
Abstract
Objectives
The medical home model is a widely accepted model of team-based primary care. We examined five components of the medical home model in order to better understand their unique contributions to child health outcomes.
Methods
We analyzed data from the 2016–2017 National Survey of Children’s Health (NSCH) to assess five key medical home components – usual source of care, personal doctor/nurse, family-centered care, referral access, and coordinated care – and their associations with child outcomes. Health outcomes included emergency department (ED) visits, unmet health care needs, preventive medical visits, preventive dental visits, health status, and oral health status. We used multivariate regression controlling for child characteristics including age, sex, primary household language, race/ethnicity, income, parental education, health insurance coverage, and special healthcare needs.
Results
Children who were not white, living in non-English households, with less family income or education, or who were uninsured had lower rates of access to a medical home and its components. A medical home was associated with beneficial child outcomes for all six of the outcomes and the family-centered care component was associated with better results in five outcomes. ED visits were less likely for children who received care coordination (aOR 0.81, CI 0.70–0.94).
Conclusions for Practice
Our study highlights the role of key components of the medical home and the importance of access to family-centered health care that provides needed coordination for children. Health care reforms should consider disparities in access to a medical home and specific components and the contributions of each component to provide quality primary care for all children.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
What is Already Known on this Subject
The medical home model for children is associated with quality primary care and improved child health outcomes, but medical home access is characterized by disparities. Evidence is limited regarding which components of the medical home model contribute to its success.
What this Study adds
Examining five components of the medical home showed consistent association between specific components and child outcomes. Our results highlight the importance of family-centered and coordinated care and addressing ongoing disparities in access. Understanding the role of medical home components contributes to the refinement of the model and can inform health care policy efforts to improve health equity for all children.
Introduction
In the late 1960s, the medical home model of care was originally developed for children with special health care needs as a way to improve care coordination for a complex set of medical needs that require additional support for children and families (Kilo & Wasson, 2010; Sia et al., 2007). By the late 1970s, the medical home was viewed as a model of care for children more broadly. The American Academy of Pediatrics (AAP) issued its first policy statement on the medical home in 1992, defining the model as providing care that is accessible, family-centered, continuous, comprehensive, coordinated, compassionate, and culturally effective. In the early 2000s, the medical home gained traction as a model for care for people of all ages. Because medical home initiatives have been heterogeneous in goals, designs, settings, and outcomes, identifying key components is important in order to guide policy decisions that affect primary care (Jimenez et al., 2021; Sinaiko et al., 2017). The medical home provides valuable guidance as a conceptual model, but as a multicomponent intervention, the evidence base for its efficacy is limited by variation in or lack of information about its implementation. Understanding the unique contributions of each component of the medical home model and disparities in access will support further refinement of effective and equitable primary care.
Currently, the Medicaid and Children’s Health Insurance Program (CHIP) programs have indicated growing interest in refining the model for the purposes of improving health outcomes for children and reducing health disparities through payment reform (Demeester et al., 2017; Price et al., 2020). Many new methodologies are being developed in the Medicaid and CHIP programs, which serve a disproportionate share of low-income children, who experience worse health outcomes than children in families with greater household income. While medical home status may be assessed by health care providers, a strength of survey data is to evaluate medical home access from a family perspective and investigate the association with child outcomes. The National Survey of Children’s Health (NSCH) provides information on access to a medical home as defined by family experiences of five medical home components, along with a rich set of child demographics, health care utilization, and health status.
To date, very few studies have examined which components of the medical home have the greatest impact on child outcomes (Fleary, 2019; Long et al., 2013). Several studies have focused on disparities in access to the medical home and its components (Diao et al., 2017; Kan et al., 2016; Lichstein et al., 2018; Weller et al., 2020; Zickafoose & Davis, 2013). These analyses found significant disparities and challenges across subpopulations of children in accessing the medical home and its components for effective care. Children were more likely to have a medical home if they were white or lived in households with greater income, higher levels of parental education, or English as the primary household language. However, less is known about the impact of specific medical home components on child health outcomes. We evaluated access to medical home and its components and the association between components and a range of health outcomes, including emergency room (ED) visits, unmet care needs, preventive medical and dental visits, overall health status, and oral health status.
Methods
We studied the health outcomes of children with a medical home or specific medical home components compared to those without a medical home or specific components. Study data were from the 2016–2017 National Survey of Children’s Health (NSCH), a nationally representative cross-sectional survey of noninstitutionalized children aged 0–17. The NSCH is directed by the Health Resources and Services Administration’s Maternal and Child Health Bureau (MCHB). Since 2016, the redesigned NSCH has been conducted as a mail and web-based survey by the Census Bureau, which is subject to appropriate ethical standards including informed consent. This survey provides comprehensive data on children’s physical health, mental health, and access to primary care, and characteristics of children and their families, including whether the child has special health care needs. A series of items in this survey captures family experiences related to medical home access, based on the AAP definition.(CAHMI, n.d.-a). We used publicly available, de-identified data via the Child and Adolescent Health Measurement Initiative (CAHMI), which is supported by MCHB.
Data and sample. We analyzed two years of pooled data from the 2016–2017 NSCH to examine health outcomes of U.S. children. Combining multiple years of data is recommended by CAHMI for the most reliable estimates (CAHMI, n.d.-b). The NSCH oversamples children with special health care needs (CSHCN) and children aged 0–5. The survey subject was one randomly selected child per household, and all responses were provided by parents or caregivers. The study sample included children with at least one medical care visit in the past 12 months (n = 61,572) representing 85.8% of the total pooled sample of 71,721).
Outcomes. Outcomes included health care utilization: ED visits (≥ 1 during the past year); unmet health care needs (yes/no to unmet medical, dental, hearing, vision, or mental health need); preventive medical visit during the past year; preventive dental visit during the past year (limited to ages 1–17); and health status measures: parent-reported child health (fair or poor versus excellent, good, or very good), parent-reported oral health, queried as “teeth condition” (fair or poor versus excellent, good, or very good; limited to ages 1–17).
Medical home. The medical home was a composite measure based on 16 survey items in the 2016–2017 survey; our definition of the medical home and components followed guidance from MCHB and CAHMI (CAHMI, n.d.-a, n.d.-b, 2009). Children with a medical home had a personal doctor/nurse, usual source of care, family-centered care, no problems getting needed referrals, and effective care coordination when needed. The NSCH assesses five of the seven AAP criteria with these components, including family-centered care and care coordination. Family-centered care also encompasses compassionate and culturally effective care, and comprehensive care is delineated by access to a usual source of care and referrals. Children who met criteria for at least one medical home component and for whom the remainder of responses were either missing or legitimately skipped were considered to have a medical home, and those with a negative response to any component were categorized as not having a medical home.
Following the survey design, evaluation of family-centered care was limited to those who reported a medical visit in the past year, including sick-child or well-child visits, hospitalizations, or any other medical care. Care was considered family-centered if the respondent answered “usually” or “always” to five survey items: the provider spends enough time with the child, listens carefully, is sensitive to family values/customs, gives the specific information needed, and the family feels like a partner in the child’s health care. Access to referrals was defined by reports that the child had no referral problems (big or small), if they needed a referral. Coordinated care was assessed for children with a past year medical visit, and children who saw less than two providers were assumed to not need coordination. Care coordination could include communication between doctors when needed, between schools and doctors when needed, or getting needed help with care coordination. Care coordination and referral access were recoded as variables with three categories (e.g., received the component, did not need the component, or needed and did not receive the component), and the other components were recoded as binary variables. This approach retained children who did not need coordination or referrals in the denominator, which resulted in a consistent sample population across regression models and allowed us to adjust for all model components in the main analysis.
Covariates. We controlled for selected child characteristics including age (age 0–5, 6–11, 12–17), sex (male/female), race/ethnicity (white non-Hispanic, Hispanic, Black non-Hispanic, other non-Hispanic), primary language spoken at home (English or non-English), poverty (< 100% of the federal poverty level [FPL], 100–199% FPL, 200–399% FPL, ≥ 400% FPL), parental education (less than high school, high school, some college, college degree), CSHCN (binary variable based on the 5-item screener used by MCHB (Bethell et al., 2002)), and health insurance coverage (uninsured, public only, private). Children with both public and private insurance were coded as private coverage.
Analyses. We tabulated the sociodemographic and health characteristics of children with at least one medical visit by medical home component status and by study outcomes, and we conducted bivariate analyses with design-based F statistics. We used multivariate logistic regression to assess the association between (1) having a medical home and health outcomes, and (2) having each of the medical home components and health outcomes. In the main analysis, all components were included in the model in order to quantify the contribution of each component, adjusting for the other four components and covariates. To evaluate the robustness of our results, we included a sensitivity analysis using an alternative model. In this approach, we used a separate model for each component.
We used complete case analysis and dropped observations with missing data for medical home, primary language spoken at home, parental education, and health insurance coverage (unweighted n = 61,572 after 3.7% of the sample was dropped due to missingness). Missing data for poverty were imputed in each year of data by the Census Bureau, and we followed the same approach as CAHMI and used a single imputed value for income (i1) (CAHMI, n.d.-b). Analyses were conducted with Stata version 16 using survey weights to account for the complex sample design (StataCorp, College Station, TX). Statistical tests were conducted at a 95% confidence level (p-value < 0.05).
Results
Sample characteristics associated with access to medical home components and study outcomes (unadjusted results). About half (51.4%) of all children with a medical visit in the past year had a medical home (Table 1).
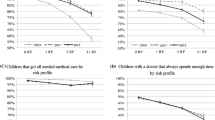
In the bivariate analysis, having a medical home was more common among white non-Hispanic children and children who had English as the primary household language, greater family income, greater parental education, no special health care needs, and private health insurance coverage. For children in families with income ≥ 400% federal poverty level (FPL) or whose parents had a college degree, the rate of having a medical home was over 60% (63.1% and 60.8%, respectively). Among children with lower household income or parental education, medical home rates were only about half to two thirds of the rates seen by children in families with income ≥ 400% FPL or with a college-educated parent. Not having a medical home was associated with being Black or Hispanic (41.4% and 40.0%, respectively), living in non-English households (35.1%), having lower family income or education, being a CSHCN (44.4%), and being uninsured or enrolled in public health insurance programs (29.7% and 40.8%, respectively). Components of the medical home showed very similar patterns of association with child characteristics.
Of the six study outcomes, ED utilization and unmet needs showed particularly wide variation by child characteristics. (Table 2)
The prevalence of having at least one ED visit ranged from 15.8 to 34.1% among children with family income < 100% FPL and ≥ 400%, respectively. Conversely, the prevalence of unmet health care needs varied from 4.6 to 1.0% for children in the lowest and highest income categories. However, reported unmet needs were the greatest for uninsured children at 10.1%. Low household income, low parental education, and being uninsured were negatively associated with all six child outcomes. Four outcomes varied significantly by race/ethnicity; compared with white children, Black and Hispanic children reported a greater frequency of ED visits and unmet health care needs, and worse overall health and oral health status.
Multivariate results. Having a medical home was associated with better outcomes in all six of the child health and health care utilization measures we examined (Table 3).
Of the five medical home components examined, family-centered care was the most frequently associated with better outcomes when comparing children with and without a given component (Table 4).
Family-centered care was associated with significantly better results in five of six measures: unmet health care needs, preventive medical or dental visits, overall health, and oral health status. Children with coordinated care were more likely to have better outcomes in four of six measures (ED visits, unmet needs, overall health, and oral health status) than children without coordinated care who needed these services. Notably, ED visits were less likely for children who received care coordination (aOR 0.81, CI 0.70–0.94). Better overall child health status and oral health status were associated with two of the five components: family-centered care (aOR 0.58, CI 0.36–0.93; aOR 0.58, CI 0.43–0.79, respectively) and care coordination (aOR 0.40, CI 0.25–0.64; aOR 0.55, CI 0.41–0.73, respectively). Children with a personal doctor/nurse were more likely to receive preventive medical and dental visits than children without a usual provider (aOR 1.31, 1.02–1.69, aOR 1.41, 1.22–1.63, respectively). Children with referral access were less likely to have unmet care needs than those who faced referral problems (aOR 0.48, CI 0.32–0.72). Having a usual source of care was not associated with significant results for any outcome.
In both the medical home model and the component model (Tables 3 and 4), many of the bivariate associations between child characteristics and outcomes shown in Table 2 remained significant after adjusting for covariates, which indicates socioeconomic disparities in these outcomes. Greater household income was associated with reduced likelihood of ED visits and unmet health care needs, and better general health and oral health status. Greater parental education was associated with fewer ED visits, more preventive dental visits, and better health and oral health status. Compared with white children, Black children were more likely to have an ED visit or report unmet needs.
Our sensitivity analysis supported the robustness of our main analysis (Table 5).
Generally, the alternative approach of modeling components separately resulted in a larger number of significant associations between the components and better outcomes. This suggests that our main analysis was more conservative than the sensitivity analysis, which was similar to the regression model structure used in a previous study with similar aims (Fleary, 2019). No outcomes that were significant in the main analysis lost significance in the alternative approach.
Discussion
Our study highlights two components of the medical home model that were strongly associated with children’s health status and health care utilization: family-centered care and care coordination. Our results provide evidence for the important role of these components in clinical practice and health policy reforms. Family-centered care was associated with better health outcomes in all of the measures we examined with the exception of ED visits, which were less likely among children with coordinated care. Care coordination and family-centered care were also associated with better child health and oral health status and fewer unmet health care needs.
Our study contributes to the growing body of research showing that children with a medical home are more likely to receive preventive medical or dental care, have fewer unmet care needs and emergency department visits, and have better overall health status (Akobirshoev et al., 2019; Strickland et al., 2011). Additionally, we extended the analysis to examine medical home components and a range of outcomes including preventive medical visits and dental visits and oral health using a robust analytic approach.
Our work also confirms the persistent disparities encountered in the use of the medical home model for the care of children (Tables 1 and 2) (Lichstein et al., 2018; Weller et al., 2020). Rates of medical home access were below 42% for Black and Hispanic children and those with non-English households, low family income or education, or public health insurance coverage. Among uninsured children, less than 30% had a medical home and the prevalence of having a usual source of care varied by over 30% points across child subgroups.
Uninsured children reported the lowest rates of having a usual source of care (64.6%) and referral access (61.6%), and children with insurance coverage were significantly less likely to report unmet health care needs and more likely to have preventive medical and dental visits (Tables 1 and 4). Similarly, although having a personal doctor/nurse was only associated with two of the six outcomes (preventive medical and dental visits), the prevalence of this component varied substantially by child characteristics, with the lowest rates reported by uninsured children (58.4%).
Our results suggest that the beneficial associations of having a medical home are primarily driven by family-centered and coordinated care. Our findings also have important implications in the context of value-based purchasing and other Medicaid/CHIP payment reform strategies. A recent study by Price et al. suggests that payment reform should include elements which incent effective use of primary care and specialty pediatric services, and mechanisms to strengthen the family-patient-provider relationship (2020). Our results provide evidence to support this approach, since coordinated care and family-based care supports the effective use of services and a positive family-patient-provider dynamic. As such, these components are important parts of a potential medical model to improve population health under payment reform.
Several current health care quality and payment reform initiatives involve medical homes for children enrolled in Medicaid/CHIP. The Affordable Care Act (ACA) included $25 million in planning grants for states to develop health care homes for Medicaid enrollees, including children, with chronic conditions (Association of Maternal and Child Health Programs, 2016). More recently, in 2020, the Center for Medicare and Medicaid Innovation (CMMI) launched the $126 million Integrated Care for Kids initiative which is a shared-savings payment model now being piloted in seven states (Centers Medicare and Medicaid Services (CMMI), n.d.). The findings from our analysis can inform these payment models by pointing to which medical home components should be included to most effectively achieve improved health outcomes among children. For example, while care coordination is often a required element of emerging medical home payment models, our study also illustrates the importance of medical homes that support the role of providers working in partnership with the family. Medicaid/CHIP coverage of enhanced services is especially needed for children from non-English or low-income households and children who are immigrants, uninsured, CSHCN, Black, or Hispanic; these populations are less likely to receive family-centered care and care coordination (Table 1) (Kan et al., 2016).
Our study has several limitations. Parental report is subject to recall bias and may reflect other factors influencing the respondents’ perceptions that are not measured. For example, parents facing barriers to care may be less likely to report a need for care (e.g., for referrals, care coordination, or unmet care needs). Additionally, when parents reported that referrals or care coordination were not needed, this does not demonstrate that such care would have been available if it had been perceived as needed. Thus, we may be underestimating rates of access to the medical home and its components. Another limitation was that data were cross-sectional and we were not able to examine causality. For example, having a usual provider or usual source of care might require continuity over time in order to improve health status. Longitudinal and prospective studies are needed to address these issues. Lastly, we did not examine interaction or additive effects of the components, which would be a useful area of future research.
Conclusions for Practice and Policy
The medical home model of care for children is well established as providing high quality care. We identified two specific components of the model that are associated with beneficial child outcomes – family-centered care and care coordination. Our results have implications for further development of the medical home model and for the new payment reform models being developed in the Medicaid and CHIP programs that focus on total costs of care. As the pediatric medical home model moves into contracting language that defines new payment models of care, it will be important to understand that the medical home is a multicomponent model and its successful implementation must include support for family experiences of care and care coordination. This information is needed both for the providers who are organizing models of care and for payers who are determining payments based on agreed upon cost and quality targets. Finally, much more work needs to be done to improve health equity in assuring access to needed care for vulnerable populations. Medicaid and CHIP outreach and enrollment strategies and use of the medical home model across populations are critical to reducing health disparities.
Data Availability
Data are publicly available.
Code Availability
Stata software code available upon request.
References
Akobirshoev, I., Parish, S., Mitra, M., & Dembo, R. (2019). Impact of Medical Home on Health Care of Children With and Without Special Health Care Needs: Update from the 2016 National Survey of Children’s Health. Maternal and Child Health Journal, 0123456789. https://doi.org/10.1007/s10995-019-02774-9
Association of Maternal and Child Health Programs. (2016). Health Reform & the Medical Home Model. Fact Sheet. Medical Homes ACA FAct Sheet - Final.pdf. http://www.amchp.org/Policy-Advocacy/health-reform/resources/Documents/
Bethell, C. D., Read, D., Stein, R. E. K., Blumberg, S. J., Wells, N., & Newacheck, P. W. (2002). Identifying children with special health care needs: Development and evaluation of a short screening instrument. Ambulatory Pediatrics, 2(1), 38–48. https://doi.org/10.1367/1539-4409(2002)002%3C0038:ICWSHC%3E2.0.CO;2
CAHMI. (n.d.-a). Medical Home Portal. Retrieved December 1 (2020). from https://action.cahmi.org/browse/medicalhome
CAHMI. (n.d.-b). National Survey of Children’s Health. Retrieved December 1 (2020). from https://www.childhealthdata.org
CAHMI (2009). Measuring Medical Home for Children and Youth
Centers Medicare and Medicaid Services (CMMI). (n.d.). Integrated Care for Kids (InCK) Model. Retrieved June 1 (2021). from https://innovation.cms.gov/innovation-models/integrated-care-for-kids-model
Demeester, B. R. H., Xu, L. J., Nocon, R. S., Cook, S. C., Ducas, A. M., & Chin, M. H. (2017). By Rachel H. DeMeester, Lucy J. Xu, Robert S. Nocon, Scott C. Cook, Andrea M. Ducas, and Marshall H. Chin. June, 1133–1139
Diao, K., Tripodis, Y., Long, W. E., & Garg, A. (2017). Socioeconomic and Racial Disparities in Parental Perception and Experience of Having a Medical Home, 2007 to 2011–2012. Academic Pediatrics, 17(1), 95–103. https://doi.org/10.1016/j.acap.2016.07.006
Fleary, S. A. (2019). Association Between the Medical Home Model of Care and Demographic Characteristics in US Children. Clinical Pediatrics, 58(3), 270–281. https://doi.org/10.1177/0009922818813568
Jimenez, G., Matchar, D., Koh, G. C. H., & Car, J. (2021). Multicomponent interventions for enhancing primary care: A systematic review. British Journal of General Practice, 71(702), E10–E21. https://doi.org/10.3399/bjgp20X714199
Kan, K., Choi, H., & Davis, M. (2016). Immigrant families, children with special health care needs, and the medical home. Pediatrics, 137(1), https://doi.org/10.1542/peds.2015-3221
Kilo, C. M., & Wasson, J. H. (2010). Practice redesign and the patient-centered medical home: History, promises, and challenges. Health Affairs, 29(5), 776–778. https://doi.org/10.1377/hlthaff.2010.0012
Lichstein, J. C., Ghandour, R. M., & Mann, M. Y. (2018). Access to the medical home among children with and without special health care needs. Pediatrics, 142(6), https://doi.org/10.1542/peds.2018-1795
Long, W. E., Cabral, H. J., & Garg, A. (2013). Are components of the medical home differentially associated with child health care utilization, health, and health promoting behavior outcomes? Clinical Pediatrics, 52(5), 423–432. https://doi.org/10.1177/0009922813479161
Price, J., Brandt, M. L., & Hudak, M. L. (2020). Principles of Financing the Medical Home for Children. Pediatrics, 145(1), https://doi.org/10.1542/peds.2019-3451
Sia, C., Tonniges, T. F., Osterhus, E., Taba, S., Sia, C., Tonniges, T. F., & Osterhus, E. (2007). Downloaded from www.pediatrics.org at Dartmouth College Library on November 16, 2007. https://doi.org/10.1542/peds.113.5.S1.1473
Sinaiko, A. D., Landrum, M. B., Meyers, D. J., Alidina, S., Maeng, D. D., Friedberg, M. W., Kern, L. M., Edwards, A. M., Flieger, S. P., Houck, P. R., Peele, P., Reid, R. J., McGraves-Lloyd, K., Finison, K., & Rosenthal, M. B. (2017). Synthesis of research on patient-centered medical homes brings systematic differences into relief. Health Affairs, 36(3), 500–508. https://doi.org/10.1377/hlthaff.2016.1235
Strickland, B. B., Jones, J. R., Ghandour, R. M., Kogan, M. D., & Newacheck, P. W. (2011). The medical home: Health care access and impact for children and youth in the United States. Pediatrics, 127(4), 604–611. https://doi.org/10.1542/peds.2009-3555
Weller, B. E., Faubert, S. J., & Ault, A. K. (2020). Youth Access to Medical Homes and Medical Home Components by Race and Ethnicity. Maternal and Child Health Journal, 24(2), 241–249. https://doi.org/10.1007/s10995-019-02831-3
Zickafoose, J. S., & Davis, M. M. (2013). Medical home disparities are not created equal: Differences in the medical home for children from different vulnerable groups. Journal of Health Care for the Poor and Underserved, 24(3), 1331–1343. https://doi.org/10.1353/hpu.2013.0117
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
Dr. Mac Arthur conceptualized and designed the study, analyzed the data, drafted the initial manuscript, and reviewed and revised the manuscript. Dr. Blewett conceptualized and designed the study and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Approval:
Not applicable.
Note
de-identified, publicly available data does not constitute human subjects research and does not require IRB review.
Consent to Participate:
Not applicable.
Consent for Publication:
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Arthur, N.S.M., Blewett, L.A. Contributions of Key Components of a Medical Home on Child Health Outcomes. Matern Child Health J 27, 476–486 (2023). https://doi.org/10.1007/s10995-022-03539-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-022-03539-7