FLAIR MRI, that maximal surgery with a higher EOR was significantly correlated with an increased overall survival by delaying malignant transformation [14–19]. As a consequence, early and radical surgical resection with preservation of the quality of life is currently the first therapeutic option to consider in GIIG, as recommended by the European Guidelines [20]. To this end, a meta-analysis studying 8,091 patients who underwent surgery for brain gliomas demonstrated that the use of intrasurgical mapping allowed a statistically significant increase of the EOR, despite a reduction of permanent deficit, even in eloquent areas [21].
Nonetheless, one could argue that the impact of EOR on survival might be biased by a more favorable molecular pattern in GIIGs amenable to a maximal resection. To our knowledge, this specific question, i.e. to know whether a better EOR is correlated to a favorable genetic profile, has so far not been addressed. To examine this issue, we performed a study with a large cohort of GIIG patients from a single institution treated by maximal tumor resection using intraoperative mapping. Within the frame of this study, we analyzed if there was a correlation between the markers 1p19q, IDH1, p53 as well as the Ki67 index of the individual GIIG and the achieved EOR.
Patients and methods
Patient selection
Charts of 254 consecutive patients with WHO grade II gliomas from a single institution (Centre Hospitalier Universitaire, Montpellier, France) from January 2007 until July 2013 have been reviewed. All patients have been operated on by the same neurosurgeon (HD) using the technique of tumor resection in awake patient under cortical and subcortical electrical stimulation with concomitant neuropsychological evaluation for functional mapping, as previously described [22]. In practice, the resection was achieved according to functional boundaries in all cases: it means that the tumor removal was pursued until eloquent structures have been encountered (but not before)—for a recent review, see [23]. The patients’ charts were screened for the correct definite histopathological diagnosis for inclusion of a grade II glioma according to the criteria of the World Health Organisation (WHO) [24]. Further inclusion criteria were the availability of magnetic resonance- (MR-) imaging meeting the Digital Imaging and Communications in Medicine (DICOM) standard pre- and postoperatively (within the 24 h following surgery) for volumetric analysis, completed analysis of the 1p19q-status, IDH1-status, p53-status and Ki67-estimation. In patients with multiple operative procedures, imaging data and molecular genetic data of the first intended maximal resection were chosen.
All patients gave their written informed consent.
MR-volumetry
Estimation of the preoperative tumor volumes and postoperative tumor volumes was performed by using the software Myrian 1.12.4 (Intrasense, France). The hyperintensity on FLAIR images has been used to estimate the tumor volumes. Segmentations were performed manually. Calculation of the EOR was done by using the values of the preoperative tumor volumes and postoperative tumor volumes. Calculation of the EOR percentage was performed by using Eq. (1).
Molecular genetic examinations
Areas with a tumor cell content of more than 60 % were selected by histopathological examination. Tumor DNA was isolated from frozen tissue according to a chaotropic method on a silica membrane (Qiagen DNA mini kit, Qiagen, Hilden, Germany). Blood DNA was extracted from the patient’s EDTA peripheral blood using the MagNA Pure Compact robot (Roche Diagnostics, Mannheim, Germany).
1p19q loss of heterozygosity
Blood and tumor DNA were genotyped for a panel of highly polymorphic microsatellite markers: on 1p (D1S2660, D41S450, D1S507, D1S234, D1S2890, D1S230, D1S207, D1S206) and 19q (D19S414, D19S420, D19S903, D19S571).
IDH1 mutation screening
IDH1 genotyping was performed by PCR amplification and direct sequencing as previously described [25].
Immunohistological analysis
Immunohistochemistry for p53 and Ki67 expression detection on paraffin-embedded tissue
Since overexpression of p53 protein approximatively reflects the TP53 gene mutational status, we used protein immunostaining as a deductive method to evaluate the mutational rate of the TP53 gene [26–29].
Antigen retrieval for p53 and Ki67 staining was done by using EDTA, pH 7–8.
Monoclonal antibodies for p53 (Ménarini Diagnostics, Florence, Italy) and Ki67 (Dako, Glostrup, Denmark) were used at dilution 1:40 and dilution 1: 100, respectively. Labeled streptavidin biotin kit was used as detection system (Benchmark Ultra, Ventana Medical Systems, Tucson, Arizona, USA). For p53, cases with more than 10 % of stained nuclei were considered as positive. Immunopositive cases were graded from 1+ to 3+ as follows: 1+ positivity: 11–33 % cells stained; 2+ positivity: 33–66 % cells stained; 3+ positivity: 66–100 % cells stained.
For Ki67 staining, areas of highest cellularity were used for quantification. The percentage of labeled cells was determined from a count of 100 cells. The retained Ki67 % labeling was assessed in the area with the highest level of proliferation.
Statistical analysis
Estimation of the predictive value of the prevalence of the markers 1p19q, IDH1, p53 and Ki67 for the EOR. 1p19q, IDH1, p53 were analyzed as categorical variables with and without clustering of the variables, Ki67 as a continuous variable (see below). All tests were performed at a significance level α of 5 %. Data were modeled in a linear model. The model was tested for effect modification by the different tumor locations and the preoperative tumor volume. It was tested for interactions and collinearity in an explorative manner and was controlled by checking the model assumptions and by inspecting the residuals and leverages.
Model using arcsin-sqrt transformation
The EOR was arcsin-sqrt transformed to better meet the assumption of a normal error distribution (Eq. 2).
Beta regression model with logit link: The usual practice used in modelling a response variable (y = EOR) in the standard unit interval y ∈ (0, 1) is the transformation as performed in the main analysis. This approach, however, has shortcomings in terms of interpretability. Therefore, in addition to the analysis described above, data were analyzed using a Beta-regression model with logit link according to Cribari and Zileis [30].
Since the Beta-regression model needs to have values 0 < y < 1 but the EOR was 1 in several cases, the EOR was transformed (Eq. 3),
where n is the number of measurements in y.
Primary analysis
Correlation of clustered molecular genetic markers with the EOR. Clustering of the different levels of 1p19q, IDH1, p53 as follows:
1p19q:
-
no deletion 1p19q
-
deletion 1p or deletion 19q
-
codeletion 1p19q, partial deletion 1p19q
IDH1:
-
no mutation
-
mutation c.394C>A or c.394C>G or c.394C>T or c.395G>A or c.395G>T
p53:
-
immunopositivity of 10 % of cells or less
-
immunopositivity 1 + , 2 + or 3 + according to the classification above.
Secondary analysis
Differentiation between the mutational subtypes without clustering.
Results
Patients
After review of 254 patient charts meeting the criteria mentioned above, 54 patients have been excluded due to one or more of the following reasons: a posteriori histopathological diagnosis of a tumor other than a WHO grade II glioma, denial of molecular-genetic examinations, refusal of study participation, incomplete or insufficient MR-data for volumetry, incomplete patient charts, lack of more than one molecular genetic examination. Finally, 200 patients have been included for the statistical analysis (see Tables 1 and 2 for patient characteristics).
The mean age of the patients was 38.9 years (median 37.0 years; SD 10.5); 109 patients were males (54.5 %) and 91 females (45.5 %). Regarding glioma localization, 114 tumors were located on the left side (57 %) and 86 on the right side (43 %); 65 tumors (32.5 %) were located completely or partially in the insular region, 90 tumors (45 %) completely or partially in the temporal region and 116 tumors (58 %) completely or partially in the frontal region. The mean preoperative tumor volume was 60.8 cm3 (median 51.0 cm3, SD 43.2, range 3.3–250 cm3). The mean postoperative tumor volume was 6.1 cm3 (median 3.0 cm3, SD 8.4, range 0–70 cm3). The mean EOR was 91.7 % (median 92.7 %, SD 0.074, range 57.4–100 %); 165 patients (82.5 %) had a postoperative tumor volume of less than 10 cm3. Remarkably, there was a statistically significant larger EOR on the right side (Tables 3, 4). No significant interactions were found between the markers, the localization of the tumors and the preoperative tumor volumes or between the markers themselves. In both analyses, the effect of the preoperative tumor volume was highly significant (p < 0.001), but very small.
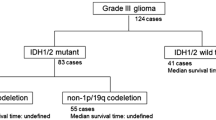
The correlation between 1p19q status and IDH1 status was as follows: 1p19q codeletion associated with IDH1 mutation: n = 52 (26 % of patients); IDH1 mutation without 1p19q codeletion: n = 103 (51.5 %); 1p19q codeletion without IDH1 mutation: n = 4 (2 %); no codeletion 1p19q and missing IDH1 mutation: n = 41 (20.5 %).
1p19q and EOR
195 patients could be evaluated concerning their 1p19q status: 118 patients (60.5 %) had no deletion of 1p and 19q; 57 patients (29.2 %) had a codeletion 1p19q; 4 patients (2.0 %) had a deletion of 1p; and 16 patients (8.2 %) a deletion of 19q. The statistical model using arcsin-sqrt transformation was significant for a lower EOR in patients with a codeletion 1p19q (p = 0.0439) but also for patients with a single deletion 1p or 19q (p = 0.0651) (see Table 3). The Beta regression model with logit link of the primary analysis confirmed this result, yielding an OR of 0.738 for 1p19q codeleted tumors (p = 0.0463) and an OR of 0.641 for tumors with a single deletion of 1p or 19q (p = 0.0168) (see Table 4). The Beta regression model of the secondary analysis (Table 5) again was significant for a lower EOR in 1p19q codeleted tumors (OR 0.733; p = 0.0491); also, the sole deletion 19q was correlated with a lower EOR (OR 0.623; p = 0.0274). A reliable statement concerning the sole 1p deletion was not possible due to the low number of patients (n = 4, p = 0.4177).
IDH1 and EOR
200 patients could be evaluated concerning their IDH1 status: 45 patients (22.5 %) had no IDH1 mutation, 155 patients (77.5 %) had one of the depicted IDH1 mutations (Table 2). In both models of the main analysis, there was no significant correlation between the IDH1 status and the EOR (p = 0.615, resp. OR 1.002, p = 0.9922) (see Tables 3, 4). The subgroup analysis was not further informative, probably since there was one predominant mutation (c.395G>A) and only small numbers for the other observed mutations (Table 5).
p53 and EOR
183 patients could be evaluated concerning their p53 status: 92 patients (50.3 %) were graded “0” since less than 11 % of nuclei were stained; 52 patients (28.4 %) were graded “1+” due to the criteria described above; 31 patients (16.9 %) were accordingly graded “2+” and 8 patients (4.4 %) were graded “3+” (Table 2). In both models of the main analysis, there was no statistically significant correlation of the p53 status and the EOR (p = 0.1570, resp. OR 1.186, p = 0.2089) (see Tables 3, 4). The subgroup analysis in the secondary evaluation failed to reach a significant correlation between the EOR and the different levels of p53 immunopositivity (Table 5).
Ki67 and EOR
198 patients could be evaluated concerning their Ki67 index, which was analyzed as a continuous variable (Table 1). Values ranged from 1.0 to 20.0 % with a mean of 5.2 % (SD 3.8; median 5.0). In the main analysis there was a weakly significant (p = 0.0603) correlation to the EOR, with a higher Ki67 value marginally associated with a higher EOR. The Beta regression model of the secondary analysis basically confirmed this result (p = 0.0788) but was also suggestive that there might be some rather small effect (OR 1.031) (see Tables 3, 4).
Except with regard to this marginal correlation with a higher Ki67, a higher EOR was not significantly associated with a specific molecular profile.
Discussion
The presented study addressed the question whether a better EOR was correlated to a more favorable genetic profile.
Before answering this question, we should first emphasize the fact that all GIIGs in this series have been removed maximally according to functional boundaries at the individual level, which was made possible by the use of intraoperative electrostimulation mapping. This means that the resection has been pursued until eloquent structures have been encountered, with no margin around these critical cortical and subcortical regions in order to optimize the EOR—as already described by the authors [22, 23, 31]. Furthermore, all these functional-mapping guided resections were carried out by only one surgeon to minimize the influence of subjective assessments of different surgeons concerning resectability and non-resectability.
Among the variables analyzed as potential confounding factors, the preoperative tumor volume was highly significant (p < 0.001), but of potentially rather small effect size. The right-sided tumor location was significantly (p = 0.020, resp. p = 0.010) associated with a higher EOR. Of note, in this study the effect of the laterality of the tumors is compensated by an approximately balanced number of left- and right sided tumors. These two latter variables could be interesting for further research concerning the establishment of prognostic predictive parameters for individual tumor patients.
1p19q and EOR
We have demonstrated in a large cohort of GIIG that a higher EOR is not correlated to a better molecular genetic prognosis, in particular that it is not correlated with 1p19 codeletion. On the contrary, we found a significant correlation of a lower EOR with a 1p19q codeletion.
This is a striking result. Indeed, as mentioned, in the modern literature with objective assessment of pre- and post-operative tumor volumes on T2/FLAIR MRI, EOR improves significantly survival. In the largest surgical series ever reported with 1509 GIIG patients, total surgical resection was independently associated with increased malignant progression-free and overall survival [16]. Nonetheless, it could be suggested that this increased survival might actually be related to a selection bias, i.e. that patients who benefited from a maximal resection were patients bearing a GIIG with a better molecular molecular pattern. According to this hypothesis, if significant correlations were identified in our present study, one could expect a higher EOR in GIIG with a 1p19q codeletion. Interestingly, we found the contrary, that is, that 1p19q codeletion was in fine significantly correlated with a lower surgical resectability. Codeletion was shown to represent a favorable prognostic [32] as well as predictive [33] spontaneous factor in GIIG, correlated with overall survival. As a consequence, our original findings support the fact that an improved survival in higher EOR is not biased by a better tumor-intrinsic prognostic factor. In other words, these results rebute the hypothesis that a better survival in GIIG with improved resection is attributable to a more favorable molecular profile. Rather, they plead in favor of an independent role of maximal resection per se, especially in GIIGs with more aggressive behavior according to their 1p19 status.
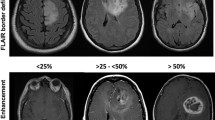
From a functional point, the reason why 1p19q codeleted GIIG are significantly less amenable to maximal resection are beyond the scope of our study. However, we could hypothesize that EOR is partly related to the tumor location: interestingly, previous reports demonstrated a significant correlation between the topographic repartition of GIIG within the brain and their molecular pattern [34, 35]. Another explanation might be relative to a more diffuse et infiltrative behavior of these tumors. Indeed, studies comparing MRI patterns of intact 1p19q and co-deleted 1p19q gliomas reported that the former had a sharp and smooth border whereas the second ones had an indistinct border [36, 37]. Logically, sharp margins were more amenable to gross total resection [38]. Finally, a larger tumor volume at diagnosis in codeleted GIIG could also be hypothesized due to later discovery—because of a less aggressive profile with a slower growth rate [33].
Ki67 and EOR
In 198 patients we observed a statistically “weak” correlation of a higher proliferative activity as indicated by the Ki67 index to a higher EOR. As stated with 1p19q, it is interesting to observe that GIIG with a potentially more aggressive behaviour could be resected to a higher extent. This is another argument supporting the independent favorable impact of maximal resection on the natural history of GIIG.
IDH1/p53 and EOR
Within the frame of the large patient cohort of this study, IDH1 and p53 could not be shown to be correlated to the EOR. Knowing the major prognostic factor of IDH1 in GIIG, as demonstrated in the recent literature [7–9], this lack of correlation is also in agreement with the independant role of EOR on prognosis.
It is important to note that we analyzed the correlation of the EOR to single molecular genetic markers instead of relating the EOR to described clusters of molecular genetic alterations [39]. Concerning the clusters of genetic alterations, the observations in our study cohort basically confirm the results of Labussière et al. But if we would have correlated the EOR to clusters of molecular genetic alterations instead to single factors, we would have lost the discrimination that the EOR is correlated to the 1p19q status—but interestingly not to the IDH1 status. This observation may potentially add aspects to the current discussion on the interrelation of 1p19q and IDH1, but the molecular genetic background of this phenomenon is beyond the scope of this study.
Taken together, these findings support the fact that early and maximal surgical resection should be considered as the first treatment option in GIIG in a systematic manner, independently of the molecular profile. The interrelationship to survival is an important issue which should be addressed in a future project.
Conclusions
For the first time to our knowledge, this study demonstrates in a large cohort of WHO grade II glioma patients that a higher EOR is not correlated to a molecular profile with better prognosis (as 1p19q codeletion or IDH1 mutation). Therefore, this result rebutes the hypothesis that the better survival reported in the modern literature in GIIG patients benefiting from a maximal EOR could be attributable to a more favorable genetic profile. Therefore, our study underscores the value of an optimized surgical resection, especially for the non-1p19q deleted GIIG subgroup with a basically inferior prognosis.
References
van den Bent MJ, Snijders TJ, Bromberg JE (2012) Current treatment of low grade gliomas. Memo 5:223–227
Bryszewski B, Tybor K, Ormezowska EA, Jaskolski DJ, Majos A (2013) Rearrangement of motor centers and its relationship to the neurological status of low-grade glioma examined on pre- and postoperative fMRI. Clin Neurol Neurosurg 115:2464–2470
Takahashi S, Jussen D, Vajkoczy P, Picht T (2012) Plastic relocation of motor cortex in a patient with LGG (low grade glioma) confirmed by NBS (navigated brain stimulation). Acta Neurochir (Wien) 154:2003–2008
Leu S, von Felten S, Frank S, Vassella E, Vajtai I, Taylor E, Schulz M, Hutter G, Hench J, Schucht P, Boulay JL, Mariani L (2013) IDH/MGMT-driven molecular classification of low-grade glioma is a strong predictor for long-term survival. Neuro Oncol 15:469–479
Daniels TB, Brown PD, Felten SJ, Wu W, Buckner JC, Arusell RM, Curran WJ, Abrams RA, Schiff D, Shaw EG (2011) Validation of EORTC prognostic factors for adults with low-grade glioma: a report using intergroup 86-72-51. Int J Radiat Oncol Biol Phys 81:218–224
Zhao J, Ma W, Zhao H (2014) Loss of heterozygosity 1p/19q and survival in glioma: a meta-analysis. Neuro Oncol 16:103–112
Kim W, Liau LM (2012) IDH mutations in human glioma. Neurosurg Clin N Am 23:471–480
Cohen AL, Holmen SL, Colman H (2013) IDH1 and IDH2 mutations in gliomas. Curr Neurol Neurosci Rep 13:345
Lewandowska MA, Furtak J, Szylberg T, Roszkowski K, Windorbska W, Rytlewska J, Jóźwicki W (2014) An analysis of the prognostic value of IDH1 (isocitrate dehydrogenase 1) Mutation in polish glioma patients. Mol Diagn Ther 18:45–53
Kim YH, Nobusawa S, Mittelbronn M, Paulus W, Brokinkel B, Keyvani K, Sure U, Wrede K, Nakazato Y, Tanaka Y, Vital A, Mariani L, Stawski R, Watanabe T, De Girolami U, Kleihues P, Ohgaki H (2010) Molecular classification of low-grade diffuse gliomas. Am J Pathol 177:2708–2714
Johannessen AL, Torp SH (2006) The clinical value of Ki-67/MIB-1 labeling index in human astrocytomas. Pathol Oncol Res 12:143–147
Torp SH (2002) Diagnostic and prognostic role of Ki67 immunostaining in human astrocytomas using four different antibodies. Clin Neuropathol 21:252–257
You G, Sha ZY, Yan W, Zhang W, Wang YZ, Li SW, Sang L, Wang Z, Li GL, Li SW, Song YJ, Kang CS, Jiang T (2012) Seizure characteristics and outcomes in 508 Chinese adult patients undergoing primary resection of low-grade gliomas: a clinicopathological study. Neuro Oncol 14:230–241
Capelle L, Fontaine D, Mandonnet E, Taillandier L, Golmard JL, Bauchet L, Pallud J, Peruzzi P, Baron MH, Kujas M, Guyotat J, Guillevin R, Frenay M, Taillibert S, Colin P, Rigau V, Vandenbos F, Pinelli C, Duffau H (2013) Spontaneous and therapeutic prognostic factors in adult hemispheric World Health Organization Grade II gliomas: a series of 1097 cases: clinical article. J Neurosurg 118:1157–1168
Pallud J, Audureau E, Blonski M, Sanai N, Bauchet L, Fontaine D, Mandonnet E, Dezamis E, Psimaras D, Guyotat J, Peruzzi P, Page P, Gal B, Párraga E, Baron MH, Vlaicu M, Guillevin R, Devaux B, Duffau H, Taillandier L, Capelle L, Huberfeld G (2014) Epileptic seizures in diffuse low-grade gliomas in adults. Brain 137:449–462
Jakola AS, Myrmel KS, Kloster R, Torp SH, Lindal S, Unsgård G, Solheim O (2012) Comparison of a strategy favoring early surgical resection vs a strategy favoring watchful waiting in low-grade gliomas. JAMA 308:1881–1888
Ius T, Pauletto G, Isola M, Gregoraci G, Budai R, Lettieri C, Eleopra R, Fadiga L, Skrap M (2014) Surgery for insular low-grade glioma: predictors of postoperative seizure outcome. J Neurosurg 120:12–23
Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha S, Tihan T, Vandenberg S, McDermott MW, Berger MS (2008) Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J Clin Oncol 26:1338–13345
Yordanova YN, Moritz-Gasser S, Duffau H (2011) Awake surgery for WHO Grade II gliomas within “noneloquent” areas in the left dominant hemisphere: toward a “supratotal” resection. J Neurosurg 115:232–239
Soffietti R, Baumert BG, Bello L, von Deimling A, Duffau H, Frénay M, Grisold W, Grant R, Graus F, Hoang-Xuan K, Klein M, Melin B, Rees J, Siegal T, Smits A, Stupp R, Wick W (2010) Guidelines on management of low-grade gliomas: report of an EFNS-EANO Task Force. Eur J Neurol 17:1124–1133
De Witt Hamer PC, Robles SG, Zwinderman AH, Duffau H, Berger MS (2012) Impact of intraoperative stimulation brain mapping on glioma surgery outcome: a meta-analysis. J Clin Oncol 30:2559–2565
Duffau H, Lopes M, Arthuis F, Bitar A, Sichez JP, Van Effenterre R, Capelle L (2005) Contribution of intraoperative electrical stimulations in surgery of low grade gliomas: a comparative study between two series without (1985–1996) and with (1996–2003) functional mapping in the same institution. J Neurol Neurosurg Psychiatry 76:845–851
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P (2007) The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114:97–109
Goze C, Mansour L, Rigau V, Duffau H (2013) Distinct IDH1/IDH2 mutation profiles in purely insular versus paralimbic WHO Grade II gliomas. J Neurosurg 118:866–872
Vet JA, Bringuier PP, Schaafsma HE, Witjes JA, Debruyne FM, Schalken JA (1995) Comparison of P53 protein overexpression with P53 mutation in bladder cancer: clinical and biologic aspects. Lab Invest 73:837–843
Anker L, Ohgaki H, Ludeke BI, Herrmann HD, Kleihues P, Westphal M (1993) p53 protein accumulation and gene mutations in human glioma cell lines. Int J Cancer 55:982–987
Louis DN, von Deimling A, Chung RY, Rubio MP, Whaley JM, Eibl RH, Ohgaki H, Wiestler OD, Thor AD, Seizinger BR (1993) Comparative study of p53 gene and protein alterations in human astrocytic tumors. J Neuropathol Exp Neurol 52:31–38
Peraud A, Kreth FW, Wiestler OD, Kleihues P, Reulen HJ (2002) Prognostic impact of TP53 mutations and P53 protein overexpression in supratentorial WHO grade II astrocytomas and oligoastrocytomas. Clin Cancer Res 8:1117–1124
Cribari-Neto F, Zileis A (2010) Beta Regression in R. J Stat Soft 34:1–24
Duffau H (2012) The challenge to remove diffuse low-grade gliomas while preserving brain functions. Acta Neurochir (Wien) 154:569–574
Duffau H, Gatignol P, Mandonnet E, Capelle L, Taillandier L (2008) Intraoperative subcortical stimulation mapping of language pathways in a consecutive series of 115 patients with Grade II glioma in the left dominant hemisphere. J Neurosurg 109:461–471
Capelle L, Oei P, Teoh H, Hamilton D, Palmer D, Low I, Campbell G (2009) Retrospective review of prognostic factors, including 1p19q deletion, in low-grade oligodendrogliomas and a review of recent published works. J Med Imaging Radiat Oncol 53:305–309
Goze C, Bezzina C, Goze E, Rigau V, Maudelonde T, Bauchet L, Duffau H (2012) 1P19Q loss but not IDH1 mutations influences WHO grade II gliomas spontaneous growth. J Neurooncol 108:69–75
Goze C, Rigau V, Gibert L, Maudelonde T, Duffau H (2009) Lack of complete 1p19q deletion in a consecutive series of 12 WHO grade II gliomas involving the insula: a marker of worse prognosis? J Neurooncol 91:1–5
Laigle-Donadey F, Martin-Duverneuil N, Lejeune J, Crinière E, Capelle L, Duffau H, Cornu P, Broët P, Kujas M, Mokhtari K, Carpentier A, Sanson M, Hoang-Xuan K, Thillet J, Delattre JY (2004) Correlations between molecular profile and radiologic pattern in oligodendroglial tumors. Neurology 63:2360–2362
Megyesi JF, Kachur E, Lee DH, Zlatescu MC, Betensky RA, Forsyth PA, Okada Y, Sasaki H, Mizoguchi M, Louis DN, Cairncross JG (2004) Imaging correlates of molecular signatures in oligodendrogliomas. Clin Cancer Res 10:4303–4306
Jenkinson MD, du Plessis DG, Smith TS, Joyce KA, Warnke PC, Walker C (2006) Histological growth patterns and genotype in oligodendroglial tumours: correlation with MRI features. Brain 129:1884–1891
Spena G, D’Agata F, Panciani PP, Buglione di Monale M, Fontanella MM (2013) Supratentorial gliomas in eloquent areas: which parameters can predict functional outcome and extent of resection? PLoS One 8:e80916
Labussière M, Idbaih A, Wang XW, Marie Y, Boisselier B, Falet C, Paris S, Laffaire J, Carpentier C, Criniere E, Ducray F, El Hallani S, Mokhtari K, Hoang-Xuan K, Delattre JY, Sanson M (2010) All the 1p19q codeleted gliomas are mutated on IDH1 or IDH2. Neurology 74:1886–1890
Acknowledgments
This work was supported by the Research Fund of the University of Basel and the Voluntary Academic Society of Basel.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cordier, D., Gozé, C., Schädelin, S. et al. A better surgical resectability of WHO grade II gliomas is independent of favorable molecular markers. J Neurooncol 121, 185–193 (2015). https://doi.org/10.1007/s11060-014-1623-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-014-1623-y