
Abstract
Approximately 20% of adolescents develop depressive symptoms. Family, friends, and teachers are crucial sources of social support for adolescents, but it is unclear whether social support impacts adolescents directly (principle-effect model) or by moderating the effect of stress (stress-buffer model) and whether each source of social support remains meaningful when their influence is studied simultaneously. To help fill this gap, we followed 1452 Australian students (average age at enrollment = 13.1, SD = 0.5; range: 11–16 years; 51.9% female) for 5 years. Based on our findings, each source of support is negatively related to depressive symptoms one year later when studied independently but when combined, only family and teacher support predicted depressive symptoms. Family support in all grades and teacher support in grade 8 to 10 but not in grade 11 directly impacted adolescent depressive symptoms 1 year later. Family support in grades 8 and 11 also buffered against the negative impact of stress on depressive symptoms one year later. Based on the unexpected findings, the most important limitations seem to be that the used instruments do not allow for a separation of different groups of friends (e.g., classmates, same-gender peers, romantic partners), types of social support, and stress. In addition, the high, nonrandom attrition rate with adolescents reporting less social support, more stressful events, a higher frequency of depressive symptoms, and/or being of Torres Strait Islander or Aboriginal background limits the generalizability of our findings. Summarized, our findings demonstrate that adolescents facing stress might benefit more from family support compared to their peers without stressful life events and that friends may have a weaker presence in adolescent lives than expected.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Previous research has shown that approximately 20% of girls and 7% of boys develop depressive symptoms before the end of their adolescent years (Angold et al. 2002; Twenge and Nolen-Hoeksema 2002), resulting in a total treatment cost of $5 billion in the U.S. in 2013 alone (Bui et al. 2017). Adolescents who experience subsyndromal or major depression have an increased risk for developing major depressive disorders in adulthood (Patel et al. 2007). In fact, about 27% of individuals experience their first major depressive episode during childhood or adolescence (Kessler et al. 2012). Empirical findings suggest that adolescent depressive symptoms are associated with interpersonal distress, low self-efficacy, suicidality (Stewart et al. 2002), social and behavioral problems (McClure et al. 1997), and substance use and abuse (Patel et al. 2007). Further, depression in adolescence is associated with decreased quality of life, poor to severe functional impairment, and serious emotional disturbances (Kessler et al. 2012). A recent study found that students demonstrated more school absences due to depression, exceeding that caused by ADHD, anxiety, and conduct disorder (Lawrence et al. 2015). Based on the high prevalence and detrimental long-term consequences of adolescent depression, it is clear that a better understanding of factors influencing the development of depression in youth is crucial.
Social Support and Depressive Symptoms in Adolescents
Bronfenbrenner’s bioecological theory (1986) is a useful model guiding the search for etiological factors relevant to the onset of depression. The model emphasizes how social influences can strongly impact one’s development, especially during a period of development in which the prevalence of depression increases (National Institute of Mental Health 2013). Bronfenbrenner and Morris (2006) reported that social influences relevant to depression can stem from an array of sources organized into five environmental systems: the microsystem (individuals), mesosystem (institutions), exosystem (society), macrosystem (culture), and chronosystem (time). As adolescents spend nearly all of their time with family, friends, and teachers (United States Department of Health and Human Services 2016), these groups are the three main sources of social influence that make up the microsystem (Bronfenbrenner 1986; Bronfenbrenner and Morris 2006). This is supported by a growing body of empirical literature that points to the positive impact social support has on depression in adolescence. Rueger et al. 2016 summarized and integrated this research in their recent meta-analysis. The authors identified 342 studies with a total of 273,430 participants and found family, friend, and teacher support to be significantly related to depressive symptoms, a finding upheld both cross-sectionally and longitudinally. However, many of the included studies did not examine the associations of all three sources of social support on depression within the same study, and Rueger et al. (2016) did not separately analyze the few studies that did examine all three sources. Doing so seems pertinent as it is possible that social support from different sources prevents depressive symptoms in a similar way. Thus, it could be expected that social support from multiple sources is not more beneficial than social support from one source. If this is the case, all three sources of support might appear relevant throughout adolescence when studied independently, yet it is possible that one or more sources of support may become irrelevant when all three sources are examined at once. Moreover, which source of support is most beneficial might change during adolescence.
The few studies that investigate the relations of all three sources of social support with depression within the same analysis seem to point to different patterns depending on the age of the adolescents, further supporting the considerations above. McMahon et al. (2013) found in their study with 10–15 year olds that when ratings from all three sources of support were included in a single statistical model, only family support significantly predicted depressive symptoms. However, a similar study with 15–18 year olds found that all three sources of social support were significantly associated with depressive symptoms (Colarossi and Eccles 2003). Thus, based on these two studies, one might conclude that support from friends and teachers become more important in late adolescence.
While these are only two studies, this seeming increase of importance of social support from friends and teachers is consistent with other empirical findings showing that non-parental adults and peers become important sources of social support in the beginning of middle childhood, and same-gender peers become more important during the transition into early adolescence (Buhrmester 1996; Levitt et al. 1993). Then, in late adolescence, romantic partners become increasingly more relevant sources of social support (Collins and Laursen 2004; Meeus et al. 2007). Thus, it makes sense that family remains the only relevant source of social support in 5 to 10th graders when all sources are considered simultaneously, while all other sources are relevant for 10 to 12th graders. However, this conclusion is based on only a few studies, none of which conducted a more fine-grained examination to identify when changes regarding primary sources of support truly occur.
The limited research examining social support from all three sources within the same statistical model is problematic, as this seems important in order to better understand the influence each has on the development of depressive symptoms. Consequently, it is warranted that a study (a) examines each source of support, controlling for the other sources of support, spanning the entirety of adolescence and (b) explore potential changes in the relevance of each source of social support throughout high school.
Principle-Effect and Stress-Buffer Model
Throughout the literature examining the association between social support and depressive symptomatology, two theoretical models have been established: the principle-effect model (Dumont and Provost 1999) and the stress-buffer model (Cohen and Willis 1985). The principle-effect model, which is a main effect model, asserts that social support has an equally positive impact on individuals regardless of stressful life situations. There is research to support a main effect between social support and symptoms of depression in adolescence. In fact, family support was negatively related to depressive symptomatology in two studies investigating adolescent females age 12–18 years (Kerr et al. 2006; Trask-Tate et al. 2010). Moreover, there has been longitudinal research indicating that adolescents age 11–15 years who lack family support have an increased likelihood of developing depressive symptoms (Stice et al. 2004). Consequently, the principle-effect model may be the best fitting explanation for the relationship between social support and depressive symptomatology in adolescents from 11–18 years of age. If so, social support could be beneficial for every adolescent.
In contrast, the stress-buffer model, which is a moderation model, posits that social support’s positive impact is magnified for individuals facing stressful life events (Cohen and Willis 1985). The stress-buffer model is commonly used to explain the development and maintenance of depression. For example, the well established cognitive stress-vulnerability model of depression (Beck 1976) and the self-esteem vulnerability model (Brown and Harris 1978) are stress-buffer models. Thus, these models provide a context to examine the stress-buffer model and studies examining either of these two models have repeatedly found support for the stress-buffer effect (e.g., Lewinsohn et al. 2001). Similarly, some studies focusing on social support and depressive symptoms provided support for the stress-buffer model as well. To be precise, Murberg and Bru (2004) and Ystgaard et al. (1999) found that family support buffers against the harmful impact of negative life-events on depressive symptoms in students grade 8 and grade 11, respectively. Further, Desjardins and Leadbeater (2011) found a similar moderating effect of paternal support on the association between relational victimization and depressive symptoms in adolescents ages 12 to 19 years. Finally, Pössel et al. (2013) found that teacher support buffers against the impact of negative life-events on depressive symptoms in students grade 8 to 10 but not grade 11 and 12. However, based on Rueger and colleagues’ (2016) meta-analysis, there were no differences regarding the role of social support between adolescents who were stressed and non-stressed, lending support to the principle-effect rather than the stress-buffer model. Nevertheless, the empirical literature regarding principle-effect vs. stress-buffer effect seems somewhat inconsistent.
Current Study
Previous literature examined two different models of how social support might have a positive effect on depressive symptoms in adolescence. On the one hand, the principle-effect model, a main effect model, asserts that social support has an equally positive impact on individuals regardless of stressful life situations (Dumont and Provost 1999). On the other hand, the stress-buffer model, a moderation model, posits that social support’s positive impact is magnified for individuals facing stressful life events (Cohen and Willis 1985). Because the majority of the empirical findings seem to favor the principle-effect model over the stress-buffer model (Kerr et al. 2006; Rueger et al. 2016; Stice et al. 2004; Trask-Tate et al. 2010), we proposed that the principle-effect model will be a better fit for each of the sources of social support. In other words, we propose that social support from family, friends, and teachers are negatively related to later depressive symptoms in all adolescents (hypothesis 1). Further, based on previous empirical findings (Colarossi and Eccles 2003; McMahon et al. 2013), we proposed that all three sources of social support are negatively related to later depressive symptoms in adolescence when tested independently (hypothesis 2). However, we finally proposed that when all three sources of social support are included in one model, only family support remains significant in adolescents up to grade 10, while all three sources remain significant in the last grades of high school (hypothesis 3).
Methods
Participants
Participants were 1452 Australian students from 24 secondary schools that were part of the control condition of a large-scale depression prevention study entitled beyondblue (for a detailed description of the prevention program see Sawyer et al. 2010). Over the 5-year period, there were no significant differences in depressive symptoms, risk factors, or protective factors between students in the intervention and control group (Sawyer et al. 2010). Nevertheless, for the purpose of this paper, only the students of the control condition were included.
Researchers obtained informed consent from all participating students and their parents before the baseline assessment. Students in the beyondblue study completed a baseline assessment in grade 8 and were followed until grade 12. Students’ average age at the time of the baseline assessment was 13.1 (SD = 0.5; range: 11–16 years) years old and 51.9% of the students identified as female (grade 9: 52.2%; grade 10: 53.2%; grade 11: 54.0% grade 12: 56.9%). At baseline about 92.5% of participants were born in Australia (grade 9: 93.0%; grade 10: 93.7%; grade 11: 94.2% grade 12: 92.3%), while 4.4% identified as Aboriginal or Torres Straight Islander (grade 9: 3.9%; grade 10: 3.8%; grade 11: 2.6% grade 12: 2.8%). In addition, the majority of participants (88.8%) had at least one parent that was a full-time employee at baseline (grade 9: 89.8%; grade 10: 90.4%; grade 11: 91.3% grade 12: 91.2%).
In Australia, grade 8 is generally the first academic year of high school, and students attend school from February to early December. All participating students in grade 8 completed the baseline assessment during the second of four terms (May to June) and the assessments in grades 9 to 12 during the last term of the school year (October to December). At baseline 2545 students (n = 1314; 51.6% female) participated and 2405 or 94.5% (n = 1251; 52.0% female) of them completed the follow-up assessments in grade 9, 2219 or 87.2% (n = 1165; 52.5% female) in grade 10, 1717 or 67.5% (n = 936; 54.5% female) in grade 11, and 1452 or 57.1% (n = 826; 56.9% female) in grade 12. This retention rate is consistent with other Australian longitudinal studies with high school students and reflects the attrition rates of students in Australia (e.g., Caldwell et al. 2004; Heaven and Ciarrochi 2008).
Altogether, 437 students (21.1%) left their baseline school during the course of the study. The 1452 students who did not leave their baseline school made up the sample in the present study. Students left their school for a variety of reasons (e.g., family relocated, transferred to vocational school, dropped out). There were no baseline differences between students who left their baseline school and students who did not on sex [χ²(1) = 2.06, p = .358], age [t(2333.39) = 0.94, p = .350], or whether or not participants were born in Australia [χ²(1) = 1.01, p = .604]. However, significantly more students who left their baseline school identified as Aboriginal and/or Torres Strait Islander [χ²(1) = 21.06, p < .001], perceived less social support from family [t(2527) = 19.38, p < .001], friends [t(2527) = 48.24, p < .001], and teachers [t(2527) = 8.23, p < .001] at the baseline assessment, underwent more stressful events [t(1999.84) = −6.57, p < .001], and experienced a higher frequency of depressive symptoms [t(2180.28) = −5.14, p < .001].
Measures
Depressive symptoms
At each wave of data collection, the Center for Epidemiological Studies Depression Scale (CES-D; Radloff 1991) was used to describe and evaluate depressive symptomatology. The CES-D is comprised of 20 items (e.g., “I felt lonely.”), whereby students use a 4-point scale to rate the degree to which they experienced each symptom in the last week (1 = Rarely or none of the time [less than 1 day] to 4 = Most or all of the time [5–7 days]). Items 4, 8, 12, and 17 are positively worded and need to be reverse coded. After that, the scores are summed to create an overall score, with higher scores signifying increased amounts of depressive symptoms in the last week. The CES-D scores have demonstrated strong construct validity and reliability in this age group (Garrison et al. 1989). Table 1 shows means, standard deviations, and internal consistencies of CES-D scores, by grade level.
Stressful life-events
The List of Threatening Experiences Questionnaire (LTEQ) was adapted to evaluate 13 events identified as having a potential long-term impact (e.g., pregnancy; illness or death; Brugha et al. 1985). Items were adapted from the original scale to better fit an adolescent age group (e.g. break-up from partner rather than divorce). Students responded with yes or no to indicate whether each event had occurred in their life in the last 6 months. The items are then summed to create an overall score between 0 and 13, with higher scores signifying a higher level of life events. Sawyer et al. (2009) found that the modified LTEQ was not only predictive of depressive symptoms at baseline but also of depressive symptoms 1 year later in high school students. Table 1 shows means, standard deviations, and internal consistencies of stressful events by grade level.
Social support
An instrument to measure general social support from teachers was developed for the current study (for the details about the instrument development see Pössel et al. 2013). The instrument is comprised of 9 items (e.g., “I feel I can go to my teacher with the things that are on my mind”), selected from several pre-existing scales (Arthur et al. 2002; Bond et al. 2004; Epstein and McPartland 1976; Goodenow 1993; Roeser et al. 1996). Via a 4-point scale (1 = NO! to 4 = YES!), students indicate their agreement with each statement. The items are then summed to calculate an overall score. Table 1 shows means, standard deviations, and internal consistencies of stressful events by grade level.
Social support from family and friends was assessed using the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al. 1988). The MSPSS is one of the three most commonly used instruments to measure perceived general social support from family and friends (Rueger et al. 2016). Students are asked to rate how strongly they agree or disagree with each statement on a 7-point Likert type scale (1 = very strongly disagree to 7 = very strongly agree). For the present study only the family and peer items were used including 4 items measuring family support (e.g. “My family really tries to help me.”) and 4 items measuring friend support (e.g. “I can count on my friends when things go wrong.”). Table 1 shows means and standard deviations of stressful events, by grade level.
Design and Procedure
After obtaining ethics approval in each state, a letter explaining the study was sent to each parent with a student enrolled in grade 8 in all schools that agreed to participate (see Sawyer et al. 2009, 2010), for a detailed description of the demographics, selection protocol, and eligibility criteria). Of the 8837 students invited to participate, parental consent for 5633 (participation rate: 63%) was received. Researchers administered the measures, while the teachers supervised the students during data collection. Participants completed the measures in approximately 30 min and were assessed in assembly halls or classrooms during school hours. To reduce missing data, absent students were re-contacted. Neither teachers, students, nor parents were compensated for participating in the study.
Data Analysis
HLM 6.03 (Raudenbush et al. 2004) was used to test for effects of between-school differences, as students were nested in schools. The unconditional means model demonstrated that differences in social support from teachers between schools is .0575 as measured by the ICC. In other words, 5.75% of the total variability in social support from teachers can be explained by school-level variability. Further, only 1.36% of the variability in depressive symptoms can be attributed to schools. Because the variance in social support from teachers and depressive symptoms explained by schools is <10%, using school as the nesting variable was regarded as unnecessary in subsequent analyses (Lee 2000).
To perform path analyses, AMOS 21.0 with full information maximum likelihood (FIML) estimation was used (Arbuckle 1999), as FIML is not affected by missing data (Enders 2001). Moreover, χ², the RMSEA, and the CFI were used to examine goodness of fit of models. When interpreting findings, nonsignificant χ² values are preferred. Further, RMSEA values of <.05 are interpreted as sign for a good model fit and values of <.08 demonstrate an acceptable fit (Hu and Bentler 1998). Finally, CFI values of >.95 are considered good model fit and values of >.90 are interpreted as acceptable (Hu and Bentler 1998).
To identify the best fitting model, χ² difference tests were used to compare nested models. In this test, the χ² and dfs values of the compared models are subtracted from each other. The models are significantly different from each other when Δχ² is significant for Δdf. In this case, the model with fewer dfs has better model fit compared to the competing model. When the Δχ² is non-significant, this indicates that there is no difference in model fit and the model with more dfs (the more parsimonious model) should be retained.
First, the principle-effect model (associations from source of support at wave X to depressive symptoms at wave X + 1) and the stress-buffer model (associations from source of social support, and source of social support by stressful events interactions, at wave X to depressive symptoms at wave X + 1) were calculated separately for each source of social support. Second, and as described above, χ² difference tests were used to compare the models with each other separately by source of social support. The purpose of this step was to identify the best fitting model for each individual source of social support. As it is possible that the best fitting model for the different sources of support are not identical, these analyses were calculated separately for each source of social support. Finally, the best fitting models for each source of social support (principle-effect or stress-buffer model) were integrated into one model and the individual paths within this model were examined. Because girls are more likely to develop depressive symptoms than boys (Angold et al. 2002; Twenge and Nolen-Hoeksema 2002), sex was used as covariates in all tested models.
Results
Preliminary Analyses
Descriptive statistics and correlations are shown in Table 1. As expected, while most constructs correlated moderately with each other, age did not correlate significantly with most other constructs. Further, friends’ social support was largely unrelated to stress in grades 8 and 9, but in later years stress and social support from friends had a small negative correlation (r = −.04 to −.11). However, it should be noted that these correlations are likely only significant because of the large sample size, as stress and social support from friends share maximal 1.2% variance.
Hypothesis Testing
Model comparisons separated by sources of social support
To identify the model that fit the data best and to examine hypotheses 1 and 2, six different models were tested separately by source of social support and pair-wise compared with each other. First, the comparison of the principle-effect model with family as source of social support, χ² (136, N = 2076) = 1017.57, p < .001, CFI = 0.898, RMSEA = 0.056, (explained variance [EV] in adolescents’ depressive symptoms in the subsequent year: grade 9: 28.4%; grade 10: 34.5%; grade 11: 29.3%; grade 12: 32.2%) and the stress-buffer model with family as source of social support, χ² (132, N = 2076) = 1007.95, p < .001, CFI = 0.898, RMSEA = 0.057, (EV in adolescents’ depressive symptoms in the subsequent year: grade 9: 28.8%; grade 10: 34.6%; grade 11: 29.4%; grade 12: 32.3%) supported the stress-buffer model, Δχ² (4, N = 2076) = 9.62, p = .047. However, the stress-buffer model explained only up to 0.4% more variance in adolescents’ depressive symptoms.
Second, the principle-effect model with friends as source of social support, χ² (136, N = 2076) = 833.45, p < .001, CFI = 0.905, RMSEA = 0.050, (EV in adolescents’ depressive symptoms in the subsequent year: grade 9: 28.5%; grade 10: 35.6%; grade 11: 29.7%; grade 12: 33.4%) and the stress-buffer model with friends as source of social support, χ² (132, N = 2076) = 827.11, p < .001, CFI = 0.906, RMSEA = 0.050, (EV in adolescents’ depressive symptoms in the subsequent year: grade 9: 28.6%; grade 10: 35.6%; grade 11: 29.6%; grade 12: 33.4%) were calculated. The principle-effect model explained maximal 0.1% more variance in adolescents’ depressive symptoms, and the χ² difference test comparing the two models also supported the principle-effect model, Δχ² (4, N = 2076) = 6.34, p = .175.
Finally, the principle-effect model with teachers as source of social support, χ² (136, N = 2076) = 823.85, p < .001, CFI = 0.921, RMSEA = 0.049, (EV in adolescents’ depressive symptoms: grade 9: 29.4%; grade 10: 35.7%; grade 11: 31.2%; grade 12: 33.4%) and the stress-buffer model with teachers as source of social support, χ² (132, N = 2076) = 818.87, p < .001, CFI = 0.922, RMSEA = 0.050, (EV in adolescents’ depressive symptoms: grade 9: 29.5%; grade 10: 35.7%; grade 11: 31.2%; grade 12: 33.4%) were calculated and compared. As the χ² difference test was not significant, Δχ² (4, N = 2076) = 4.98, p = .289, the principle-effect model, which explained up to 0.1% less variance of adolescents’ depressive symptoms, was retained. Consistent with hypothesis 2 social support from each source are associated with later depression. However, contrary to our hypothesis 1, only social support from friends and teachers impacts depressive symptoms directly (principle-effect model). Social support from family, however, reduces the negative impact of stress on later depressive symptoms in our sample of adolescents (stress-buffer model).
Combining all sources of support into an integrated model
Next, the stress-buffer models with family as source of social support and the principle-effect model with friends and teachers as source of social support were integrated into one model, χ² (316, N = 2076) = 1672.74, p < .001, CFI = 0.922, RMSEA = 0.045 (EV in adolescents’ depressive symptoms: grade 9: 28.5%; grade 10: 33.4%; grade 11: 28.6%; grade 12: 31.3%) to examine the effects when all three sources of social support were entered simultaneously.
Additionally, we predicted that, when all three sources of social support are included in one model, only family support remains significant in adolescents up to grade 10, while all three sources remain significant in the last grades of high school (hypothesis 3). To examine this, we inspected the individual paths between waves in the integrated model. Contrary to our hypothesis, friend support was not significantly associated with levels of depressive symptoms in the combined model at any grade. Thus, we removed the associations between friend support and depressive symptoms from the combined model, χ² (320, N = 2076) = 1673.42, p < .001, CFI = 0.922, RMSEA = 0.045 (EV in adolescents’ depressive symptoms: grade 9: 28.5%; grade 10: 33.4%; grade 11: 28.5%; grade 12: 31.4%), and compared it with the original combined model in which all three sources of support are associated with levels of depressive symptoms. As the χ² difference test was not significant, Δχ² (4, N = 2076) = 0.68, p = .954, the combined model without friend support was retained.
A close inspection of the cross-wave paths revealed that teacher support and stress at grade 11 were not significantly associated with the levels of depressive symptoms in the next grade and teacher support at grade 8 was only marginally significantly associated with depressive symptoms 1 year later. In addition, the family support by stress interactions at grades 9 and 10 were not significantly associated with levels of depressive symptoms in the next grade. Thus, we compared the previously described integrated model, including both main effects of family and teacher support as well as family by stress interaction effects, to an integrated model with exclusively main effects of family and teacher support, χ² (324, N = 2076) = 1684.80, p < .001, CFI = 0.922, RMSEA = 0.045, (EV in adolescents’ depressive symptoms: grade 9: 28.1%; grade 10: 33.4%; grade 11: 28.4%; grade 12: 31.3%). As the χ² difference test was significant, χ² (4, N = 2076) = 11.38, p = .023, the integrated model with family support by stress interaction, which explained maximal 0.4% more variance of adolescents’ depressive symptoms, was retained.
Description of the final integrated model
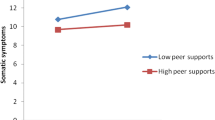
The individual paths between waves of the integrated model without friend support are presented in Table 2 and Fig. 1, and the correlations between constructs within the waves are presented in Table 3. Model-implied graphs were then constructed to further examine the association between the family support by stress interactions at grade 8 and 11 and later depressive symptoms (Fig. 2). The graphs demonstrate that stress was associated with depressive symptoms 1 year later but also that family support reduced the negative effect of stress on depressive symptoms. In other words, these findings are consistent with the stress-buffer model.

Significant marginally significant (dashed arrow) associations between constructs across grades in the integrated model without friends as source of social support (the stress-buffer model with family as source of social support and the principle-effect model with teachers as source of social support). Strengths and p-values of associations between constructs across grades and error terms of constructs within grades are presented in Tables 2 and 3, respectively

Model implied graphs of the standardized interaction effect between family support and stressful events at grade 8 predicting depressive symptoms in grade 9 (top) as well as between family support and stressful events at grade 11 predicting depressive symptoms in grade 12 (bottom)
Discussion
Based on the high prevalence of adolescent depression (Angold et al. 2002; Twenge and Nolen-Hoeksema 2002), the costs associated with it (Bui et al. 2017), and its detrimental long-term consequences (Kessler et al. 2012a, b; Lawrence et al. 2015; McClure et al. 1997; Patel et al. 2007; Stewart et al. 2002), it is clear that a thorough understanding of factors influencing the development of depression in youth is imperative. Following Bronfenbrenner’s bioecological theory (1986) and a multitude of empirical studies (for a meta-analysis see Rueger et al. 2016), family, friend, and teacher support seem to be crucial for depressive symptoms in adolescence. However, significant gaps in our knowledge exist regarding how relevant these three sources of support are throughout adolescence, which source(s) are relevant when all three are examined simultaneously, if they influence depressive symptoms directly (principle-effect model; Dumont and Provost 1999) or by reducing the negative impact of stress (stress-buffer model; Cohen and Willis 1985) on depressive symptoms, and if the relevance of the individual sources of social support changes during adolescence (Buhrmester 1996; Colarossi and Eccles 2003; Collins and Laursen 2004; Levitt et al. 1993; McMahon et al. 2013; Meeus et al. 2007). The present 5-year longitudinal study helps to fill in these gaps by following 1452 Australian students from grade 8 to 12.
Based on the above described literature, we proposed that the main effects of social support from family, friends, and teachers, but not the interactions between support from those sources and stressful events, would be related to later depressive symptoms (hypothesis 1). Further, we proposed that, when each source of social support is independently examined, all three sources of support would be negatively related to later depressive symptoms (hypothesis 2). When integrated into one model, we proposed that only family support would remain significant in adolescents up to grade 10, while all three sources would remain significant in grades 11 and 12 (hypothesis 3).
As proposed, when independently examined, each source of social support explained a meaningful and similar amount of variance of depressive symptoms. However, when all three sources of social support were combined and examined, friend support did not contribute in a meaningful way to adolescent depressive symptoms across the examined grades. Further, only teacher support at grade 9 and 10 were significant and teacher support at grade 8 was only marginally significant in their association with the levels of depressive symptoms in the next grade. Finally, as predicted, the principle-effect model (Dumont and Provost 1999) fit the data better for friend and teacher support. Inconsistent with our prediction, the stress-buffer model (Cohen and Willis 1985) fit the data better for family support. Associated with that finding, only the family support by stress interactions at grade 8 and 11, though not at grade 9 and 10, were related to depressive symptoms 1 year later. Inspecting the interactions in more detail revealed that family support reduced the negative effect of stress on depressive symptoms (see Fig. 2).
While most findings are consistent with our hypotheses, friend support did not contribute meaningfully to depressive symptoms throughout adolescence while teaching support in fact lost relevance throughout adolescence. As stated above, peers become important sources of social support in the beginning of middle childhood, and same-gender peers become more important during the transition into early adolescence (Buhrmester 1996; Levitt et al. 1993) while romantic partners become relevant sources of social support in late adolescence (Collins and Laursen 2004; Meeus et al. 2007). One possible reason for lack of relevance of friend support when combined with other sources of social support might be that we did not define “friend” (e.g., classmates, same-gender peers, romantic partners). Thus, it might be that different students interpreted friendship differently which consequently defused the influence of friend social support. With this in mind, future studies should utilize instruments that include all three types of friends but intentionally separate them out. Similarly, at least for college-bound individuals, it is likely that all types of friends become more important when they leave home as the frequency of social interactions with family may decrease. Future studies should therefore build on our study to examine the influence of family and friend support in late adolescence/early adulthood.
One possible explanation for decreased teacher influence toward the end of high school, despite family support moderating the effect of stress on depressive symptoms during the same developmental period, might be a change in the source of stress adolescents typically experience close to graduation. For example, Byrne et al. (2007) found in a sample of Australian adolescents grades 7 to 12 that stress was related to family, future uncertainty, financial pressure, and emerging adult responsibilities, while stressors related to school and teachers remained stable. As the stress students experience in late adolescence is less related to the sphere in which teachers can provide support, families remain relevant and might even gain influence. This highlights another possible explanation related to why family support moderates the effect of stress on adolescents’ depressive symptoms at the end of high school, but not during all of adolescence. Social support can be separated into different types (e.g., appraisal, emotional, informational, and instrumental; Malecki and Demaray 2003). Depending on the type of stress, some types of social support may impact depressive symptoms directly while others may moderate the effect of stress. While we are unaware of empirical studies examining these proposed differences, one can speculate that instrumental (family) support (incl. spending resources like time, materials, or money; Malecki and Demaray 2003) might be particularly beneficial for adolescents under a lot of financial pressure (e.g., costs for college) than for their peers with less financial pressure (e.g., working a full-time job). However, without studies examining these possible explanations in more detail, these considerations must remain speculative.
The current study had several strengths that should be noted. For instance, the study included a large community sample, which helped reduce selection bias, making the results more generalizable. This is because findings on individuals with depressive symptoms in a community sample are more generalizable to the general population than findings on individuals with depressive disorders as these individuals have systematic differences from those in the general population (Cohen and Cohen 1984). Further, the current study used a 5-wave longitudinal design, so data were collected throughout the students’ entire high school career.
In addition to its strengths, the current study had several limitations. First, as mentioned above, this study measured “general” social support and negative life events as this might be associated with some unexpected findings it can be seen as a limitation. As already outlined, instruments that better differentiate between different types of social support and different types of stress might be able to explain unexpected findings and therefore build on our study. For example, the Child and Adolescent Social Support Scale (CASSS; Malecki et al. 2000) separated four types of social support from four different sources (classmates, close friends, parents, and teachers) and the Adolescent Stress Questionnaire (ASQ; Byrne et al. 2007) measures 10 different types of stress typical for adolescents. Second, and related to the first limitation, there is limited information regarding the validity of the support instrument used in this study. Pössel et al. (2013) provide some evidence for construct validity via two factor analyses, and practical metric invariance across sex (girls vs. boys), condition (prevention vs. control condition), and time (grade 8 vs. grade 12). However, further investigation into this instrument is needed, as all analyses examining the validity of the support measure were conducted using the beyondblue sample. Therefore, future studies should investigate the validity of the instrument using other samples. Third, our study relied on the sole use of student-report measures, which might result in an overestimation of the relationships between family, friend, and teacher support, stressful events, and depressive symptoms. Fourth, and related to this limitation, depressive symptoms were measured using a self-report checklist as opposed to a diagnostic interview; thus, it is unclear if our findings are generalizable to adolescents experiencing clinical levels of depression. However, research demonstrates that adolescent depression is best conceptualized dimensionally (e.g., Hankin et al. 2005), which makes it likely that the findings of the current study could be replicated in a sample of adolescents with depressive disorders.
Moreover, a fifth limitation is that the study’s longitudinal design was characterized by a high, nonrandom attrition rate of 46.63% between grade 8 and grade 12. As stated above, those who left their baseline school reported less family, friend, and teacher support at baseline, more stressful events, a higher frequency of depressive symptoms, and/or were of Torres Strait Islander or Aboriginal background. It is important to note that Australian students who wish to eventually have a vocational career leave traditional high school after grade 10 in lieu of specialized vocational high schools, or they undertake apprenticeships or some other form of employment, partially explaining the 20% attrition rate from grades 10 to 11. In particular, students who come from an Aboriginal background are more likely to transfer to a vocational school or drop out altogether (Gray et al. 2000). Adolescents who report more negative events (Dyregrov 2004), less teacher support (Davis and Dupper 2004), and more depressive symptomatology (Lewinsohn and Clarke 1999) are also more likely to change schools or drop out compared to other students. With these patterns in mind, the generalizability of the findings is limited for these groups and future research regarding family, friend, and teacher support should focus on these students.
Finally, some might see it as a limitation that biological sex was not considered as a potential moderator in these analyses. However, we decided not to do so as Rueger et al. (2016) found negligibly small differences in the effects of social support on depression in female and male adolescents. In particular, for girls, social support explained only 0.09% more variance in cross-sectional studies and 0.25% more variance in longitudinal studies compared to boys. This is also reflected in the primary literature, as one group of studies found sex differences (12–18 years, Kerr et al. 2006), another found sex differences in some but not all examined associations (13–18 years, Pössel et al. 2013), and a final group of studies found no sex differences (15–18 years, Colarossi and Eccles 2003; 14–15 years, Murberg and Bru 2004; 12–14 years, Shochet et al. 2011). The age of participants did not seem to impact whether sex differences were found or not. While it is understandable that one might expect the biological sex of the students to moderate the associations between social support and depressive symptoms in adolescents, there is no consistent empirical support for such an effect.
Conclusions
Considering the crucial developmental changes occurring in adolescence, our findings provide a concrete foundation that future work can build on to better understand the impact different sources of social support have on depressive symptoms in high school students. Combined with previous studies examining the relationships between support from family, friends, and teachers and depressive symptoms in youth (Colarossi and Eccles 2003; McMahon et al. 2013; Rueger et al. 2016), our findings demonstrate that support from family and teachers is related to later depressive symptoms in adolescence, while support from friends appear irrelevant when studied in combination with the other two sources of social support. Additionally, it is important to note that family is the most stable source of support throughout adolescence. Further, our study found that the stress-buffer model was the best fit for support from family only, demonstrating the possibility that adolescents facing stress might benefit more from family support compared to their peers without stressful life events. If replicated, our findings emphasize the relevance of adult social support throughout high school, begging the question: how can these findings be implicated in applied work?
When discussing the implications of our findings, we must first acknowledge that the outcomes from the current study contribute to the well-known fact that adolescence can be summarized in one word—change. With radical biological, social, and intrapersonal change occurring (Cole et al. 2008), it is important to hone in on the details that occur in adolescent lives. In a high school world that seems governed by peer interactions and pressures where the reward circuitry of the brain is activated simply by having peer influences around (Chein et al. 2011), it is easy to assume that peers should be targeted as social supports in preventing depressive symptoms. However, our findings demonstrate that peers may have a weaker presence in adolescent lives than expected. Only when we begin to raise insight about the extent of the role that these individuals play in adolescents’ lives will we be able to contribute to not only the understanding of the implications of adolescent developmental change on social support, but we may also begin the process of positive change in preventing depressive symptoms.
References
Angold, A., Erkanli, A., Silberg, J., Eaves, L., & Costello, E. J. (2002). Depression scale scores in 8-17-year-olds: Effects of age and gender. Journal of Child Psychology and Psychiatry, 43, 1052–1063.
Arbuckle, J. L. (1999). AMOS user’s guide. Chicago, IL: SmallWaters.
Arthur, M. W., Hawkins, J. D., Pollard, J. A., Catalano, R. F., & Baglioni, Jr., A. J. (2002). Measuring risk and protective factors for substance use, delinquency, and other adolescent problem behaviors: The Communities That Care Youth Survey. Evaluation Review, 26, 575–601.
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York, NY: International University Press.
Bond, L., Patton, G., Glover, S., Carlin, J. B., Butler, H., Thomas, L., & Bowes, G. (2004). The gatehouse project: Can a multi-level school intervention affect emotional well being and health risk behaviours? Journal of Epidemiology and Community Health, 58, 997–1003.
Bronfenbrenner, U. (1986). Ecology of the family as a context for human development: Research perspectives. Developmental Psychology, 22, 723.
Bronfenbrenner, U., & Morris, P. A. (2006). The bio-ecological model of human development. In W. Damon & R. M. Lerne (Eds.), Handbook of child psychology: Volume 1: Theoretical models of human development. 6th edn (pp. 793–828). Hoboken, NJ: Wiley.
Brown, G. W., & Harris, T. O. (1978). Social origins of depression. London, UK: Free Press.
Brugha, T., Bebbington, P., Tennant, C., & Hurry, J. (1985). The list of threatening experiences: A subset of 12 life event categories with considerable long-term contextual threat. Psychological Medicine, 15, 189–194.
Buhrmester, D. (1996). Need fulfillment, interpersonal competence, and the developmental contexts of early adolescent friendship. In W. M. Bukowski, A. F. Newcomb & W. W. Hartup (Eds.), The Company they keep: Friendship in childhood and adolescence (pp. 158–185). New York, NY: Cambridge University Press.
Bui, A. L., Dieleman, J. L., Halmavid, H., Birger, M., Chapin, A., & Murray, C. J. L. (2017). Spending on children’s personal health care in the United States, 1996-2013. JAMA Pediatrics, 171, 181–189. doi:10.1001/jamapediatrics.2016.4086.
Byrne, D. G., Davenport, S. C., & Mazanov, J. (2007). Profiles of adolescent stress: The development of the adolescent stress questionnaire (ASQ). Journal of Adolescence, 30, 393–419. doi:10.1016/j.adolescence.2006.04.004.
Caldwell, M. S., Rudolph, K. D., Troop-Gordon, W., & Kim, D.-Y. (2004). Reciprocal influences among relational self-views, social disengagement, and peer stress during early adolescence. Child Development, 75, 1140–1154. doi:10.1111/j.1467-8624.2004.00730.x.
Chein, J., Albert, D., O’Brien, L., Uckert, K., & Steinberg, L. (2011). Peers increase adolescent risk taking by enhancing activity in the brain’s reward circuitry. Developmental Science, 14, F1–F10. doi:10.1111/j.1467-7687.2010.01035.x.
Cohen, P., & Cohen, J. (1984). The clinician’s illusion. Archives of General Psychiatry, 41, 1178–1182.
Cohen, S., & Willis, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310–357.
Colarossi, L. G., & Eccles, J. S. (2003). Differential effects of support providers on adolescents’ mental health. Social Work Research, 27, 19–30. doi:10.1093/swr/27.1.19.
Cole, D. A., Ciesla, J. A., Dallaire, D. H., Jacquez, F. M., Pineda, A. Q., LaGrange, B., & Felton, J. W. (2008). Emergence of attributional style and its relation to depressive symptoms. Journal of Abnormal Psychology, 117, 16–31. doi:10.1037/0021-843X.117.1.16.
Collins, W. A., & Laursen, B. (2004). Changing relationships, changing youth: Interpersonal contexts of adolescent development. Journal of Early Adolescence, 24, 55–62. doi:10.1177/0272431603260882.
Davis, K. S., & Dupper, D. R. (2004). Student-teacher relationships: An overlooked factor in school dropout. Journal of Human Behavior in the Social Environment, 9, 179–193.
Desjardins, T. L., & Leadbeater, B. J. (2011). Relational victimization and depressive symptoms in adolescence: Moderating effects of mother, father, and peer emotional support. Journal of Youth and Adolescence, 40, 531–544. doi:10.1007/s10964-010-9562-1.
Dumont, M., & Provost, M. A. (1999). Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. Journal of Youth and Adolescence, 28, 343–363. doi:10.1023/A:1021637011732.
Dyregrov, A. (2004). Educational consequences of loss and trauma. Educational and Child Psychology, 21, 77–84.
Enders, C. K. (2001). A primer on maximum likelihood algorithms available for use with missing data. Structural Equation Modeling: A Multidisciplinary Journal, 8, 128–141.
Epstein, J. L., & McPartland, J. M. (1976). The concept and measurement of the quality of school life. American Educational Research Journal, 13, 15–30.
Garrison, C. Z., Schluchter, M. D., Schoenbach, V. J., & Kaplan, B. K. (1989). Epidemiology of depressive symptoms in young adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 343–351.
Goodenow, C. (1993). The psychological sense of school membership among adolescents: Scale development and educational correlates. Psychology in the Schools, 30, 79–90.
Gray, M. C., Huber, B., & Schwab, R. G. (2000). Trends in indigenous educational participation and attainment, 1986-96. Australian Journal of Education, 44, 101–117.
Hankin, B. L., Fraley, R. C., Lahey, B. B., & Waldman, I. (2005). Is depression best viewed as a continuum or discrete category? A taxometric analysis of childhood and adolescent depression in a population-based sample. Journal of Abnormal Psychology, 114, 96–110. doi:10.1037/0021-843X.114.1.96.
Heaven, P. C. L., & Ciarrochi, J. (2008). Parental styles, conscientiousness, and academic performance in high school: A three-wave longitudinal study. Personality and Social Psychology Bulletin, 34, 451–461. doi:10.1177/0146167207311909.
Hu, L., & Bentler, P. M. (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3, 424–453. doi:10.1037/1082-989X.3.4.424.
Kerr, D. C. R., Preuss, L. J., & King, C. A. (2006). Suicidal adolescents’ social support from family and peers: Gender-specific associations with psychopathology. Journal of Abnormal Child Psychology, 34, 103–113. doi:10.1007/s10802-005-9005-8.
Kessler, R. C., Avenevoli, S., Costello, J., Greif Green, J., Gruber, M. J., McLaughlin, K. A., & Merikangas, K. R. (2012a). Severity of 12-month DSM-IV disorders in the national comorbidity survey replication adolescent supplement. Archives of General Psychiatry, 69, 381–389. doi:10.1001/archgenpsychiatry.2011.1603.
Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Wittchen, H.-U. (2012b). Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. International Journal of Methods in Psychiatric Research, 21, 169–184. doi:10.1002/mpr.1359.
Lawrence, D., Hafekost, J., Johnson, S. E., Saw, S., Buckingham, W. J., Sawyer, M. G.,… & Zubrick, S. R. (2015). Key findings from the second Australian child and adolescent survey of mental health and wellbeing. Australian and New Zealand Journal of Psychiatry, 10.1177/0004867415617836
Lee, V. E. (2000). Using hierarchical linear modeling to study social contexts: The case of school effects. Educational Psychologist, 35, 125–141. doi:10.1207/S15326985EP3502_6.
Levitt, M. J., Guacci-Franco, N., & Levitt, J. L. (1993). Convoys of social support in childhood and early adolescence: Structure and function. Developmental Psychology, 29, 811–818. doi:10.1037/0012-1649.29.5.811.
Lewinsohn, P. M., & Clarke, G. M. (1999). Psychosocial treatments for adolescent depression. Clinical Psychology Review, 19, 329–342.
Lewinsohn, P. M., Joiner, Jr., T. E., & Rohde, P. (2001). Evaluation of cognitive diathesis-stress models in predicting major depressive disorder in adolescents. Journal of Abnormal Psychology, 110, 203–215. doi:10.1037/0021-843X.110.2.203.
Malecki, Ch. K., & Demaray, M. K. (2003). What type of support do they need? Investigating student adjustment as related to emotional, informational, appraisal, and instrumental support. School Psychology Quarterly, 18, 231–252.
Malecki, C. K., Demaray, M. K., & Elliott, S. N. (2000). The child and adolescent social support scale. DeKalb, IL: Northern Illinois University.
McClure, E., Rogeness, G. A., & Thompson, N. M. (1997). Characteristics of adolescent girls with depressive symptoms in a so-called ‘normal’ sample. Journal of Affective Disorders, 42, 187–197.
McMahon, S. D., Coker, C., & Parnes, A. L. (2013). Environmental stressors, social support, and internalizing symptoms among African American youth. Journal of Community Psychology, 41, 615–630. doi:10.1002/jcop.21560.
Meeus, W. H., Branje, S. J., van der Valk, I., & de Wied, M. (2007). Relationships with intimate partner, best friend, and parents in adolescence and early adulthood: A study of the saliency of the intimate partnership. International Journal of Behavioral Development, 31, 569–580. doi:10.1177/0 165025407080584.
Murberg, T. A., & Bru, E. (2004). Social support, negative life events and emotional problems among Norwegian adolescents. School Psychology International, 25, 387–403. doi:10.1177/0143034304048775.
National Institute of Mental Health. (2013). Major depression among adolescents. http://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adolescents.shtml
Patel, V., Flisher, A. J., Hetrick, S., & McGorry, P. (2007). Mental health of young people: A global public-health challenge. Lancet, 369, 1302–1313. doi:10.1016/S0140-6736(07)60368-7.
Pössel, P., Rudasill, K. M., Sawyer, M. G., Spence, S. H., & Bjerg, A. C. (2013). Associations between teacher emotional support and depressive symptoms in Australian adolescents: A 5-year longitudinal study. Developmental Psychology, 49, 2135–2146. doi:10.1037/a0031767.
Radloff, L. S. (1991). The use of the center for epidemiologic studies depression scale in adolescents and young adults. Journal of Youth and Adolescence, 20, 149–166.
Raudenbush, S., Bryk, A., Cheong, Y. F., Congdon, R., & du Toit, M. (2004). HLM6: Hierarchical linear and non-linear modeling. Lincolnwood, IL: Scientific Software International.
Roeser, R. W., Midgley, C., & Urdan, T. C. (1996). Perceptions of the school psychological environment and early adolescents’ psychological and behavioral functioning in school: The mediating role of goals and belonging. Journal of Educational Psychology, 88, 408–422.
Rueger, S. Y., Malecki, C. K., Pyun, Y., Aycock, C., & Coyle, S. (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychological Bulletin, 142, 1017–1067. doi:10.1037/bul0000058.
Sawyer, M. G., Pfeiffer, S., & Spence, S. H. (2009). Life events, coping and depressive symptoms among young adolescents. A one-year prospective study. Journal of Affective Disorders, 117, 48–54.
Sawyer, M. G., Pfeiffer, S., Spence, S. H., Bond, L., Graetz, B., Kay, D., & Sheffield, J. (2010). School-based prevention of depression: A randomised controlled study of the Beyondblue schools research initiative. Journal of Child Psychology and Psychiatry, 51, 199–209.
Shochet, I. M., Smith, C. L., Furlong, M. J., & Homel, R. (2011). A prospective study investigating the impact of school belonging factors on negative affect in adolescents. Journal of Clinical Child & Adolescent Psychology, 40, 586–595. doi:10.1080/15374416.2011.581616.
Stewart, S. M., Lewinsohn, P. M., Lee, P. W., Ho, L. M., Kennard, B., Hughes, C. W., & Emslie, G. J. (2002). Symptom patterns in depression and “subthreshold” depression among adolescents in Hong Kong and the United States. Journal of Cross-Cultural Psychology, 33, 559–576. doi:10.1177/022022102238269.
Stice, E., Ragan, J., & Randall, P. (2004). Prospective relations between social support and depression: Differential direction of effects for parent and peer support? Journal of Abnormal Psychology, 113, 155–159. doi:10.1037/0021-843X.113.1.155.
Trask-Tate, A., Cunningham, M., & Lang-DeGrange, L. (2010). The importance of family: The impact of social support on symptoms. Research in Human Development, 7, 164–182. doi:10.1080/15427609.2010.504458.
Twenge, J. M., & Nolen-Hoeksema, S. (2002). Age, gender, race, socioeconomic status, and birth cohort differences on the children’s depression inventory: A meta-analysis. Journal of Abnormal Psychology, 11, 578–588. doi:10.1037/0021-843X.111.4.578.
United States Department of Health & Human Services (2016). America’s Adolescents: A Day in the Life. http://www.hhs.gov/ash/oah/adolescent-health-topics/americas-adolescents/day.html. Accessed 3 Aug 2017.
Ystgaard, M., Tambs, K., & Dalgard, O. S. (1999). Life stress, social support and psychological distress in late adolescence: A longitudinal study. Social Psychiatry and Psychiatric Epidemiology, 34, 12–19.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52, 30–41.
Acknowledgements
We would like to thank the adolescents, parents, and teachers involved in this project.
Author Contributions
M.S. and S.S. were lead investigators for the beyondblue schools study; J.S. was a project manager for the beyondblue schools study; J.S., M.S., and S.S. were responsible for its design and implementation; J.S. and S.S. also developed the prevention program and evaluation materials; J.S. also oversaw data collection in one of the participating states; B.C., P.P., and S.B. drafted the manuscript; P.P. performed the statistical analysis; All authors read and approved the final manuscript.
Funding
This study was funded by beyondblue and the National Health and Medical Research Council, Australia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Pössel, P., Burton, S.M., Cauley, B. et al. Associations between Social Support from Family, Friends, and Teachers and depressive Symptoms in Adolescents. J Youth Adolescence 47, 398–412 (2018). https://doi.org/10.1007/s10964-017-0712-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-017-0712-6