
Abstract
The use of psychoeducational interventions with parents of children diagnosed with a disability has been found to be effective in promoting parental well-being and improving family functioning. Such interventions typically require multiple sessions which, although well-meaning, impose time burdens on frequently overwhelmed parents. Research on brief interventions has shown promise for both children and adults in reducing emotional distress and improving psychological functioning. This study sought to assess the efficacy of a single-session intervention designed to reduce emotional distress and improve resilience among parents with a child diagnosed with a low-incidence disability. Results supported the efficacy of a single-session intervention for these parents. Twenty-six parents/primary caregivers of children diagnosed with low-incidence disabilities participated in a single-session intervention, a 5.5-hour psychoeducation workshop, to determine effects on measures of parental depression, anxiety, and stress, resilience, self-efficacy, and well-being. Comparisons of pretest-posttest mean scores revealed statistically significant differences on six of eight measures, all in an improved direction (i.e., lower posttest levels on measures of anxiety and stress, and higher posttest levels on measures of resilience, self-efficacy, and well-being). Positive post-workshop evaluation ratings also support the value of this intervention for parents. A description of workshop methods and content is provided to facilitate study replication. Authors discuss strategies for using brief, interactive, and resource-based psychoeducational parent training sessions to benefit families of children with disabilities.
Highlights
-
A single-session intervention resulted in improved psychological-emotional outcomes for parents with a child with a disability;
-
Findings included improved self-efficacy, well-being, and resilience and reduced anxiety and stress, but not depression;
-
Results of this study suggest the value of replication using a pre-post, control group, experimental design;
-
An unanticipated outcome was the degree to which participants created opportunities to develop strong emotional bonds.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Research findings reveal that parents of children diagnosed with intellectual disabilities and other low-incidence disabilities experience stressors that have negative consequences for the family system (Dabrowska & Pisula, 2010; Davis & Carter, 2008; Estes et al., 2009; Hayes & Watson, 2013; Pastor-Cerezuela et al., 2015; Phetrasuwan & Shandor Miles, 2009; Shawler & Sullivan, 2017). The U.S. Department of Education (2019) defined a low incidence disability as (a) a visual or hearing impairment, or simultaneous visual and hearing impairments; (b) a significant cognitive impairment; or (c) any impairment for which a small number of personnel with highly specialized skills and knowledge are needed for children with that impairment to receive early intervention services or a free appropriate public education. As such, a low incidence disability is not a medical diagnosis, but a label used in education systems.
A common dynamic that exacerbates parental stress in families with a child diagnosed with a low incidence disability is the need for parents to focus inordinate amounts of time and energy on the child. (Mazefsky et al., 2008). This may result in resentment and emotional distancing among family members as typically shared resources are consistently directed toward supporting the child diagnosed with a disability (van der Veek et al., 2009). Other everyday stressors include lack of parental free time and restricted family activities (Uskin & Undogar, 2010; Weiss & Lunsky, 2011); significant financial strain due to the need for specialized medical care and treatment (Buescher et al., 2014); and marital discord (Pastor-Cerezuela et al., 2015; van der Veek et al., 2009).
Left unchecked, chronic stress may result in negative physical and psychological consequences for family members that include the development of elevated stress levels (Dabrowska & Pisula, 2010; Hayes & Watson, 2013); physical health problems such as immune, digestive, cardiovascular, and sleep disorders, as well as heart disease, hypertension, and diabetes (National Institute of Mental Health, n.d.); psychological disorders such as anxiety, depression, hopelessness (Ergüner-Tekinalp & Akkök, 2004; Falk et al., 2014; Martin et al., 2019; Scherer et al., 2019; van der Veek et al., 2009); reduced levels of psychological well-being (Hickey et al., 2020); and reduced coping abilities (Pisula & Kossakowska, 2010). These consequences may exacerbate extant stressors to create a cycle of hopelessness for some or all family members.
Supporting a child with a low incidence disability requires specialized services from community- and school-based professionals as well as substantive knowledge, skill, patience, time, and financial resources from parents and primary caregivers. Parents and caregivers are often expected to be partners in treatment and intervention plans for their children. However, they are often ill-equipped to successfully consult with medical/school-based staff, mobilize necessary child and family resources, intervene effectively with their children at home, and provide necessary self-care (Kobak et al., 2011; Suppo, 2012). In the absence of knowledge and resources, parents may adopt inappropriate or unrealistic expectations for themselves, other family members, or service providers that increase already-elevated stress levels. The current study examines the impact of a single-session psychoeducational intervention designed to provide knowledge and skills that promote parental and family resilience and well-being. Because the intervention can be implemented by a variety of community- and school-based professionals, this model has the potential to efficiently and economically benefit parents and families.
Rationale for Use of a Single-Session Intervention
The purpose of this study was to determine the effectiveness of a brief psychoeducational intervention to reduce stress, depression, and anxiety and improve resilience, self-efficacy, and psychological well-being among parents of children diagnosed with a low-incidence disability. The traditional rationale for using a non-experimental and short-term intervention is that they provide information on potential efficacy before more in-depth and costly experimental methods are implemented. Single-session interventions provide information on inclusion/exclusion criteria, usefulness of instrumentation, material development, and preparation of researchers and research assistants (Leon et al., 2011). However, growing evidence suggests that, in some instances, a one-session intervention may be the intervention of choice (Ollendick et al., 2009; Öst et al., 2001; Schleider & Weisz, 2017a). Longer interventions do not necessarily translate to more effective outcomes and single-session mental health interventions have yielded positive effects for a variety of problems (Schleider & Weisz, 2017a; Schleider & Weisz, 2017b; cf. Carney & Myers, 2012). A key feature of single-session interventions is that they target population-specific needs. Terminology related to brief interventions that appear in the research literature differs, which likely reflects authors’ theoretical conceptualizations or research designs. Terminology includes single-session interventions (Schleider & Weisz, 2017b; Sung et al., 2021); single session therapy (Ryan & O’Connor, 2017); and one-session treatments (Öst et al., 2001). In some cases, single-session interventions are also described as a feasibility study or a pilot study (Bastida-Pozuelo et al., 2018; Lane et al., 2021).
A meta-analysis of single-sessions interventions for youth with psychiatric problems found greatest effect for anxiety and conduct problems, smaller effect size differences for self-efficacy and substance abuse, and none for depression (Schleider & Weisz, 2017a). Muskett et al., (2020) reported positive results in reduction of phobias for children with ASD traits using a one session intervention incorporating cognitive-behavioral therapy (CBT). Other studies have shown positive results for adults as well as children with phobias and for parent training (McConnell et al., 2020). McConnell et al. demonstrated that a single session of feedback and coaching with follow-up short texts improved parents’ well-being and emotional attachment as well as availability for their young children (0–3 years old). Lane et al., (2021) reported that single-session training using pre-post data collection methods was shown to be effective in increasing parent knowledge and self-efficacy in promoting physical literacy for their children. Single-session interventions have also been used in training interventions for parents of children with disabilities or behavioral problems. Single-session consultations with parents has been found to decrease stress and improve self-efficacy for dealing with their child’s behaviors (Sommers-Flanagan, 2007). Nock & Kazdin, (2005) reported the success of a brief motivational intervention designed to increase parental attendance at treatment sessions for their children who were diagnosed with conduct disorders compared to parents who did not participate in the brief motivational intervention. Parents of children diagnosed with ASD rated positively their experience with a single-session consultation and this single intervention was shown to improve their participation when a long-term intervention was established (Ryan & O’Connor, 2017). Sung et al., (2021) reported success of an online brief intervention to reduce parental accommodation of their child’s anxiety. Sofronoff et al. (2011) successfully used a brief didactic intervention (two, 2 h seminars) for parents of children with a disability. The intervention resulted in reductions in child behavior problems, improved parenting styles, and less parental conflict. Kasperzack et al., (2020) successfully used a single group design for delivering the Stepping Stones Triple P group parenting program to parents of children with ASD.
Psychological Resilience
Abidin (1992) stated that specific characteristics of children (i.e., behavior, self-care skills, and intellectual ability) and parents (i.e., select personality features, perceived availability of resources, and parenting self-efficacy) are essential factors to consider when helping parents of children with disabilities deal with stress. Numerous studies have identified psychological resilience and social supports as variables that moderate the effects of negative life experiences and emotions on psychological well-being (Bekhet et al., 2012; Bitsika et al., 2013; Dyches et al., 2016). Pastor-Cerezuela et al., (2015) explained that not all parents of children with a diagnosed disability report high stress levels. An event is experienced as stressful based on the meaning attributed to the event and perceived coping resources. Bitsika et al., (2013) demonstrated that even relatively low resilience levels served as a buffer against anxiety and depression for parents of children diagnosed with autism spectrum disorder. These findings suggest the critical role of resilience in equipping parents to navigate family challenges with a child diagnosed with a disability.
Psychological resilience reflects the notion that individuals can recover from stressful events (Smith et al., 2008) and thrive, adapt, and cope beyond simple recovery (Connor & Davidson, 2003). Luthar et al., (2000 p. 543) defined resilience as a “dynamic process encompassing positive adaptation within the context of significant adversity.” When faced with adversity, resilient parents better adapt to change, effectively parent their children with disabilities, and meet their own needs (Bekhet et al., 2012). Pastor-Cerezuela et al., (2015) found that parents of children with disabilities who perceived themselves as more resilient to adversity reported less stress associated with depressive symptoms and greater feelings of competence about their role as parents.
Theoretical Models of Adaptation and Stress
Several theoretical models were considered in conceptualizing and developing the single-session workshop intervention. With a focus on variables related to resilience, McCubbin & Patterson’s (1983) Double ABCX Model of Family Adaptation describes relationships between stressful life events, available resources, and the appraisal of a situation on the family’s ability to adapt to stressors. As Dabrowska & Pisula, (2010) noted, this model addresses three essential resources: personal resources of family members (physical and emotional health, personality characteristics, financial well-being); internal resources of the family system (cohesion and adaptability, communication patterns, mutual support); and social support from external resources. This theory suggests that stress may affect parents’ abilities to care for a child with special needs and that stress can be mitigated by adopting parental coping strategies.
The Transactional Theory of Stress and Coping (TTSC, Lazarus, 1966; Lazarus & Folkman, 1987) proposes that stress results from a transactional process between a person and his/her environment. This process includes four components: an external event (stressor), a cognitive appraisal of this event, coping mechanisms, and the stress reaction involving the mind and body. Cognitive appraisal refers to the personal interpretation of a situation that ultimately influences how the situation is perceived (i.e., stressful, or not stressful). It is the process of assessing (a) whether a situation or event threatens our well-being, (b) whether there are sufficient personal resources available for coping with the demand of the situation, and (c) whether our strategy for dealing with the situation is effective (Lazarus, 1991, 1993). The Double ABCX Model of Family Adaptation and the Transactional Theory of Stress and Coping reveal common elements: (a) the capacity to appraise personal circumstances to moderate stress responses and (b) the ability to learn rational and effective appraisal/decision-making skills. These elements influenced the design of the single-session intervention reported in this paper.
In crafting the didactic and discussion sections of the psychoeducational workshop we incorporated standard instructional design elements as well as recommendations by Catalano et al.. (2018) for designing educational interventions for parents of children diagnosed with autism spectrum disorder. These recommendations included: social support, professional training in cognitive-behavioral skill development, and knowledge acquisition including resource information. Effective social support involved real-time face-to-face engagement, reduced isolation by talking with parents with similar concerns, and receiving validation from peers. The professional training in cognitive-behavioral skill development component included a presentation on strategies to promote rational thinking, stress-management, and problem-solving. The final component, knowledge acquisition about their child’s diagnosis and information about local resources and services, included information provided by content experts.
Although Catalano et al., (2018) focused on parents of children with ASD, we decided that it is reasonable to extrapolate the instructional elements proposed by Catalano et al. to our sample of parents whose children include those with ASD and as well as other low-incidence disabilities. A few studies have found similar high stress impacts on families who have a child diagnosed with ASD and other neurodevelopment disorders (Ashworth et al., 2019), although less so with parents of children with Downs syndrome (Dabrowska & Pisula, 2010; Sanders & Morgan, 1997). Other researchers suggest that the stress levels of parents who have a child diagnosed with ASD are higher than those of with parents of children with other neurodevelopmental disorders (see literature review in Pastor-Cerezuela et al., 2021). However, until research can robustly differentiate relevant parental differences, we believe that sufficient similarities exist to use the Catalano et al. recommendations as an instructional guide.
Need for the Study
Although a comprehensive review of professional literature yielded several studies that examined the effectiveness of psychoeducational interventions for parents of children with disabilities, no reported studies were consistent with the intervention type, length, methods, or variables reported in the current study. With an understanding of psychological dynamics in families with a child diagnosed with a low incidence disability, the present findings suggest that a single-session workshop may improve parental levels of psychological and emotional functioning.
Method
Sample
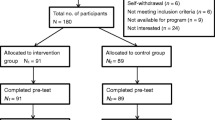
Before implementation, this study was approved by the Institutional Review Board for Human Subjects. Subjects were 26 parents or primary caregivers of children diagnosed with low incidence disabilities who attended a single-session (5.5 h) psychoeducational workshop. Workshop attendees were predominantly female (88.5%), White, non-Hispanic (96.2%), married (68%), and had attended some college (38.5%). Almost half (46.2%) of the participants were 40–50 years old, and nearly 81% of the parents were under 50. Their median income was between $40,000–$49,999, with lower and upper intervals from under $20,000 to over $100,000. The predominance of female participants in our sample is consistent with other parent training programs where mothers or grandmothers are in greater attendance. The percent of participants who are white is consistent with county demographics where 80% of its residents are white, but the median income is slightly lower than $50,000. Based on the U. S. Department of Education definition of low incidence disabilities (2019), all workshop participants were parents or primary caregivers of a child diagnosed with a low incidence disability who received specialized and intensive instruction in the school setting. All parents reported that their child’s diagnosis was made at age four or earlier. A majority of subjects (n = 17, 65.4%) reported that their child was diagnosed with autism spectrum disorder (5 of these subjects identified multiple disabilities); 6 parents identified having a child with an intellectual disability or developmental disability with intensive needs (3 of these subjects identified Down Syndrome); and 3 identified having a child with another significant low incidence disability. Seventy percent of parents (n = 19) indicated that their child received intensive and specialized instruction for more than 75% of each school day.
Procedures
The first step in planning the psychoeducational workshop was to identify an advisory group of stakeholders including regional education and community service providers and a representative from the funding agency that supported this study. In response to a presentation of proposed content, advisory board members strongly encouraged us to ask parents what information or services they needed. Consequently, we implemented a planning workshop consisting of parents with a child diagnosed with a low incidence disability. We presented information about proposed topics and delivery methods using didactic presentations, large group sessions, and focus group activities. The planning workshop served as a “dry-run” for the single-session intervention described in this paper with embedded opportunities to obtain parents’ feedback on specific content and processes: what worked, what didn’t work, and what should be added. We incorporated parents’ feedback from this planning workshop into the design of the current single-session intervention, which is the focus of this study.
We collaborated with regional educational and community service providers who worked with students with intensive needs to identify parents and caregivers as potential participants in the single-session workshop. These students attended schools for students diagnosed with low incidence disabilities. Once parents were identified, a cover letter was mailed that explained the purposes of the workshop intervention, an invitation to participate, procedures for participation, and information about a cash-equivalent incentive for participation. Participants received a grocery store card ($150.00 value) incentive for participation in the study. The workshop was held at a university setting in a wing of the student union available to community groups. There was a large meeting room and adjacent small rooms for focus groups/small group activities.
On the day of the workshop, parents received a comprehensive description of the study and completed an informed consent form. They also received handouts corresponding to didactic presentations and color-coded packets containing pre-and post-workshop assessment instruments (with coded I.D. numbers). After welcoming participants, one of the researchers provided directions for completing pre-workshop assessments. At the end of the workshop, parents completed post-workshop assessments.
The didactic portions of the workshop were presented by content experts who provided information on four topics which are described in the next section. Each workshop component included use of a didactic presentation and other handout materials. Two didactic presentations were made during the morning session and two during the afternoon session. Immediately following each presentation, parents broke-out into one of four parallel focus groups related to the same topic. During focus group sessions, participants were asked structured interview questions and then provided opportunities to ask additional questions and share feedback. All focus group sessions were audio-recorded, transcribed, and analyzed to identify themes and trends in parents’ communications.
Workshop Materials session
Component One
Content for this component was designed to provide information and strategies to promote psychological resilience and well-being and decrease levels of depression, anxiety, and stress for parents. This didactic component was led by the second author, (KLM) who is a professor of counseling and a licensed professional clinical counselor. A cognitive-behavioral therapy (CBT) model guided development of session content as CBT has been shown to be robust and effective for treating a variety of psychological disorders including anxiety, stress, depression, phobias, and autism (Reavell et al., 2018).
This didactic component included the following topics: definitions of resilience, research findings on the importance of resilience for psychological health and well-being, positive and negative effects of raising a child diagnosed with a disability, and three strategies for promoting psychological resilience. These strategies include (a) healthy choices (e.g., adequate sleep, healthy diet, regular physical exercise); (b) clear thinking (e.g., strategies for rational thinking, reasonable expectations); and (c) human connections (e.g., family relationships, community connections).
The presentation emphasized the important role that resilience plays for all family members when a child has been diagnosed with a disability. Participants were given additional information related to resilience as a learnable skill/life strategy, strategies to build resilience, external factors that impact resilience development, case study presentation designed to demonstrate rational vs. irrational thinking and resilient vs. non-resilient responses, and a video presentation. Participants were provided ample opportunities to ask questions and comment on topics addressed during the didactic presentation which included discussions of personal challenges and successes in developing personal resilience.
Component Two
Content for this didactic presentation was designed to provide information to parents regarding the importance of home-school collaboration and to enhance effective parental communication and home-school collaboration skills. This component was led by the first author (RWV), a professor in school psychology. Topics covered included the need for active listening, perspective taking, appropriate assertiveness, and ways to manage conflict. Parents were encouraged to serve as active team members during home-school collaboration and manage their own personal feelings while simultaneously advocating for their children. Participants were provided with opportunities for reflection and discussion.
Component Three
This workshop component focused on understanding parental rights related to disability services and was led by a statewide disability advocate. The objective was to aid participants in developing clarity about parental rights related to disability services and to provide strategies for resolving conflicts with schools and agencies. Parents had the opportunity to pose questions in the large group setting, thus hearing the types of problems encountered by others, and potential solutions for those conflicts.
Component Four
The fourth didactic presentation was led by a community social worker who provided in-depth information about local, state, and national resources for families of children with disabilities. Each parent received a comprehensive directory of these resources. Part of the presentation involved a discussion of strategies that parents could use when encountering problems while gathering resource information. Because the agency had extensive experience working with this population, the most relevant resources were pre-selected, but parents were provided opportunities to meet with agency personnel individually and in small groups to discuss needs for addition information.
Instrumentation
Workshop participants completed assessments on relevant variables of interest prior to the workshop and again at the end of the workshop. Directions for completing instruments in the pretest condition used standardized administration directions (e.g., “how have you have felt during the past two weeks”). Participants were asked to base their posttest responses on “how they felt at present.”
Demographic Variables: Demographic/Personal Information Form (D/PIF)
This author-developed instrument was designed to collect relevant personal information about participating parents and their child/children. Data were collected on (a) parental variables: age, gender, race/ethnicity, family income level, marital status, completed education; (b) family support variables: level of partner’s support in caring for the child, level of extended family support; and (c) child’s situation: time since child’s diagnosis (in years), child’s age at the time of diagnosis, parent’s age at the time of diagnosis, and parent’s adjustment to child’s diagnosis.
Resilience: Brief Resilience Scale (BRS)
The authors of the Brief Resilience Scale (BRS), Smith et al., (2008), defined their instrument as assessing "the ability to bounce back or recover from stress." The BRS consists of six items using a 1 (strongly disagree) to 5 (strongly agree) response format. The final score is calculated as the mean, with higher scores reflecting greater resilience. Smith et al. reported Cronbach’s alphas (a = 0.80–0.91) for four samples in their initial report. A principal component analysis revealed a unitary construct was positively related to optimism and life purpose characteristics and negatively related to pessimism, denial, and self-blame.
Connor-Davidson Resilience Scale (CD-RISC)
The Connor-Davidson Resilience Scale (CD-RISC) authors conceptualized resilience through a larger lens. Rather than centering the definition on recovery, they included ideas of thriving, adaptation, and coping in their definition of resilience (Connor & Davidson, 2003). The CD-RISC consists of 25 items to which responses are made on a 5-point from 0 (rarely true) to 4 (true nearly all of the time) summed to achieve a final scale score. The authors reported an internal consistency coefficient of 0.89 for the general population sample.
Depression, Anxiety, and Stress Scale (DASS)
The DASS-42 was created by Lovibond & Lovibond, (1995) to assess and distinguish three dimensions of emotional distress that frequently co-occur: depression, anxiety, and stress. The initial instrument was modified to a 21-item short form with seven items assessing each construct/subscale, which mirrored the good psychometric properties of the DASS-42 (Anthony et al., 1998). A principal component analysis across clinical and non-clinical groups revealed a three-factor structure corresponding with the hypothesized three subscales of depression, anxiety, and stress. Cronbach’s alphas reported for the subscales were a = 0.94 for depression, a = 0.87 for anxiety, and a = 0.91 for stress. Henry and Crawford (2005) found similar reliability estimates for a large non-clinical group: a = 0.88 for depression, a = 0.82 for anxiety, a = 0.90 for stress and a = 0.93 for total scale.
General Self-Efficacy Scale (GSE)
Schwarzer and Jerusalem designed the 20-item General Self-Efficacy Scale (GSE) to assess an individual’s sense of competence to deal effectively with a wide range of life stressors. It was later shortened to 10 items using a 4-point response format from 1 (not at all true) to 4 (exactly true) summed to produce a final score. Authors reported Cronbach’s alphas from a = 0.76–0.90 (Schwarzer & Jerusalem, 1995). Luszczynska et al., (2005) reported Cronbach alphas from a = 0.86–0.94.
WHO-5 Well Being Index (WHO-5)
The 5-item Well-Being Index emerged from work by the World Health Organization (World Health Organization, 1998) to produce a questionnaire that focused only on generic, positive mental health (Topp et al., 2015). The index consists of five statements (e.g., I have felt calm and relaxed) deliberately constructed to reflect global rather than domain-specific content or symptoms. Respondents self-rate the applicability of each statement on a Likert-type scale ranging from 0 (at no time) to 5 (all of the time). To facilitate comparison to similar scales, the raw score can be multiplied by 4 to yield a continuum from worst possible quality of life (0) to best possible quality of life (100). In a study of 9,542 Danish citizens, Bech et al., (2006) reported a Cronbach alpha of 0.84 which suggests good internal consistency for short scales.
Workshop Evaluation Form
This evaluation form consists of seven items designed to capture participants’ perceptions of workshop quality and effectiveness. Evaluation criteria include: preference for face-to-face receipt of information; feeling respected for workshop contributions; perceived clarity of purpose of workshop; whether workshop is worth respondent’s time; whether workshop participation enhanced understanding of respondent’s roles as an expert and consultant; whether information presented is useful to the respondent, and; whether the respondent liked the format of workshop presentations. Respondents are asked to rate these items on a 5-point Likert-type scale where 1 = Strongly Disagree to 5 = Strongly Agree. The evaluation form also includes two open-ended questions designed to solicit qualitative feedback on strengths and limitations of the workshop.
Results
Pre-Post Scores on Dependent Variables
We used a within-subjects, pretest-posttest design to determine the extent to which parents’ levels of resilience, self-efficacy, well-being, depression, anxiety, and stress were influenced by participation in a single-session psychoeducational workshop. A one-way within-subjects ANOVA was conducted for each dependent variable using IBM SPSS Statistics (Version 26). Statistical findings are presented in Table 1.
Brief Resilience Scale
A one-way within-subjects analysis of variance (ANOVA) was conducted to evaluate change in pre-post resilience scores following participation in the psychoeducational workshop (N = 26). The null hypothesis was rejected; there was a statistically significant effect of the intervention, Wilks’ Lambda = 0.673, F(1, 25) = 12.12, p = 0.002. The effect size was satisfactory, η (eta) = 0.327.
Conner-Davidson-Resilience Scale
In contrast to the outcome on the Brief Resilience Scale, measuring resilience using the Connor-Davidson Resilience Scale yielded no statistically significant effect, Wilks’ Lambda = 0.929, F(1, 25) = 1.91, p = 0.180.
Depression Anxiety and Stress Scales (DASS)
A one-way within subjects analysis of variance (ANOVA) revealed a statistically significant effect on total score, Wilks’ Lambda = 0.705, F(1, 25) = 10.47, p = 0.003; subscale score for anxiety, Wilks’ Lambda = 0.564, F(1, 25) = 19.32, p = 0.000; and subscale score for stress, Wilks’ Lambda = 0.795, F(1, 25) = 6.45, p = 0.018. No statistically significant effect was found on the subscale score for depression, Wilks’ Lambda = 2.77, F(1, 25) = 2.77, p = 0.108.
General Self-Efficacy Scale (GSE)
A one-way within subjects analysis of variance (ANOVA) revealed a statistically significant effect for the intervention: Wilks’ Lambda = 0.740, F(1, 25) = 8.76, p = 0.007, with an effect size, ƞ (eta) = 0.260.
WHO-5 Well Being Index (WHO-5)
A one-way-within subjects ANOVA yielded a statistically significant effect of the workshop on parents’ sense of well-being: Wilks’ Lambda = 0.596, F(1,25) = 16.27, p = 0.000, and eta = 0.404. Compared to a pretest raw score mean of 12.60 (5.05), the posttest raw score mean was 15.60 (5.48). Using the recommendation for multiplying scores to a 100-point scale, the pretest is 50.40% and the posttest of 62.40%. An increase of 10% indicates clinical change (Bech et al., 2007).
Workshop Evaluation
At the end of the 5.5 h workshop, participants were provided an evaluation form to rate their levels of satisfaction with the event. All participants (N = 26) fully completed this evaluation. Questions were presented using a five-point Likert scale from 1 = Strongly Disagree to 5 = Strongly Agree. The inclusion of rich information regarding the community, state, and national resources and services may help to explain parents’ strong overall endorsement (\(\overline X\) = 4.59/5.00) of the psychoeducational workshop on the end-of-day evaluation.
Table 2 lists mean scores on evaluation items in descending order with corresponding standard deviations. These data reveal that participants overwhelmingly supported the value of face-to-face opportunities to receive information versus web/individual-based access. They endorsed the value of a clearly stated workshop purpose and felt respected for their contributions throughout the workshop activities. Participants further reported that the workshops helped them understand their roles as experts and consultants in securing necessary services for their children. The information presented during the workshop was reported to be helpful. Within the comments section of the evaluation, parents remarked, “I feel that all items today were very useful” and “Sharing was such a blessing.” One parent responded, “Face-to-face workshops are the best, as they provide opportunities to really connect.” Another added that “Many parents of children with disabilities feel alone, so face to face workshops (like these) are great for parents to have the opportunity to engage with others.” Parents found the program content to be helpful in addition to the opportunities to share their ideas during focus group sessions.
Most of the items on the evaluation form measured participants reactions to the workshop and their reactions were positive. According to Kirkpatrick’s evaluation model (Kirkpatrick, 2006) although reactions are the first level of measurement (followed by learning, improved performance, and organizational change), it is an important level. Reactions likely influence a willingness to learn, as well as participant willingness to attend similar workshops and to suggest such opportunities to others. According to Kirkpatrick’s model (Reio et al., 2017), a level 2 evaluation is assessment of learning that occurs as the result of the training content. For this study, learning can be interpreted as the positive improvements found on posttest measures. Smidt et al., (2009) recommended Kirkpatrick’s model for evaluating training programs for adults working with individuals with disabilities.
Discussion
The primary finding of this study was the potential value of a single-session intervention for improving resilience, anxiety, stress, self-efficacy, and well-being levels for parents of a child diagnosed with a low-incidence disability. These results suggest that a relatively short-term intervention can benefit parents who struggle with challenging personal and familial dynamics. It provides preliminary support for school and community-based mental health professionals to add single-session psychoeducational workshops to their interventions for working with families. Overall, the potential efficacy of the single-session group intervention is indicated by statistically significant improvements on six of the eight variables of interest in the desired direction (i.e., lower posttest scores on anxiety, stress, and total DASS score; higher posttest scores on one measure of resilience, self-efficacy, and well-being). Although the small sample size inhibits generalizability, the similarity of parents’ scores to those known in other clinical studies reduces the impact of this problem.
Participation in the single-session intervention had a short-term, positive effect on parental resilience. Parents produced statistically significant higher scores (i.e., greater resilience) on the Brief Resilience Scale posttest (M = 3.69) compared to the pretest (M = 3.40). Resilience has been identified as an important predictor of parents’ abilities to create and maintain a good quality of life for themselves and their families and to respond productively to their child’s needs and demands. There are few published studies with similar samples to enable comparative interpretations of BRS scores.
Workshop parents demonstrated moderately low resilience pretest scores on the Connor-Davidson Resilience Scale (M = 71.54 on a scale of 0–100). This mean was only slightly higher than parents of children with ASD reported by Bitsika et al., (2013) for a sample of 73 mothers (M = 67.04) and 35 fathers (M = 65.05). As anticipated, parents attending the psychoeducational workshop were less resilient compared to Connor and Davidson’s, (2003) sample (N = 577) from the general population (M = 80.40). Workshop parents’ CD-RISC resilience mean score was higher at posttest, but not at a statistically significant level. This finding is incongruent with parents’ mean scores on the BRS that were statistically significantly higher (greater resilience) at posttest, except that the movement is in the positive direction. Outcomes of future studies may help explain this discrepancy.
Parents’ level of anxiety at pretest was in the mild range (M = 9.23). This mean is consistent with findings from other studies with U.S. fathers (M = 9.71) and mothers (M = 10.50) reported by Falk et al., (2014) and Australian parents (M = 8.95) reported by Firth & Dryer, (2013). At posttest, the mean parental anxiety score (6.62) was in the normal range, and this difference (less anxious) was statistically significant. Similarly, stress levels of workshop parents improved from mild (M = 17.00) at pretest to normal (M = 13.92) at posttest, and this difference (less stress) was also statistically significant. Comparison samples for pretest means consisted of Australian parents (M = 21.43) who scored in the moderate range (Firth & Dryer), and U.S. fathers and mothers who scored in the normal range, M = 10.11 and M = 11.6, respectively (Falk et al.).
We anticipated that participation in the single-session workshop would improve parents’ sense of self-efficacy. We anticipated that the range of workshop components would not only enhance parenting knowledge and skills but also result in broader positive beliefs about managing stress and challenging life tasks. The mean GSE pretest mean score of parents who attended the workshop was 31.08, and the posttest mean score was 33.31, a statistically significant increase in self-efficacy. The General Self-Efficacy Scale (Schwarzer & Jerusalem, 1995) has been used worldwide to examine patients’ responses to medical conditions, but we were able to locate only a few studies focusing on parents. Sevigny & Loutzenhiser (2009) reported on 62 mothers and 62 fathers of toddlers with no developmental disabilities. On the GSE, the mothers’ pretest mean score was 32.94, and the fathers’ pretest mean score was 32.60. Barlow et al., (2007) assessed parents of children with disabilities who were randomized into an experimental group and a (control) wait-list group. Their pretest means were 29.1 and 29.3, respectively, which were just slightly lower than the scores of workshop parents at pretest.
Consistent with the other positive outcomes of the single-session workshop, parents reported statistically significantly higher scores on well-being at posttest. Parents’ pretest mean on the WHO-5 was 50.77, which is just above the cut-off score (≤ 50) as an indicator of depression. The posttest score of 62.4 indicated a clinically significant change, as it exceeded a 10% difference, which is the recommended interval for determining a clinical change (World Health Organization, 1998).
A large-scale study comparing depression of parents of children with ASD to a control group (42,649 families in each group) found that mothers and fathers of a child with ASD had scores which were 2.9 and 2.4, respectively more likely to have a clinical diagnosis of depression compared to those in the control group (Cohrs &cLeslie, 2017). This was not the case for parents in the current study. Parents’ mean pretest score on the depression scale of the DASS was in the normal range (M = 8.92), and this score likely accounts for the lack of statistical significance at posttest (M = 7.46). Given this pre-test score, we can speculate that parents who volunteered to participate in this workshop were not suffering from depression. It is noteworthy that the posttest DASS score did drop in an improved direction. Some studies of parents of children diagnosed with autism spectrum disorder have found similar depression scores in the normal range, but parents in these studies were not from the United States (e.g., Chinese caregivers = 7.81, Chan et al., 2020; Indian parents = 6.13, Selvakumar & Panicker, 2020). A comparison of workshop parents’ mean pretest and posttest DASS depression scale scores is also inconsistent with findings by Falk et al., (2014) of U.S. mothers and fathers with a child diagnosed with autism spectrum disorder (M = 12.01 and M = 11.96, respectively, mild range). Finally, we need to consider the possibility of an interaction effect between the treatment modality (single-session) and type of subject-assigned variable (e.g., depression). A meta-analysis of single-sessions interventions from 50 studies for youth with psychiatric problems found no effect on depression although other outcomes such as anxiety and self-efficacy improved (Schleider & Weisz, 2017a). Further study is needed to identify workshop components that may enhance the potential of single-session interventions for reducing depression or alternatively, rule-out the use of a single-session intervention for this condition.
Limitations
Adoption of a single-session workshop intervention limits generalizability of findings. The absence of delayed post-testing to investigate long-term outcomes is consistent with current trends in parent education for children with autism spectrum disorders (Schultz et al., 2011), but it constrains a more robust understanding. We found that demands on parents’ availability to participate in even a single-session, day-long activity prohibited recruitment of a sufficient number of participants to establish treatment and control groups. These limitations require that findings from this study be interpreted with caution. Research using single-session interventions for parent training is in its infancy with an expectation that methodologies will evolve with additional research. Of note, our sample consisted of more female parents, which is the same limitation that occurs in almost all research on parent training programs. The racial composition of the sample was similar to that of the local county (80% white) with a median income slightly lower than the $50,000 median in the county. In these respects, the sample reflected the local population.
The design we employed was identified by Campbell, (1957) as a one-group pretest-posttest design. He noted the most important confounding threats to validity for this design were history, maturation, testing effects, instrument decay, and regression to the mean. Given the short duration of the intervention (5.5 h), we believe that the threats of history, maturation, and instrument decay were minimal or non-existent. We believe that testing effects and regression to the mean are worthy of concern. Testing effects are changes in a second administration of measures, especially when testing is not part of the test takers typical environment or when the subject becomes self-conscious due to the nature of questions asked. Because we asked questions related to parents’ own cognitions, emotions, and behaviors as they participated in focus groups during the workshop, it is possible that the questions themselves produced reactive responses on the second administration of the measures. We hope that this threat was mitigated as the description provided to the parents about what they could expect during the workshop included expectations for testing, and all participants were simultaneously engaged in the same procedures. A second limitation that we acknowledge in the manuscript is the possibility that regression toward the mean may have been operant in the testing process. We also acknowledge that a change in standardized directions in the administration of instruments from pretest to posttest may have resulted in a threat to accurate interpretations of test results. At posttest, participants were asked to respond to assessment items based their immediate feelings versus how they felt during the past two weeks.
All workshop participants were parents or primary caregivers of children who received services in settings designed for students with intensive special education needs, which may limit understanding of the efficacy of the psychoeducational workshop for parents of children educated in other learning environments. Incentives to participate in the study included: two $75.00 grocery store cards, a midday lunch, morning and afternoon snacks, and workshop content designed to improve both parental and family well-being. The magnitude of these incentives may have skewed participant responses on assessment instruments and workshop evaluation forms in positive directions. However, our observations of the sheer joy parents expressed in engaging with other parents in similar circumstances was unmistakable. Additionally, the deviation in standardized instrument directions for the posttest session (i.e., respond to each item “based on how you are feeling right now” [deviation from the standard direction] versus “based on how you have felt during the past two weeks” [standard direction]) may have produced less interpretable posttest scores.
Implications for Future Research and Conclusions
We were meticulous in conceptualizing and developing workshop components to be effective in reducing parental emotional distress and improving resilience. This attention may have resulted in the promising findings of this exploratory study. However, we strongly suspect that the quality of the parent-to-parent interactions played an unanticipated role in the results. We observed that during didactic workshop components and focus groups, parents created opportunities to share personal struggles and successes related to providing best care for their children. In these contexts, parents shared profound fears and joys that created strong emotional bonds and potential support systems. Future researchers who replicate this intervention should create ample opportunities for parents to develop close emotional bonds and evaluate how they can be fostered to enhance resilience.
We advocate the value of single-session interventions for parents of children with disabilities. Thus, future studies could attempt to replicate the results of this study and build a body of evidence for the effectiveness of this single-session design. Alternatively, future studies could opt for a true-experimental design to provide a deeper understanding of relationships among these variables. Longitudinal studies are needed to determine the extent to which changes in pretest-posttest scores are enduring. At least two delayed posttest data collections points will help assess longer-term impact. Adapting the workshop for virtual presentations with more racially, ethnically, and gender-diverse samples of participants may: (a) reduce barriers to child care; (b) promote parental participation and create opportunities for use of larger sample sizes, and; (c) create more generalizable results. Additionally, creating more focused open-ended questions regarding workshop quality/effectiveness on the Workshop Evaluation Form will provide researchers with crucial data for improving the research design. Despite these limitations, findings of the current study suggest that a single-session psychoeducational workshop has the potential to provide parents and caregivers of children diagnosed with low incidence disabilities with strategies required for reducing emotional distress and building resilience.
References
Abidin, R. R. (1992). The determinants of parenting behavior. Journal of Clinical Child Psychology, 21, 407–412. https://doi.org/10.1207/s15374424jccp2104_12
Ashworth, M., Palikara, O., & Van Herwegen, J. (2019). Comparing parental stress of children with neurodevelopmental disorders: The case of Williams syndrome and autism spectrum disorders. Journal of Applied Research in Intellectual Disabilities, 32, 1047–1057. https://doi.org/10.1111/jar.12594
Anthony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. https://doi.org/10.1037/1040-3590.10.2.176
Barlow, J. H., Powell, L. A., Gilchrist, M., & Fotiadou, M. (2007). The effectiveness of the training and support program for parents of children with disabilities: A randomized trial. Journal of Psychosomatic Research, 64, 55–62. https://doi.org/10.1016/j.jpsychores.2007.06.006
Bastida-Pozuelo, M.-F., Sanchez-Ortuno, M.-M., & Meltzer, L. J. (2018). Nurse-led brief sleep education intervention aimed at parents of school-aged children with neurodevelopmental and mental health disorders: Results from a pilot study. Journal for Specialists in Pediatric Nursing, 23, e12228. https://doi.org/10.1111/jspn.12228
Bech, P., Lunde, M., Bech-Andersen, G., Lindberg, L., & Martiny, K. (2007). Psychiatric outcome studies (POS): Does treatment help the patients? A Popperian approach to research in clinical psychiatry. Nordic Journal of Psychiatry, 61(46), 4–80. https://doi.org/10.1080/08039480601151238
Bech, P., Olsen, L. R., Kjoller, M., & Rasmussen, N. K. (2006). Measuring well-being rather than the absence of distress symptoms: A comparison of SF-36 Mental Health subscale and the WHO-Five Well-Being scale. International Journal of Methods in Psychiatric Research, 12(2), 85–91. https://doi.org/10.1002/mpr.145
Bekhet, A. K., Johnson, N. L., & Zauszniewski, J. A. (2012). Resilience in family members of persons with autism spectrum disorder: A review of the literature. Issues in Mental Health Nursing, 33(10), 650–656. https://doi.org/10.3109/01612840.2012.671441
Bitsika, V., Sharpley, C. F., & Bell, R. (2013). The buffering effect of resilience upon stress, anxiety, and depression in parents of a child with an autism spectrum disorder. Journal of Developmental and Physical Disabilities, 25, 533–543. https://doi.org/10.1007/s10882-013-9333-5
Buescher, A. V., Cidav, Z., Knapp, M., & Mandell, D. S. (2014). Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatrics, 168, 721–728. https://doi.org/10.1001/jamapediatrics.2014.210
Campbell, D. T. (1957). Factors relevant to the validity of experiments in social settings. Psychological Bulletin, 34(4), 297–312. https://doi.org/10.1037/h0040950
Carney, T., & Myers, B. (2012). Effectiveness of early interventions for substance-using adolescents: Findings from a systematic review and meta-analysis. Substance Abuse Treatment, Prevention and Policy, 7, 25 https://doi.org/10.1186/1747-597X-7-25
Catalano, D., Holloway, L., & Mpofu, E. (2018). Mental health interventions for parent carers of children with autistic spectrum disorder: Practice guidelines from a critical interpretive syntheses (CIS) systematic review. International Journal of Environmental Research and Public Health, 15(2), 341–364. https://doi.org/10.3390/ijerph15020341
Chan, B. S. M., Deng, J., Li, Y., Li, T., Shen, Y., Wang, Y., & Yi, L. (2020). The role of self-compassion in the relationship between post-traumatic growth and psychological distress in caregivers of children with autism. Journal of Child and Family Studies, 29, 1692–1700. https://doi.org/10.1007/s10826-019-01694-0.
Cohrs, A. C., & Leslie, D. L. (2017). Depression in parents of children diagnosed with spectrum disorder: A claims-based analysis. Journal of Autism and Developmental Disorders, 47, 1416–1422. https://doi.org/10.1007/s10803-017-3063-y
Connor, K. M., & Davidson, J. R. T. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18, 76–82. https://doi.org/10.1002/da.10113
Dabrowska, A., & Pisula, E. (2010). Parenting stress and coping styles in mothers and fathers of pre-school children with autism and down syndrome. Journal of Intellectual Disability Research, 54(3), 266–280. https://doi.org/10.1111/j.1365-2788.2010.01258.x
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal of Autism & Developmental Disorders, 38(7), 1278–1291. https://doi.org/10.1007/s10803-007-0512-z
Dyches, T., Christensen, R., Harper, J., Mandleco, B., & Roper, S. (2016). Respite care for single mothers of children with autism spectrum disorders. Journal of Autism & Developmental Disorders, 46(3), 812–824. https://doi.org/10.1007/s10803-015-2618-z
Ergüner-Tekinalp, B., & Akkök, F. (2004). The effects of a coping skills training program on the coping skills, hopelessness, and stress levels of mothers of children with autism. International Journal for the Advancement of Counselling, 26(3), 257–269. https://doi.org/10.1023/B:ADCO.0000035529.92256.0d
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X.-H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism: The International Journal of Research & Practice, 13(4), 375–387. https://doi.org/10.1177/1362361309105658
Falk, N. H., Norris, K., & Quinn, M. G. (2014). The factors predicting stress, anxiety, and depression in the parents of children with autism. Journal of Autism and Developmental Disorders, 44, 2189–3203. https://doi.org/10.1007/s10803-014-2189-4
Firth, I., & Dryer, R. (2013). The predictors of distress in parents of children with autism spectrum disorder. Journal of Intellectual & Developmental Disability, 38(2), 163–171. https://doi.org/10.3109/13668250.2013.773964
Hayes, S. A., & Watson, L. L. (2013). The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(3), 629–642. https://doi.org/10.1007/s10803-012-1604-y
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in large non-clinical sample. British Journal of Clinical Psychology, 44, 227–239. https://doi.org/10.1348/014466505X29657
Hickey, E. J., Hartley, S. L., & Papp, L. (2020). Psychological well‐being and parent‐child relationship quality in relation to child autism: An actor‐partner modeling approach. Family Process, 59(2), 636–650. https://doi.org/10.1111/famp.12432
Kasperzack, D., Schrott, B., Mingebach, T., Becker, K., Burghardt, R., & Kamp-Becker, I. (2020). Effectiveness of the Stepping Stones Triple P group parent program in reducing comorbid behavioral problems in children with autism. Autism, 24(2), 423–436. https://doi.org/10.1177/1362361319866063.
Kirkpatrick, D. L. (2006). Seven keys to unlock the four levels of evaluation. Performance Improvement, 45(7), 5–8. https://doi.org/10.1002/pfi.2006.4930450702
Kobak, K. A., Stone, W. L., Wallace, E., Warren, Z., Swanson, A., & Robson, K. (2011). A web-based tutorial for parents of young children with autism: Results from a pilot study. Telemedicine and e-Health Journal, 17, 804–808. https://doi.org/10.1089/tmj.2011.0060
Lane, C., Carson, V., Morton, K., Reno, K., Wright, C., Predy, M., & Naylor, P.-J. (2021). A real-world feasibility study of the PLAYshop: A brief intervention to facilitate parent engagement in developing their child’s physical literacy. Pilot and Feasibility Studies, 7, 113 https://doi.org/10.1186/s40814-021-00849-5
Lazarus, R. S. (1966). Psychological stress and the coping process. New York, NY: McGraw-Hill
Lazarus, R. S., & Folkman, S. (1987). Transactional theory and research on emotions and coping. European Journal of Personality, 1, 141–169.
Lazarus, R. S. (1991). Cognition and motivation in emotion. American Psychologist, 46(4), 352–367. https://doi.org/10.1037/0003-066X.46.4.352.
Lazarus, R. S. (1993). From psychological stress to the emotions: A history of changing outlooks. Annual Review of Psychology, 44, 1–21.
Leon, A. D., Davis, L. L., & Kraemer, H. C. (2011). The role and interpretation of pilot studies in clinical research. Journal of Psychiatric Research, 45, 626–629. https://doi.org/10.1016/j.jpsychires.2010.10.008
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. https://doi.org/10.1016/0005-7967(94)00075-U
Luszczynska, A., Scholz, U., & Schwarzer, R. (2005). The General Self-Efficacy Scale: Multicultural validation studies. The Journal of Psychology, 139(5), 439–457. https://doi.org/10.3200/JRLP.139.5.439-457
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562. https://doi.org/10.1111/1467-8624.00164
Martin, F., Clyne, W., Pearce, G., & Turner, A. (2019). Self-management support intervention for parents of children with developmental disorders: The role of gratitude and hope. Journal of Child & Family Studies, 28(4), 980–992. https://doi.org/10.1007/s10826-018-01308-1
Mazefsky, C. A., Williams, D. L., & Minshew, N. J. (2008). Variability in adaptive behavior in autism: Evidence for the importance of family history. Journal of Abnormal Child Psychology, 36, 591–599. https://doi.org/10.1007/s10802-007-9202-8
McConnell, M., Closson, L., Morse, B., Wurster, H., Flykt, M., Sarche, M., & Biringen, Z. (2020). The “EA brief”: A single session of parent feedback and coaching to improve emotional attachment and emotional availability (EA). Infant Mental Health Journal, 41(6), 783–792. https://doi.org/10.1002/imhj.21867
McCubbin, H. I., & Patterson, J. M. (1983). The family stress process: The double ABCX model of adjustment and adaptation. Marriage & Family Review, 6(1-2), 7–37. https://doi.org/10.1300/J002v06n01_02.
Muskett, A., Radtke, S. R., & Ollendick, T. A. (2020). A pilot study of one-session treatment for specific phobias in children with ASD traits. Journal of Child and Family Studies, 29, 1021–1028. https://doi.org/10.1007/s10826-019-01620-4
Nock, M. K., & Kazdin, A. E. (2005). Randomized control trial of a brief intervention for increasing participation in parent management training. Journal of Counseling and Clinical Psychology, 73(5), 872–879. https://doi.org/10.1037/0022-006X.73.5.872
Ollendick, T. H., Ost, L.-G., Reuterskiold, L., Costa, N., Cederlund, R., Sirbus, C., Davis, T. E. III, & Jarret, M. A. (2009). Journal of Counseling and Clinical Psychology, 77(3), 504–516. https://doi.org/10.1037/a0015158
Öst, L.-G., Svensson, L., Hellström, K., & Lindwall, R. (2001). One-session treatment of specific phobias in youths: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 69(5), 814–824. https://doi.org/10.1037/0022-006X.69.5.814
Pastor-Cerezuela, G., Fernandez-Andres, M. I., Perez-Molina, D., & Tijeras-Iborra, A. (2021). Parental stress and resilience in autism spectrum disorder and Down syndrome. Journal of Family Issues, 42(1), 3–36. https://doi.org/10.1177/0192513X20910192
Pastor-Cerezuela, G., Fernández-Andrés, M. I., Tárraga-Mínguez, R., & Navarro-Peña, J. M. (2015). Parental stress and ASD: Relationship with autism symptom severity, IQ, and resilience. Focus on Autism and Other Developmental Disabilities, 31(4), 300–311. https://doi.org/10.1177/1088357615583471
Phetrasuwan, S., & Shandor Miles, M. (2009). Parenting stress in mothers of children with autism spectrum disorders. Journal for Specialists in Pediatric Nursing, 14(3), 157–165. https://doi.org/10.1111/j.1744-6155.2009.00188.x
Pisula, E., & Kossakowska, Z. (2010). Sense of coherence and coping with stress among mothers and fathers of children with autism. Journal of Autism and Developmental Disorders, 40, 1485–1494. https://doi.org/10.1007/s10803-010-1001-3
Reavell, J., Hopkinson, M., Clarkesmith, D., & Lane, D. A. (2018). Effectiveness of cognitive behavioral therapy for depression and anxiety in patients with cardiovascular disease: A systematic review and meta-analysis. Psychosomatic Medicine, 80(8), 742–753. https://doi.org/10.1097/PSY.0000000000000626
Reio, Jr., T. G., Rocco, T. S., Smith, D. H., & Chang, E. (2017). A critique of Kirkpatrick’s evaluation model. New Horizons in Adult Education & Human Resource Development, 29(2), 35–53. https://doi.org/10.1002/nha3.20178
Ryan, C., & O’Connor, S. (2017). Single session psychology clinic for parents of children with autism spectrum disorder: A feasibility study. Journal of Child and Family Studies, 26, 1614–1621. https://doi.org/10.1007/s10826-017-0681-0
Sanders, J. L., & Morgan, S. B. (1997). Family stress and adjustment as perceived by parents of children with autism or Down Syndrome: Implications for intervention. Child & Family Behavior Therapy, 19(4), 15–32. https://doi.org/10.1300/J019v19n04_02
Schleider, J. L., & Weisz, J. R. (2017a). Little treatments, promising effects? Meta-analysis of single-session interventions for youth psychiatric problems. Journal of the American Academy of Child and Adolescent Psychiatry, 56(2), 107–115. https://doi.org/10.1016/j.jaac.2016.11.007
Schleider, J. L., & Weisz, J. R. (2017b). Can less be more? The promise and perils of single-session youth mental health interventions. The Behavior Therapist, 40(7), 256–261
Scherer, N., Verhey, I., & Kuper, H. (2019). Depression and anxiety in parents of children with intellectual and developmental disabilities: A systematic review and meta-analysis. PLOS ONE, 14(7), 1–18. https://doi.org/10.1371/journal.pone.0219888
Schultz, T. R., Schmidt, C. T., & Stichter, J. P. (2011). A review of parent education programs for parents of children with autism spectrum disorders. Focus on Autism and Other Developmental Disorders, 26(2), 96–104. https://doi.org/10.1177/1088357610397346
Schwarzer R., & Jerusalem, M. (1995). Generalized Self-Efficacy scale. In J. Weinman, S. Wright, & M. Johnston eds, Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35–37). Windsor, UK: NFER-NELSON
Selvakumar, N., & Panicker, A. S. (2020). Stress and coping styles in mothers of children with autism spectrum disorder. Indian Journal of Psychological Medicine, 42(3), 225–232. https://doi.org/10.4103/IJPSYM.IJPSYM_333_19
Sevigny, P. R., & Loutzenhiser, L. (2009). Predictors of parenting self-efficacy in mothers and fathers of toddlers. Child: Care, Health and Development, 36(2), 179–189. https://doi.org/10.1111/j.1365-2214.2009.00980.x
Shawler, P. M., & Sullivan, M. A. (2017). Parental stress, discipline strategies, and child behavior problems in families with young children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 32(2), 142–151. https://doi.org/10.1177/1088357615610114
Smidt, A., Balandin, S., Sigafoss, J., & Reed, V. A. (2009). The Kirkpatrick model: A useful tool for evaluation training outcomes. Journal of Intellectual & Developmental Disability, 34(3), 266–274. https://doi.org/10.1080/13668250903093125
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The Brief Resilience Scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15, 194–200. https://doi.org/10.1080/10705500802222972.
Sofronoff, K., Jahnel, D., & Sanders, M. (2011). Stepping Stones triple p seminars for parents of a child with a disability: A randomized controlled trial. Research in Developmental Disabilities, 32, 2253–2262. https://doi.org/10.1016/j.ridd.2011.07.046
Sommers-Flanagan, J. (2007). Single-session consultation for parents: A preliminary investigation. The Family Journal: Counseling and Therapy for Couples and Families, 15(1), 24–29. https://doi.org/10.1177/1066480706294045
Sung, J. Y., Mumper, E., & Schleider, J. L. (2021). Empowering anxious parents to manage child avoidance behaviors: Randomized control trial of a single-session intervention for parental accommodation. JMIR Mental Health, 8(7), e29538. https://doi.org/10.2196/29538
Suppo, J. L. (2012). Expanding training opportunities for parents of children with autism. [Doctoral Dissertation, 181, West Virginia University] The Research Repository@WVU. https://doi.org/10.33915/etd.181
Topp, C. W., Ostergaard, S. D., Sondergaard, S., & Bech, P. (2015). The WHO-5 Well-Being Index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84, 167–176. https://doi.org/10.1159/000376585
U.S. Department of Education (2019). Individuals with Disabilities Act, Section 1462 (C) (3). https://sites.ed.gov/idea/statute-chapter-33/subchapter-iv/part-b/1462/c
Uskin, E., & Undogar, D. (2010). The levels of stress, depression, and anxiety of parents of disabled children in Turkey. Disability and Rehabilitation, 32(23), 1917–1927. https://doi.org/10.3109/09638281003763804
van der Veek, S. M. C., Kraaij, V., & Garnefski, N. (2009). Cognitive coping strategies and stress in parents of children with down syndrome: A prospective study. Intellectual and Developmental Disabilities, 47(4), 295–306. https://doi.org/10.1352/1934-9556-47.4.295
Weiss, J., & Lunsky, Y. (2011). The Brief Family Distress Scale: A measure of crisis in caregivers of individuals with autism spectrum disorders. Journal of Child and Family Studies, 20(4), 521–528. https://doi.org/10.1007/s10826-010-9419-y
World Health Organization. (1998). The WHO-5 Well-being Index by the Psychiatric Research Unit. Hillerød, De: Mental Health Centre North Zaland. http://www.psykiatri-regionh.dk/who-5/Pages/default.aspx
Acknowledgements
This study was supported by the University of Cincinnati, Grant Development Center (#171221). The study was approved by the Youngstown State University Institutional Review Board prior to initiating.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
VanVoorhis, R.W., Miller, K.L. & Miller, S.M. A Single-Session Intervention Designed to Promote Resilience for Parents of Children with Disabilities. J Child Fam Stud 32, 2406–2418 (2023). https://doi.org/10.1007/s10826-023-02622-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02622-z