
Abstract
Osteoinductive capacity of demineralized bone matrix (DBM) is sometimes insufficient or shows high variability between different batches of DBM. Here, we tried to improve its osteoinductive activity by alkali-urea or trypsin treatment but this strategy was unsuccessful. Then, we tested the enrichment of DBM with a bone protein extract (BPE) containing osteogenic growth factors comparing two sources: cortical bone powder and DBM. The osteoinductive capacity (alkaline phosphatase activity) of the obtained BPEs was evaluated in vitro in C2C12 cells. Specific protein levels present in the different BPE was determined by enzyme-linked immunosorbent assay or by a multiplex assay. BPE from cortical bone powder showed a lack of osteoinductive effect, in agreement with the low content on osteoinductive factors. In contrast, BPE from DBM showed osteoinductive activity but also high variability among donors. Thus, we decided to enrich DBM with BPE obtained from a pool of DBM from different donors. Following this strategy, we achieved increased osteoinductive activity and lower variability among donors. In conclusion, the use of a BPE obtained from a pool of demineralized bone to enrich DBM could be used to increase its osteoinductive effect and normalize the differences between donors.

Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Demineralized bone matrix (DBM) is an osteoinductive allograft that constitutes an attractive alternative to autologous bone. Obtained by decalcification of cadaveric cortical bone, DBM lacks the structural strength but retains the trabecular structure of the original tissue. It has been estimated that 93% of DBM consists of an osteoconductive collagen scaffold, while the remainder of its components are soluble osteoinductive proteins, with residual mineralized matrix accounting for the additional 2% [1]. By removing the mineral phase of bone, the osteoinductive proteins are made more bioavailable; and indeed, DBM shows more osteoinductive potential than standard mineralized allografts [2].
As stated before, the osteoinductive nature of DBM is attributed to the presence of matrix associated growth factors [3], being the bone morphogenetic proteins (BMPs) the best characterized [4]. BMPs belong to the transforming growth factor beta (TGF-β) superfamily, with BMP-2, BMP-4 and BMP-7 believed to be the most osteoinductive [5]. In addition to BMP, bone matrix contains other factors that are able to modulate the DBM osteoinductive activity, among them TGF-b1, insulin like growth factor-I (IGF-I), vascular endothelial growth factor (VEGF) and platelet derived growth factor (PDGF) [6], although the total protein composition present in DBM and responsible of its activity is still unknown.
The growth factors concentrations may vary in relation with donor, extraction techniques and processing [7], and it is thought that such variability might explain the variable results found on the osteoinductive potency of DBM [8], leading to a low level of evidence of the clinical efficiency of DBM [9].
In the present work we evaluated different strategies for improving DBM effect, first we tested different extraction strategies in order to eliminate possible inhibitors of native BMPs; another strategy was to enrich DBM with a bone protein extract (BPE) either from cortical bone or from DBM. Our hypothesis is that the addition to the DBM of a mixture of multiple growth factors at physiological doses would enhance its osteoinductive activity while at the same time decrease variability.
2 Materials and methods
2.1 Preparation of cortical powder
The fragments of bone used in this study (cortical rings from femoral diaphysis) were obtained from the fragments usually discarded for clinical use during the processing of bone tissue from conventional musculoskeletal tissue donations. The femur epiphysis were used to obtain cancellous bone and the diaphysis was denuded of soft tissue, cut into bone rings and milled in a M20 universal mill (IKA®-Werke GMBH and Co., Staufen, Germany) to powder. The powder was mechanically sieved to a particle size within the range 250–800 µm by using BA 200N electromagnetic and digital sieve shaker with appropriately certified test sieves (CISA, Barcelona, Spain). Then, cortical bone powder was washed and defatted through sequential washes with milliQ water (Millipore Corporation, Billerica, MA, USA) at 60 °C, 70% ethanol (Sigma-Aldrich, St. Louis, MO, USA) and absolute ethanol (Sigma-Aldrich), and allowed to dry at room temperature. All the process was developed inside a laminar flow cabinet in sterile conditions.
In both the process of selection as well as in the procurement and processing the Standards of the Spanish Association of Tissue Banks were followed. The samples were used, with the approval of the Ethical Committee of Balearic Islands (CEIC-IB), after an informed consent.
2.2 Obtention of DBM
Cortical powder, previously extracted with PBS or Guanidine solution (see next section) was demineralized through three incubations of 1 h with 0.5 N HCl (Sigma-Aldrich). Then, demineralized bone particles were washed with milliQ water (Millipore Corporation, Billerica, MA, USA) until reaching a neutral pH. Finally, DBM samples were frozen −80 °C for 48 h, lyophilized for 48 h and stored at −80 °C until use.
Two different DBM groups were obtained (Fig. 1) according to the extraction buffer that was applied to the cortical powder used for demineralization: DBMPBS and DBMGu.

Diagram of the experimental design followed to obtain the different BPE and DBM samples. c-BPEPBS: Bone protein extract obtained by extraction of cortical powder with phosphate buffer saline (PBS). c-BPEGu: bone protein extract obtained by extraction of cortical powder with Guanidine extraction solution (Gu). DBMGu: DBM obtained from cortical powder that has previously been extracted with Gu. DBMPBS: DBM obtained from cortical powder that has previously been extracted with PBS. d-BPEPBS: bone protein extract obtained by extraction of DBMPBS with Gu. d-BPEGu: bone protein extract obtained by extraction of DBMGu with Gu
2.3 Obtention of BPEs
BPE were first obtained from cortical powder using two different extracting solutions: PBS or a Guanidine solution (Gu) (4 M Guanidin-HCl (Sigma-Aldrich), 50 mM Tris-HCl (Sigma-Aldrich), 10 mM EDTA (Sigma-Aldrich) at a pH = 6.9), by mixing 300 mg of cortical bone with 5 mL of extracting solution. The mixtures were maintained under rotative agitation for 24 h at 4 °C, then, samples were centrifuged at 12,000 × g, at 4 °C for 30 min. Then, the supernatants were dialyzed against milliQ water through a dialysis tubing (3000 Da molecular weight cutoff) (Sigma-Aldrich), frozen at −80 °C, lyophilized for 48 h, and stored at −80 °C until use.
The cortical powder thus extracted was next demineralized as described in previous section and again extracted in this case with Guanidine solution.
All the process is depicted in Fig. 1, were can be observed that 4 different BPE were obtained depending on the starting material (cortical bone (c) or DBM (d)) and on the extracting solution (Gu or PBS): c-BPEPBS, c-BPEGu, d-BPEPBS and d-BPEGu.
2.4 Alkali urea extraction of DBM
DBM was subjected to a process of alkali-urea extraction [10]. In short, 500 mg DBM was extracted with 3 ml of a solution that had been prepared by adding equal volumes of 6 M urea and 0.1 M KOH. The pH of the solution was adjusted to 10.5 with 1 M KOH and corrected at 0.5, 1, and 4 h but not subsequently. The following day the supernatant was removed by decanting and the remaining solid material was then washed with a large volume of water and stored frozen at −80 °C until use.
2.5 DBM treatment with trypsin
An enzymatic protocol previously described was applied [11]. Briefly, lyophilized DBM was rinsed with distilled water and incubated in a solution of 0.05% trypsin (Sigma–Aldrich) and 0.02% ethylenediamine tetraacetic acid (EDTA) (Sigma–Aldrich) at 37 °C under continuous agitation for 24 h. The resultant material was rinsed in PBS and stored frozen at −80 °C until use.
2.6 Cell culture
The mouse myoblast cell line C2C12 was purchased from DSMZ GmbH (Braunschweig, Germany). Cells were cultured at 37 °C/5% CO2, and maintained in RPMI (Biowest, Nuaillé, France) supplemented with 10% fetal bovine serum (FBS, PAA Laboratories GmbH, Pasching, Austria), penicillin (100 U/mL) and streptomycin (100 µg/mL) (Biowest).
For the in vitro osteoinduction tests, C2C12 cells were seeded in 24-well plates at a density of 5 × 104 cell/well. At confluence, cells were subjected to a serum reduction (1%) and were treated with the different amounts of BPE (0.01, 0.1, 1, 10, 100 µg), DBM samples (5 mg), or a combination of BPE (1 µg) with 5 mg of DBM per well. After 48 h of treatment culture media were collected to test cytotoxicity and cells were harvested to analyze the alkaline phosphatase (ALP) activity.
When a mixture of DBM and BPE was used to treat cells, 100 µL containing the desired amount of BPE total protein were added to 5 mg of DBM and the mixture was lyophilized for 48 h and stored at −80 °C until use.
An in vivo validated DBM sample used clinically (DBM Putty, Barcelona Tissue Bank, Banc de Sang I Teixits, Barcelona, Spain) was used as control DBM.
2.7 LDH activity
Lactate dehydrogenase (LDH) activity in the culture media 48 h after treatment was used as an index of cell death. The LDH activity was estimated according to the manufacturer’s kit instructions (Roche Diagnostics, Mannheim, Germany) by assessing the rate of oxidation of NADH at 490 nm in presence of piruvate. Results were presented relative to the LDH activity in the media of cells without treatment (negative control, 0% of cell death) and of cells treated with 1% Triton X-100 (positive control, 100% cell death). The percentage of LDH activity was calculated using the following equation: cytotoxicity (%) = (exp. value – negative control)/ (positive control – negative control) × 100.
2.8 ALP activity
Cell monolayers were collected in order to determine ALP activity. Proteins were solubilized by adding PBS containing 0.1% Triton X-100. Then, cell lysates were put into freeze/thaw cycles to improve protein recovery. After centrifugation at 33,000 × g for 15 min at 4 °C, supernatants were acquired and assayed for ALP activity. The method used measures the cleavage of p-nitrophenyl phosphate (pNPP; Sigma-Aldrich) in a soluble yellow end product which absorbs at 405 nm. A volume of 100 µL of this substrate was used in combination with 25 µL of each sample supernatant or standard point. The standard curve was prepared from calf intestinal alkaline phosphatase (CIAP, 1 U/µL) (Promega, Madison, WI, USA) by mixing 1 µL from the stock CIAP with 5 ml of PBS containing 0.1% Triton X-100 (1:5000 dilution), and then making a dilution series. Once the reaction was carried out, after 2 h in dark at 37 °C, absorbance was read at 405 nm.
2.9 Bone morphogenetic protein-2 quantification
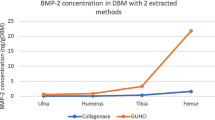
The bone morphogenetic protein-2 (BMP-2) levels in the different BPE were quantified using an enzyme-linked immunosorbent assay following instructions described by the manufacturer (Quantikine Immunoassay, R&D Systems, Minneapolis, MN, USA). Total protein was determined using a BCA protein assay kit (Pierce, Rockford, IL, USA) and used for correction of BMP-2 levels, expressed in ng BMP-2/g protein.
2.10 Growth factor analysis
BPE were analysed for fibroblast growth factor 2 (FGF-2), matrix metalloproteinase 2 (MMP-2), osteopontin (OPN), hepatocyte growth factor (HGF), PDGF-BB, stem cell factor (SCF), TGF-B and VEGF-A using the solid phase sandwich multiplex bead immunoassays (ProcartaPlexTM Multiplex Immunoassays, Affimetris, eBioscience, San Diego, CA, USA) according to the manufacturer’s protocol. Multianalyte profiling was performed on the Luminex® MAGPIX xPONENT 4.2 (Luminex Corporation, Austin, TX, USA). Specific protein levels were corrected by total protein, expressed in pg/mg protein.
2.11 Statistical analysis
All data are presented as mean values ± standard error of the mean (SEM). The Kolmogorov-Smirnov test was done to assume parametric or non-parametric distributions. Differences between groups were assessed by one-way ANOVA test using Bonferroni or Dunnett’s multiple comparison tests as post hoc comparisons was used when more than two experimental groups were compared; when two groups were compared, differences between groups were assessed by Student t-test or by paired-t-test. The SPSS® program for Windows, version 17.0 (SPSS, Chicago, IL, US) was used. Results were considered statistically significant at the p-values < 0.05.
3 Results
3.1 Comparison of the osteoinductive in vitro effect of produced DBM with a certified control DBM
First, we compared the osteoinductive in vitro effect of DBM obtained from 7 different donors with those of a control DBM already certified with an osteoinductive in vivo assay. As shown in Fig. 2, our obtained DBM induced ALP activity in a similar manner or even more than the control DBM. It was also evidenced the high variability of the in vitro osteoinductive effect of the DBM between the different donors.

Comparison of osteoinductive in vitro effect of produced DBM with a certified control DBM. ALP activity induced by DBM obtained from different donors with reference to that of a control DBM (dashed line). Values represent the mean ± SEM
3.2 Effect of different pre-treatments on the derived DBM osteoinductive activity
The presence in DBM of inhibitors of native BMP, like noggin, that could be eliminated by extracting the DBM with an alkali-urea solution has previously been described [10]. We considered plausible that the individual differences in the osteoinductive activity of BMP preparations obtained from different donors could be due to the presence of some of such inhibitors at different levels in the different donors. In addition, it has also been described [11] that the treatment of DBM with trypsin increases the proliferation of osteogenic cell populations. Following this idea, we were interested in testing whether the trypsin treatment could increase the osteogenic activity of DBM, leading to a more homogeneous product. However, as shown in Fig. 3 and contrary to our hypothesis, neither an alkali-urea extraction nor trypsin digestion resulted in an increase of the osteoinductive effect of the resulting DBM.

Evaluation of ALP activity in C2C12 cells incubated for 48 h with DBM obtained from cortical powder that has previously been treated with trypsin or with urea. ALP activity in C2C12 cells incubated with different types of DBM. The experiment was performed in triplicate using four different DBM donors. Values represent the mean ± SEM. Results were statistically compared by ANOVA, and Bonferroni as post hoc test: *p < 0.05 vs. inactive DBM
3.3 Osteoinductive effect of BPE obtained from different sources
Having been unable to obtain an increase of the osteogenic effect of DBM samples by direct manipulation, we reasoned that another approach to obtain a homogeneous product could be the enrichment of DBM with a BPE containing osteogenic growth factors. Although it has been widely described that the main osteogenic activity is present in the BPE obtained from demineralised bone, it has also been reported [12] that the extract of mineralized bone shows a certain osteoinductive capacity. Thus, we obtained different BPE from both mineralized and demineralised cortical bone as described in Material and Methods and depicted in Fig. 1.
We tested the capacity of the different BPE obtained to induce ALP activity in C2C12 cells. Although some osteoinductive effect could be observed when cortical bone powder extract (c-BPEGu) was added to the culture, the results were not consistent and did not reach significance (data not shown). It should be noted that the c-BPEPBS group could not be tested since no detectable amounts of protein were obtained. In contrast, when different BPE obtained from demineralized bone (d-BPEPBS, d-BPEGu), were tested individually, a different level of osteogenic activity in the samples was observed, as shown in Fig. 4, in accordance with the heterogeneity described with the DBM preparations.

Evaluation of ALP activity in C2C12 cells incubated for 48 h with different BPE. ALP activity in C2C12 cells incubated with 1 µg of d-BPEPBS or d-BPEGu. Three different donors were used. The experiment was performed in sextuplicate. Data present mean ± SEM for each group. Results were statistically compared by ANOVA, no significant differences were found
3.4 Analysis of the presence of osteoinductive factors in the different BPE preparations
In order to better characterize these data, we decided to measure the specific protein levels of several growth factors present in the different BPE. As can be observed in Fig. 5a, two different patterns of protein content among the different groups were observed. Those growth factors that were in a greater extent extracted from DBM (BMP-2, PDGF-BB, TGF-B, MMP-2, OPN, SCF) and those mainly extracted from cortical powder (VEGF-A, HGF and FGF-2). It is important to notice that both, c-BPEPBS and c-BPEGu had to be concentrated in order to allow determinations; moreover, BMP-2 levels were about 10-fold lower in BPE from cortical bone compared to those obtained from DBM and that osteoinductive proteins were present in higher amounts in BPE obtained from DBM. Moreover, when the concentration of the different factors was analyzed individually in the d-BPEPBS a clear pattern of heterogeneity was evident (Fig. 5b); for instance, the levels of BMP2 showed a variability of ten-fold and other growth factors were present in some BPE and absent in others. For that reason, and given the high variability in such protein levels among the different donors and in order to obtain a more homogeneous product, we decided use a pool of BPE from different donors to enrich the osteoinductivity of DBM.

Specific protein levels detected in the different BPE. (a) Proteins levels in BPE represented in a heat map. Cell colors display the relative amount of protein per row, being red the maximum and blue the minimum. Values present mean ± SEM. Results were statistically compared by ANOVA, and student t-test as post hoc test: *p < 0.05 vs. c-BPEPBS; # p < 0.05 vs. c-BPEGu. (b) Specific protein levels detected in d-BPEPBS evaluated in six different donors. The determination was performed in duplicate, means are presented. Those proteins with very low levels are not shown
3.5 BPE-enriched DBM cytotoxicity and osteoinductive activity on C2C12 cells
For the evaluation of the effect of BPE-enriched DBM using a BPE obtained from a pool of different donors, we first tested the enrichment of DBM with different amounts of BPE. DBM enriched with d-BPEPBS induced higher cytotoxicity than controls (Fig. 6a), although values were <3%. Increased ALP activity of C2C12 cells was found in the BPE-enriched DBM groups compared to DBM alone in a concentration dependent manner (Fig. 6b). So, our results demonstrated that 5 mg of DBM enriched with 1 µg of d-BPEPBS obtained from a pool of different donors per well enhanced osteoinductive activity compared with using DBM alone.

Evaluation of LDH activity and ALP activity in C2C12 cells incubated for 48 h with DBM supplemented with d-BPEPBS. (a) LDH activity and b ALP activity in C2C12 cells incubated with DBM supplemented with different amounts of d-BPEPBS. Inactive DBM was used as a negative control. One DBM donor was used and d-BPEPBS was obtained from a pool of different donors. The experiment was performed in sextuplicate. Results were statistically compared by ANOVA, and Bonferroni as post hoc test: *p < 0.05 vs. inactive DBM, #p < 0.05 vs. DBMPBS without d-BPEPBS addition. (c) ALP activity in C2C12 cells incubated with DBM supplemented with 1 µg of BPE. Six different donors were evaluated and the experiment was performed in triplicate. Both data from each donor and means ± SEM for each group are presented. Results were statistically compared by paired t test (*p < 0.05)
Next, we confirmed our findings using different DBM donors (Fig. 6c), our results showed that this strategy significantly induced ALP activity compared to DBM alone. In addition, variability among donors was decreased from a coefficient of variation of 40.3% for DBM alone to a 13.7% for the BPE-enriched DBM group.
4 Discussion
We found that enrichment of DBM with a BPE obtained from a pull of different DBMs enhances its osteoinductive activity and decreases variability among donors. Variability is considered the most important disadvantage to the use of DBM, since there is considerable inconsistency in terms of osteoinductive potency as a result of donor and processing variability [6, 8, 14,15,16]. In fact, we also found donor-dependentAvailable clinical studies show a low level of evidence con differences in the osteoinductive activity induced by our DBM in the seven donors that were evaluated. cerning DBM efficiency [9], having been proposed that a variable amount of growth factors in the used DBM product might explain this variable results [8]. Despite this, many surgeons prefer using DBM, as this product improve facilitation of new bone formation and avoid the main problems of the “gold standard” autogenous cancellous bone, such as limited availability and high morbidity and morbility during the harvest [13,14,15,16].
One strategy to enhance DBM osteoinductivity that has been explored is the addition of recombinant BMP-2 to DBM [17, 18]. However, some safety concerns to the use of recombinant BMP-2 have been raised [19, 20]. We then hypothesized that the use of a DBM BPE would add to the DBM a mixture of multiple growth factors at physiological doses and enhance its osteoinductive activity while at the same time decrease variability. It has been shown that very high doses of the recombinant BMPs are needed to achieve the same osteoinduction levels obtained by the natural cocktail of BMPs and associated growth factors found in the DBM. This finding is supported by the observation that a better osteoinduction is obtained by the heterodimers BMPs (natural BMPs) compared to homodimers like they are in the recombinant BMPs [21,22,23], hence, making our strategy of using a natural cocktail of growth factors ideal. However, the resultant DBM after the BPE extraction process lacks any osteoinductive activity [12], thus in the present study we evaluated the possibility of using a BPE from cortical powder extracted prior to demineralization in combination with the DBM obtained from the same extracted cortical powder. Unfortunately, no positive results were found when testing this strategy, since a poor osteoinductive effect was observed when using BPE obtained from cortical bone powder, contrary to the positive effect found for d-BPE.
To understand the results obtained, the levels of different growth factors present in the different BPE were evaluated. Of importance is to highlight that the amount of protein extracted from bone cortical powder was far less than the amount extracted from DBM, and to be able to measure specific proteins from bone cortical powder, samples were concentrated by lyophilization. These results can be explained by the fact that the demineralization process of DBM results in exposure of the osteoinductive noncollagenous proteins, making them more available to the surrounding tissues [2] and to the extracting reagent, as shown by our results.
The higher levels of FGF-2, HGF and VEGF-A in the extracts from cortical powder suggest that these proteins are associated to the mineral component of bone, being mainly eliminated during the demineralization step during DBM procurement. In agreement with our observations, it has been suggested that FGF-2 and HGF adsorbs to hydroxyapatite surfaces in a selective and irreversible manner [24, 25]. Both, FGF-2, HGF and VEGF are potent angiogenesis inducers [26, 27], which is of particular importance in bone tissue regeneration.
The factors that were mainly extracted from DBM account for those that are osteoinductive and are related to bone formation. Among them, BMP-2 is one of the most abundant growth factor that we and others [6] detected, the most extensively studied growth factor regarding induction of new bone formation [28], and thought to be the main responsible for the osteoinductive effect of DBM [2, 3, 8, 29,30,31]. At molecular level, BMP-2 regulates transcription of osteogenic genes inducing differentiation of progenitor cells into the osteoblast lineage [32]. In strong connection with BMP signaling in osteoblast differentiation also acts TGF-B [33, 34], another of the growth factors that was mainly extracted from DBM yielding levels within the same range of those previously reported [31]. Other proteins found in high amounts in the BPE from DBM in our study and by others [35] are OPN, a bone matrix protein synthesized by osteoblastic cells that regulates crystal growth [36, 37] and MMP-2, a metalloendopeptidase that degrades proteins of the extracellular matrix that has been proposed to help during new bone formation by facilitating angiogenesis, growth factor release and mesenchymal stem cell recruitment [38].
We want to highlight that the only use of the extracted BPE does not achieve the same osteoinduction levels as it does when combined with DBM, pointing at the importance of osteoconductivity for the effect of DBM. Nonetheless, the ostoconductivity effect of DBM alone is not sufficient for osteoinduction, as shown when using DBM after BPE extraction (inactive DBM). Since we did not measure the osteoinductive activity effect of inactive DBM combined with the BPE pull, nor combined with recombinant BMP-2, it is not possible to claim whether our strategy using a mixture of multiple growth factors at physiological doses would give better results than using recombinant BMP-2 in combination with DBM as an osteoconductive scaffold. In fact, we have only tested the mixture of growth factors resulting from cortical bone powder or from DBM, and showed that the protein composition among extracts differs, thus suggesting that a mixture of both extracts should also be tested as a potential osteoinductive cocktail.
There are some limitations to the current study. Only in vitro experiments were performed to support our results, however, the in vitro assay that we have used has previously been shown to correlate with the in vivo assay in assessing the osteoinductive potential of DBM [39]. In addition, pooling BPEs from different donors might not be acceptable for clinical use as regards to biovigilance and traceability [40], as it has been proposed previously [7]. One possible way to proceed is to use different vials from different donors combining in each DBM and d-BPE from the same donor.
In conclusion, the enrichment of DBM with a BPE from the same donor does not enhance the osteoinductive activity of DBM, neither when the extract is obtained from cortical bone nor from DBM. In contrast, enrichment of DBM with a bone protein extract obtained from a pull of different DBMs enhances its osteoinductive activity and decreases variability among donors.
References
Ajiboye R, Eckardt M, Hamamoto J, Plotkin B, Daubs M, Wang J. Outcomes of demineralized bone matrix enriched with concentrated bone marrow aspirate in lumbar fusion. Int J Spine Surg. 2016;10:35.
Dinopoulos H, Giannoudis P. Safety and efficacy of use of demineralised bone matrix in orthopaedic and trauma surgery. Expert Opin Drug Saf. 2006;5:847–66.
Shigeyama Y, D’Errico Ja, Stone R, Somerman MJ, Shigeyama Y, D’Errico J, Stone R, et al. Commercially prepared allograft material has biological activity in vitro. J Periodontol. 1995;66:478–87.
Urist MR. Bone: formation by autoinduction. Science. 1965;150:893–9.
Blum B, Moseley J, Miller L, Richelsoph K, Haggard W. Measurement of bone morphogenetic proteins and other growth factors in demineralized bone matrix. Orthopedics. 2004;27:s161–5.
Wildemann B, Kadow-Romacker a, Pruss a, Haas NP, Schmidmaier G. Quantification of growth factors in allogenic bone grafts extracted with three different methods. Cell Tissue Bank. 2007;8:107–14.
Hinsenkamp M, Collard J-F. Growth factors in orthopaedic surgery: demineralized bone matrix versus recombinant bone morphogenetic proteins. Int Orthop. 2015;39:137–47.
Bae H, Zhao L, Zhu D, Kanim LE, Wang JC, Delamarter RB. Variability across ten production lots of a single demineralized bone matrix product. J Bone Jt Surg Am. 2010;92:427–35.
Drosos GI, Touzopoulos P, Ververidis A, Tilkeridis K, Kazakos K. Use of demineralized bone matrix in the extremities. World J Orthop. 2015;6:269–77.
Behnam K, Brochmann EJ, Murray SS. Alkali-urea extraction of demineralized bone matrix removes noggin, an inhibitor of bone morphogenetic proteins. Connect Tissue Res. 2004;45:257–60.
Sawkins MJ, Bowen W, Dhadda P, Markides H, Sidney LE, Taylor AJ, et al. Hydrogels derived from demineralized and decellularized bone extracellular matrix. Acta Biomater. 2013;9:7865–73.
Sampath TK, Reddi aH. Distribution of bone inductive proteins in mineralized and demineralized extracellular matrix. Biochem Biophys Res Commun. 1984;119:949–54.
Traianedes K, Russell JL, Edwards JT, Stubbs HA, Shanahan IR, Knaack D. Donor age and gender effects on osteoinductivity of demineralized bone matrix. J Biomed Mater Res B Appl Biomater. 2004;70:21–9.
Schwartz Z, Somers a, Mellonig JT, Carnes DL, Dean DD, Cochran DL, et al. Ability of commercial demineralized freeze-dried bone allograft to induce new bone formation is dependent on donor age but not gender. J Periodontol. 1998;69:470–8.
Lohmann CH, Andreacchio D, Köster G, Carnes DL, Cochran DL, Dean DD, et al. Tissue response and osteoinduction of human bone grafts in vivo. Arch Orthop Trauma Surg. 2001;121:583–90.
Bormann N, Pruss A, Schmidmaier G, Wildemann B. In vitro testing of the osteoinductive potential of different bony allograft preparations. Arch Orthop Trauma Surg. 2010;130:143–9.
Jang YS, Choi CH, Cho YB. Recombinant human BMP-2 enhances osteogenesis of demineralized bone matrix in experimental mastoid obliteration. Acta Otolaryngol. 2014;134:785–90.
Huber E, Pobloth A-M, Bormann N, Kolarczik N, Schmidt-Bleek K, Schell H, et al. Demineralized bone matrix as a carrier for bone morphogenetic protein-2: burst release combined with long-term binding and osteoinductive activity evaluated in vitro and in vivo. Tissue Eng Part A. 2017;23:1321–30.
Tannoury CA, An HS. Complications with the use of bone morphogenetic protein 2 (BMP-2) in spine surgery. Spine J Elsevier Inc. 2014;14:552–9.
Carragee EJ, Hurwitz EL, Weiner BK. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: Emerging safety concerns and lessons learned. Spine J Elsevier Inc. 2011;11:471–91.
Valera E, Isaacs MJ, Kawakami Y, Belmonte JCI, Choe S. BMP-2/6 heterodimer is more effective than BMP-2 or BMP-6 homodimers as inductor of differentiation of human embryonic stem cells. PLoS ONE. 2010;5(6): e11167.
Aono A, Hazama M, Notoya K, Taketomi S, Yamasaki H, Tsukuda R, et al. Potent ectopic bone-inducing activity of bone morphogenetic protein-4/7 heterodimer. Biochem. Biophys. Res. Commun. 1995;210(3):670–7.
Bessho K, Kusumoto K, Fujimura K, Konishi Y, Ogawa Y, Tani Y, et al. Comparison of recombinant and purified human bone morphogenetic protein. Br J Oral Maxillofac Surg. 1999;37(1):2–5.
Jeong I, Yu H-S, Kim M-K, Jang J-H, Kim H-W. FGF2-adsorbed macroporous hydroxyapatite bone granules stimulate in vitro osteoblastic gene expression and differentiation. J Mater Sci Mater Med. 2010;21:1335–42.
Hossain M, Irwin R, Baumann MJ, McCabe LR. Hepatocyte growth factor (HGF) adsorption kinetics and enhancement of osteoblast differentiation on hydroxyapatite surfaces. Biomaterials. 2005;26:2595–602.
Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor. Endocr Rev. 1997;18:4–25.
Bikfalvi A, Klein S, Pintucci G, Rifkin DB. Biological roles of fibroblast growth factor-2. Endocr Rev. 1997;18:26–45.
Aryal R, Chen X, Fang C, Hu Y. Bone morphogenetic protein-2 and vascular endothelial growth factor in bone tissue regeneration: new insight and perspectives. Orthop Surg. 2014;6:171–8.
Pietrzak WS, Dow M, Gomez J, Soulvie M, Tsiagalis G. The in vitro elution of BMP-7 from demineralized bone matrix. Cell Tissue Bank. 2012;13:653–61.
Han B, Tang B, Nimni ME. Quantitative and sensitive in vitro assay for osteoinductive activity of demineralized bone matrix. J Orthop Res. 2003;21:648–54.
Wildemann B, Kadow-Romacker A, Haas NPP, Schmidmaier G. Quantification of various growth factors in different demineralized bone matrix preparations. J Biomed Mater Res A. 2007;81:437–42.
Lian JB, Stein GS. Development of the osteoblast phenotype: molecular mechanisms mediating osteoblast growth and differentiation. Iowa Orthop J. 1995;15:118–40.
Baylink DJ, Finkelman RD, Mohan S. Growth factors to stimulate bone formation. J Bone Miner Res. 1993;8:S565–72.
Chen G, Deng C, Li YP. TGF-β and BMP signaling in osteoblast differentiation and bone formation. Int J Biol Sci. 2012;8:272–88.
Wei L, Miron RJ, Shi B, Zhang Y. Osteoinductive and osteopromotive variability among different demineralized bone allografts. Clin Implant Dent Relat Res. 2015;17:533–42.
Sodek J, Chen J, Nagata T, Kasugai S, Todescan R, Li IW, et al. Regulation of osteopontin expression in osteoblasts. Ann N Y Acad Sci. 1995;760:223–41.
Hunter GK. Role of osteopontin in modulation of hydroxyapatite formation. Calcif Tissue Int. 2013;93:348–54.
Izal I, Ripalda P, AA A, Álvarez E, Forriol F. Análisis de la presencia de TGF-ß1, BMP- 7, MMP- 2 y PEDF en distintas matrices óseas desmineralizadas. Patol Del Apar Locomot. 2006;4:125–30.
Zhang M, Powers RM, Wolfinbarger L. A quantitative assessment of osteoinductivity of human demineralized bone matrix. J Periodontol. 1997;68:1076–84.
Hinsenkamp M, Muylle L, Eastlund T, Fehily D, Noël L, Strong DM. Adverse reactions and events related to musculoskeletal allografts: reviewed by the World Health Organisation Project NOTIFY. Int Orthop. 2012;36:633–41.
Acknowledgements
This work was supported by the by the Instituto de Salud Carlos III, Ministerio de Economía y Competividad and ESF European Social Fund (Fondos FSE) (PI13/00372 and MS16/00124), the Programa Campus de Excelencia Internacional del Ministerio de Educación Cultura y Deporte (contract to M.M.), the Conselleria d’Educació, Cultura i Universitats del Govern de les Illes Balears (PD/018/2014).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Ramis, J.M., Calvo, J., Matas, A. et al. Enhanced osteoinductive capacity and decreased variability by enrichment of demineralized bone matrix with a bone protein extract. J Mater Sci: Mater Med 29, 103 (2018). https://doi.org/10.1007/s10856-018-6115-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10856-018-6115-8