
Abstract
During slot machine gambling, near-miss outcomes occur when the final winning icon lands one position off the pay-line. To understand how near-misses promote gambling behaviour in healthy populations, autonomic arousal is often used to index outcome response valence. Findings remain equivocal, possibly owing to the limited ecological validity of computer simulations. Relevant psychological traits, such as impulsivity, which increase the risk of problem gambling, are often not examined. Here, we used immersive virtual reality (VR) to investigate near-miss-induced changes in physiological arousal and VR gambling behaviour. Sixty adult participants with no history of problem gambling were immersed in a VR casino-bar where they engaged with a self-selected slot machine. Real-time heart rate (HR) data were acquired during immersion. Within-subjects analyses were conducted on HR and post-reinforcement pauses (PRPs; i.e., time taken to initiate next-spin) across wins, losses and near-misses. Significant HR acceleration occurred for both near-misses and losses compared to wins, indexing an initial orientation response. Both types of losses were associated with faster next-spin responses. Near-misses did not apparently have unique HR or PRP profiles from losses, although this may reflect our loss control condition, which in itself may have been a subtler near-miss outcome. Impulsivity measured by the SUPPS-P was not associated with near-miss responses. Losses may encourage gambling as participants experience more immediate HR acceleration (indexing arousal unique to losing) and initiate faster responses. Future studies should clarify this effect by investigating problem gambling cohorts and develop VR paradigms taking into consideration the current findings and limitations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gambling disorder affects 0.5–5% of the general population (Williams et al. 2012). Slot machines are widely considered the most addictive form of gambling and are consistently associated with the greatest gambling-related harms (Dowling et al. 2005; Gainsbury et al. 2014; Productivity Commission 2010). These harms include detriments to personal health, financial difficulties, work performance, relationship conflict and criminal activity both in the gambler and affected others (Productivity Commission 2010; Li et al. 2017). These machines are thought to be uniquely alluring because of their structural characteristics which are designed to induce ongoing gambling (Parke and Griffiths 2006). These characteristics include visual and sound effects, more frequent rewards than expected from chance (e.g., ‘losses disguised as wins’), and strategic inclusion of near-misses (Parke and Griffiths 2006; Sharman et al. 2015). Despite substantial investigations of the significance of near-misses, their effects on gambling remain unclear (Barton et al. 2017). By understanding near-misses, we can start to target this characteristic directly in treatment, and guide harm minimisation policies (Griffiths 1993; Dixon and Schreiber 2004; Yücel et al. 2017, 2018).
Near-misses are losses that physically resemble a jackpot win, but fall just short on the final, winning icon (Reid 1986). In games of skill, such as a sport (e.g., football), near-misses are useful cues as they provide feedback suggesting that a win may be within reach (e.g., just missing the goal). By contrast, slot machines are games of chance, whereby near-miss outcomes give no indication of future success since individuals have no actual control over the outcome (Reid 1986). In spite of this, individuals may perceive near-misses as evidence of having personal control over gambling outcomes (Clark et al. 2012). Furthermore, near-misses may induce frustration as the goal (of winning) is not fulfilled (Reid 1986). Such frustration may be the catalyst encouraging ongoing behaviour (Amsel 1958, 1992), ultimately leading to harmful gambling. Near-misses have been identified as a key feature in developing harmful gambling (Griffiths 1991; Clark et al. 2009; Yücel et al. 2017), and knowing this, gambling industries purposefully design slot machines to manipulate the probability at which these outcomes occur (Harrigan 2009). Gamblers and non-gamblers show different responses to near-misses (Chase and Clark 2010; Ulrich et al. 2016), which identifies the need to foremost understand near-miss responses in a healthy population.
Psychophysiological measures of autonomic arousal offer an objective measure to understand the impact of near-misses beyond self-report methods (Clark et al. 2012; Dixon et al. 2010). Changes in heart rate (HR) have consistently been used to index excitement from slot machine gambling (Anderson and Brown 1984). HR is a marker of autonomic arousal which follows a biphasic response to emotional stimuli, whereby an initial deceleration is followed by acceleration (Bradley and Lang 2000; Clark et al. 2012). Deceleration is thought to reflect anticipation or orientation to a stimulus, whereas the subsequent acceleration has been linked to the emotional processing of a stimulus (Bradley and Lang 2000). An overview of the slot machine literature demonstrates that near-misses yield unique HR profiles from wins and losses although findings are heterogeneous across studies (see Table 1), with differences found in both the deceleration and acceleration components. Resolving how HR responds to near-misses will provide insights into how these events differ from other outcomes, leading the way for future valence inferences.
At a behavioural level, near-misses have also been shown to function similarly to wins, presumably by encouraging and extending time on device (Reid 1986; Kassinove and Schare 2001; Barton et al. 2017). The time taken to initiate the next spin following the receipt of an outcome is known as a post-reinforcement pause (PRP; Belisle and Dixon 2016), which is thought to be an important variable in understanding persistence after near-misses. Like psychophysiological arousal research, findings have been inconsistent (Table 1). Shorter PRPs following near-misses may reflect a desire to quickly alleviate the frustration from nearly-winning (Dixon et al. 2011). Alternatively, a near-miss PRP more similar to a win PRP may reflect stimulus generalisation, indicating that near-misses may be hedonically pleasurable as they appear visually similar to a win (Belisle and Dixon 2016). As near-misses are financially no different from losing, it is important to elucidate the mechanisms underpinning the encouragement and motivation of continual gambling.
Over and above autonomic arousal, traits tapping into inhibitory control have also been linked to the reinforcing effects of slot machine gambling (Lutri et al. 2018). For example, reduced inhibitory control is associated with high trait impulsivity, and impulsive individuals show greater HR responses while gambling on blackjack in a real-world casino (Krueger et al. 2005). Little is known, however, about how impulsivity relates to HR changes in response to slot machine gambling outcomes. To our knowledge, only one study has investigated impulsivity and HR response to winning, losing and nearly-winning, using a computerised slot machine simulation (Lole et al. 2012). They found no relationship between impulsivity and participants’ HR changes. Examining whether impulsivity is associated with the arousal elicited by near-miss events may help to clarify the development and maintenance of gambling harm (Lole et al. 2012), as it is conceivable that more impulsive individuals may find near-miss events more arousing.
To date the majority of near-miss research has used two-dimension desktop computer delivered slot machine paradigms. These slot machine simulations lack ecological validity, which may be contributing to the variable results of research in this area. Gambling paradigms that better replicate the real-world gambling experience may be a way to resolve this variability and elicit stronger more realistic psychophysiological near-miss responses from gamblers. Immersive virtual reality (VR) simulations provide an excellent opportunity to achieve this. There is emerging evidence that VR gambling environments can induce gambling cravings (Giroux et al. 2013; Bouchard et al. 2014, 2017) and these cravings have been induced in frequent gamblers by simply walking around a virtual casino (Park et al. 2015).
This study sought to use an immersive VR gambling environment to better understand autonomic arousal and behavioural responses to near-miss outcomes within a healthy sample, and whether impulsivity was related to such responses. In keeping with previous findings (Clark et al. 2012, 2013), we hypothesised that near-misses would be associated with greater HR acceleration compared to wins and losses. Secondly, we hypothesised that near-misses would be associated with shorter PRPs than wins and losses, reflecting the time delay associated with the processing of appetitive outcomes. As a secondary aim, we investigated whether trait impulsivity was linked to HR and PRP responses.
Methods
Participants
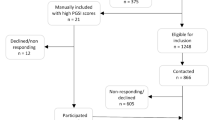
Sixty participants (27 female) aged 18–54 years (M = 23.82, SD = 8.26) were recruited online using social media (i.e. Facebook; see Fig. 1). Inclusion criteria required participants to be fluent in English and have corrected to normal or normal vision. Participants were excluded if they met criteria for history of problem gambling as determined by the National Option Research Center Diagnostic Screen (NODS; Gerstein et al. 1999), were currently taking psychotropic medications, had self-reported lifetime history of mental illness or neurological condition, or reported having experienced severe motion sickness, as this can severely limit presence within virtual environments (Witmer and Singer 1998; Moss and Muth 2011). Eligibility was ascertained through a telephone screen. Three participants experienced moderate motion sickness during VR immersion and their testing session were halted mid-way through. Their data was excluded from analysis. Ethics approval was obtained from the Monash University Human Research Ethics Committee, and written informed consent was obtained from all participants. Participants were informed that their reimbursement for the study would depend on how much they won; that they could keep their remaining funds (pre-determined at $20) in the form of a gift voucher displayed on the machine at the end of the gambling session.

Recruitment process detailing exclusion criteria
Virtual Reality Equipment
A HTC Vive headset with over-ear surround sound headphones was used. The VR environment was a custom-made Unity-coded software developed in collaboration between the Turner Institute for Brain and Mental Health and SensiLab (Faculty of Information Technology, Monash University). Two wireless base stations detected head movements, which controlled the direction an individual was facing in the virtual environment, while participants were seated throughout immersion and a Logitech hand-held controller was used by the dominant hand for walking.
Virtual Reality Slot Machine Simulation
Visual features of the virtual slot machines varied by external lights and colours, but all displayed an identical 4-reel design with a single pay-line (see Fig. 2). Reel design was purposefully designed as an extension of a previously validated 2-reel paradigm (Clark et al. 2009). Participants commenced machine use with $50 virtual money and bet amount was fixed at $1. Wins occurred when all four reels displayed the same icon. Losses occurred when reel combinations comprised three matching icons and one incongruous icon. Near-misses were similar to losses however the fourth and final winning icon landed exactly one position off the pay-line, representing a ‘near-win’ (see Fig. 3). We chose our loss design to control for the exact moment participants realised that they had lost (i.e., the outcome was always reliant on the forth reel). This also ensured that there was a sufficiently long spin-up period in which participants could use the machines without pausing in-between each trial (contributing to the overall immersion of the experience) while ensuring an ample HR recording window.

Screenshot of a virtual reality slot machine showing the single 4-reel design

Pokies machine outcomes. a Wins occurred when all four icons were identical. b Near-misses occurred when the winning icon was one position either before or after the pay-line. c Losses occurred when the winning icon was neither side of the pay-line
Wins resulted in a $5 pay-out in virtual currency and were accompanied by a ‘jackpot’ audio-visual presentation of ‘fireworks’ filling the screen with the sound of money falling into a coin tray. Both losses and near-misses resulted in a $1 loss. The schedule of wins, near-misses and losses were predetermined as 12 wins, 24 near-misses and 54 losses, counterbalanced and randomised in six blocks of fifteen reel spins to ensure an even distribution of outcomes (Belisle and Dixon 2016). Kassinove and Schare (2001) found, compared to 15% or 45%, near-misses occurring in 30% of trials lead to greater gambling persistence. Our near-miss schedule (26.67%) was chosen based on past near-miss research and is in keeping with the ideal proportion of near-miss outcomes previously cited (Clark et al. 2009, 2012). Stimulus presentation was fixed, with participants receiving the same order of trials. At the end of 90 trials, all machines finished with $20 of total funds remaining. The total spin time prior to landing for each of the first three reels (M = 2.5 s, range = 2.4–2.6 s) and the final reel (M = 5.0 s, range = 4.8–5.2 s) was counterbalanced across outcome type (wins, near-misses and losses) within blocks, to prevent HR response habituation.
The software was programmed to send triggers to LabChart (Version 8; ADInstruments, Sydney, Australia), marking stimuli on psychophysiological traces as they occurred in real-time. Triggers were sent to mark when each reel landed and when participants pressed the controller to initiate each new trial (i.e. when all reels were spun).
Heart Rate Acquisition
HR was recorded using an ADInstruments PowerLab and Bio-Amplifier. Data was acquired in LabChart and sampled at 1000 Hz with a 35 Hz low-pass filter. Three disposable pre-gelled Ag/AgCl electrodes were used to record HR data and positioned on the sternum, between the left-torso 9th and 10th ribs, and on the left tricep (ground electrode).
Psychological Measures
Gambling Pathology
The NODS is a validated 17-item telephone screen used to measure lifetime history of DSM-V defined criteria of pathological gambling (Hodgins 2002). Scores of 0 indicate no history of pathological gambling, scores of 1 or 2 suggests an individual may have been “at-risk” for problem gambling, scores of 3 or 4 indicate a potential subclinical syndrome of pathological gambling (i.e. problem gambling) and a score of 5 or more indicates pathological gambling (Toce-Gerstein et al. 2003). The Problem Gambling Severity Index (PGSI; Ferris and Wynne 2001) is a self-administered questionnaire which was used to measure current gambling severity in analysis.
Impulsivity
The short 20-item version of the UPPS-P Impulse Behaviour Scale (SUPPS-P; Cyders et al. 2014; Lynam 2013) was used to measure impulsivity. The UPPS-P includes five impulsivity subdomains: negative urgency, positive urgency, lack of premeditation, lack of perseverance and sensation seeking. The short version is considered a valid and reliable equivalent of the UPPS-P which is sensitive to gambling-related impulsivity in at-risk and healthy populations (Blain et al. 2015; Cyders et al. 2014).
Presence
The presence questionnaire (PQ; Witmer and Singer 1998) measures the extent to which individuals experience a sense of “being there” in a virtual environment. Twenty-two items are marked on a seven-point scale with three anchor ratings that depend on the question, such as never, occasionally and often. A higher total score indicates more immersion and is related to increased emotion experienced in VR (Robillard et al. 2003).
Procedure
Prior to immersion participants completed the PGSI, the SUPPS-P and the simulator sickness questionnaire (SSQ; Kennedy et al. 1993) to rule out pre-existing motion sickness symptoms scored as moderate or higher. They were then fitted with the VR headset and invited to explore the casino simulation in a demonstration period before testing commenced in order to familiarise them with the hand-held controller. They were free to explore the sports room, bar area, and slot machine area (see Fig. 4) at their leisure. They then exited VR and repeated the SSQ to check for immersion motion sickness.

The three rooms in the virtual reality casino-bar. a The sports room, b the bar area and c the pokies room
Participants then entered the VR environment again and were instructed to choose a machine to gamble on for approximately 15–20 min. Participants were asked not to change machines during this time. Following the slot machine use, participants exited VR and filled out the PQ.
HR Data Analysis
Inter-beat intervals (IBIs), the temporal distances in milliseconds between the R-waves of consecutive heart beats (Dixon et al. 2011), were extracted from HR data. For each trial (i.e. reel spin), seven IBIs were extracted (see Fig. 5). One IBI was extracted for the period immediately preceding the outcome presentation (baseline), one for the period around outcome delivery (outcome) and five following the outcome period (IBIs 1-5). PRP data were measured in milliseconds from the final reel stopping until the next spin was initiated (see Fig. 5).

Visual representation of the measurement of inter-beat intervals (IBI) and post-reinforcement pause (PRP) data in LabChart (ADInstruments, Sydney, Australia)
Data were averaged separately for each participant across wins, near-misses and losses and mean IBI and PRPs were calculated for each event. Outlier (> ±3.29 SD from the mean; Field 2013) checking revealed no outliers for IBIs and 10% of outlier values for PRPs. These data points were replaced with the next highest (non-outlier) value (Field 2013). Three participants were excluded from analyses due to PQ scores < 2 standard deviations below the mean (M = 86.72, SD = 14.25) indicative of poor VR immersion (Witmer and Singer 1998).
Data Analysis
HR data was analysed using two-way (3 × 7) repeated measures analysis of variance (rmANOVA) with outcome (win, loss and near-miss) and time (baseline, outcome and IBIs 1-5) within-subjects factors. To determine where outcomes differed in the time course, contrasts were performed between outcomes for each IBI compared to the proceeding IBI to establish the nature of this change. An independent rmANOVA analysed PRP with outcome as the within-subjects factor. Mauchly’s test was used to assess for violations in sphericity, and Greenhouse–Geisser corrections were applied where necessary. An alpha of p < .05 was used, and Bonferroni corrections for multiple comparisons were applied within each contrast (p < .017, when multiplying p < .05 by 3 to adjust for wins, losses and near-misses).
To explore whether trait impulsivity was associated with HR and PRP changes, non-parametric correlational analyses were conducted. Variation scores between wins and losses, wins and near-misses and losses and near-misses were created between total average PRPs and between each successive IBI (e.g., between baseline and outcome, outcome and IBI1, IBI1 and IBI2, etc.) This was to ascertain whether a variation in response between each outcome may be linked to SUPPS-P score.
Previous near-miss research (Clark et al. 2013; Sharman and Clark 2016) has differentiated between the final reel landing before or after the pay-line (suggesting a motivating or aversive effect, respectively). Our analyses revealed no significant differences between these two types of near-misses in terms of HR profiles [F(2.40,120.04) = .21, p = .846] and PRP lengths [t(50) = − 1.35, p = .188] therefore, all analyses herein average across near-misses from either side of the pay-line.
Results
Sample Characteristics
The final analysis was conducted on 51 participants (25 female), with an age range of 18–54 (M = 23.59 years, SD = 7.79). According to the PGSI, 33 participants classified as non-problem gamblers, 14 low-risk, and 4 moderate-risk, while no participants met criteria for problematic gambling behaviour. Of the low-risk and moderate-risk participants, 35.7% and 75% had gambled on slot machines at least once in their lifetime, respectively. No participants gambled on slot machines weekly. The PQ showed a mean score of 88.39 (SD = 12.66), corresponding to a moderate level of presence in a virtual environment (Witmer and Singer 1998), which was considered to validate our VR approach in this study.
HR
Figure 6 shows change in HR across time, as indexed by change in IBIs. The rmANOVA revealed a significant main effect for time [F(2.90, 145.10) = 47.05, p < .001], supporting a biphasic response of an initial deceleration component at the outcome followed by an acceleration. A significant main effect of outcome was also found [F(2, 100) = 3.35, p = .039], suggesting different HR profiles between outcomes. The rmANOVA revealed a significant interaction effect between outcome and time [F(4.88, 244.02) = 2.99, p = .013], suggesting that as time progressed following the outcome, IBIs differed depending on the outcome. This was unpacked by exploring individual contrasts.

Heart rate plotted across time. IBI = inter-beat interval
There were no significant IBI differences between baseline and outcome for wins, losses or near-misses (p’s > .017), inferring no difference in HR change before the outcome was presented. There was a significant difference in HR change between outcome and IBI1 for wins compared to losses [F(1, 50) = 29.75, p < .001] and to near-misses [F(1, 50) = 8.95, p = .004], whereby wins were associated with prolonged deceleration. No significant difference in HR change was found between losses and near-misses [F(1, 50) = 1.71, p = .197].
The contrasts between IBI1 and IBI2 were not significant for wins and losses [F(1, 50) = 1.31, p = .258], wins and near-misses [F(1, 50) = .255, p = .616], or losses and near-misses [F(1, 50) = .04, p = .837] suggesting all outcomes accelerated in a similar fashion. Between IBI2 and IBI3, wins and losses had a different HR change profile [F(1, 50) = 9.20, p = .004]. Specifically, wins had shorter IBIs compared to losses, indexing greater acceleration. No difference in HR change between wins and near-misses, [F(1, 50) = 4.64, p = .036], or near-misses and losses, [F(1, 50) = .67, p = .417] were observed after controlling for multiple comparisons. There were no other significant interactions in HR change (p’s > .017).
PRP
The ANOVA demonstrated a significant effect of outcome on PRP, F(1.03, 54.44) = 80.36, p < .001. Figure 7 shows this effect. Bonferroni-adjusted contrasts revealed that wins were associated with longer pauses than losses, F(1, 53) = 83.35, p < .001 and near-misses, F(1, 53) = 78.70, p < .001. There was no difference between loss and near-miss pauses after correcting for multiple comparisons, F(1, 53) = 5.17, p = .027.

Average post-reinforcement pause per outcome
Impulsivity
The exploratory analysis revealed no significant associations between SUPPS-P total scores and variations in HR or PRP responses between outcomes, after controlling for multiple comparisons.
Discussion
The current study investigated whether near-misses in VR slot machine gambling uniquely influenced responses that can be distinguished from wins and losses. As hypothesised, participants showed significantly greater HR acceleration for near-miss outcomes compared to wins. However, near-misses did not appear to result in greater HR acceleration than losses. This finding potentially suggests that near-misses may not be uniquely arousing events in non-problem gambling populations, as both events elicited similar psychophysiological and behavioural responses and differed from wins in the same manner. However, our loss control was visually similar to near-misses, which may have acted as a subtler near-miss condition and obscured our ability to detect a near-miss effect. This converges with the behavioural data where near-miss PRPs were shorter than wins, but were no different from losses.
HR response showed a biphasic temporal pattern of initial deceleration in the time interval straddling the outcome presentation, followed by acceleration. This pattern is consistent with previous slot machine research (Clark et al. 2012; Lole et al. 2012). A deceleration component initiated before an outcome may be interpreted as anticipation (Bradley and Lang 2000; Ulrich et al. 2016). The subsequent post-outcome acceleration may index the emotional processing of the outcome (Lacey et al. 1963; Bradley and Lang 2000). Wins differed from near-misses and losses as there was a distinct deceleration followed by later acceleration, compared to losses, which demonstrated an immediate acceleration after the outcome. This interaction effect corroborates prior findings that wins produce different arousal profiles to losses in slot machine gambling (Anderson and Brown 1984; Lole et al. 2012; Wulfert et al. 2005).
One likely mechanism responsible for the delayed HR deceleration after wins is that the emotive ‘fireworks’ display may have led to greater perceptual processing beyond loss outcomes (Lacey 1967). It is plausible that processing the additional audio-visual stimuli and not the actual condition of winning itself contributed to the observed deceleration. Nevertheless, this is not likely to account for the win HR response in its entirety given past research has demonstrated that wins not accompanied by attention-grabbing cues are sufficient to induce differential arousal from losses (Lole et al. 2012).
The extent that HR accelerated following the outcome is also noteworthy. Although previous psychophysiological studies have been successful in differentiating near-misses from losses in non-clinical populations (Clark et al. 2012; Dixon et al. 2011), others studies have not (Clark et al. 2013; Lole et al. 2012). Heightened HR acceleration following a gambling outcome may reflect frustration associated with nearly-winning (Clark et al. 2012; Reid 1986). This study revealed no significant difference in the amount of acceleration following each outcome; rather a difference in the timing of the acceleration. As such, it does not seem appropriate to infer valence from our HR data, but instead suggests that we may have observed a state of vigilance (Lole et al. 2012; Barry 2006), which differentiated winning from losing on VR slot machines. Valence inferences will be possible in future research which provides a distinguishable loss control condition.
Consistent with past findings, both near-misses and losses had shorter PRPs than wins (Dixon et al. 2013; Worhunsky et al. 2014), which suggests that near-misses were not misinterpreted as wins (Belisle and Dixon 2016), as they had similar pauses to regular losses. Indeed, Dixon et al. (2013) suggested that if near-misses were even slightly pleasurable, yet lacked the same temporal pattern due to a lack of reinforcing winning stimuli, they would produce somewhat longer pauses than losses. Further, Dixon et al. (2013) suggested that a shorter pause was indicative of frustration, and participants gambling continue to spin reels in order to relieve this negative affect by a potential, subsequent win. The current findings suggest that both losses and near-misses may demonstrate an equal motivation to initiate quicker gambling.
Similar to the findings of Lole et al. (2012), impulsivity was not correlated with near-miss HR change or, unique to our study, PRPs. As such, healthy individuals with higher trait impulsivity may not respond differentially to near-misses from losses or wins. To the best of our knowledge, this was only the second attempt to link impulsivity to slot machine outcomes, both studies of which used non-clinical populations. It remains to be seen whether impulsivity is associated with near-miss responses in clinical populations using an immersive VR simulation.
Limitations and Future Directions
Regarding limitations, the near-miss and loss outcomes were visually similar, in that every loss outcome involved three matching icons, with only the final, winning icon varying in position from the pay-line. A lack of HR or PRP difference between the two kinds of losses occurred potentially because they appeared more alike than if the loss outcome involved four completely different icons (i.e. the losses were a subtler near-miss outcome). This may account for nil differences currently observed between near-misses above or below the pay-line (Clark et al. 2013; Sharman and Clark 2016). Nonetheless, the reels were designed as an extension paradigm created by Clark et al. (2009) and were chosen to assist with comparability to this study, and to control for participants’ expectations when receiving the outcome. A challenge of implementing losses that less resemble near-misses is that if the loss outcome is clear when the second reel lands, the spin-up is shorter which interferes with the window to capture psychophysiological responses from the previous trial. Therefore, having outcomes determined at the fourth reel landing provided the greatest possible time window for physiological recording of responses from the previous outcome, without pausing in-between each trial, which in turn increased immersiveness.
Future research should include problem gambling populations to extend current findings. Problem gambling is often associated with distinct cognitive profiles such as a reduced ability to delay reward, poor error monitoring, diminished reward sensitivity and stronger physiological responses to near-misses (Goudriaan et al. 2014). Further, impulsivity is more pronounced in problem gamblers seeking treatment than in problem gamblers in the community (Knezevic and Ledgerwood 2012). As such, near-miss findings need to be quantified by the populations which are likely to be most sensitive to the near-miss effect (Yücel et al. 2017). The current and previous null findings (Lole et al. 2012) linking impulsivity to near-misses may reflect how this relationship does not exist for people with a low-risk of problem gambling. It is conceivable that relationships will emerge between autonomic arousal and near-miss outcomes in populations with or at risk of problem gambling. The current study was the first to examine the near-miss effect using VR and to account for presence while using automated slot machines. We were able to enhance ecological validity and, accordingly, the potential real-world physiological and behavioural signatures, during the simulation. Future studies should directly compare the ecological validity between a VR immersion compared with a computer simulation.
Conclusion
This was the first study to investigate the influence of slot machine near-misses using an immersive VR environment. The gambling environment was designed to resemble real-world settings in which more ecologically valid responses could be measured. Wins during slot machine gambling had distinct HR patterns and PRPs compared to losses in healthy individuals, however no differences between losses and near-misses were observed. Whether near-misses have a unique motivational effect on gambling remains to be clarified. Our findings are limited by the characteristics of the loss condition. Nevertheless, this initial study using immersive VR provides evidence that it is possible to measure event-related, phasic responses to winning and losing in a VR gambling environment, paving the way for future near-miss research. Going forward, research should differentiate near-misses from losses and examine clinical populations in immersive environments to better understand the development and maintenance of problem gambling.
References
Amsel, A. (1958). The role of frustrative nonreward in noncontinuous reward situations. Psychological Bulletin, 55(2), 102.
Amsel, A. (1992). Frustration theory: An analysis of dispositional learning and memory (Vol. 11). Cambridge: Cambridge University Press.
Anderson, G., & Brown, R. I. (1984). Real and laboratory gambling, sensation-seeking and arousal. British Journal of Psychology, 75(3), 401–410.
Barry, R. J. (2006). Promise versus reality in relation to the unitary orienting reflex: A case study examining the role of theory in psychophysiology. International Journal of Psychophysiology, 62(3), 353–366. https://doi.org/10.1016/j.ijpsycho.2006.01.004.
Barton, K., Yazdani, Y., Ayer, N., Kalvapalle, S., Brown, S., Stapleton, J., et al. (2017). The effect of losses disguised as wins and near misses in electronic gaming machines: A systematic review. Journal of Gambling Studies. https://doi.org/10.1007/s10899-017-9696-0.
Belisle, J., & Dixon, M. R. (2016). Near misses in slot machine gambling developed through generalization of total wins. Journal of Gambling Studies, 32(2), 689–706. https://doi.org/10.1007/s10899-015-9554-x.
Blain, B., Richard Gill, P., & Teese, R. (2015). Predicting problem gambling in Australian adults using a multifaceted model of impulsivity. International Gambling Studies, 15(2), 239–255. https://doi.org/10.1080/14459795.2015.1029960.
Bouchard, S., Loranger, C., Giroux, I., Jacques, C., & Robillard, G. (2014). Using virtual reality to provide a naturalistic setting for the treatment of pathological gambling. In C. S. Lányi (Ed.), The thousand faces of virtual reality. InTech: Rijeka.
Bouchard, S., Robillard, G., Giroux, I., Jacques, C., Loranger, C., St-Pierre, M., et al. (2017). Using virtual reality in the treatment of gambling disorder: The development of a new tool for cognitive behavior therapy. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2017.00027.
Bradley, M. M., & Lang, P. J. (2000). Emotion and Motivation. Handbook of Psychophysiology, 2, 602–642.
Chase, H. W., & Clark, L. (2010). Gambling severity predicts midbrain response to near-miss outcomes. The Journal of Neuroscience, 30(18), 6180. https://doi.org/10.1523/JNEUROSCI.5758-09.2010.
Clark, L., Crooks, B., Clarke, R., Aitken, M. R., & Dunn, B. D. (2012). Physiological responses to near-miss outcomes and personal control during simulated gambling. Journal of Gambling Studies, 28(1), 123–137. https://doi.org/10.1007/s10899-011-9247-z.
Clark, L., Lawrence, A. J., Astley-Jones, F., & Gray, N. (2009). Gambling near-misses enhance motivation to gamble and recruit win-related brain circuitry. Neuron, 61(3), 481–490. https://doi.org/10.1016/j.neuron.2008.12.031.
Clark, L., Liu, R., McKavanagh, R., Garrett, A., & Dunn, B. (2013). Learning and affect following near-miss outcomes in simulated gambling. Journal of Behavioral Decision Making, 26(5), 442–450. https://doi.org/10.1002/bdm.1774.
Cyders, M., Littlefield, A., Coffey, S., & Karyadi, K. (2014). Examination of a short English version of the UPPS-P Impulsive Behavior Scale. Addictive Behaviors, 39(9), 1372. https://doi.org/10.1016/j.addbeh.2014.02.013.
Dixon, M., Harrigan, K., Jarick, M., Maclaren, V., Fugelsang, J., & Sheepy, E. (2011). Psychophysiological arousal signatures of near-misses in slot machine play. International Gambling Studies, 11(3), 393–407. https://doi.org/10.1080/14459795.2011.603134.
Dixon, M., Harrigan, K. A., Sandhu, R., Collins, K., & Fugelsang, J. A. (2010). Losses disguised as wins in modern multi-line video slot machines. Addiction, 105(10), 1819–1824. https://doi.org/10.1111/j.1360-0443.2010.03050.x.
Dixon, M., MacLaren, V., Jarick, M., Fugelsang, J. A., & Harrigan, K. A. (2013). The frustrating effects of just missing the jackpot: Slot machine near-misses trigger large skin conductance responses, but no post-reinforcement pauses. Journal of Gambling Studies, 29(4), 661–674. https://doi.org/10.1007/s10899-012-9333-x.
Dixon, M. R., & Schreiber, J. E. (2004). Near-miss effects on response latencies and win estimations of slot machine players. Psychological Record, 54(3), 335.
Dowling, N., Smith, D., & Thomas, T. (2005). Electronic gaming machines: Are they the ‘crack-cocaine’of gambling? Addiction, 100(1), 33–45.
Ferris, J., & Wynne, H. (2001). The Canadian problem gambling index. Ottawa: Canadian Consortium for Gambling Research.
Field, A. (2013). Discovering statistics using IBM SPSS statistics. Thousand Oaks: Sage.
Gainsbury, S., Russell, A., Hing, N., Wood, R., Lubman, D. I., & Blaszczynski, A. (2014). The prevalence and determinants of problem gambling in Australia: Assessing the impact of interactive gambling and new technologies. Psychology of Addictive Behaviors, 28(3), 769. https://doi.org/10.1037/a0036207.
Gerstein, D., Volberg, R. A., Toce, M., Harwood, H., Johnson, R., Buie, T., et al. (1999). Gambling impact and behavior study: Report to the national gambling impact study commission. Chicago: National Opinion Research Center.
Giroux, I., Faucher-Gravel, A., St-Hilaire, A., Boudreault, C., Jacques, C., & Bouchard, S. (2013). Gambling exposure in virtual reality and modification of urge to gamble. Cyberpsychology Behavior Social Networking, 16(3), 224–231. https://doi.org/10.1089/cyber.2012.1573.
Goudriaan, A. E., Yücel, M., & van Holst, R. J. (2014). Getting a grip on problem gambling: What can neuroscience tell us? Frontiers in Behavioral Neuroscience. https://doi.org/10.3389/fnbeh.2014.00141.
Griffiths, M. (1991). Psychobiology of the near-miss in fruit machine gambling (slot machines). The Journal of Psychology, 125(3), 347.
Griffiths, M. (1993). Fruit machine gambling: The importance of structural characteristics. Journal of Gambling Studies, 9(2), 101–120.
Harrigan, K. A. (2009). Slot machines: Pursuing responsible gaming practices for virtual reels and near misses. International Journal of Mental Health and Addiction, 7(1), 68–83.
Hodgins, D. C. (2002). Using the NORC DSM Screen for gambling problems (NODS) as an outcome measure for pathological gambling: Reliability and validity. Gambling Research: Journal of the National Association for Gambling Studies (Australia), 14(1), 5.
Kassinove, J. I., & Schare, M. L. (2001). Effects of the “near miss” and the “big win” on persistence at slot machine gambling. Psychology of Addictive Behaviors, 15(2), 155.
Kennedy, R. S., Lane, N. E., Berbaum, K. S., & Lilienthal, M. G. (1993). Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. The International Journal of Aviation psychology, 3(3), 203–220. https://doi.org/10.1207/s15327108ijap0303_3.
Knezevic, B., & Ledgerwood, D. M. (2012). Gambling severity, impulsivity, and psychopathology: Comparison of treatment-and community-recruited pathological gamblers. The American Journal on Addictions, 21(6), 508–515.
Krueger, T. H. C., Schedlowski, M., & Meyer, G. (2005). Cortisol and heart rate measures during casino gambling in relation to impulsivity. Neuropsychobiology, 52(4), 206–211. https://doi.org/10.1159/000089004.
Lacey, J. I. (1967). Somatic response patterning and stress: Some revisions of activation theory. In M. H. Appley & R. Trumbell (Eds.), Psychological stress: Issues in research (pp. 14–42). New York: Appleton-Century-Croft.
Lacey, J. I., Kagan, J., Lacey, B. C., & Moss, H. (1963). The visceral level: Situational determinants and behavioral correlates of autonomic response patterns. In P. H. Knapp (Ed.), Expression of the emotions in man (pp. 161–196). New York: International Univeristies Press.
Li, E., Browne, M., Rawat, V., Langham, E., & Rockloff, M. (2017). Breaking bad: Comparing gambling harms among gamblers and affected others. Journal of Gambling Studies, 33(1), 223–248.
Lole, L., Gonsalvez, C. J., Blaszczynski, A., & Clarke, A. R. (2012). Electrodermal activity reliably captures physiological differences between wins and losses during gambling on electronic machines. Psychophysiology, 49(2), 154–163. https://doi.org/10.1111/j.1469-8986.2011.01290.x.
Lutri, V., Soldini, E., Ronzitti, S., Smith, N., Clerici, M., Blaszczynski, A., et al. (2018). Impulsivity and gambling type among treatment-seeking disordered gamblers: An explorative study. Journal of Gambling Studies, 34, 1341–1354.
Lynam, D. (2013). Development of a short form of the UPPS-P Impulsive Behavior Scale. Unpublished Technical Report.
Moss, J. D., & Muth, E. R. (2011). Characteristics of head-mounted displays and their effects on simulator sickness. Human Factors, 53(3), 308–319.
Park, C. B., Park, S. M., Gwak, A. R., Sohn, B. K., Lee, J. Y., Jung, H. Y., et al. (2015). The effect of repeated exposure to virtual gambling cues on the urge to gamble. Addictive Behaviors, 41, 61–64. https://doi.org/10.1016/j.addbeh.2014.09.027.
Parke, J., & Griffiths, M. (2006). The psychology of the fruit machine: The role of structural characteristics. International Journal of Mental Health and Addiction, 4(2), 151–179. https://doi.org/10.1007/s11469-006-9014-z.
Productivity Commission. (2010). Gambling Canberra.
Reid, R. (1986). The psychology of the near miss. Journal of Gambling Behavior, 2(1), 32–39. https://doi.org/10.1007/BF01019932.
Robillard, G., Bouchard, S., Fournier, T., & Renaud, P. (2003). Anxiety and presence during VR immersion: A comparative study of the reactions of phobic and non-phobic participants in therapeutic virtual environments derived from computer games. CyberPsychology & Behavior, 6(5), 467–476. https://doi.org/10.1089/109493103769710497.
Sharman, S., Aitken, M. R., & Clark, L. (2015). Dual effects of losses disguised as wins’ and near-misses in a slot machine game. International Gambling Studies, 15(2), 1–12. https://doi.org/10.1080/14459795.2015.1020959.
Sharman, S., & Clark, L. (2016). Mixed emotions to near-miss outcomes: A psychophysiological study with facial electromyography. Journal of Gambling Studies, 32(3), 823–834. https://doi.org/10.1007/s10899-015-9578-2.
Toce-Gerstein, M., Gerstein, D. R., & Volberg, R. A. (2003). A hierarchy of gambling disorders in the community. Addiction, 98(12), 1661–1672.
Ulrich, N., Ambach, W., & Hewig, J. (2016). Severity of gambling problems modulates autonomic reactions to near outcomes in gambling. Biological Psychology, 119, 11–20. https://doi.org/10.1016/j.biopsycho.2016.06.005.
Williams, R. J., Volberg, R. A., & Stevens, R. M. (2012). The population prevalence of problem gambling: Methodological influences, standardized rates, jurisdictional differences, and worldwide trends. Ontario Problem Gambling Research Centre.
Witmer, B. G., & Singer, M. J. (1998). Measuring presence in virtual environments: A presence questionnaire. Presence Teleoperators and Virtual Environments, 7(3), 225–240.
Worhunsky, P. D., Malison, R. T., Rogers, R. D., & Potenza, M. N. (2014). Altered neural correlates of reward and loss processing during simulated slot-machine fMRI in pathological gambling and cocaine dependence. Drug and Alcohol Dependence, 145, 77–86. https://doi.org/10.1016/j.drugalcdep.2014.09.013.
Wulfert, E., Roland, B. D., Hartley, J., Wang, N., & Franco, C. (2005). Heart rate arousal and excitement in gambling: Winners versus losers. Psychology of Addictive Behaviors, 19(3), 311–316. https://doi.org/10.1037/0893-164X.19.3.311.
Yücel, M., Carter, A., Allen, A. R., Balleine, B., Clark, L., Dowling, N. A., et al. (2017). Neuroscience in gambling policy and treatment: An interdisciplinary perspective. The Lancet Psychiatry, 4(6), 501–506. https://doi.org/10.1016/S2215-0366(16)30369-8.
Yücel, M., Carter, A., Harrigan, K., van Holst, R. J., & Livingstone, C. (2018). Hooked on gambling: A problem of human or machine design? The Lancet Psychiatry, 5(1), 20–21.
Acknowledgements
This research was supported by partial funding from Monash University School of Psychological Science and the David Winston Turner Endowment Fund.
Funding
Murat Yücel has received funding from the National Health and Medical Research Council of Australia (APP#1117188), the Australian Research Council, the David Winston Turner Endowment Fund, and Monash University. He has also received funding from the law firms in relation to expert witness report/statement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the Monash University Human Research Ethics Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Detez, L., Greenwood, LM., Segrave, R. et al. A Psychophysiological and Behavioural Study of Slot Machine Near-Misses Using Immersive Virtual Reality. J Gambl Stud 35, 929–944 (2019). https://doi.org/10.1007/s10899-018-09822-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-018-09822-z