
Abstract
Efforts to examine barriers to the implementation of evidence-based practices (EBPs) have largely focused on community mental health settings, although many people receive mental health services in private practice settings. Clinicians working in private practice likely face unique barriers to EBP implementation, but identifying strategies to increase EBP use in this setting is an understudied area of implementation research. The consolidated framework for implementation research (CFIR) provides an overview of multi-level determinants that influence implementation. The Characteristics of Individuals domain of the CFIR focuses on individual-level implementation determinants, such as perceptions of an intervention and self-efficacy in delivering it. Within the private practice context, little is known about how individual clinicians perceive EBPs and how this might influence their use of them. Thus, this study examined responses from qualitative interviews with 20 private practice clinicians to assess individual-level EBP implementation determinants in this context. Clinicians identified a range of attitudes towards EBPs and described how client factors influence their EBP use. Concerns about EBPs included perceptions that EBPs are too structured, are not generalizable to clinical practice, and are not suitable for a range of client populations. Clinicians also described several barriers and facilitators related to training in EBPs. Clinicians with training in exposure therapy (a well-established, but difficult-to-implement EBP) generally reported more positive attitudes, fewer barriers, and more frequent EBP use. Potential strategies to support EBP implementation in private practice are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Despite extant literature that highlights the importance of using evidence-based practices (EBPs) for mental health disorders to improve patient outcomes (e.g., Aarons et al., 2017; Weisz et al., 2005), EBPs remain underutilized in routine clinical settings (Kazdin, 2017; Waller & Turner, 2016). The field of implementation science aims to promote the integration of research into clinical practice (Eccles & Mittman, 2006) by considering the contexts in which implementation occurs and using tailored strategies to address implementation determinants. The consolidated framework for implementation research (CFIR; Damschroder et al., 2009) outlines the multi-level determinants that influence implementation, such as individual clinician factors (e.g., knowledge of and beliefs about an intervention; referred to as Characteristics of Individuals) and contextual factors (e.g., organizational climate and external policies; referred to as Inner Setting and Outer Setting). While there is clear value in examining contextual factors that influence EBP implementation (Becker-Haimes et al., 2019), many barriers to EBP implementation exist at the individual level and may be responsive to intervention (e.g., via training; Frank et al., 2020). The CFIR highlights the importance of assessing individual level determinants given that collective changes in individual behavior is what leads to organizational, professional, and cultural change. Furthermore, understanding individual-level determinants can inform the development of organization-level implementation strategies that support broad behavioral change.
Efforts to examine implementation determinants for mental health EBPs have largely focused on community mental health and other publicly funded mental health services, yet many receive mental health services in private practice (Wray et al., 2021) and clinicians working in private practice represent a large portion of the workforce (Michalski et al., 2010). While clinicians working in private practice have been included as a subset of participants in studies of practicing clinicians (e.g., Borntrager et al., 2009; Reid et al., 2017), few studies have focused specifically on clinicians in the private sector (Reif et al., 2012). Research focused on implementation in community mental health and other settings may not generalize to private practice given differences in individual- and organization-level factors across settings. Thus, to bridge the research-practice gap, more research is needed to identify the unique determinants of EBP implementation reported by private practice clinicians.
One key barrier to EBP implementation across multiple settings is insufficient training (Kilbourne et al., 2018; Whiteside et al., 2016). Lack of training may be due in part to a lack of access to training (Kobak et al., 2017) and costs associated with training (Powell et al., 2013; Stewart et al., 2012). Organizational support can facilitate training attendance and subsequent EBP implementation in community mental health settings (Becker-Haimes et al., 2020; Wolitzky-Taylor et al., 2018), but may be more limited in private practice (Frank et al., 2022). Similarly, tailoring training to clinicians’ preferences may increase training attendance and effectiveness, but no studies have examined the specific training preferences and needs of private practice clinicians. More research is needed to assess training barriers and preferences reported by private practitioners in order to create training approaches that respond to clinicians’ needs, facilitate attendance, and support EBP implementation in this setting.
Another determinant of EBP implementation across multiple settings is clinician attitudes toward EBPs. Some clinicians report negative attitudes toward EBPs broadly (Aarons et al., 2004; Pagoto et al., 2007), while others report positive attitudes toward EBPs but reluctance to use specific EBPs (e.g., manuals) in clinical practice (Borntrager et al., 2009). Clinician concerns include that EBPs cannot be tailored to individual clients, do not prioritize therapeutic alliance, and are not feasible to use in routine practice (Nelson et al., 2006; Reid et al., 2017). Exposure therapy (“exposure”), which involves encouraging patients to gradually approach feared situations, is the most common element across a range of evidence-based treatments for anxiety, obsessive–compulsive, and traumatic stress disorders (Chorpita & Daleiden, 2009), yet it yields particularly negative attitudes (Deacon et al., 2013; Farrell et al., 2013). Many clinicians report beliefs that exposure will be intolerably aversive for the client or clinician, can exacerbate client symptoms, and may lead to dropout (Pittig et al., 2019). These negative attitudes predict less exposure use (de Jong et al., 2020; Reid et al., 2018) and are one explanation for the low adoption of this intervention in routine clinical settings (Becker-Haimes et al., 2017; Whiteside et al., 2016). While negative attitudes toward EBPs may be a result of misconceptions of EBPs in some instances (Lilienfeld et al., 2013), there may be other instances in which clinicians’ experiences in practice highlight limitations of existing EBPs that need to be addressed (i.e., practice-based evidence; Barkham & Mellor-Clark, 2003). For example, while exposure delivered by trained clinicians poses few risks to clients, exposure has the potential to cause harm if applied improperly or to populations for whom it is contraindicated (see McKay et al., 2021). Understanding negative attitudes is critical both to inform training strategies to address misconceptions and to inform efforts to modify existing EBPs to fit the needs of practicing clinicians. In particular, while previous studies have examined attitudes toward EBPs and exposure in samples that include clinicians working in private practice (e.g., Borntrager et al., 2009; Reid et al., 2018), few have focused exclusively on this clinical setting.
Another factor worth consideration is how client characteristics impact clinicians’ perceptions of EBPs. Given that the population of clients who receive services through private practice differs from those who receive services through community mental health settings, there are likely differences in how client characteristics influence EBP implementation in each setting. For example, client demographic and socioeconomic characteristics differ between community mental health and private practice settings (Wray et al., 2021), and it is likely that clients’ needs and resources (e.g., financial, emotional) are factored into clinical decision-making. In addition, existing evidence highlights that clients’ clinical presentations affect clinicians' decisions related to EBP use (Ringle et al., 2015; Stewart et al., 2018). Still, no studies have examined specific client characteristics that affect clinicians’ implementation of EBPs in private practice. More research is needed to understand individual-level factors that influence EBP use among private practitioners to inform efforts to tailor EBPs and support their effective implementation.
The current study addresses this gap in the literature by using qualitative interviews conducted with private practice clinicians to assess individual-level EBP implementation determinants as outlined by the CFIR domain Characteristics of Individuals. This domain includes individuals’ perceptions of an intervention, their self-efficacy in delivering the intervention, their readiness for change, their relationship to their organization, and other personal traits. We also assessed perceptions of and preferences for training given that this is a frequently cited barrier to clinicians' adoption of EBPs broadly and exposure specifically.
Method
Participant Recruitment
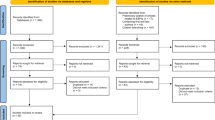
All procedures were approved by the Lifespan Institutional Review Board. We used purposive sampling to recruit approximately equal numbers of mental health clinicians with and without previous training in exposure. To recruit participants with previous training in exposure, we contacted clinicians who had previously participated in a training study (NIMH #3R01MH112516) and agreed to be contacted for future studies. Additional participants with and without prior training in exposure were recruited through electronic study advertisements. Participants who completed qualitative interviews were asked if they were willing to provide information about the study to colleagues to facilitate additional recruitment. Participant recruitment was informed by the Dillman Tailored Design Survey Method (Hoddinott & Bass, 1986). Participants who indicated interest in the study were contacted via email to complete a demographics survey and schedule a qualitative interview. Data saturation was met after 20 interviews after which we did not recruit or interview additional clinicians.
Qualitative Interview Procedure
Two interviewers, a postdoctoral fellow and doctoral student, conducted semi-structured, one-on-one phone interviews with participants. The postdoctoral fellow had previous experience conducting qualitative interviews and trained the doctoral student. Both interviewers deliver exposure therapy and conduct research on methods to increase the uptake of EBPs. Interviewers did not have previous relationships with participants, nor did they have contact with participants after interviews. Participants were told that the interviewers were affiliated with a specialty anxiety clinic and interested in understanding factors that influence EBP use.
Qualitative Interview Guide
A semi-structured qualitative interview guide (available upon request) was used to assist interviewers in assessing clinicians' perceived determinants of EBP and exposure use. All participants were provided with a definition of exposure given potential variability in familiarity with this term. Participants were asked about how training and consultation could support their use of EBPs and exposure. Follow-up probes for each question were informed by the CFIR, as well as by the Policy Ecology Framework (Raghavan et al., 2008). A separate manuscript reports on outcomes related to the Policy Ecology Framework (Frank et al., 2022). Interviews were audio recorded and lasted approximately one hour each. Study procedures adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Tong et al., 2007).
Qualitative Data Analysis
Interview recordings were transcribed using NVivo transcription services, checked by undergraduate research assistants, and spot checked by study authors. Interviews were coded by a postdoctoral fellow and a research assistant using a directed content analysis approach (Hsieh & Shannon, 2005) wherein data were analyzed deductively using an a priori coding framework developed from components of the CFIR (i.e., Characteristics of Individuals domain) and existing literature on factors influencing EBP and exposure use (i.e., training). Emergent themes not represented in this framework derived through inductive analysis were also examined. Coders collaboratively reviewed six transcripts to inform their iterative development of a codebook and then independently applied codes to two transcripts to determine initial interrater reliability. Both coders independently coded transcripts with 20% overlap (n = 4 transcripts). Coding discrepancies were resolved through discussion and consensus. Data were managed within NVivo qualitative data software to allow for ease of coding across multiple analysts.
Results
Participant Characteristics
Participants included 20 mental health clinicians (M age = 46.25, 90% female, 90% White, 100% non-Hispanic) who hold an advanced degree (65% Doctoral, 35% Master’s) in a mental health field and work in a solo (55%) or group (45%) private practice clinical setting. Participants endorsed the following theoretical orientations, with several selecting more than one: cognitive-behavioral (n = 8), eclectic (n = 4), family systems (n = 4), feminist (n = 3), third wave (n = 2), humanistic (n = 1), solutions-focused (n = 1), strengths-based (n = 1), none reported (n = 5). Nine clinicians (45%) had previously attended a full-day or longer exposure training, whereas eleven clinicians (55%) had never attended an exposure training.
Overview of Findings
Analysis of qualitative data yielded several themes that are consistent with the CFIR domain Characteristics of Individuals and with this study’s emphasis on understanding training related EBP implementation determinants. Rather than covering the entire Characteristics of Individuals CFIR domain (i.e., knowledge and beliefs about the intervention, self-efficacy, individual stage of change, individual identification with organization, other personal attributes), most responses focused on clinicians’ attitudes toward EBPs. ‘Client-related EBP implementation determinants’ was an emergent code derived through inductive analysis. In the following sections, we first report on clinician-related implementation determinants that align with the CFIR Characteristics of Individuals domain, including knowledge of, beliefs about, and attitudes toward EBPs and exposure. Second, we describe responses from our emergent code, which focused on client-related determinants of EBP and exposure implementation. Given existing research suggesting that training can affect attitudes and perceptions of barriers, we describe how reports of clinician- and client-related determinants varied based on whether clinicians had received previous training in exposure. Finally, we report on clinicians’ perceptions of training, including barriers, facilitators, and preferences.
Characteristics of Individuals: Clinician-Related Implementation Determinants
Attitudes Toward EBP Broadly
Clinicians with exposure training generally endorsed positive attitudes toward EBPs. In contrast, clinicians without exposure training reported more mixed attitudes toward EBPs. Although some clinicians without exposure training reported neutral or positive attitudes, many reported negative attitudes toward EBPs. One clinician described, “when it comes to evidence-based practices, [there is] negative stigma around that word for me.” Many clinicians without exposure training also endorsed skepticism about what is called ‘evidence-based’ given that not every clinical presentation can be studied.
Attitudes Toward Evidence-Based Assessment
There were not specific differences in attitudes toward evidence-based assessment based on training history. Some clinicians described using evidence-based assessment to inform their clinical practice. These clinicians cited different purposes for using standardized progress measures, including informing treatment goals and planning, assessing client symptoms and treatment progress, and providing feedback to the client. In contrast, other clinicians reported that they do not find evidence-based assessment helpful to inform clinical practice.
Concerns About the Generalizability of Research to Clinical Practice
Clinicians identified limitations of research, particularly concerns about the generalizability of research to clinical practice. They expressed concern that randomized controlled trials do not necessarily reflect the complexity of most cases and that one EBP may be too narrow in scope to address all of a client’s needs. One clinician described, “I’m a firm believer that one protocol does not treat a whole person.” Clinicians with exposure training reported combining multiple EBPs to address these limitations but identified a need for more information on what steps to take if the primary intervention does not work for a particular client. Clinicians without exposure training emphasized the importance of prioritizing rapport and tailoring treatment to the individual. Clinicians without exposure training also reported that EBPs often take more time in their practice than manuals recommend, and that the principles of EBPs may be more helpful than the manualized steps.
Concerns About EBP Structure
Clinicians cited EBP structure as a barrier to its implementation, such that EBPs are often not practical to use exactly as they are designed. Clinicians with exposure training indicated that they use EBPs flexibly to address this barrier, whereas clinicians without exposure training indicated that the amount of structure in protocols acts as a barrier to EBP implementation.
Exposure-Specific Attitudes
Clinicians with and without exposure training noted the need for more training in exposure, and especially in what to do when exposure does not work for a particular client. Clinicians with exposure training generally described exposure positively, reporting that they enjoy using it with clients and in their own lives. Some clinicians with exposure training noted prior worry or skepticism about exposure (“It felt so uncomfortable to actively make clients anxious. It's so foreign to most of what we're doing”) but reported that seeing exposure work for their clients motivated them to continue using it. Clinicians with exposure training described that exposure is generally well-received by clients, but that they sometimes need to provide rationale for exposure to obtain initial client buy-in from those who are hesitant. They also noted that treatment progress using exposure can be slow, especially for clients who are not adherent in completing exposures outside of session. Clinicians without exposure training reported more mixed attitudes toward exposure. Some clinicians without exposure training noted that exposure can be helpful and may provide the client with a sense of self-efficacy. Others noted that exposure is useful but poses challenges for the clinician, such as by requiring a strong therapeutic relationship, client buy-in, and steps to avoid potential harm. Some clinicians without exposure training reported that exposure “sounds awful” for the client, causes stress for themselves as clinicians, and is not a modality they want to use.
Client-Related Implementation Determinants
Client Diagnoses/Clinical Presentations
Clinicians indicated that they consider clients’ diagnoses and clinical presentations when deciding whether to implement an EBP. Clinicians with exposure training indicated a tendency to default to using EBPs, to consider a patient’s treatment to guide the selection of EBPs, and to integrate other treatment approaches when necessary for co-occurring problems. Some clinicians with exposure training described difficulty sustaining EBP use when patients do not exhibit treatment response as expected (e.g., “For patients who have been in care for a longer time, […] it is hard to keep coming up with evidence-based ideas”). Clinicians without exposure training described looking to the evidence base when unsure what to do for a particular case but noted the limitation that there is not an evidence base for certain populations (e.g., transgender clients).
Client Age/Developmental Considerations
Clinicians also noted considerations for working with children. They noted the importance of considering a child’s cognitive level when selecting an intervention, and that some EBPs may feel too formal or advanced for young children. Still, clinicians generally reported that it is easier to use EBPs with younger rather than older children, in part because younger children may respond better to structure (e.g., worksheets) and older children may have less buy-in and motivation for treatment. There were no notable differences in descriptions of client age/developmental considerations between clinicians with and without exposure training.
Client Expectations and Motivation for Treatment
Clinicians reported that client expectations and motivation for treatment often inform their clinical decision-making and use of EBPs. They highlighted the importance of building rapport with clients to facilitate communication about treatment goals and shared decision-making of which interventions to use. Clinicians also emphasized the necessity of flexibility to deviate from EBPs when necessary to preserve rapport. They reported greater comfort and ease using EBPs with clients who are more willing and motivated, as clients who are unwilling or unmotivated may not adhere to the intervention, which may lead to treatment non-response and clinician burnout. Providing psychoeducation before beginning an EBP was described as increasing client motivation. However, participants noted that some clients remain unwilling to engage in EBPs; those who do not initially experience symptom improvement may be less interested in EBPs in future sessions. Overall, clinicians indicated that if a client is unwilling to engage in an EBP, they may try a different intervention first. There were no notable differences in descriptions of client expectations between clinicians with and without exposure training.
Client and Family Resources
Clinicians reported that client and family resources can facilitate EBP use. Financial resources, such as the ability to afford treatment, transportation, childcare, and technology (i.e., for telehealth), can facilitate treatment adherence and progress, particularly for EBPs that require parental involvement or homework completed outside of session. Client education was also described as facilitating EBP implementation. There were no notable differences in descriptions of client and family resources between clinicians with and without exposure training.
Client Characteristics that Affect Exposure Implementation
Clinicians noted that client age and developmental level affect exposure implementation such that older children may be more cognitively able to understand exposure rationale and/or more motivated to do exposure independently without parental involvement. Clinicians mentioned that building rapport is especially important before beginning exposure because exposure requires trust from the client. One clinician described, “If I've been working with someone for a while […], I kind of feel like I can push them more.” Client willingness and motivation were described as affecting exposure implementation similarly to EBP implementation broadly, such that higher willingness and motivation facilitates exposure implementation. Clinicians with exposure training indicated that they would always default to using exposure for diagnoses for which it is appropriate. Clinicians with exposure training cited obsessive–compulsive disorder, social anxiety, and specific phobia as diagnoses for which exposure is their treatment of choice, and cited depression and generalized anxiety disorder as examples of diagnoses that may warrant other, non-exposure intervention (e.g., cognitive therapy). In contrast, clinicians without exposure training indicated an understanding of the theoretical rationale for using exposure, but do not necessarily use exposure as their default intervention. Clinicians without exposure training reported that it might not be effective to do exposure immediately if a client is too distressed to engage in exposure, if they are not cognitively able to understand it, or if they have other concerns that warrant treatment first.
Clinicians’ Perceptions of Training
Barriers to Training
Clinicians reported receiving training in EBPs from various sources including via graduate school, peer consultation (within their organization or externally), professional organizations, and online (e.g., listservs, Facebook groups). Despite citing several avenues through which they seek training, clinicians identified barriers to attending training. Time constraints were noted as a key barrier to both formal and informal training. Clinicians described difficulty attending formal training events, participating in peer consultation, and attending online trainings due to time constraints. Availability of training (at a desired skill level, covering topics of interest), travel, cost, and organizational support were also identified as barriers to training attendance. Training barriers were described as impeding EBP implementation.
Preferences for and Facilitators of Training
Clinicians described training preferences that may facilitate training attendance and subsequent EBP implementation. Although time constraints remain a potential barrier, clinicians indicated that longer and more frequent training would help support EBP implementation. Splitting training into multiple separate parts rather than a long, multi-day event was described as one way to facilitate attendance. The availability of “in-house” training offered by their organization was described as a way to improve training attendance and subsequent EBP implementation. One clinician described, “I think it was incredibly valuable for [clinicians] to all have gone through the training together and to have it as a common modality and have the supervision. It’s bonding.” The availability of online training was also described as addressing some attendance barriers such as travel burden and time constraints. Clinicians also indicated that certain teaching styles may better facilitate content learning. Clinicians reported that an ideal training would include both theory and practice and would include interactive or multi-media components rather than solely lecture format. Experiential training, role-play, live supervision, and offering take-home materials were identified as particularly helpful for learning. Clinicians also highlighted the value of expert consultation to support training in EBPs. Some clinicians noted the benefit of receiving certification from training, although it was not indicated as necessary for training attendance or EBP use. Finally, clinicians expressed that, after receiving formal training, weekly to monthly consultation within their organization and/or yearly refresher courses would be ideal, although these are not always feasible to attend due to time constraints.
Exposure-Specific Training Barriers and Preferences
Clinicians generally described difficulty finding training in exposure compared to other EBPs. In addition, clinicians noted that learning to use exposure may require more or different training than learning to use other EBPs. One clinician described, “If someone is learning exposure and response prevention for the first time, in-person is the most [helpful] because you can ask questions in the moment and do role-play.” Responses from clinicians suggested that, while broad clinician preferences for training should be considered, there may also be intervention-specific considerations for tailoring training.
Discussion
This study used the consolidated framework for implementation research (CFIR) Characteristics of Individuals domain to guide inquiry into clinicians’ perceptions of EBP implementation determinants in private practice. Results focused on clinician attitudes toward EBPs, perceptions of client characteristics that affect EBP implementation, and training barriers and preferences. Findings were generally consistent with studies of EBP implementation determinants in community mental health settings but highlight specific individual-level factors that influence implementation in private practice. These results provide insight into clinicians’ perspectives of EBPs and potential strategies to support EBP implementation in this setting.
Clinicians in this study emphasized the importance of training to support the implementation of new interventions, including EBPs, in their routine clinical practice. Clinicians described seeking training from a wide range of sources but reported several barriers to training attendance and subsequent intervention implementation. Availability of training in desired content areas, travel, cost, and time constraints were identified as key barriers to training attendance, while offering training online or “in-house”, utilizing interactive training formats, and providing ongoing consultation and/or certification after training were described as facilitating training attendance and content learning. These findings are consistent with previous studies examining training-related implementation determinants in private practice (Reid et al., 2017; Stewart et al., 2012) and other routine clinical settings (Herschell et al., 2014; Powell et al., 2013) and point to ways in which trainings may be modified to respond to clinician needs. Offering training online may reduce financial barriers and is likely equally effective as in-person training (Frank et al., 2020). Splitting training into multiple parts rather than one long, multi-day event was described by clinicians as an effective way to reduce time-related barriers and increase the feasibility of attending training. Tailoring training activities to the content areas of interest and skill levels of the intended audience and offering certification from training may also facilitate training attendance. Furthermore, interactive and experiential training components and providing take-home materials may facilitate content learning. In addition, as noted by the CFIR, organizational support can likely facilitate training attendance and content learning (e.g., offering compensation for training, training and refresher courses within the organization, ongoing supervision, or expert consultation after training), but organizational support varies widely in private practice (Frank et al., 2022). Larger-scale efforts may be needed to increase organizational support for clinicians working in private practice settings in order to facilitate training attendance and subsequent EBP implementation in this setting. This may involve creating consortiums of clinicians to pool resources for training activities. Lastly, training attendance and EBP implementation are likely influenced by attitudes toward EBPs (Stewart et al., 2012), and these attitudes likely vary based on context.
In this vein, respondents reported varying knowledge and beliefs about EBPs, which is a construct within the Characteristics of Individuals CFIR domain that has been a focus of much prior research focused on individual behavior change. Respondents described concerns about the generalizability of EBP research to practice, the ability to tailor EBPs to clients, and the structured nature of EBPs, which are all consistent with concerns reported by clinicians in publicly funded mental health settings (Borntrager et al., 2009; Ringle et al., 2015). Notably, clinicians with exposure training generally described more positive attitudes toward and use of EBPs, whereas clinicians without exposure training reported more mixed attitudes and identified more barriers to EBP use. This aligns with research suggesting that clinicians form unique attitudes toward EBPs based on personal experience and contextual factors (Corrie & Callanan, 2001). It is also possible that training in exposure improved attitudes toward EBPs broadly, complementing evidence that broad EBP training improves attitudes toward exposure (Woodard et al., 2021). Alternatively, clinicians with more positive attitudes toward EBPs may have been more likely to seek training in exposure. In any case, it is evident that efforts are needed to better understand negative attitudes toward EBPs reported by private practice clinicians. Training offers one opportunity to address negative attitudes, and training in EBPs should directly target misconceptions about EBPs and about research more broadly. Training in EBPs should also emphasize the flexible nature of EBPs and describe clear steps for what to do when an EBP does not work as expected. Still, it is necessary to acknowledge the limitations of existing EBPs for certain clinical populations and provide guidance for using a synthesis of clinical judgment with any existing research evidence (APA Presidential Task Force, 2006).
Accordingly, clinicians in this study described various client characteristics that act as determinants of EBP implementation. Respondents indicated that clients' clinical presentations, ages, and resources (e.g., financial) inform EBP use. They identified specific characteristics that impede EBP use, such as the presence of comorbid diagnoses, client identities for which EBPs have not yet been developed, non-response to previous psychotherapy, and lack of client motivation or resources to facilitate EBP adherence. Findings are generally consistent with studies conducted in community mental health settings (Chu et al., 2015; Ringle et al., 2015), although there was no mention of emergent needs (e.g., food or housing insecurity), which have been identified as barriers to EBP implementation in community settings (Frank et al., 2021). Efforts to target client-related implementation barriers may aim to increase training in the flexible application of EBPs to treat clients with diverse backgrounds, identities, and presenting problems. Training should also focus on creating client buy-in for EBPs. Moreover, larger-scale efforts are needed to reduce barriers to accessing EBPs for families, such as by leveraging technology to deliver EBPs via telehealth (Sugarman et al., 2021).
Lastly, this study describes individual-level factors that influence the implementation of exposure therapy, a well-established but difficult to implement EBP. Clinicians reported wide variability in attitudes toward exposure. Clinicians with exposure training generally endorsed more positive attitudes, although they still noted limitations of exposure and barriers to its implementation. In contrast, clinicians without exposure training reported more mixed to negative attitudes and more concerns about using exposure in their practice. Similar negative attitudes toward exposure have been reported in other studies and appear to act as an implementation barrier (Deacon et al., 2013). Although research evidence may dispel some misconceptions about exposure (Meyer et al., 2014), clinicians may rely more on clinical experience than research evidence to make clinical decisions (Stewart et al., 2018). Clinicians described difficulty finding training in exposure compared to other EBPs, as is consistent with previous studies of private practice (Reid et al., 2017) and community mental health (Wolitzky-Taylor et al., 2018) clinicians. Clinicians emphasized the importance of interactive training to teach exposure compared to other EBPs, consistent with literature suggesting that experiential learning can effectively alleviate concerns about exposure (Farrell et al., 2016; Frank et al., 2020). Thus, strategies to facilitate exposure implementation in private practice should focus on increasing the availability of specialized training in exposure (Wolitzky-Taylor et al., 2018) and providing corrective information about exposure during training (e.g., that exposure is not harmful when delivered appropriately, that exposure can be used with a wide range of clients; Farrell et al., 2013). Organizations that wish to increase exposure use should provide ongoing consultation and support for clinicians delivering exposure (Becker-Haimes et al., 2020; Frank et al., 2022). Still, while there is value in disseminating research evidence to address certain “myths” about exposure, there is also likely information about exposure implementation in routine clinical care that is not reflected in the literature. More efforts are needed to center the perspectives of clinicians and clients (i.e., practice-based evidence; Barkham & Mellor-Clark, 2003) and tailor exposure (and other EBPs) to meet the needs of those delivering and receiving them (Trivasse et al., 2020). The goals of practice-based evidence and EBPs are complementary and should be considered in tandem to harness the value of clinicians’ knowledge with existing research evidence. Overall, these recommendations are largely consistent with those that have been proposed to increase exposure use in other settings, but more research is needed to assess the feasibility of such approaches within the private practice context.
A key strength of this study is the use of purposive sampling to include clinicians with and without exposure training, given that training in a difficult-to-implement EBP may influence clinician attitudes and preferences for training. An additional strength of this study is the inclusion of clinicians working in a range of private practice settings (e.g., solo versus group private practice), as this organizational context may also affect attitudes and training preferences. This study also has some limitations. The sample size of this study was small, and the sample of clinicians included in this study lacked diversity across several dimensions, including ethnoracial identity, geographical location, and theoretical orientation. It is imperative that future research assess perspectives across a diverse range of clinicians and consider the ways in which clinicians' identities, geographical locations, and theoretical orientations may affect attitudes toward and implementation of EBIs and exposure. In addition, clinicians included in this study were all those who agreed to participate in a research study, and some of the clinicians in this study had previously participated in a clinician training research study conducted by the same organization. Participation in this study may indicate that these clinicians are open to research and/or hold more positive attitudes toward EBPs than those who would refuse to participate in a research study. Even among our participants, they noted a perceived disconnect between research and real-world practice. Thus, it will be critical for future research to include clinicians with a wide array of perceptions of research. Furthermore, it is important to note that the researchers conducting interviews and analyses have an interest in supporting the increased use of EBPs and made this known to participants, which likely had an influence on ensuing discussions. This study is also limited in that we did not measure actual EBP use in clinicians’ routine practice, nor did we collect information on the nature of previous training in exposure for clinicians with previous training. Finally, this study focused primarily on one set of individuals—clinicians—relevant to the Characteristics of Individuals domain of the CFIR. We did not receive input from other stakeholders involved in the delivery and receipt of mental health care, such as patients, policymakers, and organization leaders; these perspectives are central understanding the full breadth of implementation determinants as outlined by the CFIR. Assessing perceptions of EBPs among these stakeholders and across other CFIR domains will likely yield important information to complement the current study and inform strategies to tailor EBPs to meet the needs of all involved in mental health care.
Nonetheless, this study provides novel information about EBP implementation determinants in private practice as measured at the individual clinician level. Specifically, this study highlights training-related barriers and facilitators, clinician attitudes, and client characteristics that may affect the implementation of EBPs in private practice. Our findings are used to inform suggestions for implementation strategies to address barriers to EBP use in this setting. Overall, it is evident that the perspectives of individual clinicians are one aspect of many that contribute to successful EBP implementation. These results should be considered in the context of other CFIR domains, such as the Inner Setting and Outer Setting, which likely have a bidirectional influence on individuals. For instance, contextual factors such as organizational support and implementation climate (Becker-Haimes et al., 2019) interact with individual-level factors to impede or facilitate successful EBP implementation. Tailoring our proposed individual-level implementation strategies for the private practice context (Inner Setting) may mark one step toward increasing EBP implementation and sustainment in private practice mental health.
References
Aarons, G. A. (2004). Mental health provider attitudes toward adoption of evidence-based practice: The evidence-based practice attitude scale (EBPAS). Mental Health Services Research, 6(2), 61–74.
Aarons, G. A., Sklar, M., Mustanski, B., Benbow, N., & Brown, C. H. (2017). “Scaling-out” evidence-based interventions to new populations or new health care delivery systems. Implementation Science, 12(1), 111.
APA Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61, 271–285.
Barkham, M., & Mellor-Clark, J. (2003). Bridging evidence-based practice and practice-based evidence: Developing a rigorous and relevant knowledge for the psychological therapies. Clinical Psychology & Psychotherapy, 10(6), 319–327.
Becker-Haimes, E. M., Byeon, Y. V., Frank, H. E., Williams, N. J., Kratz, H. E., & Beidas, R. S. (2020). Identifying the organizational innovation-specific capacity needed for exposure therapy. Depression and Anxiety, 37(10), 1007–1016.
Becker-Haimes, E. M., Okamura, K. H., Wolk, C. B., Rubin, R., Evans, A. C., & Beidas, R. S. (2017). Predictors of clinician use of exposure therapy in community mental health settings. Journal of Anxiety Disorders, 49, 88–94.
Becker-Haimes, E. M., Williams, N. J., Okamura, K. H., & Beidas, R. S. (2019). Interactions between clinician and organizational characteristics to predict cognitive-behavioral and psychodynamic therapy use. Administration and Policy in Mental Health and Mental Health Services Research, 46(6), 701–712.
Borntrager, C. F., Chorpita, B. F., Higa-McMillan, C., & Weisz, J. R. (2009). Provider attitudes toward evidence-based practices: are the concerns with the evidence or with the manuals? Psychiatric Services, 60(5), 677–681.
Chorpita, B. F., & Daleiden, E. L. (2009). Mapping evidence-based treatments for children and adolescents: Application of the distillation and matching model to 615 treatments from 322 randomized trials. Journal of Consulting and Clinical Psychology, 77(3), 566–579.
Chu, B. C., Crocco, S. T., Arnold, C. C., Brown, R., Southam-Gerow, M. A., & Weisz, J. R. (2015). Sustained implementation of cognitive-behavioral therapy for youth anxiety and depression: Long-term effects of structured training and consultation on therapist practice in the field. Professional Psychology, Research and Practice, 46(1), 70–79.
Corrie, S., & Callanan, M. M. (2001). Therapists’ beliefs about research and the scientist-practitioner model in an evidence-based health care climate: A qualitative study. British Journal of Medical Psychology, 74(2), 135–149.
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., & Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science, 4(1), 50.
de Jong, R., Lommen, M. J. J., van Hout, W. J. P. J., de Jong, P. J., & Nauta, M. H. (2020). Therapists’ characteristics associated with the (non-)use of exposure in the treatment of anxiety disorders in youth: A survey among Dutch-speaking mental health practitioners. Journal of Anxiety Disorders, 73, 102230.
Deacon, B. J., Farrell, N. R., Kemp, J. J., Dixon, L. J., Sy, J. T., Zhang, A. R., & McGrath, P. B. (2013). Assessing therapist reservations about exposure therapy for anxiety disorders: The therapist beliefs about exposure scale. Journal of Anxiety Disorders, 27(8), 772.
Eccles, M. P., & Mittman, B. S. (2006). Welcome to implementation science. Implementation Science. https://doi.org/10.1186/1748-5908-1-1
Farrell, N. R., Deacon, B. J., Dixon, L. J., & Lickel, J. J. (2013). Theory-based training strategies for modifying practitioner concerns about exposure therapy. Journal of Anxiety Disorders, 27(8), 781–787.
Farrell, N. R., Kemp, J. J., Blakey, S. M., Meyer, J. M., & Deacon, B. J. (2016). Targeting clinician concerns about exposure therapy: A pilot study comparing standard vs. enhanced training. Behaviour Research and Therapy, 85, 53–59.
Frank, H. E., Becker-Haimes, E. M., & Kendall, P. C. (2020). Therapist training in evidence-based interventions for mental health: A systematic review of training approaches and outcomes. Clinical Psychology: Science and Practice, 27(3), e12330.
Frank, H. E., Last, B. S., AlRabiah, R., Fishman, J., Rudd, B. N., Kratz, H. E., Harker, C., Fernandez-Marcote, S., Jackson, K., Comeau, C., Shoyinka, S., & Beidas, R. S. (2021). Understanding therapists’ perceived determinants of trauma narrative use. Implementation Science Communications, 2(1), 131.
Frank, H. E., Milgram, L., Freeman, J. B., & Benito, K. G. (2022). Expanding the reach of evidence-based mental health interventions to private practice: Qualitative assessment using a policy ecology framework. Frontiers in Health Services, 50.
Herschell, A. D., Reed, A. J., Person Mecca, L., & Kolko, D. J. (2014). Community-based clinicians’ preferences for training in evidence-based practices: A mixed-method study. Professional Psychology: Research and Practice, 45(3), 188–199.
Hoddinott, S. N., & Bass, M. J. (1986). The dillman total design survey method. Canadian Family Physician, 32, 2366.
Hsieh, H.-F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288.
Kazdin, A. E. (2017). Addressing the treatment gap: A key challenge for extending evidence-based psychosocial interventions. Behaviour Research and Therapy, 88, 7–18.
Kilbourne, A. M., Beck, K., Spaeth-Rublee, B., Ramanuj, P., O’Brien, R. W., Tomoyasu, N., & Pincus, H. A. (2018). Measuring and improving the quality of mental health care: A global perspective. World Psychiatry, 17(1), 30–38.
Kobak, K. A., Wolitzky-Taylor, K., Craske, M. G., & Rose, R. D. (2017). Therapist training on cognitive behavior therapy for anxiety disorders using internet-based technologies. Cognitive Therapy and Research, 41(2), 252–265.
Lilienfeld, S. O., Ritschel, L. A., Lynn, S. J., Cautin, R. L., & Latzman, R. D. (2013). Why many clinical psychologists are resistant to evidence-based practice: Root causes and constructive remedies. Clinical Psychology Review, 33(7), 883–900.
McKay, D., Abramowitz, J. S., & Storch, E. A. (2021). Mechanisms of harmful treatments for obsessive–compulsive disorder. Clinical Psychology: Science and Practice, 28(1), 52–59.
Meyer, J. M., Farrell, N. R., Kemp, J. J., Blakey, S. M., & Deacon, B. J. (2014). Why do clinicians exclude anxious clients from exposure therapy? Behaviour Research and Therapy, 54, 49–53.
Michalski, D., Mulvey, T., & Kohout, J. (2010). 2008 APA survey of psychology health service providers. American Psychological Association.
Nelson, T. D., Steele, R. G., & Mize, J. A. (2006). Practitioner attitudes toward evidence-based practice: Themes and challenges. Administration and Policy in Mental Health and Mental Health Services Research, 33(3), 398–409.
Pagoto, S. L., Spring, B., Coups, E. J., Mulvaney, S., Coutu, M.-F., & Ozakinci, G. (2007). Barriers and facilitators of evidence-based practice perceived by behavioral science health professionals. Journal of Clinical Psychology, 63(7), 695–705.
Pittig, A., Kotter, R., & Hoyer, J. (2019). The struggle of behavioral therapists with exposure: self-reported practicability, negative beliefs, and therapist distress about exposure-based interventions. Behavior Therapy, 50(2), 353–366.
Powell, B. J., McMillen, J. C., Hawley, K. M., & Proctor, E. K. (2013). Mental health clinicians’ motivation to invest in training: results from a practice-based research network survey. Psychiatric Services, 64(8), 816–818.
Raghavan, R., Bright, C. L., & Shadoin, A. L. (2008). Toward a policy ecology of implementation of evidence-based practices in public mental health settings. Implementation Science, 3(1), 26.
Reid, A. M., Bolshakova, M. I., Guzick, A. G., Fernandez, A. G., Striley, C. W., Geffken, G. R., & McNamara, J. P. (2017). Common barriers to the dissemination of exposure therapy for youth with anxiety disorders. Community Mental Health Journal, 53(4), 432–437.
Reid, A. M., Guzick, A. G., Fernandez, A. G., Deacon, B., McNamara, J. P. H., Geffken, G. R., McCarty, R., & Striley, C. W. (2018). Exposure therapy for youth with anxiety: Utilization rates and predictors of implementation in a sample of practicing clinicians from across the United States. Journal of Anxiety Disorders, 58, 8–17.
Reif, S., Torres, M. E., Horgan, C. M., & Merrick, E. L. (2012). Characteristics of practitioners in a private managed behavioral health plan. BMC Health Services Research, 12(1), 283.
Ringle, V. A., Read, K. L., Edmunds, J. M., Brodman, D. M., Kendall, P. C., Barg, F., & Beidas, R. S. (2015). Barriers to and facilitators in the implementation of cognitive-behavioral therapy for youth anxiety in the community. Psychiatric Services, 66(9), 938–945.
Stewart, R. E., Chambless, D. L., & Baron, J. (2012). Theoretical and practical barriers to practitioners’ willingness to seek training in empirically supported treatments. Journal of Clinical Psychology, 68(1), 8–23.
Stewart, R. E., Chambless, D. L., & Stirman, S. W. (2018). Decision making and the use of evidence-based practice: Is the three-legged stool balanced? Practice Innovations, 3(1), 56–67.
Sugarman, D. E., Horvitz, L. E., Greenfield, S. F., & Busch, A. B. (2021). Clinicians’ perceptions of rapid scale-up of telehealth services in outpatient mental health treatment. Telemedicine and e-Health, 27(12), 1399–1408.
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357.
Trivasse, H., Webb, T. L., & Waller, G. (2020). A meta-analysis of the effects of training clinicians in exposure therapy on knowledge, attitudes, intentions, and behavior. Clinical Psychology Review, 80, 101887.
Waller, G., & Turner, H. (2016). Therapist drift redux: Why well-meaning clinicians fail to deliver evidence-based therapy, and how to get back on track. Behaviour Research and Therapy, 77, 129–137.
Weisz, J. R., Sandler, I. N., Durlak, J. A., & Anton, B. S. (2005). Promoting and protecting youth mental health through evidence-based prevention and treatment. American Psychologist, 60(6), 628–648.
Whiteside, S. P., Deacon, B. J., Benito, K., & Stewart, E. (2016). Factors associated with practitioners’ use of exposure therapy for childhood anxiety disorders. Journal of Anxiety Disorders, 40, 29–36.
Wolitzky-Taylor, K., Fenwick, K., Lengnick-Hall, R., Grossman, J., Bearman, S. K., Arch, J., Miranda, J., & Chung, B. (2018). A preliminary exploration of the barriers to delivering (and receiving) exposure-based cognitive behavioral therapy for anxiety disorders in adult community mental health settings. Community Mental Health Journal, 54(7), 899–911.
Woodard, G. S., Triplett, N. S., Frank, H. E., Harrison, J. P., Robinson, S., & Dorsey, S. (2021). The impact of implementation climate on community mental health clinicians’ attitudes toward exposure: An evaluation of the effects of training and consultation. Implementation Research and Practice, 2, 26334895211057884.
Wray, C. M., Khare, M., & Keyhani, S. (2021). Access to care, cost of care, and satisfaction with care among adults with private and public health insurance in the US. JAMA Network Open, 4(6), e2110275.
Funding
This work was supported by funding from the National Institute of Mental Health (T32MH019927) and from the Warren Alpert Medical School of Brown University, Department of Psychiatry and Human Behavior.
Author information
Authors and Affiliations
Contributions
HEF conceived of the study design, conducted interviews with research participants, coded and analyzed the data, drafted sections of the manuscript, and substantially revised the manuscript. LM assisted with data analysis and drafted and substantially revised several sections of the manuscript. KGB and JBF provided input on the study design, assisted with participant recruitment, and provided feedback on the manuscript. ARE provided input on the qualitative methods and interpretation of qualitative data. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interest
The authors have no relevant financial or non-financial interests to disclose.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Lifespan Corporation Institutional Review Board (IRB #1516465).
Informed Participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Milgram, L., Freeman, J.B., Benito, K.G. et al. Clinician-Reported Determinants of Evidence-Based Practice Use in Private Practice Mental Health. J Contemp Psychother 52, 337–346 (2022). https://doi.org/10.1007/s10879-022-09551-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10879-022-09551-w