
Abstract
Suicides are among the 10 leading causes of death in U.S. children 12 years of age and younger. The purpose of this study was to examine trends and methods of suicide in children by race and gender from 2010 to 2019, the most recent years of data available from the Centers for Disease Control and Prevention. Child suicides statistically significantly increased for black (95%), white (158%), male (95%), and female (300%) children during the decade. Additionally, the methods children used to commit suicide did not significantly differ by race or gender. The leading method of suicide used by children was strangulation/suffocation depending on race and gender (67%–85%). The second most common method of suicide was by the use of a firearm, again depending on race and gender (11%–30%). Northeastern states had the fewest child suicides during the decade and Texas and California had the most child suicides. Policymakers need to commit more resources and research funding to better detect risk factors, protective factors, and effective interventions for reducing child suicides.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Suicide related epidemiological research in the United States (U.S.) has traditionally focused on adolescents, adults, and the elderly [1,2,3]. However, in recent years there has been greater attention paid to suicide in children [4,5,6,7,8,9,10]. The first of the seven recent studies on child suicides used Web Based Injury Statistics Query and Reporting System (WISQARS) data on children 5 to 11 years of age for the years 1993-2012 [4]. In this study, it was found that an average of 33 children per year committed suicide and 84% of them were males. Over the two decades of the study data, white child suicides significantly decreased and black child suicides significantly increased for males but not for females. Hanging/suffocation was the main method of suicide (78%) followed by firearms (18%) and other methods (4%). Importantly, this was the first study to report higher suicide rates for black individuals compared to white individuals [4]. The second study compared children with typical development to children with psychiatric disorders [5]. The authors found that children less than 12 years of age were more likely to report suicidal ideation if they had a diagnosis of anorexia (50%), oppositional defiant disorders (ODD) (28%), depression/anxiety (22%), or attention deficit/hyperactivity disorder (ADHD) (20%). Suicidal ideation and attempts were significantly higher in children with a psychiatric disorder than in children without such illnesses [5]. The third study examined suicidal thoughts, plans, or attempts in children ages 3 to 7 years (n = 306) [6]. The authors found that 28 children had persistent thoughts about death and/or suicide, 5 had suicidal behavior or attempts, and 4 had suicidal plans and intent. Approximately, 11% (n = 34) of the children presented with suicidal thoughts, plans or attempts and 73% of these children in elementary school continued to have these suicidal cognitions and behaviors. Like the previous study [5], children with ADHD, ODD, and anxiety disorders, or depression were more likely to have suicidal cognitions and behaviors. The fourth of these major studies on childhood suicide trends in the US used the National Violent Death Reporting System (NVDRS) data from 2003 to 2012 for children ages 5 to 14 years [7]. The findings supported the previous study findings in that the children who died by suicide were more likely to be males, black, and died by strangulation/suffocation [4, 5]. Additional findings included the children usually died at home, approximately a third of them had a mental health issue, and 29% had disclosed their intent to commit suicide to another person. Relationship problems with family or friends were the dominant precipitating factors for the younger children to commit suicide. The next study explored suicide ideation and attempts in youths 5 to 18 years of age who presented to an emergency department [8]. Using the National Hospital Ambulatory Medical Care Survey (NHAMCS) data from 2007 to 2015, the authors found that 43% of youth visits for suicide ideation and attempts of youths 5 to 18 years of age occurred in children 5 to 11 years of age. The sixth study used WISQARS data for the years 2001 to 2015 and examined youths ages 5 to 17 years [9]. The authors found that 74% of the suicides were among black youths and 74% were among males. The key finding of this study was that among children 5 to 12 years of age, black children had a significantly higher (82%) suicide rate than white children. However, from 13 to 17 years, white youths had a suicide rate almost double the rate for black youths [9]. The final study of these seven major previous ones used the NVDRS data from 2013 to 2017 to do a content analysis of case narratives regarding the circumstances of suicide among children 5 to 11 years of age [10]. It was found that suicide by hanging/suffocation was the most common (78%) method followed by firearms (19%). All of the firearm deaths were due to unsafely stored firearms in the home. The vast majority of suicides occurred in child’s home (95.5%), most often the bedroom of the child. Almost one-third (31%) of the children had a mental health concern, 27% had experienced trauma (e.g. neglect, domestic violence, death of a family member/friend), 40% had family problems (e.g. parental substance abuse or divorce, family history of psychological problems, etc.), and school problems were found in 36% (e.g. suspension, bullying, change in school, etc.). On the day of suicide, 32% were disciplined, often about school related issues and 47% of this group were punished by being sent to their bedroom.
The purpose of the current study was to update the child suicide data by using the most recent data from WISQARS (2010 to 2019). In addition, we explored the child suicide data by race, gender, and methods of suicide used by each group. Finally, we identified the 10 states that had the highest number of child suicides during the decade of the study period.
Methods
The Web Based Injury Statistics Query and Reporting System (WISQARS) of the Centers for Disease Control and Prevention (CDC) was used to obtain childhood suicide data [11]. Childhood was defined as 12 years of age or younger. Annual numbers of suicide deaths were obtained by gender and race (black or white). Annual numbers of suicides were aggregated in 2 years blocks to ensure adequate sample size to assess changes in incident rates over time. Descriptive statistics were used to represent most findings. However, to assess gender and race incidence trends Pearson correlation coefficients were calculated and significance levels were established a priori at p < 0.05.
Results
In 2019, suicide was the 10th leading cause of death in the U.S. [11]. However, in 2019, for children 12 years of age or younger, suicide was the 9th leading cause of death for black children, 8th leading cause of death for male children, and 7th leading cause of death for both white children and female children in the U.S. During the decade 2010 to 2019, black children composed 16.2% of the child population and 24.1% of child suicides. In contrast, white children were 75.3% of the population but 68.3% of child suicides. Males were 51% of the child population and 66.7% of child suicides (females were 49% of the children’s population and 33.3% of child suicides).
Between 2010 and 2019, a total of 1,148 children 12 years of age or younger died by suicide, approximately 115 per year with 61,609 potential years of life lost before the age of 65 years. During this decade, black children consistently had higher rates of suicide than white children (Table 1). During this decade, the black child population decreased by 1.3% but the rate of suicides increased significantly (95.4%; r = 0.98; p < 0.05). The white child population decreased 2.5% during the decade and their suicide rate increased significantly (158%; r = 0.98; p < 0.05). An examination of gender distribution during this decade found that the number of male children decreased by 1.0% and the number of female children decreased by 1.1%. However, the rate of male child suicides increased significantly by 95.0% (r = 0.99; p < 0.05) and the rate of female child suicides increased significantly by 300% (r = 0.92; p < 0.05) (Table 1).
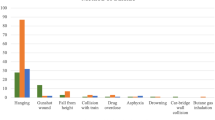
Analysis of child suicides by states found there were 12 states that did not report any child suicides during 2010-2019. These states were primarily located in the northeast (e.g., Delaware, Connecticut, Maine, New Hampshire, Rhode Island, and Vermont). However, based in part, on the size of the child population in some states, there were states that stood out for having a disproportionate share of child suicides (Table 2). Texas was the state with the most child suicides (n = 110) between 2010 and 2019 and California was ranked second (n = 69). Texas had a child suicide almost every month. The methods used by children to commit suicide in Texas were very similar to the total U.S. population of children who commit suicides (strangulation/suffocation = 67.3% and firearms = 30%). The two states with the highest child suicide rate were not among the top 10 states with the greatest number of child suicides, New Mexico (7.2 per million, n = 26) and Mississippi (4.2 per million, n = 22). Analysis of methods used by children to commit suicide were conducted based on race and gender. Regardless of race or gender, there were only two major suicide methods- strangulation/suffocation and firearms that accounted for 90% of all child suicides (Table 3). Strangulation/suffocation was the dominant method of child suicide, accounting for between two-thirds and 85% of the suicides depending on race and gender.
Discussion
We found there were statistically significant increases in the suicide mortality rates for black and white children and for both male and female children over the 2010 to 2019 decade. The two previous studies using the WISQARS data on child suicide found significant increases in suicides among black children but not among white children [4, 9]. This difference could be due to a difference in age ranges and due to differences in time periods that were used in the studies. One of the studies assessed change in suicide rates for girls but did not find a significant difference [4]. Whether the increases in suicide rates that we found were because of little being done to reduce suicides in children or whether what was implemented was ineffective would be sheer speculation without further research.
Our findings seem to highlight the considerable similarity in suicide methods used by children regardless of their race or gender. Strangulation/suffocation was the most common method of suicide by children and firearms were a distant second method for all children. Means restriction, especially in the case of firearms, is commonly touted as an important method of reducing suicides in youths [12, 13]. However, if means restriction of firearms is the major focus to reduce child suicides, such a focus would, at best, reduce child suicides by approximately 25%. In other words, safe storage of firearms and a federal Child Access Prevention (CAP) law would have very limited success against child suicides. In addition, means restriction of items to prevent strangulation/suffocation would be considerably more difficult than means restriction of firearms because of the variety of objects (e.g., ropes, belts, electrical cords, pet leashes, clothes, etc.) that could be used for self-strangulation. An analysis of child suicides by geographic location (e.g., state) found that many northeastern states reported no child suicides for a decade, potential evidence that child suicides can be averted. Texas was the state with the most child suicides during the decade, 59.4% greater than the second state in ranking (California). The top 10 states in prevalence of child suicides would seem to be ideal targets for funded interventions to reduce child suicides.
When we have talked with elementary school teachers and parents in child health workshops regarding child suicide the most commonly mentioned method thought to be used by children is poisoning. However, this study and previous studies have shown that typically fewer child suicides are by poisoning [7]. Such a misconception could cause parents to focus on a method of suicide that plays a minor role in child suicides while ignoring the major role of strangulation/suffocation. Also, critically important was the research confirming a central role for mental health issues in suicide intentions and behaviors [5, 6, 10] One of the studies found that ideation or attempts were 48 times higher in children with psychiatric diagnoses than in a typical group of children [5]. More than 90% of youths (e.g., teenagers) who commit suicide have a mental health condition [14]. To reduce suicide intentions and behaviors we support universal screening for suicidality across healthcare and school settings. For youths of color that needs to be culturally informed treatments by more racially congruent mental health professionals. Additionally, we need to address lack of insurance coverage, especially mental health coverage and services not being affordable. Stigma associated with mental health issues often leads to denial of such illness and avoidance of care.
This study had several potential limitations. First, we did not limit the lower age range for children who may have engaged in suicidal behaviors even though it is widely acknowledged that suicides before the age of 5 years are extremely rare [11]. Second, there is some evidence that black youths have a greater potential to have their suicides underreported [15]. To the extent this may have occurred, it would be a threat to the internal validity of the results. Third, we did not have adequate number of suicides for some racial groups (e.g., American Indian/ Alaska Native, and Asian/Pacific Islander children), thus these groups were not examined and could limit the generalizability of our findings on children’s suicide trends.
It should be noted that one the best possible ways to prevent child suicides is to approach it from a primary prevention perspective since the two methods of suicide used by children have high fatality rates. To consider the true burden of suicide in children, suicidal ideation, planning, and attempts must also be considered for effective prevention. Unfortunately, there is not much empirical evidence on how to reduce these cognitive concerns (e.g., suicidal ideation and planning) and completed suicides. Additional research is needed on child risk factors for suicide by race and gender with well-designed prospective studies and community trials. Research regarding child suicide and socioeconomic status, precipitating factors, family structure and functioning, stressors, and protective factors are inadequately understood. Until such information is available, programs such as The Good Behavior Game and Signs of Suicide Prevention Program have been reported to be effective in reducing suicide related behaviors and thoughts [16,17,18,19].
Conclusions
Using a national database (i.e., WISQARS), we found the child suicide rates by race and gender significantly increased from 2010 to 2019. In addition, the dominant methods used to commit suicide (suffocation/strangulation and firearms) were the same for all children 12 years of age or youngers regardless of race and gender. Suicide has now emerged as a leading cause of death in the U.S. The toll of suicide related deaths is increasing across the lifespan (i.e., from children to the elderly) and across the spectrum for various groups based on race and gender [1,2,3, 20, 21]. drop 19, add 21 Comprehensive suicide prevention strategies tailored to various population subgroups are few or lack rigorous evaluation. Investment in research, mental health services, and community-based prevention trials are urgently warranted to counter the rising burden of suicide related morbidity and mortality. Such investments should take a lifespan approach to suicide prevention and reduction with emphasis on schools, healthcare systems, and communities.
References
Price, J. H., & Khubchandani, J. (2019). The changing characteristics of African-American adolescent suicides, 2001–2017. Journal of Community Health, 44(4), 756–763.
Yockey, R. A., King, K., & Vidourek, R. (2021). Trends in suicidal behaviors among US adults 2015–2018. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 42(5), 351–359. https://doi.org/10.1027/0227-5910/a000732
Price, J. H., Khubchandani, J., & Price, J. A. (2021). The rising tide of elderly African-American suicides: a call for action. Journal of the National Medical Association, 46,1050–1058.1 https://doi.org/10.1016/j.jnma.2021.03.009
Bridge, J. A., Asti, L., Horowitz, L. M., Greenhouse, J. B., Fontanella, C. A., Sheftall, A. H., et al. (2015). Suicide trends among elementary school–aged children in the United States from 1993 to 2012. JAMA Pediatrics, 169(7), 673–677.
Mayes, S. D., Calhoun, S. L., Baweja, R., & Mahr, F. (2015). Suicide ideation and attempts in children with psychiatric disorders and typical development. Crisis, 36(1), 55–60.
Whalen, D. J., Dixon-Gordon, K., Belden, A. C., Barch, D., & Luby, J. L. (2015). Correlates and consequences of suicidal cognitions and behaviors in children ages 3 to 7 years. Journal of the American Academy of Child & Adolescent Psychiatry, 54(11), 926–937.
Sheftall, A. H., Asti, L., Horowitz, L. M., Felts, A., Fontanella, C. A., Campo, J. V., et al. (2016). Suicide in elementary school-aged children and early adolescents. Pediatrics, 138(4), e20160436.
Burstein, B., Agostino, H., & Greenfield, B. (2019). Suicidal attempts and ideation among children and adolescents in US emergency departments, 2007–2015. JAMA Pediatrics, 173(6), 598–600.
Bridge, J. A., Horowitz, L. M., Fontanella, C. A., Sheftall, A. H., Greenhouse, J., Kelleher, K. J., et al. (2018). Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatrics, 172(7), 697–699.
Ruch, D. A., Heck, K. M., Sheftall, A. H., Fontanella, C. A., Stevens, J., Zhu, M., et al. (2021). Characteristics and precipitating circumstances of suicide among children aged 5 to 11 years in the United States, 2013–2017. JAMA Network Open, 4(7), e2115683.
Centers for Disease Control and Prevention. (2021). Web-based Injury Statistics Query and Reporting System (WISQARS): Fatal Injury Reports, 2010–2019, for National, Regional, and States. Retrieved September 27, 2021, from https://www.cdc.gov/injury/wisqars/index.html
Fowler, K. A., Dahlberg, L. L., Haileyesus, T., Gutierrez, C., & Bacon, S. (2017). Childhood firearm injuries in the United States. Pediatrics, 140(1), e20163486.
Salhi, C., Azrael, D., & Miller, M. (2021). Parent and adolescent reports of adolescent access to household firearms in the United States. JAMA Network Open, 4(3), e210989.
Cavanagh, J. T., Carson, A. J., Sharpe, M., & Lawrie, S. M. (2003). Psychological autopsy studies of suicide: a systematic review. Psychological Medicine, 33(3), 395–405.
Mohler, B., & Earls, F. (2001). Trends in adolescent suicide: Misclassification bias? American Journal of Public Health, 91(1), 150
Wilcox, H. C., Kellam, S. G., Brown, C. H., Poduska, J. M., Ialongo, N. S., Wang, W., & Anthony, J. C. (2008). The impact of two universal randomized first-and second-grade classroom interventions on young adult suicide ideation and attempts. Drug and Alcohol Dependence, 95 (Suppl 1), S60–S73
Kellam, S. G., Mackenzie, A. C., Brown, C. H., Poduska, J. M., Wang, W., Petras, H., et al. (2011). The good behavior game and the future of prevention and treatment. Addiction Science & Clinical Practice, 6(1), 73–85
Schilling, E. A., Aseltine, R. H., & James, A. (2016). The SOS suicide prevention program: Further evidence of efficacy and effectiveness. Prevention Science, 17(2), 157–166.
Schilling, E. A., Lawless, M., Buchanan, L., & Aseltine, R. H., Jr. (2014). “Signs of Suicide” shows promise as a middle school suicide prevention program. Suicide and Life-Threatening Behavior, 44(6), 653–667
Price, J. H., & Khubchandani, J. (2021). Firearm suicides in the elderly: A narrative review and call for action. Journal of Community Health, 46, 1050–1058
Price, J. H., & Khubchandani, J. (2017). Latina adolescents health risk behaviors and suicidal ideation and suicide attempts: Results from the National Youth Risk Behavior Survey 2001–2013. Journal of Immigrant and Minority Health, 19(3), 533–542.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Price, J.H., Khubchandani, J. Childhood Suicide Trends in the United States, 2010–2019. J Community Health 47, 232–236 (2022). https://doi.org/10.1007/s10900-021-01040-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-021-01040-w