
Abstract
Suicides in Hispanic adolescents have been increasing significantly. Less clear is the extent of suicides in Hispanic children younger than 12 years of age. The purpose of this study was to explore the trends and methods of suicides in Hispanic children from 2010 to 2019 (latest data available across the United States). Suicide is the 7th leading cause of death for Hispanic children. Hispanic child suicides statistically significantly increased during the decade. From 2010 to 2019, Hispanic child suicide rates increased by 92.3%. The suicide deaths were primarily in boys (59.6%) and among those 10–12 years of age (94.9%). Hispanic child suicides were most common in the West and South and least common in the Northeastern US The method used to commit suicide was overwhelmingly (76–85%) hanging/strangulation/suffocation. To help assure Hispanic children flourish and mature into healthy adults, it is essential that policymakers commit more resources for access to healthcare for all youths and that research funding for minorities include research regarding Hispanic children’s suicide risk factors, protective factors, and effective interventions to reduce suicides of Hispanic children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Suicide is an increasing public health crisis for most segments of the United States population. Most national studies on trends of suicide in the US population have focused on adolescents, adults, or the elderly [1,2,3]. While suicide is not common before puberty, it does occur in vulnerable children [4]. Contrary to popular belief, children are not too developmentally immature to engage in suicidal thoughts and behaviors (STBs include suicidal ideation, suicide planning, and suicide attempts) [5]. Research has found that between 4% and 13% of preschoolers have reported STBs [6, 7]. Development of the understanding of death as a biologically permanent event appears to universally develop between 4 and 7 years of age [8]. Furthermore, the development of the concept of suicide has been found in 10% of first graders, 50% of third graders, and 95% of fifth graders and is directly related to cognitive development and experiences with suicide [9]. Other research has found that by the third grade, school children have a well-developed understanding of suicide [10].
There are numerous recent studies that have explored various facets of STBs in children [11,12,13,14]. However, these studies have focused their research on the changing characteristics of suicide among Black and White children in the US Suicide research in Hispanic youths is mostly focused on Hispanic adolescents [1, 15,16,17]. Even when Hispanic children have been studied, there is conflicting evidence on the burden of suicide in Hispanic children. For example, a study using the Web-Based Injury Statistics Query and Reporting System (WISQARS) data from the Centers for Disease Control and Prevention (CDC) for the years 1992–2006 explored suicide rates for young persons 10–24 years of age who used hanging/suffocation or firearms. The study found that hanging/suffocation related suicide increased 26% for 10–14-year-old and 40% for Hispanic children, but suicides using firearms decreased 45% [18]. Whereas, a study of suicide trends in elementary school-aged children (9–11 years of age) from 1993 to 2012 that included Hispanic children did not find a statistically significant incidence rate ratio change during the 20-year interval [19]. While a study of hospitalizations for STBs in children’s hospitals from 2008 to 2015 found a statistically significant increase in the percent of youths (ages 5–17 years) who were Hispanic (10.4% in 2008/2011 to 12.1% in 2012/2015) [20]. Another study of child STBs that included Hispanics explored their perceived discrimination and STBs in children recruited at 9–10 years of age and followed up 1 year later. This study found that 5.5% of Hispanic children reported discrimination and 7.8% reported having engaged in STBs [21]. Hispanic children with high perceived discrimination had STBs 2.4 times the rate of Hispanic children who had lower perceived discrimination.
Given the inconsistent findings on trends in Hispanic children’s suicide and the lack of nationwide studies, we explored Hispanic child suicide rates and characteristics for the decade 2010 to 2019. This investigation is also critical as the Hispanic population is one of the largest ethnic minority populations and has grown considerably over the past 2 decades; in year 2000 they were 12.6% of the US population growing to 16% in 2010 and 18% by 2019 [22,23,24]. Also, Hispanics are the youngest racial/ethnic group in the US with a median age of 30. In 2000, Hispanic youths < 16 years of age were 17.2% of that age group, in 2010 and 2019 they comprised 23.5% and 25.8% respectively in this age group of youths [22,23,24]. Health issues affecting Hispanic children (< 13 years of age) can be expected to grow in a similar fashion. Thus, the purpose of this study was to provide additional and comprehensive evidence that characterizes Hispanic child suicides for the decade of 2010 to 2019.
Methods
We used the WISQARS data from the CDC to obtain Hispanic child suicide related data from 2010 to 2019 [25]. Childhood was defined as 12 years of age or younger. Annual numbers of suicides were aggregated in 2-year cycles to create adequate sample sizes to ensure stable estimates for assessing changes in incident rates over time. Descriptive statistics were used to characterize the findings. A Pearson’s correlation coefficient was calculated to assess whether there was a trend in suicide incidence rates with statistical significance levels set at p < 0.05.
Results
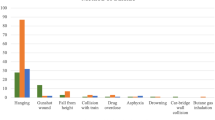
In 2019, Hispanic children 12 years of age or younger were 25.9% of that age segment of the U.S. population and they were 26.4% of all the suicides in that age category [22, 23]. Suicide is the 7th leading cause of death for Hispanic children 1–12 years of age. Analysis of rates of suicides from 2010 to 2019 found a 92.3% increase in the suicide rate (r = 0.87, p < 0.05) (Table 1). The Hispanic child suicides were predominantly observed in boys (59.6%, n = 130) with girls comprising 40.4% (n = 88) of the suicides. The vast majority (94.9%, n = 207) of Hispanic child suicides were observed among 10–12-year-old children. Hispanic child suicides were most common in the West (n = 82) and South (n = 80) and least common in the Northeast (n = 24) and Midwest (n = 32). Examination of methods used to commit suicide by Hispanic children found that strangulation/hanging/suffocation was responsible for 76–85% of suicides depending on the year examined (Table 2).
Discussion
Our findings provide evidence of a statistically significant increase from 2010 to 2019 in Hispanic child suicides, we found boys were more likely than girls to commit suicide, hanging/suffocation was the most common method employed to commit suicide, and the vast majority of the Hispanic child suicides were observed in older children [4, 26]. These trends align with suicides in children across all racial groups in the US [14]. Suicide rates have been rising in youths in general. Whether the Hispanic child suicide increase is part of a general trend or is due to unique circumstances of this population (e.g., lack of access to healthcare, unmet mental health needs, socioeconomic deprivation, etc.) is a matter of speculation [23, 24, 27].
Hispanics use mental health services at about half the rate of non-Hispanic whites [28]. There are several potential explanations for the lower use of mental health services in Hispanics (e.g., shame associated with mental illness, stigma and guilt, concerns about government identification and deportation, and some attribute suicide to a lack of faith more than to mental health issues) [28, 29]. Additionally, Hispanics do not have access to culturally and linguistically appropriate mental health services. A recent assessment found that Child and Adolescent Psychiatry fellows in training decreased by almost 40% between 2011 and 2020 [30]. These statistics are disconcerting since Hispanic youths are known to have higher rates of depressive symptoms and unmet mental health needs compared to youths from other racial/ethnic groups [17, 31]. In relation to socioeconomic deprivation, Hispanic children have higher rates of poverty (a risk factor for suicide). Hispanic youths are 50% more likely to be in poverty than their proportion in the US youth population. Hispanic youths had a poverty rate of 20.6% in 2019 compared to the rate of 8% for non-Hispanic whites. Poverty is also linked with lack of access to healthcare and health insurance (recent estimates suggest the lack of insurance to be 9.2% for Hispanic youth compared to 4.3% for non-Hispanic white youths under the age of 18 years) [24, 32,33,34].
Research on Hispanic health issues is generally lacking [24]. It should not be surprising that there are no rigorously evaluated and evidence-based strategies to reduce Hispanic child suicides. Prevention strategies for Hispanic child suicides can be explored through the lens of the public health prevention model and possibly based on strategies for adolescent suicide prevention, especially since no effective or evidence-based child suicide prevention programs are noted in existing literature [1, 5, 15,16,17, 35]. Primary prevention may seem like an appealing strategy to prevent child suicides which often focuses on means restriction [3, 14, 36]. However, means restriction in the case of hanging/suffocation would be extremely difficult, if not impossible. There are too many objects in homes that can be used for self-strangulation (e.g., ropes, pet leashes, clothes, belts, electrical cords, etc.). In addition, the empirical evidence on how to reduce STBs in elementary school children using primary prevention is extremely limited. It is also virtually impossible to predict which individuals will commit suicide [3, 14, 35,36,37]. The mental health field has focused efforts on mitigation of risk factors as a primary prevention strategy that is not grounded in evidence and can create false positives for individuals perceived to be at risk of suicide. However, a growing area of behavioral research emphasizes resilience; efforts to increase resilience may help children handle a variety of adverse circumstances that are linked with STBs. Such resilience building interventions can focus on creating ways to develop caring and nurturing relationships; teaching children empathy and social skills; conflict resolution and healthy relationships; educating parents about the importance of communication, connectedness, social support, and strong parent-child relationships and school-home relationships, just to name a few that have been suggested along with training for school personnel to identify children at risk [1, 6, 15,16,17]. Research also suggests that programs such as The Good Behavior Game and Signs of Suicide Prevention Program are effective at reducing STBs in youths [38,39,40].
Our analyses should be viewed in light of potential limitations. First, we did not have sufficient numbers of suicides to examine differences in suicide trends by gender. Second, we do not know whether classifying child suicide deaths changed from 2010 to 2019. Because hanging/suffocation/strangulation are the dominate methods used to commit suicide by Hispanic children and it is increasingly important to consider whether new trends like the Choking Game, Passing Out Challenge, the Blackout Challenge are contaminates of youth suicides [41, 42]. For example, the Choking Game is intentional asphyxiation as a means of inducing euphoric feelings before loss of consciousness and when the blood and oxygen rush back to the brain. The intention is to acquire euphoria and not end one’s life, but youths who engage in this game sometimes end up dying accidentally [41, 42]. Whether such deaths are classified as suicides or some suicides are classified as accidental deaths is unknown. However, to the extent that such misclassification occurs, this would impact child suicide rates. Third, important demographic variables (e.g., socioeconomic status, family composition, school enrollment and school characteristics, etc.) and suicide risk factors (e.g., psychopathology, social isolation and neglect, childhood adversity, etc.) could not be controlled for as the WISQARS database does not include these variables. Despite these limitations, this is the largest community-based and multiyear assessment of Hispanic child suicides and evidence from this study suggests that concrete steps should be taken by communities and policymakers to halt the rising rates of Hispanic child suicides.
Conclusions
Using WISQARS data, we explored the trends of Hispanic child suicides from years 2010 to 2019. We found that boys were more likely to commit suicide than girls and the vast majority of these Hispanic child suicides were observed in older children. The most frequently used method for suicide was hanging/suffocation, a method of suicide with high lethality. The decade we explored found a significant increase in Hispanic child suicides. These findings underscore the urgency to identify effective strategies to reduce STBs in Hispanic children. STBs can only be successfully reduced in children by greater investments in research related to risk and protective factors that influences STBs in children. Investments in research and prevention practice as it relates to STBs in children should be cross-sectoral and adopt frameworks such as the Social Ecological Model to address all the individual, interpersonal, and societal risk factors for STBs in children.
References
Price, J. H., & Khubchandani, J. (2017). Latina adolescents health risk behaviors and suicidal ideation and suicide attempts: Results from the national youth risk behavior survey 2001–2013. Journal of Immigrant and Minority Health, 19(3), 533–542.
Yockey, R. A., King, K., & Vidourek, R. (2021). Trends in suicidal behaviors among US adults 2015–2018. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 42(5), 351–359.
Price, J. H., Khubchandani, J., & Price, J. A. (2021). The rising tide of elderly African–American suicides: A call for action. Journal of the National Medical Association, 113(5), 493–498.
Dervic, K., Brent, D. A., & Oquendo, M. A. (2008). Completed suicide in childhood. Psychiatric Clinics of North America, 31(2), 271–291
Whalen, D. J., Hennefield, L., Elsayed, N. M., Tillman, R., Barch, D. M., & Luby, J. L. (2021). Trajectories of suicidal thoughts and behaviors from preschool through late adolescence. Journal of the American Academy of Child & Adolescent Psychiatry. https://doi.org/10.1016/j.jaac.2021.08.020
Whalen, D. J., Dixon-Gordon, K., Belden, A. C., Barch, D., & Luby, J. L. (2015). Correlates and consequences of suicidal cognitions and behaviors in children ages 3 to 7 years. Journal of the American Academy of Child & Adolescent Psychiatry, 54(11), 926–937.
Martin, S. E., Liu, R. T., Mernick, L. R., DeMarco, M., Cheek, S. M., Spirito, A., & Boekamp, J. R. (2016). Suicidal thoughts and behaviors in psychiatrically referred young children. Psychiatry Research, 246, 308–313
Panagiotaki, G., Nobes, G., Ashraf, A., & Aubby, H. (2015). British and Pakistani children’s understanding of death: Cultural and developmental influences. British Journal of Developmental Psychology, 33(1), 31–44
Normand, C. L., & Mishara, B. L. (1992). The development of the concept of suicide in children. OMEGA-Journal of Death and Dying, 25(3), 183–203
Mishara, B. L. (1999). Conceptions of death and suicide in children ages 6–12 and their implications for suicide prevention. Suicide and Life-Threatening Behavior, 29(2), 105–118
Bridge, J. A., Horowitz, L. M., Fontanella, C. A., Sheftall, A. H., Greenhouse, J., Kelleher, K. J., & Campo, J. V. (2018). Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatrics, 172(7), 697–699
Sheftall, A. H., Asti, L., Horowitz, L. M., et al. (2016). Suicide in elementary school-aged children and early adolescents. Pediatrics, 138(4), E20160436
Burstein, B., Agostino, H., & Greenfield, B. (2019). Suicidal attempts and ideation among children and adolescents in US emergency departments, 2007-2015. JAMA Pediatrics, 173(6), 598–600.
Price, J. H., & Khubchandani, J. (2021). Childhood suicide trends in the United States, 2010–2019. Journal of Community Health. https://doi.org/10.1007/s10900-021-01040-w.
Hall, M., Fullerton, L., FitzGerald, C., & Green, D. (2018). Suicide risk and resiliency factors among Hispanic teens in New Mexico: Schools can make a difference. Journal of School Health, 88(3), 227–236
Villarreal-Otálora, T., Jennings, P., & Mowbray, O. (2019). Clinical interventions to reduce suicidal behaviors in Hispanic adolescents: A scoping review. Research on Social Work Practice, 29(8), 924–938
Khubchandani, J., & Price, J. H. (2018). Violence related behaviors and weapon carrying among Hispanic adolescents: Results from the national youth risk behavior survey, 2001–2015. Journal of Community Health, 43(2), 391–399.
Bridge, J. A., Greenhouse, J. B., Sheftall, A. H., Fabio, A., Campo, J. V., & Kelleher, K. J. (2010). Changes in suicide rates by hanging and/or suffocation and firearms among young persons aged 10–24 years in the United States: 1992–2006. Journal of Adolescent Health, 46(5), 503–505
Bridge, J. A., Asti, L., Horowitz, L. M., Greenhouse, J. B., Fontanella, C. A., Sheftall, A. H., Kelleher KJ, Campo, J. V. (2015). Suicide trends among elementary school–aged children in the United States from 1993 to 2012. JAMA Pediatrics, 169(7), 673–677
Plemmons, G., Hall, M., Doupnik, S., Gay, J., Brown, C., Browning, W., et al. (2018). Hospitalization for suicide ideation or attempt: 2008–2015. Pediatrics, 141(6), E20172426.
Argabright, S. T., Visoki, E., Moore, T. M., Ryan, D. T., DiDomenico, G. E., Njoroge, W. F., Taylor JH, Guloksuz S, Gur RC, Gur RE, Benton TD, (2021). Association between discrimination stress and suicidality in preadolescent children. Journal of the American Academy of Child & Adolescent Psychiatry. https://doi.org/10.1016/j.jaac.2021.08.011.
Noe-Bustamante, L., Lopez, M. H., & Krogstad, J. M. U.S. Hispanic population surpassed 60 million in 2019, but growth has slowed. Pew Research Center. Retrieved July 7, 2020, from https://www.pewresearch.org/fact-tank/2020/07/07/u-s-hispanic-population-surpassed-60-million-in-2019-but-growth-has-slowed/
Frey, W. H. (2020). The nation is diversifying even faster than predicted, according to new census data. Metropolitan Policy Program. Washington D.C.: Brookings Institution
Price, J. H., & Khubchandani, J. (2016). Health education research and practice literature on Hispanic health issues: have we lost sight of the largest minority population? Health Promotion Practice, 17(2), 172–176
Centers for Disease Control and Prevention (2021). Web-based injury statistics query and reporting system (WISQARS): Fatal injury reports, 2010–2019, for national, regional, and states. Retrieved October 30th, 2021, from https://www.cdc.gov/injury/wisqars/index.html
Soole, R., Kõlves, K., & De Leo, D. (2015). Suicide in children: A systematic review. Archives of Suicide Research, 19(3), 285–304.
Act, C. (2021). Health insurance coverage and access to care among Latinos: Recent trends and key challenges. Retrieved October 30th, 2021, from https://aspe.hhs.gov/reports/health-insurance-coverage-access-care-among-latinos
Caplan, S. (2019). Intersection of cultural and religious beliefs about mental health: Latinos in the faith-based setting. Hispanic Health Care International, 17(1), 4–10
Jewers, M., & Ku, L. (2021). Noncitizen children face higher health harms compared with their siblings who have US citizen status: Study compares citizen and noncitizen siblings living in mixed-status families to determine differences in health insurance coverage and access to medical care. Health Affairs, 40(7), 1084–1089
Saboor, S., Naveed, S., Chaudhary, A. M. D., Safdar, B., Malik, S., & Khosa, F. (2021). Exploring gender and racial disparity in child and adolescent psychiatry: A step toward diversity. Journal of the American Academy of Child and Adolescent Psychiatry, 60(11), 1329–1332
Kann, L., McManus, T., & Harris, W. A., et.al (2018). Youth risk behavior surveillance—United States, 2017. MMWR Surveillance Summaries, 67(8), 1
Haider, A. (2021). The basic facts about children in poverty. Center for American Progress, January, 12. Retrieved October 30th, 2021, from https://www.americanprogress.org/article/basic-facts-children-poverty/
Semega, J., Kollar, M., Creamer, J., & Mohanty, A. (2019). Income and poverty in the United States: Current population reports, US Department of Commerce. [Online]. Retrieved October 4th, 2021 from www.census.gov/library/publications/2019/demo/p60-266.html
Keisler-Starkey, K., & Bunch, L. N. (2020). Health insurance coverage in the United States: 2019. Washington, DC: U.S. Census Bureau.
Robinson, J., Bailey, E., Witt, K., Stefanac, N., Milner, A., Currier, D., et al. (2018). What works in youth suicide prevention? A systematic review and meta-analysis. EClinicalMedicine, 4, 52–91.
Stanley, I. H., Hom, M. A., Rogers, M. L., Anestis, M. D., & Joiner, T. E. (2017). Discussing firearm ownership and access as part of suicide risk assessment and prevention: “Means safety” versus “means restriction”. Archives of Suicide Research, 21(2), 237–253
Paris, J. (2021). Can we predict or prevent suicide? An update. Preventive Medicine, 152, 106353
Wilcox, H. C., Kellam, S. G., Brown, C. H., Poduska, J. M., Ialongo, N. S., Wang, W., & Anthony, J. C. (2008). The impact of two universal randomized first-and second-grade classroom interventions on young adult suicide ideation and attempts. Drug and Alcohol Dependence, 95(Suppl 1), S60–S73
Kellam, S. G., Mackenzie, A. C., Brown, C. H., Poduska, J. M., Wang, W., Petras, H., et al. (2011). The good behavior game and the future of prevention and treatment. Addiction Science & Clinical Practice, 6(1), 73–85
Schilling, E. A., Aseltine, R. H., & James, A. (2016). The SOS suicide prevention program: Further evidence of efficacy and effectiveness. Prevention Science, 17(2), 157–166
Dake, J. A., Price, J. H., Kolm-Valdivia, N., & Wielinski, M. (2010). Association of adolescent choking game activity with selected risk behaviors. Academic Pediatrics, 10(6), 410–416
Toblin, R. L., Paulozzi, L. J., Gilchrist, J., & Russell, P. J. (2008). Unintentional strangulation deaths from the” Choking Game” among youths aged 6-19 years–United States, 1995–2007. Journal of Safety Research, 39(4), 445–448
Funding
This research received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Price, J.H., Khubchandani, J. Hispanic Child Suicides in the United States, 2010–2019. J Community Health 47, 311–315 (2022). https://doi.org/10.1007/s10900-021-01054-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-021-01054-4