
Abstract
Human papillomavirus (HPV) vaccine was first recommended for female adolescents in the United States in 2006, and for male adolescents in 2011. In 2016, national HPV vaccine coverage was 43.4%, and slightly higher in Georgia (45.6%). Little is known about sub-state-level variation in HPV vaccination or Georgia specific research conducted to improve HPV vaccine uptake. We aimed to describe current uptake of HPV vaccination and synthesize Georgia-specific research of HPV vaccine uptake. We reviewed existing published and grey literature for different development, implementation and best practices related to vaccine uptake in adolescents. Studies measuring HPV vaccine uptake in Georgia utilizing quantitative, qualitative, or mixed-methods approaches were included alongside state-level information from National Immunization Survey-Teen, Community Health Needs Assessments, Behavioral Risk Factor Surveillance and Georgia Adolescent Immunization Surveys. Key findings across these reports were summarized. Forty-two titles and abstracts were identified through electronic database search for literature published between 2006 and 2017. Of these, five were from database sources and 37 were from additional sources. The most often mentioned barriers of HPV vaccine uptake in Georgia include cultural norms, vaccination education and a misalignment of vaccine uptake goals between the state and regional hospital community needs assessments. Increasing knowledge and uptake of HPV vaccine in Georgia requires significant research and to understand the vast socioeconomic, cultural and geographic barriers preventing uptake among adolescents. Georgia-specific efforts have been limited, however ongoing collaborations spearheaded by the Georgia Cancer Control Coalition provide opportunities for state-level support of research to address these barriers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Background
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States with about 79 million Americans currently infected [1]. Approximately 70% of cervical cancer cases are caused by HPV types 16 and 18 [2]. HPV also causes about 95% of anal cancers and 70% of oropharyngeal cancers [1]. Pap smear and HPV testing are common forms of secondary prevention of HPV-related cancers,[3] however no test for HPV infection or cytologic abnormalities in men is currently approved [1].
HPV vaccination provides a means of primary prevention. In 2006, HPV vaccination was recommended for adolescent females in the United States (US), with a recommendation for adolescent males in 2011 [4,5,6]. Currently, a nine-valent HPV vaccine (9vHPV) is recommended for use in the US, providing protection against HPV types that cause up to 90% of cervical cancers and 90% of genital warts [7].
In 2016, the National Immunization Survey-Teen (NIS-Teen) estimated that 67.3% of adolescents (aged 13–17) initiated the vaccine series in the state of Georgia (77.0% female and 58.0% male adolescents) while only 45.6% completed the full series (55.4% female and 36.2% male) [8]. National data from NIS-Teen 2016 estimated that 60.4% of adolescents initiated the vaccine (65.1% female and 56.0% male adolescents) and 43.4% of adolescents completed the vaccine (49.5% female and 37.5% male adolescents) [8]. Low HPV vaccine uptake in Georgia was identified as a priority area in the 2014–2019 Georgia Cancer Plan released by the Georgia Cancer Control Consortium (GC3), with a goal to reach 50% vaccine series completion for females and males by 2019 [9].
Why Is It Important to Do This Review?
While the NIS-Teen presents national-level HPV vaccine uptake by sociodemographic measures, it does not provide this level of detailed information for state-level estimates. With a population of more than 10 million and high diversity in terms of race (38.4% of the population is a racial minority), ethnicity (9.2% of the population is Hispanic or Latino) [10], and socioeconomic status (17.8% of the population live below the poverty level; 15.8% have no health insurance coverage), [10] understanding state-specific factors impacting HPV vaccine uptake is critical to reaching optimal HPV vaccine coverage levels.
Considering the current status of HPV vaccine uptake, as well as needs identified by the GC3, this review aimed to uncover and capture additional data on HPV vaccine series since its introduction in 2006, including more local vaccine uptake and research conducted specific to the population of Georgia. This can lead to more appropriate development and implementation of effective strategies accounting for this population level diversity to improve vaccine coverage. The goal of this review is to develop a greater understanding of the status of HPV vaccine, alongside its facilitators and barriers to uptake.
Objectives
The objective of this systematic review was to evaluate the current status of HPV vaccine in the state of Georgia and the needs identified for the vaccine since its introduction in 2006 while also considering the complex issues related to population-level diversity. This was done by reviewing the literature for different development, implementation and best practices related to vaccine uptake in males and females. The secondary aim was to generate a better understanding of the perceived benefits and barriers that might affect the status of the vaccine across the state. This systematic review answers the following questions:
-
1.
Is there currently a state level initiative in Georgia for the HPV vaccine? If so, who is leading it?
-
2.
What research has occurred specific to the state regarding the HPV vaccine? How can current programs (if any) be developed (or developed further) to increase the uptake of the vaccine among males and females in the state?
-
3.
What are the needs that have been identified by the state regarding the HPV vaccine?
-
4.
Are there existing barriers within the diverse population associated with race, ethnicity, socioeconomic status and urbanicity? If so, what can be done to alleviate these barriers?
The primary outcome of interest for this study was a synthesis of current information on the state of HPV vaccine uptake and research in Georgia alongside identifying unaddressed needs particularly regarding variability by race, ethnicity, urbanicity, and socioeconomic status.
Methods
Institutional Review Board Approval
This review is considered nonhuman subject research and therefore exempt, as it is existing, from Emory IRB approval. This review used public data with no health identifiers or personally identifiable information.
Participants (Eligibility Criteria)
Any study related to HPV vaccine in adolescents ages 9–26 in the state of Georgia were included. This incorporates interviews of parents and community members as well as data and evaluations on a state or district level. Any studies that refer to Georgia were also included. Only publications from 2006 to 2017 were accepted in the review. Adolescents who have either started an HPV vaccine series, completed a vaccine series or not started the series were included. This allowed for analysis of the current status of the vaccine within the state. Any information found on the current status of the HPV vaccine in the state of Georgia, the different barriers towards the vaccine and identified vaccine needs surrounding the vaccine have been included. Previous programs or interventions done by the state of Georgia have been considered in the review.
Setting
This is a systematic review of studies related to the HPV vaccine in the state of Georgia. Studies that utilized mixed methods (e.g. community health needs assessments) were used to extract findings that combined both approaches to understanding the state of HPV vaccine coverage in the state. National and state-level surveillance systems, such as the Georgia Adolescent Immunization Survey (GAIS) and the Behavioral Risk Factor Surveillance System (BRFSS), were also included, to gain information on surveillance data in the catchment area.
Assessments/Survey Instruments
Electronic Searches
Qualitative and quantitative studies were sought for this review through automated and manual search strategies. No study design filtering was imposed on the search. A date filter was imposed on the search for articles published between 2006 and 2017. Location filtering was utilized so that information regarding the vaccine in the state of Georgia is found. PubMed, MEDLINE, Web of Science, Popline, ACP Medicine, Alt HealthWatch and EMBASE were utilized (Table 1). Specific search strategies were created by one of the report authors (MHR), a Health Sciences Librarian with expertise in systematic review searching.
Searching Other Resources
In addition to the electronic resources used, there is also information on HPV vaccine uptake from key stakeholders throughout Georgia. These include reports from GAIS and BRFSS as well as CHNAs conducted across the state. Manual searches using online search engines were conducted to identify these reports and assessments.
Study Records
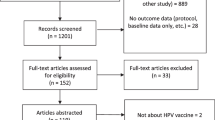
The review authors independently screened the titles and abstracts from the search against the inclusion criteria. Full reports were obtained for all titles that fit the inclusion criteria. After an independent screening, the review authors screened the full text reports together and determined if the reports fit the inclusion criteria (Fig. 1). Disagreement was resolved through discussion and records of excluded reports were maintained.

PRISMA flow chart diagram for systematic review of HPV vaccination in the state of Georgia
Statistical Analysis/Data Synthesis
Due to the variety of quantitative, qualitative and mixed study titles and abstracts pulled for this review, it was not possible to meaningfully pool data for meta-analysis or meta-synthesis from the 42 sources that were chosen for this review.
Findings
Thirty-three unique titles and abstracts were identified from the search terms through electronic database searches between the years of 2006–2017. Roughly half of the results provided abstracts or titles that were directly related to the state of Georgia (N = 14). Of the 14 results, five full-text papers met the inclusion criteria for the synthesis due to their relevance to the state of Georgia (Fig. 1). Forty-four additional records were identified through searches for Georgia adolescent immunization coverage and CHNAs, of which 37 met our eligibility criteria and were the most up-to-date documents for inclusion (Fig. 1).
Findings
Finding 1: Current State Level Initiatives for Improving HPV Vaccine Uptake Exist
The 2014–2019 Georgia Comprehensive Cancer Control Plan [9] identifies HPV as an issue of importance. As such the plan has two primary objectives related to increasing HPV vaccinations in the state. The first objective is to increase the number of adolescents who receive the vaccine to Advisory Committee on Immunization Practices (ACIP) standards [9]. Initiatives and strategies mentioned include engaging community-based organizations in implementing comprehensive culturally appropriate cervical cancer campaigns and programs targeted towards parents of young children to promote vaccine importance. The second objective is for pediatric providers to recommend HPV vaccination to parents of adolescents routinely by promoting the vaccine alongside adolescent vaccinations like Tdap and meningococcal vaccine (MCV4). The goal by 2019 is to achieve a 50% series completion rate in adolescents between 13 and 17 years old and to reduce annual cervical cancer incidence from 8.2 to 7.4 per 100,000 population [9].
Beyond its focus on HPV vaccination, the GC3 Plan also focuses on cancer screenings. Objectives include increasing genetic screening to low income and rarely screened women 18 years of age and older as well as sustaining community-based cervical cancer screening programs that screen at least 60% of women that are of racial and ethnic minority groups. An additional target by 2019 is to increase the proportion of women who receive cervical cancer screenings from 87 to 93% and to reduce income and insurance coverage disparities in cervical cancer screening rates by 10% [9].
Finding 2: Current Data on the HPV Vaccine Can Be Found in GAIS and NIS-Teen for Adolescents Across All Districts of the State However, Vaccine Uptake Varies by District
Since 2015, the GAIS report publishes rates of uptake among adolescents for recommended and required childhood and adolescent vaccinations by Georgia health district and sex, including comparisons of data from prior years. GAIS data is obtained through the Georgia Registry of Immunization Transactions and Services (GRITS) for cohorts of 7th grade children.
While gains have been made in state- and health district-level HPV vaccine series initiation and completion between the 2015 (overall initiation 42.5%; overall series completion 14.8%) and 2017 (overall series initiation 47.9%; overall series completion 23.3%) GAIS, vaccine coverage rates are still suboptimal (Table 2) [11,12,13]. Additionally, there is high variability between health districts, with a consistent difference in HPV vaccine series initiation of nearly 28% points between the highest and lowest performing health districts between 2015 (57.1% vs. 29.3% in the highest and lowest health districts, respectively) and 2017 (64.7% vs. 37.2% in the highest and lowest health districts, respectively), and an increasing disparity in HPV vaccine series completion between 2015 (19.9% vs. 8.5% in the highest and lowest health districts, respectively) and 2017 (34.3% vs. 16.6% in the highest and lowest health districts, respectively) [11,12,13].
Vaccine coverage rates in Georgia for adolescents aged 13–17 years are also reported by NIS-Teen (series initiation: 77.0% for females and 58.0% for males; series completion: 55.4% for females and 36.2% for males) [8]. These rates, which are higher than those reported through GAIS for adolescents in seventh grade, highlight that even for children who are receiving HPV vaccine, many are not getting it at the recommended ages.
Finding 3: HPV Vaccination Needs and Promotion of Cervical Cancer Prevention Are Lacking Significantly or Only Briefly Mentioned in Georgia Hospital Community Needs Assessments
The 2010 Patient Protection and Affordable Care Act (ACA) requires all nonprofit hospitals to conduct a Community Health Needs Assessment (CHNA) every three years to maintain tax-exempt status [14]. Georgia Watch Health Access Program reviewed 38 of the 82 first round CHNAs from Georgia nonprofit hospitals in 2013 finding that only 11 CHNAs used local data sources to determine community needs. It also found that few hospitals collected data on social determinants of health beyond education level, income and healthy food access. Additionally, Georgia Watch found that hospitals needed to focus their efforts on geographic areas with high concentrations of poverty instead of where the majority of the catchment population lived as it provided an incomplete picture of the community [14].
CHNAs from 2016 were reviewed to assess their coverage of HPV related topics in community needs. While some CHNAs addressed cervical cancer incidence rates and Pap test screenings [15,16,17] each lacks significant coverage of HPV vaccine coverage as a cancer prevention method or community needs related to HPV prevention. Some CHNAs [18, 19] mention the HPV vaccine as a preventive measure protecting against cervical cancer, alongside preventive screenings and pap smears [19]. These CHNAs also present information on HPV vaccine’s efficacy in preventing HPV related cancers and the importance of regular pap smears however, there is no mention of increasing these services within the catchment area of Memorial Hospital or if they are a community needs priority. The Stephens County Hospital CHNA also mentions a need for cancer prevention programming due to the various modifiable risk factors exhibited by its population [19], however it does not specifically aim to increase cervical cancer prevention programs.
In the Archbold Medical Center CHNAs [20,21,22,23] there was a mention of increasing free access to cervical cancer screenings through pap smears and increasing education on cervical cancer, but no mention of HPV vaccine. Five CHNAs stated that cancer prevention is a priority for their community needs, however, there is no mention HPV vaccination [24,25,26,27,28]. In the remaining CHNAs, there was no mention of cancer of any kind [26, 29,30,31,32,33,34].
Finding 4: Various Barriers for HPV Vaccine Exist and Vary Throughout the State of Georgia. Barriers Are Particularly Difficult to Overcome in Rural Areas and Among Minority Populations
We identified five articles that addressed Georgia-specific HPV vaccine uptake and barriers [35,36,37,38,39], and the findings from this research provide needed context to the vaccine coverage estimates summarized above.
With roughly 39% of its population being non-white and significant variability in socioeconomic status, Georgia has an extremely diverse population. Cultural barriers to the vaccine have been documented among Hispanic women caused by fears of embarrassment or stigma if they go to the clinic for vaccination or screening against HPV [35]. Additional barriers among Hispanic adolescents include fear caused by a lack of knowledge about HPV as well as cultural issues surrounding acceptability of sexual behavior, low English proficiency, distrust of healthcare, and general lack of information [36].
It has been shown that parental opinions of the HPV vaccine vary in rural communities among different racial and/or ethnic groups, and seemingly caused by a significant lack of access to HPV-related information [38]. In rural areas of Georgia, the local culture shapes people’s perceptions or risk of perceived vulnerability and people trust experts who have cultural backgrounds that are similar to their own [38]. Rural culture could be impacting access to information about healthcare interventions like the HPV vaccine as well as access to this preventative care [38]. Understanding cultural norms within these rural communities is essential when developing interventions aimed at increasing vaccine uptake.
Another potential barrier in Georgia’s rural counties is the pressure to conform to social norms and a fear of “what might others think” if women get vaccinated [37]. There is a significant lack of discussion of HPV related topics among physicians and adolescents in areas like Eastern Georgia [39]. Parents and physicians are more likely to vaccinate for HPV in older adolescents, although vaccinating at a younger age is more beneficial [39]. Underwood states that physician recommendation is critical for increasing vaccine uptake among adolescents, however significant barriers persist and prevent such recommendations.
Discussion
After reviewing Georgia county-level CHNAs, it is evident that cervical cancer and HPV vaccination are rarely, if ever, recognized among community needs. As HPV-related cancer rates increase and HPV vaccine uptake remains suboptimal, it is clear that increased education and efforts to increase uptake are critically needed. While state vaccine uptake initiatives exist, there is an apparent lack of emphasis on understanding cultural diversity throughout the state which presents significant issues impeding vaccine uptake. Although breast and cervical cancer screenings have been priorities identified by the GC3 Plan, CHNAs have not identified them as such and thus HPV vaccination and screenings for various cancers are commonly overlooked. The GC3 Plan has addressed the need to increase HPV vaccination coverage, however objectives outlined in the plan have not created improvements in education or understanding of HPV related risks in Georgia, therefore, vaccine coverage remains suboptimal. CHNAs conducted by individual hospitals throughout the state did not mention the GC3 Plan or its goals for 2019 suggesting a lack of communication of state-level goals with hospital needs assessment teams.
It remains evident that many challenges and complex barriers exist in Georgia, and targeted efforts are required to overcome and encourage increased uptake of HPV vaccine. While many parents remain concerned about HPV vaccine safety, HPV-related education and information dissemination is lacking; in turn preventing increased understanding and acceptance of the vaccine. Another barrier between physicians and parents creates confusion related to vaccine series timing, preventing further understanding of HPV vaccine related topics. Gender also appears to be a barrier with studies reporting that female adolescents have higher HPV initiation and completion rates compared to male adolescents [39]. Due to Georgia’s diverse population, there are barriers created by religious beliefs and cultural norms with complexities that must be addressed by culturally competent, but comprehensive, methods. Demographic and socio-economic differences also exist, requiring targeted strategies to encourage greater community engagement in health advocacy.
GAIS reports from 2015 to 2017 [11,12,13] present the variability of uptake of the HPV vaccine among adolescents in health districts throughout Georgia. Some districts consistently achieve high HPV vaccine coverage rates with others maintaining sub-optimal rates while other district’s vaccination rates fluctuate each year with no apparent reasoning. Vaccine coverage rates differ among males and female adolescents throughout all districts in Georgia, presenting a clear need for further research to understand potential causes of variation and the influences of yearly coverage rate fluctuation. GAIS has also began reporting coverage rates among private and public school adolescents, presenting yet another focus area which requires more research to understand motivators and barriers among this population.
There is limited research into the barriers and facilitators of HPV vaccination among Georgia residents. Notably, we found only five research articles specific to this population [35,36,37,38,39]. In the research that has been done, reports reiterate that barriers continue to persist throughout the state, but need greater attention to be overcome. Future research and public health practice should address targeted intervention efforts to increase HPV vaccine uptake across the state, with a focus on health districts with consistently low HPV vaccine coverage.
Conclusions
Since its first approval in 2006, HPV coverage has increased in Georgia. However, series completion has consistently remained below 50% for females and 40% for males. To increase HPV coverage rates in the state, the gaps in knowledge about the barriers that the state faces need to be addressed. This could be lead, in part, by the Georgia Department of Public Health alongside with Winship Cancer Institute and Georgia Cancer Coalition with further assistance provided by regional cancer coalitions. HPV vaccine importance is recognized within the GC3 Plan 2014–2019, but varied vaccine coverage rates present a need for new implementation strategies to be researched to increase uptake of the vaccine in Georgia. In reviewing district specific coverage rates and understanding the barriers that the state faces, targeted programs for implementation can be developed for diverse areas of Georgia.
There are groups focused on preventing cancer throughout the state, including the Georgia Cancer Control Consortium and its HPV Vaccine Working Group, the Winship Cancer Institute- the only NCI Designated Comprehensive Cancer Center in the state of Georgia- and regional cancer alliances. These groups urge the importance of early detection and screening efforts throughout the state for cervical cancer as well as increase education and promotion efforts for HPV vaccine. In understanding the landscape of the state and the barriers that affect the promotion of the HPV vaccine, greater coordination of efforts across these groups, and the stakeholders and partners they serve, is needed. Some strategic initiatives mentioned by the GC3 are to engage the community in culturally appropriate campaign programs which promote the vaccine to parents of young children [9]. In collaborating with groups like these, new strategies for promotion and coverage can be reached and identified leading to greater vaccine coverage.
Implications for Policy and Practice
-
The diverse population of Georgia presents many challenges to achieving high HPV vaccine coverage. This review summarizes the current state of the research and surveillance for HPV vaccination in Georgia, to provide a baseline for future policy development and public health practice activities.
-
There has been little research conducted specifically with adolescent populations in Georgia, which makes broad policy and practice initiative difficult to develop and implement, without appropriate context. This gap should be addressed by researchers in the state of Georgia.
-
The differences between Georgia Adolescent Immunization Survey data and National Immunization Survey-Teen data for Georgia highlights differences in age of vaccination that need to be addressed to ensure the highest level of protection for adolescents at the recommended ages of 11–12 years.
-
Local awareness to HPV vaccine needs is limited, and future community health needs assessments should address HPV vaccine-related disparities in the areas where these assessments are conducted.
References
National Cancer Institute. (2016). HPV and cancer. Retrieved October 26, 2018, from https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-fact-sheet.
Forman, D., de Martel, C., Soerjomataram, I., Lortet-Tieulent, J., & Franceschi, S. (2012). Global burden of human papillomavirus and related diseases. Vaccine, 20(5), F12–F23. https://doi.org/10.1016/j.vaccine.2012.07.055.
Cuzick, J., Bergeron, C., von Knebel Doeberitz, M., Gravitt, P., Jeronimo, J., Lorincz, A. T., & Szarewski, A. (2012). New technologies and procedures for cervical cancer screening. Vaccine, 30(5), F107–F116.
Centers for Disease Control and Prevention. (2006). CDC’s advisory committee recommends human papillomavirus virus vaccination. Retrieved October 26, 2018, from https://www.cdc.gov/media/pressrel/r060629.htm.
Centers for Disease Control and Prevention. (2011). Recommendations on the use of quadrivalent human papillomavirus vaccine in males—Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morbidity and Mortality Weekly Report, 60(50), 1705–1708.
Markowitz, L. E., Dunne, E. F., Saraiya, M., Lawson, H. W., Chesson, H., & Unger, E. R. (2007). Quadrivalent human papillomavirus vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and Reports, 56(Rr-2), 1–24.
Petrosky, E., Bocchini, J. A., Hariri, S., Chesson, H., Curtis, C. R., Saraiya, M., & Markowitz, L. E. (2015). Use of 9-valent human papillomavirus (HPV) vaccine: Updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR Morbidity and Mortality Weekly Report, 64(11), 300–304.
Walker, T. Y., Elam-Evans, L. D., Singleton, J. A., Yankey, D., Markowitz, L. E., Fredua, B., & Stokley, S. (2017). National, regional, state and selected local area vaccination coverage among adolescents aged 13–17 years—United States, 2016. Morbidity and Mortality Weekly Report (MMWR) Centers for Disease Control and Prevention, 66(33), 874–882.
Georgia Cancer Control Consortium. (2014). Georgia cancer plan 2014–2019. Retrieved October 26, 2018, from ftp://ftp.cdc.gov/pub/Publications/Cancer/ccc/georgia_ccc_plan.pdf.
U.S. Census Bureau. (2018). Demographic and housing estimates, 2012–2016 American community survey 5-year estimates (Georgia). Retrieved October 26, 2018, from https://factfinder.census.gov/bkmk/table/1.0/en/ACS/16_5YR/DP05/0400000US13.
Machado, F. R., Tuttle, J., Drensek, C., & Lovett, S. (2016). Georgia adolescent immunization study 2016. Retrieved October 26, 2018, from https://dph.georgia.gov/sites/dph.georgia.gov/files/2016GAIS.pdf.
Machado, F. R., Tuttle, J., Drenzek, C., & Lovett, S. (2017). Georgia adolescent immunization study 2017. Retrieved October 26, 2018, from https://dph.georgia.gov/sites/dph.georgia.gov/files/Adolescent%20Immunization%20Study%202017%20Final%20Report_Georgia.pdf.
Rema, M. T., Tuttle, J., Drenzek, C., & Lovett, S. (2015). Georgia adolescent immunization study 2015. Georgia department of public health immunization program acute disease epidemiology section. Retrieved October 26, 2018, from https://dph.georgia.gov/sites/dph.georgia.gov/files/Immunizations/2015%20GAIS%20Report%20final.pdf.
Stephens, B. (2015). Nonprofit hospital community health needs assessments in Georgia. Retrieved October 26, 2018, from http://www.georgiawatch.org/wpcontent/uploads/2015/06/Formatted-CHNA-Report-06022015-FINAL.pdf.
Georgia Health Policy Center. (2016). Grady community health needs assessment 2016. Retrieved October 26, 2018, from https://www.gradyhealth.org/resources/pdfs/GHS%20Community%20Health%20Needs%20Assessment%202016.pdf.
Professional Research Consultants Inc. (2015). 2015 Community health needs assessment: Muscogee County, Georgia. Retrieved October 26, 2018, from https://columbusregional.com/media/1588/2015-chna-report-muscogee-county-gapdf.pdf.
WellStar Health System. (2016). Wellstar: Implementation strategy 2016 community health needs assessment 2016. Retrieved October 26, 2018, from https://www.wellstar.org/about-us/documents/chna/chna_implementation_strategy_2016.pdf.
Draffin & Tucker LLP (2016). 2016 Memorial hospital and Manor community health needs assessment: Decatur and Seminole Counties. Retrieved October 26, 2018, from https://www.mh-m.org/wp-content/uploads/2017/08/chna-2016.pdf.
Draffin & Tucker LLP (2016). 2016 Stephens County hospital community health needs assessment: Stephens and Franklin Counties. Retrieved October 26, 2018, from http://stephenscountyhospital.com/fullpanel/uploads/files/health-needs-assessment-2016.pdf.
Archbold Medical Center. (2018). Brooks County—2016–2017 community health needs assessment. Retrieved October 26, 2018, from https://archbold.org/uploads/groups/3/documents/Brooks-KeyHealthIssues-2016-Aug18.pdf.
Archbold Medical Center. (2018). Grady County–2016–2017 community health needs assessment. Retrieved October 26, 2018, from https://archbold.org/uploads/groups/3/documents/Grady-KeyHealthIssues-2016-Aug18.pdf.
Archbold Medical Center. (2018). Mitchell County—2016–2017 community health needs assessment. Retrieved October 26, 2018, from https://archbold.org/uploads/groups/3/documents/Mitchell-KeyHealthIssues-2016-Aug18.pdf.
Archbold Medical Center. (2018). Thomas County—2016–2017 community health needs assessment. Retrieved October 26, 2018, from https://archbold.org/uploads/groups/3/documents/Thomas-KeyHealthIssues-2016-Aug18.pdf.
Gwinnett Medical Center. (2016). Gwinnett community health needs assessment 2015–2016. Retrieved October 26, 2018, from https://gwinnetthospital.thehcn.net/content/sites/gwinnetthospital/Gwinnett_2016_CHNA_Final.pdf.
Meadows Regional Medical Center. (2016). Community health needs assessment. Retrieved October 26, 2018, from http://meadowshealth.com/documents/Toombs-CHNA.pdf.
Northeast Georgia Medical Center. (2016). Community health needs assessment. Retrieved October 26, 2018, from https://www.nghs.com/fullpanel/uploads/files/nghs-chna-report-2016.pdf.
South Georgia Medical Center. (2016). South Georgia medical center community health needs assessment and implementation plan. Retrieved October 26, 2018, from https://www.sgmc.org/sites/www/Uploads/files/CHNA/SGMC%202016%20CHNA%20Report%20(1-17-17)%20%20.pdf.
Taylor Regional Hospital. (2016). Community health needs assessment Taylor regional hospital. Retrieved October 26, 2018, from https://taylorregional.org/pdfdocs/CHNA-2016.pdf.
Broyard, F., III, & Hui, E. (2015). Community health needs assessment 2015. Retrieved October 26, 2018, from https://www.piedmont.org/media/file/2015-CHNA-Athens.pdf.
Coffee Regional Medical Center. (2013). Coffee Regional Medical Center: 2013 community needs assessment. Retrieved October 26, 2018, from https://www.coffeeregional.org/wp-content/uploads/2013/12/Community%20health%20needs%20assesment%202013-final.pdf.
Phoebe Putney Memorial Hospital. (2016). Phoebe Putney Memorial Hospital 2016 community health. Retrieved October 26, 2018, from http://www.phoebehealth.com/media/file/CHNA/CHNA_PPMH2016.pdf.
Piedmont Healthcare. (2016). Piedmont healthcare community health needs assessment. Retrieved October 26, 2018, from https://www.piedmont.org/media/file/2016-CHNA-Full-Report.pdf.
Southeast Georgia Health System. (2016). Camden campus community health needs assessment. Retrieved October 26, 2018, from https://www.sghs.org/documents/Community-Benefits/community-health-needs-assessment-camden-2016.pdf.
University Health Care System. (2016). 2016 community health needs assessment. Retrieved October 26, 2018, from https://www.universityhealth.org/fullpanel/uploads/files/chna%20-%20final.pdf.
Luque, J. S., Mason, M., Reyes-Garcia, C., Hinojosa, A., & Meade, C. D. (2011). Salud es Vida: Development of a cervical cancer education curriculum for promotora outreach with Latina farmworkers in rural southern Georgia. American Journal of Public Health, 101(12), 2233–2235.
Luque, J. S., Raychowdhury, S., & Weaver, M. (2012). Health care provider challenges for reaching Hispanic immigrants with HPV vaccination in rural Georgia. Rural and Remote Health. 12(2).
Thomas, T. L., Strickland, O., Diclemente, R., & Higgins, M. (2013). An opportunity for cancer prevention during preadolescence and adolescence: Stopping human papillomavirus (HPV)-related cancer through HPV vaccination. Journal of Adolescent Health, 52(50), S60–S68.
Thomas, T. L., Strickland, O., Diclemente, R., Higgins, M., & Haber, M. (2012). Rural African American parents’ knowledge and decisions about human papillomavirus vaccination. Journal of Nursing Scholarship, 44(4), 358–367.
Underwood, N. L., Weiss, P., Gargano, L. M., Seib, K., Rask, K. J., Morfaw, C., & Sales, J. M. (2015). Human papillomavirus vaccination among adolescents in Georgia. Human Vaccines & Immunotherapeutics, 11(7), 1703–1708.
Acknowledgements
This project was supported by the National Cancer Institute, through an administrative supplement to the Winship Cancer Institute Cancer Center Support Grant (3 P30 CA138292-09S2). The funding agency had no role in the conceptualization, design, or scripting of the systematic review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical Approval
The project supporting this work was reviewed and approved by the Emory University Institutional Review Board.
Human Rights and Informed Consent
This report was a review of existing materials, and did not involve any human subjects research, and did not require informed consent.
Rights and permissions
About this article

Cite this article
Dennison, C., King, A.R., Rutledge, H. et al. HPV Vaccine-Related Research, Promotion and Coordination in the State of Georgia: A Systematic Review. J Community Health 44, 313–321 (2019). https://doi.org/10.1007/s10900-018-0589-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-018-0589-7