
Abstract
Autoantibodies against thyroid peroxidase (TPO); described initially as thyroid microsomal antigen, are found in most of the patients with autoimmune thyroid disorders. The present study comprised of development, optimization and validation of ‘sandwich’ radioassay for the measurement of TPOAb in human serum. The standardized TPOAb radioassay has maximum binding of 25–30%, non-specific binding of < 0.4%, analytical sensitivity of approximately around 1 IU/ml, acceptable intra- and inter-assay %CV, with a standard working range up to 1400 IU/ml. The in-house developed assay is simple, robust and cost-effective, and therefore can be used for routine measurement of TPOAb in clinical samples.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In autoimmune thyroid disorders, humoral and cell-mediated mechanisms are the prime underlying causative factors responsible for the cellular damage followed by thyroid gland dysfunction. The sensitized T-lymphocytes, autoantibodies or both bind to the follicular cell membranes resulting in cell lysis and inflammatory reactions ensuing cellular damage. An action of stimulating or blocking autoantibodies on cell membrane receptors alters the thyroid gland function [1]. Measurement of thyroid autoantibodies helps in the evaluation of patients with autoimmune thyroid diseases (AITD). Three clinically significant principal thyroid autoantibodies are anti-thyroid peroxidase (TPOAb), anti-thyroglobulin (TgAb) and anti-TSH receptor (TRAb) [2]. Though circulating TgAb and TPOAb are considered to be the early indicators of AITD [3, 4], the measurement of TgAb has more significance in the detection of potential interferences in thyroglobulin (Tg) immunoassays and TPOAb being a significant serological hallmark of AITD [5, 6]. Human thyroid peroxidase (TPO) is a membrane-bound glycosylated protein composed of 933 amino acids (110 kDa) present at the apical pole on the thyrocytes; facing colloidal lumen, where the main steps of hormonogenesis take place. Thus, thyroid peroxidase (TPO) is the crucial enzyme in the synthesis of thyroid hormones essential for normal thyroid function [2]. TPO autoantibodies were initially described as anti-microsomal autoantibodies (AMA) since they were found to react with the crude preparations of thyroid cell membranes. TPOAb is present in > 90% of the patients with Hashimoto thyroiditis (HT), 85% of patients with Graves’ disease (GD) and in up to 26% of healthy subjects. However, the clinical significance of low TPOAb levels in euthyroid individuals is still unknown. Determination of TPOAb levels is one of the most important and sensitive tests not only required for the detection of AITD, but it also represents a risk factor for the development of autoimmune thyroiditis in several conditions [7]. The older class of immunoassays, generally defined as “the first generation” like AMA immunofluorescence and passive tanned red cell agglutination tests are still being used in addition to the newer, more sensitive competitive and non-competitive TPOAb immunoassays. These new “second generation” procedures represented by immunometric methods with a radioisotope, enzymatic, and luminescent tracers are quantitated in international units; using reference preparation MRC 66/387 and are gradually replacing the older AMA agglutination tests as they are quantitative, more sensitive and can easily be automated. However, wide variability in the analytical sensitivity and specificity of these new TPOAb methods persists [1]. Immunoassays based on the solid phase separation are favoured widely because of their ease of separation and amenability to automation, despite heavy consumption of coating reagent required for coupling. Due to this reason the antibody/antigen coated plastic tubes or 'coated tube' assay is the preferred solid phase assay system adopted by most of the commercial kit manufacturers. However, large-scale production of these coated tubes demands sophisticated technology with automatic equipment to ensure uniform coating and large quantities of coating material thereby making it expensive. In developing countries where the production sizes are often small, the use of solid phase assays based on antibodies/antigens adsorbed to magnetic particles probably offers the benefits of a solid phase system without sacrificing the ease of preparing the reagents or economy of small-scale procedures. Being a Nuclear Medicine Centre, our centre is equipped with the infrastructure for the development of isotopic kits for routine in-vitro patient services. The purpose of the present study was to develop and validate a simple and economical radioassay for TPOAb in human serum using magnetizable cellulose particles (as a solid support) as an import substitute for the commercial isotopic anti-TPO kit; for routine measurement of TPOAb at our centre. Present paper reports a classical one-step sandwich radioassay which involves the use of magnetizable cellulose iron oxide particles covalently linked with Protein A (solid phase immunosorbent) for the entrapment of TPOAb in patient’s serum sample by binding to the constant region of TPOAb, which is an IgG molecule; and later detected using radiolabeled recombinant TPO (125I-rTPO).
Experimental
Materials
Bovine serum albumin (BSA) and 1,1′-Carbonyldiimidazole (CDI) were from Sigma Chemical Company, USA; PD-10 columns (pre-packed with Sephadex G-25) were obtained from Amersham Biosciences, Magnetizable cellulose iron oxide particles from Scipac (M-100) and BRIT Laboratories, Mumbai, India, Carrier free 125I as Sodium Iodide was obtained from BARC, Recombinant Thyroid Peroxidase from Prospec, Recombinant Protein A from BioVision, (California, US), Anti-TPO RIA kit (Immunotech, Beckman and Coulter; France).
Preparation of capture immunosorbent solid phase
For the activation process, 0.5 g of magnetic particles were taken in a container and washed thrice using 20 ml distilled water followed by 20 ml acetone for 3 times. To this particles, 200 mg of CDI was added and suspended in 1 ml acetone and rotated for 1 h at room temperature. Additionally, the particles were washed 4 times each with 20 ml acetone and distilled water. Further, the magnetic particles were washed twice with coupling buffer (0.1 M borate buffer, pH 8). To the activated particles 10 mg of recombinant Protein A was added, and the volume was adjusted to 20 ml with coupling buffer. The suspension was kept on a rotator for overnight at room temperature. Next day, the particles were washed twice with 20 ml of coupling buffer followed by 0.6% ethanolamine in borate buffer. The suspension was rotated for 20 min, resuspended in 0.1 M acetate buffer, pH 4 and then rotated for another 20 min. The particles were washed twice with PBS containing 2% BSA and 0.01 g of sodium azide and adjusted the total volume to 250 ml with the same buffer. All the washing steps, as mentioned earlier were carried out using a magnetic separator. Magnetic particles coupled with Protein A were then stored at 8 °C till further use. The coupling efficiency of Protein A to magnetic particles was checked in terms of non-specific binding (NSB) (binding with TPOAb standard of 0 IU/ml concentration) and maximum binding (Bmax which is binding with TPOAb standard of 1400 IU/ml concentration).
Preparation of detector or tracer recombinant TPO
Radioiodinations of recombinant TPO were performed using 125I-NaI by Chloramine-T method [8] and Iodogen method [9] with minor modifications as detailed in Tables 1 and 2 respectively to obtain a specific activity of approximately 0.74 × 10–3 GBq/µg. Further, purification was carried out by gel filtration over Sephadex G-25 (PD-10 column) and purified fractions were pooled,diluted in PBS containing 2% BSA and stored in aliquots at − 20 °C for further evaluation in the assay. Total CPM of 70 × 103 was found to be ideal with minimum NSB and high maximum binding.
Preparation of TPOAb standards
Six different TPOAb standard pools with concentrations of 0 IU/ml, 5 IU/ml, 40 IU/ml, 120 IU/ml, 700 IU/ml and 1400 IU/ml containing 0.1% sodium azide as a preservative were prepared from left-over sera of patients with autoimmune thyroid disease visiting our laboratory for routine follow-up. These in-house prepared standards were calibrated against the secondary standards provided by the commercial Anti-TPO RIA kit from Immunotech. Calibrators are liquid, ready-to-use, and ensure calibration stability of about 60 days when aliquoted and preserved at − 20 °C. The broad dynamic range of 1.0–1400 IU/ml, reduces the need for sample dilution.
Optimized assay procedure
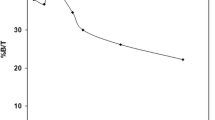
The optimized radioassay protocol for TPOAb measurement was established after the optimization of various assay parameters such as reaction kinetics, the concentration of Protein A coupled to magnetizable cellulose, amount of 125I labelled rTPO (tracer), the volume of standard/samples etc. to accomplish optimal sensitivity and assay range. Final assay procedure involved incubation of 5 μl of standards/sample along with 250 μl of Protein A coupled to magnetizable cellulose particles and 250 μl of 125I-rTPO for 4 h at room temperature with gentle shaking. At the end of the incubation, 2 ml of wash buffer (PBS containing 0.05% Tween-20) was added, and the assay tubes containing reaction mixture were placed on a magnetic rack for 15 min. The particles sedimented to form a firm pellet. The supernatant was discarded by gently inverting the rack. The radioactivity associated with the solid phase particles were measured using multi-well gamma counter calibrated for 125I. A standard curve was constructed by plotting %B/T (Y-axis) versus TPOAb concentration (X-axis) on a semi-log graph sheet. The TPOAb levels in test samples were estimated from the standard curve by interpolation. Standard curves obtained at different time intervals are depicted in Fig. 2. Using this standardized protocol, the performance of the assay was evaluated by studying the basic assay parameters like sensitivity, precision, working range, hook effect and method comparison.
Results and discussion
Unlike antibody coated tubes or microtiter plates, capture reagent prepared using magnetizable cellulose particles, as per the requirement, have flexibility in varying their concentration. The intelligent and extensive use of Protein A in the immunoassays has been as a ‘universal tracer’ and as a separating reagent [10]. Besides, magnetic particles tagged with Protein A can also serve as a ‘universal immunocapture’ solid phase reagent in the development of assays for autoantibodies, as it has the capability of binding to the Fc part of IgG. However, to avoid steric hindrance, it is essential to consider the size of the labelled molecule as it may overall affect the kinetics of the molecules resulting in a decreased binding. Assays designed for autoantibodies generally make use of purified antigens or monoclonal antibodies coated on various solid phases. To cater to the needs of the routine clinical application, TPO is required in large quantities for coating. However, it is challenging to obtain purified TPO in large amounts as it is a membrane-bound protein. Using either purified native or recombinant human TPO have, however, resulted in differences in the sensitivity and specificity of the methods [2]. Therefore, we tried to use recombinant Protein A for coupling to magnetizable cellulose particles which would make local production of these kits economical. BRIT, Mumbai and Scipac, UK manufactured particles were verified for their performance which yielded somewhat similar results with regard to %Bmax (21.19% and 26.81% respectively) and %NSB (0.24% and 0.32% respectively). Consequently, due to availability and suitability, BRIT manufactured particles were continued for the study.
Preparation of magnetizable cellulose particles showed 70–80% uptake of Protein A. The coupling efficiency was checked spectrophotometrically by measuring Protein A concentration before and after the coupling reaction. This magnetic particle suspension stored at 4 °C retained immunoreactivity for about 15 months. At our Centre magnetizable cellulose particles have also been used for the development of Tg radioimmunoassay (RIA) and immunoradiometric assay (IRMA) [5], and T4 RIA.
Both chloramine-T and iodogen methods used for the preparation of 125I-rTPO (Fig. 1) were found to be consistent and reproducible (Table 3) showing an insignificant difference between their %Bmax and %NSB. However, the iodogen method was chosen as a method of choice as it is published that it pose less damage to the proteins during radioiodination as compared to Chloramine-T method [10]. In addition, simplicity, effectiveness and versatility of iodogen makes it a reagent of choice for iodination of most proteins. Combination of trace amounts of rTPO for labelling and Protein A as an ‘immunocapture’ makes the assay unique and economical. This design of the test ensures both the sensitivity and specificity of the assay.

Elution profile of 125I-rTPO post radiolabeling with chloramine T and iodogen method
Standard curves were established for the assays performed at different time intervals by assaying graded amounts of TPOAb prepared in-house from left-over patient sera (Fig. 2). Due to the scarcity of the primary standard (MRC 66/387) they were calibrated against the secondary standards provided by the commercial kit. Now there is a call for the preparation of New International Reference Preparation for TPOAb as it was prepared and lyophilized almost five decades back.

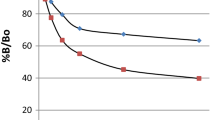
Calibration stability determined by constructing standard curves for TPOAb by plotting %B/T (Y-axis) versus TPOAb concentration (X-axis) at different time intervals (every 20 days) using in-house prepared standards calibrated against the commercial Anti-TPO RIA kit standards
Analytical sensitivity of the assay was determined by assaying ten tubes of zero TPOAb standard. Mean and the standard deviation was calculated for these ten zero standard tubes. Sensitivity was calculated by extrapolating Mean + 2SD (95% confidence) from the standard curve. Reproducibility of the radioassay was checked by assaying four serum samples with varying concentrations. The intra- and inter-assay variation was found to be < 7.2% and 12.8% respectively representing an acceptable precision (Table 4). The accuracy of the assays established for autoantibodies is generally deranged. Therefore, it is known that recovery and dilution tests may not provide satisfactory results. Human thyroglobulin and thyroid peroxidase may share common antibody epitopes in the serum of patients with AITD, thereby reacting simultaneously with both the analytes [11]. As a result, the cross-reactivity issue may be faced in poorly designed assays. We have protected this by formatting the assay design where 125I-rTPO is used as a tracer thereby making the test more specific.
The sandwich type of assays encounters the problem of hook effect or the prozone effect. The hook effect or the prozone effect occurs in an immunologic phenomenon where the efficacy of antibodies to form immune-complexes is decreased due to excess concentrations of a particular antibody or antigen (analyte to be measured) and is most prevalent in one-step (sandwich) immunoassays. In this, phenomenon, formation of immune-complexes stops increasing with greater concentrations of the analyte and then gradually decreases resulting in false negative value. To study this phenomenon in our assay system, we serially diluted (1:2 to 1:2000) a patient serum sample with TPOAb value of > 5000 IU/ml (concentration ascertained by commercial Anti-TPO RIA kit), using the hormone-free serum. A plateau was observed at 1:4 dilution, corresponding to a concentration of 1400 IU/ml, and a fall in TPOAb level subsequently, indicating hook effect. Therefore, the working range for the in-house developed radioassay was set up to 1400 IU/ml which can be comfortably used for the management of patients with autoimmune thyroid disorders. The issue of the hook effect can be managed to a certain degree by increasing the amount of capture reagent. Use of magnetizable cellulose particles as immunoadsorbents makes this convenient which is otherwise not possible with coated microtiter plates or tubes [12].
Using the developed method, TPOAb concentration was measured in 114 left-over serum samples of the patients with known autoimmune thyroid disorders. The TPOAb values thus obtained were compared with those values obtained by an established commercial kit (Immunotech, France) with an acceptable correlation (Y = 0.413x + 48.5 IU/ml; r = 0.714; p < 0.001) (Fig. 3).

Scatter plot for anti-TPO using in-house developed assay and Immunotech KIT in the patients with known autoimmune thyroid disorders
In the upcoming years, immunoassays will target on the assays with enhanced analytical sensitivity, specificity, simultaneous multiplexed capability, use of protein microarrays and microfluidics. The clinical practicality depends on the eminence of the tests used by the diagnostic laboratory. However, the selection of analysis depends upon the clinical setting and, higher sensitivity and specificity strongly depends on the cut-off value established by the research laboratory. Therefore, the centre should adopt an ideal diagnostic test that aims at achieving both, high sensitivity and specificity [13], and at the same time being economical too.
Conclusion
Present work describes a unique and novel assay format which shows the use of Protein A coupled with magnetic particles as a solid phase reagent in the development of assay for TPO autoantibodies using specific tracer. A trace amount of purified recombinant TPO is required for radiolabelling, making the test cost-effective with an additional advantage of flexibility in the use of magnetizable immunosorbent solid phase. The sensitivity, specificity, high precision and automation of the in-house developed radioassay make it perfectly suitable for the routine investigations. Conventionally, different kits for different autoantibodies demand specific purified antigens or monoclonal antibodies coated on various solid phases. Whereas our assay which proposes the use of ‘universal immunocapture’ format (for the detection of array of autoantibodies) would help in reducing overall time and cost during the kit production.
References
D’Aurizio F, Metus P, Polizzi AA, Villalta D, Ferrari A, Castello R, Giani G, Tonutti E, Bizzaro N, Tozzoli R (2015) Autoimmun Highlights 6(3):31–37
Sinclair D (2008) Autoimmunity 41(1):46–54
Gholve CS, Kumarasamy J, Kulkarni S, Rajan MGR (2017) Ind J Clin Biochem 32(1):39
Ojo OA, Ikem RT, Kolawole BA, Ojo OE, Ajala MO (2019) JEMDSA 24(3):92–97
Gholve CS, Kumarasamy J, Damle A, Kulkarni S, Rajan MGR (2016) Indian J Appl Res 6(3):468–472
Gholve CS, Kumarasamy J, Damle A, Kulkarni S, Venkatesh M, Banerjee S, Rajan MGR (2018) Ind J Clin Biochem. https://doi.org/10.1007/s12291-018-0768-4
Czarnocka B, Eschler DC, Godlewska M, Tomer Y (2013) Autoantibodies, 3rd edn. Elsevier BV, Amsterdam, pp 365–373
Greenwood FC, Hunter WM, Klopper A (1964) Br Med J 1(5374):22–24
Fraker PJ, Speck JC (1978) Biochem Biophys Res Commun 80:849–857
Chard T (1982) An introduction to radioimmunoassay and related techniques, 2nd edn. Elsevier Biomedical Press, Amsterdam
Estienne V, Duthoit C, Costanzo VD, Lejeune PJ, Rotondi M, Kornfeld S, Finke R, Lazarus JH, Feldt-Rasmussen U, Franke WG, Smyth P, D’Herbomez M, Conte-Devolx B, Persani L, Carella C, Jourdain JR, Izembart M, Toubert ME, Pinchera A, Weetman A, Sapin R, Carayon P, Ruf J (1999) Eur J Endocrinol 141:563–569
Rasmi RR, Shenoy KB, Sarnaik J, Kadwad VB, Somashekarappa HM, Sivaprasad N (2014) J Radioanal Nucl Chem 302:1271–1275
Hasson SS, Al-Balushi MS, Al-Jabri AA (2012) Asian Pac J Trop Dis 2:159–162
Acknowledgements
The authors are thankful to Dr. Vijay Kadwad, Sr. Manager, RPHP, BRIT, Mumbai for the supply of in-house produced magnetizable cellulose iron oxide particles.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gholve, C., Banerjee, S. & Kulkarni, S. Novel radioassay for anti-thyroperoxidase autoantibodies using protein A coupled magnetizable cellulose particles as an immunoadsorbent. J Radioanal Nucl Chem 323, 1041–1046 (2020). https://doi.org/10.1007/s10967-020-07023-w
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10967-020-07023-w