
Abstract
Factors that might exacerbate or mitigate the transmission of depressive symptoms from parents to adolescents and the continuity of depressive symptoms into early adulthood are poorly understood. This study tested the hypothesis that the intergenerational transmission and stability of depressive symptoms would be stronger for girls than boys over adolescence and into early adulthood, while considering the possibility that the pattern of gender moderation might vary depending on parent gender and developmental timing. The participants were 667 rural Midwestern adolescents (52 % female) and their parents. Survey data on maternal and paternal depressive symptoms (at youth age 11) and on adolescent and young adult depressive symptoms (at youth ages 11, 18, and 21) were analyzed via multiple group structural equation modeling. Maternal depressive symptoms predicted increased late adolescent depressive symptoms for girls but not boys, and adolescent depressive symptoms were more stable in girls. Paternal depressive symptoms predicted increased late adolescent depressive symptoms for all youth. The findings suggest the need for early, tailored interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Levels of depressive symptoms increase in adolescence and early adulthood (Garber et al. 2002), especially among girls (Angold et al. 2002; Hankin et al. 1998), and are associated with increased risk for subsequent suicide and other adverse mental and physical health outcomes, including depression diagnoses (Lepine and Briley 2011; Rudolph et al. 2006). For these reasons, considerable attention has been directed toward understanding the developmental etiology of depressive symptoms in youth. Additional research is needed, particularly research directed toward understanding the factors that might mitigate or exacerbate the risk for depression. The current study examines the intergenerational transmission and stability of depressive symptoms in a sample of rural youth followed from the outset of adolescence, at age 11, into early adulthood, at age 21, and tests youth’s gender as a potential moderator of these developmental risk processes.
Depression clusters in families (Beardslee et al. 1996; Harrington 1996; Merikangas et al. 1988; Pilowsky et al. 2006; Silberg et al. 2010). Children of depressed parents are as much as 3 times more likely to develop depression than children of non-depressed parents (Weissman et al. 2006). Likewise, parents’ elevated depressive symptoms have been shown to increase depressive symptoms in their children (e.g., Garber and Cole 2010). Heritability plays a role in the intergenerational transmission of depression diagnoses and symptoms (Klein et al. 2001; Silberg et al. 2010; Sullivan et al. 2000), perhaps more so for females than males (Kendler et al. 2001). However, genetic influences are only a partial explanation.
There is evidence for a substantial role of the environment in the etiology of depression, and the intergenerational transmission of depressive symptoms is due, in part, to psychosocial factors (England and Sim 2009; Goodman 2002; Silberg et al. 2010), such as parenting. Although peer influences increase during adolescence, parents continue to influence their children throughout the teen years (Fleming et al. 2010; Pardini et al. 2008). Hammen et al. (2004) provided support for an interpersonal stress model in which maternal depression disrupts the development of positive parenting and youth social competence, both of which increase, in turn, risk for adolescent depression (indicated by both current depression diagnoses and current depressive symptoms). Similarly, Garber and Cole (2010) reported results consistent with a “launch and grow” model characterized by maternal depression cascading into a series of developmental risk processes, such as disrupted family relationships, leading to increased growth in adolescent’s depressive symptoms.
Thus, it has become evident that the intergenerational transmission of depressive symptoms is due to a combination of genetic and environmental influences. Even while important lines of research continue to elucidate the precise biopsychosocial mechanisms involved in such transmission, broader questions about the conditions under which parents’ depressive symptoms influence that of their children remain relatively unanswered. In particular, risk for elevated depressive symptoms among children may vary depending on which parent struggles with depression, for example, due to differences often observed between mothers and fathers in their parenting roles (e.g., primary caregiver) and time spent directly interacting with children. The vast majority of the extant studies have restricted their attention to the influence of maternal depression on offspring (Cummings and Davies 1994; Fergusson et al. 1995; Goodman and Gotlib 1999; Goodman et al. 2011; Lovejoy et al. 2000); therefore, less is known about the influence of paternal depression (Wilson and Durbin 2010). Generally, depression in fathers does appear to increase the risk for depressive symptoms in children (Connell and Goodman 2015; Kane and Garber 2015; Phares and Compas 1992; Wilson and Durbin 2010), although some exceptions to this finding do exist (Agerup et al. 2015; Tully et al. 2008). Among studies that have directly compared the effects of maternal and paternal depression, the findings tend to show that the magnitude of effects from mothers and fathers is comparable (Reeb and Conger 2009; Reeb et al. 2015). Given the relative lack of attention to understanding the consequences of paternal versus maternal depression and mixed findings in existing studies, there is a pressing need for additional research that includes both fathers and mothers.
Youth’s gender also is an important consideration, and the intergenerational transmission of depressive symptoms may be sensitive to the gender match between parents and their children, although the issue of gender match has received relatively little attention in prior research. Gender differences in depressive symptoms emerge in early adolescence, with greater risk for girls compared to boys, and these differences continue to diverge into early adulthood (Angold et al. 2002; Hankin et al. 1998). A few studies have examined variation in the intergenerational transmission of depression across youth gender groups, often guided by the gender intensification hypothesis, which posits that adolescence brings increased pressures for girls and boys to conform to stereotypical gender roles in the move toward adulthood, and that such roles (e.g., femininity) increase vulnerability for depression among girls (Hill and Lynch 1983). This suggests that the intergenerational transmission of depressive symptoms would be particularly strong between mothers and their daughters. Indeed, evidence suggests that maternal depression places girls at greater risk for depression-related outcomes, including depressive symptoms, than boys during adolescence (Chen et al. 2009; Cortes et al. 2006; Davies and Windle 1997; Goodman et al. 2011).
However, the gender intensification hypothesis has been called into question (Priess et al. 2009) and other findings have been mixed. For example, among the few studies that include fathers, some results have suggested that adolescent girls experience greater risk for depressive symptoms than boys in the presence of elevated paternal depressive symptoms (Reeb and Conger 2009; Reeb et al. 2015). By contrast, Eberhart et al. (2006) found that paternal depression diagnoses increased risk for adolescent depression diagnoses among boys but not girls. Others have reported no gender moderation in the intergenerational transmission of depression diagnoses and symptoms (Currier et al. 2006; Pettit et al. 2008). This study extends the literature regarding the role of a gender match in the intergenerational transmission of depressive symptoms, examining parents’ depressive symptoms when their children were in early adolescence, a critical period in which gender differences in depressive symptoms emerge (Angold et al. 2002; Hankin et al. 1998).
Once established in youth, elevated depressive symptoms and depression diagnoses tend to persist and recur after periods of remission. Numerous longitudinal studies have demonstrated that earlier depression and depressive symptoms confer risk for subsequent depression diagnoses and elevated depressive symptoms among young people (Devine et al. 1994; Hammen and Brennan 2003; Lewinsohn et al. 1999; Pine et al. 1999). For example, as many as 50 % of individuals treated for a depression diagnosis will have a recurring episode, often within less than 5 years of their first diagnosis (American Psychiatric Association 2000). These findings reflect significant longitudinal stability, although studies often only cover a short period of time or a single developmental period (e.g., adolescence). This study examined the stability of depressive symptoms from early to late adolescence and into early adulthood, testing for gender moderation of stability coefficients across these developmental periods. Prior findings concerning gender moderation of the stability of depressive symptoms are equivocal; some studies have found no such gender differences during adolescence (Holsen et al. 2000; Tram and Cole 2006), although when gender differences are observed they tend to reveal higher stability coefficients for girls than boys (Wickrama et al. 2012). It is likely that depressive symptoms, once established in the early adolescent years, remain stable to a greater degree for girls than boys, perhaps due to the pressures faced by young women to conform to relatively inviolate, culturally-based gender roles that may increase girls’ vulnerability for depressive symptoms (Hill and Lynch 1983). As gender differences continue to diverge into early adulthood and depressive symptoms become more deeply rooted, the stability of depressive symptoms may become even stronger for young women compared to young men.
Hypotheses
To help fill gaps in the literature, the current study examines potential gender moderation of the intergenerational transmission and stability of depressive symptoms throughout adolescence and into adulthood, from age 11 to age 21. This study provides advancements over many prior investigations by (a) including both mothers and fathers, (b) capitalizing on the availability of longitudinal data over a 10-year time frame spanning two developmental periods, (c) drawing on multi-rater assessments of adolescent depressive symptoms, and (d) conducting latent variable analyses. Based on studies indicating gender differences in vulnerability for elevated depressive symptoms (Cortes et al. 2006; Davies and Windle 1997; Reeb and Conger 2009), it was expected that intergenerational transmission and stability would be stronger for girls than boys, although analyses considered the possibility that the pattern of gender moderation might vary depending on parent gender and developmental timing (i.e., early to late adolescence and late adolescence to early adulthood).
Method
Participants
Data were drawn from a longitudinal randomized prevention trial of family-focused substance misuse preventive interventions. Families of 6th graders enrolled in 33 rural schools in 19 counties of a Midwestern state in the United States participated in the trial. Targeted schools were those in communities with a population of less than 8500 and in districts with at least 15 % of families eligible for free or reduced cost lunches. Blocking by school size and proportion of students residing in low income households, 11 schools each were randomly assigned to one of three conditions: a minimal-contact control condition, a Preparing for the Drug Free Years (PDFY; Haggerty et al. 1999) condition, and an Iowa Strengthening Families Program (ISFP; Molgaard and Kumpfer 1993) condition. Of the 1309 eligible families, 667 (51 %) were enrolled and completed pretesting in the fall of 1993, including 208 control, 221 PDFY, and 238 ISFP families. Given the study sites, most participants were Caucasian (97 %). Families had an average of three children, and 85 % were dual-parent. The average age of target children was 11.3 years (SD = .50) when the study began; 52 % of these children were girls (n = 345). Nineteen percent of mothers and 22 % of fathers had graduated from college. The median annual household income in 1993 was $33,400.
In addition to pretest data collected in early adolescence during the 6th grade, current analyses used data collected from youth and their parents in late adolescence during the 12th grade (n = 457 families; 69 % retention), when youth were age 17.7 years on average (SD = .54), and in early adulthood, (n = 483; 72 % retention), when youth were age 21.6 years on average (SD = .44). Analyses from this ongoing project have documented the representativeness of enrolled families and found little evidence for selective attrition, except a consistent tendency for parents with a higher educational level to remain in the study compared to those with a lower education level (Spoth et al. 2001, 2009).
Procedures
Informed consent was obtained from parents for their participation and for the participation of their adolescent child, who also provided assent during adolescence and consent in early adulthood. All study procedures were approved by the Institutional Review Boards at Iowa State University and the University of Washington. Participating families received a packet in the mail that included information about the study and initial questionnaires. Then, a home visit was made, which lasted about 2.5 h, to obtain additional separately-completed assessments with parent(s) and their child. Participants were assured of the confidentiality of their responses, and each family member was compensated $10/h for their participation. Families were notified about their condition assignment after pretesting. Similar procedures were used at the follow-up assessments during adolescence, whereas phone interviews were conducted with young adult participants at age 21.
Interventions
Although the interventions were not a primary focus of the current analyses, prior research has demonstrated that the family-focused substance misuse prevention programs had spillover effects on reduced levels of adolescent depressive symptoms (Mason et al. 2007; Trudeau et al. 2007). The interventions have been described in detail elsewhere (Spoth et al. 2009), and both incorporate similar content and components. Briefly, PDFY has five two-hour sessions designed to help parents develop and communicate clear expectations and consequences regarding substance misuse, and increase involvement, reduce conflict, and promote bonding in the family. One of the five sessions focuses on peer resistance skills and is attended by parents and adolescents. In each of the seven ISFP sessions, adolescents and parents participate separately in the first hour and then join together during the second hour. ISFP sessions focus on helping parents improve communication and parenting skills as well as reduce family conflict, whereas adolescents are taught problem solving, coping, and peer resistance skills. Control families received four leaflets describing different aspects of adolescent development.
Measures
Parental Depressive Symptoms
Maternal depressive symptoms and paternal depressive symptoms were latent variables represented by 10 of 13 depression scale items from the Symptom Checklist-90—Revised (SCL-90-R; Derogatis 1983), completed by each parent at pretest. The item stem was “During the past week, how much were you distressed or bothered by… “(e.g., “Feeling low in energy or slowed down”, “Feeling blue”, and “Feeling everything is an effort”) rated on a 5-point scale from 1 to 5 (“not at all”, “a little bit”, “a moderate amount”, “quite a bit”, and “extremely”). Three of the original SCL-90-R depression scale items (thoughts of ending life, crying easily, and feeling lonely) were excluded due to extreme non-normality (e.g., kurtosis values over 50 for suicidal thoughts) or poor performance in the measurement model (e.g., factor loading <.30 for crying easily in fathers). Alpha reliabilities for the 10-item scales were acceptable (maternal α = .89; paternal α = .86).
Early Adolescent Depressive Symptoms
Early adolescent depressive symptoms were represented as a latent variable composed of multiple rater reports (mother, father, child) completed at pretest (age 11). The mean of a subset of 8 items drawn from the anxiety/depression scale of either the Youth Self-Report (YSR) or the corresponding child behavior checklist (CBCL) (Achenbach and Rescorla 2001) was computed for each reporter. The item stem for YSR items, for example, was “How true is each of these statements for you now or in the past 6 months?” (e.g., “I feel lonely”, “I cry a lot”, “I am unhappy, sad, or depressed”), with a rating scale of “not true” (0), “somewhat or sometimes true” (1), and “very true or often true” (2). Parents completed the corresponding CBCL with item wording specific to caregiver completion rather than self-report; for the few single parent families in the sample, scores from the absent parent were treated as missing in the latent variable analyses. Alpha reliabilities for maternal, paternal and self-report were 0.75, 0.73, and 0.76, respectively.
Late Adolescent Depressive Symptoms
Late adolescent depressive symptoms were measured the same way as early adolescent depressive symptoms, except they were assessed at the end of high school (age 18). Alpha reliabilities were 0.78 for both maternal and paternal reports, and 0.84 for adolescent self-report.
Young Adult Depressive Symptoms
Depressive symptoms at age 21 were represented as a latent variable with indicators from two self-rated instruments: (1) the Adult Self-Report (ASR; Achenbach and Rescorla 2003) and (2) the Diagnostic Interview Schedule (DIS; Robins et al. 1989). While the ASR is scaled the same as the YSR, only 5 of the original 8 items were common to both measures and thus collected across all 3 ages (11, 18, and 21). The 5 items in common were: “I cry a lot”, “I feel that no one loves me”, “I feel worthless or inferior”, “I feel too guilty”, “I am unhappy, sad, or depressed” (excluded from the ASR were: “tries to hurt self”, and “thinks of suicide”). At age 21, “There is very little that I enjoy”, was added as another indicator of depressive symptoms. The average of these 6 items (α = .67) yielded one indicator of young adult depressive symptoms. The second indicator for the latent variable was past year major depressive disorder at age 21, measured using the DIS to capture the emergence of a diagnosis, indicating the presence (coded 1) or absence (coded 0) of a disorder according to DSM-IV criteria (American Psychiatric Association 2000).
Covariates
As noted, prior project analyses have demonstrated PDFY and ISFP intervention effects on reduced adolescent depressive symptoms (Mason et al. 2007; Trudeau et al. 2007); therefore, intervention condition was included as a covariate. Specifically, a family intervention variable was coded 1 for randomization into either the PDFY or ISFP groups and 0 for randomization into the control group. PDFY and ISFP have similar program components, and direct comparisons have revealed very few statistically significant differences in intervention effects across PDFY and ISFP conditions (Spoth et al. 2001). At pretest, each parent answered an item regarding their highest grade of schooling completed, coded 0 for “kindergarten/no grade completed” through 20 for “Ph.D. or other doctorate.” Parent education was a measure of the average education level for parent(s) in the family.
Analyses
Multiple group structural equation modeling analyses were conducted using Mplus 7.11 (Muthén and Muthén 1998-2015) to test the conceptual model depicted in Fig. 1. Parameter estimates were generated using the weighted least squares means- and variance-adjusted (WLSMV) estimator, due to the categorical major depressive disorder indicator of the young adult depressive symptoms latent variable. In Mplus, the WLSMV estimator incorporates a pair-wise deletion strategy for handling missing data, which retained the overall sample size of 667. School was specified as a clustering variable. Multiple group analyses were conducted based on gender as the grouping variable, including family intervention and parent education as covariates by allowing them to correlate with the early adolescent exogenous variables and predict the late adolescent and young adult endogenous variables.

Conceptual model of the intergenerational transmission and stability of depressive symptoms
Analyses began with an evaluation of the measurement model via confirmatory factor analysis (CFA), including tests of metric invariance (i.e., invariance of the factor loadings) across gender groups as well as over time. After establishing the measurement model, tests of structural differences between gender groups were conducted via structural equation modeling (SEM) using a two-step process that compared structurally unconstrained and structurally constrained models, as reported in the Results section. The fit of the constrained model was compared to that of the unconstrained model using the difftest option in Mplus to compute a Chi square difference test. A statistically significant Chi square value indicates an overall group difference, in which case independent difference tests, with each constrained pathway compared in turn to the structurally unconstrained model, were conducted to determine which specific paths varied for girls and boys.
The goal of these analysis steps was to settle on a final multiple group model with a combination of free and constrained parameter estimates based on results from the Chi square difference tests to reveal similarities and differences in paths across gender groups. Model fit was evaluated using the Chi square statistic, the comparative fit index (CFI), and the root mean square error of approximation (RMSEA) based on recommended guidelines for acceptable fit (e.g., about .95 or greater for the CFI and about .06 or less for the RMSEA; Hu and Bentler 1999). The model in Fig. 1 permits an opportunity to examine the indirect effects of parent depressive symptoms on the young adult outcome through late adolescent depressive symptoms. Statistical significance of the indirect effects was determined based on the Sobel test using the model indirect command in Mplus (Sobel 1982).
A series of analyses was conducted to determine whether or not it was permissible to pool the sample across experimental conditions by testing for potential differences in the hypothesized path coefficients in the family intervention group versus the control group. An unconstrained SEM that allowed all path coefficients to vary across these groups, Χ2 (798 df, N = 667) = 937.876, p < .05, CFI = .937, RMSEA = .023, was compared to one in which all structural paths were constrained to equality across groups, Χ2 (809 df, N = 667) = 940.449, p < .05, CFI = .940, RMSEA = .022. Results showed that the parameter constraints did not significantly reduce model fit, Χ2 Δ (11 df, N = 667) = 8.683, p = .6511, indicating that there were no differences in the path coefficients for family intervention versus control groups. Thus, the sample was pooled across these groups and the analyses reported below focused on tests of gender moderation, including the family intervention variable as one of the covariates.
Results
Means and standard deviations by gender are reported in Table 1. Multiple gender differences were found. Mothers of boys rated themselves as having more depressive symptoms of blaming self, worrying too much, and feelings of worthlessness. At early adolescence (age 11), paternal ratings of child depressive symptoms were higher for girls than boys. Self-report of depressive symptoms was higher for girls than boys at every age (11, 18, 21) collected. As young adults (age 21), more young women met criteria for major depressive disorder than did young men.
Multiple group CFAs conducted across gender groups began with a fully unconstrained measurement model, Χ2 (784 df, N = 667) = 929.369, p < .05, CFI = .940, RMSEA = .024. Next, a model was estimated in which each factor loading was forced to take on the same value across groups and, for the repeated measures, the same value over time. The fit between the data and the constrained model was acceptable, Χ2 (809 df, N = 667) = 937.385, p < .05, CFI = .947, RMSEA = .022, and this model did not fit significantly worse than the unconstrained model, Χ2 Δ (25 df, N = 667) = 29.866, p = .229. Thus, results supported a measurement model that was invariant across gender groups and over time. Factor loadings from the final CFA are reported by gender in Table 2. Correlations among study variables included in the CFA are reported by gender in Table 3. Correlations were in expected directions; for example, there were statistically significant positive correlations among measures of depressive symptoms in early adolescence, late adolescence, and early adulthood for both boys and girls. The measurement model from this CFA served as the basis for subsequent multiple group SEM analyses.
Next, a structurally unconstrained multiple group SEM was estimated to begin testing for gender group differences in the paths depicted in Fig. 1. This model was structurally saturated and displayed the same fit statistics as the final measurement model. This initial SEM was compared to one in which all structural paths were constrained to equality across groups, Χ2 (820 df, N = 667) = 963.563, p < .05, CFI = .941, RMSEA = .023. Results showed that the parameter constraints contributed to a statistically significant decrement in model fit, Χ2 Δ (11 df, N = 667) = 32.046, p = .001. Thus, a series of independent difference tests was conducted according to the steps described above to determine which specific paths varied across groups. The series of tests is summarized in Table 4. Results showed that gender group constraints on two path coefficients were untenable: the paths from maternal depressive symptoms and early adolescent depressive symptoms to late adolescent depressive symptoms. Thus, a final model was estimated that released the constraints on these two paths, while retaining all other structural model constraints. The fit between the data and the final model was acceptable, Χ2 (818 df, N = 667) = 940.794, p < .05, CFI = .950, RMSEA = .021, and this model did not fit significantly worse than the structurally unconstrained model, CFA, Χ2 Δ (9 df, N = 667) = 7.489, p = 0.586.
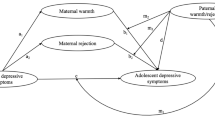
Path coefficients from the final multiple group gender model are reported in Fig. 2. Coefficients in bold were freely estimated for boys and girls. Beginning with group invariant paths involved in the intergenerational transmission of depressive symptoms, results showed that paternal depressive symptoms had a statistically significant positive association with late adolescent depressive symptoms. Neither paternal nor maternal depressive symptoms had statistically significant direct associations with young adult depressive symptoms for either boys or girls. Two paths involved in the stability of adolescent depressive symptoms were invariant across groups. Specifically, both early adolescent depressive symptoms and late adolescent depressive symptoms had statistically significant positive associations with young adult depressive symptoms, and these effects were equal in magnitude for boys and girls.

Final multiple group gender model results. Note: G Girls, B Boys; Unstandardized coefficients are presented with standardized coefficients in parentheses; Bold paths that were unconstrained across groups; r Correlation; *p < .05; Parent education and family intervention were included as covariates (not shown)
There were two gender differences in the structural portion of the model, one involved in the intergenerational transmission pathway and one involved in the stability pathway. Maternal depressive symptoms was a statistically significant positive predictor of late adolescent depressive symptoms for girls but not boys. Moreover, early adolescent depressive symptoms had a stronger positive relationship with late adolescent depressive symptoms for girls than boys. Results further showed that there was a statistically significant indirect effect of paternal depressive symptoms on the young adult outcome via late adolescent depressive symptoms for both girls (b = .019, s.e. = .008), p < .05; β = .073) and boys (b = .019, s.e. = .008, p < .05; β = .085), whereas the indirect effect for maternal depressive symptoms was statistically significant for girls (b = .024, p < .05; β = .107) but not for boys (b = .000, s.e. = .006, p > .05; β = −.001).
Examination of covariate effects (results not reported in full, but available on request), showed that the family intervention variable predicted decreased depressive symptoms from early to late adolescence similarly for both boys (b = −.04, s.e. = .02, p < .05; β = −.12) and girls (b = −.04, s.e. = .02, p < .05; β = −.11). Taken together, variables in the model explained an estimated 14 % of the variance in late adolescent depressive symptoms and 33 % of the variance in young adult depressive symptoms for boys, and 25 % of the variance in late adolescent depressive symptoms and 32 % of the variance in young adult depressive symptoms for girls.
Discussion
Parents’ depressive symptoms influence those of their children (England and Sim 2009; Goodman 2002; Silberg et al. 2010), particularly during early adolescence when depressive symptoms tend to emerge and gender differences reflecting increased vulnerability among girls compared to boys arise (Angold et al. 2002; Hankin et al. 1998). Once established in youth, depressive symptoms tend to persist over time, with gender differences increasing into early adulthood (Devine et al. 1994; Hammen and Brennan 2003; Lewinsohn et al. 1999; Pine et al. 1999). Many studies in this area of research have focused on the influence of maternal depression, leaving questions about the role of gender match between parents and their children in the intergenerational transmission and stability of depressive symptoms relatively unanswered. The current study examined gender moderation of the intergenerational transmission and stability of depressive symptoms during adolescence and early adulthood. Results showed that youth’s gender moderated two key pathways. Maternal depressive symptoms predicted increased late adolescent depressive symptoms for girls but not boys. Moreover, the stability of depressive symptoms from early to late adolescence was stronger for girls than boys. Paternal depressive symptoms increased depressive symptoms in late adolescence, which predicted, in turn, young adult depressive symptoms for all youth. It is also interesting that early adolescent depressive symptoms had a persistent positive relationship with the young adult outcome, over and above late adolescent depressive symptoms and the other predictors in the model.
Few studies have examined the relative influences of both maternal and paternal depressive symptoms across youth’s gender. Most studies have focused on mothers, typically showing a stronger influence of maternal depression on girls than boys (Cortes et al. 2006; Davies and Windle 1997; Goodman et al. 2011). Consistent with these findings, our results indicated that maternal depressive symptoms predicted increased adolescent depressive symptoms for girls but not for boys. The findings regarding the impact of paternal depression are mixed, with studies reporting a stronger influence on girls (Reeb and Conger 2009; Reeb et al. 2015), a stronger influence on boys (Eberhart et al. 2006), or a comparable influence across gender groups (Currier et al. 2006; Pettit et al. 2008). Here, results supported the latter by failing to reveal gender moderation in the pathway from paternal depressive symptoms to increased adolescent depressive symptoms; the positive association was comparable for boys and girls. The gender match between mothers and their daughters appears to play an important role in the progression of depressive symptoms for adolescent girls (Davies and Windle 1997), consistent with the gender intensification hypothesis (Hill and Lynch 1983). It is interesting that depressive symptoms in fathers appears to impact both their daughters and sons. It is possible that this reflects the elevated risk for depression that girls experience in a variety of circumstances. It also might reflect the importance of a gender match between fathers and sons in the development of depression among boys; however, additional research on the intergenerational transmission of depression in fathers and their sons is needed to examine, for example, promising mechanisms (e.g., parent–child relationship quality) of effects.
There was also an indication that depressive symptoms remained more stable over adolescence for girls than boys, which is consistent with some prior research (Wickrama et al. 2012). Interestingly, stability into early adulthood was comparable across gender groups, which may indicate that adolescence is a particularly sensitive period for the emergence of gender differences not only in the onset but also the maintenance of depressive symptoms during the teen years. Future studies should examine the mechanisms involved in this finding. A promising line of theory and research focuses on rumination or the tendency to repetitively reflect on the symptoms and causes of depression, a process that was unmeasured in the current study. Consistent with response styles theory (Nolen-Hoeksema 1991), rumination is more common among girls than boys (Rood et al. 2009), as is co-rumination with peers (Stone et al. 2011), and both processes may contribute to the intergenerational transmission and stability of depressive symptoms over time (e.g., Woody et al. 2016).
Additional findings, although secondary to the primary research questions, are noteworthy. Interestingly, neither maternal nor paternal depressive symptoms directly predicted the young adult outcome over and above adolescent depressive symptoms. There was, however, a statistically significant indirect effect of paternal depressive symptoms for all youth as well as a statistically significant indirect effect of maternal depressive symptoms for girls. In contrast, early adolescent depressive symptoms had a persistent positive direct effect on young adult depressive symptoms. This could be an indication that the early emergence of elevated depressive symptoms carries unique risk for lasting problems, perhaps because early emergence represents a more serious manifestation of depression or because it culminates in an extended period of risk exposure. Factors known to contribute to early onset of depression and risk for later major depressive disorder include parental depression and antisocial behavior, childhood mistreatment, childhood poor academic functioning, early pubertal development, and negative emotionality (Wilson et al. 2014).
This study has several strengths, including the prospective longitudinal design spanning two developmental periods (adolescence and young adulthood), the inclusion of both mothers and fathers, the multi-rater assessments of adolescent depressive symptoms, and the latent variable analyses. These features provide advancements over much prior research, which typically has analyzed cross-sectional or short-term longitudinal data via traditional analytic techniques (e.g., regression) and focused primarily on the consequences of maternal depression for children.
Still, there are some noteworthy limitations. The sample is homogenous, reflecting the rural Midwestern study location. Although rates of depressive symptoms can be elevated in rural populations (Probst et al. 2005), the degree to which the current findings generalize to more diverse youth in metropolitan settings is unknown. Measures of adolescent depressive symptoms, although demonstrating strong content coverage and adequate reliability, were derived from truncated scales. It is unknown how valid the truncated scales are in relation to the full scales. Also, these measures were checklists that permitted an assessment of adolescent depression-related symptoms over a short recall period according to either parent or adolescent report; thus, we were unable to determine the presence of adolescent clinical depression. Likewise, depression diagnoses were not assessed in the parents. An additional caveat is that assessments of depressive symptoms for target youth, although identical in adolescence, changed somewhat at the young adult assessment period. Correlations between the adolescent depressive symptoms constructs and the young adult outcome were positive and statistically significant, as anticipated; however, a lack of consistency in the assessments may have contributed to an underestimation of stability into early adulthood and biased predictive paths. Finally, although the study spanned early adolescence to early adulthood, addressing stability across these developmental periods, analyses did not consider dynamic changes that occur over the large gap between ages 11 and 18; further analyses that address questions of short-term change and bidirectional influences (e.g., between parents’ and adolescents’ depressive symptoms throughout the teen years) are needed.
Conclusion
Although the intergenerational transmission (England and Sim 2009; Goodman 2002; Silberg et al. 2010) and stability (Devine et al., 1994; Hammen and Brennan 2003; Lewinsohn et al. 1999; Pine et al. 1999) of adolescent depressive symptoms have been well documented, questions remain about the role of parent and adolescent gender, and the gender match between parents and their children, in these developmental processes. This study helps fill gaps in the literature by examining moderation by youth’s gender of the influence of both mothers’ and fathers’ depressive symptoms on that of their children. A key finding was that maternal depressive symptoms predicted increased late adolescent depressive symptoms for girls but not boys, which is consistent with the gender intensification hypothesis (Hill and Lynch 1983). Interestingly, however, paternal depressive symptoms influenced late adolescent depressive symptoms equally across gender groups. The stability of depressive symptoms during adolescence was stronger for girls than boys. The findings from this study may have implications for understanding the developmental etiology, prevention, and treatment of adolescent and young adult depressive symptoms. Specifically, the findings reinforce the elevated risk for depression experienced by girls, and support efforts to target young women, in particular, with tailored depression-related programming. Given the role of parental depression and the enduring influence of early emerging depressive symptoms, early family-focused depression prevention efforts are needed (Beardslee et al. 2003). It is encouraging that family-focused substance misuse preventive interventions can have spillover effects on depression as a non-targeted outcome, as demonstrated in our prior research (Mason et al. 2007; Trudeau et al. 2007). With replication and extension, these findings hold promise for helping to improve intervention efforts designed to reduce the burden of depressive symptoms among adolescents and young adults.
References
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms and profiles. Burlington, VT: Univesity of Vermont, Research Center for Children, Youth, and Families.
Achenbach, T. M., & Rescorla, L. A. (2003). Manual for the ASEBA adult forms & profiles. Burlington, VT: University of Vermont.
Agerup, T., Lydersen, S., Wallander, J., & Sund, A. M. (2015). Maternal and paternal psychosocial risk factors for clinical depression in a Norwegian community sample of adolescents. Nordic Journal of Psychiatry, 69, 35–41.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, fourth edition, text revision (DSM-IV-TR). Washington, DC: American Psychiatric Association.
Angold, A., Erkanli, A., Silberg, J., Eaves, L., & Costello, E. J. (2002). Depression scale scores in 8-17-year-olds: Effects of age and gender. Journal of Child Psychology and Psychiatry, 43, 1052–1063.
Beardslee, W. R., Gladstone, T. R., Wright, E. J., & Cooper, A. B. (2003). A family-based approach to the prevention of depressive symptoms in children at risk: Evidence of parental and child change. Pediatrics, 112(2), e119–e131.
Beardslee, W. R., Keller, M. B., Seifer, R., Lavori, P. W., Staley, J., Podorefsky, D., & Shera, D. (1996). Prediction of adolescent affective disorder: Effects of prior parental affective disorders and child psychopathology. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 288.
Chen, M., Johnston, C., Sheeber, L., & Leve, C. (2009). Parent and adolescent depressive symptoms: The role of parent attributions. Journal of Abnormal Child Psychology, 37, 119–130.
Connell, A. M., & Goodman, S. H. (2015). The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: A meta-analysis. Psychological Bulletin, 128, 746–773.
Cortes, R. C., Fleming, C. B., Catalano, R. F., & Brown, E. C. (2006). Gender differences in the association between maternal depressed mood and child depressive phenomena from grade 3 through grade 10. Journal of Youth and Adolescence, 35, 815–826.
Cummings, E. M., & Davies, P. T. (1994). Maternal depression and child development. Journal of Child Psychology and Psychiatry, 35, 73–112.
Currier, D., Mann, M. J., Oquendo, M. A., Galfalvy, H., & Mann, J. J. (2006). Sex differences in familial transmission of mood disorders. Journal of Affective Disorders, 95, 51–60.
Davies, P. T., & Windle, M. (1997). Gender-specific pathways between maternal depressive symptoms, family discord, and adolescent adjustment. Developmental Psychology, 33, 657–668.
Derogatis, L. R. (1983). Administration, scoring, and procedures manual II. Baltimore: Clincial Psychometric Research.
Devine, D., Kempton, T., & Forehand, R. (1994). Adolescent depressed mood and young adult functioning: A longitudinal study. Journal of Abnormal Child Psychology, 22, 629–640.
Eberhart, N. K., Shih, J. H., Hammen, C., & Brennan, P. (2006). Understanding the sex difference in vulnerability to adolescent depression: An examination of child and parent characteristics. Journal of Abnormal Child Psychology, 34, 495–508.
England, M. J., & Sim, I. J. (2009). Depression in parents, parenting, and children: Opportunities to improve identification, treatment, and prevention. Washington, DC: National Academies Press.
Fergusson, D. M., Horwood, L. J., & Lynskey, M. T. (1995). Maternal depressive symptoms and depressive symptoms in adolescents. Journal of Child Psychology and Psychiatry, 36, 1161–1178.
Fleming, C. B., Catalano, R. F., Haggerty, K. P., & Abbott, R. D. (2010). Relationships between level and change in family, school, and peer factors during two periods of adolescence and problem behavior at age 19. Journal of Youth and Adolescence, 39, 670–682.
Garber, J., & Cole, D. A. (2010). Intergenerational transmission of depression: A launch and grow model of change across adolescence. Development and Psychopathology, 22, 819–830.
Garber, J., Keiley, M. K., & Martin, N. C. (2002). Developmental trajectories of adolescents’ depressive symptoms: Predictors of change. Journal of Consulting and Clinical Psychology, 70, 79–95.
Goodman, S. H. (2002). Early experiences and depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression and its treatment (pp. 245–267). New York: Guilford.
Goodman, S. H., & Gotlib, I. H. (1999). Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review, 106, 458–490.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14, 1–27.
Haggerty, K., Kosterman, R., Catalano, R. F., & Hawkins, J. D. (1999). Preparing for the Drug Free Years. Washington, DC: Office of Juvenile Justice and Delinquency Prevention.
Hammen, C., & Brennan, P. A. (2003). Severity, chronicity, and timing of maternal depression and risk for adolescent offspring diagnoses in a community sample. Archives of General Psychiatry, 60, 253–258.
Hammen, C., Shih, J. H., & Brennan, P. A. (2004). Intergenerational transmission of depression: Test of an interpersonal stress model in a community sample. Journal of Consulting and Clinical Psychology, 72, 511–522.
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., McGee, R., & Angell, K. E. (1998). Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107, 128–140.
Harrington, R. (1996). Family-genetic findings in child and adolescent depressive disorders. International Review of Psychiatry, 8, 355–368.
Hill, J. P., & Lynch, M. E. (1983). The intensification of gender-related role expectations during early adolescence. In J. Brooks-Gunn & A. Petersen (Eds.), Girls at puberty: Biological and psychosocial perspectives (pp. 201–228). New York: Plenum.
Holsen, I., Kraft, P., & Vitterso, J. (2000). Stability in depressed mood in adolescence: Results from a 6-year longitudinal panel study. Journal of Youth and Adolescence, 29, 61–78.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55.
Kane, P., & Garber, J. (2015). The relations among depression in fathers, children’s psychopathology, and father-child conflict: A meta-analysis. Clinical Psychology Review, 24, 339–360.
Kendler, K. S., Gardner, C. O., Neale, M. C., & Prescott, C. A. (2001). Genetic risk factors for major depression in men and women: Similar or different heritabilities and same or partly distinct genes? Psychological Medicine, 31, 605–616.
Klein, D. N., Lewinsohn, P. M., Seeley, J. R., & Rohde, P. (2001). A family study of major depressive disorder in a community sample of adolescents. Archives of General Psychiatry, 58, 13–20.
Lepine, J. P., & Briley, M. (2011). The increasing burden of depression. Neuropsychiatric Disease and Treatment, 7(Supplement 1), 7.
Lewinsohn, P. M., Rohde, P., Klein, P., & Seeley, J. R. (1999). Natural course of adolescent major depressive disorder, I: Continuity into young adulthood. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 56–63.
Lovejoy, M. C., Graczyk, P. A., O’Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20, 561–592.
Mason, W. A., Kosterman, R., Haggerty, K., Hawkins, J. D., Spoth, R., & Redmond, C. (2007). Influence of a family-focused substance use preventive intervention on growth in adolescent depressive symptoms. Journal of Research on Adolescence, 17, 541–564.
Merikangas, K. R., Prusoff, B. A., & Weissman, M. M. (1988). Parental concordance for affective disorders: Psychopathology in offspring. Journal of Affective Disorders, 15, 279–290.
Molgaard, V., & Kumpfer, K. L. (1993). The Iowa strengthening families program for families with pre- and early adolescents. Ames, IA: Social and Behavioral Research Center for Rural Health.
Muthén, L. K., & Muthén, B. O. (1998-2015). Mplus User’s Guide: Seventh edition. Los Angeles, CA: Muthen & Muthen.
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569–582.
Pardini, D. A., Fite, P. J., & Burke, J. D. (2008). Bidirectional associations between parenting practices and conduct problems in boys from childhood to adolescence: The moderating effect of age and African-American ethnicity. Journal of Abnormal Child Psychology, 36, 647–662.
Pettit, J. W., Olino, T. M., Roberts, R. E., Seeley, J. R., & Lewinsohn, P. M. (2008). Intergenerational transmission of internalizing problems: Effects of parental and grandparental major depressive disorder on child behavior. Journal of Clinical Child and Adolescent Psychiatry, 37, 640–650.
Phares, V., & Compas, B. E. (1992). The role of fathers in child and adolescent psychopathology: Make room for daddy. Psychological Bulletin, 111, 387–412.
Pilowsky, D. J., Wickramaratne, P. J., Rush, J. A., Hughes, C. W., Garber, J., Malloy, E., & Weissman, M. M. (2006). Children of currently depressed mothers: A STAR*D ancillary study. Journal of Clinical Psychiatry, 67, 126–136.
Pine, D. S., Cohen, E., Cohen, P., & Brook, J. (1999). Adolescent depressive symptoms as predictors of adult depression: Moodiness or mood disorder? American Journal of Psychiatry, 156, 133–135.
Priess, H. A., Lindberg, S. M., & Hyde, J. S. (2009). Adolescent Gender-Role Identity and Mental Health: Gender Intensification Revisited. Child Development, 80(5), 1531–1544.
Probst, J. C., Laditka, S., Moore, C. G., Harun, N., & Powell, M. P. (2005). Depression in rural populations: Prevalence, effects on life quality, and treatment-seeking behavior. Columbia, SC: South Carolina Rural Health Resource Center.
Reeb, B. T., & Conger, K. J. (2009). The unique effect of paternal depressive symptoms on adolescent functioning: Associations with gender and father-adolescent relationship closeness. Journal of Family Psychology, 23, 758–761.
Reeb, B. T., Wu, E. Y., Martin, M. J., Gelardi, K. L., Chan, S. Y. S., & Conger, K. J. (2015). Long-term effects of fathers’ depressed mood on youth internalizing symptoms in early adulthood. Journal of Research on Adolescence., 25(1), 151–162.
Robins, L., Helzer, J., Cottler, L., & Goldring, E. (1989). NIMH Diagnostic Interview Schedule: Version III revised (DIS-III-R), question by question specifications. St. Louis, MO: Washington University.
Rood, L., Roelfos, J., Bogels, S., Nolen-Hoeksema, S., & Schouten, E. (2009). The influence of emotion-focused rumination and distraction on depressive symptoms in non-clinical youth: A meta-analytic review. Clincal Psychology Review, 29, 606–617.
Rudolph, K. D., Hammen, C., & Daley, S. E. (2006). Adolescent mood disorders. In D. A. Wolfe & E. J. Mash (Eds.), Behavioral and emotional disorders in adolescence: Nature, assessment, and treatment (pp. 300–342). New York: Guilford.
Silberg, J. L., Maes, H., & Eaves, L. J. (2010). Genetic and environmental influences on the transmission of parental depression to children’s depression and conduct disturbance: An extended children of twins study. Journal of Child Psychology and Psychiatry, 51, 734–744.
Sobel, M. E. (1982). Asymptotic intervals for indirect effects in structural equations models. In S. Leinhart (Ed.), Sociological Methodology (pp. 290–312). San Francisco, CA: Jossey-Bass.
Spoth, R. L., Redmond, C., & Shin, C. (2001). Randomized trial of brief family interventions for general populations: Adolescent substance use outcomes 4 years following baseline. Journal of Consulting and Clinical Psychology, 69, 627–642.
Spoth, R., Trudeau, L., Guyll, M., Shin, C., & Redmond, C. (2009). Universal intervention effects on substance use among young adults mediated by delayed adolescent substance initiation. Journal of Consulting and Clinical Psychology, 77, 620–632.
Stone, L. B., Hankin, B. L., Gibb, B. E., & Abela, J. R. Z. (2011). Co-rumination predicts the onset of depressive disorders during adolescence. Journal of Abnormal Child Psychology, 120, 752–757.
Sullivan, P. F., Neale, M. C., & Kendler, K. S. (2000). Genetic epidemiology of major depression: Review and meta-analysis. American Journal of Psychiatry, 157, 1552–1562.
Tram, J., & Cole, D. A. (2006). A multimethod examination of the stability of depressive symptoms in childhood and adolescence. Journal of Abnormal Psychology, 115, 674–686.
Trudeau, L., Spoth, R., Randall, G., & Azevedo, K. (2007). Longitudinal effects of a universal family-focused intervention on growth patterns of adolescent internalizing symptoms and polysubstance use: Gender comparisons. Journal of Youth and Adolescence, 36, 740.
Tully, E. C., Iacono, W. G., & McGue, M. (2008). An adoption study of parental depression as an environmental liability for adolescent depression and childhood disruptive disorders. American Journal of Psychiatry, 165, 1148–1154.
Weissman, M. M., Wickramaratne, P., Nomura, Y., Warner, V., Pilowsky, D., & Verdeli, H. (2006). Offspring of depressed parents: 20 years later. Archives of General Psychiatry, 163, 1001–1008.
Wickrama, K. A. S., Conger, R. D., Lorenz, F. O., & Martin, M. (2012). Continuity and discontinuity of depression from late adolescence to young adulthood: The mediating and moderating effects of young adults’ socioeconomic attainment. Journal of Adolescence, 35, 648–658.
Wilson, S., & Durbin, C. E. (2010). Effects of paternal depression on fathers’ parenting behaviors: A meta-analytic review. Clinical Psychology Review, 30, 167–180.
Wilson, S., Vaidyanathan, U., Miller, M. B., McGue, M., & Iacono, W. G. (2014). Premorbid risk factors for major depressive disorder: Are they associated with early onset and recurrent course? Development and Psychopathology, 26, 1477–1493.
Woody, M. L., Kudinova, A. Y., McGeary, J. E., Knopik, V. S., Palmer, R. H. C., & Gibb, B. E. (2016). Influence of maternal depression on children’s brooding rumination: Moderation by CRHR1 TAT haplotype. Cognition and Emotion, 30, 302–314.
Acknowledgments
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Author Contributions
WM formulated the research question and data analysis plan, and developed the initial manuscript draft. MC conducted the data analyses and tabled the results, and contributed to writing the manuscript. LT contributed to shaping the research question and data analysis plan, and contributed to writing the manuscript. RS led the design and implementation of the larger study, and contributed to writing the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interests.
Funding
This study was supported by the National Institute on Alcohol Abuse and Alcoholism (Grant AA14702), the National Institute on Drug Abuse (Grant DA10815), and the National Institute of Mental Health (Grant MH49127).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Mason, W.A., Chmelka, M.B., Trudeau, L. et al. Gender Moderation of the Intergenerational Transmission and Stability of Depressive Symptoms from Early Adolescence to Early Adulthood. J Youth Adolescence 46, 248–260 (2017). https://doi.org/10.1007/s10964-016-0480-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-016-0480-8