
Abstract
Experiences of peer victimization are common in adolescence and have been associated with a broad variety of psychopathology in adolescence. The present study aimed to test whether some types of victimization are more harmful than others; whether the harms associated with different types of peer victimization are specific to particular domains of psychopathology; and whether these relationships vary by gender. Participants included adolescents aged 14–15 from a nationally representative cohort study (n= 3335; mean age 14.4 years; 49.1% female; 90.1% spoke English as the main language at home). Participants provided self-report information on their experiences of peer victimization, as well as symptoms of depression, anxiety, conduct problems, hyperactivity and inattention, and substance use. These data were analyzed in a dimensional and hierarchical framework using latent variable indirect effects modeling. The associations between peer victimization and psychopathology were not unique to specific symptom domains, but rather showed broadband associations with all symptom domains via a transdiagnostic association with general psychopathology. For example, an average of only 9% of the total relationship with each symptom domain was unique to the symptom-domain level, with the remaining proportion accounted for by higher-order factors (i.e., internalizing, externalizing, and general psychopathology). Further, the strength of the relationships did not vary as a function of the type of peer victimization experience (i.e., physical, verbal, or relational), and showed evidence of strict measurement invariance by gender. These findings suggest that peer victimization might present a useful target for the prevention of general psychopathology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Experiences of peer victimization are common and harmful (Vaillancourt et al. 2010). The negative effects of physical (e.g., pushing, hitting), verbal (e.g., name calling), and relational (e.g., exclusion, rumor spreading) victimization are pervasive—spanning poor school adjustment (Juvonen et al. 2011), negative social outcomes (Kokkinos and Kipritsi 2012), low self-worth (Hawker and Boulton 2000), and poor physical health (Bogart et al. 2014). The association with psychopathology (i.e., mental illness) is particularly robust. For example, exposure to peer victimization has been found to predict earlier onset and greater severity of specific mental disorders (e.g., Snyder et al. 2004), as well as higher comorbidity (e.g., Ranta et al. 2009), and poorer treatment outcomes (e.g., Nanni et al. 2012), with these adverse outcomes persisting into adulthood (Arseneault 2017). However, there are three noteworthy key gaps in the literature regarding the strength, specificity, and gender invariance of the relationships between different types of peer victimization and domains of psychopathology, as described below. This study aimed to address these three gaps in the literature during the key developmental period of adolescence.
Several meta-analytic efforts to synthesize the large literatures on the relationships between victimization experiences and psychopathology have concluded that peer victimization is separately associated with symptoms of most common mental disorders, particularly internalizing problems. For example, Hawker and Boulton’s (2000) meta-analysis found a particularly strong relationship with depression, and a smaller but significant relationship with anxiety. Similarly, Reijntjes et al. (2010) meta-analyzed the longitudinal literature and found bidirectional associations among peer victimization and internalizing problems in childhood and adolescence. Extending the findings beyond internalizing problems, Reijntjes et al. (2011) found prospective bidirectional associations of a similar magnitude with externalizing problems. More recently, Moore et al. (2017) conducted a meta-analysis on 165 prospective and cross-sectional studies on the consequences of peer victimization in childhood and adolescence, finding strong evidence for relationships with depression, anxiety, and drug use, and smaller associations with externalizing disorders and alcohol use. Most recently, Schoeler et al. (2018) meta-analyzed the extant quasi-experimental literature (i.e., studies based on twin designs, fixed effects analysis, or propensity score matching) to quantify the detrimental consequences of peer victimization on both internalizing (e.g., depression, anxiety, and stress) and externalizing (e.g., violence, misconduct, hyperactivity) symptoms. While shared genetic influences have been found to account for part of the relationship between experiences of peer victimization and psychopathology (e.g., 44–61% of the association with delinquent behavior and a brief measure of internalizing symptoms; Connolly and Beaver 2016), Schoeler et al. (2018) found evidence of adverse causal effects on both internalizing and externalizing domains after taking these shared genetic influences into account. Taken together, the literature suggests that there are associations between experiences of peer victimization and symptoms of psychopathology that span most of the common mental disorders in childhood and adolescence.
Three Gaps in the Literature
While a large body of literature demonstrates consistent evidence of psychological harm associated with experiences of peer victimization, research in this field over the past 30 years has tended to fall into four silos: (1) Examining a specific form of bullying (e.g., verbal, physical, or relational) and its association with an individual disorder (e.g., social anxiety or major depression; Siegel et al. 2009); (2) investigating a specific type of bullying (e.g., physical) and its links with global measures of mental health (e.g., general well-being or life satisfaction; Martin and Huebner 2007); (3) aggregating experiences of peer victimization to examine the relationships with a specific disorder (e.g., depression; Sweeting et al. 2006); or (4) examining the associations between global measures of both peer victimization and mental health (e.g., Salle et al. 2018). These approaches have converged on robust evidence for the relationship between experiences of peer victimization and psychopathology, but leave three key questions unanswered (see Vachon et al. 2015 for an introduction to these questions in the context of the effects of child maltreatment).
First, the question of (non-)equivalence of harm: Are some types of peer victimization experiences (e.g., relational, physical, or verbal) more strongly related to psychopathology than others? There is an implicit assumption underlying current school policy and staff responsiveness that physical victimization is the most harmful form, as it results in harsher penalties at considerably lower thresholds (i.e., immediate suspension or dismissal) than other more covert forms of victimization (e.g., relational victimization), which are reprimanded less explicitly or consistently (Bauman and Del Rio 2006; Byers et al. 2011). Ironically, there is some evidence that relational bullying is not only more common, but more harmful than physical and verbal victimization for social anxiety in particular (e.g., Siegel et al. 2009; Storch et al. 2005). However, the literature to date has compared these relationships for only a few specific domains of psychopathology and largely aggregates peer victimization experiences (e.g., Moore et al. 2017; Sweeting et al. 2006). The possibility that differences exist in the strength of the associations for different types of peer victimization experiences with psychopathology has therefore not been systematically explored. If such differences exist, they have important implications for policy, as well as for maximizing efficiency in the development and distribution of resources for targeting peer victimization.
Second, the question of outcome specificity: Do particular types of peer victimization experiences have associations with specific disorders, or do they represent broadband risks for psychopathology in general? In the extant literature, there is some evidence for specificity. For example, two recent studies have found evidence that peer victimization experiences are uniquely and prospectively associated with symptoms of both depression and anxiety after controlling for their overlap (Forbes et al. 2019; Stapinski et al. 2015). Further, Forbes et al. (2019) found preliminary evidence that specific types of peer victimization may have differential associations with psychopathology symptom domains. For example, childhood symptoms of depression, but not anxiety, were related to experiences of physical and relational victimization in early adolescence; and anxiety, but not depressive symptoms, was related to cyber victimization. These findings are consistent with meta-analytic evidence that depression is more strongly related to peer victimization than anxiety (e.g., Hawker and Boulton 2000), but have not been replicated. Further, outcome specificity has not been examined systematically for any type of peer victimization experience across the common symptom domains of adolescent psychopathology, which include depression and anxiety, but also externalizing behaviors such as conduct problems, hyperactivity and inattention, and substance use. It therefore remains unknown whether there are additional disorder-specific relationships beyond the internalizing domains examined to date. It is also unclear to what extent the disorder-specific relationships in the literature will be generalizable. Finding robust outcome specificity would have important implications for the development of targeted interventions. In contrast, finding non-specificity would indicate that broadband preventive interventions and transdiagnostic treatments may be more efficacious.
Third, the question of gender invariance: Does gender moderate the strength of the associations between peer victimization experiences and psychopathology? The prevalence of peer victimization experiences is often found to vary by gender, where girls are victimized more, particularly in high school (Vaillancourt et al. 2010), but boys experience more physical victimization (Hymel and Swearer 2015). Further, girls experience more internalizing symptoms and boys experience more externalizing symptoms (Martel 2013), with this pattern persisting into adulthood (Boyd et al. 2015). There is preliminary evidence that gender may moderate the strength of the associations between peer victimization and psychopathology, which would be consistent with these differential patterns of prevalence (e.g., anxiety has been found to relate more strongly to peer victimization for girls; Sentse et al. 2017). However, many studies have found the relationships to be invariant by gender (e.g., Forbes et al. 2019; Kendrick et al. 2012; Lösel and Bender 2011; Schaefer et al. 2018; Storch et al. 2005). Finding boys or girls to be differentially vulnerable to specific types of victimization would have further implications for the development of targeted treatments and would aid in identifying potentially vulnerable individuals for additional support.
To address these three gaps in the literature, adolescence represents a key developmental period, as peer victimization experiences are common and peer relationships become increasingly important and more complex (Sentse et al. 2015). At the same time, emotion regulation is underdeveloped (Gogtay et al. 2004) and stress-reactivity is heightened (Spear 2009), suggesting experiences of victimization in adolescence may be associated with an increased emotional response and greater difficulty regulating these responses (Schaefer et al. 2018). Further, adolescence is a key period of vulnerability for the onset of common mental disorders such as depression and substance abuse, which have very low prevalence prior to this age (Kessler et al. 2005).
Taking a Transdiagnostic and Hierarchical Approach to These Questions
An emerging literature has proposed the use of a transdiagnostic and hierarchical model of psychopathology to examine these questions with respect to the relationships between environmental stressors and psychopathology (cf. Conway et al. 2019, 2018; Forbes et al. 2015; Kotov et al. 2017). This type of model is based on the systematic patterns of co-occurrence among common mental disorders in adults (Krueger et al. 1998) and common behavior problems in children (Achenbach and Edelbrock 1978), which highlight broad dimensions of internalizing and externalizing psychopathology that underlie these patterns. This internalizing-externalizing model has also been extended hierarchically to include a general factor of psychopathology that represents the overlap between internalizing and externalizing psychopathology (Kotov et al. 2017; see Fig. 1). The general factor of psychopathology is hypothesized to account for the effects of non-specific causal factors that increase risk for all symptom domains of psychopathology (Lahey et al. 2017).

An example of the paths compared in the latent variable indirect effects modeling. Paths A, B, and C each represent total effects for a specific type of victimization with a specific symptom domain of psychopathology. Path A’ represents a direct effect, after controlling for higher-order factors (i.e., the association unique to depressive symptoms, specifically)
To date, several studies have examined childhood adversity in this kind of framework—comparing transdiagnostic versus diagnosis-specific pathways—finding that broad transdiagnostic factors such as internalizing, externalizing, and general psychopathology either largely or fully account for the relationships between childhood adversity and psychopathology (e.g., Conway et al. 2018; Keyes et al. 2012; Meyers et al. 2015; Vachon et al. 2015). Schaefer et al. (2018) recently examined the effect of adolescent poly-victimization (i.e., the number of types of severe victimization experiences spanning maltreatment, neglect, sexual victimization, family violence, peer/sibling victimization, internet/mobile phone victimization, and crime victimization), finding transdiagnostic and likely causal associations with general psychopathology in early adulthood. Other studies have found similar results for the associations between psychopathology and racial discrimination (Rodriguez-Seijas et al. 2015), traumatic experiences (Meyers et al. 2015; Sunderland et al. 2016), minority stress (Eaton 2014), and marital distress in adulthood (South et al. 2011). That is, these environmental stressors have non-specific associations with psychopathology, apparently increasing risk for symptoms of various mental disorders via their association with broad transdiagnostic factors, but do not appear to have specific or unique relationships with particular symptom domains (Conway et al. 2019, 2018).
The extant literature on peer victimization and psychopathology mirrors the early findings in the childhood adversity literature, in that peer victimization experiences have apparent causal associations with concurrent symptoms of depression, anxiety, hyperactivity and inattention, and conduct problems (Schoeler et al. 2018; Singham et al. 2017). However, it has not been tested to date whether these systematic associations can be parsimoniously accounted for by transdiagnostic factors, as has been found for other environmental stressors. Taking a hierarchical approach to understand these associations in other literatures has accelerated research on the etiology of psychopathology, and is ideal for examining the specificity of the associations between peer victimization and specific psychopathology symptom domains as well as broader relationships with higher-order transdiagnostic factors. It also allows us to compare the strength of these relationships to test for non-equivalence of harm, and to test whether the strengths of these relationships vary as a function of gender.
Current Study
The extant literature suggests that peer victimization experiences are associated with a wide variety of psychopathology, but silos in the literature have prevented integration and synthesis of these findings, leaving three key questions: First, are some types of peer victimization experiences more strongly related to psychopathology than others (Question 1; (non-)equivalence of harm)? Second, do particular types of peer victimization have associations with specific disorders, or do they represent broadband risks for psychopathology in general (Question 2; outcome specificity)? Finally, does gender moderate the strength of the associations between peer victimization experiences and psychopathology (Question 3; gender invariance)? Thus, the primary objective of the present study was to clarify these gaps in the literature in a hierarchical and transdiagnostic framework in a nationally representative sample of mid-adolescents aged 14–15. To the authors’ knowledge, this is the first study to examine all domains of common psychopathology in adolescence and their relationships with physical, verbal, and relational peer victimization experiences.
Hypotheses were not documented a priori, but based on preliminary evidence in the extant literature reviewed above, it was expected that experiences of relational victimization would be more psychologically harmful than physical and verbal victimization. It was also expected that experiences of peer victimization would have broadband associations with general psychopathology—and only small or non-significant unique associations with specific domains of psychopathology—in line with studies that have integrated similar literatures based on other types of environmental stressors. Finally, gender invariance was expected, in line with evidence that gender does not tend to moderate the strength of the relationships between peer victimization and psychopathology.
Methods
Sample and Procedure
Participants were part of the Longitudinal Study of Australian Children (LSAC) led by the Australian Institute of Family Studies (see Soloff et al. 2005 for a detailed description of the methods). Briefly, LSAC is a longitudinal study of development drawn from a nationally representative sample based on stratified two-cluster sampling—first selecting postcodes from across all Australian states and territories, then selecting children from the Medicare database from within those postcodes.
The present study is based on data collected in 2015 in the older cohort of LSAC participants (born between March 1999 and February 2000) when they were aged 14–15, and includes all participants with self-report victimization data available at that time (n= 3335; 94% of the full cohort at ages 14–15, 67% of the original full cohort from ages 4–5). Detailed information on response rates and sample characteristics at each wave are available in Australian Institute of Family Studies (2016). The included sample was compared to participants who dropped out before this wave and/or with missing self-report victimization data at age 14–15 (n= 1648). These groups did not differ in terms of sex (χ2(1) = 0, p = 0.986, φ = 0), but had statistically significant differences associated with small effect sizes for other demographic variables, including being less likely to report English to be the main language spoken at home (χ2(1) = 60.69, p < 0.0001, φ = 0.11), having lower mean indexes of relative socio-economic advantage and disadvantage (t(3369.74) = 4.584, p < 0.0001, Cohen’s d = 0.14), and being younger (t(3135.19) = 1.999, p = 0.046, Cohen’s d = 0.05).
Bias in the present study due to attrition was reduced by applying survey weights in all analyses (Norton and Monahan 2016). These weights were initially calculated for each participant at Wave 1 based on the inverse probability of selecting the child, adjusted to align with population benchmarks for demographic variables drawn from the Australian Bureau of Statistics Estimated Resident Population and the Census. The Wave 1 weights were then adjusted for differential sample attrition over time, using Wave 1 characteristics to predict response propensity in the current wave. Applying these weights thus maximizes demographic representativeness of the population of Australian adolescents aged 14–15. Full information maximum likelihood was used to account for the remaining missingness (0–2.3% of cases) on psychopathology variables.
Participants included in the present study had a mean (standard deviation) age of 14.4 (0.49) years, 49.1% (n = 1638) were female, 90.1% (n = 3005) reported English to be the main language spoken at home, and 42.7% (n = 1424) came from the lower 50% of socio-economic conditions in Australia. All participants provided informed consent, and the questionnaires were completed in participants’ homes. The study was approved by the Ethics Committee at the Australian Institute of Family Studies. The present study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Measures
LSAC collects a broad variety of measures related to development throughout childhood and adolescence. Descriptive statistics for the variables included in the present study are shown in Table 1, and the measurement and calculation of these variables are described below.
Type of peer victimization
Participants were asked about the frequency of their experiences of physical victimization (i.e., “kids hit or kicked me”; “kids grabbed or shoved me”), verbal victimization (i.e., “kids said mean things or called me names”; “kids threatened to hurt me”), and relational victimization (i.e., “kids tried to keep others from being my friend”; “kids did not let me join in”)—excluding interactions with family members—in the past month, rated not at all (0), once or twice (1), about once a week (2) or several times a week (3). There was not sufficient endorsement of each frequency category to run the analyses in an ordinal regression framework, so in line with the literature emphasizing repeated harm as central to the definition of bullying (e.g., Olweus 1999; Smith et al. 2002), face validity was emphasized in operationalizing experiences of peer victimization as present (1) or absent (0) based on individuals reporting one or more of the victimization experiences in each domain with a frequency of “about once a week” or more. For example, an individual was classified as having experienced verbal victimization if kids had said mean things or called them names or threatened to hurt them at least once a week in the past month. Given the aim of the brief assessment was to capture breadth of content, the pairs of items measuring each type of victimization did not have substantial overlap, and correspondingly did not have high internal consistency (α = 0.75, α = 0.41, and α = 0.51 for physical, verbal, and relational victimization, respectively). To determine whether the focus here on repeated peer victimization missed important information in the relationship between less frequent experiences of victimization and psychopathology, sensitivity analyses are also reported for Questions 1 and 2 based on reports of any peer victimization experiences for each domain in the past month (see Table S1 for detailed results).
Psychopathology symptom domains
Psychiatric and behavioral symptoms were assessed across the five core domains of child and adolescent psychopathology that are developmentally coherent into adulthood (see Forbes et al. 2015; Krueger et al. 1998; Lahey et al. 2004).
Depressive symptoms
Depressive symptoms were assessed using the Short Mood and Feelings Questionnaire (Angold et al. 1995), which includes 13 items (e.g., “I felt miserable or unhappy”) assessed over the past two weeks rated not true (0), sometimes (1), or true (2).
Anxiety
Symptoms of anxiety were assessed based on eight items derived from the Spence Children’s Anxiety Scale short form (Spence, 1998; i.e., “I worry about things”; “I feel afraid”; “I feel afraid I will make a fool of myself in front of other people”; “I worry that bad things will happen to me”; “I feel nervous”; “I wake up feeling scared”; “I worry what other people think of me”; “All of a sudden I feel really scared for no reason at all”) rated from never (1) to always (4).
Conduct problems
Conduct problems were assessed using the conduct problems scale of the Strengths and Difficulties Questionnaire (SDQ; Goodman 1997), which has five items (e.g., “I am often accused of lying or cheating”) rated not true (0), somewhat true (1) or certainly true (2) over the past six months.
Hyperactivity/Inattention
Hyperactivity and inattention symptoms were also assessed using the SDQ inattention-hyperactivity scale, which has five items (e.g., “I am easily distracted”) assessed in the same format as the conduct problems scale described above.
Substance use
Finally, substance use was assessed based on the number of substances used in the past 12 months, including alcohol, cigarettes, marijuana, inhalants, and other drugs of abuse—each rated as yes (1) or no (0).
Each psychopathology domain was represented as a summed total score and standardized on the full sample for analysis, given the varying ranges of each measure. Cronbach’s alpha was lower for the five-item conduct problems, inattention-hyperactivity, and substance use scales (α = 0.60, α = 0.77 and α = 0.62, respectively), and higher for the longer anxiety and depressive symptom measures (α = 0.89 and α = 0.94, respectively).
Data Analyses
All analyses were conducted in MPlus version 7.4 using sample weights in the recently developed latent variable indirect effects modeling framework (Muthén and Muthén 1998–2018). While the effect sizes are the focus of the analyses, an uncorrected alpha level of 0.01 was used for significance testing to err on the side of sensitivity to detecting evidence against the null hypotheses regarding lack of outcome specificity in these relationships.
The hierarchical structure of psychopathology was parameterized in a second-order latent variable model based on the empirical structure of common mental disorders (Kotov et al. 2017; see Fig. 1): An internalizing factor represented the overlap between depressive symptoms and anxiety; externalizing represented the overlap between conduct problems, hyperactivity/inattention, and substance use. General psychopathology represented the overlap between internalizing and externalizing. All loadings were estimated freely, and the latent variables were standardized to have means of zero and variances of 1 to identify the model. A maximum likelihood estimator with robust standard errors was used in all analyses to account for non-normality in the observed variables. Standardized loadings and coefficients are reported in the STDY metric to represent the predicted change (in standard deviation units) in each domain of psychopathology for the presence of each type of victimization. After ascertaining adequate fit and gender invariance of the latent variable model of psychopathology in a multi-group framework, the primary analyses were then conducted by examining the total, indirect, and direct effects separately for each type of victimization with each domain of psychopathology, as described below.
Analyses for (non-)equivalence of harm (Question 1) were based on testing for differences in the strength of the associations for each type of victimization with each domain of psychopathology. Specifically, the 99% confidence intervals of the total effects were compared—both in models with the three types of peer victimization entered separately, and simultaneously—to determine whether specific types of victimization had stronger relationships with psychopathology. For example, paths A, B, and C in Fig. 1 represent the total effects for the associations between experiences of physical, relational and verbal victimization with depressive symptoms. These total effects are akin to linear regression coefficients and do not account for the shared variance among the psychopathology variables.
Analyses for outcome specificity (Question 2) were based on examining whether these victimization—psychopathology associations were unique to specific symptom domains of psychopathology (i.e., to depressive symptoms, anxiety, conduct problems, hyperactivity/inattention, or substance use specifically), to the overlap among these symptom domains (i.e., in the broader common factors of internalizing or externalizing), or to general psychopathology. Specifically, each total effect was compared with its corresponding direct effect. Direct effects represent the unique association between each type of victimization and each domain of psychopathology after controlling for the shared variance captured in higher-order factors in the model, and are akin to a multivariate regression coefficients. For example, path A’ in Fig. 1 represents a direct effect—the proportion of the total effect between physical victimization and depressive symptoms that is unique to depressive symptoms specifically. By contrast, the difference between paths A and A’ is the indirect effect—the proportion of the total effect that is accounted for by internalizing and general psychopathology (i.e., not unique to depressive symptoms).
Finally, the gender invariance of each model was tested (Question 3). Specifically, Satorra–Bentler chi-squared difference testing (Satorra and Bentler 2010) and a critical value of 0.01 change in the comparative fit index (CFI; Cheung and Rensvold 2002) were used to compare models that allowed parameters to vary by gender and models that constrained parameters to equality by gender.
Results
Structural Model of Psychopathology
The hierarchical structural model of psychopathology depicted in Fig. 1 provided a good fit to the data, and met criteria for configural, metric, and scalar invariance by gender (Muthén and Muthén 1998–2018; see Table 2). Subsequent analyses were run holding scalar invariance.
(Non-)Equivalence of Harm
All victimization experiences had moderate to strong positive and significant total effects with all symptom domains of psychopathology (from b = 0.45 to b = 1.09, ps < 0.01; see Table 3). The strength of these associations did not appear to vary as a function of type of victimization. Specifically, the 99% confidence intervals overlapped for all types of victimization experiences for each domain of psychopathology symptoms in the models with each type of peer victimization entered separately (see Fig. 2), and with all three entered simultaneously to account for the correlations among them (see Fig. S1). Further, sensitivity analyses examining the association of any (versus repeated) peer victimization in each domain showed very similar results, albeit with weaker total effects (from b = 0.42 to b = 0.80, ps < 0.01; Table S1), indicating that infrequent victimization experiences had weaker associations with psychopathology.

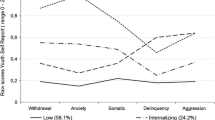
Standardized total effects and 99% confidence intervals for each type of victimization experience with each domain of psychopathology constrained to equality for male participants (flat marker) and female participants (circular marker). The effect sizes represent the estimated difference in each domain of psychopathology (in standard deviation units) associated with the experience of each type of victimization (e.g., paths A, B, and C in Fig. 1)
Outcome Specificity
Outcome specificity was tested by examining the extent to which each total effect in Fig. 2 was specific to each symptom domain (see Table 3). A large proportion (73–100%) of each total effect size was consistently accounted for by the higher-order factors. All direct effects—representing the proportion of the total effect unique to each symptom domain—were small and non-significant (bs < 0.26, ps > 0.01). In the sensitivity analyses, similar proportions of the total effects were accounted for by any peer victimization experience in each domain (73–100%; all bs < |0.22|), although there were small but statistically significant direct effects with anxiety and depressive symptoms (Table S1). However, nearly all of these direct effects were smaller in both absolute and proportional effect size. The one exception was for verbal victimization, which had a stronger and proportionately larger positive direct effect associated with anxiety (b = 0.18, p = 0.002; 23% of the total effect). This may suggest that a lower severity (frequency) level of verbal peer victimization is associated with anxiety symptoms specifically, compared to other domains of psychopathology.
Moving up to the next level of the hierarchy, the total effects for each type of victimization with internalizing and externalizing psychopathology were again strong and significant (from b= 0.93 to b= 1.59, ps < 0.01), but 72–100% of each association was accounted for by general psychopathology such that all direct effects were substantially smaller and non-significant (bs < 0.36, ps > 0.01). The same pattern was also evident in the sensitivity analyses, but with weaker effects (total effects from b = 0.77 to b = 1.22, ps < 0.01; direct effects b < 0.21, ps > 0.01; 83–100% accounted for by general psychopathology; Table S1).
Taken together, these results indicate that the associations between peer victimization and psychopathology are not unique to specific symptom domains, but rather broadband associations with all symptom domains captured by an association with general psychopathology (see Fig. 3 for a visual summary of the parameters presented in Table 3). In line with this, the general psychopathology factor had strong and significant associations with all types of victimization (from b= 1.26 to b = 1.56, ps < 0.01; and from b = 0.95 to b = 1.23, ps < 0.01 in the sensitivity analyses).

Visual summary of the total versus direct effects (parameters specified in Table 3) for each type of victimization experience with each domain of psychopathology. The regression line weights (between the victimization and psychopathology variables) are proportional to the strength of the standardized effects shown in Table 2, averaged for male and female participants. Solid lines represent significant effects, and dashed lines denote non-significant effects at p < 0.01. Note that the direct effect for general psychopathology is equal to the total effect, as there are no higher-order variables controlled for in this association.
Gender Invariance
Gender was examined as a moderator in all analyses using a multi-group framework and comparing models with regression paths constrained and unconstrained by gender. All models were invariant by gender, including all ΔCFI < 0.01 and all Satorra–Bentler chi-squared difference test ps > 0.05.
Discussion
Experiences of peer victimization are common in adolescence and have been associated with a broad variety of psychopathology in adolescence. However, silos in the literature have prevented integration and synthesis of the findings of studies spanning multiple types of peer victimization and domains of psychopathology. The present study examined (1) whether some types of peer victimization experiences were more strongly related to psychopathology than others ((non-)equivalence of harm); (2) whether particular types of victimization have unique associations with specific symptom domains (outcome specificity); and (3) whether the strength of these associations varied by gender (gender invariance). Specifically, a hierarchical and transdiagnostic framework was used to examine the relationships among adolescent experiences of relational, verbal, and physical peer victimization and manifest symptoms of depression, anxiety, conduct problems, hyperactivity and inattention, and substance use. The results indicated that physical, verbal, and relational victimization had similar and broadband associations across all common domains of psychopathology, including all levels of a hierarchical model of psychopathology, and that these associations were invariant by gender. The implications of these findings are discussed in the context of the literature below.
Implications
Equivalence of harm was indicated by the finding that repeated experiences of physical, verbal, and relational victimization had similar, moderate to strong relationships with all symptom domains of psychopathology examined. The associations with substance use tended to be weaker than for other symptom domains, but these differences did not reach significance, suggesting broad equivalence between types of peer victimization and domains of psychopathology. This finding is in contrast to previous studies finding that relational victimization experiences are more psychologically harmful than verbal or physical victimization (e.g., Siegel et al. 2009; Storch et al. 2005), and has potential implications for policy. For example, legislation and school-level policies often disproportionately penalize physical victimization, which is directly observable and thus more easily detected. This may be in part due to a concern about the potential for physical harm. The sensitivity analyses indicated that less frequent victimization experiences had weaker associations with psychopathology (cf. van der Ploeg et al. 2015). However, the finding that experiences of all forms of victimization were associated adverse psychological outcomes highlights the need to raise awareness of the broader potential harms of these experiences, and to develop interventions for detecting and minimizing less noticeable forms of peer victimization.
All levels of the hierarchical model of psychopathology were also robustly associated with experiences of peer victimization, with the strongest relationships at the level of the transdiagnostic internalizing, externalizing, and general psychopathology factors. However, there was no evidence of outcome specificity associated with repeated peer victimization experiences, as most of the domain-specific relationships were accounted for by the association between peer victimization and general psychopathology. In the sensitivity analyses examining any experiences of peer victimization in each domain, there was a unique association between verbal victimization and anxiety that may indicate a lower severity threshold for this relationship specifically, although this finding requires replication.
Overall, of the total association between each symptom domain and each victimization experience, an average of only 9% of the relationship was unique to the symptom domain level after controlling for the higher-order factors (8% in the sensitivity analyses). This suggests that the associations between peer victimization experiences and psychopathology were largely attributable to the shared transdiagnostic factors that capture the overlap among the symptom domains, in line with other literatures that have found transdiagnostic factors to be the best predictors of important risks and outcomes (e.g., Eaton 2014; Keyes et al. 2012; Meyers et al. 2015; Rodriguez-Seijas et al. 2015). The finding of an association at the level of the general psychopathology factor is also consistent with Singham et al.’s (2017) recent research using a twin differences design that found evidence for a causal relationship between exposure to peer victimization and varied manifestations of psychopathology that included indicators of the thought disorder spectrum (e.g., paranoid thoughts and cognitive distortions; Kotov et al. 2017)—extending the potential implications of this research to a broadband risk for lower prevalence psychopathology as well.
Interestingly, these results are largely in contrast to evidence for outcome specificity—including from a previous study we conducted using LSAC data that consistently found depressive symptoms and anxiety to have unique relationships with peer victimization experiences (Forbes et al. 2019). This is potentially in part because the unique relationships examined in the current study controlled not only for the overlap between depressive symptoms and anxiety (i.e., in the internalizing factor), but also for the overlap between internalizing and externalizing psychopathology (i.e., in the general psychopathology factor, which is a strong indicator of psychopathology severity; Lahey et al. 2017). Regardless, the results of the present study suggest that the few examples of significant unique relationships documented in the literature (e.g., Forbes et al. 2019; Stapinski et al. 2015) may only represent a small proportion of the full direct effects, which are largely captured in the overlap between disorders.
Peer victimization has recently been hypothesized to effect change in emotion processing, executive function, brain-based responses to stress, and epigenetic mechanisms (McLaughlin 2016; Singham et al. 2017). These transdiagnostic processes could represent candidate mechanisms that account for associations between experiences of peer victimization and general psychopathology. However, the mechanisms of action linking victimization experiences with individuals’ manifest symptoms are almost certainly multifactorial and likely to differ across symptom domains, reflecting individual differences in pre-existing vulnerabilities, traits and responses to stress (see Forbes et al. 2015 for a discussion). For example, adolescents high in externalizing may be more likely to experience peer victimization because of their own bullying behaviors (Reijntjes et al. 2011), whereas those high in internalizing may be more likely to be targeted because of perceived vulnerability (Reijntjes et al. 2010; Schacter and Juvonen 2017). Similarly, developing hostile social-cognitive biases in response to peer victimization experiences is more likely to result in aggressive externalizing behaviors (Reijntjes et al. 2011), whereas experiencing fear and helplessness is more likely to manifest as symptoms of internalizing psychopathology (Reijntjes et al. 2010). The finding of gender invariance is noteworthy in this context, as the gender-related biases towards internalizing versus externalizing behaviors were not manifest in differential relationships here. Overall, these results are in line with the findings of studies that have examined other environmental stressors in a transdiagnostic framework, and suggest that peer victimization may act as a broadband stressor—generating general distress that manifests in a variety of ways, based on individual differences (i.e., multifinality). Here, as for other environmental stressors (e.g., Schaefer et al. 2018), these relationships could be captured parsimoniously by a general psychopathology factor.
Limitations and Future Directions
These results should be considered in light of the study limitations. The primary limitations were regarding measurement. First, the reliance on self-reported experiences of peer victimization means that social desirability and demand characteristics may have led to an underestimation of the prevalence of victimization and correspondingly weaker relationships with psychopathology. The relatively low prevalence of reported peer victimization meant it was not possible to comprehensively examine the role of the severity or frequency of the victimization experiences, which would be an interesting avenue for future research. The use of a single informant—compared to multiple informants—has also been associated with stronger relationships between reports of peer victimization and psychopathology. Meta-analytic evidence suggests this is likely due in part to increased shared measurement variance between the domains (Reijntjes et al. 2010) and perhaps some individuals’ underlying tendency to report negative feelings and experiences (Schoeler et al. 2018). The shared measurement variance related to the reliance on self-report will also have inflated the amount of variance captured in the general psychopathology factor. While the LSAC study includes parents, caregivers, and teachers as informants, multi-informant reports were not collected on the different types of peer victimization and most of the psychopathology symptom domains. It would be ideal if future research could extend and replicate these findings to examine generalizability in a multi-informant framework, as reliance on self-report is a limitation of much of the extant research in this field (Hawker and Boulton 2000; Moore et al. 2017).
Measurement error is also important to consider for the psychopathology variables, as the externalizing variables in particular had lower internal consistency that may have weakened the estimated relationships with peer victimization as well as decreasing the likelihood of finding statistically significant associations. By contrast, the use of structural equation modeling in this field has been found to lead to more precise effects by reducing error in effect sizes (Reijntjes et al. 2010). Together with the use of an uncorrected alpha level of 0.01 for significance testing and the multiple comparisons in a large sample, this meant that these analyses were sensitive to evidence for non-equivalence of harm and specificity of outcomes for the internalizing and externalizing variables in particular, so the failure to reject the corresponding null hypotheses is noteworthy. Another limitation related to the measurement of psychopathology here is that the skewness of the substance use and male depressive symptom variables will likely have resulted in lost information due to floor effects. Overall, more comprehensive and sensitive measurement of all of the constructs of interest should be a priority for future research on this topic.
The use of cross-sectional data also meant that the direction of the relationships examined here could not be determined. Psychopathology was referred to as the “outcome” in interpreting these results, in line with the growing body of research that has found peer victimization to have likely causal relationships with psychopathology symptoms, even after accounting for their shared genetic factors (e.g., Schaefer et al. 2018; Schoeler et al. 2018; Singham et al. 2017). Notably, the causal effects dissipate over time, and evidence to date suggests that causal relationships between peer victimization and psychopathology operate in short-term time frames of generally less than one year (Schoeler et al. 2018; Singham et al. 2017). The waves of the LSAC study are measured two years apart, so may not be able to capture these causal relationships. However, while examination of these transdiagnostic relationships in cross-sectional data is an important first step, extending these findings in longitudinal (ideally, quasi-experimental) data with varying time lags will provide opportunities to test the generalizability and robustness of these findings and to account for the potential confound of recent victimization exposure affecting current functioning or recall bias.
Future research should also include analyses of cybervictimization, which was not examined here. Extant research indicates that cybervictimization is associated with internalizing and externalizing problems (Fisher et al. 2016), including depression (Hamm et al. 2015), anxiety (Juvonen and Gross 2008), aggression (Ybarra et al. 2007), and substance use (Suzuki et al. 2012). Taken together, this pattern of relationships would be consistent with the current transdiagnostic findings, but the equivalence, specificity, and gender invariance of these relationships should be explicitly tested.
Finally, there was no distinction made between “victims” versus “bully-victims” (i.e., individuals who also perpetrate peer victimization), which is often done in the bullying literature (e.g., Haynie et al. 2001), so qualitative differences between these groups may have been missed (e.g., Kaltiala-Heino et al. 2000). However, the inclusion of conduct problems in these analyses meant that continuous individual differences in aggression were accounted for in the model, and there was no evidence for differential relationships between repeated experiences of peer victimization and conduct problems, or for other symptom domains after controlling for individual differences in levels of externalizing psychopathology.
Conclusion
This study examined the relationships between experiences of peer victimization and psychopathology during the key developmental period of adolescence. Using a transdiagnostic and hierarchical model of psychopathology, this study focused on whether some types of victimization are more harmful than others; whether the harms associated with different types of peer victimization are specific to particular domains of psychopathology; and whether these relationships vary by gender. Taken together, the results suggested that experiences of peer victimization, regardless of type, may pose a broadband risk for general psychopathology. This research extends the literature on the utility of broad transdiagnostic factors to account for the important and prevalent problem of adolescent peer victimization. The findings of equivalence, non-specificity, and invariance by gender suggest it may be less useful to take a siloed victimization-specific, disorder-level, or gender-specific approach to research. Similarly, treatments may be most effective when targeted at the broadband level, rather than tailored to specific types of victimization or symptom domains. Importantly, these results reinforce the emphasis of schools on targeting peer victimization, and highlight the importance of further targeting less noticeable (non-physical) forms of victimization. Adolescence is a vulnerable period for developing psychopathology, so these findings indicate particular need for effective early interventions.
References
Achenbach, T. M., & Edelbrock, C. S. (1978). The classification of child psychopathology: a review and analysis of empirical efforts. Psychological Bulletin, 85(6), 1275–1301.
Angold, A., Costello, E. J., Messer, S. C., & Pickles, A. (1995). Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research, 5(4), 237–249.
Arseneault, L. (2017). The long-term impact of bullying victimization on mental health. World Psychiatry, 16(1), 27–28.
Australian Institute of Family Studies. (2016). The longitudinal study of Australian Children Annual statistical report 2015. Melbourne: AIFS.
Bauman, S., & Del Rio, A. (2006). Preservice teachers’ responses to bullying scenarios: comparing physical, verbal, and relational bullying. Journal of Educational Psychology, 98(1), 219.
Bogart, L. M., Elliott, M. N., Klein, D. J., Tortolero, S. R., Mrug, S., Peskin, M. F., Schuster, M. A. (2014). Peer Victimization in fifth grade and health in tenth grade. Pediatrics. https://doi.org/10.1542/peds.2013-3510.
Boyd, A., Van de Velde, S., Vilagut, G., De Graaf, R., Florescu, S., & Alonso, J., Investigators, E.-W. (2015). Gender differences in mental disorders and suicidality in Europe: results from a large cross-sectional population-based study. Journal of Affective Disorders, 173, 245–254.
Byers, D. L., Caltabiano, N. J., & Caltabiano, M. L. (2011). Teachers’ attitudes towards overt and covert bullying, and perceived efficacy to intervene. Australian Journal of Teacher Education, 36(11), 105.
Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255.
Connolly, E. J., & Beaver, K. M. (2016). Considering the genetic and environmental overlap between bullying victimization, delinquency, and symptoms of depression/anxiety. Journal of Interpersonal Violence, 31, 1230–1256.
Conway, C. C., Forbes, M. K., Forbush, K. T., Fried, E. I., Hallquist, M. N., Kotov, R., ... & Eaton, N. R. (2019). A hierarchical taxonomy of psychopathology can transform mental health research. Perspectives on Psychological Science, 14(3), 419–436.
Conway, C. C., Raposa, E. B., Hammen, C., & Brennan, P. A. (2018). Transdiagnostic pathways from early social stress to psychopathology: a 20-year prospective study. Journal of Child Psychology and Psychiatry, 59(8), 855–862.
Eaton, N. R. (2014). Transdiagnostic psychopathology factors and sexual minority mental health: evidence of disparities and associations with minority stressors. Psychology of sexual orientation and gender diversity, 1(3), 244–254.
Fisher, B. W., Gardella, J. H., & Teurbe-Tolon, A. R. (2016). Peer cybervictimization among adolescents and the associated internalizing and externalizing problems: a meta-analysis. Journal of Youth and Adolescence, 45, 1727–1743.
Forbes, M. K., Fitzpatrick, S., Magson, N. R., & Rapee, R. M. (2019). Depression, anxiety, and peer victimization: bidirectional relationships and associated outcomes transitioning from childhood to adolescence. Journal of Youth and Adolescence, 48(4), 692–702.
Forbes, M. K., Tackett, J. L., Markon, K. E., & Krueger, R. F. (2015). Beyond comorbidity: toward a dimensional and hierarchical approach to understanding psychopathology across the life span. Development and Psychopathology, 28, 971–986. https://doi.org/10.1017/s0954579416000651.
Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein, D., Vaituzis, A. C., & Toga, A. W. (2004). Dynamic mapping of human cortical development during childhood through early adulthood. Proceedings of the National Academy of Sciences, 101(21), 8174–8179.
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Hamm, M. P., Newton, A. S., Chisholm, A., Shulhan, J., Milne, A., Sundar, P., & Hartling, L. (2015). Prevalence and effect of cyberbullying on children and young people: a scoping review of social media studies. JAMA Pediatrics, 169, 770–777.
Hawker, D. S., & Boulton, M. J. (2000). Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry, 41(4), 441–455.
Haynie, D. L., Nansel, T., Eitel, P., Crump, A. D., Saylor, K., Yu, K., & Simons-Morton, B. (2001). Bullies, victims, and bully/victims: distinct groups of at-risk youth. The Journal of Early Adolescence, 21(1), 29–49. https://doi.org/10.1177/0272431601021001002.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal, 6(1), 1–55.
Hymel, S., & Swearer, S. M. (2015). Four decades of research on school bullying: an introduction. American Psychologist, 70(4), 293.
Juvonen, J., & Gross, E. F. (2008). Extending the school grounds?—Bullying experiences in cyberspace. Journal of School health, 78, 496–505.
Juvonen, J., Wang, Y., & Espinoza, G. (2011). Bullying experiences and compromised academic performance across middle school grades. The Journal of Early Adolescence, 31(1), 152–173. https://doi.org/10.1177/0272431610379415.
Kaltiala-Heino, R., RimpelÄ, M., Rantanen, P., & RimpelÄ, A. (2000). Bullying at school—an indicator of adolescents at risk for mental disorders. Journal of Adolescence, 23(6), 661–674. https://doi.org/10.1006/jado.2000.0351.
Kendrick, K., Jutengren, G., & Stattin, H. (2012). The protective role of supportive friends against bullying perpetration and victimization. Journal of Adolescence, 35(4), 1069–1080.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602.
Keyes, K. M., Eaton, N. R., Krueger, R. F., McLaughlin, K. A., Wall, M. M., Grant, B. F., & Hasin, D. S. (2012). Childhood maltreatment and the structure of common psychiatric disorders. The British Journal of Psychiatry, 200(2), 107–115.
Kokkinos, C. M., & Kipritsi, E. (2012). The relationship between bullying, victimization, trait emotional intelligence, self-efficacy and empathy among preadolescents. Social Psychology of Education, 15(1), 41–58. https://doi.org/10.1007/s11218-011-9168-9.
Kotov, R., Krueger, R. F., Watson, D., Achenbach, T. M., Althoff, R. R., Bagby, R. M., & Zimmerman, M. (2017). The hierarchical taxonomy of psychopathology (HiTOP): a dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 126(4), 454–477.
Krueger, R. F., Caspi, A., Moffitt, T. E., & Silva, P. A. (1998). The structure and stability of common mental disorders (DSM-III-R): a longitudinal-epidemiological study. Journal of abnormal psychology, 107(2), 216–227.
Lahey, B. B., Applegate, B., Waldman, I. D., Loft, J. D., Hankin, B. L., & Rick, J. (2004). The structure of child and adolescent. Psychopathology: Generating New Hypotheses, 113(3), 358–385.
Lahey, B. B., Krueger, R. F., Rathouz, P. J., Waldman, I. D., & Zald, D. H. (2017). A hierarchical causal taxonomy of psychopathology across the life span. Psychological bulletin, 143(2), 142–186.
Lösel, F., & Bender, D. (2011). Emotional and antisocial outcomes of bullying and victimization at school: a follow-up from childhood to adolescence. Journal of Aggression, Conflict and Peace Research, 3(2), 89–96.
Martel, M. M. (2013). Sexual selection and sex differences in the prevalence of childhood externalizing and adolescent internalizing disorders. Psychological Bulletin, 139(6), 1221–1259.
Martin, K. M., & Huebner, E. S. (2007). Peer victimization and prosocial experiences and emotional well‐being of middle school students. Psychology in the Schools, 44(2), 199–208. https://doi.org/10.1002/pits.20216.
McLaughlin, K. A. (2016). Future directions in childhood adversity and youth psychopathology. Journal of Clinical Child & Adolescent Psychology, 45(3), 361–382. https://doi.org/10.1080/15374416.2015.1110823.
Meyers, J. L., Lowe, S. R., Eaton, N. R., Krueger, R., Grant, B. F., & Hasin, D. (2015). Childhood maltreatment, 9/11 exposure, and latent dimensions of psychopathology: A test of stress sensitization. Journal of psychiatric research, 68, 337–345.
Moore, S. E., Norman, R. E., Suetani, S., Thomas, H. J., Sly, P. D., & Scott, J. G. (2017). Consequences of bullying victimization in childhood and adolescence: a systematic review and meta-analysis. World Journal of Psychiatry, 7(1), 60.
Muthén, L. K., & Muthén, B. O. (1998–2018). Mplus user’s guide. 8th ed. Los Angeles, CA: Muthén & Muthén.
Nanni, V., Uher, R., & Danese, A. (2012). Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: a meta-analysis. American Journal of Psychiatry, 169(2), 141–151.
Norton, A. & Monahan, K. (2016). The longitudinal study of Australian children: LSAC technical paper no. 15: Wave 6 weighting and non-response. Canberra, ACT: Australian Bureau of Statistics.
Olweus, D. (1999). Sweden. In P. K. Smith, Y. Morita, J. Junger-Tas, D. Olweus, R. Catalano & P. Slee (Eds) The nature of school bullying: a cross-national perspective (pp. 7–27). New York, NY: Routledge.
Ranta, K., Kaltiala-Heino, R., Pelkonen, M., & Marttunen, M. (2009). Associations between peer victimization, self-reported depression and social phobia among adolescents: the role of comorbidity. Journal of Adolescence, 32(1), 77–93.
Reijntjes, A., Kamphuis, J. H., Prinzie, P., Boelen, P. A., van der Schoot, M., & Telch, M. J. (2011). Prospective linkages between peer victimization and externalizing problems in children: a meta‐analysis. Aggressive Behavior, 37(3), 215–222. https://doi.org/10.1002/ab.20374.
Reijntjes, A., Kamphuis, J. H., Prinzie, P., & Telch, M. J. (2010). Peer victimization and internalizing problems in children: a meta-analysis of longitudinal studies. Child Abuse & Neglect, 34(4), 244–252.
Rodriguez-Seijas, C., Stohl, M., Hasin, D. S., & Eaton, N. R. (2015). Transdiagnostic factors and mediation of the relationship between perceived racial discrimination and mental disorders. JAMA psychiatry, 72(7), 706–713.
Salle, T. L., George, H. P., McCoach, D. B., Polk, T., & Evanovich, L. L. (2018). An examination of school climate, victimization, and mental health problems among middle school students self-identifying with emotional and behavioral disorders. Behavioral Disorders, 43(3), 383–392. https://doi.org/10.1177/0198742918768045.
Satorra, A., & Bentler, P. M. (2010). Ensuring positiveness of the scaled difference chi-square test statistic. Psychometrika, 75(2), 243–248.
Schacter, H. L., & Juvonen, J. (2017). Depressive symptoms, friend distress, and self-blame: risk factors for adolescent peer victimization. Journal of Applied Developmental Psychology, 51, 35–43.
Schaefer, J. D., Moffitt, T. E., Arseneault, L., Danese, A., Fisher, H. L., Houts, R., ... & Caspi, A. (2018). Adolescent victimization and early-adult psychopathology: approaching causal inference using a longitudinal twin study to rule out noncausal explanations. Clinical Psychological Science, 6(3), 352–371.
Schoeler, T., Duncan, L., Cecil, C. M., Ploubidis, G. B., & Pingault, J.-B. (2018). Quasi-experimental evidence on short- and long-term consequences of bullying victimization: a meta-analysis. Psychological Bulletin, 144(12), 1229–1246. https://doi.org/10.1037/bul1000171.
Sentse, M., Kretschmer, T., & Salmivalli, C. (2015). The longitudinal interplay between bullying, victimization, and social status: age‐related and gender differences. Social Development, 24(3), 659–677.
Sentse, M., Prinzie, P., & Salmivalli, C. (2017). Testing the direction of longitudinal paths between victimization, peer rejection, and different types of internalizing problems in adolescence. Journal of Abnormal Child Psychology, 45(5), 1013–1023. https://doi.org/10.1007/s10802-016-0216-y.
Siegel, R. S., La Greca, A. M., & Harrison, H. M. (2009). Peer victimization and social anxiety in adolescents: prospective and reciprocal relationships. Journal of Youth and Adolescence, 38(8), 1096–1109. https://doi.org/10.1007/s10964-009-9392-1.
Singham, T., Viding, E., Schoeler, T., Arseneault, L., Ronald, A., Cecil, C. M., ... Pingault, J. B. (2017). Concurrent and longitudinal contribution of exposure to bullying in childhood to mental health: the role of vulnerability and resilience. JAMA psychiatry, 74(11), 1112–1119.
Smith, P. K., Cowie, H., Olafsson, R. F., & Liefooghe, A. P. (2002). Definitions of bullying: a comparison of terms used, and age and gender differences, in a fourteen–country international comparison. Child Development, 73, 1119–1133. https://doi.org/10.1111/1467-8624.00461.
Snyder, J., Prichard, J., Schrepferman, L., Patrick, M. R., & Stoolmiller, M. (2004). Child impulsiveness—inattention, early peer experiences, and the development of early onset conduct problems. Journal of Abnormal Child Psychology, 32(6), 579–594.
Soloff, C., Lawrence, D., & Johnstone, R. (2005). Sample design. Melbourne: Australian Institute of Family Studies.
South, S. C., Krueger, R. F., & Iacono, W. G. (2011). Understanding general and specific connections between psychopathology and marital distress: a model based approach. Journal of abnormal psychology, 120(4), 935–947.
Spear, L. P. (2009). Heightened stress responsivity and emotional reactivity during pubertal maturation: implications for psychopathology. Development and Psychopathology, 21(1), 87–97.
Spence, S. H. (1998). A measure of anxiety symptoms among children. Behaviour research and therapy, 36(5), 545–566.
Stapinski, L. A., Araya, R., Heron, J., Montgomery, A. A., & Stallard, P. (2015). Peer victimization during adolescence: concurrent and prospective impact on symptoms of depression and anxiety. Anxiety, Stress, & Coping, 28(1), 105–120.
Storch, E. A., Masia‐Warner, C., Crisp, H., & Klein, R. G. (2005). Peer victimization and social anxiety in adolescence: a prospective study. Aggressive Behavior, 31(5), 437–452.
Sunderland, M., Carragher, N., Chapman, C., Mills, K., Teesson, M., Lockwood, E., … & Slade, T. (2016). The shared and specific relationships between exposure to potentially traumatic events and transdiagnostic dimensions of psychopathology. Journal of anxiety disorders, 38, 102–109.
Suzuki, K., Asaga, R., Sourander, A., Hoven, C. W., & Mandell, D. (2012). Cyberbullying and adolescent mental health. International Journal of Adolescent Mental Health, 24, 27–35. https://doi.org/10.1515/ijamh.2012.005.
Sweeting, H., Young, R., West, P., & Der, G. (2006). Peer victimization and depression in early–mid adolescence: a longitudinal study. British Journal of Educational Psychology, 76(3), 577–594.
Vachon, D. D., Krueger, R. F., Rogosch, F. A., & Cicchetti, D. (2015). Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry, 72(11), 1135–1142.
Vaillancourt, T., Trinh, V., McDougall, P., Duku, E., Cunningham, L., Cunningham, C., & Short, K. (2010). Optimizing population screening of bullying in school-aged children. Journal of School Violence, 9(3), 233–250.
van der Ploeg, R., Steglich, C., Salmivalli, C., & Veenstra, R. (2015). The intensity of victimization: associations with children’s psychosocial well-being and social standing in the classroom. PLoS ONE10(10), e0141490.
Ybarra, M. L., Diener-West, M., & Leaf, P. J. (2007). Examining the overlap in Internet harassment and school bullying: implications for school intervention. Journal of Adolescent Health, 41(6), S42–S50.
Acknowledgements
This article uses unit record data from Growing Up in Australia, the Longitudinal Study of Australian Children (LSAC). The study is conducted in partnership between the Department of Social Services (DSS), the Australian Institute of Family Studies (AIFS) and the Australian Bureau of Statistics (ABS). The findings and views reported in this paper are those of the authors and should not be attributed to DSS, AIFS or the ABS.
Funding
LSAC was funded by the DSS, the AIFS, and the ABS. This work was also supported in part by an Australian Research Council (ARC) under Laureate Fellowship grant number FL150100096, a Macquarie University Research Fellowship, and the National Health and Medical Research Council (NHMRC) under grant APP1047185. These funding bodies had no further role in the study design; in the collection, analysis, and interpretation of data; in writing; nor in the decision to submit the manuscript for publication.
Data Sharing and DeclarationThe data that support the findings of this study were obtained from the Department of Social Services under license. Restrictions apply to the availability of these data, so they are not publicly available.
Author information
Authors and Affiliations
Contributions
M.K.F. and R.M.R. conceived of the study; M.K.F. designed and conducted the statistical analyses, interpreted the results, drafted the Abstract, Method, Results, and Discussion, and revised the manuscript critically for intellectual content; N.R.M. drafted the Introduction, and revised the manuscript critically for intellectual content; R.M.R. participated in drafting all sections of the manuscript, and revised the full manuscript critically for intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The Longitudinal Study of Australian Children was approved by the Australian Institute of Family Studies Ethics Committee.All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
All individual participants provided informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
Forbes, M.K., Magson, N.R. & Rapee, R.M. Evidence that Different Types of Peer Victimization have Equivalent Associations with Transdiagnostic Psychopathology in Adolescence. J Youth Adolescence 49, 590–604 (2020). https://doi.org/10.1007/s10964-020-01202-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-020-01202-4