
Abstract
Although increasing numbers of children have socially transitioned to live in line with their gender identities, little is known about factors associated with their wellbeing. This study examines the associations between parent-reported family, peer, and school support for a youth’s gender identity, as well as an objective measure of state-level support, with parent-reported internalizing symptoms in 265 transgender youth (67.2% transgender girls, 32.8% transgender boys), ages 3–15 years (M = 9.41, SD = 2.62). Parents who reported higher levels of family, peer, and school support for their child’s gender identity also reported fewer internalizing symptoms; the objective measure of state-level support was not related to internalizing symptoms. Additionally, peer and school support buffered against the association between gender-related victimization and internalizing symptoms, as reported by parents. This work demonstrates that even among transgender youth with families who supported their transitions, parents see better well-being in their children when they also see more support for the child’s gender identity from family, peers, and schools.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Society’s awareness that transgender youth exist has grown precipitously recently (Steinmetz, 2014; Yong, 2019), as have the number of youth who are supported in transgender identities at young ages (Ehrensaft et al. 2018; Kuvalanka et al. 2014). Though many researchers and lay authors have posited that social support for a transgender child’s gender identity may be associated with lower levels of psychopathology (Kuvalanka et al. 2017; Turban & Ehrensaft 2018; Holpuch 2016; Spitzer 2016), very little empirical work has tested this link. The present work aims to fill this gap by testing whether gender-related support is associated with lower levels of internalizing psychopathology in young transgender youth. Specifically, this study tests whether parent’s reports of the amount of family support, peer support, and school support a youth receives for their gender identity, as well as an objective measure of state-level support, are associated with lower levels of internalizing symptoms in socially transitioned transgender youth, ages 3–15.
A small proportion of youth persistently and consistently assert that they feel a sense of incongruence between their assigned sex at birth and their gender identity (De Vries & Cohen-Kettenis 2012; Spack et al. 2012). Recent, large scale studies suggest that between 1 and 3% of all youth identify as transgender or gender nonconforming (TGNC) (Eisenberg et al. 2019; Perez-Brumer et al. 2017), and numerous studies report that TGNC children and adolescents have higher levels of internalizing psychopathology than do their cisgender counterparts (Holt et al. 2016; Steensma et al. 2014; Wallien et al. 2007). The high levels of psychopathology among TGNC youth mirror high rates found in TGNC adults (Bockting et al. 2013; Budge et al. 2013). Identifying factors that may protect against the development of internalizing psychopathology is of critical importance for this vulnerable group.
In contrast with the high levels of internalizing symptoms reported in many TGNC youth and adult samples, some recent samples of TGNC youth—specifically binary, socially transitioned transgender youth ranging in age from 3 to 14—reflect average or only slightly elevated levels of anxiety and depression based on both parent and child report (Durwood et al. 2017; Hill et al. 2010; Kuvalanka et al. 2017; Olson et al. 2016). Social transitions describe the process of changing one’s name, pronouns, hairstyle, and clothing in order to allow the child to live as the gender with which a person identifies. Youth who have made childhood social transitions are necessarily highly supported in their gender identities at least by their parents, without the support of whom they would not have been able to make such a transition. Given the relatively low levels of internalizing symptoms in these socially transitioned transgender youth, researchers and popular press reporters have posited that these lower levels of internalizing symptoms can be attributed to the high levels of support these children receive for their gender identities and expressions (Kuvalanka et al. 2017; Turban & Ehrensaft 2018; Holpuch 2016; Spitzer 2016). Importantly, the role of support for a person’s gender identity has also been described in qualitative work and in personal narratives from transgender authors articulating the emotional impact of being seen and accepted as the gender with which they identify (Boylan 2013; Devor 2004; Mock 2014). Though the link between gender-related social support and internalizing symptoms has been articulated across a variety of mediums, empirical work testing the association between gender-related social support and mental health in young transgender youth is very limited.
The role of social support has been studied frequently in the general population (i.e., samples recruited without respect to gender identity), and this work demonstrates multiple pathways by which social support may protect against psychopathology (Cohen & Wills 1985). For one, social support is thought to protect against psychopathology through a direct pathway, whereby greater social support is directly associated with better mental health outcomes. Via the direct pathway, social support is thought to promote positive adjustment regardless of whether someone is experiencing stress, through for example increasing one’s self-esteem and sense of belonging (Berkman et al. 2000; Cohen & Willis 1985). Though the present work is focused on gender-related support in particular, one can imagine that social support for a transgender youth’s gender identity might work in a similar fashion; youth who experience high levels of support for their gender identity may feel, for example, higher esteem about being transgender and/or a greater sense of belonging in their social contexts.
Social support in the general population has also been shown to be protective against psychopathology indirectly through a stress buffering pathway, by which higher levels of social support attenuate the harmful effects of stressful experiences on mental health (Cohen & Willis 1985; Cohen 2004). Via this indirect pathway, social support is thought to play a protective role only when a person is experiencing stress by providing the person with emotional support that facilitates adaptive coping, thus protecting against the harmful effects of those stressors (Cohen 2004; Kawachi & Berkman 2001). Given the minority stress hypothesis, which posits that minority groups often show higher levels of psychopathology than majority groups because of the unique stressors they experience (Hatzenbuehler 2009; Meyer 2003), this stress buffering pathway may be particularly relevant to transgender youth. Transgender youth experience high levels of gender-related victimization, like bullying (Gordon et al. 2018; Witcomb et al. 2019), and the presence of individuals or structures who are supportive of their gender identities may protect them, at least in part, from the emotional effects of these minority stress experiences.
Work in samples of LGB and LGBT adolescents and young adults show that social support from various sources are directly associated with lower levels of internalizing symptoms. In such samples, family support (McConnell et al. 2015; Miller et al. 2020; Ryan et al. 2010; Shilo & Savaya 2011; Watson et al. 2019), peer support (Sheets & Mohr 2009; Watson et al. 2019), school support (Toomey et al. 2011), and support from state-level laws and policies (Hatzenbuehler et al. 2009; Hatzenbuehler et al. 2010) have each been shown to associated with lower levels of internalizing symptoms. Some studies with LGBT adolescents and young adults have also examined whether social support protects against internalizing psychopathology via the stress buffering pathway—by buffering against the harmful effects of stressful experiences, which are common among LGBT youth (Gordon et al. 2018; Russell et al. 2011; Toomey et al. 2013; Witcomb et al. 2019). One such study failed to find that family support moderated the association between victimization experiences and depression (Espelage et al. 2008), while another study found that school support did moderate the same association (Toomey et al. 2011). Another study found that sexuality-related social support buffered against the association between minority stress and emotional distress (Doty et al. 2010).
Studies with exclusively transgender—rather than LGBT—adolescents and young adults also show that family support is directly associated with lower levels of internalizing psychopathology (Gower et al. 2018; Grossman et al. 2019; Lefevor et al. 2019; Pariseau et al. 2019; Simons et al. 2013; Wilson et al. 2016), as is school support (Gower et al. 2018) and generalized social support (Grossman et al. 2011; Veale et al. 2017). Tests of the association between other forms of support and internalizing symptoms in transgender adolescents and young adults are lacking, as are tests of the potential role of social support in buffering against the association between victimization experiences and internalizing symptoms.
Only one study examines the association between social support and internalizing symptoms in transgender children, perhaps because of the challenge of recruiting transgender children, and because social transitions in childhood have become common only recently. This study, which featured a clinical sample of TGNC children, examined the potential direct association between gender-related parent support and depressive symptoms, and it counterintuitively found that higher levels of support were associated with more depressive symptoms (Kolbuck et al. 2019). Thus, while social support has been demonstrated to be associated with lower levels of internalizing symptoms in lesbian, gay, bisexual, and transgender adolescents and adults, no work has demonstrated that social support for one’s gender identity is associated with lower levels of psychopathology in transgender children.
Current Study
The present study aims to fill the critical gap in knowledge about the association between gender-related social support and internalizing symptoms in young transgender youth. The association between parents’ reporting of various forms of gender-related social support (from family, peers, and schools), as well as an objective measure of support from state-level laws and policies, with parent-reported internalizing symptoms are tested in a sample of transgender youth, ages 3–15. The present work tests the hypothesis that higher levels of gender-related social support from each of these sources are directly associated with lower levels of internalizing symptoms. Next, this study examines whether each form of support moderates the association between parents’ report of gender-related victimization experienced by their child and internalizing symptoms, with the hypothesis that support at each level (family, peer, school, state) will attenuate this association.
Methods
Participants and Procedure
Participants signed up for the present study as part of recruitment for a large, ongoing, national study of gender diverse youth in North America. Families signed up to participate either via an email address or through a website, which were advertised through vehicles like support groups, camps, word of mouth, and press coverage. Parents of all youth enrolled in the broader research study (n = 369 youth at that time) were invited to complete the present measures via an online survey, and parents completed the survey between February and June 2017.
The present study includes binary, socially-transitioned transgender youth. To be included in the present study, youth had to use the gendered pronouns stereotypically thought to be “opposite” their assigned sex at birth in all contexts; e.g., youth who were assigned male at birth and use “she/her” pronouns, or youth who were assigned female at birth and use “he/him” pronouns. They also needed to have at least one parent who filled out the survey. This yielded 357 parent informants for 265 transgender youth. Of these 265 youth, 173 had one parent respondent and 92 had two parent respondents. When youth had two parent responders, parents’ responses to single items were averaged, though see the Supplementary Materials for analyses using only one parent reporter per youth (see Specification 1).
Of the families participating in the present survey, two families were from Canada and the remaining were from 38 US states or the District of Columbia. The youth in the sample ranged from age 3 to 15, M = 9.41, SD = 2.62, with the majority of participants falling in the 6–12 age range (see Fig. 1). Each youth in the sample socially transitioned at the age of 12 or younger, which was a criterion for recruitment in the ongoing national study. The sample is predominantly white and high socio-economic status, and it included about twice as many transgender girls (assigned male at birth) as transgender boys (assigned female at birth). See Table 1 for demographics.

Age distribution
Parents responded to the present measures as part of a battery of other measures that took ~30–60 min to complete. Parent report was used instead of child report so that young transgender children, who were too young to fill out an online survey, could be included in the sample. Informed consent was gathered prior to administering the survey. Parents were compensated with a $5 gift card for their time. The Institutional Review Board of the University of Washington approved all study procedures.
Measures and Variable Creation
Of note, the authors faced a number of decisions with regards to creating variables representing parent-reported family, peer, and school support—e.g., what items should be included in these composite variables, how those variables should be computed, whether only one parent reporter should be used vs. an average of two parent reports, etc. In light of recent discussions in the field about “researcher degrees of freedom” in conducting analyses that are not pre-registered (Wicherts et al. 2016), a core set of analyses were completed for the main paper, based on a set of analytic decisions determined by the authors to be most optimal. Supplementary analyses (referred to here as “specifications”), representing different but also reasonable analytic decisions, were completed and are reported in the Supplementary Materials (see Tankard & Paluck 2017 for a similar approach; see Table S1). The reasoning for this type of approach is that authors can have greater confidence in their findings that are observed across a variety of analytic decisions, and less confidence in those that are significant in few specifications (Hässler et al. 2020; Steegen et al. 2016). The full results of the additional specifications are reported in the Supplemental Material (see Table S2). In all cases, the results reported in the main text were stable across a majority of specifications.
Family support
Parents were asked to report on how accepting various family members are currently of the child’s gender/gender presentation on a scale of 1–7, (1 being “unaccepting,” 7 being “fully accepting”), or they could select “not applicable.” “Not applicable” responses were removed for analysis. Parents rated levels of acceptance of the child’s gender/gender presentation from each of the following family members: the parent completing the survey, the child’s other parent (if applicable), the parent’s spouse or partner (if applicable and if different from the child’s other parent), the child’s sibling(s), and the child’s extended family.
If the relevant family member(s) was not aware that the child was transgender, parents were not asked to report on that person’s level of acceptance. Awareness of the child’s gender/gender presentation was gauged by a previous question, “Does your child’s [family member] know that your child is gender nonconforming or transgender?” with the options “yes, all of them know,” “yes, some of them know,” and “no.” If the parent responded that “no,” the person or group was not aware, then the parent was not asked to report on how accepting that person or group is. If the parent responded that “yes, some of them know” that the child is transgender, the parent was asked to answer the acceptance questions with only those who did know that the child is transgender in mind.
Levels of current acceptance from each family member were averaged to create one family support score (see Table S3 for correlations between the different constructs). In Specification 2 in the Supplementary Material, we averaged current acceptance and another rating—initial acceptance—in these calculations. In Specification 3, we calculated parental support and family support slightly differently than in the main analyses.
Peer support
Parents were asked to report on how accepting the child’s peers are of the child’s gender/gender presentation on a scale of 1–7, (1 being “unaccepting,” 7 being “fully accepting”), or they could select “not applicable.” “Not applicable” responses were removed for analysis. For peer support, parents rated levels of acceptance of the child’s gender/gender presentation from each of the following groups: close friends and peers, other peers, and peers’ parents (the latter were excluded from analyses in Specification 4 of the Supplementary Materials). Similar to the family support questions, if the relevant peer group(s) was not aware that the child was transgender, parents were not asked to report on that group’s acceptance level. Awareness was gauged by a previous question, as was done for family members. Levels of current acceptance from each peer group were averaged to create one peer support score (see Table S4 for correlations between the different constructs). Eleven children who did not have a value for the peer support score, as the parent(s) selected “not applicable” for all the items, were removed from the analysis involving this score.
School support
Parents were asked to report how accepting the child’s teacher(s) are of the child’s gender/gender presentation, again on a scale of 1–7, or they could select “not applicable.” “Not applicable” responses were removed for analysis. Similar to the family/peer support questions, if the child’s teacher(s) was not aware that the child is transgender, parents were not asked to report how accepting the teacher(s) was of the child’s gender/gender presentation. Awareness was gauged by a previous question, as was done for family/peer members.
The remaining school support items were not asked if parents indicated on a previous question that their child was either homeschooled or too young to be in school (parent 1: n = 16, parent 2: n = 8).
Parents were asked to indicate how satisfied they were overall with the child’s school’s treatment of their child’s gender identity/expression, again on a scale of 1–7 (1 being “very unsatisfied,” 7 being “very satisfied”).
Parents completed an 11-item checklist indicating whether the school provided various supports related to their child’s gender identity. Example items from the school checklist include: “the school has an anti-bullying and harassment policy that specifically mentions gender identity and/or expression,” “the school has discussed gender diversity with the school community (e.g., a letter to parents, parent information night, assemblies, etc.),” “attendance lists and/or school documents reflect my child’s preferred gender,” “my child is allowed to use their preferred bathroom (female, male, gender neutral),” and “my child is allowed to participate in sports and clubs according to their preferred gender.” For each item on the school checklist, parents could respond “yes,” “no,” or “not sure.” “Not sure” responses were removed for analysis. One checklist score was computed by creating a mean score of the 11-item check-list only including the yes (1) and no (0) answers (and excluding the ‘not sure’).
These three values (teacher acceptance, overall parent satisfaction, and the school checklist score) were then rescaled to range from 0 to 1 and then averaged to create one school support score (see Table S5 for correlations between the different constructs; See Specification 5 in the Supplementary Material for analyses excluding the checklist score). Two children, who did not have values for the school support score, were removed from the analysis involving this score.
State-level support
An objective variable representing U.S. state-level support for a youth’s gender identity was computed using six state laws that were relevant to transgender youth at the time the study was conducted, as identified by the Movement Advancement Project organization (“Mapping Transgender Equality in the United States,” 2017). Participants who came from Canada (n = 2) were removed from the analysis involving the state-level support score. The six laws and policies that were coded to create the state-level support variable were as follows: (1) whether state non-discrimination laws include gender identity as a protected class; (2) whether state anti-bullying laws prohibit bullying on the basis of gender identity; (3) whether states require foster parents to attend a training about gender identity; (4) whether states ban conversion therapy on the basis of gender identity; (5) whether states have a “don’t say gay” law, which prohibit schools from discussing LGBT issues with students; and (6) whether states ban non-discrimination laws that protect gender identity.
The first two laws/policies were coded by the Movement Advancement Project organization on a 0–4 scale, reflecting how supportive the laws/policies are of transgender youth, with higher scores indicating more support for transgender youth (“Safe Schools Laws,” 2017). The remaining laws were coded by the Movement Advancement Project organization on a binary scale, with 0 indicating less support and 1 indicating more support for transgender youth (“Conversion Therapy Laws,” 2017; “Foster and Adoption Laws,” 2017; “Safe Schools Laws,” 2017). These scores were rescaled to range from 0 to 1 and averaged to create one state-level support score for each state.
Internalizing symptoms
Parents filled out the NIH PROMIS Scales for Anxiety and Depression, parent proxy short forms (Varni et al. 2012). These scales ask parents to respond to eight items about their child’s anxiety symptoms and six items about their child’s depression symptoms in the past 7 days. Example items for anxiety included “My child felt nervous,” and “My child felt scared.” Example items for depression included “My child felt sad,” and “My child felt like everything in his/her life went wrong.” Responses were provided on a 5-point Likert scale ranging from “never” to “almost always.”
Average t-scores, with 50 representing the national average and 10 representing one standard deviation, were computed for anxiety and depression. Anxiety and depression t-scores were then averaged to create one Internalizing Score for the analysis, though see Specification 6 in the Supplementary Material for separate analyses for anxiety and depression.
Victimization
Parents were asked whether their child had ever experienced gender-related bullying, and they were given the options “never,” “seldom,” “sometimes,” “often” and “I don’t know.” “I don’t know” responses (n = 10) were removed for analysis. Parents were also asked to indicate whether their child has ever experienced gender-related discrimination (“treated unfairly”) at school, and given “yes” and “no” response options. Because the discrimination item was specific to one context (school), we did not include it in the main analyses (though we use it in Specification 7 in the Supplementary Material).
Scoring
Because the support and victimization measures are assessed on different scales (e.g., satisfaction with school ranged from 1 being “very unsatisfied” to 7 being “very satisfied” and the school check-list from 0 to 1), we converted these measures into the same meaningful unit. All scores for the independent variables were converted into possible scores between a minimum of 0 and a maximum of 100, creating so-called percent of maximum possibility (POMP) scores (Cohen et al. 1999) using the following formula 1.
(1) POMP = [(observed − minimum)/(maximum − minimum)] × 100, where observed = the observed score for a single case, minimum = the minimum possible score on the scale, and maximum = the maximum possible score on the scale.
We use these converted POMP scores in our analyses for ease of interpretation of the unstandardized coefficients.
Data Analysis
Preliminary analyses were first conducted to assess the correlation between each construct (see Table 3). Next, a multivariate regression analysis was estimated to test the association between the different forms of gender-related support (family support, peer support, school support, and state-level support) and internalizing symptoms, controlling for age (in months) and gender (with girl as reference category). Finally, to gauge whether each type of gender-related support (family, peer, school, and state-level) buffered against the association between gender-related victimization and internalizing symptoms, a regression model was first estimated to test the association between victimization and internalizing symptoms, controlling for age (in months) and gender. Then, four regression models were estimated to test whether each type of support moderated the association between victimization and internalizing symptoms, controlling for age (in months) and gender. An FDR correction was used to correct for four moderation tests. Significant interactions were then probed and plotted at multiple levels of the moderator (McCabe et al. 2018).
Due to the vast age range in the present sample, exploratory moderation analyses were also conducted to test whether the child’s age (in months) moderated the association between each form of support and internalizing symptoms. Because most of our participants ranged from age 6 to 12–making younger (3–5) and older children (13–15) less represented in our sample—sensitivity analyses were also completed to see if the results remained the same if tested in only 6–12 year old participants. The results of these additional moderation and sensitivity analyses are also reported in the Supplementary Material (see Specification 8).
To handle missing data, pairwise deletion was applied (i.e., children with missing values in all the items of one source of support were excluded from the analyses involving this source of support; see also Table 2 for final sample sizes). In Specification 9 in the Supplementary Material, we report analyses using listwise deletion.
Results
Descriptive Statistics
On average, parents reported that their children experienced levels of support for their gender identities on the high end of the scales used, and they experienced levels of gender-related victimization on the low end of the item(s) used. Further, according to their parents’ reports, youth had internalizing symptoms in the normal to slightly elevated range. On a nationally normed scale with an average of 50, and with 10 representing one standard deviation, participants had a mean depression t-score of 51.34 (SD = 8.85) and a mean anxiety t-score of 51.51 (SD = 10.26). See Table 2 for means and standard deviations of each variable. See Table 3 for bivariate correlations between all constructs.
Social Support and Internalizing Symptoms
Please note that all the analyses reported below are conducted on parents’ reporting of the gender-related family, peer, and school support their children received, as well as parents’ reporting of their child’s internalizing symptoms and gender-related victimization experiences. Three of the four social support sources were negatively associated with internalizing symptoms (see Table 3). As expected, greater family support was associated with fewer internalizing symptoms, r = –0.22, p < 0.001. Similarly, higher levels of peer support, r = –0.27, p < 0.001, and school support, r = –0.19, p = 0.002, were also associated with fewer internalizing symptoms. State-level support, however, was not associated with internalizing symptoms, r = −0.00, p = 0.99.
When all forms of support were entered into a regression model controlling for age and gender (R2 = 0.13; F (6, 243) = 5.93, p < 0.001), greater family support was—as expected—associated with fewer internalizing symptoms, b = –0.16, p = 0.012. Similarly, greater peer support, b = –0.14, p = 0.003, was also associated with fewer internalizing symptoms. Contrary to our expectations, higher levels of school support, however, were not associated with fewer internalizing symptoms, b = –0.05, p = 0.210. Further, state-level support was also not associated with internalizing symptoms, b = –0.00, p = 0.859. Finally, age was associated with higher internalizing symptoms, b = 0.04, p = 0.020, while gender had no effect, b = –0.66, p = 0.557. Please note that we report unstandardized coefficients to ease the interpretations of the findings based on POMP scores. Notably, age and gender were not transformed; therefore, the range of coefficients are not comparable to those of the support constructs.
Interactions of Social Support and Victimization
Victimization experiences were positively associated with internalizing symptoms, F (3, 251) = 10.42, p < 0.001), b = 0.10, p < 0.001. In line with our expectations, peer support (F (5, 239) = 9.93, p < 0.001), b < –0.01, p = 0.022, and school support (F (5, 247) = 9.20, p < 0.001), b < –0.01, p = 0.002, moderated the association between victimization and internalizing symptoms. Contrary to our expectations, however, family support and state-level support did not moderate this association (family support, F (5, 249) = 10.27, p < 0.001: b < –0.01, p = 0.097; state-level support, F (5, 247) = 6.20, p < 0.001: b = –0.00, p = 0.549).
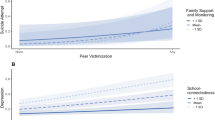
Simple slopes for the associations between victimization and internalizing symptoms were examined at very low (−1.0 SD), low (−0.5 SD), mean, high (+0.5 SD) and very high (+1.0 SD) levels of peer support. This revealed a positive association between victimization and internalizing symptoms at very low, low, mean, and high levels of peer support (very low: b = 0.11, 95% CI = [0.06, 0.15]; low: b = 0.09, 95% CI = [0.05, 0.13]; mean: b = 0.07, 95% CI = [0.03, 0.11]; high: b = 0.05, 95% CI = [0.00, 0.09]), but no association between victimization and internalizing symptoms at very high levels of peer support (very high: b = 0.03, 95% CI = [−0.03, 0.08]). Figure 2 displays simple slopes.

The association between victimization experiences and internalizing symptoms at varying levels of peer support
In addition, there was a positive association between victimization and internalizing symptoms at very low, low, mean, and high levels of school support (very low: b = 0.15, 95% CI = [0.10, 0.20]; low: b = 0.12, 95% CI = [0.07, 0.16]; mean: b = 0.09, 95% CI = [0.05, 0.13]; high: b = 0.06, 95% CI = [0.01, 0.10]); but no association between victimization and internalizing symptoms at very high levels of school support (b = 0.02, 95% CI = [−0.03, 0.08]). Figure 3 displays simple slopes.

The association between victimization experiences and internalizing symptoms at varying levels of school support
Discussion
An increasing number of children have socially transitioned to live in transgender identities, yet very little is known about what factors may contribute to their wellbeing (Malpas 2011; Ehrensaft et al. 2018). Though gender-related social support has been frequently suggested as a potential predictor of psychopathology in such youth (Turban & Ehrensaft 2018; Holpuch 2016), and though some studies have demonstrated the relation between psychopathology and social support for one’s LGBT identity in adolescents and young adults (Hatzenbuehler et al. 2009; Pariseau et al. 2019; Ryan et al. 2010; Shilo & Savaya 2011; Toomey et al. 2011), very little empirical work tests the potential protective role of gender-related social support in young transgender youth.
Parent-reported levels of gender-related family support, peer support, and school support were each associated with lower levels of parent-reported internalizing symptoms in transgender youth ages 3–15 years, but an objective measure of state-level support was not. When all types of support were considered in the same model, family support and peer support for a youth’s gender identity continued to be associated with lower levels of internalizing symptoms. Higher levels of peer and school support for the youth’s gender identity also buffered against (moderated) the association between gender-related victimization and internalizing symptoms, such that the positive association between victimization and internalizing psychopathology was not present among youth with very high levels of support from these sources.
The direct associations between higher levels of support and lower levels of internalizing symptoms found here are generally consistent with prior work in older samples of LGBT adolescents and young adults (Hatzenbuehler et al. 2009; Pariseau et al. 2019; Ryan et al. 2010; Shilo & Savaya 2011; Toomey et al. 2011). The present study’s finding that higher levels of parent-reported family support for the youth’s gender identity is associated with lower levels of internalizing symptoms runs counter to a recent finding in a clinical sample of gender diverse children, which found that higher levels of gender-related parent support were associated with more depression symptoms (Kolbuck et al. 2019), a contrast perhaps attributable to differences between clinical and community samples. In addition to contributing this finding—that family support for one’s gender identity is associated with lower internalizing symptoms—this work also contributes that peer support and school support for a child’s gender identity are significantly associated with lower internalizing symptoms, through both a direct and an indirect (buffering) pathway.
Our finding that state-level support for a child’s gender identity was not associated with parent-reported internalizing psychopathology in the present sample does not align with work with LGBT adolescents and young adults indicating that state laws protecting LGBT people are associated with lower levels of psychopathology (Hatzenbuehler et al. 2009; Hatzenbuehler et al. 2010). This may be because youth in this sample are protected from the instrumental effects of some unsupportive state laws (e.g., anti-bullying laws that do not protect on the basis of gender identity) by more proximal supportive entities (e.g., schools that protect transgender students from bullying regardless of state laws). Many of the participants in the current work, who are as young as three, may not even be aware of their state laws, thus protecting them from the emotional impact of unsupportive laws. Future work might investigate the potential impact of gender-related state-level support on internalizing symptoms in a sample of transgender adolescents.
Parent-reported peer support and school support for a transgender youth’s gender identity both moderated the association between gender-related victimization experiences and internalizing symptoms. Not surprisingly, gender-related victimization experiences were associated with higher levels of internalizing symptoms; however, for youth with very high levels of peer or school support for their gender identities, gender-related victimization experiences and internalizing symptoms were not associated. These findings are in line with some studies of LGBT adolescents and young adults showing that social support buffers against the association between victimization and internalizing symptoms (Doty et al. 2010; Toomey et al. 2011). The present work extends this previous work by providing preliminary evidence that, amongst young transgender youth specifically, gender-related support from peers and schools may be important in buffering against the harmful effects of gender-related victimization. The fact that peer and school support were the sources of support that played a buffering role in this sample could reflect aspects of the specific victimization experiences examined in the present work. Prior work on the stress buffering role of social support indicates that a critical factor in support acting as a buffer is a person’s perception that they would have appropriate support available to them if they needed it (Cohen 2004). Given that bullying was used to capture victimization experiences in this sample, and given that this particular kind of victimization experience often occurs in the presence of peers and/or at school, it is possible that peer and school support played a significant buffering role because these forms of support (as opposed to family or state-level support) are particularly appropriate for youth experiencing this form of victimization.
These findings are especially notable given the young age of this sample (M = 9.41 years), and because the present work examined gender-related support rather than social support more broadly. While one might imagine that general social support would be beneficial to all youth—and in gender diverse children, non-gender related measures like family functioning/discord and peer relations have indeed been shown to be associated with lower levels of psychopathology (De Vries et al. 2016; Munroe et al. 2020; Sievert et al. 2020)—the question of whether children should be supported in transgender identities has continued to be a matter of debate in the literature (Drescher & Pula 2014; Ehrensaft et al. 2018). Often, the hypothesized protective role of support for a child’s gender identity/expression has been weighed against other factors—e.g., whether a child is likely to continue identifying as transgender as an adult (Ehrensaft et al. 2018; Steensma & Cohen-Kettenis 2011)—though until now there has been limited evidence for the association between gender-related support and lower levels of psychopathology in relevant samples. Despite the inherent limitations in any specific study, our results do provide evidence that gender-related social support for young transgender youth is associated with lower levels of internalizing symptoms.
The transgender youth in the present study are by and large supported in their gender identities and expressions, and they likely experience victimization that is less frequent and less severe than transgender youth more broadly. These characteristics represent both a strength and a limitation of this study. On the one hand, the fact that the range of responses was constrained makes this work a conservative test of the role of social support for a transgender child’s gender identity. On the other hand, these findings may be limited in the degree to which they can be extended to other samples, given that some studies indicate that the specific mix of sources from which a child experiences support (e.g., from family only, from friends but not from family, etc.) and the severity of the victimization they experience (e.g., teasing vs. physical violence) may influence the associations of interest here. One study, for example, found that LGBT youth with non-family support only (e.g., support from friends but not family) had overall worse outcomes than those with high overall support, and were mostly indistinguishable from youth with no support (McConnell et al. 2015). Thus, it may be the case that non-family support is more likely to protect a child against psychopathology when family support is also in place. Other work suggests the possibility that support may buffer against the harmful effects of victimization the most when victimization is mild (Hershberger & D’augelli 1995; Toomey et al. 2011); when youth experience frequent, severe forms of victimization, support may not be able to buffer against deleterious outcomes.
Another key limitation of this work is the correlational and cross-sectional design, which precludes inferences that support caused lower levels of psychopathology. The same is true for the interactions between support and victimization. Although these findings may reflect a buffering role of gender-related peer and school support, another possible explanation is that youth whose internalizing symptoms are not significantly associated with gender-related victimization experiences are also youth who are more likely to elicit support for their gender identities from their peers and schools.
A third limitation of the present work is its reliance on parent report. Parent report was used here to include young transgender youth (as young as age three in the present sample), who are too young to complete an online survey themselves but are a group for whom these questions are of great importance. The drawback of using parent report, however, is that youth’s views of how much gender-related support they experience, and/or their reports of their symptoms of anxiety and depression, could differ from those of their parents. Indeed, in broader clinical samples, parents often under-report internalizing symptoms in their children, presumably because these are internal experiences that may not be obvious to parents (Achenbach et al. 1987; Cantwell et al. 1997; De Los Reyes & Kazdin 2005). It is also possible that, because both the majority of the support variables and the internalizing variables used were gauged via parent report, that parent response style (generally positive vs. generally negative) drove the direct associations found between various forms of support and internalizing symptoms. Consistent with this possibility, the one objective variable used—state support—was not significantly associated with internalizing symptoms (at least in younger children in our sample, see Supplementary Materials for the moderating role of age) lending credence to this potential interpretation. Despite this limitation, parent report is commonly used to gauge psychopathology as well as peer relationships in children (Achenbach 1999; Reynolds & Kamphaus 2002), and work with transgender youth specifically has found similar results when using parent vs. child report (Durwood et al. 2017; Olson et al. 2016). In the participants reported in Durwood et al. (2017), which included both child- and parent-reported internalizing symptoms in transgender youth, new analyses indicate that parent- and child-reported symptoms were significantly correlated, r = 0.25, p = 0.048, N = 63. Nonetheless, particularly as youth in this sample (and others) mature such that a substantial number are old enough to provide these kinds of reports themselves, it is critical that their experiences be measured directly.
A fourth limitation of this work is the use of a single-item measure to assess victimization experiences. Multi-item scales are often preferred to single-item measures as they limit measurement errors and increase the validity of the measurement (Diamantopoulos et al. 2012). Although analyses including another source of victimization (i.e., gender-related discrimination at school) led to similar results (see Supplementary Material), future research should aim to assess victimization experiences with multiple items. For instance, victimization experiences could be assessed with items capturing discrimination, bullying, social exclusion, and physical violence.
Conclusion
An increasing number of children have socially transitioned to live in transgender identities, yet very little is known about what factors are protective against psychopathology in transgender youth who have made such a transition (Malpas 2011; Ehrensaft et al. 2018). Though it has frequently been suggested that social support for a youth’s gender identity may be associated with lower levels of psychopathology in this group (Turban & Ehrensaft 2018; Holpuch 2016), very little empirical work has examined this potential association. The present work fills this gap by finding—using parent report—that family support, peer support, and school support for a transgender child’s gender identity are all associated with lower levels of internalizing symptoms in binary, socially transitioned transgender youth, ages 3–15 years. Moreover, parent-reported peer support and school support for a youth’s gender identity buffered the association between gender-related victimization and internalizing symptoms. While this work warrants replication with longitudinal data and in samples of youth who experience less gender-related support, these results suggest possible mental health benefits of families, peers, and schools supporting young transgender youth’s gender identities and expressions.
References
Achenbach, T. M. (1999). The Child Behavior Checklist and related instruments. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (p. 429–466). Lawrence Erlbaum Associates Publishers. https://doi.org/10.1192/bjp.178.1.93-a
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavioral and emotional problems: implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101(2), 213. https://doi.org/10.1037/0033-2909.101.2.213.
Berkman, L. F., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science & Medicine, 51(6), 843–857. https://doi.org/10.1016/S0277-9536(00)00065-4.
Bockting, W. O., Miner, M. H., Swinburne Romine, R. E., Hamilton, A., & Coleman, E. (2013). Stigma, mental health, and resilience in an online sample of the US transgender population. American Journal of Public Health, 103(5), 943–951. https://doi.org/10.2105/AJPH.2013.301241.
Boylan, J. F. (2013). She’s not there: A life in two genders. Broadway Books.
Budge, S. L., Adelson, J. L., & Howard, K. A. (2013). Anxiety and depression in transgender individuals: the roles of transition status, loss, social support, and coping. Journal of Consulting and Clinical Psychology, 81(3), 545. https://doi.org/10.1037/a0031774.
Cantwell, D. P., Lewinsohn, P. M., Rohde, P., & Seeley, J. R. (1997). Correspondence between adolescent report and parent report of psychiatric diagnostic data. Journal of the American Academy of Child & Adolescent Psychiatry, 36(5), 610–619. https://doi.org/10.1097/00004583-199705000-00011.
Cohen, P., Cohen, J., Aiken, L. S., & West, S. G. (1999). The problem of units and the circumstance for POMP. Multivariate Behavioral Research, 34(3), 315–346. https://doi.org/10.1207/S15327906MBR3403_2.
Cohen, S. (2004). Social relationships and health. American Psychologist, 59(8), 676. https://doi.org/10.1037/0003-066x.59.8.676.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310. https://doi.org/10.1037/0033-2909.98.2.310.
Devor, A. H. (2004). Witnessing and mirroring: a fourteen stage model of transsexual identity formation. Journal of Gay & Lesbian Psychotherapy, 8(1-2), 41–67. https://doi.org/10.1300/J236v08n01_05.
Diamantopoulos, A., Sarstedt, M., Fuchs, C., Wilczynski, P., & Kaiser, S. (2012). Guidelines for choosing between multi-item and single-item scales for construct measurement: a predictive validity perspective. Journal of the Academy of Marketing Science, 40(3), 434–449. https://doi.org/10.1007/s11747-011-0300-3.
Doty, N. D., Willoughby, B. L., Lindahl, K. M., & Malik, N. M. (2010). Sexuality related social support among lesbian, gay, and bisexual youth. Journal of Youth and Adolescence, 39(10), 1134–1147. https://doi.org/10.1007/s10964-010-9566-x.
Drescher, J., & Pula, J. (2014). Ethical Issues Raised by the Treatment of Gender‐Variant Prepubescent Children. Hastings Center Report, 44(s4), S17–S22. https://doi.org/10.1002/hast.365.
Durwood, L., McLaughlin, K. A., & Olson, K. R. (2017). Mental health and self-worth in socially transitioned transgender youth. Journal of the American Academy of Child & Adolescent Psychiatry, 56(2), 116–123. https://doi.org/10.1016/j.jaac.2016.10.016.
Ehrensaft, D., Giammattei, S. V., Storck, K., Tishelman, A. C., & Keo-Meier, C. (2018). Prepubertal social gender transitions: what we know; what we can learn—A view from a gender affirmative lens. International Journal of Transgenderism, 1–18. https://doi.org/10.1080/15532739.2017.1414649.
Eisenberg, M. E., Gower, A. L., Rider, G. N., McMorris, B. J., & Coleman, E. (2019). At the intersection of sexual orientation and gender identity: Variations in emotional distress and bullying experience in a large population-based sample of U.S. adolescents. Journal of LGBT Youth, 16(3), 235–254. https://doi.org/10.1080/19361653.2019.1567435.
Espelage, D. L., Aragon, S. R., Birkett, M., & Koenig, B. W. (2008). Homophobic teasing, psychological outcomes, and sexual orientation among high school students: What influence do parents and schools have? School Psychology Review, 37(2), 202–217. https://doi.org/10.1080/02796015.2008.12087894.
Gordon, A. R., Conron, K. J., Calzo, J. P., White, M. T., Reisner, S. L., & Austin, S. B. (2018). Gender expression, violence, and bullying victimization: Findings from probability samples of high school students in 4 US school districts. The Journal of School Health, 88(4), 306–314. https://doi.org/10.1111/josh.12606.
Gower, A. L., Rider, G. N., Brown, C., McMorris, B. J., Coleman, E., Taliaferro, L. A., & Eisenberg, M. E. (2018). Supporting transgender and gender diverse youth: protection against emotional distress and substance use. American Journal of Preventive Medicine, 55(6), 787–794. https://doi.org/10.1016/j.amepre.2018.06.030.
Grossman, A. H., D’augelli, A. R., & Frank, J. A. (2011). Aspects of psychological resilience among transgender Youth. Journal of LGBT Youth, 8(2), 103–115. https://doi.org/10.1080/19361653.2011.541347.
Grossman, A. H., Park, J. Y., Frank, J. A., & Russell, S. T. (2019). Parental responses to transgender and gender nonconforming youth: associations with parent support, parental abuse, and youths’ psychological adjustment. Journal of Homosexuality, 1–18. https://doi.org/10.1080/00918369.2019.1696103.
Hatzenbuehler, M. L. (2009). How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychological Bulletin, 135(5), 707 https://doi.org/10.1037/a0016441.
Hatzenbuehler, M. L., Keyes, K. M., & Hasin, D. S. (2009). State-level policies and psychiatric morbidity in lesbian, gay, and bisexual populations. American Journal of Public Health, 99(12), 2275–2281. https://doi.org/10.2105/AJPH.2008.153510.
Hatzenbuehler, M. L., McLaughlin, K. A., Keyes, K. M., & Hasin, D. S. (2010). The impact of institutional discrimination on psychiatric disorders in lesbian, gay, and bisexual populations: a prospective study. American Journal of Public Health, 100(3), 452–459. https://doi.org/10.2105/AJPH.2009.168815.
Hershberger, S. L., & D’augelli, A. R. (1995). The impact of victimization on the mental health and suicidality of lesbian, gay, and bisexual youths. Developmental Psychology, 31(1), 65 https://doi.org/10.1037/0012-1649.31.1.65.
Hill, D. B., Menvielle, E., Sica, K. M., & Johnson, A. (2010). An affirmative intervention for families with gender variant children: Parental ratings of child mental health and gender. Journal of Sex & Marital Therapy, 36(1), 6–23. https://doi.org/10.1080/00926230903375560.
Holpuch, A. (2016). ‘Crucial’ study of transgender children links mental health with family support. Feb Retrieved in 2018. https://www.theguardian.com/society/2016/feb/26/crucial-study-transgender-children-mental-health-family-support.
Holt, V., Skagerberg, E., & Dunsford, M. (2016). Young people with features of gender dysphoria: demographics and associated difficulties. Clinical Child Psychology and Psychiatry, 21(1), 108–118. https://doi.org/10.1177/1359104514558431.
Hässler, T., Ullrich, J., Bernardino, M., Shnabel, N., & Van Laar, C., et al. (2020). A large-scale test of the link between intergroup contact and support for social change. Nature Human Behaviour, 4(4), 380–386. https://doi.org/10.1038/s41562-019-0815-z.
Kawachi, I., & Berkman, L. F. (2001). Social ties and mental health. Journal of Urban Health, 78(3), 458–467. https://doi.org/10.1093/jurban/78.3.458.
Kolbuck, V. D., Muldoon, A. L., Rychlik, K., Hidalgo, M. A., & Chen, D. (2019). Psychological functioning, parenting stress, and parental support among clinic-referred prepubertal gender-expansive children. Clinical Practice in Pediatric Psychology, 7(3), 254. https://doi.org/10.1037/cpp0000293.
Kuvalanka, K. A., Weiner, J. L., & Mahan, D. (2014). Child, family, and community transformations: findings from interviews with mothers of transgender girls. Journal of GLBT Family Studies, 10(4), 354–379. https://doi.org/10.1080/1550428X.2013.834529.
Kuvalanka, K. A., Weiner, J. L., Munroe, C., Goldberg, A. E., & Gardner, M. (2017). Trans and gender-nonconforming children and their caregivers: gender presentations, peer relations, and well-being at baseline. Journal of Family Psychology, 31(7), 889. https://doi.org/10.1037/fam0000338.
Lefevor, G. T., Sprague, B. M., Boyd-Rogers, C. C., & Smack, A. C. (2019). How well do various types of support buffer psychological distress among transgender and gender nonconforming students? International Journal of Transgenderism, 20(1), 39–48. https://doi.org/10.1080/15532739.2018.1452172.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131(4), 483. https://doi.org/10.1037/0033-2909.131.4.483.
Malpas, J. (2011). Between pink and blue: a multi‐dimensional family approach to gender nonconforming children and their families. Family Process, 50(4), 453–470. https://doi.org/10.1111/j.1545-5300.2011.01371.x.
McCabe, C., Kim, D., & King, K. (2018). Improving Present Practices in the Visual Display of Interactions. Advances in Methods and Practices in Psychological Science, 1(2), 147–165. https://doi.org/10.1177/2515245917746792.
McConnell, E. A., Birkett, M. A., & Mustanski, B. (2015). Typologies of social support and associations with mental health outcomes among LGBT youth. LGBT Health, 2(1), 55–61. https://doi.org/10.1089/lgbt.2014.0051.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 129(5), 674. https://doi.org/10.1037/0033-2909.129.5.674.
Miller, K. K., Watson, R. J., & Eisenberg, M. E. (2020). The Intersection of Family Acceptance and Religion on the Mental Health of LGBTQ Youth. Annals of LGBTQ Public and Population Health, 1(1), 27–42. https://doi.org/10.1891/LGBTQ.2019-0005.
Mock, J. (2014). Redefining realness: My path to womanhood, identity, love & so much more. Simon and Schuster.
Movement Advancement Project. (2017). Mapping Transgender Equality in the United States. Retrieved March, 2017. http://www.lgbtmap.org/mapping-trans-equality.
Movement Advancement Project. (2017). Foster and Adoption Laws. Retrieved March 24, 2017. http://lgbtmap.org/equality-maps/foster_and_adoption_laws.
Movement Advancement Project. (2017). Safe Schools Laws. Retrieved March 24, 2017. http://lgbtmap.org/equality-maps/safe_school_laws.
Movement Advancement Project. (2017). Conversion Therapy Laws. Retrieved March 24, 2017. http://lgbtmap.org/equality-maps/conversion_therapy.
Munroe, C., Clerkin, E. M., & Kuvalanka, K. A. (2020). The Impact of Peer and Family Functioning on Transgender and Gender-Diverse Children’s Mental Health. Journal of Child and Family Studies. https://doi.org/10.1007/s10826-020-01729-x.
Olson, K. R., Durwood, L., DeMeules, M., & McLaughlin, K. A. (2016). Mental health of transgender children who are supported in their identities. Pediatrics, 137(3). https://doi.org/10.1542/peds.2015-3223.
Pariseau, E. M., Chevalier, L., Long, K. A., Clapham, R., Edwards-Leeper, L., & Tishelman, A. C. (2019). The relationship between family acceptance-rejection and transgender youth psychosocial functioning. Clinical Practice in Pediatric Psychology, 7(3), 267. https://doi.org/10.1037/cpp0000291.
Perez-Brumer, A., Day, J. K., Russell, S. T., & Hatzenbuehler, M. L. (2017). Prevalence and Correlates of Suicidal Ideation Among Transgender Youth in California: Findings From a Representative, Population-Based Sample of High School Students. Journal of the American Academy of Child & Adolescent Psychiatry, 56(9), 739–746. https://doi.org/10.1016/j.jaac.2017.06.010.
Reynolds, C. R., & Kamphaus, R. W. (2002). The clinician’s guide to the Behavior Assessment System for Children (BASC). Guilford Press. https://doi.org/10.1076/chin.9.3.234.16453
Russell, S. T., Ryan, C., Toomey, R. B., Diaz, R. M., & Sanchez, J. (2011). Lesbian, gay, bisexual, and transgender adolescent school victimization: Implications for young adult health and adjustment. Journal of School Health, 81(5), 223–230. https://doi.org/10.1111/j.1746-1561.2011.00583.x.
Ryan, C., Russell, S. T., Huebner, D., Diaz, R., & Sanchez, J. (2010). Family acceptance in adolescence and the health of LGBT young adults. Journal of Child and Adolescent Psychiatric Nursing, 23(4), 205–213. https://doi.org/10.1111/j.1744-6171.2010.00246.x.
Sheets, Jr, R. L., & Mohr, J. J. (2009). Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. Journal of Counseling Psychology, 56(1), 152. https://doi.org/10.1037/0022-0167.56.1.152.
Shilo, G., & Savaya, R. (2011). Effects of family and friend support on LGB youths’ mental health and sexual orientation milestones. Family Relations, 60(3), 318–330. https://doi.org/10.1111/j.1741-3729.2011.00648.x.
Sievert, E. D., Schweizer, K., Barkmann, C., Fahrenkrug, S., & Becker-Hebly, I. (2020). Not social transition status, but peer relations and family functioning predict psychological functioning in a German clinical sample of children with Gender Dysphoria. Clinical Child Psychology and Psychiatry. https://doi.org/10.1177/1359104520964530.
Simons, L., Schrager, S. M., Clark, L. F., Belzer, M., & Olson, J. (2013). Parental support and mental health among transgender adolescents. Journal of Adolescent Health, 53(6), 791–793. https://doi.org/10.1016/j.jadohealth.2013.07.019.
Spack, N. P., Edwards-Leeper, L., Feldman, H. A., Leibowitz, S., Mandel, F., Diamond, D. A., & Vance, S. R. (2012). Children and adolescents with gender identity disorder referred to a pediatric medical center. Pediatrics, 129(3), 418–425. https://doi.org/10.1542/peds.2011-0907.
Spitzer, G. (2016). Parent Support May Help Transgender Children’s Mental Health. April Retrieved in 2018. https://www.npr.org/sections/health-shots/2016/04/11/473292576/parent-support-may-help-transgender-childrens-mental-health.
Steegen, S., Tuerlinckx, F., Gelman, A., & Vanpaemel, W. (2016). Increasing transparency through a multiverse analysis. Perspectives on Psychological Science, 11(5), 702–712. https://doi.org/10.1177/1745691616658637.
Steensma, T. D., & Cohen-Kettenis, P. T. (2011). Gender Transitioning before Puberty? Archives of Sexual Behavior, 40(4), 649–650. https://doi.org/10.1007/s10508-011-9752-2.
Steensma, T. D., Zucker, K. J., Kreukels, B. P., VanderLaan, D. P., Wood, H., Fuentes, A., & Cohen-Kettenis, P. T. (2014). Behavioral and emotional problems on the Teacher’s Report Form: a cross-national, cross-clinic comparative analysis of gender dysphoric children and adolescents. Journal of Abnormal Child Psychology, 42(4), 635–647. https://doi.org/10.1007/s10802-013-9804-2.
Steinmetz, K. (2014). The transgender tipping point. Time Magazine, 183(22), 38–46. https://time.com/magazine/us/135460/june-9th-2014-vol-183-no-22-u-s/. Retrieved in 2020..
Tankard, M. E., & Paluck, E. L. (2017). The effect of a supreme court decision regarding gay marriage on social norms and personal attitudes. Psychological Science, 28(9), 1334–1344. https://doi.org/10.1177/0956797617709594.
Toomey, R. B., Ryan, C., Diaz, R. M., Card, N. A., & Russell, S. T. (2013). Gender-nonconforming lesbian, gay, bisexual, and transgender youth: School victimization and young adult psychosocial adjustment. Psychology of Sexual Orientation and Gender Diversity, 1(S), 71–80. https://doi.org/10.1037/2329-0382.1.S.71.
Toomey, R. B., Ryan, C., Diaz, R. M., & Russell, S. T. (2011). High school gay–straight alliances (GSAs) and young adult well-being: An examination of GSA presence, participation, and perceived effectiveness. Applied Developmental Science, 15(4), 175–185. https://doi.org/10.1080/10888691.2011.607378.
Turban, J. L., & Ehrensaft, D. (2018). Research review: gender identity in youth: treatment paradigms and controversies. Journal of Child Psychology and Psychiatry, 59(12), 1228–1243. https://doi.org/10.1111/jcpp.12833.
Varni, J. W., Thissen, D., Stucky, B. D., Liu, Y., & Gorder, H., et al. (2012). PROMIS® Parent Proxy Report Scales: an item response theory analysis of the parent proxy report item banks. Quality of Life Research, 21(7), 1223–1240. https://doi.org/10.1007/s11136-011-0025-2.
Veale, J. F., Peter, T., Travers, R., & Saewyc, E. M. (2017). Enacted stigma, mental health, and protective factors among transgender youth in Canada. Transgender Health, 2(1), 207–216. https://doi.org/10.1089/trgh.2017.0031.
De Vries, A. L., & Cohen-Kettenis, P. T. (2012). Clinical management of gender dysphoria in children and adolescents: the Dutch approach. Journal of Homosexuality, 59(3), 301–320. https://doi.org/10.1080/00918369.2012.653300.
De Vries, A. L., Steensma, T. D., Cohen-Kettenis, P. T., VanderLaan, D. P., & Zucker, K. J. (2016). Poor peer relations predict parent-and self-reported behavioral and emotional problems of adolescents with gender dysphoria: a cross-national, cross-clinic comparative analysis. European Child & Adolescent Psychiatry, 25(6), 579–588. https://doi.org/10.1007/s00787-015-0764-7.
Wallien, M. S., Swaab, H., & Cohen-Kettenis, P. T. (2007). Psychiatric comorbidity among children with gender identity disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1307–1314. https://doi.org/10.1097/chi.0b013e3181373848.
Watson, R. J., Grossman, A. H., & Russell, S. T. (2019). Sources of social support and mental health among LGB youth. Youth & Society, 51(1), 30–48. https://doi.org/10.1177/2F0044118X16660110.
Wicherts, J. M., Veldkamp, C. L., Augusteijn, H. E., Bakker, M., Van Aert, R., & Van Assen, M. A. (2016). Degrees of freedom in planning, running, analyzing, and reporting psychological studies: a checklist to avoid p-hacking. Frontiers in Psychology, 7, 1832. https://doi.org/10.3389/fpsyg.2016.01832.
Wilson, E. C., Chen, Y. H., Arayasirikul, S., Raymond, H. F., & McFarland, W. (2016). The impact of discrimination on the mental health of trans* female youth and the protective effect of parental support. AIDS and Behavior, 20(10), 2203–2211. https://doi.org/10.1007/s10461-016-1409-7.
Witcomb, G. L., Claes, L., Bouman, W. P., Nixon, E., Motmans, J., & Arcelus, J. (2019). Experiences and Psychological Wellbeing Outcomes Associated with Bullying in Treatment-Seeking Transgender and Gender-Diverse Youth. LGBT Health, 6(5), 216–226. https://doi.org/10.1089/lgbt.2018.0179.
Yong, E. (2019). Young Trans Children Know Who They Are. The Atlantic. Jan Retrieved in 2020. https://www.theatlantic.com/science/archive/2019/01/young-trans-children-know-who-they-are/580366/.
Acknowledgements
We thank Riley Lowe for assistance with data collection, Nandana Rao for assistance with data preparation, and the families for participating in this study.
Author information
Authors and Affiliations
Contributions
K.O. was responsible for funding acquisition and project administration. L.D., K.M., and K.O. shared responsibility for study conception and design. K.O., L.D., S.B., and C.J. shared responsibility for material preparation. Data analysis were conducted by L.E., L.D., and K.F. The first draft of the paper was written by L.D., edited by K.O., K.M., and L.E., and all authors read and approved the final paper.
Funding
This work was supported by the National Institutes of Health (NIH) under Grant HD092347 to K.R.O. and an NSF Graduate Research Fellowship to L.D.
Data Sharing and Declaration
Because some key variables (e.g., state support) could be used, particularly in conjunction with other variables (e.g., race) to potentially identify participants, full data are not publicly available. However, the questions asked to participants are available at https://osf.io/fn37j/?view_only=97399257437c4ac9b7f91f5938296b5b. The data analysis code is available at https://osf.io/fn37j/?view_only=97399257437c4ac9b7f91f5938296b5b.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed were approved by the Institutional Review Board of the University of Washington. All procedures were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants included in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Durwood, L., Eisner, L., Fladeboe, K. et al. Social Support and Internalizing Psychopathology in Transgender Youth. J Youth Adolescence 50, 841–854 (2021). https://doi.org/10.1007/s10964-020-01391-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-020-01391-y