
Abstract
Purpose Many industrialised nations have systems of injury compensation and rehabilitation that are designed to support injury recovery and return to work. Despite their intention, there is now substantial evidence that injured people, employers and healthcare providers can experience those systems as difficult to navigate, and that this can affect injury recovery. This study sought to characterise the relationships and interactions occurring between actors in three Australian injury compensation systems, to identify the range of factors that impact on injury recovery, and the interactions and inter-relationships between these factors. Methods This study uses data collected directly from injured workers and their family members via qualitative interviews, analysed for major themes and interactions between themes, and then mapped to a system level model. Results Multiple factors across multiple system levels were reported by participants as influencing injury recovery. Factors at the level of the injured person’s immediate environment, the organisations and personnel involved in rehabilitation and compensation processes were more commonly cited than governmental or societal factors as influencing physical function, psychological function and work participation. Conclusions The study demonstrates that injury recovery is a complex process influenced by the decisions and actions of organisations and individuals operating across multiple levels of the compensation system. Changes occurring ‘upstream’, for instance at the level of governmental or organisational policy, can impact injury recovery through both direct and diffuse pathways.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Reducing the burden of work-related injury and illness, and enhancing the productivity and wellbeing of the working population, are major public health and social policy priorities. It has been estimated that there were 2.3 million deaths attributable to work in 2012 globally [1]. The direct cost to USA workers’ compensation systems of the ten most disabling working conditions amounted to $55 billion in 2011 [2]. In Australia it is estimated that approximately 242,000 people access financial support through workers’ compensation systems on an annual basis [3] with an economic cost of more than $60 billion [4].
Australia, like numerous other industrialised nations, has a complex legislative and policy architecture governing its systems of injury compensation and rehabilitation [5]. Typically, Australian injury systems task government regulatory authorities with the responsibility of facilitating post-injury recovery and return to work. These systems have substantial interactions with related healthcare, legal, financial and social welfare systems. Evidence about the impact of coordination between actors within the compensation system on effective injury recovery and return to work has been demonstrated at the level of systematic review [6].
Research to date has shown that recovery from injury is a complex process [7, 8]. There is also now compelling evidence that those receiving compensation for injury have difficulty navigating injury compensation processes [9, 10]. Other system actors including healthcare providers [11], employers [12] and case managers [8] are also challenged by complex system processes. Similar issues exist in nations with similar regulatory approaches to injury compensation as Australia such as Canada and the United States, as well as in those with quite different policy architecture to Australia such as the Netherlands, New Zealand and Sweden [10].
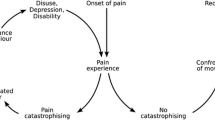
There is also an emerging evidence base regarding the interaction between actors in injury compensation systems [10, 11, 13,14,15]. These studies make it clear that injury recovery and other system performance measures such as costs of compensation and responsiveness to client needs, are influenced by the interactions between actors in the rehabilitation process, and that these actors relate to each other in dynamic and non-linear ways. For example Kilgour et al. [10] identified a cyclical set of interactions between injured workers, healthcare providers, insurance case managers and employers in workers’ compensation systems. Kilgour et al. identified that in some injured workers with complex health conditions, negative interactions contribute to poor recovery and return to work outcomes. These features of interaction, non-linearity and dynamism are hallmarks of complex adaptive systems [16].
In the field of occupational health and safety and injury prevention, systems based thinking has been applied to understand the complex factors involved in accidents and their interactions [17,18,19]. This thinking is underpinned by the idea that safety, and hence accidents, are emergent properties arising from interactions between multiple components across complex sociotechnical systems [19]. In this context, the behaviour of those at the front line of system operation (e.g. employees) is not considered the primary cause of accidents. Rather it is treated as a consequence of decisions and actions throughout all levels of the system. This thinking now represents an accepted approach to improving safety in complex adaptive systems.
A fundamental underpinning of complex systems theory is the concept of non-linearity, or that the behaviour of the system is greater than the sum of the behaviours of all of its parts. Systems are made up of many interacting components (‘agents’ or ‘actors’) that act and react with other agents in a local situational or environmental context. Although the interactions are local, wide ranging impacts can arise via the innate connectivity of the system, and the close coupling of agents within the system. The overall behaviour of a system thus emerges from the actions of individual agents within the system, their inter-relationships and their interactions with situational and environmental factors [20, 21]. Agents interact in a dynamic manner, with their actions and reactions changing continuously and in response to other agents. This ‘dynamic complexity’ is in addition to combinatorial complexity, which is an indication of the number of possible states, components, or interactions between agents within a given system. Actions occurring in one part of the system ripple out across other components of the system and can have multiplicative effects [20, 22].
Another important implication is that the adaptive nature of complex systems can lead to policy resistance [20], or the tendency for policy interventions to be overcome by the adaptation of the system to the intervention. Because emergent properties of systems are the result of relationships between agents, understanding these relationships and system interactions is critical to understanding emergence within a system, and thus to developing interventions that can achieve system performance objectives. It follows that interventions informed by such an understanding will be more likely to succeed than otherwise. Therefore effective injury recovery system design and management requires a nuanced understanding of the interactions between system agents (workers, insurers, employers, healthcare providers, lawyers etc) and their behavioural and other drivers.
One implication of complex systems theory is that reductionist approaches to policy or practice can have unintended consequences. There are numerous examples of this occurring in injury compensation and rehabilitation settings. Perhaps the most obvious is that engagement in compensation systems appears to delay recovery and return to work [9, 23]. Two hypotheses have been posed to explain this phenomenon. The secondary gain hypotheses that some injured workers are consciously, or unconsciously, incentivised to remain unwell. In contrast, the secondary victimisation hypotheses proposes that involvement in compensation processes can be stressful and aggravating, and that this gives rise to negative outcomes via renewed ‘victimisation’ of the injured person (in other words, the system is a cause of additional disability) [24]. These are not mutually exclusive phenomena. One interpretation of the secondary gain hypothesis has been that the injured person is overtly or deliberately malingering in order to gain financial benefit [25]. This interpretation represents the fundamental attribution error described by Sherman [20] as misperception of system feedback, in which we attribute negative outcomes to the nature or disposition of the individual rather than to situational or system level factors.
Systems thinking has also being applied to enhance our understanding of injury recovery within compensation and rehabilitation contexts. For example, Jetha et al. [26] developed a system dynamic model of return to work to examine how relationships between individual, psychosocial, and organizational factors comprise a work disability system and influence return to work outcomes. Implicit within such studies is the proposition that improving injury recovery and return to work outcomes requires an enhanced understanding of system dynamics, and how system level interactions affect the injured person.
In summary, system based approaches have substantial potential to inform models of injury recovery and rehabilitation. This study sought to characterise the relationships and interactions occurring between actors in three Australian injury compensation systems, to identify the range of factors that impact on injury recovery, and the interactions and inter-relationships between these factors.
Methods
This study uses data collected directly from injured workers and their family members via qualitative interviews, analysed for major themes and interactions between themes, and then mapped to a system level model. The study was approved by the Monash University Human Research Ethics Committee.
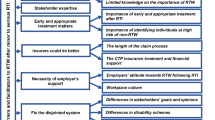
We sought to analyse and map interactions affecting recovery within the injury compensation system via the application of Rasmussen’s [18] Accimap risk management framework. The Accimap technique was developed to graphically represent how the conditions, decisions and actions of various actors within a given system interact with one another to create a safety critical incident or accident. The Accimap describes the system in question as comprising multiple levels that can be adapted to reflect the domain of interest. Factors at each of six descending levels, spanning social to individual factors are identified and linked together to represent the existence of any cause-effect relationships. The Accimap technique has been applied to represent large-scale organisational accidents in multiple domains [27] and to multiple incident analyses [17, 28]. In this study, the Accimap was adapted to represent the linkages and inter-dependencies within and across system levels in three Australian injury compensation and rehabilitation systems. Table 1 represents the modified AcciMap (herein referred to as a RecoveryMap).
There are now multiple systems modelling methods used in public health settings, including approaches such as Agent-Based Modelling, Systems Dynamic and Network Models. Although there is overlap, these methods approach the study of complex systems in different ways, and have different features. For a review of these approaches we refer the reader to Luke and Stamatakis [29]. These approaches differ from the AcciMap method as they are tools for modelling systems, whereas the AcciMap is a framework for visualising and understanding system interactions.
Data Sources
Data was collected from three Australian injury compensation schemes including the Victorian workers’ compensation system, the Victorian motor vehicle accident compensation scheme, and the commonwealth of Australia workers’ compensation scheme. An overview of each system is provided in Table 2.
Each compensation scheme provides access to a range of benefits including wage replacement, payments for healthcare and rehabilitation, lump sum payments for disability. These benefits are provided mainly on a no-fault basis. Healthcare is provided on the basis that it is ‘reasonable and necessary’. Wage replacement is provided as a percentage of pre-injury earnings and are time limited, with some exceptions for seriously injured persons. Schemes are regulated by government authorities, with the case management function either provided in-house within the regulators or out-sourced to private sector insurance companies. Insurance case managers perform essentially the same role within each system, including engaging with the injured person, their healthcare providers, employers and other actors to administer the workers compensation claims and assist recovery or return to work. Treatment and rehabilitation may be accessed via both public and private health care systems. In addition, persons who meet criteria for serious permanent impairment may be eligible to make a claim through the common law processes for pain and suffering and/or economic loss. In this respect, common law payments are another major area of expenditure for schemes.
Eligibility is determined on the basis of the injury “arising out of, or in the course of, any employment” for the two workers compensation schemes or on the basis of injury in a land-based transport accident in the case of the motor vehicle compensation scheme. There are substantial differences between schemes in policy and processes, which have been described elsewhere [5].
Data Collection
Individuals who had sustained a compensable injury were recruited using a purposive sampling technique. A representative of each compensation authority generated a list of claims stratified by injury type (physical or psychological) and by time since injury (< 12, > 12 months). The compensation authority then contacted these individuals to determine if they were willing to have their contact details provided to the research team. Contact details for those giving consent were then provided to the research team, who then made contact and sought consent to participate. Participation on part of injured clients was voluntary and the compensation authority was not advised of those injured persons participating in the study. All interviews were conducted independently by the research team, and study data were not provided to the compensation authority. Twenty-five injured people were approached by the research team and 17 consented to participate. This included six people from the commonwealth workers’ compensation scheme, five from the Victorian motor vehicle compensation scheme and six from Victorian workers’ compensation scheme. Injured people had experienced a range of compensable conditions that are commonly observed in Australian injury compensation systems including psychological injury, upper body musculoskeletal disorders, spinal cord injury, whiplash, and back pain. 14 of the 25 participants were female.
Interviews with family members of injured persons were also conducted. At the completion of each interview, the injured person was asked to forward project information to their family member, in the anticipation that the family member would be willing to participate in an interview. The family member was asked to contact the Monash research team directly if they were willing to participate in the interview. Eight family members, including spouses and children (18+), gave consent to participate in an interview. Summary information of participants is provided in Table 3.
All interviews were conducted in person over approximately 1 h. Interviews were recorded and transcribed. Any identifying information, including names of individuals or workplaces, was removed prior to data analysis to ensure anonymity and confidentiality.
An interview schedule was developed for interviews with injured persons and their family members. Questions were designed to probe experiences and interactions with other actors in the recovery process, including insurance case managers, employers and co-workers, healthcare providers, lawyers and family members. Questions were designed to reflect the core aspects of systems thinking including the assumptions of non-summativity, which means that the whole is greater than the sum of its parts; the assumption of homeostatis, which refers to the tendency for a system to maintain stability in the face of change; and the assumption of equifinality, which suggests that there are multiple paths the group can take to achieve its goals and there may be multiple goals that the group needs to address (refer to Appendix for example questions). The interview schedule was piloted with research team members and representatives in the compensation scheme to ensure clarity of questions and comprehensiveness. Informed consent was obtained from all individual participants included in the study.
Data Analysis
The interviews were analysed by two analysts using nVivo 10 (London, UK, 2012). Coding was conducted over five stages. First, two researchers identified the factors influencing recovery from injury, and the relationships between them, present within each interview. To be included, factors and relationships identified had to be explicitly stated rather than inferred. Second, the factors and relationships were aggregated using a thematic analysis approach (adapted from Braun and Clarke [30]). This involved descriptively coding responses into themes to develop a coding template. The coding template was hierarchically structured with two levels: the first level described the actor involved (e.g. the injured person, regulator); and the second level identified the specific factor or theme (e.g. pain, financial stress). For example, the statement “There was absolutely nothing. Even managers just looked at me weirdly. There were even periods where even the directors didn’t even say hello to me, they didn’t want to even acknowledge me” was coded as “Injured worker: Feeling isolated”.
Relationships between factors were also coded. For example, “well, we’ve always been a fairly close-knit family. Like, so, I don’t sit back and not do anything sort of thing, but now it’s up to me to do stuff” was coded as a relationship between “Injured work: physical limitations and pain” and “Family: physical support”. Third, two researchers reviewed the coding template to ensure the codes were distinct from each other. Disagreements were resolved through consensus discussion. Fourth, the data was then re-coded by two analysts using the final coding template to ensure reliability. Finally, the factors were classified according to the adapted RecoveryMap framework. Frequency counts representing the number of times each theme (i.e., referred to as factors) and relationships between factors appeared across the interviews were then calculated, and a RecoveryMap was constructed.
Construction of the RecoveryMap involved (1) constructing a list of all the factors and relationships identified via the qualitative interviews analysis; (2) where possible, combining factors into categories to simplify data presentation; and (3) visually depicting the factors and relationships on Rasmussen’s framework, including the inter-relationships and their reported direction. Some prior studies also represent the number of references to each factor in the interviews as part of the mapping diagram. To simplify visualisation we chose instead to include this data in Table 4.
Results
The outputs of the thematic analysis were integrated to develop an overall RecoveryMap of factors influencing recovery, as shown in Fig. 1. Table 4 presents a summary of the factors including the number and percentage of participants reporting each factor and the number of references made to each factor across the sample. The factors reported by injured persons and family members were consistent; that is, family members did not report any new or different factors affecting the recovery of the injured person than reported by the injured person themselves. Thus, their responses have not been separately reported.

RecoveryMap. The figure shows the factors reported by participants as affecting recovery and the interactions between factors. Arrows represent direction of relationships
Visualisation of the factors affecting recovery and inter-relationships between them using the RecoveryMap approach demonstrates clearly that injury recovery is a systems phenomenon. The map shows that factors across all levels of the system have an impact on injured worker outcomes such as physical function, psychological function and work participation. Further the map demonstrates a complex set of interactions across the different levels of the system. For example, at the Government level, the policy and actions of the compensation scheme regulator influences the workplace involvement in RTW and access to healthcare at the organisation level. In turn workplace involvement in RTW is affected by the supervisor’s competence in RTW and the quality and continuity of insurance case management, both factors at the management level. In the immediate environment, the injured person’s financial circumstances are influenced by a range of other factors at multiple levels, and in turn, influence the person’s family and social relationships, co-worker relationships and psychological function. Physical function is influenced by multiple factors including quality of healthcare, work participation, workplace involvement in RTW and the physical impact on the injury. In turn, this influences psychological function, work participation and family and social relationships.
Combined with the data in Table 4, the RecoveryMap provides insight into the relative strength or importance of different factors on the injured person outcomes. For example family and social relationships were referenced a total of 99 times across interviews, spanning 22 of 25 respondents. The RecoveryMap shows that the injured person’s family and social relationships are influenced by a range of factors at the immediate environment and injured person levels, and in turn influence the impact on the injured person’s physical function. Similarly, the actions, decisions and communication of the insurer were referenced on 99 occasions by 21 of the 25 respondents. The RecoveryMap shows that respondents identified insurer decisions as affecting their psychological function, medical assessments, and their personal financial circumstances, and in turn being influenced by the workplace supervisor’s competence in RTW.
Each of the levels presented in the RecoveryMap will be addressed in turn.
Societal Level
At the societal level two seriously injured people reported that societal attitudes to disability had impacted on their recovery, notably by public facilities not catering for people with limited mobility. More common at this level were reports that the economic climate and the business or employment cycle affected the injured person’s ability to find work or return to productive employment. Some respondents commented that their injury co-occurred with substantial changes at their workplace such as retrenchments occurring during the 2008 global financial crisis, and noted that this made return to work more difficult. The economic climate was noted as affecting the actions of the system regulator at the next (Government) level of the map.
Government Level
There were a smaller number of references to factors at the government level as being influential for injury recovery. The most commonly reported factors related to the policy and procedure of the injury compensation system regulator. These related predominantly to the compensation system rules around coverage of specific treatments or rates of income and wage replacement. Injured person respondents also noted the impact of legal system policy and procedure on recovery. This related mainly to legal processes during common law claims and the amount of time taken to engage in, and resolve, these claims. There were also a number of comments related to healthcare policy, mainly relating to in-patient hospital stays. There were multiple interactions between this level and other levels of the map, mainly arising from the policy and actions of the system regulator, but also via the operation of the legal system.
Organisation Level
A majority of participants reported that policies and procedures, and the decisions and actions of organisations involved in the rehabilitation process affected their recovery. Most common at this level were observations of the decisions and actions of insurers in managing the compensation claim. This included time taken to review and approve treatment and rehabilitation related to claims, decisions around approval of treatment and rehabilitation by the insurer, and the communication practices of insurers.
They organised for me to see a psychiatrist to help them write their report. So they could make a recommendation about whether the claim got accepted or not. That was really frustrating…. because I only had limited sick leave, and I was taking sick leave until such time as a claim got accepted….I said, well what am I supposed to do, you know, I can’t afford to be without pay. If I go back to the workplace I might be, like... the injury is exacerbated.
Issues associated with accessing healthcare services were also reported by a majority of respondents, including commentary on factors such as approval processes and procedures for treatment, costs of healthcare, and referral processes. There was also considerable reference to workplace involvement in injury recovery, including a mix of positive and negative factors including the role of RTW co-ordinators in the workplace, workplace policy and procedures with respect to RTW, and the negative impact on recovery of lack of contact with the workplace.
I know the psychologist did help, but I think the return coordinator made it so much easier, almost like a shoulder to cry on….She did make discussions with the management and after a while things seemed to sort of happen which I think was because of her.
At this level the workplace involvement in RTW, and the insurer actions and decisions, interacted with multiple other levels of the map. For example, the policy and actions of the regulator at the government level influenced the workplace involvement in RTW, which in turn influenced the physical workplace environment.
Management Level
Most participants reported that the quality of healthcare and the quality and continuity of case management as factors influencing recovery. With respect to healthcare, injured people reported as positive factors the alignment of the healthcare provider’s goals with those of the injured person, advocacy by the healthcare provider on behalf of the injured person, and the healthcare provider taking an active role in return to work. One participant with a work-related mental health condition reported goal alignment and advocacy as positive aspects of her interaction with both her doctor and rehabilitation provider.
I think because both of them... we were all working towards the same sort of goals all along. Both the rehab provider and my doctor sort of realised from the get go, that you know, going back to that workplace would not work, so the aim from the beginning was a different work place. Yeah and I just sort of felt like they were on my side.
Negative experiences with healthcare providers were also reported as adversely impacting recovery. Similarly, the quality and continuity of case management was considered to be an important factor in recovery. Participants reported that turnover of case managers negatively impacted recovery, and their perception that case managers were the gate- keepers to approval of treatment and rehabilitation. Communication between case managers and the injured worker was the most commonly reported factor, with positive communication considered to support recovery and vice versa.
Well I’ll tell you one really, really critical thing…When you lodge documents, or emails, or approval or acceptance or anything, you email it to a case manager. Now if you want to ring up a couple of days later to see if there’s any progress on that report, you don’t speak to that person, you speak to somebody else, they can’t access his email. So you’re in limbo. You don’t know what’s going on. So he’s said, they say, “Look, we’ll give him the message, we’ll call you back”. You might not get a phone call for a week. This went on the whole, all the way through.
Within the workplace, the direct line manager or supervisor was reported by the majority of respondents as playing an important role in recovery and return to work. Few respondents from the TAC scheme noted this role, with nearly all injured people from the two workers’ compensation systems identifying the supervisor’s role as important. Respondents identified communication practices within the workplace, recognition of their injury as legitimate and provision of work accommodations as positive experiences that facilitated recovery.
Over the course of that time, and they were all really fantastic. Oh she’ll need a work station, and oh she’ll need this and new headsets and all that sort of stuff. I’m quite sure I cost them a fortune, but they were great. In fact, my director had also been injured once before, and she said whatever it takes to make it easier for you to work, we’re going to do because that’s really important and we need to make sure you are okay to be working. We don’t want you in pain at work.
Negative experiences were also reported and included having the injured person’s concerns ignored and lack of communication.
Finally at this level, respondents discussed medico-legal processes such as independent medical examinations (IMEs) and engagement with legal practitioners during common law processes as factors affecting their recovery. Seven injured people reported IMEs as an event that affected their recovery and/or their access to system benefits such as healthcare and income. Around half of respondents reported that their engagement with lawyers, usually as part of a common law claim, affected their recovery. Specifically, clients commented on the alignment of legal practitioners’ goals with their own.
All of the factors reported in the management level had some degree of interaction with other levels of the map. For example the quality of healthcare was reported as affecting the person’s physical function and work participation directly, while the supervisor competence was reported as affecting the physical environment at work.
Immediate Environmental Context
Within the immediate environment, the person’s personal financial circumstances, their family and social relationships, co-worker relationship and the psychological impact of the injury were reported by most participants as factors contributing to injury recovery.
Twenty-two of the 25 participants described the importance of their personal financial circumstances on recovery. This included both examples of how access to financial support through employers, the insurer or family members had assisted with recovery, but also many examples of financial strain related to rehabilitation. This included examples of injured people using savings to fund treatment and rehabilitation while insurance claims were being adjudicated. For example, one injured person stated:
Umm …we spent a lot of our house deposit initially on the operation, we’ve got most of it back but yeah financially it definitely took a huge amount of money from us initially. We’ve got most of that back… but…that caused a fair amount of stress thinking that we were, you know, not going to be able to get the house now because of the operation.
The importance of relationships with family members, co-workers and friends in supporting recovery was commonly reported, as were the negative impacts of injury and the rehabilitation and compensation process on family members, notably children and spouses.
I reckon [injured person]’s circle of friends were also very supportive. They were there, you know he had these particular, very close-knit group of friends. There must have been maybe 7 or 8 of them, one is an ambulance officer, a couple of nurses, one is a doctor. That group really, really was a very strong influence in [injured person]’s and my life at that time because they were there alongside us, if you know what I mean.
Injured people reported that the psychological impacts of the injury had a substantial impact on their overall recovery. This included feeling uncertain about recovery, concerns about being ostracised or bullied at work, and for people with psychological conditions a concern that others, including employers and co-workers, may doubt the veracity of their ‘invisible injury’.
The physical environment at work and home was also reported as a factor impacting recovery. Home and work modifications that accommodated injury-related physical limitations were reported to facilitate return to usual activity.
Injured Person Level
Most participants reported the injured person’s participation in work, and their physical and psychological function as markers of injury recovery, and as factors affecting recovery. For example injured workers reported that returning to work was an important part of recovering from injury, and conversely that not being able to participate in work was detrimental to recovery. One injured person stated:
I can say that work provides not only income but it provides people with dignity of being self-sufficient and having a social network as well a working network, and what have you. We are now feeing quite isolated, and there is certainly a loss of self-esteem in not being gainfully employed. So that is another issue.
Conversely other workers reported that their physical or psychological function was an important factor in determining their ability to participate in rehabilitation and other activities that may assist recovery. For example one worker reported in relation to the feeling of persistent pain:
Yeah so I’ve pretty much just got to the point where I think I’ll just have to put up with it. Yeah, yeah. I don’t know where to go from here because it’s not..umm… it’s not worth all the pain going to the physio.
Some family members also reported physical and psychological function and pain as having an impact on participation in rehabilitation and recovery activity.
Discussion
This study identified a broad range of factors within injury compensation systems that affect recovery from injury. These factors occur across multiple levels of the compensation system, including the level of the injured person, their immediate environment at work and home, including the individuals and organisations with which the injured person interact, the system regulator and other related government authorities and even to a broad societal level. The study confirms that multiple actors involved in injury compensation systems play unique and important roles in recovery. Importantly, this study also supports the assertion that recovery from injury within an injury compensation system emerges from the complex interplay of factors involving multiple actors. The relationship between the factors, as represented in in the RecoveryMap indicates how actions, decisions or behaviours at one level of the system are connected with those at other system levels but that those connections are not always synergistic or direct. The RecoveryMap shows that changes occurring ‘upstream’, for example at the level of government or organisations, can affect injury recovery through both direct and diffuse pathways.
There is a diverse and growing literature on complex social systems that supports these findings. In the past two decades complex systems approaches has been applied to healthcare [21] and to other areas of social policy such as education [22], economics [31], urban planning [32] and the environment [33]. More recently, we have seen examples in return to work [26, 34]. These studies have identified some of the challenges that system complexity poses for policy makers in these settings. Complex systems theory holds that the performance of injury systems (say, in their ability to return injured workers to the workforce) is an emergent property of the numerous interconnected interactions between agents within the system. Efforts to improve performance succeed or fail based on the non-liner inter-dependencies of system actors, rather than on pressure for improved performance applied by an external party or by a single actor. The ‘control’ of complex systems tends to be highly dispersed and decentralised. Thus it will be very difficult for any single person or organisation to have a strong influence over system outcomes. The model of injury compensation schemes in many developed nations invests the ‘regulation’ of the system in a government authority. In reality, and as demonstrated in this study, there are many other actors with influential roles in injury recovery.
Support for this approach has been demonstrated in injury prevention. Systems thinking frameworks have been used successfully to identify safety interventions that can reduce incidents, injury and illness in the workplace. For example in a study of manual handling tasks in the transport and storage industry, Goode et al. [17] identified that policy and procedure, training programs, staffing levels and conflicts between safety and productivity were important factors contributing to manual handling related injury. The authors concluded that addressing these upstream, policy oriented factors would have a greater impact in preventing manual handling injury than initiatives focused on the individual worker. In a striking example, Hopkins [35] developed an AcciMap of a gas plant explosion in 1998 that killed two workers in the Victorian town of Longford. The analysis showed how factors that were removed from the accident sequence contributed to the explosion, such as changes within the company that owned the gas plant and the state government’s failure to ensure an alternative gas supply.
In these examples, systems approaches have been used to understand where to intervene or which levers are most influential in improving safety. In the same way, this approach can help us to understand where to focus injury recovery and rehabilitation interventions. In the present study, for instance, the majority of factors were reported at the management and immediate environment levels of the RecoveryMap. This suggests that interventions at these levels may be effective at improving recovery outcomes than interventions at the societal or government level. While further studies using alternate data sources are required to develop a more comprehensive understanding of the system of factors contributing injury recovery, this study does suggest that such an understanding will assist policy makers to identify potentially effective interventions.
There are now also sophisticated system modelling techniques that can provide substantial insight into the inter-relationships between factors affecting recovery, and that can be used to test the impact of interventions in simulated environments. Approaches such as agent-based modelling (ABM) provide useful tools for understanding the mechanisms behind injury events or safety phenomena, and testing them in simulated environments. For example Thompson et al. used ABM to investigate the policy and client management interventions on the performance of a motor-accident compensation system across health outcomes, satisfaction with services and financial viability [36]. Another technique known as System Dynamic Modeling was used by Jetha [26] to examine interactions between actors in a return to work process. The application of ABM, system dynamic and network modelling approaches in public health settings have been described by Luke and Stamatakis [29].
This study has several advantages and some limitations. Use of the Rasmussen risk management framework has enabled visualisation and understanding of the factors affecting injury recovery and their interactions. The framework has the capacity to represent the influence of factors across multiple system actors and across multiple system levels, enabling a more comprehensive understanding of the interaction between these actors and these different levels of the system. The RecoveryMap approach also provides the ability to integrate large quantities of information into a single visual ‘map’ of system function. The thematic data analysis underpinning the map followed robust qualitative analysis techniques that we have reported previously, and the sample was sufficiently diverse to ensure a broad cross section of injury, gender and experience was captured. The study also included participant information from three different injury compensation systems in Australia, enhancing the generalisability of the findings to similar no-fault, statutory benefits injury compensation systems such as those in place throughout Australia, in workers’ compensation in Canada and accident compensation in New Zealand.
The study is limited by its reliance on data from two sets of actors in the system. The use of personal perspectives may also be associated with some element of recall bias. Future studies would benefit from reporting system dynamics from the view of a broader range of actors including case managers, healthcare providers, employers and colleagues. This may provide a different view of system function and different emphasis on the importance of certain factors for injury recovery. Another limitation is the limited ability, using qualitative data to develop the Accimap, to understand the importance or magnitude of the relationship between actors. We describe counts of interactions consistent with the method by Goode and colleagues [17] however this provides limited information with respect to the relative importance of interactions. Finallywhilst we consider that the RecoveryMap conceptualisation of agents and the structure of their interaction demonstrates face validity, it should be currently be viewed as a ‘candidate’ structure, only [37] and a tool for insight rather than prediction or ‘numbers’ [38]. Regardless, we contend that even at this early stage, the RecoveryMap framework could be used by system managers or policy makers to assist in identifying areas of intervention more likely to have impact on client outcomes than others. Future work focused on converting this and/or similar models into more dynamic representations of relationships using system dynamics, agent-based modelling or similar complex systems tools as described above may provide further mechanistic and/or predictive insight.
Conclusion
This study demonstrates that injury recovery can be characterised as occurring within a complex system involving multiple actors at multiple levels. There are multiple factors across levels of the compensation system that affect the injured person’s recovery from injury. These factors interact in complex ways to exert a range of direct and diffuse influences on physical function, psychological function and work participation. The study confirms and extends related work describing return to work following injury in system dynamic models. The study applied an established system mapping technique to the injury compensation environment, providing unique information for system actors to understand the impact of their actions on injury recovery. Perhaps most importantly, the findings suggest the need to think differently about injury recovery, to move away from a deterministic and reductionist biomedical model of injury compensation to a holistic, connected and collaborative approach that recognises the influence of psychological and social factors on recovery, and the complex interplay between factors and system actors.
References
Takala J, Hamalainen P, Saarela KL, Yun LY, Manickam K, Jin TW, et al. Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hyg. 2014;11(5):326–337.
Liberty Mutual Research Institute for Safety. 2013 Liberty Mutual Workplace Safety Index. Liberty Mutual Research Institute for Safety, Boston. 2013. http://www.libertymutualgroup.com/researchinstitute. Accessed 18 Oct 2017.
Lane TJ, Collie A, Hassani-Mahmooei B. Work-related injury and illness in Australia, 2004 to 2014. What is the incidence of work-related conditions and their impact on time lost from work by state and territory, age, gender and injury type? Melbourne: Institute for Safety Compensation and Recovery Research; 2016. Report No. 118-0616-R02.
SafeWork Australia. The cost of work-related injury and illness for Australian employers, workers and the community: 2012-13. Canberra: Commonwealth of Australia; 2016.
Collie A, Lane TJ, Hassani-Mahmooei B, Thompson J, McLeod C. Does time off work after injury vary by jurisdiction? A comparative study of eight Australian workers’ compensation systems. BMJ Open. 2016;6(5):e010910.
Cullen KL, Irvin E, Collie A, Clay F, Gensby U, Jennings PA, et al. Effectiveness of workplace interventions in return-to-work for musculoskeletal, pain-related and mental health conditions: an update of the evidence and messages for practitioners. J Occup Rehabil. 2017;28(1):1–15.
Newnam S, Collie A, Vogel AP, Keleher H. The impacts of injury at the individual, community and societal levels: a systematic meta-review. Public Health. 2014;128(7):587–618.
Newnam S, Petersen A, Keleher H, Collie A, Vogel A, McClure R. Stuck in the middle: the emotional labours of case managers in the personal injury compensation system. Work 2016;55(2):347–357.
Harris I, Mulford J, Solomon M, van Gelder JM, Young J. Association between compensation status and outcome after surgery: a meta-analysis. JAMA 2005;293(13):1644–1652.
Kilgour E, Kosny A, McKenzie D, Collie A. Interactions between injured workers and insurers in workers’ compensation systems: a systematic review of qualitative research literature. J Occup Rehabil. 2015;25(1):160–181.
Brijnath B, Mazza D, Singh N, Kosny A, Ruseckaite R, Collie A. Mental health claims management and return to work: qualitative insights from Melbourne, Australia. J Occup Rehabil. 2014;24(4):766–776.
Kosny A, Brijnath B, Singh N, Allen A, Collie A, Ruseckaite R, et al. Uncomfortable bedfellows: employer perspectives on general practitioners’ role in the return to work process. Policy Pract Health Saf 2015;13(1):65–76.
Kilgour E, Kosny A, McKenzie D, Collie A. Healing or harming? Healthcare provider interactions with injured workers and insurers in workers’ compensation systems. J Occup Rehabil. 2015;25(1):220–239.
Brijnath B, Mazza D, Kosny A, Bunzli S, Singh N, Ruseckaite R, et al. Is clinician refusal to treat an emerging problem in injury compensation systems? BMJ Open. 2016;6(1):e009423.
Mazza D, Brijnath B, Singh N, Kosny A, Ruseckaite R, Collie A. General practitioners and sickness certification for injury in Australia. BMC Fam Pract. 2015;16(1):100. https://doi.org/10.1186/s12875-015-0307-9.
Anaf S, Drummond C, Sheppard LA. Combining case study research and systems theory as a heuristic model. Qual Health Res. 2007;17(10):1309–1315.
Goode N, Salmon PM, Lenne MG, Hillard P. Systems thinking applied to safety during manual handling tasks in the transport and storage industry. Accid Anal Prev. 2014;68:181–191.
Rasmussen J. Risk management in a dynamic society: a modelling problem. Saf Sci. 1997;27(2–3):183–213.
Leveson N. A new accident model for engineering safer systems. Saf Sci. 2004;42(4):237–270.
Sterman JD. Learning from evidence in a complex world. Am J Public Health. 2006;96(3):505–514.
Sturmberg JP, O’Halloran DM, Martin CM. People at the centre of complex adaptive health systems reform. Med J Aust. 2010;193(8):474–478.
Keshavarz N, Nutbeam D, Rowling L, Khavarpour F. Schools as social complex adaptive systems: a new way to understand the challenges of introducing the health promoting schools concept. Soc Sci Med. 2010;70(10):1467–1474.
Gabbe BJ, Cameron PA, Williamson OD, Edwards ER, Graves SE, Richardson MD. The relationship between compensable status and long-term patient outcomes following orthopaedic trauma. Med J Aust. 2007;187(1):14–17.
Beardwood BA, Kirsh B, Clark NJ. Victims twice over: perceptions and experiences of injured workers. Qual Health Res. 2005;15(1):30–48.
Akkermans AJ. Reforming personal injury claims settlement: paying more attention to emotional dimension promotes victim recovery. 2009. http://ssrn.com/abstract=1333214. Accessed 26 Feb 2009.
Jetha A, Pransky G, Fish J, Hettinger LJ. Return-to-work within a complex and dynamic organizational work disability system. J Occup Rehabil. 2016;26(3):276–285.
Salmon PM, Read GJM, Stanton NA, Lenne MG. The crash at Kerang: investigating systemic and psychological factors leading to unintentional non-compliance at rail level crossings. Accid Anal Prev. 2013;50:1278–1288.
Newnam S, Goode N, Salmon P, Stevenson M. Reforming the road freight transportation system using systems thinking: an investigation of Coronial inquests in Australia. Accid Anal Prev. 2017;101:28–36.
Luke DA, Stamatakis KA. Systems science methods in public health: dynamics, networks, and agents. Annu Rev Public Health. 2012;33:357–376. https://doi.org/10.1146/annurev-publhealth-031210-101222.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Wang W, Chen Y, Huang JP. Heterogeneous preferences, decision-making capacity, and phase transitions in a complex adaptive system. Proc Natl Acad Sci USA. 2009;106(21):8423–8428.
Glouberman S, Gemar M, Campsie P, Miller G, Armstrong J, Newman C, et al. A framework for improving health in cities: a discussion paper. J Urban Health. 2006;83(2):325–338.
Olsson P, Folke C, Berkes F. Adaptive comanagement for building resilience in social-ecological systems. Environ Manag. 2004;34(1):75–90.
Jetha A, Pransky G, Hettinger LJ. Capturing complexity in work disability research: application of system dynamics modeling methodology. Disabil Rehabil. 2016;38(2):189–194.
Hopkins A. Lessons from Longford: the ESSO gas plant explosion. Sydney: CCH Australia Ltd; 2000.
Thompson J, McClure R, DeSilva A. A complex systems approach for understanding the effect of policy and management interventions on health system performance. Conference of the Computational Social Science of the Americas; Santa Fe: ACM; 2017.
Epstein JM. Generative social science: studies in agent-based computational modeling. Princeton: Princeton University Press; 2006.
Nikolic I, van Dam KH, Kasmire J. Practice. In: van Dam K, Nikolic I, Lukszo Z, editors. Agent-based modelling of socio-technical systems. Dordrecht: Springer; 2013.
Acknowledgements
This study was funded by WorkSafe Victoria, the Transport Accident Commission, Comcare and the Australian Research Council (ARC) via an ARC Industry Linkage Grant to the first author (Grant #LP11020019). The authors would like to acknowledge Ms Amy Allen for her contributions to data analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures were in accordance with institutional ethical standards and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Monash University Human Research Ethics Committee.
Appendix: Example Questions
Appendix: Example Questions
Non-summativity
Tell me about your experiences dealing with your case manager following your injury….were they helpful and in what ways?
Homeostatis
Did your relationship with the case manager change over the course of your recovery? If so, how?
Equfinality
What do you think the case managers wanted to achieve during this process?
Rights and permissions
About this article

Cite this article
Collie, A., Newnam, S., Keleher, H. et al. Recovery Within Injury Compensation Schemes: A System Mapping Study. J Occup Rehabil 29, 52–63 (2019). https://doi.org/10.1007/s10926-018-9764-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-018-9764-z