
Abstract
Significant health disparities exist for transgender female (trans*female) youth. We assessed differences in mental health outcomes based on exposure to discrimination among transgender female youth in the San Francisco Bay Area aged 16–24 years. Youth were recruited using a combination of respondent driven sampling with online and social media methods. Logistic regression models were used to estimate odds ratios for the mental health outcomes, comparing levels of discrimination and levels of resiliency promoting protective factors among sexually active youth in the sample (N = 216). High transgender-based discrimination was significantly associated with greater odds of PTSD (AOR, 2.6; 95 % CI 1.4–5.0), depression (AOR, 2.6; 95 % CI 1.2–5.9), and stress related to suicidal thoughts (AOR 7.7, 95 % CI 2.3–35.2). High racial discrimination was significantly associated with greater odds of psychological stress (AOR 3.6; 95 % CI 1.2–10.8), PTSD (AOR 2.1; 95 % CI 1.1–4.2) and stress related to suicidal thoughts (AOR 4.3, 95 % CI 1.5–13.3). Parental closeness was related to significantly lower odds of all four mental health outcomes measured, and intrinsic resiliency positively reduced risk for psychological stress, PTSD, and stress related to suicidal thoughts. Transgender and racial discrimination may have deleterious effects on the mental health of trans*female youth. Interventions that address individual and intersectional discrimination and build resources for resiliency and parental closeness may have success in preventing mental health disorders in this underserved population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High prevalence and significant disparities in mental health exist for transgender youth assigned a male sex at birth who identify as a different gender (trans*female youth) [1–3]. Studies assert that prejudice towards transwomen occurs because they are perceived to transgress societal gender norms [4]. Prejudice is enacted in numerous forms of discrimination resulting in everything from discrimination in education, employment and health care to unpunished violence and murder of transwomen, especially transwomen of color [5, 6]. Discrimination and rejection due to gender nonconformity often starts at an early age and puts trans*female youth at risk of isolation, school dropout and academic performance issues [7]. From a systems perspective, discrimination based on transgender identity leads to unequal access to education, employment, and other economic resources [6, 8], which then create economic insecurity impacting safe housing and income. Economic hardship due to transphobia may be a primary reason why some transwomen turn to sex work, which raises their risk for HIV, other sexually transmitted diseases and violence [9–11].
An important and understudied area of research is the link between discrimination and mental health outcomes for trans*female youth. Discrimination has been linked to poor mental health outcomes among adult transgender people. Prevalence of suicide attempts in the transgender population range from 18 to 41 %, which is 15–38 percentage points higher than in the overall U.S. population [5]. Compared with cisgender females, transwomen have reported lower overall mental health and quality of life [12]. A study of transwomen and transmen in Australia recently found that almost half of the sample experienced psychological distress; psychological distress was associated with younger age, lack of family social support and greater number of victimization experiences, pointing to heightened need for research with youth in the trans population [13]. Recent research found that transgender youth had significantly higher risk for depression, anxiety, and suicide when compared to cisgender youth matched controls [3]. In a study of transmen and transwomen, factors associated with substance use disorder and a history of substance use treatment included being a transwoman, lifetime PTSD, current depression, and current mental health treatment [14]. In a previous analysis of this dataset, we found that transgender-related discrimination is associated with increased odds of alcohol and drug use in our sample of trans*female youth [15]. Stress related to transgender-based discrimination may similarly affect mental health outcomes in this population.
Racial discrimination on top of gender-based stigma may exert a profound effect on mental health. Racism has been linked to poor mental health among racial/ethnic minority populations [16, 17]. New research has investigated the pathways to poor health outcomes and identified stress as a primary mechanism affecting the mental health of racial/ethnic minority individuals [18]. For racial/ethnic minority trans*female youth who manage multiple marginalized social identities (i.e., racial minorities who are gender minorities), extreme heightened stress and fewer coping mechanisms may result in poorer mental health [19]. In the transgender literature, there are major gaps in how intersections of race and transgender identity impact mental health outcomes among transgender people. Such research is needed to determine if there are disparities in mental health risks within the trans community and to properly target prevention and care interventions.
Resiliency factors that protect from risks related to discrimination are also needed. Positive parental relationships may be a critical protective factor for transgender youth as has been found with gay, lesbian and bisexual youth [20]. Though the literature is limited, one study found that trans*female youth who reported having support from at least one parent were more likely to report consistent safe sex compared to youth who were rejected by family [21]. Intrinsic resiliency, or the ability, assets, and skills of youth to overcome adversity and have positive health and social outcomes, may also be protective of various forms of discrimination [22]. There may also be resiliency promoting factors that are specific to trans*female youth, such as access to transgender-specific health care for youth who are interested in such care. A study by Rotundi found that transgender people ready but not able to medically transition were more likely to have depressive symptoms than peers who began the transition process [23]. Conversely, in a study comparing quality of life between transwomen on and off hormones, utilization of hormonal therapy was associated with higher quality of life scores in general and better mental health overall [24]. Having friends who are transgender or supportive of one’s gender identity may also be a unique and important resiliency-promoting factor. Such friends may be protective from bullying and could serve as positive forms of social support and information about transitioning [25, 26].
The current study was conducted to determine the prevalence of transgender-based, racial and trans-racial discrimination experienced by participants in a large cohort of trans*female youth aged 16–24 years. We also examined the relationship between discrimination and mental health to determine if high exposure to discrimination is associated with poor mental health outcomes. To do so, we assessed three different types of discrimination—transgender-based, racial, and combined transgender-based and racial (trans-racial) discrimination—on the mental health of trans*female youth. We also sought to test the protective effect of important youth resiliency promoting factors to give providers and interventionists directions for supporting trans*female youth who face discrimination that negatively impacts their mental health.
Methods
Participants
SHINE is a study of HIV risk and resiliency among trans*female youth in the San Francisco Bay Area; the present analysis uses data from enrollment visits between August 2012 and December 2013 as a cross-sectional sample. The target sample size for the study was 300. Study participants were initially recruited using a peer-referral method to obtain a diverse sample of this hard-to-reach population. Slow recruitment chains resulted in adaptations to the sampling methodology including allowance of e-referrals and expanding the number of referrals that successful recruiters could have [27]. In total, 79 participants were recruited through peer referral only, while 221 participants were recruited using respondent driven sampling (RDS) in combination with social networking outreach [28]. In addition to peer referral, participants were recruited through outreach on social networking sites (e.g., Facebook, Tumblr), in person at events attended by trans*female youth (e.g., Trans March, Queer Prom), and with referrals from both community-based organizations that provide social services to transgender women and youth and gender-specific health clinics (additional details provided in a manuscript outlining the recruitment methods [28]). Individuals were eligible for the study if they: [1] self-identified as any gender other than that typically associated with their assigned male sex at birth, [2] were 16–24 years of age, and [3] lived in the San Francisco Bay Area. Data for this analysis only included participants who were HIV-negative. Informed consent was obtained before starting the behavioral survey, which was administered via hand-held tablet computers and took about 1 h on average to complete, and conducting a rapid HIV test. Youth were given a $50 incentive for participation in the study. All study procedures were approved by the Institutional Review Board at the University of California, San Francisco. Written consent was obtained from all youths. For those who were under 18 years of age, written consent was provided in accordance with a review board waiver of parental consent.
Measures
Socio-demographic Factors
Basic demographic factors assessed were age, gender, race/ethnicity, whether youth were born in the U.S. or abroad, sexual orientation (straight/heterosexual, lesbian/gay, queer, bisexual, pansexual, questioning, no p1.00), HIV status, education (in school/GED/HS graduate; highest grade attained); income (inclusive of all sources of income and dichotomized to those above and below the federal poverty level); unstable housing currently (defined as a hotel, rooming house, transitional housing, or homeless shelter) and as a child between kindergarten and age 16 (Y/N responses); and living situation as a child (i.e., with parents of origin, family caregiver, were adopted or lived in foster care).
Predictors
Discrimination ever based on transgender identity, race or both were the primary exposures to predict risk for mental health disorders as measured by brief mental health screeners conducted as part of this study. Racial discrimination measures were drawn from the discrimination items in Nancy Krieger’s standardized “experiences of discrimination measure” [29] that all begin with the preface, “Have you ever experienced discrimination, been prevented from doing something, or been hassled or made to feel inferior in any of the following situations because of your race, ethnicity or color?” Experiences of transgender-based discrimination were measured as yes/no responses to various types of discrimination due to youths’ gender identity or gender presentation. We measured transgender and racial discrimination based on five items—(1) discrimination in trying to get a job, (2) discrimination at school (race)/having to change schools or drop out (gender), (3) discrimination at work (race)/losing a job or career opportunity (gender), (4) discrimination in obtaining housing (race)/having to move from family or friends (gender), and (5) discrimination in medical care (race)/getting health care services (gender). Youth who responded yes to 2 or more items for each type of discrimination were categorized as having high exposure to racial, and/or transgender- related discrimination. Youth who reported high exposure to both transgender-based and racial discrimination were categorized as experiencing high trans-racial discrimination.
Outcomes
Psychological distress was measured with the 18 item version of the Brief Symptom Inventory (BSI-18), converting the BSI-18 Global Severity Index (GSI) to T-scores and using a validated clinical cutoff of T > 62 for symptomatic psychological distress in the last 7 days [30–32]. The BSI-18 assesses symptoms in the last 12 months. We rescaled the BSI and our cutoff for psychological stress was a score of 62 or greater. The BSI-18 T-scores calculated in this study had high internal consistency (Cronbach’s alpha = 0.92). We assessed depressive symptoms in the past week using the short version of the Center for Epidemiologic Studies Depression Scale [33]. Based off of 4 items measured, each with possible values of 0, 1, 2, or 3, we required that at least 3 of the 4 items have responses of 2 or greater to be categorized as having symptoms of depression. We used the primary care posttraumatic stress disorder screen items from the brief New York PTSD Risk Score [34] to assess trauma symptoms in the past year. Based off of 4 yes/no items, we required that at least 3 of the 4 items have a response of yes. PTSD scores calculated in this study had high internal consistency (Cronbach’s alpha = 0.70). Stress related to thoughts of suicide was measured with the item, “How much were you distressed by thoughts of ending your life?” Responses we measured on a 5-point Likert scale ranging from “not at all” to “extremely”. Any response other than “not at all” was coded as positive. This item was asked about stress related to thoughts of suicide over the last year.
Resiliency Promoting Protective Factors: For this study, we utilized the Connor Davidson Resilience Scale (CD-RS) [35] of intrinsic resiliency for trans*female youth. The CD-RISC contains 25 items, all of which carry a 5-point range of responses with a maximum score of 100 for each participant. The CD-RS scores calculated in this study had high internal consistency (Cronbach’s alpha = 0.89). To measure support from transgender peers, we used our transgender community connectedness measure, which is an 11-item scale that was adapted from the gay community connectedness measure and has been previously validated in minority populations [36]. To measure social support, we used an adapted social support measure developed based on the 12-item Multidimensional Scale of Perceived Social Support (MSPSS) [37] that first asked youth from whom they get the most support (e.g., parents, chosen family, mentor). The participant’s chosen support was then inserted in place of the word ‘‘family’’ for four of the items assessed in the MSPSS. Youth were asked questions like ‘‘I can talk about my problems with my [person(s) listed above].’’ A scaled global social support value was then computed as the sum of the responses to the individual questions; the alpha coefficient for this sample was 0.9 in a prior study with this population [36]. Parental acceptance was measured by developing 10 questions based on research from the Family Acceptance Project [38]. Parental closeness was measured with 5 items: (a) warmth and love from parents while growing up, (b) parents encouraging independence, (c) teaching right from wrong, (d) satisfaction with mother–child communication, and (e) satisfaction with closest parent relationship. The absence of barriers to transgender-specific health care was assessed with the question, “Have you ever had any problems getting health care because of your gender identity or presentation?”
Analysis
The original study was conducted to identify risk and resiliency promoting factors related to HIV. To inform HIV prevention efforts, this analysis was conducted with youth in the sample who self-reported being HIV-negative. The first step of the analysis was to assess exposure to racial and transgender-related discrimination overall for youth in the sample, separately and combined. Next we assessed differences in mental health outcomes (i.e., BSI, PTSD, Depression and stress related to suicidal thoughts) between those with high versus low exposure to racial, transgender-related and trans-racial discrimination. To do so, we fit logistic regression models to estimate odds ratios for the mental health outcomes, comparing levels of discrimination types and adjusting for age and race. Age and race covariates were chosen a priori. Youth who reported high exposure to both racial and transgender-related discrimination were part of a separate group for analysis having high exposure to trans-racial discrimination. We then assessed whether protective factors were related to mental health outcomes. First, we conducted analyses to determine if there were significant differences in reporting of the protective factors of resiliency, community connectedness, social support, parental acceptance and parental closeness by age and race. We then fit logistic regression models to estimate odds ratios for mental health outcomes, comparing levels of protective factors and adjusting for age and race. We used cubic spline adjustment for age, with knots at the quartiles. We used a 95 % level for all confidence intervals. We conducted all analysis in R (Revolution Analytics, Palo Alto, CA).
Results
Demographics and Exposure to Discrimination
There were a total of 216 sexually active HIV-negative trans*female youth in this sample (Table 1). Nearly half (44 %) were aged 21 years and under, while 56 % were aged 22–24. Most youth in the sample (81.9 %) were aged 20–24 years. Most youth identified as female (44.4 %), followed by transgender (31.9 %), and genderqueer (i.e., identify as neither woman nor man) (16.7 %). The sample was 34.3 % White, 23.1 % Latina, 15.3 % mixed race, 13.4 % African American, and 5.6 % Asian; 8.3 % identified as other. Almost half of youth had some college or more education (46.8 %). Almost three quarters lived on $1000 or less month (71 %) and 21.8 % were unstably housed. Almost half of youth moved two or more times during their childhood (43.5 %), and 81.5 % lived with their family of origin as a child.
More than one quarter of youth (26.2 %) reported high racial discrimination, almost half (45.9 %) reported high transgender-based discrimination, 15.9 % reported high transgender-based and high racial discrimination (Table 1). Only 37 % reported low exposure to discrimination. Racial discrimination as trans-racial discrimination (30.3 %) was disproportionately higher among African Americans (28.3 %) relative to the composition of the overall sample (only 13.4 % were African American). The same was true for heterosexuals. Racial (42.3 %) and trans-racial discrimination (48.5 %) were elevated among heterosexuals who only made up 32.3 % of those comparing sexual orientation groups. Racial (28.3 %) and trans-racial discrimination (39.4 %) was also disproportionately higher for those who were unstably housed (21.8 % were unstably housed). Racial discrimination and trans-racial discrimination were disproportionately higher among those who had moved 2 or more times as a child (65.4 and 66.7 %, respectively compared to 43.5 % overall who had moved 2 or more times as a child). Disproportionately high rates of racial and trans-racial discrimination were reported by youths who were in foster care as children (11.3 and 12.1 %, respectively vs. 5.1 % of the overall population).
Discrimination and Mental Health Disorders/Psychological Stress
Discrimination has differential impacts on mental health depending on the type of discrimination. Those with higher exposure to transgender-based discrimination had almost three times the odds of PTSD compared to those with lower exposure (AOR, 2.6; 95 % CI 1.4–5.0) (Table 2). Those with higher exposure to transgender-based discrimination had more than 2 times the odds of depression than those with lower exposure (AOR, 2.6; 95 % CI 1.2–5.9). High exposure to transgender-based discrimination had the most significant impact on stress related to thoughts of suicide. Those reporting higher exposure to transgender-based discrimination reporting almost 8 times higher odds of stress related to thoughts of suicide compared to those with lower exposure (AOR 7.7, 95 % CI 2.3–35.2), though the confidence intervals were wide. Those with higher exposure to racial discrimination had significantly higher odds of psychological distress (i.e., as measured by the BSI) (AOR 3.6; 95 % CI 1.2–10.8) and PTSD symptoms (AOR 2.1; 95 % CI 1.1–4.2) than those with lower exposure. Those with higher exposure to racial discrimination had significantly higher odds of stress related to thoughts of suicide than those with lower exposure (AOR 4.3, 95 % CI 1.5–13.3). Those with higher exposure to both transgender-based and racial discrimination had higher odds of PTSD symptoms (AOR 2.5, 95 % CI 1.0–6.7) and stress related to thoughts of suicide (AOR 3.4, 95 % CI 1.1–10.8) compared to those with lower exposure to both types of discrimination.
Protective Factors for Mental Health Disorders/Psychological Stress
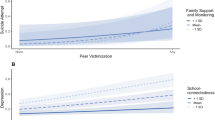
Parental Closeness was the most consistently protective resiliency promoting factor for mental health disorders and psychological distress (Table 3). Youth with higher parental closeness had significantly lower odds of psychological distress (AOR 0.3, 95 % CI 0.1–0.9), PTSD symptoms (AOR 0.4, 95 % CI 0.2–0.7), depression (AOR 0.4, 95 % CI 0.2–0.9), and stress related to thoughts of suicide (AOR 0.2, 95 % CI 0.0–0.9) compared to those with lower parental closeness. Youth who reported higher resiliency had significantly lower odds of psychological distress (AOR 0.3, 95 % CI 0.1–0.8), PTSD symptoms (AOR 0.4, 95 % CI 0.2–0.7), and stress related to thoughts of suicide (AOR 0.1, 95 % CI 0.0–0.3) compared to those with lower resiliency. Youth with higher parental acceptance of their transgender identity reported significantly lower odds of PTSD compared to those with lower parental acceptance (AOR 0.4, 95 % CI 0.2–0.7).
Discussion
Results suggest that transgender-based discrimination is the most pervasive type of discrimination experienced by trans*female youth with the greatest impact on mental health. More than 40 % of the sample reported experiencing transgender-based discrimination, which was in turn was related to threefold higher odds of PTSD, double the odds of depression and an eightfold increase in odds for stress related to suicidal thoughts. Fewer youth reported experiencing racial discrimination; however, racial discrimination was significantly related to an almost fourfold higher odds of psychological stress and double the odds of PTSD.
The most notable mental health impact of discrimination was on stress related to suicidal thoughts. All three types of discrimination measured significantly increased the odds of stress related to suicidal thoughts. The National Transgender Discrimination Survey found that those who were bullied, harassed, assaulted, or expelled because they were transgender or gender non-conforming in school had elevated levels of suicide attempts (51 %) [5]. Clements-Nolle found in 2006 that discrimination related to being transgender was an independent predictor of suicide [39]. In 2012, Testa et al. [40] found that transwomen who experienced physical violence, of which 97 % was related to being transgender, had an almost 4 times greater odds of suicidal ideation and more than 5 times greater odds of suicide attempts.
Findings regarding the impact of transgender-based discrimination on depression were echoed in the literature with adults. A recent prospective study of transwomen found that psychological and physical gender abuse was a cause of major depression [41]. Consistent with the research among adult transwomen, levels of depression were also higher than that found in the general youth population [42]. Findings regarding psychological distress are unique and point to the important intersection of racial and gender minority status. Racial discrimination was the only type of discrimination that impacted psychological distress, which aligns with current research efforts showing adult sexual minority populations are negatively impacted by racial discrimination [43]. Given the great impact of transgender-based discrimination in relation to racial discrimination in this study, future efforts to address mental health among racial minority trans*female youth may need to consider strengthening assets to address transgender-based discrimination specifically at the intersection of gender, racial and sexual minority identities.
The overall impact of all transgender and racial discrimination on mental health for trans*female youth may have important implications for the future health and wellbeing of this population. Prior analyses of these data found a link between psychological distress and substance use, and sex while under the influence [15]. Victimized lesbian, gay and bisexual youth have exhibited higher engagement in sexual risk behavior due to feelings of isolation and psychological distress [44]. Similarly, Nuttbrock et al. [41] recently found that gender-related abuse caused depressive symptoms that predicted HIV and STIs for young transwomen. Victimization also impedes learning and other school based outcomes for youth, which then impacts youths’ ability to succeed in school and the job market [45].
The primary limitation to this study is that it was not population-based and therefore cannot be generalized to the entire trans*female youth population. However, this is the largest sample of trans*female youth in a geographical area known to be a draw to gender non-conforming people of all ages, and may represent a large portion of all trans*female youth in the San Francisco Bay Area. Also, temporal issues may have arisen in the findings about resiliency. For example, youth with higher parental acceptance may have had lower odds of PTSD because they were not abused by their parents and not because accepting parents protected from the effect of other types of trauma.
Despite these limitations, these data provide an important starting point for interventions and programs to address risk for mental health disorders that impact substance use and HIV risk. Data from this study clearly demonstrate the impact of discrimination on mental health and behaviors. Interestingly, different types of discrimination were associated with different mental health symptoms, suggesting the need for interventions that address discrimination-related stressors specific to both gender identity and race/ethnicity. Interventions seeking to address stigma need to pay particular attention to intersectional identities. This study also documents the importance of parental support. Of the six resiliency promoting protective factors, parents emerged as two of the three significant protective factors from poor mental health outcomes among trans*female youth in this study. Once again, we find that parents and caregivers are central to the health and wellbeing of our young people. Interventions that foster understanding between youth and their parents may go far in promoting the health of this important population.
References
Brennan J, Kuhns LM, Johnson AK, et al. Syndemic theory and HIV-related risk among young transgender women: the role of multiple, co-occurring health problems and social marginalization. Am J Public Health. 2012;102(9):1751–7.
Garofalo R, Deleon J, Osmer E, Doll M, Harper GW. Overlooked, misunderstood and at-risk: exploring the lives and HIV risk of ethnic minority male-to-female transgender youth. J Adoles Health Off Publ Soc Adoles Med. 2006;38(3):230–6.
Reisner SL, Vetters R, Leclerc M, et al. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. J Adoles Health Off Publ Soc Adoles Med. 2015;56(3):274–9.
Hill DB, Willoughby BLB. The development and validation of the Genderism and Transphobia Scale. Sex Roles. 2005;53:531–44.
Grant JM, Mottet LA, Tanis J, Herman JL, Harrison J, Keisling M. National Transgender Discrimination Survey Report on health and health care. National Center for Transgender Equality; 2010.
Bradford J, Reisner SL, Honnold JA, Xavier J. Experiences of transgender-related discrimination and implications for health: results from the Virginia Transgender Health Initiative Study. Am J Public Health. 2013;103(10):1820–9.
Bockting W. The inmpact of stigma on transgender identity development and mental health. In: Kreukels BPC, Steesma TD, Vries ALCd, editors. Gender dysphoria and disorders of sex development. New York: Springer; 2014. p. 319–30.
Xavier J, Honnold JA, Bradford J. The Health, health-related needs, and lifecourse experiences of transgender Virginians. Virginia Commonwealth University; 2007.
Sugano E, Nemoto T, Operario D. The impact of exposure to transphobia on HIV risk behavior in a sample of transgendered women of color in San Francisco. AIDS Behav. 2006;10(2):217–25.
Wilson EC, Garofalo R, Harris RD, et al. Transgender female youth and sex work: HIV risk and a comparison of life factors related to engagement in sex work. AIDS Behav. 2009;13:902–13.
Lombardi EL, Wilchins RA, Priesing D, Malouf D. Gender violence: transgender experiences with violence and discrimination. J Homosex. 2001;42(1):89–101.
Ainsworth TA, Spiegel JH. Quality of life of individuals with and without facial feminization surgery or gender reassignment surgery. Qual Life Res Int J Qual Life Aspects Treat Care Rehabil. 2010;19(7):1019–24.
Blosnich JR, Gordon AJ, Fine MJ. Associations of sexual and gender minority status with health indicators, health risk factors, and social stressors in a national sample of young adults with military experience. Ann Epidemiol. 2015;25(9):661–7.
Keuroghlian AS, Reisner SL, White JM, Weiss RD. Substance use and treatment of substance use disorders in a community sample of transgender adults. Drug Alcohol Depend. 2015;152:139–46.
Rowe C, Santos GM, McFarland W, Wilson EC. Prevalence and correlates of substance use among trans*female youth ages 16–24 years in the San Francisco Bay Area. Drug Alcohol Depend. 2014.
Ertel KA, James-Todd T, Kleinman K, et al. Racial discrimination, response to unfair treatment, and depressive symptoms among pregnant black and African American women in the United States. Ann Epidemiol. 2012;22(12):840–6.
Krieger N, Kosheleva A, Waterman PD, Chen JT, Koenen K. Racial discrimination, psychological distress, and self-rated health among US-born and foreign-born Black Americans. Am J Public Health. 2011;101(9):1704–13.
Berger M, Sarnyai Z. “More than skin deep”: stress neurobiology and mental health consequences of racial discrimination. Stress. 2015;18(1):1–10.
Meyer IH, Schwartz S, Frost DM. Social patterning of stress and coping: does disadvantaged social statuses confer more stress and fewer coping resources? Soc Sci Med. 2008;67(3):368–79.
Needham BL, Austin EL. Sexual orientation, parental support, and health during the transition to young adulthood. J Youth Adolesc. 2010;39(10):1189–98.
Wilson EC, Iverson E, Belzer M, the Adolescent Meicine Trials Network for HIV/AIDS Interventions. Parental support and condom use among transgender female youth. 2010.
Rutter M. Psychosocial resilience and protective mechanisms. In: Cichheti D, Nuechterlien K, Weintraub S, editors. Risk and protective factors in the development of psychopathology. New York, NY: Cambridge University Press; 1991. p. 331–74.
Rotondi NK, Bauer GR, Scanlon K, Kaay M, Travers R, Travers A. Nonprescribed hormone use and self-performed surgeries: “do-it-yourself” transitions in transgender communities in Ontario, Canada. Am J Public Health. 2013;103(10):1830–6.
Gorin-Lazard A, Baumstarck K, Boyer L, et al. Is hormonal therapy associated with better quality of life in transsexuals? A cross-sectional study. J Sexual Med. 2012;9(2):531–41.
Robinson JP, Espelage DL. Peer victimization and sexual risk differences between lesbian, gay, bisexual, transgender, or questioning and nontransgender heterosexual youths in grades 7–12. Am J Public Health. 2013;103(10):1810–9.
Sausa LA, Keatley J, Operario D. Perceived risks and benefits of sex work among transgender women of color in San Francisco. Arch Sex Behav. 2007;36(6):768–77.
Truong HM, Grasso M, Chen YH, et al. Balancing theory and practice in respondent-driven sampling: a case study of innovations developed to overcome recruitment challenges. PLoS ONE. 2013;8(8):e70344.
Arayasirikul S, Chen YH, Jin H, Wilson E. A Web 2.0 and Epidemiology Mash-Up: Using Respondent-Driven Sampling in Combination with Social Network Site Recruitment to Reach Young Transwomen. AIDS Behav. 2015; 26.
Krieger N, Smith K, Naishadham D, Hartman C, Barbeau EM. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc Sci Med. 2005;61(7):1576–96.
Derogatis LR. BSI-18: administration, scoring and procedures manual. Minneapolis, MN: National Computer Systems; 2000.
Mustanski B, Newcomb M, Garofalo R. Mental health of lesbian, gay, and bisexual youth: a developmental resiliency perspective. J Gay Lesbian Soc Serv. 2011;23(2):204–25.
Asner-Self KK, Schreiber JB, Marotta SA. A cross-cultural analysis of the Brief Symptom Inventory-18. Cult Diver Ethnic Minor Psychol. 2006;12(2):367–75.
Radloff L. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401.
Boscarino JA, Kirchner HL, Hoffman SN, Sartorius J, Adams RE, Figley CR. A brief screening tool for assessing psychological trauma in clinical practice: development and validation of the New York PTSD Risk Score. Gen Hosp Psychiatry. 2011;33(5):489–500.
Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82.
Wilson EC, Garofalo R, Harris RD, et al. Transgender female youth and sex work: HIV risk and a comparison of life factors related to engagement in sex work. AIDS Behav. 2009;13(5):902–13.
Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Person Assess. 1990;55(3–4):610–7.
Ryan C, Russell ST, Huebner D, Diaz R, Sanchez J. Family acceptance in adolescence and the health of LGBT young adults. J Child Adoles Psychiatr Nurs Off Publ Assoc Child Adoles Psychiatr Nurs 2010;23(4):205–13.
Clements-Nolle K, Marx R, Katz M. Attempted suicide among transgender persons: the influence of gender-based discrimination and victimization. J Homosex. 2006;51(3):53–69.
Testa RJ, Sciacca LM, Wang F, et al. Effects of violence on transgender people. Prof Psychol Res Pract. 2012;43(5):452–9.
Nuttbrock L, Bockting W, Rosenblum A, et al. Gender abuse, depressive symptoms, and HIV and other sexually transmitted infections among male-to-female transgender persons: a three-year prospective study. Am J Public Health. 2013;103(2):300–7.
Hoffman B. An overview of depression among transgender women. Depress Res Treat. 2014;2014:394283.
Cochran SD, Mays VM, Alegria M, Ortega AN, Takeuchi D. Mental health and substance use disorders among Latino and Asian American lesbian, gay, and bisexual adults. J Consult Clin Psychol. 2007;75(5):785–94.
Rosario M, Hunter J, Maguen S, Gwadz M, Smith R. The coming-out process and its adaptational and health-related associations among gay, lesbian, and bisexual youths: stipulation and exploration of a model. Am J Commun Psychol. 2001;29(1):133–60.
Poteat VP, Scheer JR, Mereish EH. Role of gender in educational contexts and outcomes. In: Liben LB, Bigler RS, editors Advances in child development and behavior, Vol 47. San Diego, CA: Elsevier Academic Press; 2014. p. 261–300.
Acknowledgments
The grant was completed with funding from the National Institutes of Mental Health, Grant # R01MH095598. Most importantly, we want to acknowledge and thank the trans*female youth community in the San Francisco Bay Area who contributed their time and expertise to provide a better understanding of factors affecting their health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Wilson, E.C., Chen, YH., Arayasirikul, S. et al. The Impact of Discrimination on the Mental Health of Trans*Female Youth and the Protective Effect of Parental Support. AIDS Behav 20, 2203–2211 (2016). https://doi.org/10.1007/s10461-016-1409-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-016-1409-7