
Abstract
Chronic granulomatous disease (CGD) is a primary immunodeficiency characterized by life-threatening infections, inflammation, and autoimmunity with an impact on health-related quality of life (HRQoL). Few data are available for children, whereas no study has been conducted in adults. Here, we investigated HRQoL and emotional functioning of 19 children and 28 adults enrolled in Italian registry for CGD. PEDsQL and SDQ were used for children and their caregivers, and adults completed the SF-12 questionnaire. Mean scores were compared with norms and with patients affected by chronic diseases. Comparisons were made for CGD patients who underwent or not hematopoietic stem cell transplantation (HSCT). When compared with norms, CGD children exhibited higher difficulties in social/school areas, peer relationship, and conduct/emotional problems (< 5 years of age), as scored by proxies. Differently, CGD adults reported higher difficulties both in mental and physical area than norms. Only for children, clinical status had a damaging effect on psychosocial and school dimensions, whereas age had a negative impact on social areas. No significant difference was observed between patients treated or not with HSCT. When compared with patients affected by chronic diseases, CGD children and adults both displayed fewer physical disabilities. Differently, in mental scale adults scored lower than those with rheumatology diseases and had similar impairment in comparison with patients with diabetes mellitus and cancer. This study emphasized the impact of CGD on HRQoL since infancy and its decline in adulthood, with emotional difficulties occurring early. HRQoL impairment should be considered in clinical picture of CGD and pro-actively assessed and managed by clinicians.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic granulomatous disease (CGD) is a rare inborn error of innate immunity in which a defect in one of the subunits of NADPH oxidase results in an impaired respiratory burst of phagocytic cells, causing recurrent life-threatening infections, inflammatory complications, and autoimmunity [1,2,3,4,5]. The implementation of routine antimicrobial prophylaxis and the advent of azole antifungals has significantly improved overall survival [6, 7] and reduced the estimated annual infection rate around to 0.3 per year [5, 8]. Hematopoietic stem cell transplantation (HSCT) is at now the only curative treatment for CGD as has achieved in last decade good outcomes with both matched siblings and unrelated donors. However, there is still debate about optimal timing and condition regimen of HSCT [9,10,11,12,13].
Despite improvement in management of CGD, the median age of death remains around III–IV decades of life, and patients still have to cope up with a range of disease-related symptoms for their entire life [3, 5, 8, 14]. Symptoms may be related to the infection itself, often resulting in hospitalization for prolonged courses of treatment, relapse of inflammatory comorbidities, and iatrogenic effects from medications. For this, patients become increasingly debilitated with advancing age, with a negative impact on their health-related quality of life (HRQoL). Moreover, many of the CGD patients may face with cognitive and social problems in peer relationships or school/work activities [15]. Quantifying the HRQoL in primary immunodeficiency (PID) conditions has recently began as an effort to document the patients’ perceived burden of disease, tracking changes in health over time, and assessing the effects of therapeutic intervention [16, 17]. Moreover, HRQoL has been shown to be a reliable predictor of mortalities in primary immunodeficiency [18]. For CGD, few data are available on HRQoL and they were collected only by generic instruments. Recently published data from the UK cohort has documented that children with CGD have poor HRQoL compared with healthy peers [19], whereas, to the best of our knowledge, no data has been provided on adults with CGD.
The aim of our study was to evaluate HRQoL and psychological health in Italian CGD children and adults undergoing both conventional and HSCT. HRQoL status was analyzed with regard to clinical phenotype, familiar background, and treatment. CGD HRQoL status was also compared with normative data and to individuals with other chronic diseases. The underlying hypothesis was that CGD patients have a poor HRQoL and that, in addition to clinical assessment, mental and psychological aspects should be considered because of their contribution to the burden of the disease.
Methods
Population
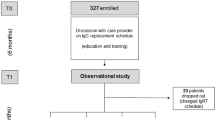
Eligible patients were CGD children and adults regularly followed up in 11 PID centers across Italy with a confirmed diagnosis according to the revised ESID registry criteria (http://www.esid.org/Working-Parties/Registry/Diagnosis-criteria). Participants were identified by the Italian CGD Registry. The registry was established in 2001 by Italian centers belonging to the Italian Association of Pediatric Hematology and Oncology (AIEOP)–Italian network for Primary Immunodeficiencies (IPINET) and it has enrolled 109 patients up to now [5].
Study Design
Participants or their caregivers were recruited during routine clinic appointments. After providing written informed consent, patients or their parents were provided with questionnaires. In CGD who underwent HSCT, questionnaires were administered at least 1-year post-HSCT. Clinical data related to CGD complications and treatments were gathered from medical records. Social status was assessed by individual interview. The clinical status was scored ranging from severe to very good considering the combination of 1) hospitalization in the last 12 months, 2) rate of infections in the last 12 months, and 3) permanent organ damage, as shown in Table 1.
Children were evaluated by the Pediatric Quality of Life Inventory™ version 4.0 (PedsQL) [20] and the Strengths and Difficulties uestionnaire (SDQ) [21]. Adults were evaluated by 12-item Short Form health survey (SF-12) [22]. The study was approved by the ethical committees of all institutions and was conducted in accordance with the provisions of the Declaration of Helsinki.
HRQoL Assessment for Children
The PedsQL is a validated self-report instrument to measure of HRQoL specifically for pediatric populations. It has been validated in Italian and consists of 23 items in four domains: physical, emotional, social, and school functioning [20, 23]. Scores can be combined to provide an overall total score and also a psychosocial score (emotional, social, and school functioning). Age-specific modules of parent report (ages 2–18) and self-report (ages 8–18 years) were used. Following the authors’ instructions, parents of children age < 8 years completed a proxy-report questionnaire and children aged 8–17 completed a self-report questionnaire with the help of their caregivers. Scores were calculated for each of the four dimensions and for the total and psychosocial summary. Maximum score for each domain is 100 with higher score indicating better the HRQoL [20, 23]. Mean scores for patients managed conservatively were compared with published norms for healthy children and for patients living with chronic diseases, including diabetes mellitus type 1 (DMT1), rheumatology diseases (RD), and malignancies [24,25,26]. PEDs scores for post-HSCT and patients managed conservatively were also compared.
The second tool used, the SDQ, is a validated instrument for screening psychopathology in children and adolescents [21]. Age-specific modules of parent report (ages ≤ 4 and ≥ 5) and self-report (ages > 11) were used. The SQD consists of five scales: emotional difficulties, conduct disorders, hyperactivity, peer difficulties, and the prosocial category. A total score is generated for all domains except for the prosocial score. Higher scores indicate more difficulties. For the prosocial domain, the best score possible is 10. Scores recorded for participants managed conservatively and for those who underwent HSCT were compared with published norms for healthy children of UK population [21] due to the lack of published Italian normative data.
HRQoL Assessment for Adults
Adults completed the SF-12, a 12-items questionnaire specifically validated to measure HRQoL in the population over 18 years of age. Scores were calculated for two domains: mental component summary (MCS) and physical component summary (PCS). Each component is scored on a scale from 0 to 100, with higher scores representing better health [27]. Mean scores for CGD participants treated conservatively were compared with published norms for healthy Italian adults (www.istat.it) and with published data on chronic conditions: DMT1, RD, and malignancies [27, 28] (https://www.istat.it/it/files//2017/12/Bes_2017.pdf). Data from CGD adults managed conservatively were also compared with data from CGD adults who underwent HSCT.
Statistical Analysis
Continuous data were described by mean and standard deviation (SD). Categorical data were presented as counts and percentages. Comparisons of continuous parameters between treatment groups were calculated with a t test if normally distributed and with a Mann-Whitney U test if not normally distributed; differences in frequencies between groups were calculated by chi-square exact test. Correlation between continuous variables were computed using Spearman’s rank correlation coefficient. Statistical significance was set at p > 0.05. Data were processed and analyzed using the SPSS version 25.
Results
Patients’ Characteristics
A total of 47 patients (28 adults and 19 children) were enrolled in the study. The sociodemographic characteristics of patients and caregivers included in the analysis are summarized in Table 2. Overall, the mean age was 7.3 ± 4.4 years for pediatric patients and 27.6 ± 8.0 years for adults. X-linked was the most frequently occurring mode of inheritance (83%). The mean age at diagnosis was 1.7 ± 1.7 years for pediatric patients and 7.3 ± 10.6 year for adults (p = 0.028). Clinicians reported a good/very good clinical conditions in 32 (68%), a poor condition in 13 (28%), and a severe condition in two patients (4%). Eight children and three adults underwent HSCT at least 1 year before the enrollment: the mean time post-HSCT was 18.5 ± 6.8 months for adults and 38.0 ± 25.5 months for children. All not-HSCT patients received antimicrobial prophylaxis with antifungal agents. No participants received prophylactic interferon gamma.
HRQoL Assessment in Children
Seventeen proxy and 8 patients reports were completed in CGD pediatric group. Figure 1a describes the result of the comparison between non-HSCT CGD children, healthy controls, and patients affected by chronic diseases for PEDsQoL scores as reported by caregivers. Among the CGD non-HSCT group, proxies reported lowest mean scores in the items related to school functioning (68.3 ± 23.9) and highest mean scores in those related to physical functioning (90.4 ± 5.5). In comparison with healthy peers, children with CGD had higher impairment in social (91.4 ± 14.4 vs 83.0 ± 12.3, p = 0.05) and school functioning (85.5 ± 17.6 vs 68.3 ± 23.9, p = 0.05). When compared with children with chronic diseases, CGD patients had less disabilities (total score) than children with RD, cancer, and DMT1 (83.4 ± 8.7 vs 71.0 ± 18.5, p = 0.0012, 69.7 ± 19.2, p = 0.0006, and 76.6 ± 14.3, p = 0.040, respectively). They also were less affected in the physical (90.4 ± 5.4 vs 66.7 ± 24.1, p < 0.0001; 68.7 ± 25.0, p < 0.0001; 82.3 ± 18.0, p = 0.0012, respectively) and emotional dimensions (85.5 ± 10.5 vs 69.0 ± 21.4, p = 0.0007; 67.5 ± 20.3, p = 0.0004; 68.5 ± 19.3, p = 0.0005, respectively). Similar scores were recorded in social and school areas between CGD and chronic diseases.

Proxy (a) and patient (b) PedsQL scales scores of pediatric patients with CGD. Scores from non-HSCT CGD participants are compared with children with other chronic diseases and the healthy pediatric population. CGD Chronic granulomatous disease, RD rheumatic diseases, DMTI diabetes mellitus type 1. *P ≤ 0.05; **P ≤ 0.01; ****P ≤ 0.001; ****P ≤ 0.0001
In addition, participants ≥ 6 years old were reported to have higher impairment in proxy-PEDsQL total score, psychosocial summary and social functioning dimension in comparison with those aged < 6 years (75.8 ± 11.3 vs 90.2 ± 5.4, p = 0.003, 73.8 ± 10.5 vs 88.6 ± 7.5, p = 0.004, and 77.1 ± 7.6 vs 93.5 ± 10.3, p = 0.003, respectively) (Table S1). Caregivers also described higher impairment in total score, psychosocial summary, and school functioning for children having poor/severe health status in comparison with those with good/very good status (72.9 ± 13.0 vs 87.8 ± 7.6, p = 0.011, 71.2 ± 9.8 vs 86.0 ± 9.7, p = 0.018, and 57.5 ± 29.0 vs 82.5 ± 14.7, p = 0.049, respectively). Mother and father’s education level and occupation did not influence the PEDSsQL scores (Table S1).
Differently from caregivers, patients reported the lowest scores on emotional and school dimensions (73.0 ± 28.4 and 73.0 ± 19.2, respectively) and the highest scores in the social functioning area (76.0 ± 22.7, Fig.1b). Data of self-report scores of CGD children were not informative because of the small sample size of not-HSCT transplanted patients who completed the PEDsQL (Fig. 1b and Table S2).
No significative difference was recorded by proxy- and patient- reported PEDsQL scores in patients who underwent HSCT and those who were managed conservatively. However, for HSCT recipients, we recorded not-significant improvement in total, psychosocial summary, social, and school functioning scores by proxy-reports (Fig. 2a), and in social and school functioning scores by self-reports (Fig. 2b).

Proxy (a) and patient (b) PedsQL scales scores of non-HSCT (white histograms) and post-HSCT children (gray histograms) with CGD. Discontinued lines represent the mean value for normative population
Nineteen children’s parents and three patients > 11 years completed the SDQs. Eight children were post-HSCT (Table 3). As reported by both proxies and patients, children treated conservatively and those who underwent HSCT had significantly higher peer problems scores when compared with population norms. Moreover, non-HSCT and post-HSCT participants aged ≥ 5 years showed higher difficulties in proxy- and self-reported total scores in comparison with age-matched healthy children. No significant difference was observed between patients treated with HSCT and those treated conservatively (data not shown).
HRQoL Assessment in Adult Patients
Overall, patients with CGD showed a decreased well-being, compared with the general Italian population (PCS score 47.8 ± 8.8 vs 53.7 ± 5.9, p < 0.0001; MCS score 45.3 ± 12.5 vs 52.8 ± 7.9, p < 0.0001, Fig. 3a).

SF-12 PCS and MCS scales scores of adults with CGD. Scores from non-HSCT CGD participants are compared with patients with other chronic conditions and the healthy adult Italian population (a). Scores from non-HSCT CGD (white histograms) were compared with post-HSCT CGD adults (gray histograms) (b). CGD Chronic granulomatous disease, RD rheumatic diseases, DMTI diabetes mellitus type 1, PCS physical component summary, MCS mental component summary. *P ≤ 0.05; **P ≤ 0.01; ****P ≤ 0.001; ****P ≤ 0.000
When compared with adults with chronic diseases, PCS scores were higher for non-HSCT CGD than RD, malignancies, and DMT1 (33.4 ± 9.1, p < 0.0001, 40.1 ± 10.0, p = 0.0002, and 40.2 ± 11.9, p = 0.002, respectively). MCS scores were lower in CGD than RD (45.3 ± 12.5 vs 49.9 ± 10.5, p = 0.040) but patients affected by CGD had similar mental impairment (MCS) than those with DMT1 and cancer (Fig.3a). Age, level of education, and working status did not correlate with MCS and PCS scores. Moreover, SF-12 scores did not differ between participants with poor/moderate and good/very good clinical status (Table S3). PCS and MCS scores also did not differ in the non-HSCT and in the post-HSCT group (Fig.3b).
Discussion
In last decades, the overall survival of patients with CGD has significantly improved thanks to prophylactic antimicrobial therapies, early aggressive treatment of infections and the advent of azole antifungals [6, 7], and most of patients now reach adulthood. The aging process of the CGD population poses new challenging problems due to the lifetime recurrence of disease-related symptoms [5, 8, 14]. In the last years, improvements in HSCT techniques for CGD with both matched sibling donors and unrelated donors have led to disease cure [9, 11] and improvement of HRQoL of patients [19]. However, it is still unknown what are the best timing and conditioning HSCT regimen [9, 13]. For these reasons, families often may take the difficult decision to continue on lifelong prophylaxis or to start a curative but potentially life-threatening treatment such as HSCT .
Considering such challenges, it is expected that CGD may affect the psychosocial development of the patient and make the planning of complex support programs necessary. At now, few data are available on HRQoL of children with CGD [15, 19] and to the best of our knowledge no study has been conducted in adults. In a recent series of 63 patients from a single center in the UK, parents and self-reported HRQoL for non-transplanted children with CGD was significantly lower than healthy norms. Emotional difficulties were also reported by proxies in comparison with healthy children [19].
In this multicenter study, we investigated the HRQoL in Italian children and adults followed up in PID care centers belonging to the IPINET group. For children, we used a generic HRQoL instrument, the PEDsQL questionnaire [20, 23] combined with the SDQ, a measure of emotional and behavioral difficulties [21)]. For adults, we used the SF-12 questionnaire, a HRQoL measure including dimensions on physical and mental aspects of well-being [22]. Here we did not confirm the observation from the UK cohort, showing that children with CGD did not show a poorer quality of life than healthy peers, as rated by parents and children themselves. This data was consistent with similar studies on chronic illnesses in children and adolescents, such as chronic kidney diseases [29]. However, in comparison with healthy, all the age brackets of CGD children were shown to be at increased risk of difficulties with peers, potentially exposing patients to psychological problems and emotional difficulties. Differently, adults with CGD showed a decreased well-being when compared with the general population, both in physical than in mental dimensions, possibly due to the incoming comorbidities over the time [5, 8, 14]. Moreover, for children, we observed a better overall parents-reported HRQoL in CGD in comparison with peers living with RD, DMT1, and cancer. Similarly, in adults, we observed less impairment in physical functions in CGD than in RD, malignancies, and DMT1. However, adults with CGD were similarly affected in mental dimension in comparison with those affected by chronic diseases. Children aged ≥ 6 years and those compromised/poor health status had worse overall HRQoL and psychosocial activity, as reported by caregivers. Poor health condition had also a negative impact on the school functioning as scored by parents. Differently, in adults, we did not identify clinical or demographic characteristics with a negative impact on QoL.
HSCT has previously been shown to have a positive impact upon QoL of children with CGD in comparison with those managed conservatively [19]. In this study, we could not confirm this observation neither in pediatric nor in adult cohort, due to the small sample of participants who underwent HSCT for each age range. Another concern is that the time of evaluation post-HSCT was < 24 months for most participants, a time where patients may still be experiencing post procedure complications. Longitudinal studies evaluating HRQoL before and after HSCT treatment are desirable to clarify the role of HSCT in reducing disabilities in CGD.
Also for CGD patients treated conservatively, the main drawback of the study is the small number of subjects enrolled in each age group. However, as reported by Apolone et al., the number of adults enrolled can be considered enough to provide reliable statistics [30].
By definition, HRQoL is the subjective perception of health status concerning physical, psychological, social functioning, and well-being. It is well documented that clinicians’ evaluation of HRQoL does not fit well with ratings made by patients themselves [31, 32]. Actually, in clinical practice, patient-reported outcome measures may be a means of facilitating doctor-patient communication, uncovering patients’ problems, monitoring disease or treatment, and screening for functional problems [16, 33]. For these reasons, their use should be encouraged. Our results highlight the importance to extend the assessment of CGD from simple clinical disease-parameters to patient-reported HRQoL measures. As for other chronic diseases [34, 35], our data can contribute to the debate about how the patients with CGD and their caregivers perceive the burden of disease across different life domains, allowing to improve care strategies and their quality of life.
References
Segal BH, Leto TL, Gallin JI, Malech HL, Holland SM. Genetic, biochemical, and clinical features of chronic granulomatous disease. Medicine (Baltimore). 2000;79:170–200.
Winkelstein JA, Marino MC, Johnston RB, Boyle J, Curnutte J, Gallin JI, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore). 2000;79:155–69.
Jones LB, McGrogan P, Flood TJ, Gennery AR, Morton L, Thrasher A, Goldblatt D, Parker L, Cant AJ Gennery AR, Morton L, Thrasher A, Goldblatt D, Parker L, Cant AJ. Special article: Chronic granulomatous disease in the United Kingdom and Ireland: a comprehensive national patient-based registry. Clin Exp Immunol 2008;152:211–218.
Magnani A, Brosselin P, Beauté J, de Vergnes N, Mouy R, Debré M, et al. Inflammatory manifestations in a single-center cohort of patients with chronic granulomatous disease. J Allergy Clin Immunol. 2014;134:655–62.
Martire B, Rondelli R, Soresina A, Pignata C, Broccoletti T, Finocchi A, et al. Clinical features, long-term follow-up and outcome of a large cohort of patients with chronic granulomatous disease: an Italian multicenter study. Clin Immunol. 2008;126:155–64.
Margolis DM, Melnick DA, Alling DW, Gallin JI. Trimethoprim-sulfamethoxazole prophylaxis in the management of chronic granulomatous disease. J Infect Dis. 1990;162:723–6.
Gallin JI, Alling DW, Malech HL, Wesley R, Koziol D, Marciano B, et al. Itraconazole to prevent fungal infections in chronic granulomatous disease. N Engl J Med. 2003;348:2416–22.
Marciano BE, Spalding C, Fitzgerald A, Mann D, Brown T, Osgood S, et al. Common severe infections in chronic granulomatous disease. Clin Infect Dis. 2015;60:1176–83.
Seger RA, Gungor T, Belohradsky BH, Blanche S, Bordigoni P, Di Bartolomeo P, et al. Treatment of chronic granulomatous disease with myeloablative conditioning and an unmodified hemopoietic allograft: a survey of the European experience, 1985-2000. Blood. 2002;100:4344–50.
Martinez CA, Shah S, Shearer WT, Rosenblatt HM, Paul ME, Chinen J, et al. Excellent survival after sibling or unrelated donor stem cell transplantation for chronic granulomatous disease. J Allergy Clin Immunol. 2012;129:176–83.
Soncini E, Slatter MA, Jones LB, Hughes S, Hodges S, Flood TJ, et al. Unrelated donor and HLA-identical sibling haematopoietic stem cell transplantation cure chronic granulomatous disease with good long-term outcome and growth. Br J Haematol. 2009;145:73–83.
Cole T, Pearce MS, Cant AJ, Cale CM, Goldblatt D, Gennery AR. Clinical outcome in children with chronic granulomatous disease managed conservatively or with hematopoietic stem cell transplantation. J Allergy Clin Immunol. 2013;132:1150–5.
Horwitz ME, Barrett AJ, Brown MR, Carter CS, Childs R, Gallin JI, et al. Treatment of chronic granulomatous disease with nonmyeloablative conditioning and a T-cell-depleted hematopoietic allograft. N Engl J Med. 2001;344:881–8.
van den Berg JM, van Koppen E, Ahlin A, Belohradsky BH, Bernatowska E, Corbeel L, et al. Chronic granulomatous disease: the European experience. PLoS One. 2009;4:e5234.
Cole TS, Jones LK, McGrogan P, Pearce MS, Flood TJ, Cant AJ, et al. Emotional and behavioural difficulties in chronic granulomatous disease. Arch Dis Child. 2012;97:87.
Jiang F, Torgerson TR, Ayars AG. Health-related quality of life in patients with primary immunodeficiency disease. Allergy Asthma Clin Immunol. 2015;29:11–27.
Peshko D, Kulbachinskaya E, Korsunskiy I, Kondrikova E, Pulvirenti F, Quinti I, et al. Health-related quality of life in children and adults with primary Immunodeficiencies: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2019;7:1929–57.
Tabolli S, Giannantoni P, Pulvirenti F, La Marra F, Granata G, Milito C, et al. Longitudinal study on health-related quality of life in a cohort of 96 patients with common variable immune deficiencies. Front Immunol. 2014;26(5):605.
Cole T, McKendrick F, Titman P, Cant AJ, Pearce MS, Cale CM, et al. Health related quality of life and emotional health in children with chronic granulomatous disease: a comparison of those managed conservatively with those that have undergone haematopoietic stem cell transplant. J Clin Immunol. 2013;33:8–13.
Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39:800–12.
Youth in mind. SDQ: Normative SDQ Data from Britain. http://www.sdqinfo.org/UKNorm.html. Accessed 02/08/2019.
Ware JE Jr, Kosinski M, Turner-Bowker DM, Gandek B. How to score version 2 of the SF-12 health survey (with a supplement documenting version 1). QualityMetric Inc: Lincoln; 2002.
Trapanotto M, Giorgino D, Zulian F, Benini F, Varni JW. The Italian version of the PedsQL in children with rheumatic diseases. Clin Exp Rheumatol. 2009;27:373–80.
Varni J, Burwinkle TM, Jacobs JR, Gottschalk M, Kaufman F, Jones KL. The PedsQLTM in type 1 and type 2 diabetes reliability and validity of the Pediatric Quality of Life InventoryTM generic core scales and type 1 diabetes module. Diabetes Care. 2003;26:631–7.
Varni JW, Seid M, Smith-Knight T, Burwinkle T, Brown J, Szer IS. The PedsQL in pediatric rheumatology. Reliability, validity and responsiveness of the Pediatric Quality of Life Inventory generic core scale and rheumatology module. Arthritis Rheum. 2002;46:714–25.
Varni JM, Burwinkle TM, Katz ER, Meeske K, Dickinson P. The PedsQL™ in pediatric cancer reliability and validity of the Pediatric Quality of Life Inventory™ generic core scales, multidimensional fatigue scale, and cancer module. Am Cancer Soc. 2002;94:2090–106.
Gandhi SK, Salmon JW, Zhao SZ, Lambert BL, Gore PR, Conrad K. Psychometric evaluation of the 12-item short-form health survey (SF-12) in osteoarthritis and rheumatoid arthritis. Clin Ther. 2001;23(7):1080–98.
Vyas A, Babcock Z, Kogut S. Impact of depression treatment on health-related quality of life among adults with cancer and depression: a population-level analysis. J Cancer Surviv. 2017;11:624–33.
Heath J, Mackinlay D, Watson AR, Hames A, Wirz L, Scott S, et al. Self-reported quality of life in children and young people with chronic kidney disease. Pediatr Nephrol. 2011;26:767–73.
Apolone G, Mosconi P, Quattrociocchi L, Gianicolo E, Groth N and Ware JE. Questionario sullo stato di salute SF-12. Versione italiana. Guerini e Associati Edition, 2005.
Drinkwater J, Gregory WM. Who should measure quality of life, the doctor or the patient? J Cancer. 1988;57:109–12.
Quinti I, Pulvirenti F, Giannantoni P, Hajjar J, Canter DL, Milito C, et al. Development and initial validation of a questionnaire to measure health-related quality of life of adults with common variable immune deficiency: the CVID_QoL questionnaire. J Allergy Clin Immunol Pract. 2016;4:1169–79.
Quinti I, Pulvirenti F. Health-related quality of life and patients’ empowerment in the health care of primary immune deficiencies. J Clin Immunol. 2017;37:615–6.
Jackson DS, Banerjee S, Sirey JA, Pollari C, Solomonov N, Novitch R, et al. Two interventions for patients with major depression and severe chronic obstructive pulmonary disease: impact on quality of life. Am J Geriatr Psychiatry. 2019;27:502–11.
Brandt Å, Pilegaard MS, Oestergaard LG, Lindahl-Jacobsen L, Sørensen J, Johnsen AT, et al. Effectiveness of the “Cancer Home-Life Intervention” on everyday activities and quality of life in people with advanced cancer living at home: a randomised controlled trial and an economic evaluation. BMC Palliat Care.2016;15:10.
Acknowledgments
We are grateful to the patients and families for their generous cooperation. We would like to thank Dr. Stefano Tabolli for his kind comments and suggestions.
Author information
Authors and Affiliations
Contributions
BM, FP, and MS conceived and designed the study design; AP, AS, AF, CP, EC, AT, AA, MM, FL, AB, SN, MC, MDC, MGF, MG, and BM collected the data; FP, BM, and MS perform data analysis and interpretation, FP, BM, IQ, and MS manuscript preparation, all the authors revised the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 27 kb)
Rights and permissions
About this article

Cite this article
Pulvirenti, F., Sangerardi, M., Plebani, A. et al. Health-Related Quality of Life and Emotional Difficulties in Chronic Granulomatous Disease: Data on Adult and Pediatric Patients from Italian Network for Primary Immunodeficiency (IPINet). J Clin Immunol 40, 289–298 (2020). https://doi.org/10.1007/s10875-019-00725-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-019-00725-1