
Abstract
Objective WHO and UNICEF recommend cup feeding for neonates unable to breastfeed in low-resource settings. In developed countries, cup feeding in lieu of bottle feeding in the neonatal period is hypothesized to improve breastfeeding outcomes for those initially unable to breastfeed. Our aim was to synthesize the entire body of evidence on cup feeding. Methods We searched domestic and international databases for original research. Our search criteria required original data on cup feeding in neonates published in English between January 1990 and December 2014. Results We identified 28 original research papers. Ten were randomized clinical trials, 7 non-randomized intervention studies, and 11 observational studies; 11 were conducted in developing country. Outcomes evaluated included physiologic stability, safety, intake, duration, spillage, weight gain, any and exclusive breastfeeding, length of hospital stay, compliance, and acceptability. Cup feeding appears to be safe though intake may be less and spillage greater relative to bottle or tube feeding. Overall, slightly higher proportions of cup fed versus bottle fed infants report any breastfeeding; a greater proportion of cup fed infants reported exclusive breastfeeding at discharge and beyond. Cup feeding increases breastfeeding in subgroups (e.g. those who intend to breastfeed or women who had a Caesarean section). Compliance and acceptability is problematic in certain settings. Conclusions Further research on long-term breastfeeding outcomes and in low-resource settings would be helpful. Research data on high risk infants (e.g. those with cleft palates) would be informative. Innovative cup feeding approaches to minimize spillage, optimize compliance, and increase breastfeeding feeding are needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Significance
What is known about this subject? Two Cochrane reviews summarized 4 randomized clinical trials and found that women who cup versus bottle or tube fed their infant were more likely to fully breastfeed at discharge. Cup feeding had no effect on any breastfeeding but extended length of stay.
What this study adds? Twenty-four studies on cup feeding cover questions and clinical outcomes that have never been synthesized. We provide the first comprehensive review of original research on a wide range of cup feeding outcomes (physiologic stability, intake, breastfeeding, length of stay, compliance, acceptability) and propose new areas for research.
Introduction
Breastfeeding offers the best nutrition and is the optimal method for feeding neonates [1, 2]. Unfortunately, not all infants can be breastfed. Preterm infants, infants with an oral cleft or other anomalies, and infants with metabolic, neurologic, or developmental immaturities may encounter breastfeeding difficulties [3, 4]. In some cases, infants are unable to breastfeed because the mother is unavailable, sick, or has nipple damage [4, 5].
Cup feeding has a long history of being a neonatal feeding option [6–8]. In high-resource settings, nasogastric tubes and bottles are the default tools of choice when an infant is unable to breastfeed. Feeding cups in high-resource settings are used by some in the short-term to deliver supplemental feeding and to avoid ‘nipple confusion’, a theory that exposure to artificial nipples interferes with a neonate’s ability to breastfeed [9]. WHO and UNICEF recommend cup feeding in low-resource settings where water quality is poor and electricity unreliable [4, 10–12]. In these settings, nasogastric tubes may not be available and bottles have crevices that promote infection [13, 14]. Cups are easier to keep clean and are less likely than bottles to be used for long-term storage of milk which can facilitate bacterial contamination. Cup feeding may supplement breastfeeding, minimize exposure to nasogastric tubes, or serve as a long-term feeding solution for those never able to breastfeed [3, 4, 15]. Advantages of cup feeding include enhanced bonding, a greater sense of maternal control and confidence, the ability to engage other family members in the infant’s care, and freeing up nursing staff when caregivers conduct feedings [3, 4, 15–19]. Studies propose that cup feeding provides the infant positive oral, tactile, and auditory stimulation, exposure to the smell and taste of breast milk, tongue and motor skill experience, and the ability to control feeding pace [3–5, 8, 17]. Reported concerns about cup feeding include that it is too slow, prone to spillage, results in insufficient intake [19–21], or that milk poured from a cup into the infant’s mouth increases the risk of choking or aspiration [5, 19].
Two Cochrane reviews evaluated the extent to which cup feeding and avoidance of bottle-feeding in the neonatal period influenced breastfeeding outcomes [22, 23]. These reviews included four of ten published RCTs. The outcomes in the Cochrane reviews were limited. There are 24 studies on cup feeding that have never been summarized, including a recently published RCT [24] and numerous observational studies that examine outcomes not in the reviews. Synthesizing the breadth of outcomes has important implications for understanding cup feeding and identifying gaps in knowledge. We conducted a systematic review of neonatal cup feeding to synthesize the broad body of evidence and identify gaps to facilitate research.
Methods
We broadly included all studies with original data collection on cup feeding in the neonatal period conducted in humans and written in English between 1990 and 2014. We searched the MEDLINE database and a global health database, CABdirect, for all papers that met these criteria. Search terms included cup*, palada* (paladai), suthi* AND newborn or infant AND human AND English from January 1, 1990 to December 2014. The search was last conducted February 27, 2015. The symbol * denotes the root word of the search. A paladai (also referred to as a suthi) is an infant feeding cup used in India which is a small (10 ml) metal cup with a long slender pour spout (Fig. 1) [14]. Research on spoon feeding was excluded.

A type of feeding cup known as a paladai used in South India
We reviewed abstracts to identify original research articles. We also reviewed the reference lists of all included papers and abstracted additional articles for review. All studies including case reports, case series, observational studies, non-randomized intervention studies and RCTs were included. We abstracted study design and country, type of participants, gestational of age, number of participants, comparison, and outcomes into Excel. To the extent available, we reported original results including means, mean differences, p values, prevalence relative risks, and 95 % confidence intervals (CIs). When not calculated, we used raw frequencies to calculate these statistics to facilitate comparisons. We grouped studies according to study design because RCTs typically have less bias that observational studies and by gestational age since effects in the outcomes we report (e.g. physiologic measures, breastfeeding outcomes) may differ based on gestational age.
Results
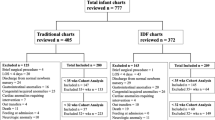
We reviewed 342 abstracts and 681 references to identify 28 studies that meet inclusion criteria (Fig. 2). There were ten RCTs, seven non-randomized intervention studies, and eleven observational studies (Table 1). Five studies employed a cross-over design where the infant acted as her own control. [21, 25–28] Four studies evaluated provider and/or caregiver preferences [29–32]. All RCTs except for one [33] were conducted in high-resource countries. Six studies were conducted in upper-middle income countries (e.g. Brazil, Turkey) and five studies were in lower-middle income countries (e.g. India, Egypt); no studies were in the least developed countries (Table 1) [34]. Twenty-three studies employed a comparison group using a different feeding method. Nineteen compared a cup to a bottle, six compared breastfeeding to a cup and/or bottle, two compared Paladai to bottle-feeding, and one compared Paladai to tube feeding (Table 1). Most studies did not describe the cup or bottle used [20, 24, 26, 28, 30, 35–39]. The scope of research was broad and fell into five domains: (1) Physiologic stability and safety; (2) Intake, duration, spillage and weight gain/loss; (3) Breastfeeding outcomes; (4) Duration of hospitalization; and (5) Feeder compliance and acceptability. We also ordered studies by topic (see Online Resource 1).

Flow chart of abstracts, references and papers reviewed to identify eligible studies
Physiologic Stability and Safety
Many clinical practitioners express concern that cup feeding may increase adverse events such as aspiration, or oxygen desaturation [5, 19, 40]. Overall, compared to bottle feeding, cup feeding tended to have higher oxygen saturation levels, and a smaller fraction of infants experiencing oxygen saturation <90 and <85 % and equivalent or less elevation of heart and respiratory rates (Table 2). There were no consistently reported adverse physiologic events across studies. Collins et al. [41] reported no adverse events in early premature infants. Marinelli et al. [25] found no differences in choking, spitting up or apnea, or bradycardia between cup and bottle fed infants (all p values > 0.05), although these were noted in both groups of neonates. Aloysius, et al. (n = 15) reported that 73 % had stress cues when paladai feeding compared to 20 % bottle feeding, but there was no difference in preterm neonate stress cues (p = 0.67) [26]. A case report proposes infant aspiration can occur with an improper feeding technique, but a recent RCT with 522 infants reported no apnea or aspiration [10, 24]. A case series of the paladai in very preterm infants found 12/68 feedings had desaturation but 7 feedings occurred in 2 infants [42].
Intake, Duration of Feeding, Spillage, and Weight Gain
Clinical practitioners express concern that cup feeding may not provide sufficient intake, is time-consuming, and that spillage results in decreased intake [19]. All comparative studies that examined intake reported lower intake with a cup compared to bottle or tube (Table 3). Of the five studies with hypothesis testing, only one reported a statistically significant lower intake with cup feeding. Findings on feeding duration were variable. Two studies reported cup feeding took more time [25, 26]; two less time [33, 43]; and one the same time [24] as bottle feeding. Cup feeding took less time than breastfeeding [27]. Cup feeding was associated with a threefold increase in spillage compared to a bottle [21, 26] and more spillage than the paladai [21]. These comparisons were statistically stable (p values < 0.01) [21, 26]. The mean spillage when using a cup was high (25–39 %) [16, 21]. No studies found statistically significant differences in newborn weight loss/gain with the cup versus bottle feeding [24, 33, 39–41, 44]. Data from six studies on weight gain were not tabulated because of variability in measures reported (see Online Resource 1) [24, 33, 39–41, 44].
Breastfeeding Outcomes
The primary reason to cup feeding in high-resource settings is to optimize the likelihood the infant will successfully initiate and sustain breastfeeding. Consequently, the extent to which cup, as compared to bottle, influences breastfeeding in infancy is a primary outcome of interest. We identified eleven reports on breastfeeding outcomes; seven of these were RCTs [24, 33, 36, 38, 39, 41, 44] and four were observational studies [3, 30, 35, 45]. The most commonly reported breastfeeding outcomes were any or exclusive/full breastfeeding. Exclusive breastfeeding was similarly defined by most studies as receiving all food from the breast [3, 35, 36, 38, 41, 44]. Two studies classified infants who had taken vitamins or minerals as exclusively breastfed [24, 41]. Two studies defined ‘full breastfeeding’ and ‘almost exclusive breastfeeding’ as breastfeeding with infrequent feedings (e.g. <1 per day) of other liquids such as water or herbal drinks [35, 44].
Breastfeeding was reported at or near the time of hospital discharge and up to 6 months of age (Table 4). Any breastfeeding at hospital discharge was reported by eight studies. All of the studies that employed a comparison group reported a greater proportion of cup-fed as compared to bottle-fed infants with any breastfeeding at hospital discharge, but the differences were mostly small and only the largest RCT [24] showed statistically significant differences [24, 30, 33, 36, 41]. Findings were similar when any breastfeeding outcomes post-discharge up to 6 months were examined. Other statistically significant differences for cup versus bottle fed infants for any breastfeeding were in subgroups (e.g. mothers who had a Caesarean section).
Most measures of exclusive breastfeeding were collected around the time of hospital discharge. Of the six studies that employed a comparison group [24, 35, 36, 38, 41, 44], all but one small study [38] reported a higher prevalence or longer duration of exclusive breastfeeding in cup versus bottle fed infants. The larger [24, 41] but not the smaller [36, 38] RCTs in preterm infants reported statistically significant differences in exclusive breastfeeding at discharge. The only RCT to examine exclusive breastfeeding at 3 and 6 months post discharge reported cup fed infants were more likely to exclusively breastfeed than bottle-fed infants (p < 0.001) [24]. Statistically significant differences were reported in subgroups (Table 4).
Length of Stay in Hospital
Four studies reported on the length of stay in hospital for cup versus bottle or tube fed infants (Table 5). Four of the 5 studies on length of stay in hospital, including a large RCT, reported stays were similar or shorter for cup versus breastfeeding infants and none of the differences in length of stay were statistically significant (Table 5). One RCT in Australia reported extended hospital stays among cup fed infants relative to bottle fed infants [41], which has raised concern that cup-feeding increases cost and demand for limited resources [22, 23, 41]. However, the authors reported no difference in duration of hospital stay among those who complied with their assigned feeding method (p = 0.27), and found that length of stay after supplemental feeding by cup or bottle was started was similar for infants fed by cup versus bottle (12 vs 11 days, p = 0.05) [41].
Compliance and Acceptability
Non-compliance with cup feeding was the primary limitation of the RCT in Australia that examined cup versus bottle-feeding on breastfeeding outcomes; 56 % of participants assigned cup feeding group were given a bottle [41]. Problems reported included spillage, taking too much time, the infant not feeding well, and staff refusing to feed an infant with a cup [41]. In the United Kingdom, mothers assigned cup feeding were 3.6 times more likely to withdraw from the trial than mothers assigned bottle feeding (p = 0.01) [36]. In contrast, an RCT in Switzerland found 9.5 % assigned to a cup feeding protocol requested a bottle or had trouble cup feeding [39]. In an RCT in Turkey, 8.7 % were non-compliant with the cup compared to 6.8 % non-compliant with a bottle (p = 0.39) [24]. A study in the US reported similar levels of compliance with 89 % and 93 % using the assigned cup or bottle respectively [44]. These studies suggest >90 % compliance with cup feeding in certain settings may be feasible.
Five studies reported on provider opinions about cup feeding [21, 26, 29, 31, 32]. The largest study (N = 103) in Canada found beliefs about ‘nipple confusion’ and safety and utility of cup feeding varied by provider type [32]. A study in the UK found that nurses found cup feeding more difficult than bottle feeding [26]. More than 50 % of nurses in Sweden reported difficulties with a new cup feeding protocol; hygiene rules were not followed and nurses thought cup feeding may not meet intake requirements [31]. An ethnographic study in the UK reported nurses thought the cup could be messy, though the majority liked the cup because it allowed the infant to ‘control the rate at which they [were] fed’. Most thought cup feeding should be given by a clinical provider—not the mother [29]. A study in India reported nurses unanimously preferred the paladai over the bottle and cup without a pour spout and thought it took less time and effort of the infant to feed than the other methods [21]. The primary disadvantage of the paladai is that, because it is made of steel, it sometimes cuts an infant’s lip [21].
Discussion
We identified 28 original research articles on cup feeding in newborn infants. All studies were initiated after birth in a hospital setting. Neonatal cup feeding appears to be physiologically safe though intake may be less and spillage greater relative to bottle or tube feeding. Similar proportions of cup and bottle fed infants were breastfed at hospital discharge but cup fed infants appear more likely to be exclusively breastfed. Among certain subgroups, cup versus bottle feeding was statistically significantly associated with an increase in any and exclusive breastfeeding. Compliance and acceptability varied and may be problematic in certain settings.
In terms of safety, evidence on respiratory stability suggests that cup feeding is as or more stable than bottle-feeding in pre- and full term neonates that are generally healthy. A greater proportion of preterm and normal term infants with oxygen desaturation were bottle-fed suggesting infants cup feeding may be more physiologically stable [25, 33, 43]. Future studies that evaluate strategies to optimize physiologic stability while cup feeding may be informative and have particular relevance for infants with respiratory or cardiac problems. Cup size and shape may influence physiologic stability of cup feeding and may benefit from investigation.
Studies reporting on intake and spillage consistently demonstrate that cup fed infants may take in less and spill more than bottle-fed infants. Though cup fed infants may have lower intake, most studies did not report a statistically significant difference in weight loss. Differences in weight loss measures make it difficult to compare studies. Standardization of this measure would benefit future studies. Bottle fed infants having greater intake and greater oxygen desaturation is consistent with our hypothesis of a faster feeding pace with bottle-feeding. Future research could test this theory by comparing cup to bottles with different flow rates. Most studies that examined intake and spillage did not report on weight loss and vice versa. Future research that comprehensively evaluates intake, spillage, weight loss, and weight gain over time in a single RCT of cup versus bottle feeding could address whether lower intake translates into poorer weight gain.
Although most studies reported no difference in ‘any breastfeeding’ at or after hospital discharge, cup fed infants were more likely to be exclusively breastfed than bottle-fed infants. Our findings on ‘any breastfeeding’ are consistent with two Cochrane reviews [22, 23]. These reviews examined the same four RCTs on cup feeding (one also included a study on nasogastric tubes) [33, 36, 38, 41]. Although not as rigorous as those in the Cochrane series, our findings included many additional studies may provide insight for future research [3, 30, 35, 39, 44]. The conclusion by one review that ‘cup feeding confers no significant benefit in maintaining breastfeeding beyond hospital discharge’ may be premature. The recent RCT from Turkey found exclusive breastfeeding was statistically significant higher at 6 months post discharge in cup fed infants [24]. Exclusive breastfeeding for the first 6 months of life has wide ranging, well-established benefits to mother and infant. Future RCTs should consider examining exclusive breastfeeding through 6 months post-hospital discharge. Several studies identified subgroups for whom cup feeding may be helpful (e.g. mothers who delivered via cesarean section or roomed-in). Since the cesarean rate is relatively high in high- and middle-income countries and is increasing in low-incomes countries this may be an important consideration in breastfeeding promotion globally [46, 47]. Although post hoc findings from subgroup analyses should be viewed with caution, they do provide directions for future research.
Existing research indicates non-compliance with cup feeding is multifactorial and may involve nursing staff training and compliance, mother’s intention, and an infant’s ability to breastfeed. Nurses and parents do not always find cup feeding acceptable [29, 36, 41]. That those who complied with cup-feeding in one RCT were 21 times more likely to breastfeed than those who complied with bottle-feeding [41] suggests that cup feeding, when used as prescribed, could be a potent solution to transitioning preterm infants to breastfeeding. The mechanism by which cup feeding may enhances breastfeeding remains unclear. One explanation is that cup feeding avoids the ‘nipple confusion’ introduced by a bottle [4]. Another possibility we posit is that cup feeding is inconvenient or inefficient enough to motivate mothers to do everything possible to breastfeed. Lower intake and greater spillage with cup feeding likely affects compliance and acceptability. Clinical staff and parent acceptance may vary by context. For example, cup feeding is acceptable and even preferable to bottles in India and Kenya [21, 48]. In Europe and other high-resource settings, hospitals that routinely use and train providers on cup feeding may have greater compliance than hospitals that do not prescribe cup feeding [8, 24, 48]. In middle-income countries (e.g. Turkey) cup feeding occurs (Table 1), however there is little information on the acceptability of cup feeding in these settings. It is known that some report poor compliance even with extensive training [41]. Reasons for non-compliance and methods to improve cup feeding compliance should be investigated further.
Extended hospital stay was the primary reason the Cochrane reviews did not recommend cup feeding. The recommendation is based on a single RCT conducted in Australia [41]. Given there was no difference in length of stay in those who complied with their assigned feeding method in this study, length of hospital stay may not be due to cup feeding per se, but dissatisfaction with the method that led to a transition to another feeding method [41]. That the four other studies, including a recent large RCT from Turkey not in the Cochrane review found minimal differences in length of hospital stay suggests this recommendation may need to be reconsidered [24, 30, 35, 40].
UNICEF and WHO programs and guidelines recommend hand expression of breast milk and cup feeding for infants unable to breastfeed in low-resource and emergency settings [12, 49–52]. Cup feeding may reduce intake and increase spillage however this needs to be carefully weighed against alternatives such as the availability of nasogastric tubes or the risks of bottle feeding in low-resource settings [53, 54]. Certain cup shapes or sizes may improve outcomes. For example, the paladai compared to a generic cup minimizes spillage [21]. A cup feeder’s training and skill may also influence intake and spillage. In low-resource settings, cup feeders are often mothers rather than nurses. Ensuring caregivers have the skill to optimally feed their infant may have a large impact on outcomes and infant survival. Current practices, compliance, and acceptability of cup feeding should be assessed in low-resource settings. Research on cup feeding is needed in low-resource settings such as Sub-Saharan Africa where cup feeding is the standard of care for infants unable to breastfeed, particularly since there is little existing research from these settings and it is the WHO and UNICEF recommendation.
There are limitations to the existing evidence. Few studies report on comparable outcomes. Within each domain, there was substantial variation in measures, making it difficult to compare studies. Several studies had methodological limitations. Some did not employ a comparison group [16, 42, 45] and many had small sample sizes [10, 16, 26–28, 38, 42]. Because most studies did not describe the cup or bottle used, it was impossible to evaluate the impact of cup design on outcomes. Shape, material, and ergonomics of feeding tools may influence intake, spillage, and feeding efficiency. Only one RCT analyzed their data using the gold standard intent-to-treat analysis [41]. Most non-randomized studies conducted unadjusted analysis [3, 20, 30, 40]. Not adjusting for confounding factors in observational studies (e.g. gestational age) could result in incorrect inference. Our search was limited to studies published in English and so we may have missed some information.
Given the wide reaching and well-established benefits of breast milk and long-term breastfeeding, perhaps the most important area of investigation is to evaluate exclusive long-term breastfeeding outcomes (e.g. 3 and 6 months), and breastfeeding outcomes in subgroups such as mothers who intend to breastfeed or had a Cesarean section. Additional research in low-resource settings is needed to optimize cup feeding in these settings. Lastly, research in infants with anomalies (cleft palate) that interfere with breastfeeding, particularly in low-resource settings, is needed to establish whether or not cup feeding is superior to other options (especially bottle) in these infants. Innovative approaches to cup feeding that optimize physiologic stability, milk intake, weight gain, and improve acceptability could potentially have a large impact on the long term health of infants with breastfeeding difficulties globally.
References
World Health Organization (WHO). (2013). Pan America Health Organization (PAHO). Canada: Beyond Survival.
Horta, B. L., Victora, C. G., & World Health Organization (WHO). (2013). Short-term effects of breastfeeding: A systematic review on the benefits of breastfeeding on diarrhoea and pneumonia mortatlity. Geneva: World Health Organization.
Lang, S., Lawrence, C. J., & Orme, R. L. (1994). Cup feeding: An alternative method of infant feeding. Archives of Disease in Childhood, 71(4), 365–369.
Thorley, V. (2005). Cup-feeding. Australian breastfeeding association. East Malvern. https://www.breastfeeding.asn.au/bfinfo/cup-feeding. Accessed April 27, 2015.
Kuehl, J. (1997). Cup feeding the newborn: What you should know. The Journal of Perinatal & Neonatal Nursing, 11(2), 56–60.
Fredeen, R. C. (1948). Cup feeding of newborn infants. Pediatrics, 2(5), 544–548.
Davis, H. V., Sears, R. R., et al. (1948). Effects of cup, bottle and breast feeding on oral activities of newborn infants. Pediatrics, 2(5), 549–558.
Lang, S. (1994). Cup-feeding: An alternative method. Midwives Chronicle & Nursing Notes, 107, 171–176.
Neifert, M., Lawrence, R., & Seacat, J. (1995). Nipple confusion: toward a formal definition. The Journal of Pediatrics, 126(6), S125–S129.
Thorley, V. (1997). Cup feeding: Problems created by incorrect use. Journal of Human Lactation, 13(1), 54–55.
Edmond, K., & Bahl, R. (2006). Optimal feeding of low-birth-weight infants: technical review. Geneva: Department of Child and Adolescent Health and Development, World Health Organization.
World Health Organization (WHO). (2009). Baby-friendly hospital initiative: Revised, updated and expanded for integrated care. Section 3: Breastfeeding promotion and support in a baby-friendly hospital. A 20-hour course for maternity staff. Geneva: World Health Organization. http://www.unicef.org/nutrition/files/BFHI_2009_s3.1and2.pdf. Accessed 21 Mar 2016.
Surjono, D., Ismadi, S. D., Suwardji, et al. (1980). Bacterial contamination and dilution of milk in infant feeding bottles. Journal of Tropical Pediatrics, 26(2), 58–61.
Armstrong, H. (1998). Research in action; techniques of feeding infants-the case for cup feeding. Cajanus, 31(4), 178–185.
Ritchie, J. F. (1998). Immature sucking response in premature babies: Cup feeding as a tool in increasing maintenance of breast. Journal of Neonatal Nursing, 4(2), 13–17.
Dowling, D. A., Meier, P. P., DiFiore, J. M., et al. (2002). Cup-feeding for preterm infants: mechanics and safety. Journal of Human Lactation, 18(1), 13–20.
Lanese, M. G. (2011). Cup feeding-a valuable tool. Journal of Human Lactation, 27(1), 12–13. doi:10.1177/0890334410396668.
Jones, E. (1994). Breastfeeding in the preterm infant. Modern Midwife, 1, 22–26.
Samuel, P. (1988). Cup feeding: How and when to use it with term babies. Practising Midwife, 1(12), 33–35
Huang, Y. Y., Gau, M. L., Huang, C. M., et al. (2009). Supplementation with cup-feeding as a substitute for bottle-feeding to promote breastfeeding. Chang Gung Medical Journal, 32(4), 423–431.
Malhotra, N., Vishwambaran, L., Sundaram, K. R., et al. (1999). A controlled trial of alternative methods of oral feeding in neonates. Early Human Development, 54(1), 29–38.
Flint, A., New, K., & Davies, M. W. (2007). Cup feeding versus other forms of supplemental enteral feeding for newborn infants unable to fully breastfeed. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD005092.pub2.
Collins, C. T., Makrides, M., Gillis, J., et al. (2008). Avoidance of bottles during the establishment of breast feeds in preterm infants. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD005252.pub2.
Yilmaz, G., Caylan, N., Karacan, C. D., et al. (2014). Effect of cup feeding and bottle feeding on breastfeeding in late preterm infants: A randomized controlled study. Journal of Human Lactation, 30(2), 174–179. doi:10.1177/0890334413517940.
Marinelli, K. A., Burke, G. S., & Dodd, V. L. (2001). A comparison of the safety of cupfeedings and bottlefeedings in premature infants whose mothers intend to breastfeed. Journal of Perinatology, 21(6), 350–355. doi:10.1038/sj.jp.7210539.
Aloysius, A., & Hickson, M. (2007). Evaluation of paladai cup feeding in breast-fed preterm infants compared with bottle feeding. Early Human Development, 83(9), 619–621. doi:10.1016/j.earlhumdev.2006.12.004.
Freer, Y. (1999). A comparison of breast and cup feeding in pre-term infants: Effect on physiological parameters. Journal of Neonatal Nursing, 5(1), 16–21.
Lopez, C. P., Chiari, B. M., Goulart, A. L., et al. (2014). Assessment of swallowing in preterm newborns fed by bottle and cup. CoDAS, 26(1), 81–86.
Cloherty, M., Alexander, J., Holloway, I., et al. (2005). The cup-versus-bottle debate: a theme from an ethnographic study of the supplementation of breastfed infants in hospital in the United kingdom. Journal of Human Lactation, 21(2), 151–162. doi:10.1177/0890334405275447.
Brown, S. J., Alexander, J., & Thomas, P. (1999). Feeding outcome in breast-fed term babies supplemented by cup or bottle. Midwifery, 15(2), 92–96.
Nyqvist, H. K., & Strandell, E. (1999). A cup feeding protocol for neonates: Evaluation of nurses and parents’ use of two cups. Journal of Neonatal Nursing, 5(2), 31–36.
Al-Sahab, B., Feldman, M., Macpherson, A., et al. (2010). Which method of breastfeeding supplementation is best? The beliefs and practices of paediatricians and nurses. Paediatrics & Child Health, 15(7), 427–431.
Rocha, N. M., Martinez, F. E., & Jorge, S. M. (2002). Cup or bottle for preterm infants: Effects on oxygen saturation, weight gain, and breastfeeding. Journal of Human Lactation, 18(2), 132–138.
World Bank. (2015). World econonmic situation and prospects: Country classification. http://www.un.org/en/development/desa/policy/wesp/wesp_archive/2015wesp_full_en.pdf. Accessed April 27, 2015.
Abouelfettoh, A. M., Dowling, D. A., Dabash, S. A., et al. (2008). Cup versus bottle feeding for hospitalized late preterm infants in Egypt: A quasi-experimental study. International Breastfeeding Journal, 3, 27. doi:10.1186/1746-4358-3-27.
Gilks, J. (2004). Improving breast feeding rates in preterm babies: Cup feeding versus bottle feeding. Journal of Neonatal Nursing, 10(4), 118–120.
Gomes, C. F., Trezza, E. M., Murade, E. C., et al. (2006). Surface electromyography of facial muscles during natural and artificial feeding of infants. Journal of Pediatrics, 82(2), 103–109. doi:10.2223/JPED.1456.
Mosley, C., Whittle, C., & Hicks, C. (2001). A pilot study to assess the viability of a randomised controlled trial of methods of supplementary feeding of breast-fed pre-term babies. Midwifery, 17(2), 150–157. doi:10.1054/midw.2000.0244.
Schubiger, G., Schwarz, U., & Tonz, O. (1997). UNICEF/WHO baby-friendly hospital initiative: does the use of bottles and pacifiers in the neonatal nursery prevent successful breastfeeding? Neonatal Study Group. European Journal of Pediatrics, 156(11), 874–877.
Rekha, S., Rao, S. D., & Fernandez, M. (1996). Two different methods for feeding low birth weight babies. Indian Pediatrics, 33(6), 501–503.
Collins, C. T., Ryan, P., Crowther, C. A., et al. (2004). Effect of bottles, cups, and dummies on breast feeding in preterm infants: A randomised controlled trial. BMJ, 329(7459), 193–198. doi:10.1136/bmj.38131.675914.55.
Dalal, S. S., Mishra, S., Agarwal, R., et al. (2013). Feeding behaviour and performance of preterm neonates on Paladai feeding. Acta Paediatrica, 102(4), e147–e152. doi:10.1111/apa.12148.
Howard, C. R., de Blieck, E. A., ten Hoopen, C. B., et al. (1999). Physiologic stability of newborns during cup- and bottle-feeding. Pediatrics, 104(5 Pt 2), 1204–1207.
Howard, C. R., Howard, F. M., Lanphear, B., et al. (2003). Randomized clinical trial of pacifier use and bottle-feeding or cupfeeding and their effect on breastfeeding. Pediatrics, 111(3), 511–518.
Gupta, A., Khanna, K., & Chattree, S. (1999). Cup feeding: An alternative to bottle feeding in a neonatal intensive care unit. Journal of Tropical Pediatrics, 45(2), 108–110.
Cavallaro, F. L., Cresswell, J. A., Franca, C. G., et al. (2013). Trends in ceasarean delivery by country and wealth quintile: cross-sectional survys in southern Asia and sub-Saharan Africa. Bulletin of the World Health Organization (WHO), 91(12), 914D–922D.
World Health Organization. (2010). The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: Overuse as a barrier to universal coverage. In World Health Report (pp. 1–31). Geneva: World Health Organization. http://www.who.int/healthsystems/topics/financing/healthreport/30C-sectioncosts.pdf. Accessed 21 Mar 2016.
Musoke, R. N. (1990). Breastfeeding promotion: Feeding the low birth weight infant. International Journal of Gynaecology and Obstetrics, 31(Suppl1), 57–59.
World Health Organization. (2010). Essential newborn care course: Trainer’s guide: Module 4, session 11 (pp. 138–144). Geneva: World Health Organization. http://apps.who.int/iris/bitstream/10665/70540/3/WHO_MPS_10.1_Training_file_eng.pdf. Accessed 21 Mar 2016.
World Health Organization. (2003). Managing newborn problems: A guide for doctors, nurses, and midwives. Geneva: World Health Organization.
World Health Organization. (2004). Guiding principles for feeding infants and young children during emergencies. http://www.who.int/nutrition/publications/guiding_principles_feedchildren_emergencies.pdf. Accessed 21 Mar 2016.
World Health Organization, The Aga Khan University, The Partnership for Maternal NCH. (2011). Essential interventions, commodities and guidelines for reproductive, maternal, newborn and child health: A global review of the key interventions related to reproductive, maternal, newborn and child health (RMNCH). Geneva: World Health Organization. http://apps.who.int/medicinedocs/documents/s21666en/s21666en.pdf. Accessed 21 Mar 2016.
World Health Organization. (2011). Guidelines on optimal feeding of low-birthweight infants in low-and middle-income countries. Geneva: World Health Organization. http://www.who.int/maternal_child_adolescent/documents/9789241548366.pdf?ua=1. Accessed 21 Mar 2016.
World Health Organization. (2008). The international code of marketing of breast-milk substitutes: Frequently asked questions. Geneva: World Health Organization. http://www.who.int/nutrition/publications/Frequently_ask_question_Internationalcode.pdf. Accessed 21 Mar 2016.
Franca, E. C., Sousa, C. B., Aragao, L. C., & Costa, L. R. (2014). Electromyographic analysis of masseter muscle in newborns during suction in breast, bottle or cup feeding. BMC Pregnancy Childbirth, 14, 154.
Gomes, C. F., Gois, M. L., Oliveira, B. C., Thomson, Z., & Cardoso, J. R. (2014). Surface electromyography in premature infants: A series of case reports and their methodological aspects. The Indian Journal of Pediatrics, 81(8), 755–759.
Acknowledgments
Dr. McKinney and Ms. Rue were supported by NIH NCATS Grant #2KL2TR000421-06. This work was also supported by the Jean Renny Endowment for Craniofacial Research, Seattle Children’s Hospital Craniofacial Center.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare they have no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
McKinney, C.M., Glass, R.P., Coffey, P. et al. Feeding Neonates by Cup: A Systematic Review of the Literature. Matern Child Health J 20, 1620–1633 (2016). https://doi.org/10.1007/s10995-016-1961-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-016-1961-9