
Abstract
Attention deficit hyperactivity disorder (ADHD) begins in childhood and is characterized by attention deficits, hyperactivity, or impulsiveness that is inconsistent with a child’s developmental level. The effects of ADHD are not limited to the child alone but can affect their familial context, particularly parenting styles. Using data from 68 parents of 6–11-year-old ADHD-diagnosed children, we attempted to identify the predictive variables of two parenting styles: criticism-rejection and permissiveness-indulgence. We analyzed two complex predictive models using structural equation modeling. We hypothesized that family impact variables would mediate the relation between the child’s behavior and parenting. The data showed that the child’s ADHD was only indirectly related to parenting styles, whereas child’s behavior problems had a direct relationship. The results stressed the central role of the child’s behavior on family social life, parents’ marital relationship, and parents’ feelings about their children. These variables mediated the relationship between the children’s disorders and parenting styles. On the other hand, perceived social support had an inverse relationship with this negative family impact, and it even had relevant indirect effects on criticism and permissiveness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The Diagnostic and Statistical Manual of Mental Disorders–5th edition (DSM-5TM) criteria for ADHD states that people with ADHD show a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development and is characterized by attention deficits, hyperactivity, or impulsiveness that is inconsistent with developmental level (American Psychiatric Association 2013). Many children and adolescents with ADHD have trouble controlling their behavior and following the norms expected for their age, which a source of problems with adapting to their development settings. In this sense, it should be underlined that the effects of ADHD are not limited to the child alone but can affect their closest social contexts and, of course, their family context (Johnston and Mash 2001).
Although it is true that family dynamics are not considered a cause of ADHD, bidirectional influences (parent-to-child and child-to-parent processes) do seem to be the key to the disorder’s course (Johnston and Jassy 2007; Pardini 2008). The behavior of children with ADHD poses strong challenges for parents, generating high levels of anxiety and family stress (Donenberg and Baker 1993; Podolski and Nigg 2001). However, family dysfunctions or maladaptive parenting styles can also aggravate both children’s ADHD symptoms and their psychological adjustment (Deault 2010; Haack et al. 2014). Several studies have been conducted from this bidirectional perspective. Some genetically based works analyze the decomposition of effects into genetic and environmental influences that can explain parent–child relationships (e.g., Harold et al. 2012, 2013). From a developmental perspective, some models have stated that children are not passive recipients of parents’ behaviors; rather, they can actively impact parenting practices and influence their environment (Bell 1968; Mischel 1973; Pearl et al. 2014). A similar model developed by Patterson (1982, 2002) has proposed a circular theory: the child’s negative behaviors increase the probability that parents will use harsh and negative discipline styles, which in a circular, negative interchange, reinforce the child’s conduct problems. The model emphasizes the relevance of identifying mediating variables on which to base intervention programs to break this escalation of inadequate parent–child interchanges.
Although a majority of developmental studies have shown that parenting has an impact on disruptive behaviors, some works have suggested that the child’s disruptive behavior influences parenting more than parenting influences the disruptive behavior. Thus, ineffective parenting practices may be a result of child’s conduct problems rather than a source of the child’s behaviors (Burke et al. 2008; Fite et al. 2006). Within this child-to-parent directional approach, many researchers have found that the severity of a child’s ADHD predicts parenting style, usually increasing the probability of recurring negative or maladaptive parenting patterns, such as permissiveness or emotional overreaction (Kaiser et al. 2011; Lange et al. 2005; McLaughlin and Harrison 2006). Furthermore, recourse to such inappropriate disciplinary techniques is more frequent when children with ADHD also present associated behavior problems (Johnston and Jassy 2007). Thus, it seems unquestionable that both ADHD symptoms themselves and comorbid problems negatively influence family functioning as a whole and parenting styles in particular. However, it is advisable to separate the effects of the two problems. In fact, some studies have reported that parenting styles are strongly associated with comorbid behavior problems in children but not with the severity of ADHD (Deault 2010; McLaughlin and Harrison 2006).
Although it is true that the same type of parenting practices may have different effects in different ethnic or cultural groups (Javo et al. 2004), several studies have shown that negative parenting is more related than positive parenting to children’s disruptive behavior. In fact, it is not very clear whether some practices, such as positive parenting or the parental use of inductive reasoning, are related to the severity of problematic child behaviors such as ADHD symptoms (Cussen et al. 2012; Haack et al. 2014; Sollie et al. 2016). There is more agreement that conduct problems are strongly associated with negative parenting practices (Kaiser et al. 2011; Lange et al. 2005; McLaughlin and Harrison 2006). Even from a practical point of view, in psychosocial interventions to improve a child’s functioning, it is more impactful to decrease negative parenting than to increase positive parenting (e.g., Haack et al. 2016).
Given that children’s disruptive behaviors increase negative parenting practices, the question then becomes “What variables could play an intermediate role in these interchanges, and how can they be used to refine prevention and intervention strategies?” As Belsky (1984) stated, an ecological view of this question requires the consideration of the context of the child-parent relationship. With this in mind, social support and family functioning variables have been identified as characteristics related to both children with ADHD (and co-morbidities) and parenting. First, research has shown a strong relationship between child ADHD and family dysfunction (e.g., Lange et al. 2005; Sollie et al. 2016). Thus, measures of the effects of family dynamics that break down the impact of children’s ADHD on different areas of the family context, such as the parent’s feelings and attitudes about the child, marital relations or the family’s social life, should also be considered (Bauermeister et al. 2010; Donenberg and Baker 1993). On one hand, a child’s ADHD and/or conduct problems impact social family life, marital relations and feelings about parenting; greater severity of conduct problems is associated with a greater effect on the family’s social life and lower participation in social events, reduced agreement between parents about child-parent interactions, and more negative feelings and attitudes of parents toward their child (Fleck et al. 2015; Shelton et al. 1998). On the other hand, family dysfunctions were significantly positively correlated with harsh/coercive parental discipline: the greater the number of family problems, the greater the probability of negative parental practices (Jansen et al. 2012; Sanders et al. 2014). Although some research has suggested that the effects of child conduct problems on parenting were indirect and completely mediated by the parents’ psychological well-being, including parental stress (Abidin 1990; Nam and Chun 2014), to the best of our knowledge, no studies have analyzed the mediating role of these family problems in child-parent processes. Thus, it would be a challenge to analyze the mediating role of different aspects of family life on the relationship between child problems and parenting styles.
Second, an abundance of evidence highlights the strong relationship between perceived social support and both the severity of child ADHD (or conduct problems) and parenting styles. Bringing up a child with ADHD is usually a serious challenge, particularly if there is no help from family or close relatives. Unfortunately, several studies have shown that the families of children with ADHD perceive having less social support and experience more social isolation than control families (Gau 2007; Lange et al. 2005). Other works stated that when social support decreased, child behavior problems increased (Akcinar and Baydar 2016; Mash and Johnston 1983). Moreover, this feeling of being alone and lacking social and family support is in turn related to less effective parenting (McLaughlin and Harrison 2006; Wallace 2013). In fact, family social support is closely related to parenting, either directly or indirectly through parental variables such as self-efficacy or psychological well-being (DeGarmo and Forgatch 1997; Forgatch and DeGarmo 1997; Izzo et al. 2014).
Given the importance of this issue, in this study, we attempted to analyze the variables most related to parenting styles in a sample of families with children with ADHD. Similar to the work of Burke et al. (2008), we stated a relationship from child ADHD (and/or conduct problems) to parenting styles. Furthermore, as in Belsky’s (1984) model, we have added two contextual variables: social support and impact on family life (measured as family functioning). Of particular interest in the present study is the mediating role of the impact on family life. Additionally, we concentrated on two negative parenting styles, authoritarian and permissive, which have been shown to be associated with negative child outcomes. We therefore analyzed the association of child and contextual variables with criticism from parents—given the high presence of this manifestation of authoritarian style in research with families of children with ADHD—and with overindulgence in the interactions with children, the typical expression of a permissive parenting style. We further considered the separate contribution of ADHD symptom severity and comorbid child behavior problems. However, no studies to date have examined the possible pathways by which child, family, and contextual variables may work together to predict parenting styles. In an attempt to respond this question, we have established the hypotheses shown in Fig. 1, which specifies the relationships among the analyzed variables, which were derived from the review of the scientific literature. Although it is a single illustration, it shows two models: one for the authoritarian style (criticism) and the other for the permissive style (indulgence). We hypothesized that (A) criticism (or indulgence) levels are directly related to (1) the child’s ADHD severity; (2) the child’s behavior problems; and (3) the impact of the child’s conduct and problems on (a) the parents’ marital relations, (b) the family’s social life, and (c) the feelings and attitudes of parents toward their child. Moreover, we expected that (B) child behavior problems and ADHD severity would be associated with a negative impact on marital relations, the family’s social life, and the parents’ feelings toward their children. (C) Perceived social support would also relate to the negative impact variables. Additionally, we hypothesized (D) that the child’s ADHD severity, the child’s behavior problems, and social support would have indirect effects on criticism (or indulgence) levels through their negative impact on marital relations, the family’s social life, and the parents’ feeling toward their child. Finally, we established (E) that the child’s ADHD severity is related to the child’s behavior problems and (F) that there is a close relationship between ADHD severity and perceived social support.

Theoretical model of parental criticism/authoritarianism and indulgence/permissiveness
Method
Participants
Sixty-eight families with girls or boys aged 6–11 years who were diagnosed with ADHD agreed to participate in this study. Table 1 shows the main characteristics of the children and their families.
As the table shows, most of the children were diagnosed with the combined or inattentive subtype. The mean length of time that the families had been living with the diagnosis of ADHD was 3 years (36.63 months, with a range of 0–96 months). Table 1 shows the most important comorbid problems, although all the families were asked about different types of associated problems, such as substance use or anxiety. Specifically, problems related to learning appeared in 32% of the cases studied.
Procedure
To recruit families, the research team visited educational assistance centers for children with ADHD and associations for families with children and adolescents with ADHD in Huelva (Spain). Professionals working with children and families sought the parents’ voluntary participation in the study. The mothers and fathers provided all the information through a self-report questionnaire, including socio-demographic variables and their children’s characteristics, diseases, and comorbid problems. The child’s ADHD was determined via a previous professional diagnosis (usually pediatricians (60%) or psychologists (40%) who worked with the family associations) according DSM-IV criteria and following Health Authority (Spanish Ministry of Health) recommendations (Ministerio de Sanidad, Política Social e Igualdad 2010).
Of the 90 families contacted to participate in the study, 68 completed the questionnaires, for a 75% response rate. The families completed the questionnaires at home and returned them through the associations and educational centers. The characteristics of the children participating in this study largely coincided with those of other studies carried out with Spanish children, especially in terms of the boys/girl ratio and the most common comorbidities (Catalá-López et al. 2012; Informe PANDAH 2015).
Measures
Criticism-rejection scale
(Bersabé et al. 2001, original version in Spanish). This scale comprises10 five-point Likert-type items (from 1, “Never,” to 5, “Always”). High scores are interpreted as symptoms of criticism, rejection, anger, lack of confidence, and general lack of acceptance of the child’s behavior (characterizing an authoritarian parenting style). Example of the items include “I criticize him/her for everything” and “I get angry about everything she/he does.” Bersabé et al. (2001) provided evidence of the reliability and validity of scores on this scale (internal consistency equal to .81). Salas et al. (2015) found alpha = .78. In this study, Cronbach’s alpha was .77.
Indulgent educational style scale
(Bersabé et al. 2001, original version in Spanish). This scale comprises 10 five-point Likert-type items (from 1, “Never,” to 5, “Always”) that measure parental permissiveness. Item examples include “As long as he/she is happy, I let him/her do whatever he/she wants” and “I don’t care if he/she obeys or not.” The scale has acceptable psychometric properties; Bersabé et al. (2001) and Salas et al. (2015) reported internal consistency values of .64 and .75, respectively. In this study, Cronbach’s alpha was .76.
Child behavior problems
The behavior problems subscale of the Strengths and Difficulties Questionnaire (SDQ-CAS) was used as a measure of child behavior problems (Goodman 1997. We used the Spanish version, available at http://www.sdqinfo.org/py/sdqinfo/f0.py). The scale comprises five Likert-type items (rated from 0, “False,” to 2, “Absolutely true”). Examples of items include “Often loses temper” and “Often lies or cheats.” Some studies have shown adequate reliability for the Spanish version (α = .74, Gómez-Beneyto et al. 2013; and α = .62, Rodríguez-Hernández et al. 2012). In this study, Cronbach’s alpha was .68.
Child ADHD symptomatology
This variable was explored using Conners’ Parent Rating Scale (Conners 1997; Spanish version by Farré-Riba and Narbona 1989), which consists of 10 items with answer choices from 0, “Not at all,” to 3, “A lot” (sample items include “Inattentive, easily distracted” and “Excitable, impulsive”). The internal consistency in this study was .83. Reliability and validity have been established for the Spanish version (e.g., Salas et al. 2015; alpha = .92).
Impact on parent feelings and attitudes scale
Donenberg and Baker (1993) (Spanish adaptation by Presentación et al. 2006) comprises 15 items. High scores indicate negative feelings and attitudes of parents toward their child (e.g., “My child brings out feelings of frustration and anger more,” “My child’s behavior bothers me more”). The answer choices on the items range from 0, “Not at all,” to 3, “Very much,” although the items are coded as 0, “No impact,” or 1, “Impact,” following the recommendations of the authors of the Spanish version. In this study, Cronbach’s alpha was .84.
Impact on social family life scale
Donenberg and Baker (1993) (Spanish adaptation by Presentación et al. 2006) comprises 10 items, which are coded as 0, “No impact,” or 1, “Impact.” It shows the degree to which the child’s behavior negatively affects the family’s relationships and participation in social events (e.g., “My family avoids social outings more (e.g., restaurants, public events) because of his/her behavior,” “I have guests over to our house less often than I would like to because of my child’s behavior”). The Cronbach’s alpha was .79 in the current study.
Impact on marital relations scale
Donenberg and Baker (1993) (Spanish adaptation by Presentación et al. 2006) comprises seven items (0, “No impact,” or 1, “Impact”) that measure the extent of distancing or disagreement between the members of the couple with regard to the child’s behavior (e.g., “My child causes more disagreements between my spouse and me”). The Cronbach’s alpha was .78 in the current study. Presentación et al. (2006, 2009) showed that the Spanish version of for the “Parent Feelings and Attitudes Scale,” the “Impact on Social Family Life Scale” and the “Impact on Marital Relations Scale” have adequate psychometric properties.
Perceived social support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al. 1988; Spanish version by Landeta and Calvete 2002) comprises 12 seven-point Likert-type items, from 1, “Very strongly disagree,” to 7, “Very strongly agree.” It evaluates the person’s perception of social support from family, friends and especially relevant people (e.g., “I get the emotional help and support I need from my family,” “I have friends with whom I can share my joys and sorrows”). The MSPSS Spanish version has been demonstrated to have adequate internal consistency (α = .89, Buesa and Calvete 2013; and α = .89, Landeta and Calvete 2002). Internal consistency in the present study for the composite “Perceived Social Support” score (α = .91) was high.
Data Analyses
We analyzed the data using SPSS 19. After checking for outliers, missing data, and the assumptions of linearity, normality, and homoscedasticity, we examined the means, standard deviations, and intercorrelations of the study variables. Next, we conducted several ANOVAs, t-tests and correlations analyses to study the relationships between each variable in the models and the clinical and socio-demographic variables to determine whether we would need to control for demographic variables in subsequent analyses.
We used AMOS v. 24 to analyze the two structural equation models and to test the direct and indirect effects. To determine the overall model fit, we used the χ 2 test, the non-normed fit index (NNFI/TLI > 0.90), the comparative fit index (CFI > 0.90), and the root mean square error of approximation (RMSEA < 0.08) (Kline 2005). In each model, the children’s problems, family and contextual variables, and one parenting style (criticism-rejection or indulgence-permissiveness) were entered simultaneously. A bootstrapping procedure was used to assess the direct and indirect effects (using 10,000 resamples) to obtain the 95% bias-corrected confidence intervals (BC CIs). A CI that did not include zero indicated a significant direct or indirect effect. This approach provides a more powerful test of effects than other approaches in small samples (Woody 2011).
To determine the extent to which our sample size was sufficient, we tested alternative models (Bentler 2006). The sample size is considered adequate and sufficient if it has the statistical power necessary to reject incorrect models (MacCallum et al. 1996). In this study, we therefore tried 12 alternative models (six with criticism-rejection and six with indulgence-permissiveness) with the same number of parameters and degrees of freedom but exchanged the independent variable (IV: one measure of impact on family life), dependent variable (DV: one measure of impact on family life), and mediating variables (MV: parenting style, perceived social support, child ADHD, child conduct problems, and one measure of impact on family life). For example, in the first alternative model, IV = impact on marital relations, DV = impact on social family life, and MV = the rest of the variables. Statistical power was calculated using the Preacher and Coffman (2006) software. Assuming a null hypothesis of close fit (H 0: RMSEA = 0.05) and an alternative hypothesis of unacceptable fit (H A: RMSEA = the RMSEA value of each alternative model), a power analysis with α = 0.05 indicated that the level of statistical power was high. The values were RMSEA (average = .252; minimum = .133; maximum = .360) and statistical power (average = .95; minimum = .60; maximum = .99).
Moreover, using the empirical power tables for the mediation models of Fritz and MacKinnon (2007), we concluded that the sample size of this work was sufficient (N = 54 in the table) to detect a mediated effect (power = .80 and large to medium paths; α = .59 and β = .39). When we used medium paths (α = .39 and β = .39), our sample size was near the N = 71 reported in the table.
Results
First, we analyzed the relationships of the variables included in the structural equation models with all the socio-demographic and clinical variables presented in Table 1 using correlations for continuous variables and t-tests or univariate ANOVAs to examine the between-groups differences for categorical variables. Significant associations were not found, and the effect sizes were small to medium. The higher correlation was .25—time from diagnosis with the impact on the family’s social life; the higher Cohen’s d was .44—indulgence-permissiveness with gender; and the highest eta squared was .06–subtype of ADHD with ADHD severity. Consequently, these demographic and clinical variables were not entered as covariates in the subsequent analyses.
Table 2 shows the means, standard deviations and correlations of the variables analyzed in this study. We should mention that the mean for child’s behavior problems in this sample was on the borderline between normality-abnormality (41% of the children had scores of 4 or higher, which is abnormal or clinical based on Goodman’s (2016) criteria). Low scores predominated in the measurements of impact. For example, on the Impact on Social Family Life Scale, only 23% of the parents had scores of 3 or higher.
The correlations and their signs were as expected based on theory and previous data. Most of the variables had statistically significant high correlations with one another. The criticism-rejection variable was highly correlated with almost all the variables, whereas indulgence-permissiveness was more moderately correlated. The impact measurements were associated with one another, with the dependent variables and with social support, conduct problems and ADHD severity. Furthermore, these two variables were closely related.
Prediction Models
Based on the theoretical relationships specified in Fig. 1, we estimated the fit indices and parameters of two different models, one for criticism-rejection and the other for indulgence-permissiveness. Although both models showed acceptable indices of fit, we found non-significant parameters and high modification indices, which suggest the inclusion of new direct paths. However, before making any modification of the original model, we considered whether these changes were theoretically acceptable and occurred in both the criticism-rejection and indulgence-permissiveness prediction models. Otherwise, to control the capitalization on chance, the statistical significance level of the dropped parameters was higher than .20, and the added parameters had a significance level lower than .001.
First, the model modification indices proposed adding one new parameter relating impact on marital relations with parental feelings and attitudes. After adding this new relationship, we proceeded to eliminate non-significant parameters that appeared in both models. The models resulting from these modifications are shown in Fig. 2 (A and B, for criticism-rejection and indulgence-permissiveness, respectively). These models fit satisfactorily and are explained in detail below.

Standardized parameters for CRIT (top) and INDUL (bottom) model. CRIT criticism-rejection of the child’s behavior/problems, INDUL parents’ indulgence-permissiveness, MARI impact of child’s problems and behavior on parents’ marital relations, SOC impact of child’s problems and behavior on the family’s social relationships, FEEL parents’ feelings and attitudes toward their child, BHVR child’s behavior problems, ADHD child’s attention deficit hyperactivity disorder symptoms, SUPP perceived social support. Bootstrapped 95% bias-corrected confidence intervals are in brackets (lower/upper)
Prediction of family impact measurements. Since the data for the parameters analyzed in this section were the same in both models, they were analyzed as if there were only one, and the analysis was applicable to both the criticism-rejection and indulgence-permissiveness prediction models (Fig. 2). The model explained up to 54% of the variability in scores for parents’ feelings and attitudes toward their child. Conduct problems were positively and significantly related to parents’ feelings and attitudes. To a lesser extent, impact on marital relations was associated with parents’ feelings and attitudes. Moreover, the parents’ feelings and attitudes variable was indirectly related to social support (through impact on marital relations) and ADHD (mainly through conduct problems; see Table 3 for indirect effects). The model further explained 47% of the variance in scores on impact on social life. Behavior problems (positive path coefficient) and social support (negative path coefficient) were related to the impact of the children’s problems on the family’s social life. Child ADHD severity is indirectly related to the impact on the family’s social life through child conduct problems. Impact on marital relations was associated with social support (path coefficient = −.39; 95% BC CI = −.64/−.13) and child ADHD symptoms (path coefficient = .18, 95% BC CI = −.01/.38), Thus, the higher the score on the Conners’ scale, the higher the score for impact on marital relations. In contrast, the higher the social support, the lower the impact on the couple’s relationship. The model explains 24% of the variance of the impact on marital relations. As the correlation matrix shows, a significant correlation between ADHD and perceived social support (−.41) appeared in both models. Furthermore, child ADHD severity was strongly related to child behavior problems.
Prediction of criticism-rejection. The criticism-rejection model explained 58% of the dependent variable. The variability of the criticism-rejection scores was associated primarily with the impact on family social life (Fig. 2a). Significant direct paths of parent feelings and attitudes, behavior problems and impact on marital relations also appeared. Perceived social support had a significant overall indirect effect on criticism-rejection (see Table 3). This indirect effect was especially manifested through the impact on the family’s social life: The more social support available, the fewer negative effects on the family’s social life; the less impact on the family’s social life, the lower the levels of rejection or criticism of the child. Similarly, the child’s ADHD severity had a relevant indirect effect on criticism-rejection through the impact on parents’ marital relations and, mainly, the child’s behavior problems.
Finally, the possible effects of mediation via the impact on the family’s social life and parents’ feelings and attitudes on the relationship between conduct problems and criticism-rejection should be emphasized. To test the hypothesis of mediation, we verified that it fulfilled the following criteria (Judd et al. 2001; MacKinnon and Dwyer 1993): (a) a direct effect of the predictive variable (behavior problems) on the predicted variable (criticism-rejection) (c’ = .23; 95% BC CI = .01/.48, see Fig. 2a), (b) a direct effect of the predictor (behavior problems) on the mediating variables: impact on the family’s social life (α 1 = .43; 95% BC CI = .24/.61) and parents’ feelings and attitudes (α 2 = .60; 95% BC CI = .42/.78), (c) a direct effect of the mediating variables impact on the family’s social life (β 1 = .35; 95% BC CI = .16/.57) and parents’ feelings and attitudes (β 2 = .23; 95% BC CI = .01/.42) on the predicted variable (criticism-rejection), and (d) an indirect effect of the predictor (behavior problems) on the predicted variable (criticism-rejection) through the mediating variables ([α 1*β 1]+[α 2*β 2] = .29; 95% BC CI = .15/.45, see Table 3). We therefore conclude that there is a mediating effect: impact on the family’s social life and parents’ feelings and attitudes mediate in the relationship between behavior problems and criticism-rejection.
Additionally, regarding causal direction, we estimated the fit of one model for criticism-rejection by reversing the path directions, i.e., with criticism-rejection as the independent variable (IV), child ADHD as the dependent variable (DV), and the rest of the variables as mediating variables (MV). This reverse model fit worse than our model: χ 2 (9) = 12.71, p = .18, NNFI = 0.96, CFI = 0.98 RMSEA = 0.078.
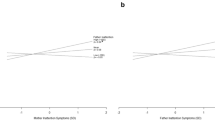
Prediction of indulgence. The specified model explained 24% of the variance in indulgence-permissiveness (Fig. 2b). The variable with the most weight was impact on marital relations, followed by conduct problems. The weights of impact on the family’s social life and parents’ feelings and attitudes were non-significant. Both social support and ADHD severity had important indirect effects through impact on marital relations (Table 3). To verify the extent to which impact on marital relations mediates the relationship between social support (and ADHD) and indulgence-permissiveness, we divided the matrix into two groups based on the median of the impact on marital relations scores. One group was made up of the families who said they experienced little or no impact on their marital relations, and the other comprised the families who said they experienced a medium to high impact. For each group, we analyzed the relationship between social support (and ADHD) and indulgence-permissiveness (see Fig. 3).

Relationship between child’s ADHD symptoms (top), perceived social support (bottom) and indulgent style, controlling for impact on marital relations. Low MARI = families who said they experienced little or no impact on their marital relations; High MARI = families who said they experienced a medium to high impact on their marital relations. * p < .05; ** p < .01; n.s. not significant
Figure 3 shows two interaction effects between social support (and ADHD) and impact on marital relations that predict indulgence-permissiveness (as moderating, not mediating, effects). In families that perceived a low impact or change in their marital relations, there was no relationship between the levels of ADHD symptoms of their children and indulgent parenting scores, whereas, when the perceived impact of ADHD symptoms on the couples’ relationship was high, there was a high direct relationship between the child’s ADHD and indulgent parenting. Additionally, at low levels of perceived social support, permissiveness was high, but only in those families in which the child’s ADHD symptoms had a strong impact on marital life. The families with low levels of impact showed low levels of permissiveness, regardless of perceived social support.
As we did previously with the criticism-rejection model, we estimated the fit of one model for indulgence-permissiveness by reversing the path directions, i.e., with indulgence-permissiveness as the IV, the child’s ADHD as DV, and the rest of variables as MV. This reverse model did not fit: χ 2 (9) = 33.59, p = .00, NNFI = 0.64, CFI = 0.84 RMSEA = 0.200.
Discussion
Our purpose was to identify predictive variables of parenting styles, specifically of two maladaptive parenting styles, criticism-rejection and permissiveness-indulgence. We hypothesized, as Burke et al. (2008) suggested, a direct (and indirect) relationship from child ADHD or conduct problems to criticism-rejection or permissiveness-indulgence. We also hypothesized that perceived social support had direct and indirect relationships with criticism-rejection or permissiveness-indulgence. Moreover, the current study extends previous studies by providing empirical support for the mediating role of the impact on the family in the relationship between child variables and parenting styles. The findings partially support our hypotheses: the models explain a significant amount of the variance in criticism-rejection (or permissiveness-indulgence) according to the child’s ADHD and social support—directly or, mainly, indirectly—through the family impact variables.
Although the parenting style was only indirectly associated with the child’s ADHD, it was directly related to the child’s behavior problems. In both models, this last variable had a significant direct positive effect, increasing permissiveness and rejection or criticism. These data coincide with other studies that emphasize the major role of behavior problems comorbid with ADHD in the use of inappropriate parenting practices, even after controlling for child´s ADHD symptoms profile (Fleck et al. 2015, Sollie et al. 2016). In contrast, child ADHD was not directly related to parenting style when behavior problems were included in the predictive model, suggesting an indirect relationship (e.g., Deault 2010; McLaughlin and Harrison 2006).
We would like to stress the central role of the impact on the family on the children’s disorders and parenting styles. As described in previous studies, the child’s ADHD and behavior problems have a severe negative impact on the parents’ marital and social life and negatively influence parents’ attitudes and feelings toward their children (Bauermeister et al. 2010; Lambek et al. 2014). In this study, such feelings were much more strongly influenced by the child’s behavior problems than by ADHD symptoms themselves, a finding consistent with other research in the same subject (McLaughlin and Harrison 2006). However, the degree of perceived social support seems to reduce the negative impact of children’s behavior on the parents’ marital and social relations and to have an indirect positive influences on parents’ feelings and attitudes. These results agree with other studies that reported that social support is a family resilience factor that reduces parental stress (Bozo et al. 2010; Weiss 2002).
More interesting is the mediating role exerted by the family impact variables. The three measurements of family impact were associated with criticism-rejection, but permissiveness was related primarily to the impact of child factors on marital relations. Children’s behavior problems generate criticism from the parents, especially because they generate negative feelings and alter the family’s social life. In contrast, ADHD symptomatology was closely related to parental permissiveness, but only in families where the child’s ADHD had a very negative impact on the parents as a couple. Thus, parenting styles are more associated with the effects of the child´s behavior in family and marital life than with the child´s disorder itself. The different relationship patterns observed in the models are a relevant area of interest. Indulgence-permissiveness was primary related to the impact on marital relations, whereas criticism was more related to the impact on the family’s social life. An explanation could be that marital disagreement or distancing could lead to laxness, minimal supervision and inaction due to the different points of view about parent-child interactions. On the other hand, the more affected the social life of the family was (e.g., because of reductions in social contacts caused by the child’s behavior in public), the greater the probability that parents trying to control the child behave in an authoritarian way by showing anger or rejection. Finally, the impact on marital relations had a relevant direct (or indirect) effect on both parenting styles: high levels of marital problems were associated with high levels of negative parenting practices. These findings are consistent with the Belsky (1984) model, which emphasizes the central role of the marital relations in the process model of the determinants of parenting. Since we do not know of previous studies that analyzed these impact variables and relationships, we think it would be desirable for future research to verify this mediating (or moderating in permissiveness model) role in other contexts and populations.
Our data also coincide with those of other authors by showing an inverse relationship between perceived social support and the child’s ADHD or behavior problems (Akcinar and Baydar 2016; Gau 2007; Lange et al. 2005; Mash and Johnston 1983). Although perceived social support did not have a direct effect on parenting styles, its effect was in the same direction described in other studies that showed its close relationship with parenting styles (DeGarmo and Forgatch 1997; McLaughlin and Harrison 2006). Belsky (1984) asserted that support enhances parenting, sometimes directly but more often through its influence on other mechanisms relevant to parenting, such as well-being. In our data, social support was negatively related to the negative impact that children’s problems have on family dynamics, and it even had relevant indirect effects on criticism (reducing the negative effect on the family’s social life) and permissiveness (mitigating the effects of the child’s ADHD on the parents’ marital relations). To better understand these indirect effects, it could be interesting to distinguish different sources of support: couple, friends, or family. Our data show that for families in which the parents’ relations are severely altered by their child’s problems, social support was negatively associated with parental permissiveness. In such cases, the support of the other parent was the strongest determinant. Parents who felt supported by their partners had a high sense of parental competence and reported greater agreement with their partners (Belsky 1984). Furthermore, as we stated previously, the greater the agreement within the couple, the greater the probability of reducing the levels of indulgence-permissiveness. On the other hand, the indirect effect of social support on criticism-rejection through the impact on the family’s social life could be explained by the family’s source of support, mainly by the instrumental support—e.g., having someone who can take care of the children so that their parents can participate in social events. Family instrumental support could reduce the impact of the child’s behavior on the family’s social life and indirectly reduce the associated high levels of rejection and criticism. This source of support was usually the most important in the Latino/Spanish culture (e.g., Bélanger et al. 2016). Unfortunately, we used only a global, undifferentiated measure of social support and could not separately analyze diverse sources of support. Future research should incorporate these differences.
From the viewpoint of intervention in families with children with ADHD, we agree with other authors (e.g., Presentación et al. 2009) who underscore that interventions with families should include a continued counseling for parents in the affective dimensions of their behavior with their children, providing them not only with techniques for managing child behavior but also problem-solving, cognitive restructuring and relaxation skills to reduce their psychological and emotional stress, and enabling them to use effective discipline and appropriate communication with their children. The effectiveness of some programs or therapies, such as behavioral parent training programs (e.g., Chacko et al. 2008; Chronis et al. 2004; Fabiano et al. 2012) and mindfulness-based therapy or mindful parenting (Corthorn and Milicic 2016; Haydicky et al. 2015; Singh et al. 2010), has been demonstrated. Some of these studies refer to clinically significant changes in various dimensions of family functioning, such as those related to educational strategies or parental stress, and even progress from clinical to normal levels (Gerdes et al. 2012).
Limitations
Despite the relevance of our findings, they should be interpreted keeping in mind some limitations of our study. First, we are aware that a cross-sectional study such as ours cannot extract definitive conclusions regarding cause-and-effect relationships among the variables analyzed. We have presented evidence of statistical mediation, but true mediation requires temporal separation of predictor, mediator, and criterion variables (MacKinnon et al. 2007). However, by testing and rejecting alternatives to the proposed models (with a worse fit), we provide some evidence supporting the hypothesized models. Future research should utilize longitudinal designs to further investigate the developmental pathway between child ADHD and parenting styles.
Second, inattentive cases represent a sizable proportion of our sample. However, some works have shown that inattentive symptoms (predominantly inattentive presentation—ADHD-I) was associated with inconsistent parental discipline, with almost the same correlation coefficient as hyperactive/impulsive symptoms (Sollie et al. 2016) or significantly predict negative parenting (Haack et al. 2014). Moreover, in our sample, we analyzed the differences in ADHD severity or conduct problems among the groups with combined (ADHD-C), predominantly inattentive (ADHD-I), and predominantly hyperactive (ADHD-H) presentations. No significant differences were found. Although we think that this did not significantly affect our findings, future research using a larger sample size could fit the models to these different groups.
Third, the sample size did not allow us to conduct a separate analysis by the gender of child and/or parents. Other studies have highlighted parent and child gender as sources of variability in parent-child relationships (e.g., Sturge-Apple et al. 2004). For example, mothers seem to be more observant and responsive to their children’s behavior than fathers, so their lives would presumably be altered to a greater extent (Calzada et al. 2004). Additionally, ADHD symptoms in boys affect family functioning more than those in girls (Bauermeister et al. 2010), and ADHD symptoms in sons are treated more harshly than in daughters (Maniadaki et al. 2005), which may lead to more negative feelings about such behavior. Related to sample size, a further limitation of this study was the limited statistical power to detect or reject a small/medium moderator effect at the conventional alpha level of 0.05 (Shieh 2009). Because of this, we could not calculate the moderator effects found in the indulgence model. It would be interesting to analyze these moderator effects in future research using a larger sample size.
Finally, this work does not discuss the role of culture in moderating the relationship between parenting styles and child or family variables. Some research literature suggests these parent–child relationships might not have the same meanings in families with different racial, ethnic or cultural contexts (e.g., Bornstein 2012; Rudy and Grusec 2006). We think that in future studies, it would be interesting to test the extent to which the findings of this study would yield different results based on the gender of the parents or children or their sociocultural contexts.
References
Abidin, R. R. (1990). Parenting stress index manual. (3rd ed.). Charlottesville, VA: Pediatric Psychology Press.
Akcinar, B., & Baydar, N. (2016). Development of externalizing behaviors in the context of family and non-family relationships. Journal of Child and Family Studies, 25, 1848–1859. doi:10.1007/s10826-016-0375016-0375-z.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5™). Arlington, TX: Author.
Bauermeister, J. J., Puente, A., Martinez, J. V., Cumba, E., Scandar, R. O., & Bauermeister, J. A. (2010). Parent perceived impact of spaniard boys’ and girls’ inattention, hyperactivity, and oppositional defiant behaviors on family life. Journal of Attention Disorders, 14(3), 247–255. doi:10.1177/1087054709347180.
Bélanger, E., Ahmed, T., Vafaei, A., Curcio, C. L., Phillips, S.P., & Zunzunegui, M.V. (2016). Sources of social support associated with health and quality of life: A cross-sectional study among Canadian and Latin American older adults. BMJ Open, 6(6) doi:10.1136/bmjopen-2016-011503.
Bell, R. Q. (1968). A reinterpretation of the direction of effects in studies of socialization. Psychological Review, 75, 81–95.
Belsky, J. (1984). The determinants of parenting: A process model. Child Development, 55, 83–96.
Bentler, P. M. (2006). EQS Structural equations program manual. Encino, CA: Multivariate Software.
Bersabé, R., Fuentes, M. J., & Motrico, E. (2001). Psychometric analysis of two scales to evaluate parenting styles. Psicothema, 13(4), 678–684.
Bornstein, M. H. (2012). Cultural approaches to parenting. Parenting: Science & Practice, 12(2-3), 212–221. doi:10.1080/15295192.2012.683359.
Bozo, Ö., Anahar, S., Ateş, G., & Etel, E. (2010). Effects of illness representation, perceived quality of information provided by the health-care professional, and perceived social support on depressive symptoms of the caregivers of children with leukemia. Journal of Clinical Psychology in Medical Settings, 17(1), 23–30. doi:10.1007/s10880-009-9177-4.
Buesa, S., & Calvete, E. (2013). Violencia contra la mujer y síntomas de depresión y estrés postráumatico: El papel del apoyo social [Violence against women and symptoms of depression and posttraumatic stress: The role of social support]. International Journal Of Psychology & Psychological Therapy, 13(1), 31–45.
Burke, J. D., Pardini, D. A., & Loeber, R. (2008). Reciprocal relationships between parenting behavior and disruptive psychopathology from childhood through adolescence. Journal of Abnormal Child Psychology, 36(5), 679–692. doi:10.1007/s10802-008-9219-7.
Calzada, E. J., Eyberg, S. M., Rich, B., & Querido, J. G. (2004). Parenting disruptive preschoolers: Experiences of mothers and fathers. Journal of Abnormal Child Psychology, 32(2), 203–213. doi:10.1023/B:JACP.0000019771.43161.1c.
Catalá-López, F., Peiró, S., Ridao, M., Sanfélix-Gimeno, G., Gènova-Maleras, R., & Catalá, M. A. (2012). Prevalence of attention deficit hyperactivity disorder among children and adolescents in spain: A systematic review and meta-analysis of epidemiological studies. BMC Psychiatry, 12, 168 doi:10.1186/1471-244X-12-168.
Chacko, A., Wymbs, B. T., Flammer-Rivera, L., Pelham, W. E., Walker, K. S., Arnold, F. W., & Herbst, L. (2008). A pilot study of the feasibility and efficacy of the strategies to enhance positive parenting (STEPP) program for single mothers of children with ADHD. Journal of Attention Disorders, 12(3), 270–280. doi:10.1177/1087054707306119.
Chronis, A. M., Chacko, A., Fabiano, G. A., Wymbs, B. T., & Pelham, Jr., W. E. (2004). Enhancements to the behavioral parent training paradigm for families of children with ADHD: Review and future directions. Clinical Child and Family Psychology Review, 7(1), 1–27. doi:10.1023/B:CCFP.0000020190.60808.a4.
Conners, C. K. (1997). Conners’ rating scales-revised: Technical manual. North Tonawanda, NY: Multi-Health Systems Inc.
Corthorn, C., & Milicic, N. (2016). Mindfulness and parenting: A correlational study of non-meditating mothers of preschool children. Journal of Child and Family Studies, 25(5), 1672–1683. doi:10.1007/s10826-015-0319-z.
Cussen, A., Sciberras, E., Ukoumunne, O. C., & Efron, D. (2012). Relationship between symptoms of attention-deficit/hyperactivity disorder and family functioning: A community-based study. European Journal of Pediatrics, 171(2), 271–280. doi:10.1007/s00431-011-1524-4.
Deault, L. (2010). A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with attention-deficit/hyperactivity disorder (ADHD). Child Psychiatry & Human Development, 41(2), 168–192. doi:10.1007/s10578-009-0159-4. 25p.
DeGarmo, D. S., & Forgatch, M. S. (1997). Confidant support and maternal distress: Predictors of parenting practices for divorced mothers. Personal Relationships, 4(4), 305–317.
Donenberg, G., & Baker, B. L. (1993). The impact of young children with externalizing behaviors on their families. Journal of Abnormal Child Psychology, 21(2), 179–198.
Fabiano, G. A., Pelham, W. E., Cunningham, C. E., Yu, J., Gangloff, B., Buck, M., & Gera, S. (2012). A waitlist-controlled trial of behavioral parent training for fathers of children with ADHD. Journal of Clinical Child and Adolescent Psychology, 41(3), 337 doi:10.1080/15374416.2012.654464.
Farré-Riba, A., & Narbona, J. (1989). Índice de hiperquinesia y rendimiento escolar: validación del cuestionario de Conners en nuestro medio [Hyperkinetic index and school performance: Validity of Conners’ scale in our context]. Acta Pediátrica Española, 47(2), 103–109.
Fite, P. J., Colder, C. R., Lochman, J. E., & Wells, K. C. (2006). The mutual influence of parenting and boys’ externalizing behavior problems. Journal of Applied Developmental Psychology, 27, 151–164. doi:10.1016/j.appdev.2005.12.011.
Fleck, K., Jacob, C., Philipsen, A., Matthies, S., Graf, E., Hennighausen, K., & Jans, T. (2015). Child impact on family functioning: A multivariate analysis in multiplex families with children and mothers both affected by attention-deficit/hyperactivity disorder (ADHD). Attention Deficit and Hyperactivity Disorders, 7(3), 211–223. doi:10.1007/s12402-014-0164-8.
Forgatch, M. S., & DeGarmo, D. S. (1997). Adult problem solving: Contributor to parenting and child outcomes in divorced families. Social Development, 6, 237–252.
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. doi:10.1111/j.1467-9280.2007.01882.x.
Gau, S. S. (2007). Parental and family factors for attention-deficit hyperactivity disorder in Taiwanese children. Australian and New Zealand Journal of Psychiatry, 41(8), 688–696. doi:10.1080/00048670701449187.
Gerdes, A. C., Haack, L. M., & Schneider, B. W. (2012). Parental functioning in families of children with ADHD: Evidence for behavioral parent training and importance of clinically meaningful change. Journal of Attention Disorders, 16(2), 147–156. doi:10.1177/1087054710381482.
Gómez-Beneyto, M., Nolasco, A., Moncho, J., Pereyra-Zamora, P., Tamayo-Fonseca, N., Munarriz, M., & Girón, M. (2013). Psychometric behaviour of the strengths and difficulties questionnaire (SDQ) in the Spanish national health survey 2006. BMC Psychiatry, 13, 95 doi:10.1186/1471-244X-13-95.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Child Psychology and Psychiatry and Allied Disciplines, 38(5), 581–586.
Goodman, R. (2016). Scoring the Strenghts and Difficulties Questionnaire. http://www.sdqinfo.com/py/sdqinfo/c0.py.
Haack, L. M., Villodas, M. T., McBurnett, K., Hinshaw, S., & Pfiffner, L. J. (2014). Parenting mediates symptoms and impairment in children with ADHD-inattentive type. Journal of Clinical Child & Adolescent Psychology, 45(2), 155–166. doi:10.1080/15374416.2014.958840.
Haack, L.M., Villodas, M., McBurnett, K., Hinshaw, S., & Pfiffner, L.J. (2016). Parenting as a mechanism of change in psychosocial treatment for youth with ADHD, predominantly inattentive presentation. Journal of Abnormal Child Psychology. Published online. doi:10.1007/s10802-016-0199-8.
Harold, G. T., Elam, K. K., Lewis, G., Rice, F., & Thapar, A. (2012). Interparental conflict, parent psychopathology, hostile parenting, and child antisocial behavior: Examining the role of maternal versus paternal influences using a novel genetically sensitive research design. Development and Psychopathology, 24(4), 1283–1295. doi:10.1017/S0954579412000703.
Harold, G. T., Leve, L. D., Barrett, D., Elam, K., Neiderhiser, J. M., Natsuaki, M. N., & Thapar, A. (2013). Biological and rearing mother influences on child ADHD symptoms: Revisiting the developmental interface between nature and nurture. Journal of Child Psychology and Psychiatry, 54(10), 1038–1046. doi:10.1111/jcpp.12100.
Haydicky, J., Shecter, C., Wiener, J., & Ducharme, J. M. (2015). Evaluation of MBCT for adolescents with ADHD and their parents: Impact on individual and family functioning. Journal of Child and Family Studies, 24(1), 76–94. doi:10.1007/s10826-013-9815-1.
Informe PANDAH (2015). TDAH en España [ADHD in Spain]. http://www.pandah.es/explore/layout/informe-pandah.html.
Izzo, C., Weiss, L., Shanahan, T., & Rodriguez-Brown, F. (2014). Parental self-efficacy and social support as predictors of parenting practices and children’s socioemotional adjustment in Mexican immigrant families. In J. F. Gillespie, & J. Primavera (Eds.), Diverse families, competent families: Innovations in research and preventive intervention practice (pp. 197–214). Bringhampton, NY: The Haword Press Inc.
Jansen, P. W., Raat, H., Mackenbach, J. P., Hofman, A., Jaddoe, V. W. V., Bakermans-Kranenburg, M., & Tiemeier, H. (2012). Early determinants of maternal and paternal harsh discipline: The generation R study. Family Relations, 61(2), 253–270. doi:10.1111/j.1741-3729.2011.00691.x.
Javo, C., Rønning, J. A., Heyerdahl, S., & Floyd, W. R. (2004). Parenting correlates of child behavior problems in a multiethnic community sample of preschool children in northern Norway. European Child & Adolescent Psychiatry, 13(1), 8–18. doi:10.1007/s00787-004-0349-3.
Johnston, C., & Jassy, J. S. (2007). Attention-deficit/hyperactivity disorder and oppositional/conduct problems: Links to parent-child interactions. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 16(2), 74–79.
Johnston, C., & Mash, E. J. (2001). Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4(3), 183–207. doi:10.1023/A:1017592030434.
Judd, C. M., Kenny, D. A., & McClelland, G. H. (2001). Estimating and testing mediation and moderation in within-subject designs. Psychological Methods, 6(2), 115–134. doi:10.1037/1082-989X.6.2.115.
Kaiser, N. M., McBurnett, & Pfiffner, L. J. (2011). Child ADHD severity and positive and negative parenting as predictors of child social functioning: Evaluation of three theoretical models. Journal of Attention Disorders, 15(3), 193–203. doi:10.1177/1087054709356171.
Kline, R. B. (2005). Principles and practice of structural equation modeling. New York, NY: Guilford Press.
Lambek, R., Sonuga-Barke, E., Psychogiou, L., Thompson, M., Tannock, R., Daley, D., Damm, D. & Thomsen, P.H. (2014). The parental emotional response to children index: A questionnaire measure of parents´ reactions to ADHD. Journal of Attention Disorders 1087054714539996, first published on 3 July 2014 as doi:10.1177/1087054714539996.
Landeta, O., & Calvete, E. (2002). Adaptación y validación de la Escala Multidimensional de Apoyo Social Percibido [Adaptation and validation of the Multidimensional Scale of Perceived Social Support]. Ansiedad y Estrés, 8(2-3), 173–182.
Lange, G., Sheerin, D., Carr, A., Dooley, B., Barton, V., Marshall, D., & Doyle, M. (2005). Family factors associated with attention deficit hyperactivity disorder and emotional disorders in children. Journal of Family Therapy, 27(1), 76–96. doi:10.1111/j.1467-6427.2005.00300.x.
MacCallum, R. C., Browne, M. W., & Sugawara, H. M. (1996). Power analysis and determination of sample size for covariance structure modeling. Psychological Methods, 1, 130–149.
MacKinnon, D. P., & Dwyer, J. H. (1993). Estimating mediated effects in prevention studies. Evaluation Review, 17(2), 144–158.
MacKinnon, D. P., Fairchild, A. J., & Fritz, M. S. (2007). Mediation analysis. Annual Review of Psychology, 58, 593–614. doi:10.1146/annurev.psych.58.110405.085542.
Maniadaki, K., Sonuga-Barke, E., & Kakouros, E. (2005). Parents’ causal attributions about attention deficit/hyperactivity disorder: The effect of child and parent sex. Child: Care, Health and Development, 31(3), 331–340. doi:10.1111/j.1365-2214.2005.00512.x.
Mash, E. J., & Johnston, C. (1983). Parental perceptions of child behavior problems, parenting self-esteem, and mothers’ reported stress in younger and older hyperactive and normal children. Journal of Consulting and Clinical Psychology, 51(1), 86–99. doi:10.1037/0022-006X.51.1.86.
McLaughlin, D. P., & Harrison, C. A. (2006). Parenting practices of mothers of children with ADHD: The role of maternal and child factors. Child and Adolescent Mental Health, 11(2), 82–88. doi:10.1111/j.1475-3588.2005.00382.x.
Ministerio de Sanidad, Política Social e Igualdad (2010). Guía de Práctica Clínica sobre el Trastorno por Déficit de Atención con Hiperactividad (TDAH) en Niños y Adolescentes[Clinical Practice Guidelines on Attention Deficit Hyperactivity Disorder (ADHD) in Children and Adolescents]. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad. Agència d´Informació, Avaluació i Qualitat en Salut (AIAQS) de Cataluña; 2010. Guías de Práctica Clínica en el SNS: AIAQS N° 2007/18.
Mischel, W. (1973). Toward a cognitive social learning conceptualization of personality. Psychological Review, 80, 252–283.
Nam, S., & Chun, S. (2014). Influencing factors on mothers’ parenting style on young children at risk for developmental delay in South Korea: The mediating effects of parenting stress. Children and Youth Services Review, 36, 81–89. doi:10.1016/j.childyouth.2013.11.008.
Pardini, D. A. (2008). Novel insights into longstanding theories of bidirectional parent-child influences: Introduction to the special section. Journal of Abnormal Child Psychology, 36(5), 627–631. doi:10.1007/s10802-008-9231-y.
Patterson, G. R. (1982). Coercive family processes. Eugene, OR: Castalia.
Patterson, G. R. (2002). The early development of coercive family process. In J. B. Reid, G. R. Patterson, & J. J. Snyder (Eds.), Antisocial behavior in children and adolescents: A developmental analysis and the Oregon model for intervention (pp. 25–44). Washington, DC: American Psychological Association.
Pearl, A. M., French, B. F., Dumas, J. E., Moreland, A. D., & Prinz, R. (2014). Bidirectional effects of parenting quality and child externalizing behavior in predominantly single parent, under-resourced African American families. Journal of Child and Family Studies, 23(2), 177–188. doi:10.1007/s10826-012-9692-z.
Podolski, C. L., & Nigg, J. T. (2001). Parent stress and coping in relation to child ADHD severity and associated child disruptive behavior problems. Journal of Clinical Child Psychology, 30, 503–513.
Preacher, K. J., & Coffman, D. L. (2006). Computing power and minimum sample size for RMSEA [Computer software]. http://quantpsy.org/.
Presentación, M. J., García, R., Miranda, A., Siegenthaler, R., & Jara, P. (2006). Familial impact of children with the combined subtype of attention deficit hyperactivity disorder: The effects of associated behavioural disorders. Revista De Neurologia, 42(3), 137–143.
Presentación, M. J., Pinto, V., Meliá, A., & Miranda, A. (2009). Efectos sobre el contexto familiar de una intervención psicosocial compleja en niños con TDAH [Effects on the family context of a complex psychosocial intervention for children with ADHD]. Escritos de Psicología, 2(3), 18–26.
Rodríguez-Hernández, P. J., Betancort, M., Ramírez-Santana, G. M., García, R., Sanz-Álvarez, E. J., & De, lC. (2012). Psychometric properties of the parent and teacher versions of the strength and difficulties questionnaire (SDQ) in a spanish sample. International Journal of Clinical and Health Psychology, 12(2), 265–279.
Rudy, D., & Grusec, J. E. (2006). Authoritarian parenting in individualist and collectivist groups: Associations with maternal emotion and cognition and children’s self-steem. Journal of Family Psychology, 20(1), 68–78. doi:10.1037/0893-3200.20.1.68.
Salas, M. D., García-Martín, M. Á., Fuentes, M. J., & Bernedo, I. M. (2015). Children’s emotional and behavioral problems in the foster family context. Journal of Child and Family Studies, 24(5), 1373–1383. doi:10.1007/s10826-014-9944-1.
Sanders, M. R., Morawska, A., Haslam, D. M., Filus, A., & Fletcher, R. (2014). Parenting and family adjustment scales (PAFAS): Validation of a brief parent-report measure for use in assessment of parenting skills and family relationships. Child Psychiatry and Human Development, 45(3), 255–272. doi:10.1007/s10578-013-0397-3.
Shelton, T. L., Barkley, R. A., Crosswait, C., Moorehouse, M., Fletcher, K., Barrett, S., Jenkins, L., & Metevia, L. (1998). Psychiatric and psychological morbidity as a function of adaptive disability in preschool children with aggressive and hyperactive impulsive inattentive behavior. Journal of Abnormal Child Psychology, 26, 475–494.
Shieh, G. (2009). Detecting interaction effects in moderated multiple regression with continuous variables power and sample size considerations. Organizational Research Methods, 12(3), 510–528. doi:10.1177/1094428108320370.
Singh, N. N., Singh, A. N., Lancioni, G. E., Singh, J., Winton, A. S. W., & Adkins, A. D. (2010). Mindfulness training for parents and their children with ADHD increases the children’s compliance. Journal of Child and Family Studies, 19(2), 157–166. doi:10.1007/s10826-009-9272-z.
Sollie, H., Mørch, W. T., & Larsson, B. J. (2016). Parent and family characteristics and their associates in a follow-up of outpatient children with ADHD. Journal of Child and Family Studies, 25(8), 2571–2584. doi:10.1007/s10826-016-0411-z.
Sturge-Apple, M., Davies, P. T., Boker, S. M., & Cummings, E. M. (2004). Interparental discord and parenting: Testing the moderating roles of child and parent gender. Parenting: Science & Practice, 4(4), 361–380. doi:10.1207/s15327922par0404_7.
Wallace, G. (2013). African-American mothers’ community social capital and parenting quality does personal outlook make a difference? Sociological Perspectives, 56(2), 261–285. doi:10.1525/sop.2013.56.2.261.
Weiss, M. J. (2002). Hardiness and social support as predictors of stress in mothers of typical children, children with autism, and children with mental retardation. Autism, 6(1), 115–130. doi:10.1177/1362361302006001009.
Woody, E. (2011). An SEM perspective on evaluating mediation: What every clinical researcher needs to know. Journal of Experimental Psychopathology, 2(2), 210–251. doi:10.5127/jep.010410.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41.
Author Contributions
A.M.S.: designed and executed the study, analyzed the data, and wrote the paper. R.L.U.: designed and executed the study, and wrote the paper. M.S.G.: executed the study, analyzed the data, and wrote the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Muñoz-Silva, A., Lago-Urbano, R. & Sanchez-Garcia, M. Family Impact and Parenting Styles in Families of Children with ADHD. J Child Fam Stud 26, 2810–2823 (2017). https://doi.org/10.1007/s10826-017-0798-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-017-0798-1