
Abstract
The accumulation of disruptive family events has a well-established association with adolescent mental health problems. In this study, we investigated whether grandparent involvement serves as a promotive or protective factor for psychological adjustment when adolescents face high levels of family adversity. The sample comprised 536 adolescents (aged 13–15 years) from two schools in Cape Town, South Africa. Data were collected using a self-report survey, and mental health was assessed by the Strengths and Difficulties Questionnaire. Structural Equation Modeling demonstrated that cumulative proximal family stress was associated with more emotional and conduct problems in adolescents, whereas grandparent involvement was associated with fewer peer and conduct problems and less hyperactivity. The results of a path analysis testing for interaction effects indicated that in high-adversity family environments, grandparent involvement only had a protective effect against peer problems for female adolescents. Nevertheless, grandparent involvement served as a promotive factor for the full sample, compensating for the negative psychological outcomes associated with family risk. The finding that grandparent involvement was associated with better adolescent mental health across all levels of family stress supports a multigenerational approach to intervention in which practitioners work across generations to foster individual, family and community resilience.
Highlights
-
We examined links between grandparent involvement and mental health in South African adolescents facing family adversity.
-
Family adversity was associated with more conduct and emotional problems in adolescents.
-
Grandparent involvement was associated with fewer conduct and peer problems and less hyperactivity in adolescents.
-
Grandparent involvement protected female adolescents in high-adversity family environments against peer problems.
-
Interventions aimed at supporting families and promoting adolescent mental health may benefit from including grandparents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
A recent trend in the study of child development has been to move away from researching only the parent–child dyad, to focus instead on the child as embedded within a larger family and social network (Levitt, 2012). Disruptions to family functioning from internal or external hazards generate stress for children, and threaten their development (Masten & Monn, 2015). At the same time, immediate and extended kin have the potential to support children in high-risk families (Luthar et al., 2015). In the present study, we investigated whether grandparent involvement is associated with beneficial psychological outcomes for adolescents facing cumulative proximal family-based adversity.
Adversity can be defined as an environmental event or condition associated with a high risk of psychopathology or negative outcomes (Luthar et al., 2015). When such risks coexist, they pose a greater threat to children’s well-being than any risk factor in isolation (Masten & Shaffer, 2006). The accumulation of negative or adverse life events has a well-established association with mental health problems in adolescence (Bøe et al., 2018). Composite risk indices predict psychological difficulties in youth even after controlling for preexisting symptoms (Grant et al., 2014).
The family remains the primary context of socialization for most adolescents, influencing both positive and negative outcomes (Masten & Shaffer, 2006). Family adversity—the accumulation of disruptive family events such as parental divorce or substance abuse—challenges adolescents’ adaptive capacities, and is linked to both internalizing and externalizing symptoms (Bakker et al., 2011, Buehler & Gerard, 2013). Even in the face of multiple stressors, however, some adolescents adapt well and do not develop adjustment problems.
The process whereby some young people display positive outcomes despite exposure to adversity is known as resilience. Resilience can be described broadly as successful adaption following significant threats or challenges to a system (Masten & Monn, 2015). Using a variable-focused approach, multivariate methods can be used to investigate two basic conceptual models of resilience theory. In a compensatory model, individual or environmental assets known as promotive factors counterbalance the negative effects of adversity. Statistically, compensatory effects are represented by significant main effects in a multivariate statistical analysis. On the other hand, a protective effect is detected statistically when a protective factor moderates (i.e., reduces) the effects of adversity on adjustment problems. In a protective effects model, a significant interaction effect indicates that a particular variable is associated with better outcomes under stressful conditions, but this same variable is not necessarily associated with better outcomes in low-stress circumstances (Zimmerman et al., 2013).
One of the variables that might promote resilience in adolescents exposed to family adversity is social support. Support from social network members appears to protect the individual from the negative effects of adversity by providing “emotional, self-enhancing, informational, and/or tangible resources” that may reduce perceptions of threat, enhance self-esteem and self-efficacy, and increase the use of effective coping strategies (Levitt, 2012, p. 366, Southwick et al., 2016). Family support appears to be particularly important for resilience to psychopathology, and has consistently been associated with fewer depressive symptoms in adolescents under stress (Pössel et al., 2018, Rueger et al., 2016). Support from significant non-parental adults has also been shown to improve adolescent psychosocial outcomes, but may not be able to compensate for a lack of support from parents (Sterrett et al., 2011).
Although teachers, friends and other peers have often been considered as sources of social support, grandparents have received less attention (Levitt, 2012). However, grandparent–adolescent relationships tend to remain affectionate and harmonious, even as parent–child conflict is increasing (Creasey & Kaliher, 1994). In decades to come, population ageing is likely to enhance the importance of grandparents still further. The global population of older persons is set to double by 2050, with a three-fold increase projected for sub-Saharan Africa (United Nations Department of Economic and Social Affairs (2019)).
Grandparent Involvement as a Promotive Factor
Grandparent involvement can be conceptualized along three dimensions: contact, involvement in caregiving, and providing support (Sadruddin et al., 2019). Although the quantity of grandparent–grandchild contact has little association with children’s well-being, evidence for the potential benefits of supportive social interactions with grandparents is growing (Smith & Wild, 2019). A link between grandparent involvement and prosocial outcomes in adolescents aged between 11 and 15 years has been observed in Israel (Attar-Schwartz & Khoury-Kassabri, 2016), South Africa (Wild, 2018) and the United States (US; Yorgason et al., 2011). Some studies have also found that greater emotional closeness to grandparents is associated with fewer internalizing and externalizing problems in preadolescent, early adolescent and late adolescent samples in Israel, the US, and the United Kingdom (UK) (Attar-Schwartz & Buchanan, 2018, Lussier et al., 2002, Ruiz & Silverstein, 2007). A main effects model of social support suggests that interactions with grandparents may confer general benefits for mental health by helping adolescents to regulate their emotions, and by providing a sense of stability and self-worth (Cohen & Wills, 1985, Rueger et al., 2016). However, positive associations between grandparent involvement and adolescent psychological outcomes have not been observed across all studies, and seem to depend in part on the gender and lineage of grandparents (Wild & Gaibie, 2014), household structure (Levetan & Wild, 2015), the way in which grandparent involvement is operationally defined (Smith & Wild, 2019) and the particular outcome being assessed. For example, previous studies conducted in the US and South Africa have found no association between grandparent involvement and adolescent substance use (Dunifon & Bajracharya, 2012; Profe & Wild, 2017).
Grandparent Involvement as a Protective Factor
Although some support has been found for a “main effects” model of grandparent involvement, theory and research on social support have been dominated by a stress-buffering hypothesis. From this perspective, social support is protective of mental health only—or primarily—in the presence of stress (Cohen & Wills, 1985). Elder and Conger (2000) suggest that grandparents may be superfluous for children in stable, nurturing families—they can reinforce existing family strengths, but have little independent influence. When faced with a family crisis, however, grandparent involvement can enhance children’s psychological adjustment.
A protective effects model is supported by Flouri et al. (2010) finding that closeness to grandparents moderated the association between a cumulative measure of stress and mental health problems in adolescents across England and Wales. Grandparent involvement has also been found to buffer British and American adolescents from the potential negative effects of specific family stressors such as maternal depression (Silverstein & Ruiz, 2006), parental substance use (Sheridan et al., 2011), and parental divorce and remarriage (Attar-Schwartz et al., 2009; Lussier et al., 2002; Ruiz & Silverstein, 2007). Support from grandparents can benefit children directly or indirectly, through enhancing parents’ behavior and well-being (Attar-Schwartz & Buchanan, 2018). However, a study of Malaysian adolescents found no evidence that grandparent involvement moderates the effects of adversity (Tan, 2018).
Two factors that may influence whether or not grandparent involvement has a protective effect are the timing of the stressful life events and the gender of the adolescent grandchild. Flouri et al. (2010) found that closeness to grandparents moderated the effects of recent or current stressors, but not those of more distal life events. There is also evidence that adolescent girls are more sensitive to interpersonal stressors and benefit more from social support than boys (Rudolph, 2002; Rueger et al., 2010). To date, the question of whether the protective effect of grandparent involvement differs according to the gender of the adolescent remains unanswered. However, analyzing data obtained from boys and girls separately is warranted in order to ensure that a lack of effect for boys does not mask an effect for girls.
The Present Study
Identifying protective and promotive factors is vital for understanding how to foster adolescent resilience in a context of adversity (Zimmerman et al., 2013). South African adolescents experience a high prevalence of mental health problems, reflecting a legacy of racial discrimination and material inequality (Das-Munshi et al., 2016). From 1948 to 1994, apartheid policies institutionalized racial segregation to benefit the White minority. Today, adolescents self-identifying as “Black” or “Colored” remain disproportionately affected by material disadvantage, violence and mental disorders (Das-Munshi et al., 2016). In South Africa, the term “Colored” is used to denote a group of people with mixed African, Asian and European ancestry, and a cultural identity distinct from that of the Black African majority.
Colonialism and apartheid entrenched a pattern of family disruption in South Africa that persists among historically disadvantaged groups (Budlender & Lund, 2011). Grandparents are an important source of care and support in South African families, particularly those identifying as Black or Colored (Budlender & Lund, 2011; Wild & Gaibie, 2014). However, empirical evidence on whether grandparent involvement can counteract adolescents’ exposure to family risk is lacking. Previous research investigating the association between grandparent involvement and adolescent mental health is equivocal. In addition, the extant literature fails to distinguish between family adversity and other environmental stressors, despite evidence that family stress and negative life events are independently associated with adolescent outcomes (Bøe et al., 2018). Important questions about other potential moderators, including adolescent gender and the broader cultural setting, also remain unanswered. This study was therefore designed to determine whether grandparent involvement is a promotive or protective factor for South African adolescents’ psychological wellbeing in the context of family adversity. The following hypotheses were tested:
-
1.
Family adversity will be positively associated with adolescents’ psychological difficulties.
-
2.
Grandparent involvement will be negatively associated with adolescents’ psychological difficulties.
-
3.
Grandparent involvement will moderate (weaken) the relationship between family adversity and adolescents’ psychological difficulties. Based on previous research (Rueger et al., 2010), we expect the hypothesized protective effect of grandparent involvement to be stronger for girls than for boys.
Method
Participants
The sample comprised 536 adolescents in grades 8 and 9 at two co-educational high schools in Cape Town, South Africa. One school was located in a working-class area, and the other in a middle-class suburb. The mean age of the participants was 13.94 years (SD = 0.70), and 58% were female. The majority of participants (90%) identified as Colored and 10% identified as Black African. Most adolescents (91%) lived with their mothers, 69% lived with their fathers, 66% lived with both parents, and 5% lived with stepparents. Nineteen percent of participants lived in three-generation households with at least one grandparent, and a further 3% lived with grandparents in skipped-generation households.
The researchers invited eight schools to participate in the study, using a combination of convenience and purposive sampling. First, we used a database provided by the Western Cape Education Department (WCED) to identify schools located within a manageable traveling distance from the researchers. We then approached those schools that served primarily Colored or Black African populations. The majority of Capetonians identify as Colored (43%) or Black African (39%; Statistics South Africa, 2012).
The principals of two of the eight schools approached (25%) consented to participate in the study, and all students in grades eight and nine at those schools were invited to take part. The original eligible sample comprised 722 adolescents, of whom two (0.3%) did not receive parental consent to participate. A total of 671 usable surveys were returned, yielding a 93% response rate. Because homogenous convenience samples produce less biased estimates with clearer generalizability than heterogeneous samples (Jager et al., 2017), we excluded participants from the final sample if they did not identify as Black African or Colored (n = 39) or were not between the ages of 13 years and 15 years (n = 45). Participants were also excluded if they had no living grandparents (n = 27), or returned questionnaires missing more than 20% of the key data (n = 24). This left a total sample size of 536 participants. The achieved sample size exceeded the minimum sample size of 470 participants which was estimated using the N:q rule (Jackson, 2003, Kline, 2016). The N:q rule states that the ratio between the sample size (N) and the number of parameters (q) should ideally be between 10:1 and 20:1.
Measures
Family adversity
Eight items from the Adverse Life Events Scale for children and adolescents (ALES; Tiet et al., 2001) were used to measure family adversity. The ALES includes 25 possible adverse life events in the parental, family, peer and community domains. Only those questions referring to adverse family events (e.g., “someone in the family died”) were used in the present study. Participants received a score ranging from 0 to 8, depending on whether or not they had experienced each adverse family event within the previous six months. Although the focus was on proximal family events, two of the items assessed potentially chronic stressors associated with a family member’s mental illness or substance use. The ALES was based on the Life Events Checklist (LEC; Coddington, 1972), which has satisfactory test–retest reliability (Brand & Johnson, 1982) and construct validity (Duggal et al., 2000).
Grandparent involvement
Adolescents were asked to report on the involvement of each of their living grandparents using an 11-item scale. Questions were based on a measure developed by Griggs et al. (2010), modified to ensure that the items were locally relevant and covered the six domains of grandparent involvement identified by Mueller and Elder (2003). Modifications were informed by a qualitative pilot study, and a quantitative pilot was conducted to test the questionnaire (Wild & Gaibie, 2014). A sample question is “How often does your grandparent help you by giving you advice or helping solve problems you have?”
Participants responded to each question using a three-point Likert scale ranging from 0 (“Not much”) to 2 (“A lot”), with possible total scores ranging from 0 to 22. If adolescents had more than one living grandparent, the score from the most involved grandparent was used. Involved grandparents tend to be closer to their grandchildren than less involved grandparents (Mueller & Elder, 2003), and close ties facilitate support-seeking (Kammrath et al., 2020). A previous study conducted with adolescents in South Africa found evidence for the scale’s reliability, with alpha coefficients ranging from 0.84 to 0.91 for each of the four possible grandparents (Wild & Gaibie, 2014). In the present study, Cronbach’s alpha was 0.87.
Psychological difficulties
The self-report version of the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) was used to measure adolescent psychological outcomes. The SDQ contains 25 items that are assessed using a three-point Likert scale. Response options for each statement range from 0 (“Not true”) to 2 (“Certainly true”), and five items are reverse coded.
The SDQ comprises five subscales. Four of these subscales assess psychological difficulties, namely hyperactivity/inattention, conduct problems, peer relationship problems and emotional problems. The emotional and peer items can be combined to form an “internalizing” subscale, whereas conduct problems and hyperactivity can be combined into an “externalizing” subscale (Goodman et al., 2010). The fifth subscale, which was not used in the present study, assesses prosocial behavior.
Goodman et al. (1998) demonstrated that the self-report version of the SDQ has acceptable internal consistency, with Cronbach’s alpha coefficients for individual subscales ranging from 0.61 for peer problems to 0.75 for emotional symptoms. The self-report SDQ has also been shown to have satisfactory test–retest reliability, as well as construct, discriminant and concurrent validity (Goodman et al., 1998, 2010). The SDQ has been used as a screening tool in many countries, including South Africa (De Vries et al., 2018). The Cronbach’s alpha coefficients in the present study were acceptable for emotional symptoms (0.67) and hyperactivity (0.66), but low for conduct problems (0.51) and peer relationship problems (0.47). Nevertheless, all four SDQ subscales had average interitem correlation coefficients (AICs) within the range of 0.15 and 0.50 recommended by Clark and Watson (2019) for scales that assess broad characteristics. Clark and Watson (2019) argue that AICs are superior to coefficient alphas as an index of internal consistency, as the latter are strongly affected by the number of items in a scale.
Procedure
The study was approved by a research ethics committee of the University of Cape Town, and by the WCED. Because the study involved minimal risk, passive parental consent procedures were used. A parent consent form was sent home with each adolescent prior to data collection, and parents were asked to return the form only if they did not consent to their child participating in the study. Parents who did not return the form were assumed to have provided consent.
On the day of data collection, the adolescents were given an assent form to complete. Both the consent and assent forms provided information about the study, explained that participation was voluntary, and indicated that adolescents could leave out certain questions or withdraw from the study at any time. Participants were also assured that their responses would be confidential and anonymous. Adolescents were informed that they could contact their school counselor if they were upset by any of the questions, and were provided with contact details for a free telephone counseling service.
Once parental consent and adolescent assent had been obtained, participants were given a survey pack and asked to complete it within a 50-minute period allotted by the schools. The students were asked to work alone, and seating was arranged so that their classmates’ responses were not visible. At least one researcher was present in the classroom and available to answer questions.
Analytic Strategy
Descriptive statistics and bivariate correlations were calculated for all numeric variables. Data were then analyzed using structural equation modeling (SEM) and path analysis (PA). The analysis was conducted using the lavaan package (Rosseel, 2012) for R Studio version 0.99.489. Missing data in the sample appeared to be missing at random, therefore the Maximum Likelihood method was used to estimate those missing data points (Kline, 2016). An alpha level of 0.05 was used for all analyses.
Structural equation model
A SEM was run to test hypotheses 1 and 2. There were six latent variables in this model, which is depicted in Fig. 1. Covariance terms were included between emotional and peer relationship problems (internalizing difficulties) and between conduct problems and hyperactivity/inattention (externalizing difficulties). The measurement models for each latent variable were tested using confirmatory factor analyses. If a measured variable did not load significantly on the latent variable and could justifiably be removed, it was dropped from the analysis. The modification indices for each path in the SEM were also calculated, and any paths where the index value was over 20.00 were entered into the model as correlated pairs. Following this, the overall fit of the model was determined using the minimum function chi-square test, comparative fit index (CFI), root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR). Recommended cut-offs that indicate a good fit are CFI ≥ 0.90, RMSEA ≤ 0.05 and SRMR < 0.08 (Kline, 2016). When fit indices disagreed, more weight was given to the RMSEA and SRMR. The chi-square statistic is almost invariably significant when the sample size exceeds 400 (Kenny, 2015), and the RMSEA has been deemed superior to the CFI in confirmatory, large-sample contexts (Rigdon, 1996).

Measurement and structural components evaluated in the SEM
Path analysis
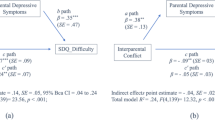
In order to test hypothesis 3, path analyses were conducted. A SEM could not be used to test this hypothesis because adding the interaction term to the model increased the number of parameters to such an extent that the size of the sample was not large enough for the model to converge. Therefore, only the structural model was tested using path analysis. This model can be seen in Fig. 2. The interaction term was computed by multiplying the total scores of the grandparent involvement scale and the family adversity scale. The path analysis was conducted for both boys and girls together (n = 536), boys only (n = 221) and girls only (n = 310). The overall fit of the models was evaluated using the minimum function chi-square test, CFI, RMSEA and SRMR.

Structural model for estimating paths in path analysis
Results
Descriptive Statistics
Descriptive statistics (means, standard deviations and ranges) for the measures are displayed in Table 1. The mean percentage of adolescents endorsing each adverse event was 15%. Girls reported more emotional symptoms (M = 4.22, SD = 2.27) than boys (M = 2.85, SD = 2.07), t(534) = − 7.11, p < 0.001, d = −0.62, 95% CI [−0.80, −0.45]. There were no other gender differences in psychological difficulties.
Correlations
The correlations presented in Table 2 indicate that there was a statistically significant positive relationship between family adversity and all four psychological difficulty subscales. The effect size of the relationship between family adversity and conduct problems was medium, whereas family adversity had small effects on emotional symptoms, hyperactivity/inattention and peer relationship problems. There was a significant negative relationship between grandparent involvement and all the psychological problem variables other than emotional symptoms, with all effect sizes being small in magnitude.
Structural Equation Model
An analysis of the measurement model’s fit statistics indicated that the model was an adequate fit for the data: XM2 (650) = 1136.08, p < 0.05, CFI = 0.86, RMSEA = 0.04, SRMR = 0.05. Modification indices indicated that the model could be improved by adding covariance terms between items 3 and 4 and items 7 and 8 on the grandparent involvement scale. The modified model’s fit statistics improved: XM2 (648) = 1074.68, p < 0.05, CFI = 0.88, RMSEA = 0.04, SRMR = 0.05. This modified model fitted the sample data significantly better than the unmodified model and therefore it was retained, ∆X2 (2) = 74.68, p < 0.05.
The fit statistics for the path model indicated that the model adequately fit the data: XM2 (648) = 1060.84, p < 0.05, CFI = 0.88, RMSEA = 0.04, and SRMR = 0.05. The path coefficients (Table 3) indicated that there was no relationship between family adversity and grandparent involvement. Family adversity was significantly positively associated with conduct problems and emotional symptoms, but was not significantly associated with hyperactivity/inattention and peer relationship problems. There was a significant negative association between grandparent involvement and all psychological difficulties except emotional symptoms. Family adversity and grandparent involvement were associated with the adolescent outcomes in opposite directions, supporting a compensatory model of grandparent involvement.
Path Analysis
The fit statistics for the path analysis model are presented in Table 4. The models for boys and for the full sample fitted the data well. The chi-square and RMSEA indicated that the model for girls provided a poor fit to the data, but the CFI and SRMR indicated a good fit. The Normed Fit Index (NFI) was therefore also calculated for the female sample and indicated an acceptable fit (0.94).
Table 5 shows the path coefficients between the interaction terms and psychological outcomes for boys, girls, and the full sample. These pathways were singled out because they represent the potential protective effect of grandparent involvement. The path coefficients indicated that grandparent involvement moderated the relationship between family adversity and peer problems for girls only, β = − 0.14, p < 0.05. Graphical inspection of the interaction (Online Resource 1) indicated that when grandparent involvement was high (≥20), there was no relationship between family adversity and peer problems. However, the relationship between family adversity and peer problems became stronger as grandparent involvement decreased. None of the other interaction terms was significantly associated with psychological difficulties.
Discussion
The primary aim of this study was to determine whether, under conditions of family adversity, grandparent involvement could act as a promotive or protective factor against psychological difficulties in South African adolescents. The majority of our participants had experienced few adverse family events and reported similar levels of psychological difficulties to a representative sample of South African adolescents (De Vries et al., 2018). Nevertheless, the mean percentage of adolescents endorsing each adverse event (15%) was higher than that reported by Tiet et al. (2001) for adolescents from four US sites (10%). In addition, participants (particularly girls) reported more emotional symptoms than their British, Chinese and Australian counterparts (De Vries et al., 2018). The results were largely consistent with a compensatory (main effects) model of resilience in which the positive consequences of grandparent involvement counteract the negative effects of adversity. However, the findings provided little support for a protective factors (moderation) model in which grandparent involvement lessons the effects of risk in an interactive manner.
In partial support of hypothesis 1, proximal family adversity was positively associated with conduct problems and emotional symptoms in adolescents. The effect size of the relationship between family adversity and conduct problems was moderate, whereas that between family adversity and emotional symptoms was small. Family adversity was also significantly related to peer relationship problems and hyperactivity in the bivariate correlations, but these relationships fell just short of significance (p < 0.07) in the SEM. These findings are in line with previous research. Studies conducted in Europe and the US have demonstrated that family adversity is modestly but significantly associated with both internalizing and externalizing mental health problems in adolescents (Bakker et al., 2011; Bøe et al., 2018; Buehler & Gerard, 2013).
The results also provided general support for the second study hypothesis. Grandparent involvement had a direct and negative relationship with adolescents’ conduct problems, hyperactivity/inattention and peer relationship problems, but was not significantly associated with emotional symptoms. In contrast to the present study, research in the UK and Israel has found a significant link between grandparent involvement and fewer emotional problems in adolescents (Attar-Schwartz & Khoury-Kassabri, 2016; Attar-Schwartz et al., 2009). Closeness to grandparents was also associated with lower levels of hyperactivity in the Israeli sample, but not with conduct or peer problems (Attar-Schwartz & Khoury-Kassabri, 2016). The quality and implications of grandparent involvement are likely to vary depending on the broader cultural and family context (Attar-Schwartz & Buchanan, 2018). In South Africa, the violence, racism and socioeconomic disadvantage associated with adolescent emotional disorders may strain family relationships and undermine the availability and impact of social support (Stansfeld et al., 2017). Emotional problems may also reflect the lasting impact of distal stressors that are not buffered by grandparent involvement (Flouri et al., 2010). At the same time, the SDQ may fail to distinguish adequately between emotional and peer problems, or between conduct problems and hyperactivity, in community samples (Goodman et al., 2010).
Despite certain discrepancies, studies in diverse settings concur that grandparent involvement is associated with fewer adolescent internalizing and externalizing problems (Attar-Schwartz & Buchanan, 2018). The present results suggest that support from grandparents is associated with more positive adolescent adjustment independent of the level of family adversity. These findings are consistent with a compensatory model of resilience in which resources offset exposure to risk through an opposite effect on outcomes. Although the effect sizes obtained in this study were small, they are similar in magnitude to the relationship between antihistamine use and relief from hay fever symptoms (Funder & Ozer, 2019).
The third hypothesis proposed that grandparent involvement would moderate the relationship between family adversity and adolescents’ psychological difficulties, and that this moderating effect would be stronger for girls than for boys. In contrast to Flouri et al. (2010) but consistent with Tan (2018), we found no evidence that grandparent involvement reduced the association between family adversity and psychological difficulties for the full sample, or for boys. For girls, however, the association between family adversity and peer relationship problems was weaker when grandparent involvement was high. Previous research has found that adolescent girls experience more stress in peer relationships than boys, and that girls may be particularly susceptible to depression in the face of interpersonal stress (Rudolph, 2002). However, adolescent girls are also more likely to seek and utilize social support than boys, particularly when coping with a peer argument (Eschenbeck et al., 2007). Support from family and other adults, in turn, appears to be particularly beneficial for girls (Cohen & Wills, 1985; Rueger et al., 2010). This may help to explain why grandparent involvement helped to protect girls, but not boys, from the negative effects of family adversity on peer relationship problems.
Evidence that grandparent involvement may counteract some of the risks associated with family adversity supports a multigenerational approach to intervention in which practitioners work across generations to support individuals, families and communities (Fredriksen-Goldsen & Bonifas, 2005). Many South African schools encourage grandparent involvement by holding “Grandparents Days,” and multigenerational housing estates are a growing trend. In the US, “foster grandparent” programs in which older adults receive a stipend to provide care and companionship to high-risk youth have been positively evaluated (Smith & Wild, 2019). Interventions for grandparents providing care to children have also shown promising results, although more rigorous research is needed to confirm their efficacy (Kirby, 2015). There are numerous influences on adolescent mental health, and it would be unrealistic to expect grandparent involvement to predict more than a small proportion of the variance. Yet small effects may accrue over time, with implications for adolescents’ adjustment in the longer term (Funder & Ozer, 2019).
When interpreting the results of the present study, there are certain limitations that warrant consideration. First, we inferred resilience based on low levels of psychological difficulties, but did not assess positive adaptation directly. Including instruments specifically designed to measure resilience would add value to subsequent studies. Second, this study made use of a cross-sectional design, which restricts the extent to which causality can be inferred. Future research would benefit from longitudinal designs, which are better able to determine the direction of effects. A third shortcoming of the study is that all the data were obtained from adolescents’ self-reports. Single source bias, and the clustering of students in classes within schools, can inflate correlations and increase the possibility of obtaining spurious results.
Another limitation of the present study is that using only the score for the most involved grandparent overlooks the possible impact of several grandparents on adolescent outcomes. In addition, household structure and the quality of the parent-adolescent and parent–grandparent relationships were not taken into account. Grandmother and grandfather involvement may have different associations with adolescent well-being (Wild, 2018). In addition, the strength of associations between grandparent involvement and adolescent mental health has been found to vary depending on characteristics of the broader family system in which the grandparent–grandchild relationship is embedded (Attar-Schwartz & Buchanan, 2018; Ruiz & Silverstein, 2007).
The findings of this research should also not be generalized beyond the limited age range assessed. In the US, for example, friends increasingly supplant grandparents in adolescents’ affections (Antonucci et al., 2010). It is also important to note that the sample for this study was composed predominantly of Colored adolescents from two schools, and is not representative of the South African population. Black African adolescents—who are at greatest risk of material disadvantage and mental disorders (Das-Munshi et al., 2016)—were underrepresented in our study.
Despite these limitations, the results of the present study add to the growing body of international literature indicating that grandparent involvement serves as a promotive or protective resource for adolescents (e.g., Attar-Schwartz et al., 2009; Flouri et al., 2010). Minimal evidence was found to suggest that grandparent involvement plays a unique role in high-adversity family contexts. However, grandparent involvement was generally associated with better psychological adjustment across all levels of family risk. In South Africa, grandparents’ important role in childrearing is increasingly acknowledged. Nevertheless, grandparents have no legal right of access to their grandchildren, and remain largely invisible on the policy agenda. Our findings support a growing body of evidence indicating that grandparent involvement is a key compensatory resource for adolescents at risk. They suggest the potential benefits of including grandparents in interventions aimed at strengthening families and promoting adolescent mental health.
References
Antonucci, T. C., Akiyama, H., & Takahashi, K. (2010). Attachment and close relationships across the life span. Attachment & Human Development, 6(4), 353–370. https://doi.org/10.1080/1461673042000303136.
Attar-Schwartz, S., & Buchanan, A. (2018). Grandparenting and adolescent well-being: Evidence from the UK and Israel. Contemporary Social Science, 13(2), 219–231. https://doi.org/10.1080/21582041.2018.1465200.
Attar-Schwartz, S., & Khoury-Kassabri, M. (2016). The moderating role of cultural affiliation in the link between emotional closeness to grandparents and adolescent adjustment difficulties and prosocial behavior. American Journal of Orthopsychiatry, 86, 564–572. https://doi.org/10.1037/ort0000195.
Attar-Schwartz, S., Tan, J. P., Buchanan, A., Flouri, E., & Griggs, J. (2009). Grandparenting and adolescent adjustment in two-parent biological, lone parent, and step-families. Journal of Family Psychology, 23(1), 67–75. https://doi.org/10.1037/a0014383.
Bakker, M. P., Ormel, J., Verhulst, F. C., & Oldehinkel, A. J. (2011). Adolescent family adversity and mental health problems: The role of adaptive self-regulation capacities. The TRAILS Study. Journal of Abnormal Child Psychology, 39(3), 341–350. https://doi.org/10.1007/s10802-010-9470-6.
Bøe, T., Serlachius, A. S., Sivertsen, B., Petrie, K. J., & Hysing, M. (2018). Cumulative effects of negative life events and family stress on children’s mental health: The Bergen Child Study. Social Psychiatry and Psychiatric Epidemiology, 53(1), 1–9. https://doi.org/10.1007/s00127-017-1451-4.
Brand, A. H., & Johnson, J. H. (1982). Note on reliability of the Life Events Checklist. Psychological Reports, 50(3, Pt 2), 1274. https://doi.org/10.2466/pr0.1982.50.3c.1274.
Budlender, D., & Lund, F. (2011). South Africa: A legacy of family disruption. Development & Change, 42(4), 925–946. https://doi.org/10.1111/j.1467-7660.2011.01715.x.
Buehler, C., & Gerard, J. M. (2013). Cumulative family risk predicts increases in adjustment difficulties across early adolescence. Journal of Youth and Adolescence, 42(6), 905–920. https://doi.org/10.1007/s10964-012-9806-3.
Clark, L. A., & Watson, D. (2019). Constructing validity: New developments in creating objective measuring instruments. Psychological Assessment, 31(12), 1412–1427. https://doi.org/10.1037/pas0000626.
Coddington, R. D. (1972). The significance of life events as etiologic factors in the diseases of children: II. A study of a normal population. Journal of Psychosomatic Research, 16(3), 205–213. https://doi.org/10.1016/0022-3999(72)90045-1.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. https://doi.org/10.1037/0033-2909.98.2.310.
Creasey, G. L., & Kaliher, G. (1994). Age differences in grandchildren’s perceptions of relations with grandparents. Journal of Adolescence, 17(5), 411–426. https://doi.org/10.1006/jado.1994.1036.
Das-Munshi, J., Lund, C., Mathews, C., Clark, C., Rothon, C., & Stansfeld, S. (2016). Mental health inequalities in adolescents growing up in post-apartheid South Africa: Cross-sectional survey, SHaW study. PLoS ONE, 11(5), e0154478 https://doi.org/10.1371/journal.pone.0154478.
De Vries, P. J., Davids, E. L., Mathews, C., & Aarø, L. E. (2018). Measuring adolescent mental health around the globe: Psychometric properties of the self-report Strengths and Difficulties Questionnaire in South Africa, and comparison with UK, Australian and Chinese data. Epidemiology and Psychiatric Sciences, 27(4), 369–380. https://doi.org/10.1017/S2045796016001207.
Duggal, S., Malkoff-Schwartz, S., Birmaher, B., Anderson, B. P., Matty, M. K., Houck, P. R., Bailey-Orr, M., Williamson, D. E., & Frank, E. (2000). Assessment of life stress in adolescents: Self-report versus interview methods. Journal of the American Academy of Child & Adolescent Psychiatry, 39(4), 445–452. https://doi.org/10.1097/00004583-200004000-00013.
Dunifon, R., & Bajracharya, A. (2012). The role of grandparents in the lives of youth. Journal of Family Issues, 33(9), 1168–1194. https://doi.org/10.1177/0192513X12444271.
Elder, G. H., Jr., & Conger, R. D. (2000). Children of the land: Adversity and success in rural America. University of Chicago Press.
Eschenbeck, H., Kohlmann, C.-W., & Lohaus, A. (2007). Gender differences in coping strategies in children and adolescents. Journal of Individual Differences, 28(1), 18–26. https://doi.org/10.1027/1614-0001.28.1.18.
Flouri, E., Buchanan, A., Tan, J. P., Griggs, J., & Attar-Schwartz, S. (2010). Adverse life events, area socio-economic disadvantage, and adolescent psychopathology: The role of closeness to grandparents in moderating the effect of contextual stress. Stress, 13(5), 402–412. https://doi.org/10.3109/10253891003671690.
Fredriksen-Goldsen, K. I., & Bonifas, R. (2005). Multigenerational practice and curricular infusion. Journal of Intergenerational Relationships, 3(3), 83–99. https://doi.org/10.1300/J194v03n03_06.
Funder, D. C., & Ozer, D. J. (2019). Evaluating effect size in psychological research: Sense and nonsense. Advances in Methods and Practices in Psychological Science, 2(2), 156–168. https://doi.org/10.1177/2515245919847202.
Goodman, A., Lamping, D. L., & Ploubidis, G. B. (2010). When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers and Children. Journal of Abnormal Child Psychology, 38(8), 1179–1191. https://doi.org/10.1007/s10802-010-9434-x.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Goodman, R., Meltzer, H., & Bailey, V. (1998). The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. European Child and Adolescent Psychiatry, 7(3), 125–130. https://doi.org/10.1007/s007870050057.
Grant, K. E., McMahon, S. D., Carter, J. S., Carleton, R. A., Adam, E. K., & Chen, E. (2014). The influence of stressors on the development of psychopathology. In Lewis, M. & Rudolph, K. (Eds), Handbook of developmental psychopathology (pp. 205–223). Springer. https://doi.org/10.1007/978-1-4614-9608-3_11.
Griggs, J., Tan, J. P., Buchanan, A., Attar‐Schwartz, S., & Flouri, E. (2010). ‘They’ve always been there for me’: Grandparental involvement and child well‐being. Children & Society, 24(3), 200–214. https://doi.org/10.1111/j.1099-0860.2009.00215.x.
Jackson, D. L. (2003). Revisiting sample size and number of parameter estimates: Some support for the N:q hypothesis. Structural Equation Modeling, 10(1), 128–141. https://doi.org/10.1207/S15328007SEM1001_6.
Jager, J., Putnick, D. L., & Bornstein, M. H. (2017). More than just convenient: The scientific merits of homogeneous convenience samples. Monographs of the Society for Research in Child Development, 82(2), 13–30. https://doi.org/10.1111/mono.12296.
Kammrath, L. K., Armstrong, III, B. F., Lane, S. P., Francis, M. K., Clifton, M., McNab, K. M., & Baumgarten, O. M. (2020). What predicts who we approach for social support? Tests of the attachment figure and strong ties hypotheses. Journal of Personality and Social Psychology, 118(3), 481–500. https://doi.org/10.1037/pspi0000189.
Kenny, D. A. (2015). Measuring model fit. http://davidakenny.net/cm/fit.htm.
Kirby, J. N. (2015). The potential benefits of parenting programs for grandparents: Recommendations and clinical implications. Journal of Child and Family Studies, 24(11), 3200–3212. https://doi.org/10.1007/s10826-015-0123-9.
Kline, R. B. (2016). Principles and practice of structural equation modeling (4th ed.). The Guilford Press.
Levetan, J. L., & Wild, L. G. (2015). The implications of maternal grandmother coresidence and involvement for adolescent adjustment in South Africa. International Journal of Psychology, 51(5), 356–365. https://doi.org/10.1002/ijop.12178.
Levitt, M. J. (2012). Social networks. In Mayes, L. C. & Lewis, M. (Eds), The Cambridge handbook of environment in human development (pp. 359–384). Cambridge University Press. https://doi.org/10.1017/CBO9781139016827.
Lussier, G., Deater-Deckard, K., Dunn, J., & Davies, L. (2002). Support across two generations: Children’s closeness to grandparents following parental divorce and remarriage. Journal of Family Psychology, 16(3), 363–376. https://doi.org/10.1037/0893-3200.16.3.363.
Luthar, S. S., Crossman, E. J., & Small, P. J. (2015). Resilience and adversity. In Lerner, R. M. & Lamb, M. E. (Eds), Handbook of child psychology and developmental science (7th ed., Vol. III, pp. 247–286). John Wiley & Sons.
Masten, A. S., & Monn, A. R. (2015). Child and family resilience: A call for integrated science, practice, and professional training. Family Relations, 64(1), 5–21. https://doi.org/10.1111/fare.12103.
Masten, A. S., & Shaffer, A. (2006). How families matter in child development: Reflections from research on risk and resilience. In Clarke-Stewart, A. & Dunn, J. (Eds), Families count: Effects on child and adolescent development (pp. 5–25). Cambridge University Press. https://doi.org/10.1017/CBO9780511616259.002.
Mueller, M. M., & Elder, G. H. (2003). Family contingencies across the generations: Grandparent–grandchild relationships in holistic perspective. Journal of Marriage and Family, 65(2), 404–417. https://doi.org/10.1111/j.1741-3737.2003.00404.x.
Pössel, P., Burton, S. M., Cauley, B., Sawyer, M. G., Spence, S. H., & Sheffield, J. (2018). Associations between social support from family, friends, and teachers and depressive symptoms in adolescents. Journal of Youth and Adolescence, 47(2), 398–412. https://doi.org/10.1007/s10964-017-0712-6.
Profe, W., & Wild, L. G. (2017). Mother, father, and grandparent involvement: Associations with adolescent mental health and substance use. Journal of Family Issues, 38(6), 776–797. https://doi.org/10.1177/0192513X15583069.
Rigdon, E. E. (1996). CFI versus RMSEA: A comparison of two fit indexes for structural equation modeling. Structural Equation Modeling: A Multidisciplinary Journal, 3, 369–379. https://doi.org/10.1080/10705519609540052.
Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36. https://doi.org/10.18637/jss.v048.i02.
Rudolph, K. D. (2002). Gender differences in emotional responses to interpersonal stress during adolescence. Journal of Adolescent Health, 30(4, Suppl), 3–13. https://doi.org/10.1016/S1054-139X(01)00383-4.
Rueger, S. Y., Malecki, C. K., & Demaray, M. K. (2010). Relationship between multiple sources of perceived social support and psychological and academic adjustment in early adolescence: Comparisons across gender. Journal of Youth and Adolescence, 39(1), 47–61. https://doi.org/10.1007/s10964-008-9368-6.
Rueger, S. Y., Malecki, C. K., Pyun, Y., Aycock, C., & Coyle, S. (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychological Bulletin, 142(10), 1017–1067. https://doi.org/10.1037/bul0000058.
Ruiz, S. A., & Silverstein, M. (2007). Relationships with grandparents and the emotional well-being of late adolescent and young adult grandchildren. Journal of Social Issues, 63(4), 793–808. https://doi.org/10.1111/j.1540-4560.2007.00537.x.
Sadruddin, A. F. A., Ponguta, L. A., Zonderman, A. L., Wiley, K. S., Grimshaw, A., & Panter-Brick, C. (2019). How do grandparents influence child health and development? A systematic review. Social Science & Medicine, 239, Article 112476. https://doi.org/10.1016/j.socscimed.2019.112476.
Sheridan, K., Haight, W. L., & Cleeland, L. (2011). The role of grandparents in preventing aggressive and other externalizing behavior problems in children from rural, methamphetamine-involved families. Children and Youth Services Review, 33(9), 1583–1591. https://doi.org/10.1016/j.childyouth.2011.03.023.
Silverstein, M., & Ruiz, S. (2006). Breaking the chain: How grandparents moderate the transmission of maternal depression to their grandchildren. Family Relations, 55(5), 601–612. https://doi.org/10.1111/j.1741-3729.2006.00429.x.
Smith, P. K., & Wild, L. G. (2019). Grandparenting. In M. H. Bornstein (Ed.), Handbook of parenting: Vol. 3. Being and becoming a parent (3rd ed., pp. 232–270). Routledge. https://doi.org/10.4324/9780429433214.
Southwick, S. M., Sippel, L., Krystal, J., Charney, D., Mayes, L., & Pietrzak, R. (2016). Why are some individuals more resilient than others: The role of social support. World Psychiatry, 15(1), 77–79. https://doi.org/10.1002/wps.20282.
Stansfeld, S. A., Rothon, C., Das-Munshi, J., Mathews, C., Adams, A., Clark, C., & Lund, C. (2017). Exposure to violence and mental health of adolescents: South African Health and Well-being Study. BJPsych Open, 3(5), 257–264. https://doi.org/10.1192/bjpo.bp.117.004861.
Statistics South Africa. (2012). Census 2011 municipal report – Western Cape (Report No. 03-01-49). http://www.statssa.gov.za/census/census_2011/census_products/WC_Municipal_Report.pdf.
Sterrett, E. M., Jones, D. J., McKee, L. G., & Kincaid, C. (2011). Supportive non-parental adults and adolescent psychosocial functioning: Using social support as a theoretical framework. American Journal of Community Psychology, 48(3-4), 284–295. https://doi.org/10.1007/s10464-011-9429-y.
Tan, J.-P. (2018). Do grandparents matter? Intergenerational relationships between the closest grandparents and Malaysian adolescents. Contemporary Social Science, 13(2), 246–260. https://doi.org/10.1080/21582041.2018.1424931.
Tiet, Q. Q., Bird, H. R., Hoven, C. W., Moore, R., Wu, P., Wicks, J., Jensen, P. S., Goodman, S., & Cohen, P. (2001). Relationship between specific adverse life events and psychiatric disorders. Journal of Abnormal Child Psychology, 29(2), 153–164. https://doi.org/10.1023/A:1005288130494.
United Nations Department of Economic and Social Affairs, Population Division. (2019). World population ageing 2019: Highlights. https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf.
Westwood, S. A. (2016). Associations between grandparental involvement and psychological outcomes in adolescents facing family adversity. [Master’s thesis, University of Cape Town]. OpenUCT. https://open.uct.ac.za/handle/11427/20622.
Wild, L. G. (2018). Grandparental involvement and South African adolescents’ emotional and behavioural health: A summary of research findings. Contemporary Social Science, 13(2), 232–245. https://doi.org/10.1080/21582041.2017.1422536.
Wild, L. G., & Gaibie, F. (2014). Grandparental involvement and South African adolescents’ psychological well-being. Journal of Intergenerational Relationships, 12(4), 425–441. https://doi.org/10.1080/15350770.2014.961871.
Yorgason, J. B., Padilla‐Walker, L., & Jackson, J. (2011). Nonresidential grandparents’ emotional and financial involvement in relation to early adolescent grandchild outcomes. Journal of Research on Adolescence, 21(3), 552–558. https://doi.org/10.1111/j.1532-7795.2010.00735.x.
Zimmerman, M. A., Stoddard, S. A., Eisman, A. B., Caldwell, C. H., Aiyer, S. M., & Miller, A. (2013). Adolescent resilience: Promotive factors that inform prevention. Child Development Perspectives, 7(4), 215–220. https://doi.org/10.1111/cdep.12042.
Author information
Authors and Affiliations
Contributions
This article is based on the dissertation completed by Sarah A. Yang (née Westwood, 2016). Both authors made substantial contributions to the content of the manuscript. Sarah A. Yang contributed to the data collection, performed the data analysis, and wrote the first draft. Lauren G. Wild conceptualized and designed the study, prepared the materials, and revised and edited the final draft. Both authors approved the submitted manuscript. The authors would like to thank Professor Colin Tredoux, who provided guidance on the statistical analyses, and Jessica Levetan, Katharina Keck, Bianca Burridge and Wade Profe, who helped with the data collection.
Funding
The financial assistance of the South African National Research Foundation (NRF) towards Mrs Yang’s research is hereby acknowledged. Opinions expressed and conclusions arrived at are those of the authors and are not necessarily to be attributed to the NRF. Dr Wild received financial support for this research from an International Society for the Study of Behavioral Development (ISSBD) Developing Country Fellowship and a Carnegie Research Development Grant.
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics Approval
Approval was obtained from a research ethics committee of the University of Cape Town and from the Western Cape Education Department. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Participation was voluntary, and all participants provided informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
Yang, S.A., Wild, L.G. Associations Between Grandparent Involvement and Psychological Difficulties in Adolescents Facing Family Adversity. J Child Fam Stud 31, 1489–1500 (2022). https://doi.org/10.1007/s10826-021-02223-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-021-02223-8