
Abstract
Eating disorder symptomatology is highly prevalent in adolescence and is regarded one of the most important precursors of clinical eating disorders. The present longitudinal study examined the development of eating disorder symptomatology in adolescents over two years. At Time 1,528 high school students filled out self-report questionnaires (50.5% female; Mage = 15 years). Multivariate latent growth curve modeling and latent class growth analyses were performed to model latent trajectories and to identify latent trajectory classes. Stable trajectories of drive for thinness and body dissatisfaction were found, whereas bulimia and BMI increased over time. Important gender differences pointed to girls experiencing more eating disorder symptoms at each time point. Additionally, more diverse trajectory classes were found in girls than in boys. Finally, classes with the most eating disorder symptoms also experienced the most problems in identity development, internalizing symptoms, and the least effortful control. The present study underscores the importance of identifying vulnerable adolescents that experience greater eating disorder symptomatology, as they also seem to experience the worst psychosocial development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescence is characterized by an increased focus on the body (Harter 1999), often accompanied by uncertainties about (changing) appearance (Tiggemann 2004). Up to 88% of adolescent girls and 83% of adolescent boys admit being dissatisfied with one or more aspects of their body (Ricciardelli and McCabe 2001), which is closely related to an internalization of perfect body ideals (Lawler and Nixon 2011). In Western societies, women are expected to be thin and slender, whereas males should have a lean and muscular body. These rather unrealistic expectations may put pressure on vulnerable youth, resulting in approximately 57% of girls and 30% of boys experimenting with disturbed eating behaviors (such as fasting, using diet pills or laxatives, purging, binge eating; Croll et al. 2002). Especially youth with a higher body mass index (BMI) are vulnerable to engage in these behaviors (Stice 2002). A higher BMI increases the social pressure to be thin and often results in a greater discrepancy between the present and ideal body weight (Jung et al. 2017). This experienced discrepancy, in turn, fosters body dissatisfaction and drive for thinness (Stice and Shaw 2002). As girls generally experience a greater increase in BMI throughout adolescence (Siervogel et al. 2003) and appear to have a stronger internalization of body ideals (Knauss et al. 2007), it is not surprising that they experience more body dissatisfaction and report more dieting and purging than boys (Lewinsohn et al. 2002). The present study aimed to investigate the development of eating disorder symptomatology in adolescent girls and boys over a period of two years by adopting both a variable-centered and person-centered approach.
Development of Eating Disorder Symptoms in Adolescence
A considerable amount of literature has been published on the development of eating disorder symptoms throughout adolescence. However, when focusing on various symptoms (such as body dissatisfaction, dieting, and bulimic symptoms), no general consensus exists. More specifically, studies that include various eating disorder symptoms find different patterns of change when comparing the symptom trajectories. Also, studies that focus on the same symptom find opposing patterns of change—possibly (partly) due to an inconsistent measurement of eating disorder symptoms in research.
With regard to body dissatisfaction (i.e., being dissatisfied with the size of specific body parts; Garner 2004), most research indicates an increase from early adolescence to young adulthood, both for boys and girls (Bucchianeri et al. 2013; Slane et al. 2014). This can partly be explained by increasing social pressures to conform to cultural ideals (Lawler and Nixon 2011; Stice 2002), but also by a general increase in BMI due to metabolic changes in adolescence (Bucchianeri et al. 2013; Siervogel et al. 2003). As in adolescence one’s appearance is important for getting accepted by peers, adolescents generally experience an increase in appearance-ideal internalization and body dissatisfaction (Lawler and Nixon 2011). However, some gender differences seem to exist. In girls, body dissatisfaction increases significantly between middle school and high school, while it remains relatively stable in the transition from high school to early young adulthood (Bucchianeri et al. 2013). In boys, an opposite pattern seems to exist as older adolescents experience a relative increase in body dissatisfaction, while younger adolescent boys reported no significant change in body dissatisfaction (Bucchianeri et al. 2013).
With regard to drive for thinness (i.e., an excessive concern with body weight and dieting, and comprising both a wish for weight loss and a fear of weight gain; Garner 2004), longitudinal studies point to general stability during adolescence in both girls and boys. However, most studies refer to dieting behavior or restrictive eating when investigating such a longitudinal trend. As drive for thinness seems to be one of the core motivations behind these types of behavior (Chernyak and Lowe 2008), the development of dieting is expected to be closely related to the development of drive for thinness. A study by Kansi et al. (2005) found dieting to have the highest correlational stability over 7 years in adolescent girls when taking various eating symptoms into account. Similarly, a study by Neumark-Sztainer et al. (2011) concluded that dieting is relatively stable from early adolescence to middle young adulthood. Hence, individuals that start engaging in dieting behavior in adolescence seem to be at risk for continued use of this behavior in adulthood as well. Recent evidence, however, points to the importance of differentiating longitudinal patterns by gender, as different trends of dieting have been found. A study by Allen et al. (2013) found dieting to be stable in girls, whereas it showed more fluctuation in boys (a decrease from age 14 to 17, followed by an increase from age 17 to 20). This gender differentiation is not surprising, as girls and boys encounter different eating disorder risk factors in life (such as the internalization of different body ideals, differences in body weight development, and females’ greater susceptibility to internalizing problems; Ferreiro et al. 2012; Keel et al. 2007; Thompson and Stice 2001).
Lastly, with regard to bulimic symptoms (such as uncontrollable episodes of overeating (bingeing) and/or purging; Garner 2004), some studies suggest that bulimic tendencies stay stable across adolescence (Neumark-Sztainer et al. 2011; Wertheim et al. 2001), whereas a larger number of studies conclude that binge eating and purging generally peak in late adolescence (e.g., Kansi et al. 2005; Slane et al. 2014). However, Abebe et al. (2012) pointed to an important gender difference as they found a general increase of bulimic symptoms from age 14 to 16 in girls, while this increase was only found in the early twenties in boys. They propose that early pubertal development may bring boys closer to the masculine body ideal, which would protect them against body dissatisfaction in early to middle adolescence and could (temporarily) decrease bulimic symptoms. In contrast, early pubertal development in girls would conflict more with the female body ideal and would make them more vulnerable to engage in bulimic symptoms early on. In sum, there is little agreement in the literature on the general development of eating disorder symptomatology and on the existence of possible gender differences.
In addition to this variable-centered approach focusing on general developmental trends, it is important to adopt a person-oriented approach and investigate heterogeneity in development by classifying individuals into latent trajectory classes. This approach allows for examining how groups of adolescent boys and girls may differ on their (developmental) pattern of ED symptoms. Previous research has demonstrated that individuals with a subclinical eating disorder profile are most at risk of developing a clinical eating disorder (Neumark-Sztainer et al. 2006; Stice 2002), whereas a healthy relation with food and the body protects against the development of such a diagnosis. Hence, identifying distinct developmental trajectory classes of eating disorder symptomatology provides clinically significant information for eating disorder prevention programs, as it can help in identifying groups of adolescents that are especially vulnerable or resilient for the development of a clinical eating disorder. This approach, which is rather new in eating disorder literature, has predominantly been carried out in female samples (Cain et al. 2010; Kansi et al. 2005; Micali et al. 2017; Swanson et al. 2014). Overall, most studies identified four main classes, mirroring the broad eating disorder diagnoses. First, the majority of adolescents are placed in an asymptomatic class, in which no substantial eating disorder symptoms are reported. Second, restrictive anorexia nervosa-like classes have been identified, characterized by dieting and varying levels of shape and weight concerns. Third, classes resembling subclinical and clinical bulimia nervosa have been repeatedly identified, with symptoms of binge eating, purging, and dieting. Lastly, most studies have uncovered classes characterized by binge eating and overeating without compensatory behaviors, which seems similar to a binge eating disorder profile. Unfortunately, as most studies were carried out in adolescent girls, no specific hypotheses can be made on such eating behavior classes in adolescent boys. Moreover, as an additional limitation, these studies examined classes at a specific time-point—only focusing on the mean scores of eating disorder symptoms at that specific time—and examined whether classification changed over time. Hence, the classes were not based on individuals’ developmental eating disorder profile. Accordingly, using the latent trajectories of eating disorder symptoms to identify classes would allow for a better understanding of the development of eating disorder symptomatology, as classes could differ on both the mean level and developmental change of eating disorder symptoms over time.
Risk and Maintenance Factors of Eating Disorder Symptoms
A large and growing body of literature has focused on various risk and maintenance factors of eating disorders (Stice 2002). One of the most well-known theories, the transdiagnostic theory of eating disorders of Fairburn et al. (2003), focuses on mood intolerance and dysfunctional self-evaluation as important maintaining mechanisms.
First, negative affect is commonly reported as both an antecedent and outcome of disturbed eating (Stice 2002). Indeed, disturbed eating behavior shows a high comorbidity with internalizing symptoms, such as depression and anxiety (Polivy and Herman 2002). Internalizing symptoms and eating disorder symptomatology seem to hold a circular relation, in which they reinforce one another over time. Puccio et al. (2017) has found that depressive feelings predict eating concerns in both female and male adolescents, which, in turn, predict anxiety. Similarly, feelings of body dissatisfaction predicts depressive feelings in both adolescent girls and boys (Ferreiro et al. 2014).
Second, effortful control—a self-regulatory aspect of temperament that comprises the ability to regulate behavior and attention to avoid future harm—appears to be especially poor in individuals engaging in binge eating and purging behavior (Claes et al. 2010). When encountered with negative emotions or general distress, individuals with poor effortful control are especially vulnerable to engage in bingeing and purging—generally described as impulsive behaviors with loss of control (Claes et al. 2010; Claes et al. 2002). A recent daily diary study (Schito et al. 2018) indeed described how low self-regulatory abilities in patients with a bingeing/purging eating disorder stimulate pathological eating behavior as maladaptive emotion regulation strategies. Moreover, in female community adolescents, both bulimic symptoms and body dissatisfaction were negatively predicted by effortful control (Kerremans et al. 2010). Hence, there seems to be a close relation between disturbed eating behavior and self-regulation—including the regulation of both emotions and behavior.
Lastly, the transdiagnostic theory of eating disorders of Fairburn et al. (2003) describes a dysfunctional self-evaluation—an overvaluation of shape and weight when evaluating the self—as the core pathological process of all eating disorders, causing a narrowly defined sense of identity (Corning and Heibel 2016; Stice 2002). Recently, there has indeed been an increasing amount of literature on identity functioning and disturbed eating. Identity development comprises one of the most central tasks in adolescence, with the purpose of experiencing oneself as an integrated person with self-identified ideals, values, and goals (Erikson 1968). Individuals who experience confusion about themselves and lack a clear sense of purpose in life (identity confusion; Erikson 1968), may be more vulnerable to internalize societal standards and, hence, to display dieting thoughts and behavior (Vartanian et al. 2018). Verstuyf et al. (2014) have demonstrated that individuals who easily conform important life choices to that of significant others (referred to as a normative identity style) are more susceptible to adopt the body perfect ideal. Consequently, these individuals report more appearance-focused eating regulation and rigid dietary restrictions. Similarly, patients with an eating disorder experience more identity confusion than individuals without this diagnosis, even hinting to the possibility of an identity disorder in these patients (Verschueren et al. 2017).
The Present Study
The present study is guided by three objectives. First, this study examined the development of eating disorder symptomatology and BMI across adolescence by estimating latent growth trajectories of drive for thinness, body dissatisfaction, bulimic symptoms, and adjusted BMI. In line with previous research, drive for thinness was expected to remain stable during adolescence, while an increase was expected for body dissatisfaction and bulimic symptoms. Moreover, as gender is important when assessing eating disorder symptoms, it was investigated whether these latent trajectories would be different for adolescent girls and boys. A higher level for all eating disorder symptoms was expected in girls, while no clear hypothesis could be made with regard to the rate of change. With regard to BMI, the present study focused on adjusted BMI, which is more appropriate for the present adolescent sample (see Measures section). As adjusted BMI takes into account the growth charts of a representative Flemish sample (Roelants and Hauspie 2004), the present study sample was assumed to have similar trajectories to the representative sample. Hence, a general stability of adjusted BMI was expected without any gender differences. To get a full understanding on (adjusted) BMI during the present study, analyses were repeated with BMI as well. It was expected that BMI would increase throughout adolescence (Bucchianeri et al. 2013), possibly more so in girls (Lee et al. 2011).
A second objective was to identify latent developmental trajectory classes of eating disorder symptomatology, with each class representing individuals with a similar developmental eating disorder profile. Based on previous research, it was expected to identify classes that would resemble the clinical eating disorder diagnoses—a restrictive anorexia-like class, a binging/purging bulimia-like class, a predominantly binge eating class, and an asymptomatic class. However, as these classes have only been identified in female samples before, no specific hypotheses were made for the male participants in the study.
The last objective of this study was to investigate whether the latent trajectory classes of eating disorder symptoms would develop differently on identity confusion, internalizing symptoms, and effortful control. As this research question is rather new in the empirical eating disorder literature, it is difficult to formulate specific hypotheses. However, it was expected that classes characterized by high eating disorder symptomatology, would also be characterized by the least adaptive functioning on these three risk factors, both in adolescent girls and boys. Specifically for effortful control, it was hypothesized that classes high on bulimic symptoms, would experience the most problems.
Materials and Methods
Participants
Data of the present longitudinal study were collected at three annual measurement waves in January 2015, January 2016, and January 2017, respectively. Through convenience sampling, a total of 1115 high school students in Flanders, the Dutch speaking part of Belgium, were invited to participate in the study. All students attended the same high school. At Time 1,528 students (50.5% female), with a mean age of 14.97 years (SD = 1.81; range 12–18), chose to participate (response rate = 47.35%). At Time 2, 385 students participated (52.71% female, retention rate = 72.92%) with a mean age of 15.51 (SD = 1.66, range 13–19) and at Time 3, 325 students participated (55.1% female, retention rate = 61.55%) with a mean age of 16.33 (SD = 1.62, range 14–20). Overall, 312 students participated at all three measurement waves (59.09%). At all time points, girls and boys did not significantly differ on age [Time 1: Mgirls = 14.82 years, Mboys = 15.12 years, F(1,523) = 0.362, p = 0.058, η2 = 0.007; Time 2: Mgirls = 15.47 years, Mboys = 15.56 years, F(1,381) = 0.269, p = 0.604, η2 = 0.001; Time 3: Mgirls = 16.34 years, Mboys = 16.33 years, F(1,322) = 0.001, p = 0.982, η2 = 0.000]. At both Times 2 and 3, drop-out was associated with descriptive and study variables on the previous wave. Students who dropped out were somewhat older [Time 2: Mretention = 14.52 years (SD = 1.66), Mdrop-out = 16.21 years (SD = 1.63), F(1,523) = 106.39, p < 0.001, η2 = 0.17; Time 3: Mretention = 15.28 years (SD = 1.58), Mdrop-out = 16.52 years (SD = 1.64), F(1,381) = 36.23, p < 0.001, η2 = 0.09], and were more likely to be female (Time 2: %femaleretention = 53.25%, %femaledrop-out = 42.86%, χ2(1) = 4.43, p = 0.035; Time 3: %femaleretention = 55.45%, %femaledrop-out = 43.84%, χ2(1) = 3.21, p = 0.073). They did not differ on adjusted BMI [Time 2: F(1, 492) = 0.67, p = 0.415; Time 3: F(1, 363) = 1.95, p = 0.163] and ED symptomatology [Time 2: F(3, 515) = 0.99, p = 0.398; Time 3: F(3, 377) = 1.29, p = 0.276]. However, Little’s (1988) Missing Completely At Random (MCAR) test was conducted to compare students with and without complete data on the three waves and produced a chi-square/degrees of freedom ratio (χ2/DF) of 1.13, which indicates that data were most likely MCAR (Bollen 1989). The Full Information Maximum Likelihood (FIML) procedure was used to handle missing values in the present study, as it is typically less biased than ad hoc procedures such as listwise or pairwise deletion (Schafer and Graham 2002).
Procedure
All students that were invited for participation received an information letter that described the longitudinal design of the study. Students were asked to fill out questionnaires at three annual measurement waves with a time interval of one year. Participation was voluntary and students were asked to sign an informed consent form. Additionally, active parental consent was obligatory for the participation of minors. Data collection took place during school hours, after which students were asked to return their questionnaires in a sealed envelope to the researchers who were present at the school. Students who chose to participate received a movie ticket as compensation. At Times 2 and 3, when students had left their high school or were absent the day of data collection, an online web-survey was send via e-mail to minimize drop-out. The online and offline data collection were executed simultaneously. The online data collection lasted one week, whereas the offline data collection lasted one month. During the entire study period, every student received a unique code number to ensure confidentiality. The study was approved by the ethical committee of the Faculty of Psychology and Educational Sciences, University of Leuven.
Measures
Body mass index
Participants reported on their height and weight, through which the Body Mass Index (BMI; weight/height2) could be calculated. No reporting bias was expected, as earlier research suggests that self-report weight and height are validly reported by both adolescents and adults (Field et al. 1999). However, when wanting to interpret BMI in an adolescent sample, age and gender must be taken into account. Hence, the growth charts of a representative Flemish sample were used (Roelants and Hauspie 2004) to calculate the adjusted BMI [(BMI/Percentile 50 of BMI for age and gender) x 100]. Moreover, the calculation of the adjusted BMI allows the determination of weight status of the participants (Van Winckel and Van Mil 2001). At Time 1, 9.50% of the participating students were underweight (adjusted BMI ≤ 85), 77.5% had a normal weight (85 < adjusted BMI < 120), 6.30% were overweight (120 ≤ adjusted BMI < 140), and 1.30% were obese (140 ≤ adjusted BMI). This weight-status distribution seemed a proper representation of the Flemish high-school population as it was almost identical to a previous Flemish study in both male and female high school students (Goossens et al. 2016).
Eating disorder symptomatology
The Eating Disorder Inventory-3 (EDI-3; Garner 2004) is a valid and reliable questionnaire that can be used as an eating disorder screening tool in community samples (Lehmann et al. 2013; Nyman-Carlsson et al. 2015). The present study made use of the eating disorder Risk Scales that comprise some of the central features of an eating disorder: drive for thinness (n = 7, example item “I am preoccupied with the desire to be thinner”), body dissatisfaction (n = 9, example item “I think that my stomach is too big”), and bulimia (n = 7, example item “I stuff myself with food”). Each item is scored on a 6-point Likert-type scale (ranging from 1_never to 6_always). Cronbach’s alpha coefficients for drive for thinness at Times 1–3 were respectively 0.91, 0.92, and 0.92, Cronbach’s alpha coefficients for body dissatisfaction were all 0.94, and Cronbach’s alphas for bulimia were 0.75, 0.79, 0.81, respectively.
Identity confusion
The Erikson Psychosocial Stage Inventory (EPSI; Rosenthal et al. 1981) has been proven to have good psychometric properties and to index identity confusion (Schwartz et al. 2009). The Identity Confusion Subscale consists of 6 items that are scored on a 5-point Likert-type scale (from 1_strongly disagree to 5_strongly agree) and measures current feelings of identity confusion. As it does not focus explicitly on the duration or chronicity of these feelings and/or their impact on someone’s life, the questionnaire may tap into both normative identity confusion and sustained (or chronic) identity diffusion. In the present study, the Cronbach’s alpha coefficients for identity confusion at Times 1–3 were respectively 0.67, 0.70, 0.74.
Internalizing symptoms
The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith 1983) was used to assess internalizing symptoms as it taps into symptoms of both depression and anxiety. A meta Confirmatory Factor Analysis (CFA) has recommended to use the HADS as a measure of general distress (Norton et al. 2013). The questionnaire contains 14 items that are scored on a 4-point Likert scale (from 0_never to 3_almost always). In the present study, Cronbach’s alpha coefficients for the total HADS score were 0.81, 0.83, and 0.87 at Times 1, 2, and 3, respectively.
Effortful control
The Adult Temperament Questionnaire (ATQ; Evans and Rothbart 2007) was used to assess the extent to which individuals experience high or low levels of effortful control. The questionnaire includes 19 items on a 7-point Likert scale (from 1_not at all applicable to 7_completely applicable). The present study made use of the total mean score of the questionnaire with Cronbach’s alpha coefficients being 0.77, 0.77, and 0.82, at Times 1, 2, and 3, respectively.
Primary Statistical Analyses
First, multivariate Latent Growth Curve (LGC) modeling in Mplus (version 7.4; Muthén and Muthén 2012) was conducted to examine developmental trajectories of eating disorder symptoms and adjusted BMI within a structural equation modeling framework. This statistical technique estimates intra-individual growth trajectories as well as individual differences in these trajectories over time by specifying the mean and variance of two latent growth factors: intercept and slope (Duncan and Duncan 2004). The factor loadings of the intercepts were fixed to 1. Given that measurement waves were equally spaced in time, the factor loadings of the linear slopes were fixed to 0, 1, and 2 for T1, T2, and T3, respectively. Model fit was evaluated using three fit indices: the Satorra-Bentler scaled chi-square (S-Bχ2), which should be as small as possible; the Comparative Fit Index (CFI), which should exceed 0.90 for reasonable fit and 0.95 for excellent fit; and the Root Mean Square Error of Approximation (RMSEA), which should be between 0.05 and 0.08 for reasonable fit and less than 0.05 for excellent fit (Kline 2005; Satorra and Bentler 2001). Next, this multivariate LGC was repeated when additionally controlling for age. More specifically, the intercepts and slopes of the eating disorder symptoms and adjusted BMI were regressed on age at Time 1, which gave virtually the same results as those in the uncontrolled modelFootnote 1.
To compare the developmental trajectories of eating disorder symptomatology and adjusted BMI between boys and girls, a multi-group approach was used. A multivariate LGC model was compared in which the estimated growth parameters of the developmental trajectories could vary among boys and girls (i.e., unconstrained model), to models in which these parameters were constrained as equal across gender (i.e., constrained models). Two constrained models were considered: (1) a model in which the intercepts were constrained and (2) a model in which the slopes were constrained. To compare the model fit of the unconstrained to the constrained models, a S-Bχ2 difference tests was conducted (Satorra and Bentler 2001).
Second, separately for girls and boys, a Latent Class Growth Analysis (LCGA) was performed to identify developmental trajectory classes of eating disorder symptomatology and adjusted BMI. LCGA is a person-centered approach in which individuals are probabilistically assigned to latent classes based upon similar patterns of responses on specified variables (Berlin et al. 2013; Muthén 2004). As LCGA assumes that individual growth trajectories are homogeneous within classes, the variance of intercept and slope were fixed to zero within a class. Several fit indices were used to decide on the optimal number of classes (Muthén and Muthén 2000; Nagin 2005). First, the Bayesian Information Criterion (BIC) for a solution with k classes should be lower than for a solution with k-1 classes. Second, entropy (E) was used to assess classification quality, as it represents the accuracy with which individuals are placed into the classes based upon the posterior classification probabilities. Values range from 0.00 to 1.00, with values greater than 0.75 indicating accurate classification (Reinecke 2006). Third, the Lo–Mendell–Rubin Loglikelihood Ratio Test (LMR-LRT) and its bootstrap variant (BLRT) were used, of which significant p-values indicate whether there is a statistically significant improvement in fit through including an additional class. Lastly, proportions for the latent classes should represent no less than 1% of the total sample (Jung and Wickrama 2008). To find a meaningful solution, class selection should ultimately be determined by these fit indices in combination with theoretical justification, parsimony, and interpretability (Johnson et al. 2007; Muthén 2003).
As the average posterior class membership probabilities ranged from 0.942 to 0.975 in girls and from 0.985 to 0.996 in boys, classification accuracy seemed excellent (Nagin 1999). Hence, class membership was identified for each participant by assigning them to the trajectory class of which their posterior probability of membership was highest. Multi-group LGC modeling was then used to investigate whether individuals belonging to the trajectory classes developed differently across time on identity confusion, internalizing symptoms, and effortful control. First, for each risk factor separately, a fully unconstrained baseline model was estimated in which intercept and slope could vary across the classes. Second, a model was estimated in which intercepts were held equal among all classes, followed by a model in which slopes were held equal. Finally, S-Bχ2 difference tests were used to compare model fit of the baseline model to these two constrained models. If the constrained models had a significantly poorer fit, this would indicate that classes differed from one another on intercept or slope. Subsequent Wald χ2-tests were used to examine which intercepts or slopes could be held equal across each possible pair of classes.
Results
Preliminary Analyses
Gender differences were found with respect to eating disorder symptoms [Wilks’Ʌ = 0.61, F(12,246) = 12.90, p < 0.001], with girls scoring significantly higher on drive for thinness, body dissatisfaction, and bulimia than boys. Conversely, girls and boys reported similar levels of adjusted BMI. At all time points, no gender differences were found between boys and girls. With regard to the risk factors, girls scored significantly higher on identity confusion and internalizing symptoms than boys, but they did not score differently on effortful control. Table 1 displays all univariate F-values. With regard to age, only body dissatisfaction was positively associated with age at Time 1 (r = 0.15, p < 0.05). Correlations among all eating disorder symptoms, adjusted BMI, and the risk factors are displayed in Table 2. Consistent positive correlations were found among all study variables, except for bulimia and adjusted BMI. All eating disorder symptoms were significantly positively associated with identity confusion and internalizing problems, and negatively with effortful control, whereas no significant correlations were found between identity confusion, internalizing problems, effortful control, and adjusted BMI.
Developmental Trajectories
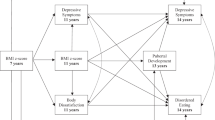
Table 3 presents unstandardized means and variances of slopes and intercepts for the multivariate LGC model in the total group, for boys and girls separately. The multivariate LGC modelFootnote 2 in the total group had an excellent fit [S-Bχ2(40) = 38,61, p = 0.532; RMSEA = 0; CFI = 1]. On average, no significant changes in drive for thinness and body dissatisfaction were observed over time (slopes of 0.00 and 0.03, respectively), whereas bulimic symptoms and adjusted BMI significantly increased over time (slopes of 0.08 and 0.58, respectively)Footnote 3. Significant variances for the growth parameters point to individual differences in intercepts and slopes of all ED symptoms and adjusted BMI trajectories. Model fit comparison between the unconstrained model and the constrained models indicated that the slopes of the developmental trajectories of ED symptomatology and adjusted BMI could be fixed as equal across gender [∆S-Bχ2(4) = 7.83, p = 0.098]. Model fit was significantly worse when constraining the intercept of the developmental trajectories across gender [∆S-Bχ2(4) = 197.02, p < 0.001], as the intercepts of all ED symptoms were consistently higher in girls (ranging from 2.00 to 3.63) than in boys (ranging from 1.79 to 2.29). Figure 1 gives an overview of the associations between intercepts and slopes of this model for both boys and girls. All intercepts were positively interrelated, as were the slopes. With respect to the positive associations among the intercepts, this indicates that when an individual has an elevated score on a specific eating disorder symptom, he/she will probably also have an elevated score on the other eating disorder symptoms and adjusted BMI. With regard to the slopes, when an individual increases on a specific eating disorder symptom over time, he/she will probably also increase on the other eating disorder symptoms. Conversely, the intercepts and slopes of drive for thinness and body dissatisfaction were negatively related to one another, indicating that the higher the intercepts of these variables, the lower their increases (or the stronger their decreases) over time.

Correlations between intercepts and slopes of the ED symptoms and adjusted BMI in the multivariate latent growth curve model with multi-group approach. All coefficients given are significant at p < 0.05, with correlations before the slash indicating the correlations in boys and correlations after the slash indicating the correlations in girls. ˟p> 0.05
Trajectory Classes
Table 4 presents all BIC, entropy, LMR-LRT, and BLRT values, as well as the trajectory class proportions for LCGA solutions with 2 through 5 classes for both girls and boysFootnote 4. In girls, a 4-class solution was preferred (BIC = 9909.397; E = 0.902) over a 3-class solution (BIC = 10028.602; E = 0.892) and a 2-class solution (BIC = 1031.179; E = 0.872). Although the LMR-LRT value of the 4-class solution was not significant (p = 0.119), the BLRT was significant (p < 0.01) which has been described as the best fit index when deciding on the number of classes in LCGA in Mplus (Nylund et al. 2007). Additionally, the 4-class solution identified a fourth class that represented overweight girls that experience more eating disorder symptoms. From a clinical perspective, this is an important class to distinguish as eating disorder symptoms could be differently motivated in overweight girls than girls with a normal weight. Taking this into account, the 4-class solution was preferred. Table 5 represents the parameter estimates of the eating disorder symptoms in all trajectory classes. Class 1 (n = 62, normal BMI/high symptoms) consisted of girls with a normal weight who reported high eating disorder symptoms. Class 2 (n = 113, normal BMI/low symptoms) consisted of girls with a normal weight as well, but they reported little eating disorder symptoms. Class 3 (n = 72, low BMI/low symptoms) resembled girls in Class 2, but consisted of girls who reported even less eating disorder symptoms than girls in Class 2 and they also reported a weight that could almost be categorized as underweight. Finally, Class 4 (n = 18, high BMI/high symptoms) consisted of girls that were overweight and reported high eating disorder symptoms. Auxiliary analyses indicated that the classes did not differ significantly on age at Time 1 [Mclass1 = 15.18 years (SD= 1.56), Mclass2 = 14.80 years (SD= 1.71), Mclass3 = 14.46 years (SD= 1.87), Mclass4 = 15.22 years (SD= 1.90); F(3, 261) = 2.45, p = 0.08].
In boys, when taking all fit indices into account, a 2-class solution was preferred (BIC = 8116.554; E = 0.978; pLMR-LRT < 0.001) over a 3-class solution (BIC = 8030.836, E = 0.788; pLMR-LRT = 0.287). Moreover, the added class in the 3-class solution did not seem to add any interesting theoretical insights, as it divided boys with a normal weight and low eating disorder symptoms (from the 2-class solution) into two classes with a normal weight but with one class having slightly more eating disorder symptoms than the other. As the differences on eating disorder symptoms was very small and the fit indices indicated a better fit for the 2-class solution, the most parsimonious solution was preferred. Class 1 (N = 47, high BMI/high symptoms) consisted of boys with a normal weight who could almost be categorized as overweight, and who also reported high eating disorder symptoms. Class 2 (N = 213, normal BMI/low symptoms) consisted of boys with a normal weight who reported little eating disorder symptoms. Auxiliary analyses indicated that the classes did not differ significantly on age at Time 1 [Mclass1 = 15.21 years (SD= 1.78), Mclass2 = 15.10 years (SD= 1.89); F(1, 258) = 0.13, p = 0.72].
Linking Trajectory Classes to Risk and Maintenance Factors
Table 6 represents all baseline parameter estimates of the multi-group LGC modeling of identity confusion, internalizing symptoms, and effortful control in girls and boys. With respect to identity confusion, the unconstrained model had an excellent fit in both girls and boys [Girls: χ2(8) = 4.94, p = 0.764; RMSEA = 0; CFI = 1; Boys: χ2(4) = 0.83, p = 0.934; RMSEA = 0; CFI = 1] and model fit comparison indicated that constraining the intercepts equal among the trajectory classes was not allowed [Girls: ∆χ2(3) = 37.00, p < 0.001; Boys: ∆χ2(1) = 11.22, p = 0.001]. In girls, follow-up analyses indicated that all pairs of intercepts differed from one another, except for Class 1 (normal BMI/high symptoms) and Class 4 [high BMI/high symptoms; Wald χ2(1) = 0.01, p = 0.922], in which individuals reported the highest levels of identity confusion. Individuals in Class 2 (normal BMI/low symptoms) and Class 3 (low BMI/low symptoms) reported less identity confusion, with girls in Class 3 reporting the lowest scores. In boys, Class 1 (high BMI/high symptoms) reported significantly more identity confusion than Class 2 (normal BMI/low symptoms). With regard to the slope, model fit comparison in girls indicated that the slope could not be constrained as equal among the trajectory classes [∆χ2(3) = 14.64, p = 0.002]. Consequently, follow-up analyses indicated that Class 4 (high BMI/high symptoms) significantly differed from the other classes, as it was the only class in which girls seemed to significantly decrease on identity confusion over time. In contrast, model fit comparison in boys indicated that the slope could be fixed among the two classes [∆χ2(1) = 1.51, p = 0.218].
For internalizing symptoms, the unconstrained model had an excellent fit for both girls and boys [Girls: χ2(8) = 5.88, p = 0.661; RMSEA = 0; CFI = 1; Boys: χ2(6) = 3.27, p = 0.775; RMSEA = 0; CFI = 1] and model fit comparison indicated that constraining intercepts equal among the classes significantly decreased model fit [Girls: ∆χ2(5) = 43.35, p < 0.001; Boys: ∆χ2 (1) = 12.55, p < 0.001]. In girls, follow-up analyses indicated a similar pattern as for identity confusion: Class 1 (normal BMI/high symptoms) and Class 4 (high BMI/high symptoms) did not significantly differ from one another [Wald χ2(1) = 0.12, p = 0.730] and reported the highest scores. However, Class 4 did not differ significantly from Class 2 (normal BMI/low symptoms) either [Wald χ2(1) = 3.07, p = 0.080]. Again, Class 3 (low BMI/low symptoms) reported the least symptoms. In boys, Class 1 (high BMI/high symptoms) experienced more internalizing symptoms than Class 2 (normal BMI/low symptoms). As for the slopes, the trajectory classes of girls did differ on developmental change of internalizing symptoms [∆χ2(5) = 5.84, p = 0.322], whereas those of boys did [∆χ2(1) = 6.46, p = 0.011]. Class 1 showed a significantly higher decrease on internalizing symptoms over time than Class 2.
Lastly, with respect to effortful control, the unconstrained model provided an excellent fit for both girls and boys [Girls: χ2(9) = 5.34, p = 0.804; RMSEA = 0; CFI = 1; Boys: χ2(4) = 4.26, p = 0.373; RMSEA = 0.02; CFI = 1]. In girls, constraining intercepts for effortful control equal across classes did not result in a significant decrease in model fit [∆χ2(3) = 4.96, p = 0.175] and, hence, was allowed. In boys, constraining intercepts across classes was not allowed [∆χ2(1) = 10.30, p = 0.001], as Class 2 (normal BMI/low symptoms) reported significantly higher effortful control than Class 1 (high BMI/high symptoms). Model fit comparison indicated that slopes could be fixed as equal among the classes for both girls and boys [Girls: ∆χ2(3) = 1.17, p = 0.759; Boys: ∆χ2(1) = 0.01, p = 0.944].
Discussion
Eating disorder symptomatology comprises both psychological and behavioral aspects of subclinical eating concerns and are highly prevalent in adolescence. As they are one of the most important risk factors for developing a clinical eating disorder, it is important to investigate how they develop in adolescence and which individuals seem to be more at risk. Although more and more research addresses this topic, inconsistent evidence has been found with respect to the developmental trajectories of eating symptomatology. More specifically, different patterns of change are found when comparing symptom trajectories. Additionally, no previous studies have distinguished different latent trajectory classes of eating disorder symptomatology in adolescence, while it is important to compare classes both on their mean level and on their developmental change over time. Hence, the present study set out to examine the development of eating disorder symptoms over a two-year period in both adolescent boys and girls and to identify latent development classes on these symptoms.
First, adopting a variable-centered approach, latent growth curves were examined. As expected, results indicated that girls consistently reported higher eating disorder symptom scores than boys, adding to the idea that girls experience more pressures to attain the body perfect ideals (Lawler and Nixon 2011). However, with regard to the slopes of the trajectories, no gender differences were found, which indicates that girls and boys do not seem to differ on changes in eating disorder symptoms over time. In line with expectations, drive for thinness remained stable over time, whereas bulimic symptoms increased significantly in both boys and girls. Adolescents seemed to experience a constant level of wishing to be thinner and/or fearing to gain weight throughout adolescence. In other words, for individuals experiencing drive for thinness, it is no temporary feeling that decreases over time, but it appears to be a continues feeling that could motivate them to engage in dieting behavior (Chernyak and Lowe 2008). With regard to bulimic symptoms, the increase in adolescence could be related to a shift in eating disorder symptoms throughout adolescence. Typically, restrictive eating and dieting are the first behaviors in which an individual engages when trying to lose weight (Fairburn and Brownell 2002). However, as these behaviors increase the attraction to food, it also increases the possibility of temporarily failing to maintain this dietary control, which would result in binge eating (and subsequent purging; Fairburn and Brownell 2002). Surprisingly, results indicated that body dissatisfaction remained stable at the group level, which is in contrast with the studies of Bucchianeri et al. (2013) and Slane et al. (2014), who found an increase in body dissatisfaction throughout adolescence. This inconsistency may be due to differences in study design, as the latent trajectories in the present study covered a two-year period compared to the 10 and 14 years in the studies of Bucchianeri et al. (2013) and Slane et al. (2014), respectively. Hence, it is possible that increases in body dissatisfaction develop gradually throughout adolescence and do not change significantly over a two-year period. The present findings could indeed represent a short-term snapshot of such a more extended developmental trajectory. With regard to adjusted BMI, a significant increase was found in both girls and boys which indicates that the present sample increased significantly more in BMI than the Flemish sample of Roelants and Hauspie in 2004. These findings corroborate earlier findings of adolescents’ BMI increasing more and more over the past decades (Lee et al. 2011).
Second, adopting a person-centered approach, latent trajectory classes of eating disorder symptoms and adjusted BMI were identified separately for girls and boys. In girls, four classes emerged that mainly differed on intercepts. As expected, the largest class (Class 2; 43%) was identified as an asymptomatic class, representing girls with a normal weight without substantial eating disorder symptoms. However, these girls still indicated to experience body dissatisfaction regularly, which corroborates the idea that negative body feelings are increasingly becoming the norm in adolescent girls (Ricciardelli and McCabe 2001; Striegel-Moore et al. 2002). Second, an alarming number of girls also had a normal weight but reported high scores on the eating disorder symptoms (Class 1, 23%), indicating that they are usually dissatisfied with their body and have a strong wish of being thinner. These findings should be a cause for worry as they illustrate the unhealthy body standards that adolescent girls are confronted with in Western society (Dittmar and Howard 2004). Pressures and internalization of the thin ideal may change the way some girls experience their own (normal) body—possibly leading to unhealthy weight control behavior. A third class was characterized by girls that were close to underweight and almost did not report any eating disorder symptoms (Class 3, 27%). This class may represent girls with a smaller body shape and, conforming to the female body ideals, they could experience less body concerns. These girls may be somewhat younger, as girls in early adolescence generally have less body fat and lower body mass as opposed to girls in late adolescence (Siervogel et al. 2003). However, auxiliary analyses indicated that, although this class seems to represent the youngest girls in the sample (MClass3 = 14.46 years), the age effect was not significant [F(3,261) = 2,25, p = 0.08]. Alternatively, it may be possible that for some (possibly older) girls in this class another explanation applies. The lower scores on eating disorder symptoms could also indicate an unintentional or deliberate denial of eating disorder thoughts and feelings, which often occurs in the early phase of an eating disorder (Vandereycken 2006). Individuals with a (subclinical) eating disorder can be reluctant to share eating disorder feelings as they fear being judged or being obligated to seek help. This denial may also function as self-deception, in which the individual convinces oneself of being healthy and not needing any social interference (Vandereycken 2006). Moreover, the research context of the present study lacks one-on-one support, which may stimulate underreporting of eating disorder symptoms (Williamson et al. 1995). Finally, the fourth class that was identified consisted of overweight girls that experience high eating disorder symptoms (Class 4, 7%). These results are not unexpected, as a high BMI is an important risk factor for disturbed eating behavior and body dissatisfaction (Stice and Shaw 2002).
In boys, less variability was found in the latent developmental trajectory classes as only two classes emerged. First, a small class was identified with boys being close to overweight and experiencing more eating disorder symptoms (Class 1, 18%). Similar to the overweight class in girls, these results could be expected (Stice and Shaw 2002). Second, the majority of the boys had a normal weight and reported almost no eating disorder symptoms (Class 2, 82%), which again may support the idea that the body perfect ideal is different for girls and boys. Whereas girls seem to internalize a body ideal that is highly focused on thinness, boys are confronted with a body ideal that promotes a lean muscular body (Cafri et al. 2005), which is less in line with drive for thinness as measured in the EDI-3. Additionally, these boys reported low scores on body dissatisfaction. However, it is important to keep in mind that this subscale in the EDI-3 focuses on the shape of specific body parts (such as waist, hips, buttocks), but does not assess muscularity. In future research, it would be interesting to include measures that focus on a drive for muscularity and excessive exercising, as it could identify very different trajectory classes in adolescent boys.
Lastly, it was investigated whether the latent trajectory classes of eating disorder symptoms would develop differently on internalizing symptoms, effortful control, and identity confusion over the two-year period. As expected, individuals in classes that were characterized by the highest eating disorder symptoms also experienced the least adaptive functioning on these eating disorder risk and maintenance factors. Hence, it is essential that health care professionals are aware of the high number of adolescents that experience eating disorder symptoms (even at a young age), as they may be the most vulnerable to experience internalizing symptoms, poor effortful control, and identity confusion as well. In girls, Classes 1 (normal BMI/high symptoms) and 4 (normal BMI/low symptoms) consistently experienced the most internalizing symptoms and identity confusion. However, with regard to effortful control, no significant differences were found among the latent trajectory classes in girls, contradicting earlier research (Claes et al. 2010; Kerremans et al. 2010). This lack of difference may be due to the fact that the four latent classes in girls did not differ as much on bulimic symptoms, as compared to drive for thinness and body dissatisfaction. As poor effortful control is most strongly related to bingeing and purging (Claes et al. 2010; Kerremans et al. 2010), it is possible that the similar levels on effortful control may be reflected in the somewhat smaller differences on bulimic symptoms between the classes. In boys, Class 1—characterized by the highest eating disorder symptoms—experienced the most problems on all risk factors. To conclude, especially internalizing symptoms and identify confusion seem to be related to these latent trajectory classes of eating disorder symptoms in adolescence. These results corroborate the transdiagnostic theory of Fairburn et al. (2003) in which mood intolerance and dysfunctional self-evaluation are described as important risk and maintenance factors of eating disorder psychopathology.
Interpretations should be made within the context of the study’s strengths and limitations. In contrast to earlier findings, the latent classes that emerged in the female sample of the present study did not mirror the different eating disorder diagnoses (anorexia nervosa, bulimia nervosa, binge eating disorder). A possible explanation for this might be that the present study made use of the EDI-3 (Garner 2004) to assess eating disorder symptoms, which measures rather general eating disorder symptoms and does not clearly assess restrictive eating and contains only one purging item. As restrictive eating may distinguish different eating disorder subtypes, it could explain why it was not possible to differentiate a restrictive anorexia-like class in the present study. Second, although the study sample included early to late adolescents, the period over which these adolescents were followed was relatively short. Results regarding change or stability levels of the eating disorder symptomatology were derived from a two year period and, hence, can only be interpreted in that way. A longer follow-up could offer more insights on the continuous changes of eating disorder symptomatology throughout adolescence. Third, the present study relied exclusively on self-report questionnaires, which may stimulate reporting bias and inflated correlations between the studied variables due to shared method variance. Including alternative methods (such as reports by family members or interviews) is advised in future research. Fourth, the present study did not include data on pubertal development of the participants, which could be an interesting indicator of eating disorder symptomatology (Baker et al. 2012). Similarly, the study only measured effortful control, but did not include emotion regulation—one of the core issues in eating pathology (Fairburn et al. 2003). Including these measures in future research on eating disorder profiles or classes would allow for a broader interpretation. Lastly, although internalizing symptoms, effortful control, and identity confusion were described as risk factors of eating disorder symptomatology throughout the paper, the present study did not investigate the directionality of effect and only focused on their simultaneous development with eating disorder symptoms.
Conclusion
Adolescence is an important life period for the development of eating disorder symptoms in both boys and girls. Previous research points to a general increase of these symptoms in adolescence, but a person-centered approach that focuses on such developmental change is lacking. The aim of the present research was to investigate the development of eating disorder symptomatology in adolescent boys and girls using both a variable-centered and person-centered approach. Results add to the growing body of research that indicates that adolescent girls are especially vulnerable to experience body dissatisfaction and have a wish of being thinner, regardless of their body weight. These findings are alarming and especially important for prevention purposes in adolescence, as BMI does not always seem to be a good indicator of eating disorder symptoms. In adolescence—a life period that is characterized by appearance preoccupation (Harter 1999)—individuals are highly susceptible for the internalization of society’s body ideals (Lawler and Nixon 2011), which seems to change individual’s perception of their own body. Additionally, the present study found drive for thinness and body dissatisfaction to be rather stable in adolescence, corroborating the idea that individuals experiencing these emotions early on are at risk for experiencing them throughout adolescence (Neumark-Sztainer et al. 2011; Slane et al. 2014). With regard to bulimia symptoms, the findings indicate an increase in both adolescent boys and girls, pointing to a possible shift from restrictive eating to bingeing and purging in adolescence. Finally, individuals with vulnerable eating profiles—experiencing more drive for thinness, body dissatisfaction, and bulimia symptoms—were also the most vulnerable to experience internalizing symptoms, poor effortful control, and identity confusion throughout adolescence.
Notes
More information can be obtained from the first author.
Details about all specific models that were tested in this study (which parameters were included and/or constrained), can be requested from the first author.
When conducting the LGC model with BMI, a significant increase can be found in both girls and boys (Interceptgirls = 19.85, Slopegirls = 0.63, Interceptboys = 19.65, Slopeboys = 0.63), mirroring earlier research (Bucchianeri et al. 2013).
Virtually the same latent classes emerged in girls and boys when including BMI instead of adjusted BMI. More information can be requested from the first author.
References
Abebe, D. S., Lien, L., & von Soest, T. (2012). The development of bulimic symptoms from adolescence to young adulthood in females and males: a population-based longitudinal cohort study. International Journal of Eating Disorders, 45, 737–745. https://doi.org/10.1002/eat.20950.
Allen, K. L., Crosby, R. D., Oddy, W. H., & Byrne, S. M. (2013). Eating disorder symptom trajectories in adolescence: effects of time, participant sex, and early adolescent depressive symptoms. Journal of Eating Disorders, 1, 32 https://doi.org/10.1186/2050-2974-1-32.
Baker, J. H., Thornton, L. M., Lichtenstein, P., & Bulik, C. M. (2012). Pubertal development predicts eating behaviors in adolescence. International Journal of Eating Disorders, 45, 819–826. https://doi.org/10.1002/eat.22022.
Berlin, K. S., Parra, G. R., & Williams, N. A. (2013). An introduction to latent variable mixture modeling (part 2): longitudinal latent class growth analysis and growth mixture models. Journal of Pediatric Psychology, 39, 188–203. https://doi.org/10.1093/jpepsy/jst085.
Bollen, K. A. (1989). Structural equations with latent variables. New York, NY: Wiley.
Bucchianeri, M. M., Arikian, A. J., Hannan, P. J., Eisenberg, M. E., & Neumark-Sztainer, D. (2013). Body dissatisfaction from adolescence to young adulthood: findings from a 10-year longitudinal study. Body Image, 10, 1–7. https://doi.org/10.1016/j.bodyim.2012.09.001.
Cafri, G., Thompson, J. K., Ricciardelli, L., McCabe, M., Smolak, L., & Yesalis, C. (2005). Pursuit of the muscular ideal: physical and psychological consequences and putative risk factors. Clinical Psychology Review, 25, 215–239. https://doi.org/10.1016/j.cpr.2004.09.003.
Cain, A. S., Epler, A. J., Steinley, D., & Sher, K. J. (2010). Stability and change in patterns of concerns related to eating, weight, and shape in young adult women: a latent transition analysis. Journal of Abnormal Psychology, 119, 255–267. https://doi.org/10.1037/a0018117.
Chernyak, Y., & Lowe, M. R. (2008). Drive for thinness is not the same as drive to be thin: on the motivation for dieting in normal weight restrained eaters and bulimic individuals. Appetite, 51, 358–358. https://doi.org/10.1016/j.appet.2008.04.054.
Claes, L., Robinson, M. D., Muehlenkamp, J. J., Vandereycken, W., & Bijttebier, P. (2010). Differentiating bingeing/purging and restrictive eating disorder subtypes: the roles of temperament, effortful control, and cognitive control. Personality and Individual Differences, 48, 166–170. https://doi.org/10.1016/j.paid.2009.09.016.
Claes, L., Vandereycken, W., & Vertommen, H. (2002). Impulsive and compulsive traits in eating disordered patients compared with controls. Personality and Individual Differences, 32, 707–714. https://doi.org/10.1016/S0191-8869(01)00071-X.
Corning, A. F., & Heibel, H. D. (2016). Re-thinking eating disorder prevention: the case for prioritizing the promotion of healthy identity development. Eating Disorders, 24, 106–113. https://doi.org/10.1080/10640266.2015.1034057.
Croll, J., Neumark-Sztainer, D., Story, M., & Ireland, M. (2002). Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: relationship to gender and ethnicity. Journal of Adolescent Health, 31, 166–175. https://doi.org/10.1016/S1054-139X(02)00368-3.
Dittmar, H., & Howard, S. (2004). Professional hazards? The impact of models’ body size on advertising effectiveness and women’s body-focused anxiety in professions that do and do not emphasize the cultural ideal of thinness. British Journal of Social Psychology, 43, 477–497. https://doi.org/10.1348/0144666042565407.
Duncan, T. E., & Duncan, S. C. (2004). An introduction to latent growth curve modeling. Behavior Therapy, 35, 333–363. https://doi.org/10.1016/S0005-7894(04)80042-X.
Erikson, E. H. (1968). Identity: youth and crisis. New York, NY: Norton.
Evans, D. E., & Rothbart, M. K. (2007). Developing a model for adult temperament. Journal of Research in Personality, 41, 868–888. https://doi.org/10.1016/j.jrp.2006.11.002.
Fairburn, C. G. & Brownell, K. D. (Eds) (2002). Eating disorders and obesity: a comprehensive handbook. 2nd ed. New York, NY: The Guilford Press.
Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behaviour Research and Therapy, 41, 509–528. https://doi.org/10.1016/S0005-7967(02)00088-8.
Ferreiro, F., Seoane, G., & Senra, C. (2012). Gender-related risk and protective factors for depressive symptoms and disordered eating in adolescence: a 4-year longitudinal study. Journal of Youth and Adolescence, 41, 607–622. https://doi.org/10.1007/s10964-011-9718-7.
Ferreiro, F., Seoane, G., & Senra, C. (2014). Toward understanding the role of body dissatisfaction in the gender differences in depressive symptoms and disordered eating: a longitudinal study during adolescence. Journal of Adolescence, 37, 73–84. https://doi.org/10.1016/j.adolescence.2013.10.013.
Field, A. E., Camargo, C. A., Taylor, C. B., Berkey, C. S., Frazier, A. L., Gillman, M. W., & Colditz, G. A. (1999). Overweight, weight concerns, and bulimic behaviors among girls and boys. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 754–760. https://doi.org/10.1097/00004583-199906000-00024.
Garner, D. M. (2004). EDI-3 eating disorders inventory-3: professional manual. Odessa, FL: Psychological Assessment Resources.
Goossens, L., Van Malderen, E., Van Durme, K., & Braet, C. (2016). Loss of control eating in adolescents: associations with adaptive and maladaptive emotion regulation strategies. Eating Behaviors, 22, 156–163. https://doi.org/10.1016/j.eatbeh.2016.06.015.
Harter, S. (1999). The construction of the self: a developmental perspective. New York, NY: Guilford Press.
Johnson, W., Hicks, B. M., McGue, M., & Iacono, W. G. (2007). Most of the girls are alright, but some aren’t: personality trajectory groups from ages 14 to 24 and some associations with outcomes. Journal of Personality and Social Psychology, 93, 266–284. https://doi.org/10.1037/0022-3514.93.2.266.
Jung, F., Spahlholz, J., Hilbert, A., Riedel-Heller, S. G., & Luck-Sikorski, C. (2017). Impact of weight-related discrimination, body dissatisfaction and self-stigma on the desire to weigh less. Obesity Facts, 10, 139–151. https://doi.org/10.1159/000468154.
Jung, T., & Wickrama, K. (2008). An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass, 2, 302–317. https://doi.org/10.1111/j.1751-9004.2007.00054.x.
Kansi, J., Wichstrøm, L., & Bergman, L. R. (2005). Eating problems and their risk factors: a 7-year longitudinal study of a population sample of Norwegian adolescent girls. Journal of Youth and Adolescence, 34, 521–531. https://doi.org/10.1007/s10964-005-8935-3.
Keel, P. K., Baxter, M. G., Heatherton, T. F., & Joiner, Jr, T. E. (2007). A 20-year longitudinal study of body weight, dieting, and eating disorder symptoms. Journal of Abnormal Psychology, 116, 422–432. https://doi.org/10.1037/0021-843X.116.2.422.
Kerremans, A., Claes, L., & Bijttebier, P. (2010). Disordered eating in adolescent males and females: associations with temperament, emotional and behavioral problems and perceived self-competence. Personality and Individual Differences, 49, 955–960. https://doi.org/10.1016/j.paid.2010.08.003.
Kline, R. B. (2005). Principles and practice of structural equation modeling. 2nd ed. New York, NY: Guilford Press.
Knauss, C., Paxton, S. J., & Alsaker, F. D. (2007). Relationships amongst body dissatisfaction, internalisation of the media body ideal and perceived pressure from media in adolescent girls and boys. Body Image, 4, 353–360. https://doi.org/10.1016/j.bodyim.2007.06.007.
Lawler, M., & Nixon, E. (2011). Body dissatisfaction among adolescent boys and girls: the effects of body mass, peer appearance culture and internalization of appearance ideals. Journal of Youth and Adolescence, 40, 59–71. https://doi.org/10.1007/s10964-009-9500-2.
Lee, H., Lee, D., Guo, G., & Harris, K. M. (2011). Trends in body mass index in adolescence and young adulthood in the United States: 1959–2002. Journal of Adolescent Health, 49, 601–608. https://doi.org/10.1016/j.jadohealth.2011.04.019.
Lehmann, V., Ouwens, M. A., Braeken, J., Danner, U. N., van Elburg, A. A., Bekker, M. H. J., & van Strien, T. (2013). Psychometric properties of the Dutch version of the eating disorder inventory–3. Sage Open, 3, 1–7. https://doi.org/10.1177/2158244013508415.
Lewinsohn, P. M., Seeley, J. R., Moerk, K. C., & Striegel-Moore, R. H. (2002). Gender differences in eating disorder symptoms in young adults. International Journal of Eating Disorders, 32, 426–440. https://doi.org/10.1002/eat.10103.
Little, R. J. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83, 1198–1202. https://doi.org/10.2307/2290157.
Micali, N., Horton, N., Crosby, R., Swanson, S., Sonneville, K., Solmi, F., & Field, A. (2017). Eating disorder behaviours amongst adolescents: investigating classification, persistence and prospective associations with adverse outcomes using latent class models. European Child and Adolescent Psychiatry, 26, 231–240. https://doi.org/10.1007/s00787-016-0877-7.
Muthén, B. (2003). Statistical and substantive checking in growth mixture modeling: comment on Bauer and Curran (2003). Psychological Methods, 8, 369–377.
Muthén, B. (2004). Latent variable analysis: growth mixture modeling and related techniques for longitudinal data. In D. Kaplan (Ed.), Handbook of quantitative methodology for the social sciences (pp. 345–368). Newbury Park, CA: Sage.
Muthén, B., & Muthén, L. K. (2000). Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcoholism: Clinical and Experimental Research, 24, 882–891. https://doi.org/10.1111/j.1530-0277.2000.tb02070.x.
Muthén, L. K., & Muthén, B. (2012). Mplus: the comprehensive modeling program for applied researchers: user’s guide. Los Angelos, CA: Muthén & Muthén.
Nagin, D. S. (1999). Analyzing developmental trajectories: a semiparametric, group-based approach. Psychological Methods, 4, 139–157. https://doi.org/10.1037/1082-989X.4.2.139.
Nagin, D. S. (2005). Group-based modeling of development. Cambridge, MA: Harvard University Press.
Neumark-Sztainer, D., Paxton, S. J., Hannan, P. J., Haines, J., & Story, M. (2006). Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. Journal of Adolescent Health, 39, 244–251. https://doi.org/10.1016/j.jadohealth.2005.12.001.
Neumark-Sztainer, D., Wall, M., Larson, N. I., Eisenberg, M. E., & Loth, K. (2011). Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. Journal of the American Dietetic Association, 111, 1004–1011. https://doi.org/10.1016/j.jada.2011.04.012.
Norton, S., Cosco, T., Doyle, F., Done, J., & Sacker, A. (2013). The hospital anxiety and depression scale: a meta confirmatory factor analysis. Journal of Psychosomatic Research, 74, 74–81. https://doi.org/10.1016/j.jpsychores.2012.10.010.
Nylund, K., Asparoutiov, T., & Muthen, B. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Structural Equation Modeling, 14, 535–569. https://doi.org/10.1080/10705510701575396.
Nyman-Carlsson, E., Engström, I., Norring, C., & Nevonen, L. (2015). Eating disorder inventory-3, validation in Swedish patients with eating disorders, psychiatric outpatients and a normal control sample. Nordic Journal of Psychiatry, 69, 142–151. https://doi.org/10.3109/08039488.2014.949305.
Polivy, J., & Herman, C. P. (2002). Causes of eating disorders. Annual Review of Psychology, 53, 187–213. https://doi.org/10.1146/annurev.psych.53.100901.135103.
Puccio, F., Fuller-Tyszkiewicz, M., Youssef, G., Mitchell, S., Byrne, M., Allen, N., & Krug, I. (2017). Longitudinal bi-directional effects of disordered eating, depression and anxiety. European Eating Disorders Review, 25, 351–358. https://doi.org/10.1002/erv.2525.
Reinecke, J. (2006). Longitudinal analysis of adolescents’ deviant and delinquent behavior: applications of latent class growth curves and growth mixture models. Methodology: European Journal of Research Methods for the Behavioral and Social Sciences, 2, 100–112. https://doi.org/10.1027/1614-2241.2.3.100.
Ricciardelli, L. A., & McCabe, M. P. (2001). Dietary restraint and negative affect as mediators of body dissatisfaction and bulimic behavior in adolescent girls and boys. Behaviour Research and Therapy, 39, 1317–1328. https://doi.org/10.1016/S0005-7967(00)00097-8.
Roelants, M., & Hauspie, R. (2004). Groeicurven 2-20 jaar, Vlaanderen 2004 [Growth charts 2-20 years, Flanders 2004]. Retrieved 28 Jul 28, 2017 (Vrije Universiteit Brussel).
Rosenthal, D. A., Gurney, R. M., & Moore, S. M. (1981). From trust on intimacy: a new inventory for examining Erikson’s stages of psychosocial development. Journal of Youth and Adolescence, 10, 525–537. https://doi.org/10.1007/BF02087944.
Satorra, A., & Bentler, P. M. (2001). A scaled difference chi-square test statistic for moment structure analysis. Psychometrika, 66, 507–514. https://doi.org/10.1007/BF02296192.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art. Psychological Methods, 7, 147. https://doi.org/10.1037//1082-989X.7.2.147.
Schito, G., Pelosi, A., Cordori, C., Marchesi, C., & De Panfilis, C. (2018). Affect regulation and effortful control in bingeing/purging eating disorders: a daily diary study. Journal of Psychosomatic Research, 109, 132–133. https://doi.org/10.1016/j.jpsychores.2018.03.137.
Schwartz, S. J., Zamboanga, B. L., Wang, W., & Olthuis, J. V. (2009). Measuring identity from an Eriksonian perspective: two sides of the same coin? Journal of Personality Assessment, 91, 143–154. https://doi.org/10.1080/00223890802634266.
Siervogel, R. M., Demerath, E. W., Schubert, C., Remsberg, K. E., Chumlea, W. C., Sun, S., & Towne, B. (2003). Puberty and body composition. Hormone Research in Paediatrics, 60, 36–45. https://doi.org/10.1159/000071224.
Slane, J. D., Klump, K. L., McGue, M., & Iacono, W. G. (2014). Developmental trajectories of disordered eating from early adolescence to young adulthood: a longitudinal study. International Journal of Eating Disorders, 47, 793–801. https://doi.org/10.1002/eat.22329.
Stice, E. (2002). Risk and maintenance factors for eating pathology: a meta-analytic review. Psychological Bulletin, 128, 825–848. https://doi.org/10.1037/0033-2909.128.5.825.
Stice, E., & Shaw, H. E. (2002). Role of body dissatisfaction in the onset and maintenance of eating pathology: a synthesis of research findings. Journal of Psychosomatic Research, 53, 985–993. https://doi.org/10.1016/S0022-3999(02)00488-9.
Striegel-Moore, R., Franko, D.L., Cash, T.F., & Pruzinsky, T. (2002). Body image issues among girls and women. In T.F. Cash & P.T. (Eds), Body image: a handbook of theory, research and clinical practice (pp. 189–191). New York, NY: The Guilford Press.
Swanson, S. A., Horton, N. J., Crosby, R. D., Micali, N., Sonneville, K. R., Eddy, K., & Field, A. E. (2014). A latent class analysis to empirically describe eating disorders through developmental stages. International Journal of Eating Disorders, 47, 762–772. https://doi.org/10.1002/eat.22308.
Thompson, J. K., & Stice, E. (2001). Thin-ideal internalization: mounting evidence for a new risk factor for body-image disturbance and eating pathology. Current Directions in Psychological Science, 10, 181–183. https://doi.org/10.1111/1467-8721.00144.
Tiggemann, M. (2004). Body image across the adult life span: Stability and change. Body Image, 1, 29–41. https://doi.org/10.1016/S1740-1445(03)00002-0.
Van Winckel, M., & Van Mil, E. (2001). Wanneer is dik te dik? In C. Braet & M. A. J. M. Van Winckel (Eds), Behandelingsstrategieën bij kinderen met overgewicht (pp. 11–26). Bohn Stafleu Van Loghum: Houten/Diegem.
Vandereycken, W. (2006). Denial of illness in anorexia nervosa—a conceptual review: part 2 Different forms and meanings. European Eating Disorders Review, 14, 352–368. https://doi.org/10.1002/erv.722.
Vartanian, L. R., Hayward, L. E., Smyth, J. M., Paxton, S. J., & Touyz, S. W. (2018). Risk and resiliency factors related to body dissatisfaction and disordered eating: the identity disruption model. International Journal of Eating Disorders, 51, 322–330. https://doi.org/10.1002/eat.22835.
Verschueren, M., Luyckx, K., Kaufman, E. A., Vansteenkiste, M., Moons, P., Sleuwaegen, E., & Claes, L. (2017). Identity processes and statuses in patients with and without eating disorders. European Eating Disorders Review, 25, 26–35. https://doi.org/10.1002/erv.2487.
Verstuyf, J., Van Petegem, S., Vansteenkiste, M., Soenens, B., & Boone, L. (2014). The body perfect ideal and eating regulation goals: investigating the role of adolescents’ identity styles. Journal of Youth and Adolescence, 43, 284–297. https://doi.org/10.1007/s10964-013-9949-x.
Wertheim, E. H., Koerner, J., & Paxton, S. J. (2001). Longitudinal predictors of restrictive eating and bulimic tendencies in three different age groups of adolescent girls. Journal of Youth and Adolescence, 30, 69–81. https://doi.org/10.1023/A:1005224921891.
Williamson, D. A., Anderson, D. A., Jackman, L. P., & Jackson, S. R. (1995). Assessment of eating disordered thoughts, feelings, and behaviors. In D. B. Allison (Ed.), Handbook of assessment methods for eating behaviors and weight-related problems (pp. 347–386). London: Sage.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361–370.
Acknowledgements
Margaux Verschueren has a Ph.D. Fellowship of the Research Foundation-Flanders. The authors thank the high school students for participating in the study.
Funding
Margaux Verschueren has a Ph.D. fellowship of the Research Foundation—Flanders (1125918N).
Authors’ Contributions
M.V. conceived of the study, participated in its design and coordination, performed the statistical analyses, and drafted the manuscript; L.C. collected the data of the present study, conceived of the study, participated in its design and coordination and drafted the manuscript; N.P. participated in the design of the manuscript and helped drafting it; A.B. participated in the design of the manuscript and helped drafting it; A.G. collected the data of the present study; P.M. participated in the design of the manuscript and helped drafting it; K.L. conceived of the study, participated in its design and coordination, performed the statistical analyses, and drafted the manuscript. All authors read and approved the final manuscript.
Data Sharing Declaration
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The study was approved by the ethical committee of the Faculty of Psychology and Educational Sciences, University of Leuven.
Informed Consent
All participants signed an informed consent form and active parental consent was obligatory for the participation of minors.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Verschueren, M., Claes, L., Palmeroni, N. et al. Eating Disorder Symptomatology in Adolescent Boys and Girls: Identifying Distinct Developmental Trajectory Classes. J Youth Adolescence 49, 410–426 (2020). https://doi.org/10.1007/s10964-019-01174-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-019-01174-0