
Abstract
Refugees encounter numerous healthcare access barriers in host countries, leading to lower utilization rates and poorer health outcomes. In the US, social inequities and fragmented health systems may exacerbate these disparities. Understanding these factors is necessary to ensure equitable care of refugee populations. A systematic literature review of qualitative studies on US adult refugee healthcare access from January 2000 to June 2021 was performed in accordance with PRISMA. Studies were analyzed deductively and then inductively to incorporate previous findings in other resettlement countries and emergence of US-specific themes. 64 articles representing 16+ countries of origin emerged from the final analysis, yielding nine interrelated themes related to health literacy, cost of services, cultural beliefs, and social supports, among others. The main challenges to refugees’ healthcare access emerge from the interactions of care fragmentation with adverse social determinants. Given diverse barriers, integrated care models are recommended in treating refugee populations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In 2021, a combination of persecution, conflict, violence, and human rights violations displaced over 84 million individuals worldwide. This number represents a new all-time high, having increased by 2 million from the year prior and by 18.4 million since 2016 [1, 2]. These displacements have led to an increased number of refugees and asylees worldwide. The US in particular has admitted over 3 million refugees and asylees since 1975, and is anticipated to receive at least an additional 170,000 by the end of 2022 [3]. As defined under US law, a refugee is a person “outside any country in which such person last habitually resided, and who is unable or unwilling to return to, and is unable or unwilling to avail himself or herself of the protection of, that country because of persecution or a well-founded fear of persecution on account of race, religion, nationality, membership in a particular social group, or political opinion”, [4]. Asylees are defined as those who meet the definition of a refugee but are already present in the US or seeking admission at a point of entry. Given both the increasing number of refugees and asylees (hereafter, “refugees”) who are resettling or have already resettled in the US, it is imperative to understand their healthcare needs and experiences both upon arrival and over time.
Many refugees arriving to the US experience a higher disease burden than the general population due to the cumulative physical and psychological trauma of their migration journeys [5,6,7]. Refugees have been documented to arrive in host countries such as the US with high incidence of tuberculosis, gastrointestinal parasites, and chronic hepatitis B infection [8,9,10,11,12,13,14]. In addition to these common communicable diseases associated with the displacement process and under-resourced conditions of refugee camps, studies have shown that refugees additionally have high rates of mental health conditions and other chronic non-communicable diseases (NCD) upon arrival [15,16,17,18]. One particular study assessing recent arrivals in the Northeast US found that half of adult refugees had at least one NCD and one in five adult refugees had more than one NCD [15]. Further, refugee populations have been found to experience adverse health outcomes with a longer duration of stay in host countries. In the US, one study found that for each additional year post-resettlement, refugees had an estimated 12% increased odds of diabetes mellitus and 7% increased odds of hypertension [19]. The progression of NCDs in refugees is influenced by reduced healthy food intake, a more sedentary lifestyle, limited English proficiency, and reduced access to healthcare [19]. Refugees in the US thus experience greater disease burden not only upon arrival but over time as a result of an interplay among multiple factors.
Social determinants of health are defined by the World Health Organization and the US Department of Health and Human Services as non-medical factors, including conditions in the environments where people are born, live, learn, work, play, worship, and age, that influence health, functioning, and quality-of-life outcomes and risks [20, 21]. A lack of access to healthcare interacting with broader poor social determinants of health are the main drivers of both initial health disparities as well as the emergence of new health disparities for US refugee populations. Healthcare access and other social determinants of health, however, are both shaped by a multiplicity of factors. As we begin to better understand the challenges around these factors for refugees in the US, there is a need to synthesize this knowledge to create a strong foundation for intervention. We thus conducted a systematic review of the literature to assess factors affecting US adult refugee healthcare access and utilization across various countries of origin, resettlement areas, and other identities which intersect with the refugee identity. To our knowledge, this is the first review addressing this specific topic. Healthcare professionals, resettlement agencies, policymakers, and other relevant stakeholders should better understand these factors and their interactions not only to better prepare for the large number of new refugees who will need to access healthcare within US health systems, but to also ensure equitable care of this growing population over time.
Methods
Search terms and strategies were devised for five topical areas: refugees/asylees, adults, health/disease, access/barriers/social determinants, and United States. The resulting systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22].
Literature Databases and Search Strategies
A medical librarian (A.D.) conducted systematic searches using both text words and controlled vocabularies (e.g., Medical Subject Headings) in relevant bibliographic databases on March 11, 2021, with an update on June 25, 2021. A core search strategy was adapted for each database: Medline/PubMed, Wiley Cochrane Library, CINAHL with Full Text, PsycINFO, Web of Science Core Collection, and Academic Search Complete. The librarian also conducted a manual search of Google Scholar and hand searched the references of selected papers. Complete search strategies for each database can be found in Table 2 in “Appendix”.
Inclusion and Exclusion Criteria
All searches were limited to articles written since 2000, and in English. To be included in the review, articles had to describe studies of adult refugee participants in the United States, and address research questions related to barriers and facilitators to health services. Studies were excluded if: participants were under age 18; were focused on students or healthcare professionals’ knowledge of refugee healthcare/curricula/educational outcomes; were interventions; or with an objective not related to facilitators and barriers to health or health services. We also excluded studies addressing mental health, as there are several recent systematic reviews that have explored refugees’ barriers and facilitators to accessing and utilizing mental health services [17, 23,24,25,26,27]. Due to the volume of studies conducted on barriers and facilitators to refugee health services, we restricted this review to qualitative studies, which offer rich sources of contextual data and can help illuminate specific examples of barriers and how refugees experience their impact. By foregrounding lived experiences of refugees in their own words (from a refugee perspective), qualitative studies also allow us to develop initial understandings on factors which can inform future quantitative reviews. In terms of sequential mixed methods understanding, starting with a qualitative review also ensures that a full range of factors are being included.
Data Screening
Database search results were imported into reference management software (EndNote X9.2), and de-duplicated [28]. Records were imported into a second reference management software (Zotero) for title and abstract screening. Records were screened in three stages. First, one team member (A.D.) reviewed titles of all imported results and removed any studies meeting exclusion criteria. A second round of screening involved reviewing titles and abstracts of remaining records to remove studies that were not excluded based on title, but met exclusion criteria. Two independent raters (C.H. and N.S.) performed this second round of screening by first confirming inter-rater reliability by independently screening the same set of ten articles and aligning on results. A final full-text screening was performed by five team members (N.S., C.H., S.B., A.D., K.M.) after the whole team went over five articles together to ensure interrater reliability. During the full-text review, studies were assessed for quality using the Critical Skills Appraisal Programme (CASP) Qualitative Studies Checklist [29]. Only studies meeting criteria for high quality (score of ≥ 8) were included. The most common reasons for excluding articles in the final round of screening were that the objective/research question did not relate directly to health services, which was not clear just from reading the abstract, and the paper not meeting quality assessment standards.
Data Extraction
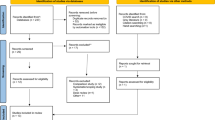
Using a standardized form, the team extracted the following study information from the final, included articles: country of origin/ethnic group of participants, study design and setting, sample size, gender of participants, age group of participants, and objective/research questions. Types of barriers and facilitators noted in previous reviews [30,31,32,33] were used to guide the extraction process through a deductive process. The team also used an inductive approach to identify additional themes or modify themes from the guiding framework. For each article, researchers indicated the types of barriers and/or facilitators that were mentioned and provided a summary of the context and the findings. After the full-text extraction process was complete, one team member (C.H.) reviewed all extraction forms, merged feedback and created the final thematic categories which were reviewed by the team. Initial searches yielded 7,851 records, of which 3,612 were unique. Of these, 140 records were retained after title and abstract screening. After full-text review, 64 articles were included. See Fig. 1 for the PRISMA Flow Diagram.

PRISMA Flow Diagram
Results
Demographic Characteristics of Sample
Sixty-four articles were included in the final analysis upon meeting inclusion and quality criteria [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97]. Details about each can be found in Table 1. 58 unique first authors were identified among the 64 final included articles. The publication dates for the final included studies range from 2003 to 2021, with twice as many publications from 2012 to 2021 (n = 44) as there were from 2003 to 2011 (n = 21) (Fig. 2). All studies were published across 41 unique peer-reviewed journals. Refer to Table 1 for more publication information.

Publication dates for final included studies
Publications included either focus on a singular country of origin (n = 38) or multiple countries of origin within their analysis (n = 26). Over 30 countries of origin were represented in our analysis, including representation from Eastern Europe (e.g., Russia, Bosnia, Turkey), Asia (e.g., Burma, Hmong, Vietnam), Central America (e.g., Mexico, Costa Rica), South America (e.g., Colombia), Africa (e.g., Egypt, Somalia, Ethiopia), and the Middle East (e.g., Iraq, Iran, Syria). Among all countries, the three most common refugee groups mentioned were Somali (n = 34), Bhutanese (n = 9), and Iraqi (n = 9).
The main methodologies commonly used were community-based participatory research (n = 24) [34, 38, 41, 42, 47, 48, 50,51,52,53, 55, 57, 61, 64, 65, 71, 73, 77, 79, 80, 87, 90, 93, 97] and ethnography (n = 9) [40, 45, 62, 67, 72, 73, 84, 88, 92]. One study [82] reported using a hermeneutic approach to qualitative research whereas the remainder did not specify the type of qualitative research approach. The main methods used among the studies included interviews (e.g., semi-structured, in-depth) (n = 19) [38, 43, 44, 47, 49, 51, 53, 58, 60, 62, 64, 73, 74, 76, 82, 85, 86, 88, 96] and focus groups (n = 16) [35, 36, 50, 54, 57, 68, 70, 75, 77, 81, 83, 84, 93,94,95, 97]. It was common for studies to employ a combination of these methods (n = 10) [34, 35, 37, 39, 42, 52, 65, 87, 89, 91] in addition to surveys (n = 4) [56, 59, 61, 69] and participant observation (n = 9) [40, 45, 48, 67, 71, 72, 79, 90, 92] Two studies also included use of artifacts (cultural or health literacy materials) to supplement participant data collection.
Many studies included key informants aside from refugees themselves (n = 20) [37, 40, 45, 46, 55, 56, 67, 72, 73, 76, 78,79,80,81, 88, 90,91,92,93, 96]. Key informants included family or neighbors (n = 2) [45, 88], healthcare professionals or other healthcare-related staff including interpreters (n = 12) [37, 40, 55, 56, 67, 72, 76, 80, 81, 90,91,92] and service providers (a broad category encompassing representatives from resettlement agencies or other organizations serving refugees, n = 16) [46, 55, 56, 67, 72, 73, 76, 78,79,80,81, 90, 92, 93, 96]. The majority of studies were conducted in the primary care setting (n = 43), though some were conducted in areas of practice such as women's health and reproductive medicine (n = 14) [34,35,36, 42, 43, 50, 55, 56, 62, 70, 84, 89, 94, 97] or at refugee or resettlement focused care centers (n = 7) [37, 58, 85, 86, 91, 95, 96].
When age was reported in publications, either the range of ages (n = 41) or the mean age (n = 5) was reported. Seventeen papers, however, did not specify the ages, instead stating that participants were over the age of 18 and categorized as adults [38, 40, 40, 50, 51, 53, 55, 62, 63, 69, 73, 75, 79, 83, 90, 93, 95]. Three of the articles had explicit focus on young adults, defining the range as either 18–25 [65, 66] or 18–30 years old [61]. In comparison, five articles focused explicitly on older adults [48, 49, 75, 88, 92]. Of those articles, three articles referred to elderly refugees as over 50 years old [48, 49, 88], whereas one article referred to elderly refugees as over 65 years old [92]. Another article did not provide age criteria for “elderly” [75].
Twenty-nine studies included both men and women, two studies focused solely on men [62, 64], 29 studies focused solely on women [34,35,36, 42,43,44, 47, 50, 52, 54,55,56, 59, 63, 68, 70, 77, 80, 82,83,84,85,86,87,88,89, 91, 94, 97] and three studies did not provide the gender composition of their participants [46, 92, 93]. One study with only male participants focused on sexual and reproductive health in terms of assessing infertility care [62] whereas the other focused on family planning in terms of the men’s views on women’s pregnancy-related health [64]. Of the articles focused on only women, five were specific to experiences with sexual and reproductive health [34, 47, 56, 70, 91], five to family planning [35, 47, 84, 89, 97], and ten to preventative cancer screenings (e.g., breast, cervical, colorectal) [50, 54, 55, 59, 68, 83, 86,87,88]. The six remaining articles with only female participants were focused on analyzing their general healthcare practices and preferences [43, 44, 77, 80, 82, 94].
In addition to focusing on the refugee identity, four studies explicitly explored intersecting identities of disability [72, 73], gender identity [46], and religion [52, 53]. Several other studies focused on refugees with specific diagnoses such as having multiple chronic conditions [92], HIV/AIDS [79], and type 2 diabetes mellitus [81]. Other studies focused on refugees who were currently pregnant [47], those with children [36], and those who were married [56]. These identities within broader refugee identity may further shape refugees’ unique experiences. Further, of the studies which reported time of immigration, five studies focused on new or recent arrivals [37, 57, 74, 95, 96], whereas only one study focused on refugees who have been resettled for at least 4 years [48].
Study Results
Our inductive analysis led to the finding of nine interrelated main themes related to refugee healthcare access: financial affordability of health services, health literacy, understanding of the healthcare system, perception of healthcare service and quality, medical (mis)trust, cultural and religious factors, transportation, use of social support networks, and immigration status.
Financial Affordability of Health Services
This theme is defined as factors affecting the ability to pay for services, including access to insurance or out-of-pocket funds. Access to healthcare for refugees was largely dependent on access to insurance, which was often reported to be expensive and difficult to navigate [41, 44, 51, 59, 61, 67, 68, 74, 76, 90, 95, 96]. Despite some refugees qualifying for public assistance, a lack of awareness of such resources along with difficulty enrolling due to challenges understanding and filling out the paperwork were barriers to affording health services [65, 67, 74, 90]. Employment also played a meaningful role in refugees’ ability to financially access health services. Not only did studies find that employment impacted refugees’ access to employment-based insurance, but it also impacted their ability to afford out-of-pocket medical expenses on top of other financial priorities [61, 76]. Inability to pay was a key contributor to the decision of not seeking medical care or turning down treatment [37, 48, 61, 62, 65, 68]. Availability of publicly funded health insurance like Medicare and Medicaid, charity care, and other financing options expanded healthcare access and was viewed favorably in addition to policies which enabled care before payment [39, 44, 49, 67, 74, 75, 95].
Health Literacy
Health literacy is defined as factors affecting the ability to obtain, read, understand, and use healthcare information to make health- and treatment-related decisions. Multiple studies indicated that a lack of interpreters in clinical and pharmaceutical settings negatively influenced health literacy, leading to barriers accessing information, understanding when and how to take medication, and scheduling appointments or obtaining refills [41, 45, 67, 69, 91, 96]. When interpreters were available, under qualification of such interpretation services and worries around potential privacy issues associated with community interpreters were noted to reduce refugees’ usage of such services [40, 41, 94]. Limited knowledge about certain diseases (e.g., cervical cancer, tuberculosis, HPV) also led to both limited awareness and testing, but also led to misconceptions about disease origins [36, 43, 50, 65, 93]. Two studies additionally found that limited understanding of acute versus chronic disease treatment differences led to lack of adherence because patients were unable to understand why certain treatments were not curative or required ongoing use of medications despite symptoms no longer being present [39, 60]. Although home healthcare services and resettlement resources were seen as essential for improving health literacy, a few studies noted that resettlement agencies often were overburdened and underfunded, leading to inadequate assistance and failure to identify prior disability-related or other health needs [59, 71,72,73, 89, 96].
Understanding of the Healthcare System
Understanding of the healthcare system is defined as factors related to the ability of refugee patients to navigate healthcare system processes and services as it pertains to knowledge possessed about such processes and services. Unfamiliarity with the American healthcare culture and practices as well as lack of previous exposure to preventative care and certain services (e.g., HIV services, prenatal care) in home countries led to difficulty navigating the healthcare system, as stated across multiple studies [44, 54, 64, 68, 78, 80, 87, 95]. The complexity of the US healthcare payment system as well as the need to book appointments in advance and receiving care at multiple facilities further contributed to navigation difficulties [39, 41, 67, 90, 96]. Community health workers and caseworkers, however, were seen as facilitating navigation by helping to book appointments and enrolling clients in insurance programs [74].
Perception of Healthcare Service and Quality
Influenced in large part by refugees’ personal experiences with healthcare systems from their origin countries and in host countries such as the US, perception of healthcare service and quality are factors affecting how refugees view the effectiveness and general quality of healthcare services. Several studies found that expectations of US healthcare before arrival to the US conflicted with actual healthcare experiences, often leading to decreased perceived quality of care [42, 69, 76, 91]. Lengthy wait times for appointments and delays in care, for example, were associated with decreased perceived quality of healthcare services [83, 92, 95]. Multiple studies also noted that the brevity of time spent with doctors also led refugees to believe that doctors were not listening and were being quick to resort to intrusive interventions, such as with the labor and delivery process [42, 69, 71, 80]. One study in particular noted how refugees saw high costs for health services as being the cause behind impersonal visits, and felt the priority was more related to business than providing quality care [37]. Unfriendly staff in addition to impatience or visible frustration by clinicians or staff due to language barriers further negatively shaped refugees’ healthcare experiences [44, 50]. Another study found that some refugees believed that they were receiving poorer quality of care due to being on public health insurance [92, 95]. Constant cycling of doctors and interpreters also negatively impacted refugees’ perception of healthcare quality due to increased concerns over privacy and decreased trust [43, 46, 78]. A lack of healthcare professionals’ understanding of patients’ culture and cultural practices alongside inadequate explanation of testing requirements by healthcare professionals led to decreased quality of care. Meanwhile, patient advocacy and adequacy of explanation by providers regarding care plans were reported to positively influence perceived quality of care [39, 41, 69, 78, 86]. Other positive influences on perceived quality of care included increased availability of quality medical equipment and medicines [48, 85].
Medical (Mis)Trust
The theme of medical (mis)trust includes factors influencing the confidence or lack of trust in medical professionals and/or medical systems that could alter perception of healthcare quality. Perceived and experienced discrimination and stereotyping based on race and ethnicity by healthcare professionals were often cited in studies as the main reasons behind refugees’ decisions to avoid or forego care [34, 37, 41, 61, 69, 80, 83, 94]. Many refugees, in particular, expressed concerns about not being taken seriously during visits or being perceived as crazy or unintelligent [61, 80, 83]. Lack of discretion and privacy concerns were noted by several studies as other key factors negatively affecting trust [34, 41, 46, 47, 50, 92]. Having long-term relationships with consistent clinicians and staff, however, was seen as a way to build trust [44, 46, 78].
Sociocultural and Religious Factors
Sociocultural and religious factors affecting healthcare access include norms, values, and practices around health and healthcare related to refugees' customs in their countries of origin. This section also discusses aspects of refugees’ experiences and backgrounds that are normative and not normative (i.e., culturally acceptable or not acceptable) compared to their host countries. One finding across several studies highlights how the low importance placed upon preventative services in home countries compared to in the US impacts healthcare utilization, where seeking health services is seen as a last resort rather than routine activity [41, 45, 54, 70, 77, 82, 87]. Refugees were also reported to use prayer and other traditional practices as complementary and sometimes primary methods of treating disease or increasing wellbeing, especially when they were dissatisfied with their healthcare visit [38, 40, 41, 48, 53, 56, 67, 70, 83]. To this end, herbalists and religious clerics were often seen as additional sources of health services [41, 83]. Beliefs around modesty and privacy also impacted refugee patients’ health preferences and experiences, such as female refugees preferring female physicians or refugee patients experiencing stigma around certain health topics like sexual and reproductive health [65, 70, 77, 78, 86].
Transportation
Transportation refers to the factors affecting physical access to health services and treatment. Thirteen studies noted that refugees lacked access to reliable transportation, leading to difficulty attending healthcare appointments [41, 44, 48, 51, 59, 60, 65, 70, 71, 78, 86, 87]. Studies noted challenges associated with being unable to drive, experiencing physical difficulties in walking to bus stops or far-away clinics, or being unable to communicate with bus and taxi drivers [48, 87]. Access to community programs with ride services, home health services, and family members, friends, or neighbors with cars, however, mitigated these transportation issues [60, 71, 86].
Use of Social Support Networks
Use of social support networks is defined as factors related to engagement with individuals and communities outside the formal healthcare network. Families were noted by studies to be an important form of support when it came to seeking health information and arranging transportation to health appointments [57, 60, 68]. Herbalists and religious clerics were additional sources of health services [41, 83]. Finding a community of others from their country of origin also helped refugees navigate health systems by helping with medical costs and serving as interpreters [56, 76]. Adolescents in the community, in particular, were found to be important interpreters to refugee patients [69]. Although one study found that refugees were skeptical of health information from unofficial sources like the internet or family members, other studies noted that family and friends were an important source of health information as well as support [54, 57, 61, 68, 88]. However, attending to family needs was often cited as a competing priority to good health [83].
Immigration Status
This theme refers to factors related to citizenship status and formal assimilation processes. Three articles detailed how fear of deportation led to avoidance of healthcare utilization [37, 78, 92]. Citizenship status also affected refugees’ ability to enroll in public insurance or buy insurance, which impacted their healthcare access [37, 92]. Although immigration medical testing requirements helped some refugees address identified diseases early, another study highlights that a lack of service integration and coordination led to lack of identification and addressal of other health needs of newly arrived refugees, particularly those living with disabilities [47, 73]. In addition to these challenges, one study details how prioritization of other resettlement challenges also led to decreased healthcare utilization [37].
A Note on the Interconnectedness among Themes
We have identified nine key distinct themes related to refugee healthcare access that are interconnected in nature. Although each theme distinguishes a key unique factor that shapes refugee healthcare access, there are elements within each theme that are related to other themes. Figure 3 illustrates the interconnectedness of the themes. The theme of medical (mis)trust, for example, is related to perception of health service and quality, sociocultural and religious factors, as well as the use of social support networks. Medical (mis)trust is related to sociocultural and religious factors in that clinical interaction expectations—and thus perceptions of trust and mistrust based on those interactions—are often times shaped by the sociocultural and religious norms and values refugees hold. Taboos against giving blood, for example, was found to influence some refugees’ decisions to remain in care and led to mistrust when clinicians did not communicate about reasons behind blood tests such as during prenatal visits [79, 95]. These negative interactions can then, in turn, impact refugees’ perceptions of health services as being of poor or insufficient quality [44, 80]. Given these negative perceptions, refugees may then turn more to their social support networks for care-related support to fill perceived care gaps [38, 56]. Another example of how the theme of transportation is similarly related to use of social support networks includes the lack of access to personal transportation resulting in higher reliance on family members and neighbors to provide rides to healthcare appointments [60, 87].

Interconnectedness of themes as identified in this review
Discussion
Main Findings
This systematic review of 64 articles synthesized the factors affecting adult refugees’ healthcare access and utilization in the US. Overall, our results reveal that refugees’ healthcare access is shaped by diverse interacting factors both within and outside of clinical spaces that are multi-level in nature. We also found that the identified themes were interwoven in nature, with many themes often overlapping. This varying dimensionality of our findings also correlate with previous literature assessing factors affecting refugees’ mental health and well-being [98]. Overall, when it comes to healthcare access and utilization, we found that refugees reported that their main challenges to healthcare access stemmed from the fragmented nature of the US healthcare system interacting with provider bias and adverse social determinants. This interrelationship among healthcare access factors and broader social determinants of health and social attitudes has been well-documented in other systematic reviews on healthcare access for marginalized health populations such as low-income individuals, racial and ethnic minorities, people living with disabilities, and LGBTQ+-identifying persons [99,100,101,102]. Although refugees may often also hold one or multiple of these identities, there are some experiences that may be unique to only refugees such as the experience of immigrating involuntarily and additional burdens associated with setting up a new life in a foreign country. Refugees’ challenges to healthcare access thus may have much overlap with yet also nuanced distinction from the challenges of these aforementioned communities. Given the complex and interconnected nature of factors affecting refugees’ healthcare access, interventions that seek to expand access and improve quality of care for US refugee patients cannot be performed in isolation. Instead, contextualized multi-level solutions that are created and executed collaboratively between healthcare systems, policymakers, and community partners are necessary to fully address the layered ecosystem of factors refugee patients face when accessing healthcare.
Our analysis revealed that care inconsistency and fragmentation within the US healthcare system served as a main barrier to healthcare access for refugee patients by decreasing trust and increasing patient work. Within the hospital setting, frequent changes in healthcare professionals and short clinical encounters strained relationships between refugee patients and their providers, leading to low levels of trust. Trust was a particularly important theme given that low levels of trust or mistrust was a key influencer in refugee patients’ decision to postpone or forego care. Healthcare professionals’ cultural awareness and attitudes contributed significantly to this trust-building as well, with perceived stereotyping and bias decreasing trust and repeated interactions and culturally-informed care increasing trust. In studies on healthcare access among racial minorities, people with disability, and LGBTQ+-identifying individuals, discriminatory attitudes of healthcare professionals and other prior negative experiences with healthcare systems led to reduced trust that have similarly been cited as barriers to care [101, 103, 104]. One distinctive aspect of the refugee experience, however, is that refugees must navigate new cultures and healthcare systems on top of other migration-related tasks in an accelerated timeline compared with other marginalized communities within the US. Not only may there be reduced trust, then, but it may also be especially difficult to establish trust in the first place. This is particularly the case when there is a further lack of representation of healthcare professionals with similar backgrounds within healthcare spaces.
Some ways institutions have been successful in cultivating trust in patient populations have been through cultural competency training like Morehouse School of Medicine’s CRASH course as well as targeted training for working with specific populations. These programs inform and orient healthcare professionals to the perspectives and needs of patients from backgrounds other than their own, while also providing actionable tools to more conscientiously interact with these less familiar patient populations [105]. In our current environment of heightened awareness in cultural competency, though, this increased training has mainly been focused on racial minorities and LGBTQ+-identifying patient populations [106, 107]. Training for refugee patients has been more limited and needs to be expanded alongside efforts to increase general diversity of representation within the medical field (e.g., those who come from a refugee background, are familiar with refugee experiences, or share a similar cultural background to refugees). Additionally, refugee-specific trainings need to also attend to the other previously mentioned intersecting identities of refugees like age, race, class, gender, and disability status. Kimberlé Crenshaw’s work on intersectionality highlights how these different social categorizations create independent yet overlapping systems of disadvantage which further shape refugees’ experiences [108]. Highlighting these additional elements in refugees’ identities within cultural competency trainings is thus essential to further educate clinicians and other healthcare professionals on how to anticipate refugees’ various needs when navigating healthcare systems. Further, by including a subset of the literature which explored intersecting identities (i.e., being a refugee woman or a refugee with disabilities), our themes reflect the needs of some refugees who simultaneously hold other marginalized identities. There is thus opportunity for significantly more work exploring intersectionality around socioeconomic class, education status, and sexual identity, among others to gain an even broader understanding of the range of barriers and facilitators to healthcare access that are experienced.
In addition to decreased trust, care fragmentation also led to increased patient task burden, which was similarly associated with decreased perceptions of quality of care and decreased healthcare utilization. The need for patients to book their own appointments and navigate between multiple independent facilities and long wait times led to coordination-related stresses in accessing care, especially when compounded with refugees’ limited familiarity with US healthcare processes. This patient burden has been documented in other studies on healthcare access but may not include the additional patient work of someone who has just moved to the US and must balance and coordinate healthcare needs with other layers of work such as language access [109, 110].
On the subject of coordination, transportation to appointments was especially challenging for refugees, who often did not own cars and were also unfamiliar with public transportation systems. Colocation of services, expanded transportation services, and streamlined appointment scheduling are thus further necessary interventions for expanding refugees’ healthcare access. These are all elements of the patient experience that remain invisible across many marginalized communities, but may be especially pronounced for refugee populations. Whereas the process of balancing multiple tasks and prioritizing different needs exist for everyone, this process is especially challenging for refugees who must do so without their normal social supports and on an accelerated timeline. Managing different tasks all at once is already difficult enough, but refugees must also face a steep learning curve with learning what tasks to do. Their unfamiliarity with US systems makes tasks like seeking medical services, applying for different social services, finding a job, and learning a new language, among others, especially challenging. In addition, the emphasis on prevention and healthcare maintenance in the US is a new concept for most refugees, and thus they may decline costly and sometimes uncomfortable or lengthy procedures without fully understanding why they need them when feeling well. Refugee patients thus need programs that help them understand and navigate these systems both within and beyond healthcare spaces.
Medical interpreters were proven to be critical assets to the care team when it comes to expanding healthcare access for refugee patients. Not only should they be present to assist with interpretation during clinical visits, but they may also alleviate language barriers in transportation coordination and appointment scheduling. When using interpreters, however, it is important to be mindful of their impact on trust-building with refugee patients. We found that constant cycling of interpreters, underqualified interpreters, or use of only community-based interpreters have been identified as key reasons for the development of mistrust due to both undermined confidence in care quality and privacy concerns. Previous studies on the use of interpreters have also shown that in-person and video interpretation were preferred over telephone interpretation services [111]. It is essential to ensure that interpretation services are not only made available but that they are also high quality and secure.
Immigration status is another distinct barrier to healthcare access for refugee patients, particularly those who came as asylees. Unlike refugees who must have legal documentation for their stay in the US before arrival, all asylees by definition will not have received official documentation upon arrival to the US. During this process of seeking asylum, which typically lasts anywhere from 6 months to several years, such asylum seekers are technically in the US without documentation until they receive either pending asylee status or official asylee status [112]. Consequently, some challenges associated with accessing healthcare stems from this confusing interim status, including fear of deportation resulting in avoidance of medical visits and lack of official documentation rendering marketplace insurance plans inaccessible [113]. It is unsurprising, then that the asylum-seeking process itself have been additionally flagged in refugee mental health literature as negatively impacting refugees’ overall wellbeing [98]. It is important to note, however, that in the United States, Emergency Medicaid (a limited form of Medicaid) is available to asylees during this stage. Once their formal application for asylum has been received by the United States Citizenship and Immigration Services, they are then eligible for Permanent Resident Under the Color of Law (PRUCOL) status which qualifies their eligibility for Medicaid [114]. Absent legality issues, though, the process of migration itself poses significant challenges to care coordination. Limited health service integration and coordination between refugee camps and the US may lead to a lack of identification of health needs of newly arrived refugees including those with prior health conditions. Although there exist early testing requirements for communicable diseases such as tuberculosis and hepatitis B, and some non-communicable conditions such as lipid disorders, additional health intakes should be incorporated into immigration policy to assist with care transitions.
Overall, our findings underscore the need for an integrated care model to address the diversity of challenges that refugee patients face when accessing healthcare. Integrated care models have been shown to be effective in addressing multiple levels of need by bringing together an interdisciplinary team that is connected to community resources [115, 116]. In the mental health space, integrated care models have been shown to further reduce racial and ethnic disparities [117]. The International Family Medicine Clinic (IFMC) within the University of Virginia Family Medicine Clinic is one example of how this team-based care model can be leveraged to specifically expand care for refugee patients [118]. Primary care professionals at the IFMC work closely with an ambulatory pharmacist, a nursing team which includes a nurse care coordinator (RN-CC), a social worker, and a behavioral health team of psychiatrists and clinical psychologists. The RN-CC serves a key role as liaison between the clinic and the health department, resettlement agency, and other community resources. The RN-CC additionally helps patients navigate their care within the larger hospital system, which includes providing education on logistics of the clinic flow at initial visits, and in this role also helps facilitate urgent referrals for specialty care when needed. The IFMC team, in conjunction with the resettlement agency, further helps patients with transportation to the clinic and medical center. By working collaboratively across agencies to address refugees’ complex needs both inside and outside clinical spaces, the integrated care model has potential to expand refugee healthcare access in multifaceted ways.
Strengths and Limitations
One main limitation of this study is that the literature search conducted may have still missed relevant articles that relate to refugee healthcare access but did not include any of the words in our search strategy or were published in a language other than English. Although we mitigated this limitation by doing manual searches for relevant literature from related articles and conducting searches at several points in time, there is still a chance that potentially relevant articles may have been missed. An additional limitation of this study emerges from the fact that literature in the refugee healthcare access space typically focuses on particular subpopulations of refugees within states that already have established refugee care centers. Experiences of these refugees may not directly translate to the experiences of refugees settling in states without these centers, where challenges with healthcare access may be further pronounced by the additional lack of focus on refugee patient populations. Further, a vast majority of studies were conducted in the primary care setting. Despite these limitations, notable strengths of this study include the focus on qualitative studies allowing for rich exploration of the themes and inclusion of only high-quality studies based on the CASP.
Future Research
Although our primary goal was to focus on the healthcare system, in doing so, much of what we found suggest that healthcare access is deeply intertwined with other social determinants of health. There is thus a need to conduct additional literature reviews that focus explicitly on social determinants of health outside the clinical setting. An example of this would be to search for articles on refugees’ access to safe housing, healthy foods, or jobs that provide health insurance. Future research should further seek to expand upon our literature review by including searches for articles in journals which are not directly categorized under healthcare access but instead relate directly to social determinants of health which may affect healthcare access. Our focus was also specific only to qualitative studies and those with refugees’ firsthand experiences, and could benefit from future research that includes quantitative studies as well as perspectives from those who interact with refugees (e.g., family members, friends, neighbors, healthcare professionals, service providers). In addition to these expanded literature reviews, primary research should further investigate the impact of time in the host country on care. There is a need to investigate whether health outcomes remain the same for those who have resettled for differing amounts of time. Although much of the literature was focused only on country of origin, future research may benefit from capturing other ways experiences of refugees may differ based on time of resettlement, disability status, age, gender, and race. Lastly, additional research should focus on refugee populations outside of areas with established refugee care centers and in specialty care settings, where limited research has been conducted.
Conclusions
The results of this literature review highlight that refugees have a unique constellation of needs that both overlap with yet are also distinct from other marginalized communities when it comes to accessing healthcare. The diverse nature of these needs indicate that multilevel interventions are necessary to improve refugee healthcare access. Our results suggest that refugee patients not only require expanded healthcare access policies and better service integration within hospital settings, but they also require additional support outside of the clinical space, including support navigating social welfare programs and accessing transportation, among others. The implementation of integrated care models similar to the University of Virginia’s IFMC may help bridge both the medical and social needs of refugee patients while eliminating several access barriers related to care coordination.
Appendix
All searches conducted on March 11 2021 and updated June 17 2021 (Table 2).
References
United Nations High Commissioner for Refugees Mid-Year Trends. In: UNHCR. https://www.unhcr.org/mid-year-trends.html. Accessed 22 Jul 2022
United Nations High Commissioner for Refugees Refugee Statistics|USA for UNHCR. https://www.unrefugees.org/refugee-facts/statistics/. Accessed 22 Jul 2022
Freel C (2022) The Presidential Determination on Refugee Admissions for Fiscal Year 2022. In: United States Department of State. https://www.state.gov/the-presidential-determination-on-refugee-admissions-for-fiscal-year-2022/. Accessed 28 Jul 2022
8 USC 1101: Definitions. https://uscode.house.gov/view.xhtml?req=granuleid%3AUSC-prelim-title8-section1101&num=0&edition=prelim. Accessed 28 Jul 2022
Brolan CE, Forman L, Dagron S, Hammonds R, Waris A, Latif L, Ruano AL. The right to health of non-nationals and displaced persons in the sustainable development goals era: challenges for equity in universal health care. Int J Equity Health. 2017;16:14. https://doi.org/10.1186/s12939-016-0500-z.
World Health Organization. REgional Office for Europe. (n.d.) Migration and Health: Key Issues. https://www.euro.who.int/__data/assets/pdf_file/0005/293270/Migration-Health-Key-Issues-.pdf
Hollifield M, Warner TD, Lian N, Krakow B, Jenkins JH, Kesler J, Stevenson J, Westermeyer J. Measuring trauma and health status in refugees: a critical review. JAMA. 2002;288:611–21. https://doi.org/10.1001/jama.288.5.611.
Ackerman LK. Health problems of refugees. J Am Board Fam Pract. 1997;10:337–48.
Proença R, Mattos Souza F, Lisboa Bastos M, Caetano R, Braga JU, Faerstein E, Trajman A. Active and latent tuberculosis in refugees and asylum seekers: a systematic review and meta-analysis. BMC Public Health. 2020;20:838. https://doi.org/10.1186/s12889-020-08907-y.
Greenaway C, Sandoe A, Vissandjee B, Kitai I, Gruner D, Wobeser W, Pottie K, Ueffing E, Menzies D, Schwartzman K (2011) Tuberculosis: evidence review for newly arriving immigrants and refugees. CMAJ 183:E939–951. https://doi.org/10.1503/cmaj.090302
Benzeguir AK, Capraru T, Aust-Kettis A, Björkman A. High frequency of gastrointestinal parasites in refugees and asylum seekers upon arrival in Sweden. Scand J Infect Dis. 1999;31:79–82. https://doi.org/10.1080/00365549950161934.
Pavli A, Maltezou H (2017) Health problems of newly arrived migrants and refugees in Europe. J Travel Med 24. https://doi.org/10.1093/jtm/tax016
Pernitez-Agan S, Wickramage K, Yen C, Dawson-Hahn E, Mitchell T, Zenner D. Nutritional profile of Syrian refugee children before resettlement. Confl Health. 2019;13:22. https://doi.org/10.1186/s13031-019-0208-y.
Benson J, Phillips C, Kay M, Webber MT, Ratcliff AJ, Correa-Velez I, Lorimer MF (2013) Low vitamin B12 levels among newly-arrived refugees from Bhutan, Iran and Afghanistan: a multicentre Australian study. PLoS One 8:e57998. https://doi.org/10.1371/journal.pone.0057998
Yun K, Hebrank K, Graber LK, Sullivan M-C, Chen I, Gupta J. High prevalence of chronic non-communicable conditions among adult refugees: implications for practice and policy. J Community Health. 2012;37:1110–8. https://doi.org/10.1007/s10900-012-9552-1.
Dookeran NM, Battaglia T, Cochran J, Geltman PL. Chronic disease and its risk factors among refugees and asylees in Massachusetts, 2001–2005. Prev Chronic Dis. 2010;7:A51.
Blackmore R, Boyle JA, Fazel M, Ranasinha S, Gray KM, Fitzgerald G, Misso M, Gibson-Helm M (2020) The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLoS Med 17:e1003337. https://doi.org/10.1371/journal.pmed.1003337
Rosenthal T. Immigration and acculturation: impact on health and well-being of immigrants. Curr Hypertens Rep. 2018;20:70. https://doi.org/10.1007/s11906-018-0872-0.
Kumar GS, Beeler JA, Seagle EE, Jentes ES. Long-term physical health outcomes of resettled refugee populations in the United States: a scoping review. J Immigr Minor Health. 2021;23:813–23. https://doi.org/10.1007/s10903-021-01146-2.
World Health Organization Social determinants of health. In: Social determinants of health. https://www.who.int/health-topics/social-determinants-of-health. Accessed 1 Feb 2023
Office of Disease Prevention and Health Promotion Social Determinants of Health—Healthy People 2030|health.gov. In: Social Determinants of Health—Healthy People 2030|health.gov. https://health.gov/healthypeople/priority-areas/social-determinants-health. Accessed 1 Feb 2023
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535. https://doi.org/10.1136/bmj.b2535
Turrini G, Purgato M, Acarturk C, Anttila M, Au T, Ballette F, Bird M, Carswell K, Churchill R, Cuijpers P, Hall J, Hansen LJ, Kösters M, Lantta T, Nosè M, Ostuzzi G, Sijbrandij M, Tedeschi F, Valimaki M, Wancata J, White R, van Ommeren M, Barbui C. Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: systematic review and meta-analysis. Epidemiol Psychiatr Sci. 2019;28:376–88. https://doi.org/10.1017/s2045796019000027.
Morina N, Akhtar A, Barth J, Schnyder U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: a systematic review. Front Psychiatry. 2018;9:433. https://doi.org/10.3389/fpsyt.2018.00433.
Uphoff E, Robertson L, Cabieses B, Villalón FJ, Purgato M, Churchill R, Barbui C (2020) An overview of systematic reviews on mental health promotion, prevention, and treatment of common mental disorders for refugees, asylum seekers, and internally displaced persons. Cochrane Database Syst Rev 9:Cd013458. https://doi.org/10.1002/14651858.CD013458.pub2
Abu Suhaiban H, Grasser LR, Javanbakht A. Mental health of refugees and torture survivors: a critical review of prevalence, predictors, and integrated care. Int J Environ Res Public Health. 2019;16:14. https://doi.org/10.3390/ijerph16132309.
Byrow Y, Pajak R, Specker P, Nickerson A (2020) Perceptions of mental health and perceived barriers to mental health help-seeking amongst refugees: a systematic review. Clin Psychol Rev 75:101812. https://doi.org/10.1016/j.cpr.2019.101812
Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016;104:240–3. https://doi.org/10.3163/1536-5050.104.3.014.
CASP Checklists—Critical Appraisal Skills Programme. In: CASP—Critical Appraisal Skills Programme. https://casp-uk.net/casp-tools-checklists/. Accessed 1 Feb 2023
Parajuli J, Horey D. Barriers to and facilitators of health services utilisation by refugees in resettlement countries: an overview of systematic reviews. Aust Health Rev. 2020;44:132–42. https://doi.org/10.1071/ah18108.
Feldman R. Primary health care for refugees and asylum seekers: A review of the literature and a framework for services. Public Health. 2006;120:809–16. https://doi.org/10.1016/j.puhe.2006.05.014.
Khanom A, Alanazy W, Couzens L, Evans BA, Fagan L, Fogarty R, John A, Khan T, Kingston MR, Moyo S, Porter A, Rhydderch M, Richardson G, Rungua G, Russell I, Snooks H (2021) Asylum seekers’ and refugees’ experiences of accessing health care: a qualitative study. BJGP Open 5. https://doi.org/10.3399/BJGPO.2021.0059
Kalich A, Heinemann L, Ghahari S. A scoping review of immigrant experience of health care access barriers in Canada. J Immigr Minor Health. 2016;18:697–709. https://doi.org/10.1007/s10903-015-0237-6.
Agbemenu K, Banke-Thomas A, Ely G, Johnson-Agbakwu C (2021) Avoiding obstetrical interventions among US-based Somali migrant women: a qualitative study. Ethn Health 16. https://doi.org/10.1080/13557858.2019.1613519
Agbemenu K, Volpe EM, Dyer E. Reproductive health decision-making among US-dwelling Somali Bantu refugee women: a qualitative study. J Clin Nurs. 2018;27:3355–62. https://doi.org/10.1111/jocn.14162.
Allen EM, Lee HY, Pratt R, Vang H, Desai JR, Dube A, Lightfoot E. Facilitators and barriers of cervical cancer screening and human papilloma virus vaccination among somali refugee women in the United States: a qualitative analysis. J Transcult Nurs. 2019;30:55–63. https://doi.org/10.1177/1043659618796909.
Asgary R, Segar N. Barriers to health care access among refugee asylum seekers. J Health Care Poor Underserved. 2011;22:506–22. https://doi.org/10.1353/hpu.2011.0047.
Assefa MT, Frounfelker RL, Tahir SA, Berent JM, Abdi A, Betancourt TS. Traditional medicine and help-seeking behaviors for health problems among somali bantu refugees resettled in the United States. Qual Health Res. 2021;31:484–97. https://doi.org/10.1177/1049732320970492.
Ayub S, Marsh V, Reed S. An exploration of chronic disease perception, management, and barriers to care in Liberian refugees resettled in Charlottesville, Virginia. J Natl Med Assoc. 2020;112:654–67. https://doi.org/10.1016/j.jnma.2020.06.013.
Bell SE. Placing care: embodying architecture in hospital clinics for immigrant and refugee patients. Sociol Health Illn. 2018;40:314–26. https://doi.org/10.1111/1467-9566.12604.
Boise L, Tuepker A, Gipson T, Vigmenon Y, Soule I, Onadeko S. African refugee and immigrant health needs: report from a community-based house meeting project. Prog Community Health Partnersh. 2013;7:369–78. https://doi.org/10.1353/cpr.2013.0045.
Brown E, Carroll J, Fogarty C, Holt C. “They get a C-section...they gonna die”: Somali women’s fears of obstetrical interventions in the United States. J Transcult Nurs. 2010;21:220–7. https://doi.org/10.1177/1043659609358780.
Carroll J, Epstein R, Fiscella K, Gipson T, Volpe E, Jean-Pierre P. Caring for Somali women: implications for clinician-patient communication. Patient Educ Couns. 2007;66:337–45. https://doi.org/10.1016/j.pec.2007.01.008.
Carroll J, Epstein R, Fiscella K, Volpe E, Diaz K, Omar S. Knowledge and beliefs about health promotion and preventive health care among Somali women in the United States. Health Care Women Int. 2007;28:360–80. https://doi.org/10.1080/07399330601179935.
Chao X, Kang BP. Health literacy among Bhutanese Adult Refugees in the United States: the sociocultural approach. Adult Educ Q. 2020;70:258–76. https://doi.org/10.1177/0741713620904047.
Chavez KR. Identifying the needs of LGBTQ immigrants and refugees in Southern Arizona. J Homosex. 2011;58:189–218. https://doi.org/10.1080/00918369.2011.540175.
Connor JJ, Hunt S, Finsaas M, Ciesinski A, Ahmed A, Robinson BB. Sexual health care, sexual behaviors and functioning, and female genital cutting: perspectives from Somali women living in the United States. J Sex Res. 2016;53:346–59. https://doi.org/10.1080/00224499.2015.1008966.
Deckys C, Springer P. The Elderly Somali Bantu Refugees’ adjustment to American Healthcare. Online J Cult Competence Nurs Healthc. 2013;3:3–15.
Dubus NM. Self-perception of when old age begins for Cambodian elders living in the United States. J Cross Cult Gerontol. 2014;29:185–99. https://doi.org/10.1007/s10823-014-9230-0.
Fang DM, Baker DL. Barriers and facilitators of cervical cancer screening among women of Hmong origin. J Health Care Poor Underserved. 2013;24:540–55. https://doi.org/10.1353/hpu.2013.0067.
Filippi MK, Faseru B, Baird M, Ndikum-Moffor F, Greiner KA, Daley CM. A pilot study of health priorities of Somalis living in Kansas City: laying the groundwork for CBPR. J Immigr Minor Health. 2014;16:314–20. https://doi.org/10.1007/s10903-012-9732-1.
Fineran S, Kohli HK. Muslim refugee women’s perspectives on intimate partner violence. J Fam Soc Work. 2020;23:199–213. https://doi.org/10.1080/10522158.2020.1742839.
Freeman PAC, Penney DS, Bettmann JE, Lecy N. The intersection of health beliefs and religion among Somali refugees: a qualitative study. J Relig Spiritual Soc Work Soc Thought. 2013;32:1–13. https://doi.org/10.1080/15426432.2013.749141.
Ghebrendrias S, Pfeil S, Crouthamel B, Chalmiers M, Kully G, Mody S. An examination of misconceptions and their impact on cervical cancer prevention practices among Sub-Saharan African and Middle Eastern Refugees. Health Equity. 2021;5:382–9. https://doi.org/10.1089/heq.2020.0125.
Grimm B, Alnaji N, Watanabe-Galloway S, Leypoldt M. Cervical Cancer Attitudes and Knowledge in Somali Refugees in Nebraska. Pedagogy Health Promot. 2017;3:81S-87S. https://doi.org/10.1177/2373379917698673.
Gurnah K, Khoshnood K, Bradley E, Yuan C. Lost in translation: reproductive health care experiences of Somali Bantu women in Hartford, Connecticut. J Midwifery Womens Health. 2011;56:340–6. https://doi.org/10.1111/j.1542-2011.2011.00028.x.
Haley HL, Walsh M, Tin Maung NH, Savage CP, Cashman S. Primary prevention for resettled refugees from Burma: where to begin? J Commun Health. 2014;39:1–10. https://doi.org/10.1007/s10900-013-9732-7.
Hauck FR, Lo E, Maxwell A, Reynolds PP. Factors influencing the Acculturation of Burmese, Bhutanese, and Iraqi Refugees into American Society: Cross-Cultural Comparisons. J Immigr Refug Stud. 2014;12:331–52. https://doi.org/10.1080/15562948.2013.848007.
Haworth RJ, Margalit R, Ross C, Nepal T, Soliman AS. Knowledge, attitudes, and practices for cervical cancer screening among the Bhutanese refugee community in Omaha, Nebraska. J Commun Health. 2014;39:872–8. https://doi.org/10.1007/s10900-014-9906-y.
Helsel D, Mochel M, Bauer R. Chronic illness and Hmong shamans. J Transcult Nurs. 2005;16:150–4. https://doi.org/10.1177/1043659604273553.
Houston AR, Lincoln A, Gillespie S, Da Fonseca T, Issa O, Ellis H, Salhi C (2021) You have to pay to live: somali young adult experiences with the US Health Care System. Qual Health Res:10497323211010160. https://doi.org/10.1177/10497323211010159
Inhorn MC, Fakih MH. Arab Americans, African Americans, and infertility: barriers to reproduction and medical care. Fertil Steril. 2006;85:844–52. https://doi.org/10.1016/j.fertnstert.2005.10.029.
Ivanov LL, Buck K. Health care utilization patterns of Russian-speaking immigrant women across age groups. J Immigr Health. 2002;4:17–27. https://doi.org/10.1023/a:1013055110631.
Johnson-Agbakwu CE, Helm T, Killawi A, Padela AI. Perceptions of obstetrical interventions and female genital cutting: insights of men in a Somali refugee community. Ethn Health. 2014;19:440–57. https://doi.org/10.1080/13557858.2013.828829.
Kaczkowski W, Swartout KM. Exploring gender differences in sexual and reproductive health literacy among young people from refugee backgrounds. Cult Health Sex. 2020;22:369–84. https://doi.org/10.1080/13691058.2019.1601772.
Kingori C, Ice GH, Hassan Q, Elmi A, Perko E. “If I went to my mom with that information, I’m dead”: sexual health knowledge barriers among immigrant and refugee Somali young adults in Ohio. Ethn Health. 2018;23:339–52. https://doi.org/10.1080/13557858.2016.1263285.
Lipson JG, Weinstein HM, Gladstone EA, Sarnoff RH. Bosnian and Soviet refugees’ experiences with health care. West J Nurs Res. 2003;25:854–71. https://doi.org/10.1177/0193945903256714.
Lor B, Ornelas IJ, Magarati M, Do HH, Zhang Y, Jackson JC, Taylor VM. We should know ourselves: Burmese and Bhutanese Refugee Women’s perspectives on cervical cancer screening. J Health Care Poor Underserved. 2018;29:881–97. https://doi.org/10.1353/hpu.2018.0066.
McHenry MS, Umoren R, Dixit A, Holliday R, Litzelman D. Exploring healthcare perspectives of Burmese Chin Refugees. J Cult Divers. 2016;23:151–7.
Mehta PK, Saia K, Mody D, Crosby SS, Raj A, Maru S, Piwowarczyk L. Learning from UJAMBO: perspectives on gynecologic care in African Immigrant and Refugee Women in Boston, Massachusetts. J Immigr Minor Health. 2018;20:380–7. https://doi.org/10.1007/s10903-017-0659-4.
Miner S, Liebel DV, Wilde MH, Carroll JK, Omar S. Somali Older Adults’ and their Families’ perceptions of adult home health services. J Immigr Minor Health. 2018;20:1215–21. https://doi.org/10.1007/s10903-017-0658-5.
Mirza M, Heinemann AW. Service needs and service gaps among refugees with disabilities resettled in the United States. Disabil Rehabil. 2012;34:542–52. https://doi.org/10.3109/09638288.2011.611211.
Mirza M, Luna R, Mathews B, Hasnain R, Hebert E, Niebauer A, Mishra UD. Barriers to healthcare access among refugees with disabilities and chronic health conditions resettled in the US Midwest. J Immigr Minor Health. 2014;16:733–42. https://doi.org/10.1007/s10903-013-9906-5.
Mitschke DB, Mitschke AE, Slater HM, Teboh C. Uncovering health and wellness needs of recently resettled Karen Refugees from Burma. J Hum Behav Soc Environ. 2011;21:490–501. https://doi.org/10.1080/10911359.2011.566466.
Morioka-Douglas N, Sacks T, Yeo G. Issues in caring for Afghan American elders: insights from literature and a focus group. J Cross Cult Gerontol. 2004;19:27–40. https://doi.org/10.1023/B:JCCG.0000015015.63501.db.
Morris MD, Popper ST, Rodwell TC, Brodine SK, Brouwer KC. Healthcare barriers of refugees post-resettlement. J Commun Health. 2009;34:529–38. https://doi.org/10.1007/s10900-009-9175-3.
Murray KE, Mohamed AS, Ndunduyenge G. Health and prevention among East African women in the US. J Health Care Poor Underserved. 2013;24:233–46. https://doi.org/10.1353/hpu.2013.0029.
Othieno J. Twin Cities care system assessment: process, findings, and recommendations. J Health Care Poor Underserved. 2007;18:189–213. https://doi.org/10.1353/hpu.2007.0086.
Othieno J. Understanding how contextual realities affect African born immigrants and refugees living with HIV in accessing care in the Twin Cities. J Health Care Poor Underserved. 2007;18:170–88. https://doi.org/10.1353/hpu.2007.0085.
Pavlish CL, Noor S, Brandt J. Somali immigrant women and the American health care system: discordant beliefs, divergent expectations, and silent worries. Soc Sci Med. 2010;71:353–61. https://doi.org/10.1016/j.socscimed.2010.04.010.
Renfrew MR, Taing E, Cohen MJ, Betancourt JR, Pasinski R, Green AR. Barriers to care for Cambodian patients with diabetes: results from a qualitative study. J Health Care Poor Underserved. 2013;24:633–55. https://doi.org/10.1353/hpu.2013.0065.
Resick LK. The meaning of health among midlife Russian-speaking women. J Nurs Scholarsh. 2008;40:248–53. https://doi.org/10.1111/j.1547-5069.2008.00233.x.
Ross Perfetti A, Abboud S, Behme M, Barg FK. Understanding wellness and barriers to care among Iraqi refugee women in the United States. Health Soc Care Commun. 2019;27:1430–7. https://doi.org/10.1111/hsc.12810.
Royer PA, Olson LM, Jackson B, Weber LS, Gawron L, Sanders JN, Turok DK. “In Africa, There Was No Family Planning. Every Year You Just Give Birth”: family planning knowledge, attitudes, and practices among somali and congolese refugee women after resettlement to the United States. Qual Health Res. 2020;30:391–408. https://doi.org/10.1177/1049732319861381.
Saadi A, Bond BE, Percac-Lima S. Bosnian, Iraqi, and Somali Refugee Women Speak: a comparative qualitative study of refugee health beliefs on preventive health and breast cancer screening. Womens Health Issues. 2015;25:501–8. https://doi.org/10.1016/j.whi.2015.06.005.
Saadi A, Bond B, Percac-Lima S. Perspectives on preventive health care and barriers to breast cancer screening among Iraqi women refugees. J Immigr Minor Health. 2012;14:633–9. https://doi.org/10.1007/s10903-011-9520-3.
Schuster RC, Rodriguez EM, Blosser M, Mongo A, Delvecchio-Hitchcock N, Kahn L, Tumiel-Berhalter L. “They were just waiting to die”: Somali Bantu and Karen experiences with cancer screening pre- and post-resettlement in Buffalo, NY. J Natl Med Assoc. 2019;111:234–45. https://doi.org/10.1016/j.jnma.2018.10.006.
Siddiq H, Pavlish C, Alemi Q, Mentes J, Lee E. Beyond resettlement: sociocultural factors influencing breast and colorectal cancer screening among Afghan Refugee Women. J Cancer Educ. 2020. https://doi.org/10.1007/s13187-020-01822-1.
Soin KS, Beldowski K, Bates E, Garcia KP, Naik S, Plumb E, Brawer R, Santana A, Altshuler M. Attitudes towards family planning among Bhutanese, Burmese, and Iraqi Refugee Women: a qualitative study. Hawaii J Health Soc Welf. 2020;79:70–7.
Springer PJ, Black M, Martz K, Deckys C, Soelberg T. Somali Bantu refugees in southwest Idaho: assessment using participatory research. ANS Adv Nurs Sci. 2010;33:170–81. https://doi.org/10.1097/ANS.0b013e3181dbc60f.
Upvall MJ, Mohammed K, Dodge PD. Perspectives of Somali Bantu refugee women living with circumcision in the United States: a focus group approach. Int J Nurs Stud. 2009;46:360–8. https://doi.org/10.1016/j.ijnurstu.2008.04.009.
Van Son CR, Gileff TY. Relying on what they know: older Slavic emigres managing chronic health conditions. Qual Health Res. 2013;23:1660–71. https://doi.org/10.1177/1049732313508842.
Wieland ML, Weis JA, Yawn BP, Sullivan SM, Millington KL, Smith CM, Bertram S, Nigon JA, Sia IG. Perceptions of tuberculosis among immigrants and refugees at an adult education center: a community-based participatory research approach. J Immigr Minor Health. 2012;14:14–22. https://doi.org/10.1007/s10903-010-9391-z.
Wissink L, Jones-Webb R, DuBois D, Krinke B, Ibrahim Q. Improving health care provision to Somali refugee women. Minn Med. 2005;88:36–40.
Worabo HJ, Hsueh KH, Yakimo R, Worabo E, Burgess PA, Farberman SM. Understanding Refugees’ perceptions of health care in the United States. JNP. 2016;12:487–94. https://doi.org/10.1016/j.nurpra.2016.04.014.
Zeidan AJ, Khatri UG, Munyikwa M, Barden A, Samuels-Kalow M. Barriers to accessing acute care for newly arrived refugees. West J Emerg Med. 2019;20:842–50. https://doi.org/10.5811/westjem.2019.8.43129.
Zhang Y, McCoy EE, Scego R, Phillips W, Godfrey E. A qualitative exploration of Somali refugee women’s experiences with family planning in the US. J Immigr Minor Health. 2020;22:66–73. https://doi.org/10.1007/s10903-019-00887-5.
Hajak VL, Sardana S, Verdeli H, Grimm S (2021) A systematic review of factors affecting mental health and well-being of Asylum seekers and refugees in Germany. Front Psychiatry 12:643704. https://doi.org/10.3389/fpsyt.2021.643704
Lazar M, Davenport L. Barriers to health care access for low income families: a review of literature. J Commun Health Nurs. 2018;35:28–37. https://doi.org/10.1080/07370016.2018.1404832.
Chauhan A, Walton M, Manias E, Walpola RL, Seale H, Latanik M, Leone D, Mears S, Harrison R. The safety of health care for ethnic minority patients: a systematic review. Int J Equity Health. 2020;19:118. https://doi.org/10.1186/s12939-020-01223-2.
Alencar Albuquerque G, de Lima Garcia C, da Silva Quirino G, Alves MJH, Belém JM, dos Santos Figueiredo FW, da Silva Paiva L, do Nascimento VB, da Silva Maciel É, Valenti VE, de Abreu LC, Adami F (2016) Access to health services by lesbian, gay, bisexual, and transgender persons: systematic literature review. BMC Int Health Hum Rights 16:2. https://doi.org/10.1186/s12914-015-0072-9
Sakellariou D, Rotarou ES (2017) Access to healthcare for men and women with disabilities in the UK: secondary analysis of cross-sectional data. BMJ Open 7:e016614. https://doi.org/10.1136/bmjopen-2017-016614
Ali A, Scior K, Ratti V, Strydom A, King M, Hassiotis A (2013) Discrimination and other barriers to accessing health care: perspectives of patients with mild and moderate intellectual disability and their carers. PLoS One 8:e70855. https://doi.org/10.1371/journal.pone.0070855
Li C-C, Matthews AK, Aranda F, Patel C, Patel M. Predictors and consequences of negative patient-provider interactions among a sample of African American Sexual Minority Women. LGBT Health. 2015;2:140–6. https://doi.org/10.1089/lgbt.2014.0127.
Holden K, McGregor B, Thandi P, Fresh E, Sheats K, Belton A, Mattox G, Satcher D. Toward culturally centered integrative care for addressing mental health disparities among ethnic minorities. Psychol Serv. 2014;11:357–68. https://doi.org/10.1037/a0038122.
Brach C, Fraser I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med Care Res Rev. 2000;57(Suppl 1):181–217. https://doi.org/10.1177/1077558700057001S09.
Rhoten B, Burkhalter JE, Joo R, Mujawar I, Bruner D, Scout N, Margolies L. Impact of an LGBTQ Cultural Competence Training Program for providers on knowledge, attitudes, self-efficacy, and intensions. J Homosex. 2022;69:1030–41. https://doi.org/10.1080/00918369.2021.1901505.
Crenshaw K. On intersectionality: essential writings. New York: New Press; 2022.
Gorman RK, Wellbeloved-Stone CA, Valdez RS. Uncovering the invisible patient work system through a case study of breast cancer self-management. Ergonomics. 2018;61:1575–90. https://doi.org/10.1080/00140139.2018.1503339.
Valdez RS, Holden RJ, Novak LL, Veinot TC. Transforming consumer health informatics through a patient work framework: connecting patients to context. J Am Med Inform Assoc. 2015;22:2–10. https://doi.org/10.1136/amiajnl-2014-002826.
Locatis C, Williamson D, Gould-Kabler C, Zone-Smith L, Detzler I, Roberson J, Maisiak R, Ackerman M. Comparing in-person, video, and telephonic medical interpretation. J Gen Intern Med. 2010;25:345–50. https://doi.org/10.1007/s11606-009-1236-x.
Fact Sheet: US Asylum Process. In: National Immigration Forum. https://immigrationforum.org/article/fact-sheet-u-s-asylum-process/. Accessed 24 Jul 2022
Health coverage for immigrants. In: HealthCare.gov. https://www.healthcare.gov/immigrants/coverage/. Accessed 24 Jul 2022
Legal Resources|Center for Human Rights. https://humanrights.weill.cornell.edu/resources/medicaid-and-legal-resources. Accessed 24 Jul 2022
World Health Organization Regional Office for Europe (2016) Integrated care models: an overview. In: Integrated care models: an overview. https://www.euro.who.int/__data/assets/pdf_file/0005/322475/Integrated-care-models-overview.pdf
Mitchell GK, Burridge L, Zhang J, Donald M, Scott IA, Dart J, Jackson CL. Systematic review of integrated models of health care delivered at the primary-secondary interface: how effective is it and what determines effectiveness? Aust J Prim Health. 2015;21:391–408. https://doi.org/10.1071/PY14172.
Lee-Tauler SY, Eun J, Corbett D, Collins PY. A systematic review of interventions to improve initiation of mental health care among Racial-Ethnic Minority Groups. Psychiatr Serv. 2018;69:628–47. https://doi.org/10.1176/appi.ps.201700382.
Elmore CE, Tingen JM, Fredgren K, Dalrymple SN, Compton RM, Carpenter EL, et. al. Utilizing an interprofessional team to provide refugee healthcare in an academic medical center. Fam Med Com Health 2019; 7e000091. https://doi.org/10.1136/fmch-2018-000091.
Author information
Authors and Affiliations
Contributions
F.H., R.S.V., and C.H. conceptualized the study. A.D. performed the literature review. C.H. and N.S. screened abstracts. C.H., A.D., S.B., N.S., and K.M. screened studies, performed the quality assessment, and coded the articles. C.H. synthesized the codes into themes and drafted the manuscript. F.H., R.S.V., M.O., N.S., and K.M. provided feedback on the manuscript. All authors reviewed and approved the final version.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that there are no conflicts of interest in conducting this review.
Ethical Approval
The authors declare that all authors have reviewed this manuscript and have approved it for submission.
Consent for Publication
The authors declare that this manuscript is not under submission elsewhere and has not been published elsewhere.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ho, C.H., Denton, A.H., Blackstone, S.R. et al. Access to Healthcare Among US Adult Refugees: A Systematic Qualitative Review. J Immigrant Minority Health 25, 1426–1462 (2023). https://doi.org/10.1007/s10903-023-01477-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-023-01477-2