
Abstract
Although recent research suggests that the proportion of the US population identifying as non-religious has been rapidly expanding over the course of the last decade, relatively little research has examined the implications of this development for health and well-being. This study uses data from a large representative survey study of religion and health in the adult US population (N = 3010) to examine group differences among religious group members (N = 2401) and three categories of non-religious individuals: atheists (N = 83), agnostics (N = 189), and those stating no religious preference (N = 329). MANCOVA was used to analyze group differences on five outcome dimensions, incorporating 27 outcome variables. Religious non-affiliates did not differ overall from affiliates in terms of physical health outcomes (although atheists and agnostics did have better health on some individual measures including BMI, number of chronic conditions, and physical limitations), but had worse positive psychological functioning characteristics, social support relationships, and health behaviors. On dimensions related to psychological well-being, atheists and agnostics tended to have worse outcomes than either those with religious affiliation or those with no religious preference. If current trends in the religious composition of the population continue, these results have implications for its future healthcare needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A growing body of evidence suggests that the proportion of the American population reporting that they are unaffiliated with any religious group has expanded rapidly in recent years (Gallup 2014; Kosmin and Keysar 2009; Pew Forum on Religion and Public Life 2012). Whereas a study by the Pew Forum on Religion and the Public Life (2015) found that only 16 % claimed no religious affiliation in 2007, by 2014 that number had grown to 23 %. Other research suggests that this trend is at least in part attributable to generational change, with members of recent birth cohorts substantially more likely to be unaffiliated than their older contemporaries (Kosmin and Keysar 2009; Pew Forum on Religion and Public Life 2012). Given that there is an extensive body of research attesting to the generally positive association between religious belonging and health outcomes (Koenig et al. 2012), these trends in affiliation and non-affiliation raise potentially important questions about potential changes in population health. To the extent that religiously uninvolved individuals lack certain social and psychological resources that help support health and well-being, secular sources of personal support (e.g., families) may play an even larger role as support systems, and other social institutions may face increasing demands. In this study, we take advantage of a large survey dataset representative of the US population to examine differences in a range of key health and well-being indicators in religiously affiliated and unaffiliated individuals. Moreover, our sample allows us to make comparisons among classes of religious non-affiliation. There may be important differences in the social and psychological characteristics of atheists, agnostics, and those who are simply not interested in religious issues that have implications for health and well-being.
Changes in Religious Non-affiliation
The question of whether or not religious involvement has declined at the societal level has as long and contentious history in the social sciences. Contrary to the expectations of secularization theory (Swatos and Christiano 1999), a large body of empirical evidence indicated that religious involvement in the US (and indeed in most of the world) remained fairly stable throughout the latter half of the twentieth century (Finke and Stark 2005; Gallup and Jones 1989; Presser and Chaves 2007). Analysis of historical sources suggests that this pattern of stability largely holds even in earlier eras (Finke and Stark 2005). More recently, this view has been significantly challenged by evidence of a relatively rapid and ongoing expansion of the non-religious population in the first decades of the twenty-first century (Gallup 2014; Kosmin and Keysar 2009; Pew Forum on Religion and Public Life 2012, 2015). Although the vast majority of the US population reports being affiliated with a particular religious group, the proportion reporting that they have no religious preference nearly doubled between 2007 and 2014 (Pew Forum on Religion and Public Life 2015). Studies that draw distinctions among categories of unaffiliated individuals show that not only are more people reporting no religious identification, but more are also identifying with specific non-religious philosophical orientations, such as atheist and agnostic (Kosmin and Keysar 2009; Pew Forum on Religion and Public Life 2012).
A noteworthy feature of these apparent changes is their relationship with age. It is the youngest cohorts that contain the greatest proportion of religiously unaffiliated individuals. Placing this in the context of generational change, this has been interpreted as evidence of a shift in values particularly among the “Millennial” generation (i.e., those born in approximately 1980 and later) (Pew Forum on Religion and Public Life 2010). This fact makes it difficult to predict how enduring these apparent changes will prove to be; there is compelling evidence for life course changes in religious involvement, with many individuals exhibiting a pattern of low interest in religion in young adulthood followed by an increasing interest in middle and especially in older adulthood (Hayward and Krause 2013a; Ingersoll-Dayton et al. 2002). Thus, we might expect that today’s religiously unaffiliated Millennials will change over time to more closely resemble today’s middle and older adults.
However, two factors may suggest that these differences are due to a genuine cohort effect between generations rather than to life course differences between age groups. First, repeated cross-sectional results indicate that non-affiliation has expanded across recent decades within the ranks of young adults; the current youngest cohort is more likely to be unaffiliated not only in comparison with older current cohorts, but also in comparison with the youngest cohort 10 years ago (Pew Forum on Religion and Public Life 2010). Second, previous life course research tended to find that although indicators of religiousness like frequency of participation in worship activities and subjective importance of religion tend to wane in young adulthood, young adults tended to continue to nominally identify with a religious tradition (Uecker et al. 2007; Willits and Crider 1989). Thus, there are reasons to take seriously the idea that there has been genuine change in the extent of religious affiliation in the US population, particularly among members of the youngest age cohorts.
Implications for Health
There is an exceptionally large and broad literature documenting the association between religious involvement and both mental and physical health outcomes (Koenig et al. 2012). Religious involvement is thought to have an impact on health via a number of pathways including integration in networks of social support (Krause 2006a), providing psychological tools for coping with stress (Pargament 1997), and by promoting self-control, which in turn leads to better health behavior (McCullough and Willoughby 2009). It is again important to make note of the ways in which age is relevant to this set of relationships. A number of studies indicate that religious involvement is especially influential in its relationship with health later in life (Krause 2006b). At the same stage in the life course when involvement in religious increases most rapidly (Hayward and Krause 2013a), its salutary association with health outcomes also reaches its peak (Krause 2006b). However, even in younger adulthood, religious involvement tends to be associated with predictors of good health, such as health behavior (Nagel and Sgoutas-Emch 2007), social support (Salsman et al. 2005), and psychological coping (Krause 2011).
Consequently, if there are enduring generational changes in religious involvement underway, the full extent of their implications for physical health will probably not be felt for decades, when the cohorts most affected reach older adulthood. Earlier impacts may arise for mental health (e.g., depression and anxiety) and well-being (e.g., life satisfaction, general happiness) outcomes, which are less prone to age-related deterioration. Religious involvement has also been related to a number of more specific factors ranging from health behaviors (such as alcohol consumption and smoking) (Afifi Soweid et al. 2004; Ellison et al. 2008; Hayward and Krause 2014) to elements of positive psychology (such as forgiveness and optimism) (Hayward and Krause 2013b; Krause and Hayward 2013; Lawler-Row 2010; Salsman et al. 2005) that may have important effects at early ages as well as cumulative health impacts across the life course. Mental and physical health problems do not only impact the individuals who suffer from them, but also have extensive familial and societal costs associated with providing care and loss of capacity contribute in other ways (e.g., Donohue and Pincus 2007; Hex et al. 2012). Therefore, it is valuable to be able to anticipate changes in demand for care that may arise at the population level in decades to come as the result of changes in patterns of religious non-affiliation.
An additional question which has received relatively little attention is the extent to which the type of non-affiliation an individual reports influences the health effects of noninvolvement. Non-affiliation may reflect either a lack of interest in religious matters or a definite set of beliefs skeptical to or opposing religious beliefs. Atheism has received a growing amount of attention in the literature, with the rise of the “New Atheist” movement as a highly visible and deliberately secular worldview promoted in opposition to religious involvement (Cimino and Smith 2011). It is possible that to the extent that this movement promotes some of the same psychological elements thought to mediate some of the benefits of religion on health (e.g., a sense of meaning, worldview defense, a sense of shared identity), it may fulfill at least some of the same functions and thus confer some of the same health benefits as religious involvement. However, there is also a strong body of evidence that atheism constitutes a highly stigmatized identity (Edgell et al. 2006; Gervais 2011), which may impede these positive effects (Friedman and Saroglou 2010).
Additionally, survey evidence indicates that self-described atheists constitute the smallest category of religious non-affiliation, with agnostics and those simply stating they have “no religious preference” making up the bulk of the unaffiliated population (Pew Forum on Religion and Public Life 2012). Agnostics may suffer with respect to mental and physical health outcomes because they may be prone to more existential uncertainty and lack of a stable worldview (Hogg et al. 2010; Vail et al. 2010) in comparison with either religiously affiliated individuals (who are likely to draw on religious worldviews) or atheists (who are likely to have more certainty in their non-religious worldviews). Individuals who report no religious preference without citing a specific non-religious orientation are more likely to simply have little interest in religious questions, although many of them are likely to attend religious services at least occasionally, and thus may obtain some of the benefits of religious belonging. Conversely, all categories of religiously unaffiliated individuals would seem to be likely to suffer in terms of social support (Krause 2006a) and positive social identity (Ysseldyk et al. 2010) that religious groups can provide their members. Finally, certain other positive psychological factors may be enhanced by non-religion in ways that may offset at least some of these potential losses. Some researchers have remarked that religious involvement may encourage the development of negative attributes such as intolerance and inflexibility (Allport and Ross 1967; Johnson et al. 2010), which may also contribute to mental health problems. Other potentially detrimental elements of religion include negative interaction with religious group members (Ellison et al. 2009) and religious doubt (Galek et al. 2007). Thus, the unaffiliated may benefit on these dimensions in comparison with those who belong to a religious group.
The Present Study
In the present study, we use new data on religion and health in the US population to explore differences in mental and physical health outcomes, as well as in some of their key precursors, among the religiously affiliated and three categories of non-affiliated individuals—atheists, agnostics, and those with no religious preferences (i.e., the “religious nones”). To our knowledge, this is the first study with a sufficient sample to examine group differences among categories of religiously unaffiliated individuals in this fashion. For the reasons outlined above, we anticipate that present direct effects on health outcomes will be relatively minor, but that more substantial differences will emerge with respect to social and psychological attributes that may have an impact on health across the life course.
Method
Data were collected as part of the Landmark Spirituality and Health Survey (LSHS). The LSHS recruited a representative sample of the adult US population and administered a survey instrument focused on religion and health outcomes. The sample was constructed using clustered random household sampling, with an oversampling of older adults. Sample weights were therefore applied to all analyses to correct for age stratification and sample effects. Sampling and data collection were conducted by NORC. Data collection was conducted via in-person interview in respondents’ homes. The sample included 3010 respondents (1312 men and 1698 women).
Measures
Except where otherwise noted, all scale item measures were assessed using a 5-point response scale from “strongly disagree” to “strongly agree” and higher scores indicate on each variable indicate higher levels of the corresponding attribute.
Religious Affiliation
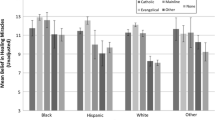
Participants responded to the question “at the present time, what is your religious preference,” with categorical responses presented by the interviewer on a Showcard. More than 80 religious preferences were recorded, which could be grouped as Catholic (21.4 %), Black Protestant (8.3 %), Evangelical Protestant (33.3 %), Mainline Protestant (10.6 %), Other (10.6 %), and None (20.0 %) using the classification system proposed by Steensland et al. (2000). For the purposes of this study, all specific religious group responses were combined into a single category representing any religious affiliation. Additional non-religious responses which were retained as individual categories were “no religious preference,” “agnostic (not sure if there is a God),” and “atheist (there is no God).”
Health Outcomes
Health factors assessed included subjective health, body mass index (BMI), chronic conditions, present symptoms of disease, and limitations activities of daily living (ADL). Subjective health was assessed with a three-item instrument including a self-rating of overall health (poor, fair, good, or excellent), and two items gauging health relative to others of a similar age to the respondent and to the respondent 1 year earlier (worse, about the same, or better). BMI was calculated based on interviewer-assessed height and weight. Number of chronic health conditions was assessed with a 14-item checklist (e.g., arthritis, hypertension). General symptoms of disease were assessed with an 11-item checklist (e.g., frequent cramps in legs, frequent headaches). ADL impairment was measured with a 15-item checklist of activities with which respondents reported having difficulty (e.g., bathing yourself, reaching over your head); because of the questionable applicability of these items to a young adult sample, only respondents aged 40 and older received this assessment.
Well-Being
Psychological well-being factors assessed included positive affect, happiness, life satisfaction, self-esteem, symptoms of depression, general anxiety, and death anxiety. Positive affect was assessed with a 5-item scale consisting of ratings of the extent to which respondents had experienced an affective state in the previous month (sample item: inspired) derived from the PANAS (Watson et al. 1988), α = 783. Composite happiness was assessed using a 3-item scale (sample item: In general I consider myself …) each with a 7-point response scale (sample anchors: not a very happy person … a very happy person) (Lyubomirsky and Lepper 1999), α = 828. Life satisfaction was assessed with a 3-item scale (sample item: the conditions of my life are excellent), α = 835. Self-esteem was assessed with a 3-item scale (sample item: I feel I am a person of worth, or at least on an equal plane with others) adapted from the Rosenberg Self-Esteem Scale (Rosenberg 1965), α = 722. Symptoms of depression in the past week were assessed using a 7-item version of the CES-D (Radloff 1977) (sample item: I felt that everything I did was an effort) with responses on a 4-point scale from “rarely/none of the time” to “most/all of the time,” α = 853. Symptoms of general anxiety in the past 2 weeks were assessed using a 7-item scale (example item: being so restless it is hard to sit still) with responses on a 4-point scale from “not at all” to “nearly every day,” α = 884. Death anxiety was measured using a 4-item scale (sample item: I find it hard to face up to the fact that I will die) (Neimeyer 1994), α = 838.
Positive Psychological Factors
Dimensions of positive psychology assessed included gratitude, optimism, meaning in life, humility, compassion, forgiveness of others, and forgiveness of self. Religious gratitude was also included in this study; however, it was not administered to those describing themselves as atheists. Gratitude was assessed with a 4-item scale (sample item: I have much in life to be thankful for) adapted from work by McCullough, Emmons, and Tsang (McCullough et al. 2002), α = 783. Optimism was assessed with a 4-item scale (sample item: In uncertain time, I usually expect the best) adapted from the Life Orientation Test (Scheier and Carver 1985), α = 772. Sense of meaning in life was assessed with a 6-item scale (sample item: I have a philosophy of life that helps me understand who I am) taken from the work of Krause (2004) α = 831. Humility was assessed with a 3-item scale (sample item: I know that I can learn from other people), α = 575. Compassion was assessed with a 5-item scale (sample item: when I see someone in a difficult situation I try to imagine how they feel), α = 737. Single items were used to assess both forgiveness of others (“I have forgiven those who hurt me”) and self (“I have forgiven myself for things I have done wrong”) on a 4-point response scale from “never” to “always or almost always.” Religious gratitude was assessed with a 3-item instrument (sample item: when I think of all the good in my life it makes me want to thank God), α = 937.
Social Support
Social factors assessed included total emotional support received from others, emotional support given to others, and sense of loneliness. Total emotional support received was measured with a 3-item scale (sample item: how often do your family members and friends let they know they love and care for you?) measured on a 4-point response scale from “never” to “very often,” α = 816. Total emotional support given to others was assessed using the same response scale, also with a 3-item scale (sample item: how often do you let your family members and friends know you love and care for them?), α = 820. Loneliness was assessed with a 3-item scale (sample item: how often do you feel left out?) with responses on a 3-point response scale from “hardly ever” to “often,” α = 759.
Health Behaviors
Measures of health behavior included smoking, alcohol use, illicit drug use, and exercise. A measure of smoking extent was computed from items asking whether respondents currently smoked cigarettes, and if so how many per day. Non-smokers were coded as zero, and smokers were coded according to the number of cigarettes they reported smoking each day. A similar approach was used to measuring alcohol use: nondrinkers were coded as 0, and for drinkers the average reported number of drinks per month was computed based on average reported frequency of drinking and average number of drinks consumed on each occasion. Illicit drug use was assessed using an inventory of reported lifetime problematic use 11 drugs (e.g., heroin, cocaine), and the variable was coded according to the number of different drugs respondents reported having used. Total exercise was determined by adding the reported frequency in terms of average days per week of moderate (e.g., fast walking, bicycling) and strenuous (e.g., jogging, soccer) exercise.
Results
Religious affiliation and non-affiliation data were available for 3002 of the full weighted sample of 3010 (<0.5 % missing). Of these, 2401 reported any religious affiliation (80.0 %), 83 were atheists (2.8 %), 189 were agnostics (6.3 %), and 329 reported no religious preference (11.0 %). Descriptive statistics for demographic factors within religious affiliation or non-affiliation category are reported in Table 1.
Significant differences among categories were detected for all of these variables, consistent with previous findings (Kosmin and Keysar 2009). The majority of members of the affiliated and no preference categories were women, whereas the majority of the atheist and agnostic groups were men (χ 2[3] = 26.89, p < .001). Atheists and agnostics had significantly higher average levels of education than those with any religious affiliation or no religious preference. Members of all three unaffiliated categories were younger on average than those with any religious affiliation, and among them, atheists and agnostics were younger on average than those with no preference. The atheist and agnostic categories contained a disproportionately large number of White individuals, whereas the affiliated and no preference categories contained disproportionately large numbers of Black and Hispanic individuals (χ 2[12] = 67.19, p < .001). Finally, regarding regional differences in religious affiliation and non-affiliation, atheists tended to come disproportionately from the west and northeast, agnostics disproportionately from the west, whereas the no preference and affiliated categories had disproportionate numbers from the south (χ 2[9] = 81.11, p < .001). A total of 85 cases (2.8 % of the sample) were missing data on at least one of these demographic factors.
Because of the large number of outcome measures examined in this study, related dimensions of outcomes were combined using MANCOVA, controlling for gender, age, education, race, and region. These dimensions correspond to physical health (subjective health, BMI, chronic conditions, disease symptoms, ADL), psychological well-being (positive affect, happiness, life satisfaction, self-esteem, depression, anxiety, and death anxiety), positive psychological traits (gratitude, optimism, meaning in life, humility, compassion, forgiveness of others, and forgiveness of self), social support (emotional support received, emotional support given, loneliness), and health behavior (smoking, alcohol use, illicit drug use, exercise). A summary of MANCOVA results for differences among the four religious affiliation categories is given in Table 2 (full model results and results for covariates are not shown).
Results for group differences are presented in Table 3 in the form of estimated marginal means (EMM) derived from models containing the categorical group affiliation or non-affiliation variable as well as controls for all of the background variables described above (gender, age, education, race, and region). Group differences in religious gratitude are summarized in table with those for the positive psychology dimensions for comparative purposes; because this instrument was not administered to self-identified atheists, including it in the corresponding MANCOVA analysis would have eliminated all members of the atheist category; hence, it is analyzed separately using a univariate model. General linear model analysis was used to derive EMMs for all outcome variables except for chronic conditions, present symptoms, ADL, smoking, alcohol, and illicit drug use, which were derived from generalized linear models for a Poisson distribution. Determination of which modeling strategy to use for each outcome was determined by screening the observed distributions of each variable (i.e., heavily right-skewed distributions representing counts). No significant group differences, as determined by non-overlap of 95 % confidence intervals, were detected for subjective health, positive affect, humility, illicit drug use, or exercise. Group differences were detected for all other variables.
In terms of health outcomes, individuals with any religious affiliation had significantly higher mean BMI, more mean ADL limitations, and reported suffering from more chronic conditions than atheists or agnostics. They also reported more symptoms of disease than those with no religious preference. On BMI and ADL, however, those with no preference more closely resembled affiliated individuals than members of the other unaffiliated groups; they did not differ from the affiliated group on BMI or ADL, but had significantly higher mean BMI than atheists and significantly more ADL limitations than either atheists or agnostics.
In terms of psychological well-being, the affiliated and no preference groups tended to fare better than either atheists or agnostics. Both of these groups reported better mean happiness, higher mean self-esteem, and lower mean anxiety in comparison with atheists and agnostics. Both groups also had significantly lower mean symptoms of depression in comparison with agnostics only. Affiliated individuals also had higher mean levels of life satisfaction and lower levels of death anxiety in comparison to agnostics.
In terms of positive psychology characteristics, a similar pattern held only for optimism; both affiliated individuals and those with no religious preference were more optimistic than either atheists or agnostics. The no preference group was intermediate between affiliated individuals on the one hand and atheists and agnostics on the other in terms of the sense of meaning in life; the affiliated group had the highest mean levels of meaning in life, with those with no preference having somewhat lower levels, and atheists and agnostics having lower levels still. Differences in gratitude followed a similar pattern, except that agnostics were neither significantly more grateful than atheists nor significantly less grateful than those with no preference. Similarly, affiliated individuals had the highest mean levels of specifically religious gratitude, with those having no religious preference scoring significantly lower, and agnostics significantly lower still (no data were collected on this measure from atheists). Conversely, affiliated individuals had higher levels of compassion than members of any of the other three non-affiliated groups. Affiliated individuals also were more forgiving of others than agnostics, and more forgiving of themselves than either atheists or agnostics.
In terms of social support relationships, those affiliated with a religious group reported both giving and receiving more mean emotional support than members of any of the three unaffiliated categories. They were also less lonely than agnostics.
Finally, in terms of health behavior, those with any religious affiliation engaged in less cigarette smoking than atheists or those with no religious preference. Alcohol use differed significantly between all groups: those with any religious affiliation drank the least on average, followed by agnostics, then by those with no religious preference, with atheists reporting the most drinking.
Discussion
Consistent with our predictions, and with previous research, these results indicated that there are differences between religiously affiliated and unaffiliated individuals on a broad spectrum of variables relevant to health and well-being. They also shed light on the relatively under-researched question of whether there are differences among different type of non-religious individuals on these health-related dimensions. One pattern of such differences emerged for a number of important variables—particularly on those related to physical health and psychological well-being—indicating that individuals with no religious preference were more similar to those having a religious affiliation than they were to atheists or agnostics. Individuals with either a religious affiliation or no religious preference fared worse in comparison with atheists and agnostics in terms of BMI and ADL impairment, but better in terms of happiness, self-esteem, depression, and anxiety. These two groups also appeared to benefit in terms of gratitude and optimism. Other differences—particularly those on dimensions of positive psychological traits and social support—appeared to be between the religiously affiliated and non-affiliated as a whole.
A striking finding was that, contrary to predictions, the overall multivariate results indicated no significant group differences in health outcomes, whereas the means estimates for its constituent elements indicated that individuals with religious affiliations tended to do somewhat worse in terms of some physical health outcomes than members of the non-affiliated groups. These differences emerged even after controlling for disparities that might be expected to arise due to age, gender, race, education, and region. One possible interpretation of these findings might be that people with more health problems are more likely to be motivated to become affiliated with a religious group as a means of coping and support. Alternatively, religious affiliates may be less likely to seek health care, perhaps due to a tendency to defer health-related control to God (Schieman 2008), or because of group-specific prohibitions in groups like Christian Scientists (Simpson 1989). The collection of longitudinal data on health and religious affiliation will be helpful in testing these hypotheses.
However, consistent with expectations, the same affiliated group appeared to do better in terms of psychological well-being, health behaviors, social relationships, and dimensions of positive psychological functioning. These differences are particularly remarkable in the context of the findings that atheists and agnostics in particular tend to fare better on certain key dimensions of physical health (obesity, presence of chronic conditions, and physical limitations). This fact would otherwise seem likely to reduce religious individuals’ well-being and opportunities to engage in social relationships in comparison with these relatively advantaged non-affiliates. These findings support previous evidence regarding some of the functional aspects of religious involvement. Psychological well-being effects may be indicative of the impact of psychological coping resources provided by religious beliefs (Pargament 1997). Health behaviors may be improved as a result of the social control exercised by specific tenets of religious belief (Ayers et al. 2009; Montgomery et al. 2007), or by more general self-control impacts of religion (McCullough and Willoughby 2009). Social benefits are likely to accrue due to the availability of support networks based in religious communities (Krause 2006a), in which both receiving and giving emotional support has been found to positively impact individuals’ health outcomes (Brown et al. 2003). The positive psychology impacts of religion are less fully researched and more contentious, but these findings may lend some support to the notion that religious groups can inculcate characteristics that have been termed “character virtues” (Krause and Hayward 2014).
As anticipated on the basis of other recent survey findings (Kosmin and Keysar 2009; Pew Forum on Religion and Public Life 2012, 2015), non-affiliation of all types was more prevalent among younger individuals. If suggestions that these differences are due in part to generational change rather than age effects, the findings of this study emphasize the risk of negative population-level changes as members of these generations enter later life stages more prone to health problems. Poorer psychological well-being, relative lack of certain positive psychology factors, lower levels of social support, and worse health behavior may have some potentially detrimental impacts on overall levels of health problems in the population. Although secular alternatives exist and may be capable of fulfilling equivalent social and psychological roles (Vail et al. 2010), the present findings suggest that their potential may not be fully realized in the population of individuals with no religious affiliation. It is possible that if non-religious orientations become more prevalent, some of these potential negative impacts will be attenuated (see e.g., Hayward and Elliott 2014 on the importance of religious norms), but this will become apparent only with repeated study over a period of years.
Limitations of this study include the cross-sectional nature of the data, which makes it impossible to determine whether well-being differences develop in response to religious non-affiliation, or whether people experiencing poor well-being outcomes exhibit different patterns of affiliation over time. This sample also does not allow us to distinguish between people who have left a religious group and those who never had a religious affiliation, which may have implications for well-being. Finally, the lack of ADL data for participants under the age of 40 limits the analysis of that variable.
As the religious composition of the population undergoes gradual but measurable change (Gallup 2014; Pew Forum on Religion and Public Life 2015), it is especially important to understand these shifts not only for their own sake, but also in order to anticipate their potential impacts on other important facets of society. These results are valuable in suggesting some of the ways in which these broad changes may impact individual health and well-being. They also emphasize the importance of disaggregating the “religious nones” to understand how different categories of religious non-affiliation may be affected in very different ways depending on how these orientations may serve to either compensate or exacerbate the missing functions of religious involvement. We hope that this paper will help provide a first step toward elucidating these issues.
References
Afifi Soweid, R. A., Khawaja, M., & Salem, M. T. (2004). Religious identity and smoking behavior among adolescents: Evidence from entering students at the American University of Beirut. Health Communication, 16, 47–62. doi:10.1207/S15327027HC1601_4.
Allport, G. W., & Ross, J. M. (1967). Personal religious orientation and prejudice. Journal of Personality and Social Psychology, 5, 432–443.
Ayers, J. W., Hofstetter, C. R., Hughes, S. C., Irvin, V. L., Sim, D. E. K., & Hovell, M. F. (2009). Exploring religious mechanisms for healthy alcohol use: Religious messages and drinking among Korean women in California. Journal of Studies on Alcohol and Drugs, 70, 890.
Brown, S. L., Nesse, R. M., Vinokur, A. D., & Smith, D. M. (2003). Providing social support may be more beneficial than receiving it: Results from a prospective study of mortality. Psychological Science, 14, 320–327. doi:10.1111/1467-9280.14461.
Cimino, R., & Smith, C. (2011). The new atheism and the formation of the imagined secularist community. Journal of Media and Religion, 10, 24–38. doi:10.1080/15348423.2011.549391.
Donohue, J., & Pincus, H. (2007). Reducing the societal burden of depression. PharmacoEconomics, 25, 7–24. doi:10.2165/00019053-200725010-00003.
Edgell, P., Gerteis, J., & Hartmann, D. (2006). Atheists as “other”: Moral boundaries and cultural membership in American society. American Sociological Review, 71, 211–234. doi:10.1177/000312240607100203.
Ellison, C. G., Barrett, J. B., & Moulton, B. E. (2008). Gender, marital status, and alcohol behavior: The neglected role of religion. Journal for the Scientific Study of Religion, 47, 660–677. doi:10.1111/j.1468-5906.2008.00434.x.
Ellison, C. G., Zhang, W., Krause, N., & Marcum, J. P. (2009). Does negative interaction in the church increase psychological distress? Longitudinal findings from the Presbyterian Panel Survey. Sociology of Religion, 70, 409–431. doi:10.1093/socrel/srp062.
Finke, R., & Stark, R. (2005). The churching of America, 1776-2005: Winners and losers in our religious economy. New Brunswick: Rutgers University Press.
Friedman, M., & Saroglou, V. (2010). Religiosity, psychological acculturation to the host culture, self-esteem and depressive symptoms among stigmatized and nonstigmatized religious immigrant groups in Western Europe. Basic and Applied Social Psychology, 32, 185–195. doi:10.1080/01973531003738387.
Galek, K., Krause, N., Ellison, C. G., Kudler, T., & Flannelly, K. (2007). Religious doubt and mental health across the lifespan. Journal of Adult Development, 14, 16–25. doi:10.1007/s10804-007-9027-2.
Gallup. (2014). Religion. Gallup. Retrieved from http://www.gallup.com/poll/1690/Religion.aspx.
Gallup, G., & Jones, S. (1989). 100 questions and answers: Religion in America. Princeton, NJ: Princeton Religion Research Center.
Gervais, W. M. (2011). Finding the faithless: Perceived atheist prevalence reduces anti-atheist prejudice. Personality and Social Psychology Bulletin, 37, 543–556. doi:10.1177/0146167211399583.
Hayward, R. D., & Elliott, M. (2014). Cross-national analysis of the influence of cultural norms and government restrictions on the relationship between religion and well-being. Review of Religious Research, 56, 23–43. doi:10.1007/s13644-013-0135-0.
Hayward, R. D., & Krause, N. (2013a). Patterns of change in religious service attendance across the life course: Evidence from a 34-year longitudinal study. Social Science Research, 42, 1480–1489. doi:10.1016/j.ssresearch.2013.06.010.
Hayward, R. D., & Krause, N. (2013b). Trajectories of change in dimensions of forgiveness among older adults and their association with religious commitment. Mental Health, Religion & Culture, 16, 643–659. doi:10.1080/13674676.2012.712955.
Hayward, R. D., & Krause, N. (2014). The effect of belonging to an alcohol-proscribing religious group on the relationship between moderate alcohol consumption and mortality. Social Science and Medicine, 101, 1–8. doi:10.1016/j.socscimed.2013.10.039.
Hex, N., Bartlett, C., Wright, D., Taylor, M., & Varley, D. (2012). Estimating the current and future costs of Type 1 and Type 2 diabetes in the UK, including direct health costs and indirect societal and productivity costs. Diabetic Medicine, 29, 855–862. doi:10.1111/j.1464-5491.2012.03698.x.
Hogg, M. A., Adelman, J. R., & Blagg, R. D. (2010). Religion in the face of uncertainty: An uncertainty-identity theory account of religiousness. Personality and Social Psychology Review, 14, 72–83. doi:10.1177/1088868309349692.
Ingersoll-Dayton, B., Krause, N., & Morgan, D. (2002). Religious trajectories and transitions over the life course. The International Journal of Aging and Human Development, 55, 51–70. doi:10.2190/297Q-MRMV-27TE-VLFK.
Johnson, M. K., Rowatt, W. C., & LaBouff, J. (2010). Priming Christian religious concepts increases racial prejudice. Social Psychological and Personality Science, 1, 119–126. doi:10.1177/1948550609357246.
Koenig, H. G., King, D. E., & Carson, V. B. (2012). Handbook of religion and health (2nd ed.). New York: Oxford University Press.
Kosmin, B. A., & Keysar, A. (2009). American nones: The profile of the no religion population. Hartford, CT: Institute for the Study of Secularism in Society and Culture. Retrieved from http://commons.trincoll.edu/aris/publications/2008-2/american-nones-the-profile-of-the-no-religion-population/.
Krause, N. (2004). Stressors arising in highly valued roles, meaning in life, and the physical health status of older adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 59, S287–S297. doi:10.1093/geronb/59.5.S287.
Krause, N. (2006a). Church-based social support and change in health over time. Review of Religious Research, 48, 125–140.
Krause, N. (2006b). Religion and health in late life. In J. E. Birren & K. W. Schaie (Eds.), Handbook of the psychology of aging (6th ed., pp. 499–518). New York: Elsevier Academic Press.
Krause, N. (2011). Stress, religious-based coping, and physical health. In A. J. Blasi (Ed.), Toward a sociological theory of religion and health (pp. 207–238). Boston: Brill.
Krause, N., & Hayward, R. D. (2013). God-mediated control and optimism: Exploring variations by denominational affiliation. Review of Religious Research, Advance online publication.,. doi:10.1007/s13644-013-0133-2.
Krause, N., & Hayward, R. D. (2014). Race, religion, and virtues. The International Journal for the Psychology of Religion,. doi:10.1080/10508619.2014.916591.
Lawler-Row, K. A. (2010). Forgiveness as a mediator of the religiosity—Health relationship. Psychology of Religion and Spirituality, 2, 1–16. doi:10.1037/a0017584.
Lyubomirsky, S., & Lepper, H. (1999). A measure of subjective happiness: Preliminary reliability and construct validation. Social Indicators Research, 46, 137–155. doi:10.1023/A:1006824100041.
McCullough, M. E., Emmons, R. A., & Tsang, J.-A. (2002). The grateful disposition: A conceptual and empirical topography. Journal of Personality and Social Psychology, 82, 112.
McCullough, M. E., & Willoughby, B. L. B. (2009). Religion, self-regulation, and self-control: Associations, explanations, and implications. Psychological Bulletin, 135, 69–93. doi:10.1037/a0014213.
Montgomery, S., Herring, P., Yancey, A., Beeson, L., Butler, T., Knutsen, S., et al. (2007). Comparing self-reported disease outcomes, diet, and lifestyles in a national cohort of Black and White Seventh-Day Adventists. Preventing Chronic Disease, 4, 1–14.
Nagel, E., & Sgoutas-Emch, S. (2007). The relationship between spirituality, health beliefs, and health behaviors in college students. Journal of Religion and Health, 46, 141–154. doi:10.1007/s10943-006-9088-8.
Neimeyer, R. A. (1994). Death anxiety handbook: Research, instrumentation, and application. Washington, DC: Taylor & Francis.
Pargament, K. I. (1997). The psychology of religion and coping: Theory, research, practice. New York: Guilford Press. Retrieved from http://mirlyn.lib.umich.edu/Record/003168667.
Pew Forum on Religion and Public Life. (2010). Religion among the Millennials. Washington, DC: Pew Research Center.
Pew Forum on Religion and Public Life. (2012). “Nones” on the rise: One-in-five adults have no religious affiliation. Washington, DC: Pew Research Center.
Pew Forum on Religion and Public Life. (2015). America’s changing religious landscape. Washington, DC: Pew Research Center.
Presser, S., & Chaves, M. (2007). Is religious service attendance declining? Journal for the Scientific Study of Religion, 46, 417–423. doi:10.1111/j.1468-5906.2007.00367.x.
Radloff, L. S. (1977). The CES-D scale. Applied Psychological Measurement, 1, 385–401. doi:10.1177/014662167700100306.
Rosenberg, M. (1965). Society and the adolescent child. Princeton, NJ: Princeton University Press.
Salsman, J. M., Brown, T. L., Brechting, E. H., & Carlson, C. R. (2005). The link between religion and spirituality and psychological adjustment: The mediating role of optimism and social support. Personality and Social Psychology Bulletin, 31, 522–535. doi:10.1177/0146167204271563.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219–247. doi:10.1037/0278-6133.4.3.219.
Schieman, S. (2008). The religious role and the sense of personal control. Sociology of Religion, 69, 273–296. doi:10.1093/socrel/69.3.273.
Simpson, W. F. (1989). Comparative longevity in a college cohort of Christian Scientists. JAMA, 262, 1657–1658. doi:10.1001/jama.1989.03430120111031.
Steensland, B., Park, J. Z., Regnerus, M. D., Robinson, L. D., Wilcox, W. B., & Woodberry, R. D. (2000). The measure of American religion: Toward improving the state of the art. Social Forces, 79, 291–318. doi:10.2307/2675572.
Swatos, W. H., & Christiano, K. J. (1999). Secularization theory: The course of a concept. Sociology of Religion, 60, 209–228. doi:10.2307/3711934.
Uecker, J. E., Regnerus, M. D., & Vaaler, M. L. (2007). Losing my religion: The social sources of religious decline in early adulthood. Social Forces, 85, 1667–1692. doi:10.1353/sof.2007.0083.
Vail, K. E., Rothschild, Z. K., Weise, D. R., Solomon, S., Pyszczynski, T., & Greenberg, J. (2010). A terror management analysis of the psychological functions of religion. Personality and Social Psychology Review, 14, 84–94. doi:10.1177/1088868309351165.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063.
Willits, F. K., & Crider, D. M. (1989). Church attendance and traditional religious beliefs in adolescence and young adulthood: A panel study. Review of Religious Research, 31, 68–81. doi:10.2307/3511025.
Ysseldyk, R., Matheson, K., & Anisman, H. (2010). Religiosity as identity: Toward an understanding of religion from a social identity perspective. Personality and Social Psychology Review, 14, 60–71. doi:10.1177/1088868309349693.
Acknowledgments
This work was supported by a Grant from the John Templeton Foundation (#40077).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hayward, R.D., Krause, N., Ironson, G. et al. Health and Well-Being Among the Non-religious: Atheists, Agnostics, and No Preference Compared with Religious Group Members. J Relig Health 55, 1024–1037 (2016). https://doi.org/10.1007/s10943-015-0179-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-015-0179-2