
Abstract
Objectives
Although research has identified interpersonal difficulties as risk factors for adolescent suicidality, parent and peer relationships are often assessed as discrete risk domains.
Methods
The current study uses a social network approach to assess individual differences in the degree to which a clinical sample of 129 adolescents being treated for suicidal ideation rely on parents or peers for their attachment needs.
Results
Youth who affiliated with deviant peers were more likely to: (a) report greater intensity (increased frequency and duration and decreased controllability) of their suicide ideation, and (b) identify peers rather than adults as attachment figures.
Conclusions
Adolescents’ peer relationships are associated with suicide ideation intensity in a clinical sample of suicidal and depressed adolescents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Interpersonal functioning has long been considered essential to theories of adult suicide (Joiner 2005), and there is a growing recognition of the need to identify and target these factors in adolescents’ social networks (Bloch 2016). Adolescents’ social networks are dynamic and complex, as they serve multiple functions and include relationships with both adults and peers. The quality of these bonds to parents and peers has been frequently implicated in a variety of problem behaviors. Parent-adolescent conflict, lack of parental bonding, negative attachment expectancies, and insecure parent-adolescent attachment have been found to be related to risk-taking behaviors and psychopathology in adolescents (Ackard et al. 2006; Conner et al. 2016; Consoli et al. 2013; Fergusson et al. 2000; Roelofs et al. 2013; Saffer et al. 2014; Zisk et al. 2017). Further, these parental risk factors have also predicted the escalation from suicidal ideation to actual attempts (Ackard et al. 2006; Consoli et al. 2013; Saffer et al. 2014). Adolescents’ peer relationships have also been implicated in the severity of suicidality, with relationship quality, peer rejection, and peer victimization linked to suicidal ideation and behaviors in both community and clinical samples of adolescents (Geoffroy et al. 2016; Prinstein et al. 2000; Wolff et al. 2014).
Although adolescents’ difficulties with parents and peers have been implicated in their suicidal ideation and behaviors, these relationships are generally treated as discrete domains. A social network approach (Fulginiti et al. 2016) offers a more useful method for understanding the different functions served by parents and peers by examining these functions in relation to each other. Adolescents develop and maintain their social networks to serve multiple functions that are subject to developmental change (Hazan and Zeifman 1994; Kobak et al. 2007). Children’s preferences for these individuals tend to be hierarchically ordered, with particular individuals serving as primary or secondary attachment figures (Bowlby 1969/1982; Cassidy 1999; Colin 1996). One way to identify the roles of parents and peers in adolescents’ social networks is to focus on which of these relationships serve attachment functions, defined as relationships that provide guidance, support, and protection for the adolescent. Starting in infancy, children form highly selective bonds with adult attachment figures, who serve the function of protection and guidance. During typical development, these primary bonds with adult caregivers persist through adolescence but begin to fade as adolescents explore peers as potential new attachment figures (Kobak et al. 2007).
Peers typically replace adults in the attachment hierarchies of young adults. However, research has shown that early reliance on a peer as an attachment figure during adolescence may increase risk for engaging in problem behaviors (Rosenthal and Kobak 2010). This can occur for several reasons. First, it is likely that most adolescents are incapable of addressing an adolescent’s attachment needs by providing responsible guidance, support, and protection, especially in dangerous or emergency situations. Further, an over-reliance on peers may suggest a reduction in adult caregivers’ abilities to monitor the adolescent’s behavior. This lack of parental monitoring may lead to increased risk-taking behaviors and a greater affiliation with deviant peers. In fact, affiliation with deviant peers has been related to risky behaviors, such as unprotected sexual behavior, substance use, and delinquency (Dishion et al. 1995; Dishion et al. 2012; Prinstein and Wang 2005). Further, deviant peer affiliation has been associated with increased suicidality (Prinstein et al. 2000; Winterrowd and Canetto 2013). In one study, the link between deviant peer affiliation and suicidality was mediated by increased substance use and depression (Prinstein et al. 2000). The combination of reliance on a peer as an attachment figure and deviant peer affiliation may amplify the adolescent’s risk for impulsive and risky behaviors (Dishion and McMahon 1998) and reduce his/her capacity for managing suicidal thoughts and behaviors.
While there is some evidence for an association between deviant peer affiliation and suicidality, less is known about the possible role of adolescents’ attachment hierarchies. One possibility is that early movement of peers into adolescents’ attachment hierarchies will be related to greater deviant peer affiliation and suicidal ideation intensity. The current study uses the Important People Interview (IPI; Rosenthal and Kobak 2010) to assess suicidal adolescents’ preferences for attachment figures and the extent to which they affiliate with deviant peers in their social networks. Two aspects of early reliance on peers are likely to increase adolescents’ difficulties in managing suicidal thoughts and feelings. More specifically, we expect that reliance on peers as attachment figures will be related to deviant behavior in the peer network and that both of these variables will be associated with greater intensity of suicide ideation. The findings from this study can help identify characteristics of social networks that may be associated with intensity of suicidal ideation among depressed and suicidal adolescents.
Method
Participants
The participants for this study were 129 adolescents enrolled in a longitudinal randomized clinical trial of treatment efficacy for suicidal adolescents comparing Attachment-Based Family Therapy (ABFT) and Family-Enhanced Non-Directive Supportive Therapy (FE-NST; NCT01537419: Attachment Based Family Therapy for Suicidal Adolescents). Participants were recruited from emergency departments, community clinicians/ primary care providers, and schools throughout a large northeastern city to participate in this outpatient treatment trial. The data used in the current study were baseline data gathered before the participants were randomized into treatment groups. Participants met inclusion criteria by endorsing severe suicidal ideation (defined as a score of 31 or above on the Suicidal Ideation Questionnaire) and moderate depression (defined as a score of 20 or above on the Beck Depression Inventory-II) and by having at least one primary parent or caregiver agree to participate. Exclusionary criteria included evidence of imminent risk of harm to self or others (i.e., requiring a higher level of care/hospitalization as determined by study staff during safety assessment and planning), evidence of psychotic symptoms or severe cognitive impairment, non-English speaking participating parent, and initiation of medication within three weeks of the initial pre-treatment assessment.
The average age of the participants was 14.96 years (SD = 1.67) with the adolescents ranging in age from 12 to 18 years old. Eighty-two percent of the participants were female. Forty-nine percent of adolescents identified as black/African American, 29% as white, 1% as American Indian/Alaska Native, 3% as Asian, 1% as Native Hawaiian/Pacific Islander, 9% as multiracial, and 8% as other. Fifteen percent of adolescents identified as Hispanic. The average number of people living in the household was 4.4 (SD = 1.7). The average income to needs ratio was 2.14 (SD = 1.46) with 31.3% reporting living below the poverty line. Forty-three percent of adolescents reported living with both of their parents (intact two-parent household), 45% reported living in a single-parent household, 7% reported living with a single parent and that parent’s partner, and 5% reported another living situation (living with kin, living alone, etc.). A quarter (25%) of adolescents had a history of hospitalization, 39.3% reported a history of suicide attempts, and 56.4% reported a history of non-suicidal self-injury (NSSI). More information on the sample and the full battery of baseline measures is presented in the primary outcome study (Diamond et al. in press).
Procedure
This study was approved by the Institutional Review Board at the primary treatment site. Parental permission and consent were required for one parent/legal guardian, as parent/caregiver participation was required of all adolescents. Adolescents not considered adults provided assent in writing. Participants completed baseline assessments, including the IPI and the C-SSRS. Participants completed the IPI on the computer via Qualtrics and the C-SSRS was administered during an in-person interview with study staff at the primary study site. Following the baseline assessment, the 129 adolescents were then randomized into two treatment groups (Non-Directive Supportive Therapy or Attachment-Based Family Therapy) and underwent 16 weeks of treatment as well as follow-up assessments. Baseline data collected before the participants were randomized into treatment groups was used in the current study.
Measures
The Important People Interview
The Important People Interview (IPI) is designed to assess adolescents’ social networks and to identify individuals within those networks who serve attachment and affiliative needs (Rosenthal and Kobak 2010). Participants were initially asked to nominate the four most important people in their lives and four additional peers. Adolescents were then asked to identify their preferences by rank ordering the individuals in three attachment contexts: closeness (to whom do they feel closest), separation distress (who would they miss the most), and safe haven behavior (who would they call in an emergency). A similar procedure was used to identify adolescents’ preferences for the individuals in their networks who they would select in affiliative contexts (i.e., enjoyable social contacts). For the purposes of the current study, we only used the adolescents’ rankings of their attachment preferences.
Reliance on peers as attachment figures
Individuals who were preferred in attachment contexts were identified by summing points across the three attachment contexts (closeness, separation distress, and safe haven behavior) for the order in which they were ranked (4 points = first ranking; 3 = second; 2 = third, 1 = fourth; 0 = not ranked). Adolescents show relatively consistent preferences for individuals across the three attachment contexts, suggesting that they maintain hierarchical ordering of attachment figures (Rosenthal and Kobak 2010). As a result, each adolescent’s primary and secondary attachment figures were identified by summing points across attachment contexts. The individual with the most points was identified as the primary attachment figure, and the individual with the next highest number of points was determined to be the secondary attachment figure. As expected, biological mothers were most frequently identified as primary or secondary attachment figures (biological mothers comprised 48% of primary attachment figures and 17% of secondary attachment figures). Fathers were identified by 6% of the participants as primary and by 15% of participants as secondary attachment figures. Peers were identified by 26% of adolescents as primary and 38% of adolescents as secondary attachment figures. When other adults (grandparents, relatives) were included with parents, and other youth (siblings, romantic partners) were included with peers, 63% of primary attachment figures were adults (37% were peers) and 46% of secondary attachment figures were adults (54% were peers). Reliance on peers was calculated by assigning a weighted point value based on the placement of peers in the hierarchy with 4 points being assigned if a peer was the primary figure and 3 points if a peer was the secondary figure.
Deviant peer affiliation
In the last section of the IPI, participants reported how often their four nominated peers engaged in deviant behavior. Each peer was rated on 5 items: school performance, cigarette smoking, doing things for which they could get in trouble, using alcohol or other drugs, and skipping class. Participants rated each peer on the five items using a 5-point Likert scale (1 = never, 2 = hardly ever, 3 = sometimes, 4 = often, 5 = very often). One-hundred and seventeen participants completed the third section of the IPI. Reliability analyses identified the first item (“How well does this friend do in school compared to other kids in your school?”) as harmful to the internal consistency, and when it was deleted, internal consistency for the remaining four items was acceptable (Cronbach’s alpha = 0.73). Scores on the four items were averaged for each peer and averaged across the four peers to measure Deviant Peer Affiliation. The values for Deviant Peer Affiliation ranged from 1 to a possible 5 points. The mean was 1.45 points (SD = 0.49).
Computerized Diagnostic Interview Schedule for Children (C-DISC)
The C-DISC is a structured psychiatric diagnostic interview for children and adolescents aged 6 to 18 that covers 36 psychiatric diagnoses that occur in children and adolescents based on DSM-IV criteria (Shaffer et al. 2000). It was developed primarily for epidemiological research but is also useful in clinical settings. For the current study, the C-DISC was used to measure substance dependence and abuse. Because substance use disorders (SUDs) were so infrequent in this sample, a composite variable was used representing adolescents who met diagnostic criteria for any substance disorder (Alcohol Dependence [n = 1]; Alcohol Abuse [n = 4]; Marijuana Dependence [n = 4]; Marijuana Abuse [n = 2]).
Columbia-Suicide Severity Rating Scale (C-SSRS)
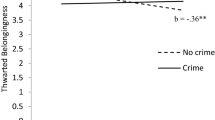
The C-SSRS is a semi-structured interview designed to assess severity of suicidal ideation and behavior (Posner et al. 2011). The C-SSRS has been validated in adult and adolescent populations with strong psychometric properties (Posner et al. 2011) and has shown predictive validity in samples of young adults and adolescents seeking psychiatric emergency services (Gipson et al. 2014; Horwitz et al. 2014). For this study, we used the C-SSRS subscale for measuring Intensity of Ideation, which has been previously shown to add incrementally to the prediction of future attempts in high-risk adolescents and young adults (Conway et al. 2017; Gipson et al. 2014; Horwitz et al. 2014). This subscale includes five items: Frequency (how often you have these thoughts), Duration (how long the thoughts last), Controllability (can you stop the thoughts if you want to), Deterrents to Active Attempt (are there things/people that stop you from acting on suicidal thoughts), and Reasons for Ideation (for revenge or escape). Each of the items was scored on a 5-point Likert scale. We excluded the Reasons for Ideation item because it was harming internal consistency. However, even after this item was excluded, internal consistency was poor (Chronbach’s alpha = 0.51). Therefore, a measurement model was tested using the items from this subscale as multiple indicators of the latent variable Suicide Intensity. Results using all five items revealed that Reasons for Ideation did not load significantly onto the latent variable, and this item was therefore dropped from the model. Using the remaining four items, we found good overall fit (χ2 = 0.58, p = 0.75; CFI = 1.00; RMSEA = 0.00; 90% CI [0.00, 0.12]). Controllability had the strongest loading (standardized β = 0.73), followed by Frequency (standardized β = 0.45), Duration (standardized β = 0.34), and Deterrents (standardized β = 0.30; see Fig. 1). This latent variable for Intensity of Suicide Ideation was used in final regression analyses.

Measurement model of intensity of suicidal ideation, with standardized beta weights reported (χ2 (2) = 0.58, p = 0.75; RMSEA = 0.00, 90% CI (0.00, 0.12); CFI = 1.0). **p<0.01; ***p<0.001
Beck Depression Inventory-II (BDI-II)
The BDI-II is a widely-used, 21-item self-report instrument designed to assess the severity of depressive symptoms in adults and adolescents (Beck et al. 1996). Each item is composed of four statements representing increasing increments of depression severity for a specific symptom. The score for each item on the scale ranges from 0 to 3, with the total score ranging from 0 to 63. Scores above 20 indicate moderate depression. A sample item is Loss of Pleasure (ranging from 0 = “I get as much pleasure as I ever did from the things I enjoy” to 3 = “I can’t get any pleasure from the things I used to enjoy”). The BDI-II has demonstrated good internal consistency in a comprehensive review of 118 studies (average α = 0.90; Wang and Gorenstein 2013). The BDI-II demonstrated high internal consistency in this sample (α = 0.85).
Data Analyses
Preliminary analyses included descriptive statistics and zero-order correlations for demographic and study variables. Twelve participants who did not complete the peer deviance questions had missing data. However, they did not differ from completers on demographic or primary study variables and were therefore assumed to be missing at random (MAR). Deviant peer affiliation for these participants was estimated using Maximum Likelihood Estimation (MLE). Our primary hypotheses were then tested using Mplus Version 7.0 (Muthén & Muthén 1998–2012). Mplus allowed for estimation of missing data and the use of measurement models to most accurately utilize scale measurements of suicidal ideation. Model fit was assessed using the Comparative Fit Index (CFI; Bentler 1990), the Root Mean Square Error of Approximation (RMSEA; Browne and Cudeck 1993), and chi-square statistics. According to Kaplan (2000), the model demonstrates adequate fit to the data if the chi-square is not significant, the CFI is above 0.9, and the RMSEA is at or below 0.05.
Results
Descriptive statistics, demographic variables, and zero-order correlations of intensity of suicidal ideation, deviant peer affiliation, and reliance on peers are presented in Table 1. Because deviant peer affiliation had skewness of 1.85 (SE = 0.22) and kurtosis of 4.31 (SE = 0.44), this variable was normalized using Templeton’s (2011) two-step transformation to produce standardized z-scores. Intensity of suicidal ideation was positively correlated with deviant peer affiliation (r = 0.32, p<0.01) such that those who affiliated with deviant peers were more likely to report increased intensity of suicidal ideation. Additionally, intensity of suicidal ideation was related to income to needs ratio (ratio of family income to the poverty threshold for family size) and was also included as a covariate (r = 0.18, p<0.01). Deviant peer affiliation was also significantly associated with reliance on peers for attachment (r = 0.28, p <0.01) and adolescent age (r = 0.27, p<0.01). Substance dependence was marginally correlated with deviant peer affiliation (r = 0.18, p<0.10) and was therefore included as a covariate in subsequent analyses.
To test our hypothesis that reliance on peers as attachment figures and deviant peer affiliation would correspond to greater intensity of suicidal ideation, we ran a regression analysis including symptoms of depression and income to needs ratio as covariates (see Table 2). Deviant peer affiliation was significantly related to intensity of suicidal ideation (β = 0.34, t = 2.58, p = 0.01), as did income to needs ratio (β = 0.29, t = 2.33, p = 0.02). Neither symptoms of depression nor reliance on peers for attachment significantly contributed to the model. The R2 for this model indicated that, overall, these variables accounted for around 15% of the variance in intensity of suicidal ideation (p<0.001). We found good fit statistics for this model (χ2(14) = 17.94, p = 0.21; CFI = 0.91; RMSEA = 0.049 (90% CI [0.00, 0.10])).
Lastly, we tested our hypothesis that reliance on peers for attachment would be associated with deviant peer affiliation. Results from our regression analysis (see Table 3) indicated that reliance on peers for attachment significantly accounted for variance of deviant peer affiliation (β = 0.26, t = 2.93, p = 0.003) above and beyond substance abuse (β = 0.23, t = 2.51, p = 0.012), age (β = 0.16, t = 1.92, p = 0.056), and intensity of suicidal ideation (β = 0.39, t = 3.39, p = 0.001). Overall, this model accounted for around 32% of the variance in deviant peer affiliation in this sample of clinically suicidal adolescents (p <0.001). We found adequate fit statistics (Kaplan 2000) for this model (χ2(17) = 24.09, p = 0.12; CFI = 0.86; RMSEA = 0.061 (90% CI [0.00, 0.11])).
Discussion
The current study explored how two aspects of adolescents’ social networks (reliance on peers as attachment figures and deviant peer affiliation) are associated with the intensity of suicidal ideation in a clinical sample of suicidal adolescents. In support of our first hypothesis and consistent with previous literature (Prinstein et al. 2000; Winterrowd and Canetto 2013), deviant peer affiliation was associated with increased suicidality in this severely clinical population. We also found support for our hypothesis that reliance on peers for attachment would be related to deviant peer affiliation above and beyond the relationship with intensity of suicide ideation. These results support the hypothesis that early reliance on peers as attachment figures is related to affiliation with deviant peers, which has been identified in this and previous studies as a significant risk factor for increased suicidality. However, we did not find support for our hypothesis that reliance on peers as attachment figures would be related to intensity of suicidal ideation.
Several factors may account for the positive relationship between deviant peer affiliation and intensity of suicide ideation in our clinical sample. Previous research has posited that engagement in substance use is one possible mechanism through which deviant peers may confer risk for suicide ideation (Prinstein et al. 2000). In the current sample, adolescents reported low rates of substance abuse, and while a composite of SUDs was related to deviant peer affiliation, substance misuse did not emerge as significantly related to intensity of suicidal ideation. As a result, other potential mechanisms should be explored. Peer deviance was also related to greater use of peers as attachment figures in our sample. Using a developmental perspective, adolescents’ peer relationships serve many important adaptive needs in meeting affiliative and supportive needs (Bowlby 1969/1982; Rosenthal and Kobak 2010). However, peers are likely not able to adequately serve the protective and guiding functions provided by adult attachment figures (Rosenthal and Kobak 2010). One potential explanation of our findings regarding increased deviant peer affiliation among adolescents who rely on their peers as attachment figures may be inadequate parental monitoring. Caregiver monitoring of children’s whereabouts and activities provide caregivers with the opportunity to intervene and reduce adolescents’ dangerous, impulsive, and risky behaviors (Dishion and McMahon 1998). However, successful and constructive monitoring is limited if adolescents either choose to or are unable to turn to their adult caregivers during times of need. Contrary to our hypothesis, we did not find support for a significant relationship between reliance on peers for attachment and intensity of suicidal ideation. One possible explanation is that the quality of the peer group may be more important than the simple distinction between peer versus adult. It is possible that attachment to high quality (e.g., non-deviant), supportive peers may compensate for inadequate adult attachment relationships in this clinical sample. More research is needed to better understand the functions and contributions of adolescent social networks, especially in high-risk contexts such as suicide.
The tendency to rely on peers rather than adults as primary or secondary attachment figures may also be indicative of problems in the adolescent-caregiver relationship, such as parent-adolescent conflict, negative expectancies for caregiver availability/responsiveness, or disruptions in relationships with caregivers (Rosenthal and Kobak 2010). Although adolescents may replace parents/caregivers in the hierarchy because they are unavailable or unresponsive, it is also possible that parents may disengage from their attachment roles. This may occur in a variety of contexts, including if caregivers perceive their children to be difficult or experience high parenting stress. In fact, one study found that parents of high-risk adolescents tend to disengage from parental monitoring earlier in development increasing risk for problem behavior (Dishion et al. 2003). Further, research suggests that youths’ perceptions of maternal attachment are related to problem behaviors when combined with other risk factors (De Winter et al. 2018). Therefore, while speculative, increased reliance on peers versus adults among already high-risk adolescents may potentially compound existing risk for deviant peer affiliation and other negative outcomes related to suicidality.
Limitations and Future Research Directions
One major limitation of this study is its cross-sectional design. Due to the lack of temporal precedence, it was not possible to infer directionality between preference on the attachment hierarchy, peer deviance, and ideation intensity. Although prior studies have identified attenuated family ties as a risk for deviant peer affiliation (Dishion et al. 2012), further evidence is needed to determine the stability of parent-child attachments during childhood and adolescence and its relationship to risk in suicidal adolescents. Longitudinal designs are needed to explore directional effects and to better inform prevention efforts. The degree to which adolescents’ preferences for attachment figures are sensitive to change as a result of clinical interventions that target attachment security will also need to be tested with pre- and post-treatment measures derived from the IPI. Further, it would be important to systematically test direction of effects with cross-lagged panel designs. Lastly, generalizability is limited due to the clinical severity of the current sample of adolescents. While demographic diversity is a relative strength of this study, it is unclear if these findings would replicate in different samples of adolescents.
It has been an ongoing challenge to adequately assess the severity of suicidality in adolescents. If we can identify risk factors that differentiate the severity of risk, we may be able to intervene earlier and target known mechanisms to prevent the transition from ideation to attempt. Future directions will require extending these findings with longitudinal designs that will provide a better understanding of the direction of effects and the degree to which adolescents’ preferences for attachment figures are subject to change. Moreover, these results point to possible mediation models, which could disentangle the relationships between peer deviance, use of social networks for attachment purposes, and substance misuse. Future research should also explore these variables as potential mechanisms of treatment, especially in treatments such as ABFT and FE-NST, which are specifically designed to enhance access to a supportive, constructive adult relationship.
In sum, this study provided preliminary support for how adolescents’ social networks are associated with the intensity of suicide ideation in a clinical sample. The quality of parent and peer relationships is clearly important in understanding risk for adolescent suicidality; yet, it is difficult to measure adolescents’ social networks due to the changing interpersonal functions that these relationships serve for youth over the course of adolescence. This study used the IPI to assess how adolescents activate their social networks to serve attachment functions and to understand varying degrees of symptom severity in a sample of suicidal adolescents. These results place importance on the functions of social networks and possible consequences of problems in parent and peer relationships. Future research in this area can help inform prevention efforts for depressed and suicidal adolescents.
References
Ackard, D. M., Neumark-Sztainer, D., Story, M., & Perry, C. (2006). Parent-child connectedness and behavioral and emotional health among adolescents. American Journal of Preventive Medicine, 30(1), 59–66. https://doi.org/10.1016/j.amepre.2005.09.013.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory–II. San Antonio, TX: Psychological Corporation.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238–246.
Bloch, M. H. (2016). Editorial: reducing adolescent suicide. Journal of Child Psychology and Psychiatry, 57(7), 773–774. https://doi.org/10.1111/jcpp.12585.
Bowlby, J. (1969/1982). Attachment and loss: Vol. 1. Attachment. 2. New York: Basic Books.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Beverly Hills: Sage.
Cassidy, J. (1999). The nature of the child’s ties. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical implications (pp. 3–20). New York, NY: Guilford Press.
Colin, V. L. (1996). Human attachment. New York, NY: McGraw Hill Book Company.
Conner, K. R., Wyman, P., Goldston, D. B., Bossarte, R. M., Lu, N., Kaukeinen, K., & Hesselbrock, V. M. (2016). Two Studies of Connectedness to Parents and Suicidal Thoughts and Behavior in Children and Adolescents. Journal of Clinical Child and Adolescent Psychology, 45(2), 129–140. https://doi.org/10.1080/15374416.2014.952009.
Consoli, A., Peyre, H., Speranza, M., Hassler, C., Falissard, B., Touchette, E., & Révah-Lévy, A. (2013). Suicidal behaviors in depressed adolescents: role of perceived relationships in the family. Child and Adolescent Psychiatry and Mental Health, 7(1), 8 https://doi.org/10.1186/1753-2000-7-8.
Conway, P.M., Erlangsen, A., Teasdale, T.W., Jakobsen, I.S. & Larsen, K.J. (2017). Predictive validity of the Columbia-Suicide Severity Rating Scale for short-term suicidal behavior: a Danish study of adolescents at a high risk of suicide. Archives of Suicide Research, 21(3). https://doi.org/10.1080/13811118.2016.1222318
De Winter, S., Waters, T. E. A., Braet, C., & Bosmans, G. (2018). Middle childhood problem behaviors: testing the transaction between responsive parenting, temperament, and attachment-related processing bias. Journal of Child and family Studies, 27, 916–927.
Diamond, G.S., Kobak, R., Krauthamer, E.S., Levy, S.A., Herres, J.L., Russon, J.M. & Gallop, R.J. (in press). Attachment-Based Family and Non-Directive Supportive Treatments for Suicidal Youth: A Comparative Efficacy Trial. Journal of the American Academy of Child and Adolescent Psychiatry.
Dishion, T. J., Capaldi, D., Spracklen, K. M., & Li, F. (1995). Peer ecology of male adolescent drug use. Development and Psychopathology, 7, 803–824.
Dishion, T. J., Ha, T., & Véronneau, M. H. (2012). An ecological analysis of the effects of deviant peer clustering on sexual promiscuity, problem behavior, and childbearing from early adolescence to adulthood: An enhancement of the life history framework. Developmental Psychology, 48(3), 703 https://doi.org/10.1037/a0027304.
Dishion, T. J., & McMahon, R. J. (1998). Parental monitoring and the prevention of child and adolescent problem behavior: a conceptual and empirical formulation. Clinical Child and Family Psychology Review, 1, 61–75.
Dishion, T. J., Nelson, S. E., & Kavanagh, K. (2003). The family check-up with high-risk young adolescents: preventing early-onset substance use by parent monitoring [Special issue]. Behavior Therapy, 34, 553–571.
Fergusson, D. M., Woodward, L. J., & Horwood, L. J. (2000). Risk factors and life processes associated with the onset of suicidal behaviour during adolescence and early adulthood. Psychological Medicine, 30(01), 23–39.
Fulginiti, A., Pahwa, R., Frey, L. M., Rice, E., & Brekke, J. S. (2016). What factors influence the decision to share suicidal thoughts? A multilevel social network analysis of disclosure among individuals with serious mental illness. Suicide Life Threatening Behavior, 46, 398–412. https://doi.org/10.1111/sltb.12224.
Geoffroy, M. C., Boivin, M., Arseneault, L., Turecki, G., Vitaro, F., Brendgen, M., & Côté, S. M. (2016). Associations between peer victimization and suicidal ideation and attempt during adolescence: Results from a prospective population-based birth cohort. Journal of the American Academy of Child & Adolescent Psychiatry, 55, 99–105. https://doi.org/10.1016/j.jaac.2015.11.010.
Gipson, P. Y., Agarwala, P., Opperman, K. J., Horwitz, A., & King, C. A. (2014). Columbia-suicide severity rating scale (C-SSRS): Predictive validity with adolescent psychiatric emergency patients. Pediatric Emergency Care, 31, 88–94. https://doi.org/10.1097/PEC.0000000000000225.
Hazan, C., & Zeifman, D. (1994). Sex and the psychological tether. In K. Bartholomew & D. Perlman (Eds.), Advances in personal relationships: Vol. 5. Attachment processes in adulthood (pp. 151–178). London: Jessica Kingsley.
Horwitz, A. G., Czyz, E. K., & King, C. A. (2014). Predicting future suicide attempts among adolescent and emerging adult psychiatric emergency patients. Journal of Clinical Child & Adolescent Psychology, 44(5), 751–761. https://doi.org/10.1080/15374416.2014.910789.
Joiner, T. (2005). Why people die by suicide. Cambridge, MA, USA: Harvard University Press.
Kaplan, D. (2000). Structural equation modeling: foundations and extensions. Thousand Oaks: Sage.
Kobak, R., Rosenthal, N. L., Zajac, K., & Madsen, S. D. (2007). Adolescent attachment hierarchies and the search for an adult pair-bond. New Directions for Child and Adolescent Development, 117, 57–72. https://doi.org/10.1002/cd.194.
Muthén, L.K. and Muthén, B.O. (1998–2012). Mplus User’s Guide. Seventh Edition.
Los Angeles, CA: Muthén & Muthén Posner, K., Brown, G.K., Stanley, B., Brent, D.A., Yershova, K.V., Oquendo, M.A. et al. (2011). The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168, 1266–1277.
Prinstein, M. J., Boergers, J., Spirito, A., Little, T. D., & Grapentine, W. L. (2000). Peer functioning, family dysfunction, and psychological symptoms in a risk factor model for adolescent inpatients' suicidal ideation severity. Journal of Clinical Child Psychology, 29(3), 392–405. https://doi.org/10.1207/S15374424JCCP2903_10.
Prinstein, M. J., & Wang, S. S. (2005). False consensus and adolescent peer contagion: examining discrepancies between perceptions and actual reported levels of friends’ deviant and health risk behaviors. Journal of Abnormal Child Psychology, 33(3), 293–306. https://doi.org/10.1007/s10802-005-3566-4.
Roelofs, J., Onckels, L., & Muris, P. (2013). Attachment quality and psychopathological symptoms in clinically referred adolescents: the mediating role of early maladaptive schema. Journal of Child and family Studies, 22, 377–385. https://doi.org/10.1007/s10826-012-9589-x.
Rosenthal, N. L., & Kobak, R. (2010). Assessing adolescents' attachment hierarchies: differences across developmental periods and associations with individual adaptation. Journal of Research on Adolescence, 20(3), 678–706. https://doi.org/10.1111/j.1532-7795.2010.00655.x.
Saffer, B. Y., Glenn, C. R., & David Klonsky, E. (2014). Clarifying the relationship of parental bonding to suicide ideation and attempts. Suicide and Life-Threatening Behavior, 45(4), 518–528. https://doi.org/10.1111/sltb.12146.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 28–38. https://doi.org/10.1097/00004583-200001000-00014.
Templeton, G.F. (2011). A Two-Step Approach for Transforming Continuous Variables to Normal: Implications and Recommendations for IS Research. In Communications of the Association for Information Systems: Vol. 28, Article 4. https://doi.org/10.17705/1CAIS.02804
Wang, Y. P., & Gorenstein, C. (2013). Psychometric properties of the beck depression inventory-II: a comprehensive review. The Brazilian Journal of Psychiatry, 35, 416–431. https://doi.org/10.1590/1516-4446-2012-1048.
Winterrowd, E., & Canetto, S. S. (2013). The long-lasting impact of adolescents’ deviant friends on suicidality: a 3-year follow-up perspective. Social Psychiatry and Psychiatric Epidemiology, 48, 245–255. https://doi.org/10.1007/s00127-012-0529-2.
Wolff, J., Esposito-Smythers, C., Becker, S., Seaboyer, L., Rizzo, C., Lichenstein, D., & Spirito, A. (2014). Social-Cognitive moderators of the relationship between peer victimization and suicidal ideation among psychiatrically hospitalized adolescents. Journal of Aggression, Maltreatment, & Trauma, 23, 3 https://doi.org/10.1080/10926771.2014.883458.
Zisk, A., Abbott, C. H., Ewing, S. K., Diamond, G. S., & Kobak, R. (2017). The suicide narrative interview: adolescents' attachment expectancies and symptom severity in a clinical sample. Attachment and Human Development, 19, 447–462. https://doi.org/10.1080/14616734.2016.
Author Contributions
C.H.A.: analyzed the data and wrote the paper. A.Z.: collaborated with the data analysis and writing of the paper. N.B.: collaborated with the writing and editing of the paper. G.S.D.: designed and executed the study, edited the final manuscript. R.K.: designed and executed the study, collaborated with the data analysis and writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This study was conducted in accordance with the ethical standards of the University of Delaware Institutional Review Board and with the 1964 Helsinki declaration and comparable ethical standards.
Informed Consent
Informed consent/assent was obtained from all participants included in the study.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Abbott, C.H., Zisk, A., Bounoua, N. et al. Peer Deviance, Social Networks, and Suicide Ideation Intensity in a Clinical Sample of Adolescents. J Child Fam Stud 28, 796–804 (2019). https://doi.org/10.1007/s10826-018-01320-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-018-01320-5