
Abstract
This article examines gambling harms from both gamblers and affected others’ perspectives. Participants (3076 gamblers and 2129 affected others) completed a retrospective survey that elicited information on harms they experienced from gambling across their lifetime. Their responses were analyzed through testing measurement invariance, estimating item-response theoretic parameters, calculating percentages, confidence intervals, and correlations, as well as regressions. The results indicated large commonalities in the experience of harms reported by gamblers and affected others. Further, gamblers appeared to ‘export’ about half of the harms they experienced to those around them. The findings also provided detailed profiles of evolving harms as problem gambling severity varies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
When you have children, you always have family. They will always be your priority, your responsibility. – Breaking Bad (Season 3, Episode 5) (polokill 2013)
Gambling can have negative impacts not only on gamblers themselves, but can also lead to adverse consequences for those connected to them, in particular their family and close friends. Children of problem gamblers could experience reduced material and non-material well-being, as well as greater risk of developing unhealthy behaviors (Darbyshire et al. 2001; Jacobs et al. 1989). Spouses or partners of people who gambled were also reported to suffer from financial insecurities, health problems, psychological difficulties, or even deteriorating relationships (Dickson-Swift et al. 2005; Holdsworth et al. 2013; Lorenz and Shuttlesworth 1983; Lorenz and Yaffee 1988). Parents of people who experienced problems with gambling might face manipulation from their gambling children, and suffer from emotional impacts such as fear, guilt, and anger (Kalischuk et al. 2006). In addition to children, partners, and parents, grandparents, siblings, or close friends of problem gamblers could also report increased mental health problems and other well-being impairments (Salonen et al. 2014). A recent review by Velleman et al. (2015) further confirmed various negative impacts (e.g., on finance, relation, or health) that might occur to gamblers’ affected others.Footnote 1
Given the complex nature of gambling harms experienced among affected others, there has been increasing number of studies assessing these experiences or their consequences, from either affected others or gamblers’ perspective. For example, Krishnan and Orford (2002) utilized interviews and a coping questionnaire to examine coping strategies and received support reported by partners, parents, and landlord of gamblers. In addition to the coping questionnaire, Orford et al. (2005) also proposed a series of other measures for testing harmful stress, ill-health experiences, and future hope among family members of people with gambling (or drug/alcohol) problems. Recently, Dowling et al. (2015) assessed problem gamblers’ opinions on the effects of their gambling on their own family, through both qualitative measurement and a newly-developed family impact scale. They found over 30 % of their respondents, namely problem gamblers who sought gambling treatment, did not admit the existence of family impact due to their gambling (Dowling et al. 2015). This potential under-reporting through ‘gamblers’ voice’, along with previous studies focusing on ‘affected others’ voice’ (e.g., Krishnan and Orford 2002; Orford et al. 2005), has highlighted the importance of assessing gambling harms from both gamblers and affected others’ perspectives. Moreover, understanding the individual level harms (rather than societal harms) requires examining both harms occurring to gamblers, as well as harms experienced by people closely connected to them. So, how do the gambling related harms experienced by gamblers themselves compare—both qualitatively and by degree—to those experienced by their family and friends (i.e., affected others)?
Two studies have provided some preliminary answers to this question. Ferland et al. (2008) conducted an exploratory study to compare the perceptions of seven pathological gamblers and their spouses. It was found that those spouses’ perceived consequences from pathological gambling were more severe than those gamblers’ perceptions (Ferland et al. 2008). However, the very limited sample size of the study advises caution in interpreting the results. In a more recent study, Langham et al. (2016) employed qualitative methods to understand gambling harms to gamblers and their affected others; via focus groups (n = 35), individual interviews (n = 25), and posts from online gambling help/support forums (n = 469). They found that harms could be organized into identical domains for both gamblers and affected others: those being financial, relationship, emotional/psychological, health, work/study, cultural, criminal activity, and lifecourse and intergenerational harms. The authors also identified a large number of specific harms within each domain, such as ‘bankruptcy’ in the financial domain, ‘reduced performance due to tiredness or distraction’ in the work/study domain, and ‘reduced engagement in cultural rituals’ in the cultural domain (Langham et al. 2016). This provides a strong conceptual basis for approaching harms from gambling, as well as a detailed enumeration of the specific types of harms within reasonable categories. However, the qualitative methodology did not permit comparisons between the two groups—e.g., whether harms to the affected others had a characteristically different profile from harms to the gamblers themselves. Quantitative work is required in order to make comparisons between gamblers and affected others regarding the prevalence and degree of harms experienced as a result of gambling.
In addition to the much-needed comparison of gambling harms as they occur to gamblers and those around them, there has been a lack of research into the conceptual similarities and differences between gambling problems (as defined by symptoms) and gambling harms (which are negative outcomes from gambling). As one of the most popular measures of gambling problems, the Problem Gambling Severity Index (PGSI) developed by Ferris and Wynne (2001) has been utilized in numerous gambling studies since its publication (e.g., Browne et al. 2015; Dixon et al. 2014; Li et al. 2016; Rockloff et al. 2014; Wohl et al. 2013). Conceptually the PGSI does not measure the ‘amount of harm experienced’, but is rather a clinical screening instrument for gambling problems (Hodgins et al. 2011). However, problem gambling is intimately connected to gambling related harms, and the PGSI does probe a limited number of key harms as indicators of problem gambling (it also includes some symptoms that are not harms; Currie et al. 2009; Svetieva and Walker 2008). What is lacking is a systematic investigation into a broad range of specific harms associated with different levels of problem gambling/gambling participation (Blaszczynski 2009; Rodgers et al. 2009), and an understanding of their relative prevalences across PGSI categories. The present paper addresses this issue, by taking a comprehensive approach and casting a ‘wide net’ in terms of probing for specific harms that may affect gamblers and those in their immediate social network.
The aims of the current study are threefold, including: examining experiences of gambling harms from both gamblers and affected others’ perspectives; testing domains of harms identified by previous qualitative research, through a large-scale retrospective survey; and assessing a comprehensive set of harms, along with their relationship to the PGSI. By accomplishing these objectives, we intend to evaluate various harms occurring to gamblers with different degrees of symptoms, as well as corresponding harms to their closely related others. The outcome of the survey could also generate insights benefiting detection of gambling related harms and problems, as well as targeted treatment and support strategies for both gamblers and affected others.
Method
Development of Harm Checklists
As mentioned, prior qualitative research (Langham et al. 2016) identified a taxonomy of specific harms based on extant literature, focus groups, interviews, and online forum posts. These harms were developed into a set of personal statements, following a series of criteria:
-
1.
Covering the comprehensive set of harms identified within the taxonomy, while using plain language and providing examples where appropriate.
-
2.
Avoiding content overlap between items while making each item unitary in scope. For example, a candidate harm ‘spent less time and got less enjoyment from spending time with people I care about’ was broken into two more specific items. This enabled respondents to respond definitively to each item.
-
3.
Using phrasing that was appropriate regardless of whether the source of the harms was one’s own gambling, or someone else’s gambling. This facilitated comparisons between the two groups.
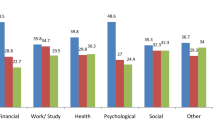
This process resulted in a set of 73 specific potential harms arising from gambling (Table 1), organized within six of those broad domains adapted from Langham et al. (2016). These six domains included financial, work/study, health, emotional/psychological, relationship, and other harms (note that other harms covered both cultural and criminal activity relevant harms). The large item set led us to adopt a checklist approach; in the interest of maintaining a reasonable time for study participants to complete, and yielding more interpretable results in terms of the relative prevalence of harms. Accordingly, for each domain, the checklist involved participants reviewing the list, and checking each item if they experienced that issue as a result of the gambling. A single 4-point Likert response item that assessed the overall level of harm experienced in that domain followed each domain checklist. For example, the financial domain concluded with the following item: ‘Overall, what level of impact did your gambling have upon your financial security during this time?’
Survey Design
The key rationale behind our survey design was to understand the prevalence of harmful outcomes, relative to different levels of gambling problems. Given the low expected prevalence of currently existing gambling problems or harms in the general population, we opted for a retrospective survey design in order to elicit information from across participants' lifetime. The cost to this decision involved accepting the use of a PGSI modified slightly to suit retrospective responding. The benefit was to greatly increase the amount of useful data obtained, for a given sampling effort. We were interested in harms that accrue to significant others around the gambler (‘affected others’), as well as the gambler themselves. Participants were requested to focus on the 12-month period of their life when gambling was causing the most problems. Throughout the survey, participants were reminded to reflect on that 12-month period. This approach of reminding participants to continue to focus on the relevant 12-month period was matched by an accompanying retrospective version of the PGSI. The PGSI items themselves were not modified except for the addition of the prefix ‘At this time…’ and the utilization of past tense (e.g., ‘At this time, did gambling cause you any health problems, including stress or anxiety?’). For affected others, the PGSI was completed second hand, from the perspective of the affected person (e.g., ‘At this time, did gambling cause the person any health problems, including stress or anxiety?’). However the harms were measured in both cases as a self-report from the person who experienced them.
Recruitment of Participants
Our goal for recruitment was to obtain a stratified sample of harms across PGSI categories, across participants' lifetime. Recruitment for online completion of the survey was done through an ISO-accredited Australian commercial panel provider in two stages. In the first stage of recruitment, the criteria for participation were either: that the participant’s own gambling had caused them problems, no matter how minor (directed toward the questionnaire for gamblers), or having had a close relationship with a person whose gambling had caused them problems, no matter how minor (directed toward the questionnaire for affected others). Participants completed only one questionnaire. In the case that a participant fulfilled both criteria, they were directed to complete the questionnaire for gamblers. Fig. 1, Panel a illustrates the recruitment process for this stage.

Overview of the recruitment process. Panel a: Stage 1 recruitment (inclusion criteria: lifetime experience of gambling harms). Panel b: Stage 2 recruitment (inclusion criteria: lifetime experience of frequent gambling)
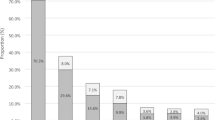
Of the 2458 gamblers and 1678 affected others who met the eligibility criteria and completed the survey, 71 % of gamblers and 81 % of affected others reported gambling problems in the most severe problem gambling category (i.e., reporting a PGSI score of 8 or more). These surprisingly high proportions were presumably due to participant interpretation of the screening criteria—those participants who admitted having problems (in the screen), also tended to be classified by the PGSI as having gambling problems. In order to achieve a greater representation of participants in lower-risk PGSI categories, we initiated a second stage of recruitment from the remaining panel members (Fig. 1, Panel b). The screening criteria were modified to indicate a time in the participant’s life when they were gambling often (directed toward the questionnaire for gamblers), or had a close relationship with someone who was gambling often (directed toward the questionnaire for affected others). Thus, the criteria for inclusion made no reference to gambling problems, only towards ‘gambling often’. A further 618 gamblers and 451 affected others were recruited in the second stage, with 35 % of gamblers and 64 % affected others in this group meeting the criteria for problem gambling based on the PGSI cut-off (i.e., reporting a PGSI score of 8 or more).
Data Analyses
All analyses were conducted in the R statistical programming environment. Specifically, we utilized the lavaan package (Rosseel 2012) for testing of measurement invariance of the PGSI instrument, and the ltm package (Rizopoulos 2006) for estimating item-response theoretic (IRT) parameters of the harm items, and general purpose functions for calculating key item indicators such as percentages, confidence intervals, and correlations.
Our sample included a reasonably large proportion of individuals who reported having experienced gambling problems and harms in the last 12 months. This allowed scope to check for the validity of retrospective reporting by testing for measurement invariance of the PGSI instrument between individuals reporting on current problems, and those who were reflecting on a historical 12-month period in their lives. We also made comparisons in PGSI responding between those reporting on their own problems, versus those reporting on the problems of a significant other. This was done via standard measurement tests (Vandenberg and Lance 2000), comparing group-variant and group-invariant confirmatory factor analysis (CFA) models using the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). These are commonly employed in questionnaire development to ascertain whether an instrument performs similarly across different groups. In the present context, this allows us to test whether the PGSI instrument was functioning similarly, as reported by gamblers and affected others. Both CFI and RMSEA incorporate penalty terms for degrees of freedom, and therefore improved fit measures are possible for more highly constrained models (in the present cases, involving a common model for both gamblers and affected others), when the extra degrees of freedom are not supported by data fit. Additionally, t-tests were employed to compare latent PGSI scale means between groups of participants.
For each domain of gambling harms considered, a separate IRT model was applied. IRT modeling assumes the existence of a latent dimensional construct (e.g. financial harm), higher scores of which are manifested by a greater probability of observing positive scores on a set of measurable indicators (i.e. the specific harms on our checklists). In a two-parameter model, items can differ in terms of their severity (i.e., 'difficulty') and discrimination parameters. A higher item severity parameter means that the indicator tends to be positive only when latent scores are relatively high. That is, sensitive for capturing differences between high degrees of gambling harm. Conversely, a lower severity parameter indicates that the item is sensitive for capturing differences between lower levels of harm. The discrimination parameter describes how reliably the indicator discriminates individuals overall with respect to the latent construct (i.e., discriminates between higher and lower levels of the latent construct). Because IRT does not make use of information outside of the items being considered, it is related to item reliability rather than validity. Therefore, correlations and cross-tabulations of checklist harms with the PGSI provide an alternative measure of item functioning with respect to an external test. Prevalence and 95 % confidence intervals were calculated for all four PGSI categories. The items’ point-biserial correlation coefficient was calculated with respect to (a) the PGSI, (b) the general domain Likert item measuring ‘overall harm’ (within the respective domain), and (c) the sum of positive answers in corresponding harm domain (item-total correlation, excluding the current item). Lastly, we summarized the overall relationship between number of harms reported and the PGSI. A series of linear and loess smoothed regressions were run for gamblers and affected others separately. In these simple regression models, the PGSI score was the predictor, and the number of specific harms reported for each harm domain, and across all domains, were the response variables. The standardized beta coefficients for these models provide a means to compare the degree to which each of the domains of harms are related to increasing gambling problems, as measured by the PGSI.
Results
In total, 3076 (1364 female) complete responses were obtained from participants reporting on harms arising from their own gambling (hereafter gamblers), and 2129 (1485 female) responses were obtained from participants reporting on harms arising from the gambling of a significant other (hereafter affected others). The age distributions in these two participant groups were very similar, with mean ages of 46.0 and 45.8, and 50 % of participants aged between 33 and 58 in both groups. Participants in the affected others group reported their relationships to the person whose gambling had affected them, and the prevalences of those relationships are presented in Table 2.
PGSI Functioning Across Measurement Groups
A relatively strong assumption can be made that both gamblers and affected others in the current sample have similar demographic backgrounds, being either online panel participants or people close to them. We would therefore expect the observed PGSI sample means and variances for the second-hand reporting done by the affected others to be similar or close to the first-hand reporting done by the gamblers themselves. Similarly, if the retrospective version of the PGSI is functioning equivalently, we would expect not to observe large differences between current and retrospective reporting. There were four groups reporting on PGSI scores: current versus retrospective reporting and self-reporting versus reporting by an affected other, allowing us to make a number of comparisons regarding equivalent functioning of the PGSI with respect to groups.
Thirty-nine percent (1206) of gamblers reported on gambling problems and harms experienced currently (i.e. in the last 12 months), while the remainder reported retrospectively on a period (median = 9 years, inter-quartile range 4–15 years) earlier in their lives. The current group had a significantly higher mean PGSI score (11.2) than the retrospective group (9.5); (t(2540.59) = 7.76, p < 0.01). However, group mean differences accounted for only 1.9 % of variance in PGSI scores.
Twenty-six percent (561) of participants in the affected-others group reported on currently experienced harms, and the rest affected others reported retrospectively on a period (median = 10 years, inter-quartile range: 4–15 years) earlier in their lives. No significant difference was observed between the means of current (11.6) and retrospective (12.1) PGSI reporting done by affected others (t(949.35) = 1.68, p = .09). The variances of PGSI scores of current and retrospective reports by affected others also did not differ significantly (F(560, 1568) = 1.09, p = .18). Table 3 shows CFI and RMSEA fit indices for a sequence of three CFA models, testing for measurement invariance on the PGSI for four contrasts between the four groups of participants. PGSI items were treated as ordinal indicators. As detailed in Table 3, each row of the table corresponds to a model with a progressively stronger assumption regarding the item-level measurement invariance of the PGSI across groups. The best fits were observed for the weakly invariant measurement model (Model 2), suggesting that item loadings, but not item (ordinal) response thresholds were invariant across participant groups.
The mean PGSI score reported first-hand by gamblers (10.1) was 1.8 points lower than that reported second-hand by affected others (11.9), though the effect of first-hand versus second-hand reporting only accounted for 2.2 % of variance in PGSI scores. The variance of retrospective PGSI scores reported by affected others compared to gamblers did not differ significantly (F(1569, 1869) = 1.05, p = .23). These results suggest that both the retrospective and second person PGSI reporting versions used provided a reasonably valid indication of the true level of problems experienced.
IRT Parameters, PGSI Categories, and Correlations
Tables 4, 5, 6, 7, 8 and 9 summarize the prevalences of specific harms, for each of the six domains considered. IRT severity and discrimination parameters are presented, and the specific harms are ordered with respect to IRT based severity, within each domain. Hence, the IRT severity parameter places the specific harm on a continuum of ‘harmfulness’ that is indicated by the whole group of items in each domain from least to most severe. Moreover, the IRT discrimination parameter indicates how well the item discriminates between low and high levels of harmfulness. Data for gamblers (Tables 4, 5, 6) and affected others (Tables 7, 8, 9) were analyzed separately, and are therefore presented in different tables. In addition, the tables also show the percentages and 95 % confidence intervals of each harm probe for the four PGSI categories (i.e., no identifiable problems, low risk, moderate risk, problem gamblers). Further, the tables present the point-biserial correlation coefficient with respect to the PGSI and the general domain Likert harm item. Finally, the item-total correlation for that harm domain (excluding the current item) is also given, providing a classical assessment of the reliability of that indicator in reflecting a presumed underlying dimension of harm within each domain. This set of statistics provide a picture of the functioning of each item, with respect to the domain and the problem gambling status. To illustrate, we consider one example, the item ‘Red. Ess. Exp.’ (less spending on essential expenses such as medications, healthcare and food), when administered to gamblers (Table 4). This item was the most effective probe for discriminating higher versus lower levels of financial harm (discrimination parameter = 3.28). It was sensitive for capturing medium to low levels of financial harm (severity parameter = 0.85). 1.7 % of non-problem gamblers responded positively to this item, as compared to 30.8 % of problem gamblers (as measured by the PGSI). The highest prevalence increase between PGSI categories for this item was between moderate risk and problem gamblers. Consistent with the IRT results, this item had the highest item-total correlation (.56), the second highest correlation with the general financial harm Likert item (.40), and the second highest correlation with the PGSI (.38), among the financial harm items.
As far as the severity parameters were concerned, items such as ‘bankruptcy’ (4.10), ‘excluded study’ (2.27), ‘emergency treatment’ (3.63), ‘escape’ (1.10), ‘actual ending’ (2.49), and ‘children unsupervised’ (2.36) indicated the most severe harm for gamblers, within the financial, work/study, health, emotional/psychological, relationship, and other domains respectively. In comparison, ‘bankruptcy’ (3.09), ‘lost job’ (2.78), ‘suicide’ (2.83), ‘failure’ (1.50), ‘neglected responsibilities’ (1.72), and ‘shame culture’ (2.94) were indicative of the most severe harm for affected others within each of the six corresponding domains. Hence, ‘bankruptcy’ was the most severe financial harm for both gamblers and affected others.
According to the discrimination parameters estimated for gamblers, items including ‘reduced essential expenses’ (3.28), ‘absent’ (2.39), ‘service’ (2.28), ‘worthlessness’ (2.89), ‘increased conflict’ (2.39), and ‘outcast’ (2.19) were the most effective in discriminating between low and high levels of harmfulness for their corresponding harm domains. In comparison, ‘reduced beneficial expenses’ (3.51), ‘absent’ (2.80), ‘service’ (2.92), ‘worthlessness’ (2.57), ‘increased conflict’ (2.42), and ‘took money’ (2.84) appeared the best discriminator for affected others within the corresponding domains. Hence, ‘absent’ was the most reliable discriminator for work/study harms on both gamblers and affected others. This was also the case for ‘service’ for health harms, ‘worthlessness’ for emotional/psychological harms, and ‘increased conflict’ for relationship harms.
Among problem gamblers identified by the PGSI, ‘reduced spending’ was reported as the most prevalent financial harm (71.3 %; 95 % confidence interval: 69.2%, 73.3%; for simplicity reason please refer to Tables 4, 5, 6, 7, 8 and 9 for the rest 95 % confidence intervals). Moreover, ‘reduced performance’ (30.4 %), ‘reduced sleep worry’ (48.3 %), ‘shame’ (60.8 %), ‘reduced time’ (51.5 %), and ‘pay money’ (18.4 %) also displayed the highest prevalence for those problem gamblers, within the work/study, health, emotional/psychological, relationship, and other domains respectively. On other hand, ‘reduced spending’ (40.6 %), ‘reduced performance’ (27.5 %), ‘reduced sleep worry’ (42.7 %), ‘distress’ (66.2 %), ‘increased tension’ (52.0 %), and ‘violence’ (16.3 %) demonstrated the highest prevalence among problem gamblers' affected others, within their corresponding domains. Hence, ‘reduced spending’ was the financial harm most frequently reported by both problem gamblers and their affected others. Likewise, for both groups, ‘reduced performance’ was the most frequently reported work/study harm, and ‘reduced sleep worry’ was the most frequently reported health harm.
For gamblers, harms such as ‘sold items’ (.41), ‘absent’ (.30)/‘reduced performance’ (.30), ‘reduced sleep worry’ (.42), ‘extreme distress’ (.50), ‘increased tension’ (.39), and ‘pay money’ (.31) had the highest correlations with their reported PGSI, within corresponding domains. Across these domains, on other hand, ‘sold items’ (.25), ‘reduced performance’ (.20), ‘stress problems’ (.23)/‘reduced sleep worry’ (.23), ‘extreme distress’ (.29), ‘neglected responsibilities’ (.17), and ‘took money’ (.18) were harms possessing the highest correlations with PGSI reported by affected others. Hence, ‘sold items’, ‘reduced performance’, ‘reduced sleep worry’, and ‘extreme distress’ were, respectively, the most reliable financial, work/study, health, and emotional/psychological consequences of increasing gambling problems, among both gamblers and affected others.
For gamblers, harms including ‘late bills’ (.43), ‘reduced performance’ (.50), ‘depression’ (.48), ‘extreme distress’ (.51), ‘increased conflict’ (.49), and ‘pay money’ (.40) displayed the strongest correlations with their corresponding general domain Likert harm items. Similarly, ‘reduced spending’ (.51), ‘reduced performance’ (.53), ‘depression’ (.51)/‘reduced sleep worry’ (.51), ‘extreme distress’ (.54), ‘increased conflict’ (.46)/‘increased tension’ (.46), and ‘violence’ (.54), as reported by affected others, also had the strongest correlations with their general domain items. Hence, ‘reduced performance’, ‘depression’, ‘extreme distress’, and ‘increased conflict’ were, respectively, the most reliable predictors of general work/study, health, emotional/psychological, and relationship harms, for both gamblers and affected others.
Based on the item-total correlations calculated for gamblers, harms like ‘reduced essential expenses’ (.56), ‘absent’ (.52), ‘stress problems’ (.49), ‘worthlessness’ (.62), ‘increased conflict’(.55)/‘neglected responsibilities’ (.55), and ‘took money’ (.44) demonstrated strongest associations with the rest items in their corresponding domains. Similarly, ‘reduced beneficial expenses’ (.61), ‘absent’ (.51), ‘depression’ (.52), ‘vulnerable’ (.54), ‘increased conflict’ (.54), and ‘took money’ (.49), as reported by affected others, also possessed the strongest item-total correlations in their respective domains. Hence, ‘absent’, ‘increased conflict’, and ‘took money’ were, respectively, the most reliable indicators in reflecting the underlying dimensions of work/study, relationship, and other harms, for both gamblers and affected others.
Number of Harms with Respect to PGSI
The number of specific harms overall, and broken down by domains, were regressed against the PGSI. As results, the linear regression slopes estimated for each harm domain and across all domains are listed in Table 10. Non-linear loess smoothed curves are displayed in Fig. 2. A common pattern arising from these regressions was greater slopes being found among gamblers who reported their own PGSI , as compared to affected others who reported others’ PGSI (in approximately 2:1 ratios). For example, each one-point increase in PGSI was associated with 0.26 (vs. 0.14) more financial harms, 0.14 (vs. 0.07) more work/study harms, 0.28 (vs. 0.13) more health harms, 0.24 (vs. 0.11) more relationship harms, and 1.34 (vs. 0.64) more harms across all domains for gamblers (vs. affected others). Hence, the amount of experienced harms was more strongly related to PGSI for gamblers than affected others. This is an unsurprising finding, given the potential link between gamblers’ PGSI and harms upon affected others is more distal than harms upon gamblers themselves. Furthermore, the strength of this link also depends on the nature of the relationships between gamblers and affected others.

Fitted regression lines
Discussion
The results of the survey point to a high level of correspondence in gambling harms experienced by gamblers and affected others. In addition, harms in all domains tended to accumulate more quickly to gamblers than to affected others as gambling problems increased. The results also provide a great deal of insights into the specific harms from each domain checklist: in terms of their prevalences, as indicators of harm severity levels, and as consequences of gambling problems. We shall discuss each of the harm domains separately below.
Financial Harms
Among all examined financial harms, bankruptcy was found to be the most severe one for both gamblers and affected others. However, it was also a relatively unreliable indicator of harm for both groups—most likely due to its low prevalence, and the fact that bankruptcy is affected by a number of other factors, such as one's capacity to borrow money and incur debt. Reduced spending (including on recreational activities) was among the least severe financial harms, supporting both the intuitive idea and the findings from Langham et al. (2016); that the first impact of even moderate gambling spending is to reduce funds available for other activities. Reduced spending on essential and beneficial items were the most reliable indicators of financial harms, for both groups. This accords with what one might propose as the definition of financial gambling harms, which is to divert money away from expenditure necessary to provide for basic needs and additional wants. The prevalence of this ‘everyday’ inability to spend money on essential and beneficial items also varied strongly with respect to evolving problem gambling status. Interestingly, the prevalence of both indicators was quite low among the non-problem gamblers (1.7 % and 1.7 % respectively), but much higher among the affected others by non-problem gamblers (18.8 % and 9.4 %). This prevalence rose dramatically to around one-third of problem gamblers (30.8 % and 31.1 %), and to a lesser degree, to around one quarter of affected others by problem gamblers (23.0 % and 23.8 %). Another harm of particular interest was sold items, which had the strongest correlations to the PGSI, among both gamblers and affected others. Hence, selling items to fund gambling should be the most reliable financial consequence of increasing gambling problems for both groups.
Work/Study Harms
Within this domain, being excluded from study, losing one’s job, and conflict at work were the most severe harms for both gamblers and affected others. On the contrary, being absent, being late, or reduced performance for work or study were the least severe, and also very reliable, indicators of work/study harms for both groups. Thus, as gambling problems begin to occur, a reliable early warning sign would appear to be the action of skipping work in order to gamble—or to deal with the consequences of a close one's gambling. Interestingly, absenteeism could be related to a number of co-morbid harms (e.g., financial, health, emotional/psychological harms), however as an isolated behavior, it offers a ready, early indicator for risk of harms among both gamblers and affected others. Performance reduction was also the most reliable work/study consequence of increasing gambling problems, as well as the most reliable predictor of general work/study harm, for both participant groups. Additionally, performance reduction was reported by the highest percentages of low-risk, moderate-risk, and problem gamblers (as identified by PGSI) , as well as their affected others.
Health Harms
Attempted suicide, requiring emergency treatment, overeating, and self-harm were the most severe indicators of health-related harms among both gamblers and affected others. However, none of these were as reliable as increased use of health services in discriminating between low and high levels of harmfulness. Early indicators of health-related harms included reduced sleep due to worry, stress, and depression. These were among the most reliable indicators of health-related harms, which more generally appeared to be those health impacts associated with emotional distress. Further, reduced sleep due to worry not only had the highest correlations with PGSI within the health domain, but was also the health harm most frequently reported by both problem gamblers and their affected others. Hence, loss of sleep is a health-related impact that could trouble both gamblers and people around them early on, then keep occurring as gambling problems become exacerbated.
Emotional/Psychological Harms
Within this domain, feelings of failure, worthlessness, escaping, extreme distress and vulnerability were the most extreme harms for both gamblers and affected others. Feelings of regret and shame were reliable early indicators of harms for gamblers themselves, whilst feelings of anger and hopelessness were among the negative emotions that tended to be first felt by those affected. These differing emotions for the two groups make sense, given the different roles, responsibilities, and perceived controls among the gamblers and the affected others. A sobering and somewhat surprising result was that feelings of worthlessness were among the most reliable indicators of emotional/psychological harms not only for gamblers, but also for affected others. This suggests that affected others tend to share and internalize the threat to self-regard that uncontrollable gambling instigates. These results are consistent with emerging awareness in terms of the psychological well-being among problem gamblers. For example, recent research indicates that pathological gambling could be associated with higher scores of anxious and depressive symptoms of psychological health (Jauregui et al. 2016).
Relationship Harms
Among both gamblers and affected others, experiencing greater relationship conflict was the most reliable discriminator and predictor of relationship harms. Conflict within relationships is generally regarded as a reliable indicator of underlying disagreements or relationship problems, and it is reasonable that it may serve as a reliable signal of gambling problems. Nevertheless, there were illuminating differences between the two groups for some indicators. For example, neglect of responsibilities was one of the earliest and least severe indicators of relationship harms for gamblers themselves. However, neglect of responsibilities appeared to be the most severe relationship harm for affected others. This has an intuitively appealing interpretation in terms of gambling problems causing a ‘cascade’ of responsibility neglect through the social networks around gamblers. Initially, gamblers are able to compensate for their time and money investments in gambling by relying on those around them to absorb the duties. However, as pressures on those around them increase with more severe gambling problems, they in turn will become more likely to neglect their responsibilities—a second order relationship effect.
Other Harms
Unlike other domains, the domain for other harms did not have an underlying construct attached, due to the diversity of harms allocated under this domain. Therefore IRT results for this domain should be interpreted with great caution. Focusing on the relationships between harm indicators and the PGSI; feeling compelled to commit a crime, not intending to pay back money, and taking money without asking first were most reliably associated with the PGSI among gamblers. This was also the case for affected others, among whom having experiences with violence and neglecting the needs of children were also more strongly associated with the PGSI. In general, associations within this domain, both in terms of reliability and with respect to the PGSI, were much lower than other domains. This reflects the fact that harms within this domain were diverse, very specific, and with quite low prevalences.
Implications
The outcome of this survey has important implications for detecting, treating, and addressing gambling related harms and problems. For both gamblers and people who are close to them, if they are only experiencing those specific harms with low IRT severity scores, that should provide them a valuable early signal. That is, early detection based on these minor harms could drive them toward acting and preventing potentially more deleterious consequences from occurring. Meanwhile, as the study findings indicate that harms could build up about twice as fast among gamblers compared to affected others, a creative detection approach would be to ‘estimate’ the degree of problems a gambler is facing by measuring the amount of harms being experienced by her/his close family or friends. This approach might be particularly valuable when gamblers try to lie or deny about the real problems (Velleman et al. 2015).
Other findings may also lead to useful insights for organizations that provide treatment or support for gamblers or affected others. These providers can prioritize their resource allocation toward those high-prevalence harms under different PGSI categories, and design corresponding strategies that can reduce or minimize their impacts. They may also pay special attention to those specific harms that could affect motivations or barriers to treatment/help-seeking. For example, not only was shame an early harm indicator, it was also most frequently reported emotional harm by problem gamblers. Since shame has been identified as a key barrier against help-seeking (Evans and Delfabbro 2005; Gainsbury et al. 2014), it would be imperative for the treatment/support providers to develop targeted public awareness campaigns to address this issue.
Conclusions and Limitations
Overall the present findings have pointed to some large commonalities in gambling-related harms occuring to gamblers and affected others. The most notable difference between the two groups appears to be in quantity, rather than quality of experienced harms. In particular, regressions of harms on PGSI among affected others have only generated slopes approximately half the size of those among gamblers. In other words, gamblers can seemingly 'export' about half of the harms they have experienced to people in their close social networks.
The results also provided evidence supporting the conceptual differences between gambling harms and PGSI-screened gambling problems. Particularly worth mentioning are those specific harms within each domain that possessed the highest correlation with PGSI, only one of which turned out the most severe harm within the corresponding domain (i.e., neglected responsibilities within the relationship domain, and only for the affected others). The checklists of harms developed for different domains, could also serve as practical and useful tools for future research into gambling related harms, on either gamblers or affected others.
There are still a few limitations to the present study. Given the complexity of the current findings and the small sample size of certain subgroups, we did not break down the heterogeneity of affected others in our analysis. However, harms experienced by affected others could vary considerably depending on the type of relationship they have with the gamblers. Hence, an important direction for future research is to examine the effects of relationship category/proximity on the type/extent of harms occurring to affected others, as well as their willingness to stay close to/supportive of the person who gambles.
Another limitation lies in the lack of cross-cultural comparisons in our study design. During recent past, a growing gambling literature has pointed to the important roles culture/ethnicity can play in shaping gambling and relevant phenomena (e.g., Chamberlain et al. 2016; Dhillon et al. 2011; Medeiros et al. 2015; Orford et al. 2005; Svetieva and Walker 2008). Investigating harm experiences and implementing the developed harm checklists cross-culturally, therefore, would lead to deeper insights on ways of evaluating and reducing harms for gamblers and affected others in different parts of the world.
Admittedly, affected others surveyed in this study assessed PGSI second-hand, and the potential issues in this approach need to be acknowledged. Argubly, participants evaluating the problems of another person would be less likely to minimize problems, leading to a potentially greater mean score. This was reflected in the slightly higher mean PGSI score reported by affected others. However, this difference accounted for only 2.2 % of the variance. In other respects, the PGSI appeared to function equivalently between participant groups. Therefore, despite this limitation, we consider the responses of affected others to provide a reasonably sound representation of harms that accrue with increasing PGSI.
The findings of this study provide critical evidence that similar harms can occur to both gamblers and people close to them. It also presents detailed profiles of evolving harms as problem gambling severity increases, and identifies the type of harms that most effectively discriminate between different levels of gambling problems. These findings are of relevance to treatment and support providers in identifying and addressing harm-minimization needs of both gamblers and affected others, and helping both break away from the ‘bad’ of gambling.
Notes
Affected others is the general term we employ to describe any person with a significant relationship to a gambler who is affected by the gambler’s behavior.
References
Blaszczynski, A. (2009). Problem gambling: We should measure harm rather than ‘cases’. Addiction, 104(7), 1072–1074.
Browne, M., Langham, E., Rockloff, M. J., Li, E., Donaldson, P., & Goodwin, B. (2015). EGM jackpots and player behaviour: An in-venue shadowing study. Journal of Gambling Studies, 31(4), 1695–1714.
Chamberlain, S. R., Leppink, E., Redden, S. A., Odlaug, B. L., & Grant, J. E. (2016). Racial-ethnic related clinical and neurocognitive differences in adults with gambling disorder. Psychiatry Research, 242, 82–87.
Currie, S. R., Miller, N., Hodgins, D. C., & Wang, J. (2009). Defining a threshold of harm from gambling for population health surveillance research. International Gambling Studies, 9(1), 19–38.
Darbyshire, P., Oster, C., & Carrig, H. (2001). The experience of pervasive loss: Children and young people living in a family where parental gambling is a problem. Journal of Gambling Studies, 17(1), 23–45.
Dhillon, J., Horch, J. D., & Hodgins, D. C. (2011). Cultural influences on stigmatization of problem gambling: East Asian and Caucasian Canadians. Journal of Gambling Studies, 27(4), 633–647.
Dickson-Swift, V. A., James, E. L., & Kippen, S. (2005). The experience of living with a problem gambler: Spouses and partners speak out. Journal of Gambling Issues,. doi:10.4309/jgi.2005.13.6.
Dixon, M. J., Harrigan, K. A., Santesso, D. L., Graydon, C., Fugelsang, J. A., & Collins, K. (2014). The impact of sound in modern multiline video slot machine play. Journal of Gambling Studies, 30(4), 913–929.
Dowling, N. A., Suomi, A., Jackson, A. C., & Lavis, T. (2015). Problem gambling family impacts: Development of the Problem Gambling Family Impact Scale. Journal of Gambling Studies,. doi:10.1007/s10899-015-9582-6.
Evans, L., & Delfabbro, P. H. (2005). Motivators for change and barriers to help-seeking in Australian problem gamblers. Journal of Gambling Studies, 21(2), 133–155.
Ferland, F., Fournier, P. M., Ladouceur, R., Brochu, P., Bouchard, M., & Pâquet, L. (2008). Consequences of pathological gambling on the gambler and his spouse. Journal of Gambling Issues, 22, 219–229.
Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index: Final report. Submitted for the Canadian Centre on Substance Abuse.
Gainsbury, S., Hing, N., & Suhonen, N. (2014). Professional help-seeking for gambling problems: Awareness, barriers and motivators for treatment. Journal of Gambling Studies, 30(2), 503–519.
Hodgins, D. C., Stea, J. N., & Grant, J. E. (2011). Gambling disorders. The Lancet, 378(9806), 1874–1884.
Holdsworth, L., Nuske, E., Tiyce, M., & Hing, N. (2013). Impacts of gambling problems on partners: Partners’ interpretations. Asian Journal of Gambling Issues and Public Health, 3(1), 1–14.
Jacobs, D. F., Marston, A. R., Singer, R. D., Widaman, K., Little, T., & Veizades, J. (1989). Children of problem gamblers. Journal of Gambling Behavior, 5(4), 261–268.
Jauregui, P., Urbiola, I., & Estevez, A. (2016). Metacognition in pathological gambling and its relationship with anxious and depressive symptomatology. Journal of Gambling Studies, 32(2), 675–688.
Kalischuk, R. G., Nowatzki, N., Cardwell, K., Klein, K., & Solowoniuk, J. (2006). Problem gambling and its impact on families: A literature review. International Gambling Studies, 6(1), 31–60.
Krishnan, M., & Orford, J. (2002). Gambling and the family: From the stress-coping-support perspective. International Gambling Studies, 2(1), 61–83.
Langham, E., Thorne, H., Browne, M., Donaldson, P., Rose, J., & Rockloff, M. (2016). Understanding gambling related harm: A proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health,. doi:10.1186/s12889-016-2747-0.
Li, E., Rockloff, M. J., Browne, M., & Donaldson, P. (2016). Jackpot structural features: Rollover effect and goal-gradient effect in EGM gambling. Journal of Gambling Studies, 32(2), 707–720.
Lorenz, V. C., & Shuttlesworth, D. E. (1983). The impact of pathological gambling on the spouse of the gambler. Journal of Community Psychology, 11(1), 67–76.
Lorenz, V. C., & Yaffee, R. A. (1988). Pathological gambling: Psychosomatic, emotional and marital difficulties as reported by the spouse. Journal of Gambling Behavior, 4(1), 13–26.
Medeiros, G. C., Leppink, E. W., Yaemi, A., Mariani, M., Tavares, H., & Grant, J. E. (2015). Electronic gaming machines and gambling disorder: A cross-cultural comparison between treatment-seeking subjects from Brazil and the United States. Psychiatry Research, 230, 430–435.
Orford, J., Templeton, L., Velleman, R., & Copello, A. (2005). Family members of relatives with alcohol, drug and gambling problems: A set of standardized questionnaires for assessing stress, coping and strain. Addiction, 100(11), 1611–1624.
Polokill. (2013). Favorite quotes from Breaking Bad. Retrieved from http://www.imdb.com/list/ls056274521/.
Rizopoulos, D. (2006). ltm: An R package for latent variable modeling and item response theory analyses. Journal of Statistical Software, 17(5), 1–25.
Rockloff, M. J., Browne, M., Li, E., & O’Shea, T. (2014). It’s a sure bet you’re going to die: Existential terror promotes gambling urges in problem players. Gambling Research, 26(1), 33–43.
Rodgers, B., Caldwell, T., & Butterworth, P. (2009). Measuring gambling participation. Addiction, 104(7), 1065–1069.
Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36.
Salonen, A. H., Castrén, S., Alho, H., & Lahti, T. (2014). Concerned significant others of people with gambling problems in Finland: A cross-sectional population study. BMC Public Health,. doi:10.1186/1471-2458-14-398.
Svetieva, E., & Walker, M. (2008). Inconsistency between concept and measurement: The Canadian Problem Gambling Index (CPGI). Journal of Gambling Issues, 22, 157–173.
Vandenberg, R. J., & Lance, C. E. (2000). A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organizational Research Methods, 3(1), 4–70.
Velleman, R., Cousins, J., & Orford, J. (2015). Effects of gambling on the family. In H. Bowden-Jones & S. George (Eds.), A clinician’s guide to working with problem gamblers (pp. 90–103). London, New York: Routledge/Taylor & Francis Group.
Wohl, M. J., Gainsbury, S., Stewart, M. J., & Sztainert, T. (2013). Facilitating responsible gambling: The relative effectiveness of education-based animation and monetary limit setting pop-up messages among electronic gaming machine players. Journal of Gambling Studies, 29(4), 703–717.
Acknowledgment
This research was funded by a grant from the Victorian Responsible Gambling Foundation. A previous version of this paper has been submitted as part of a research report to the Victorian Responsible Gambling Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
En Li has received research grants from the Victorian Responsible Gambling Foundation and Gambling Research Australia. Matthew Browne has received grants from the Victorian Responsible Gambling Foundation, the New Zealand Ministry of Health and Gambling Research Australia. Erika Langham has received grants from the Victorian Responsible Gambling Foundation, the New Zealand Ministry of Health and Gambling Research Australia. Matthew Rockloff has received grants from the Queensland Treasury, the Victorian Treasury, the Victorian Responsible Gambling Foundation, the New Zealand Ministry of Health and Gambling Research Australia. Vijay Rawat declares no conflicts of interest.
Ethical Approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Li, E., Browne, M., Rawat, V. et al. Breaking Bad: Comparing Gambling Harms Among Gamblers and Affected Others. J Gambl Stud 33, 223–248 (2017). https://doi.org/10.1007/s10899-016-9632-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-016-9632-8