
Abstract
The significance of enhancing parenting skills to reduce child maladjustment is well-established and supports the important role of evidence-based parenting programs. However, the notion that parenting should be the exclusive focus for enhancing child behavior is necessarily limiting. Evidence is growing that relationship-oriented treatments may be another powerful approach to improve child adjustment, albeit the underlying effects in couple- versus parenting-focused programs have been subject to limited study. The aim of this RCT was to compare the treatment effects of (1) a couple-focused program (the Couples Coping Enhancement Training) to (2) a parenting training (Triple P) and (3) a control group on children’s behavioral problems in 150 couples. The parents’ perceptions of relationship quality, parenting behavior, and child’s behavioral problems were assessed by means of questionnaires completed prior to and 2 weeks after the end of the treatment. Multi-group path analyses revealed that in mothers’ perception the couple-focused program reduced child behavioral problems by enhancing the relationship quality whereas improved parenting mediated the benefits in the parenting training. In fathers’ evaluations the couple-focused program reduced dysfunctional parenting which largely accounted for the benefits in child adjustment. The dearth of research on child outcomes in couple-focused intervention studies is a striking gap that should be overcome. It is a promising field because of its evident potential to foster the health of many children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The significance of enhancing positive parenting in order to reduce child maladjustment has repeatedly been shown and has led to the development of a vast number of parenting programs. However, drawing from the abundant research on the impact of interparental conflict on children (Cummings and Davies 2010), the primacy of parenting in prevention programs is necessarily limiting and omits an important piece of the puzzle: the parents’ relationship (Emery et al. 1992). An emerging line of research has found that relationship-focused treatments alone or adjunct to parenting programs may be a valuable alternative for increasing child adjustment (e.g., Cowan et al. 2011; Cummings et al. 2008), albeit the underlying effects in couple- versus parenting-focused programs have not yet been properly studied.
Scientists have gathered robust support for the importance of parenting programs in changing children’s behavior (see for an overview Dretzke et al. 2005). Evidence from the parenting literature, e.g. within evaluations of the Triple P Positive Parenting Program (Sanders 1999), confirms the promise of parenting enhancement in decreasing child behavior problems. Triple P is a parenting program aimed at improving parenting as well as parental self-efficacy and by this means preventing adjustment problems in children. It incorporates five levels of intervention. A plethora of international studies proved the efficacy of Triple P in improving parenting skills and child problem behaviors. Including the results of 55 Triple P efficacy studies, Nowak and Heinrichs (2008) found small to medium averaged effects for parenting (d = .38–.60), for child problem behavior (d = .35–.61), and for relationship quality (d = .10–.11). The most recent meta-analysis (Sanders et al. 2014) based on 101 studies found significant overall effects of Triple P on parenting (d = .58), child adjustment (d = .47), and parents’ relationship (d = .23).
Indeed, it seems feasible that family interventions should address parenting (i.e., the parent–child relationship) in order to prevent or treat child maladjustment. What is apparently less obvious is the idea that an intervention focused on the interparental relationship could lead to substantial benefits for children too. Whilst most of the avenues in family interventions give priority to parenting, studies examining the positive impact of couple-focused programs for children are still underrepresented. This is surprising given that family system theorists since the 1950s have been emphasizing the interparental relationship as pivotal in creating a positive family climate (Minuchin 1985). Couple conflict emerged empirically as one of the primary family risk factors for health problems in children. A vast corpus of research has expressed increasing concern that children who witness destructive interparental conflict may experience substantial damage in their development (e.g., Barletta and O’Mara 2006; Cummings and Davies 2010; Rhoades 2008). On the other side, there is compelling evidence for the existence of constructive conflict tactics from the child’s perspective. Children’s distress reactions are significantly reduced when interparental conflicts are resolved (e.g., El-Sheikh and Cummings 1995). Remarkably, children benefit from any progress toward resolution; distress is even reduced when conflicts are not fully resolved, proportional to the degree of resolution (Goeke-Morey et al. 2007). Goeke-Morey et al. (2003) classified interparental conflict behaviors by means of children’s responses to vignettes of adult interactions. They found a continuum from most destructive to most constructive conflicts, with physical aggression at one extreme and mutual support at the other. Notably, constructive conflict communication fostered children’s felt emotional security in the family, which, in turn, enhanced their prosocial behavior prospectively (McCoy et al. 2009). Zemp et al. (2014) investigated child outcomes as a function of the proportion of their parents’ reports of positive to negative interactions and found that the positivity-to-negativity ratio was strongly associated with children’s well-being.
In sum, the treatment of “the child alone, or the parent–child relationship alone, is necessarily incomplete because a key element of the system, the marriage, is overlooked” (Fincham 1998, p. 544). A positive interparental relationship in which conflicts are resolved constructively may directly enhance children’s well-being and indirectly by positive parenting and parent–child-relations. Thus, not only are relationship problems related to child problems, but the alleviation thereof might also reduce child problems. Clinical approaches focused on helping mothers and fathers make their relationship less distressed and more satisfying may be conducive to a healthy child development. However, research-based supports for child outcomes have been largely neglected in interventions or prevention programs for couples (collectively referred to as Couple Relationship Education CRE) previously. The most recent meta-analysis by Cowan and Cowan (2014) found that of the more than 150 CRE efficacy studies they included in their analysis, only 9 reflected RCT studies that examined the children’s well-being in addition to couple relationship outcomes. That said, contemporary approaches increasingly recognize the interparental relationship as a significant influence on children.
For instance, a brief program for improving interparental conflict in community families was developed aimed at improving relationship and child outcomes explicitly (Cummings et al. 2008). This program focuses on psycho-education about the harmful impact of couple conflict on children and includes communication trainings for parents. To evaluate the program, parents having at least one child between the ages of 4 and 8 years were randomly assigned to one of three groups: (1) a parent-only group (the standard parent program) (2) a parent–child group (the standard parent program and a child-focused program), and (3) a self-directed intervention group (couples received two publications to read at home). After the treatment, outcome measures in the parent-only group and the parent–child group did not significantly differ. Parents from both these groups increased their knowledge related to interparental conflict (d = 1.59–1.84) and improved their conflict behaviors with regard to constructiveness (d = .69–1.97) and conflict resolution (d = .72–1.72) compared to the control group. Mothers’ enhanced knowledge and conflict resolution was positively linked with her positive parenting and improved child adjustment. Increased fathers’ knowledge was associated with improved parenting exclusively. All these gains maintained over the course of the study of 1 year (Cummings et al. 2008) and at the 2-year follow-up (Faircloth et al. 2011).
A randomized clinical trial compared the effects of a couple-focused intervention with a parenting-focused program and a control group offered to couples in the year before their oldest child made the transition to elementary school (Cowan et al. 2005). Both interventions consisted of parent group meetings over 16 weeks with the identical curriculum topics except of an open-ended part of each evening, where the group leaders either emphasized a couple focus or a parenting focus. The control group was assigned to a low-dose comparison condition (opportunity for a consultation once a year for 3 years). Two years after the treatment, parents in the couple-focused groups used more effective parenting strategies and they showed no increase in interparental conflict in contrast to controls. The intervention accounted for 31 % of the variance in reductions in their children’s externalizing symptoms and 12 % of the reductions in internalizing symptoms between kindergarten and first grade. Mediation analyses revealed that improved conflict communication mediated the benefits on children’s adjustment in parents of the couple-focused group. The 10-year follow-up study (Cowan et al. 2011) found that parents assigned to the couple-focused group were more likely to maintain their marital satisfaction (r = .33 for mothers; r = .24 for fathers) and their children showed a sharper decline in teacher-reported hyperactive and aggressive behaviors (r = .22) compared to the other study groups.
Apart from these positive findings within the context of prevention programs (CRE), positive effects for children were also found in the context of couple therapy. Gattis et al. (2008) examined whether behavioral couple therapy affects child-related conflicts and child adjustment in distressed couples with at least one child under the age of 18 years. A significant decrease in conflicts over child-rearing was found from pre- to post-assessment (d = .20) and the effect was stable over 2 years (d = .17). Couples also reported significantly reduced child maladjustment over the course of therapy from pre- to post-assessment (d = .29), however the levels rebounded at the 2-year follow-up (d = .07). Mediation analyses revealed that change in child-related conflicts mediated the link between change in marital satisfaction and improved child adjustment.
Other scholars have examined whether adding couple-focused interventions to parenting programs can improve their efficacy. For instance, Griest et al. (1982) examined whether an adjunctive treatment focused on the interparental relationship may increase the efficacy of a parenting training program in clinic-referred mother–child pairs compared to a control group. All mothers completed a parenting training program and one group received an additional intervention addressing the parent’s relationship. The supplemented treatment resulted in significant gains over the standard parenting program; it reduced child’s noncompliant and deviant behavior more effectively over 2 months. Likewise, Dadds and colleagues found that, in comparison to a behavioral parent training alone, an adjunctive relationship-oriented intervention (adding a partner support training focused on couple conflict and communication) produced additional improvement in child problem behaviors in parents of children diagnosed with conduct disorder (Dadds et al. 1987a, b). In a study of Webster-Stratton (1994), families with a child diagnosed as oppositional-defiant or conduct-disordered were randomly assigned to either a parenting program (a series of videotaped parenting skills followed by a group discussion led by a therapist) or the similar program with additional treatment elements including constructive communication skill between parents. The analyses revealed significant improvements in the supplemented intervention in interparental communication and problem-solving.
Another couple-focused prevention program that was already evaluated with regard to its effect on child behavior is the Couples Coping Enhancement Training (CCET; Bodenmann and Shantinath 2004). The CCET is based on the systemic-transactional model of stress and coping in couples (Bodenmann 1997, 2005). The CCET is among the first relationship education programs that go beyond teaching constructive communication; it also addresses the enhancement of individual and dyadic skills to cope with stress. The efficacy of the program in terms of effects on relationship quality has been repeatedly supported (e.g., Bodenmann et al. 2008a; Halford and Bodenmann 2013; Ledermann et al. 2007). Notably, significant positive effects on children’s well-being were also reported (Bodenmann et al. 2008b): In a randomized controlled trial, the efficacy of CCET was compared to Triple P and a control group over 1 year (50 couples each). The parents’ perceptions of their relationship quality and parenting behavior, and their child’s behavioral problems were assessed by means of questionnaires prior to and 2 weeks after completion of the treatment, at 6-month, and at 1-year follow-up. The results showed that CCET enhanced the couples’ relationship quality significantly from pre- to post-assessment (d = .63 for mothers and d = .53 for fathers) and reduced dysfunctional parenting (d = .36 for mothers and d = .22 for fathers). Additionally, children from CCET parents showed significantly fewer behavioral problems after the treatment compared to baseline-assessments (d = .61 for mothers and d = .39 for fathers) and these effects were stable over 1 year (d = .63 for mothers and d = .46 for fathers). By comparison, Triple P was primarily effective in reducing dysfunctional parenting in parents from pre- to post-assessment (d = .89 for mothers and d = .51 for fathers) and it reduced child behavioral problems significantly (d = .54 for mothers and d = .38 for fathers). Smaller effects of Triple P were found on the couples’ relationship quality (d = .40 for mothers and d = .11 for fathers). Effect sizes for differences between the intervention groups at post-assessment and the follow-ups revealed that CCET had stronger effects on the couples’ relationship quality (d = .35–.50 for mothers and d = .25–.51 for fathers), whereas Triple P was more effective with regard to parenting skills (d = .21–.37 for mothers and d = .09–.52 for fathers), and the reduction of child behavioral problems (d = .27–.43 for mothers and d = .16–.23 for fathers). While mothers of the CCET group reported reduced dysfunctional parenting (d = .20–.33) and fewer child behavioral problems (d = .02–.35) compared to the control group, fathers did not significantly benefit from CCET regarding parenting or child adjustment compared to controls.
Taken together, whilst evidence continues to mount that couple-focused treatments in their own right or adjunct to parenting programs are a potent means of increasing child well-being, the underlying effects in couple- versus parenting-oriented programs still remain largely unclear. The goal of this study is to add to the understanding of the distinct or overlapping mechanisms of these interventions with relation to child adjustment. The current study builds on the previous investigation of Bodenmann et al. (2008b) by reanalyzing the same data in order to advance our understanding by what means the two programs (CCET, Triple P) lead to an improvement of child behavior. We hypothesize that CCET improves child well-being by an improvement of the parents’ relationship quality (the main target of this program) while the positive outcome on child behaviors in the Triple P group is explained by an improvement of parenting skills.
Method
Participants
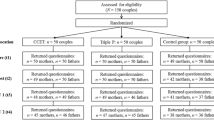
The participants constituted a universal prevention sample of 150 couples. Inclusion criteria for participation were good knowledge of German, cohabiting with spouse or partner, being in a committed relationship since at least 1 year and having at least one child aged 2–12 years. If participants had more than one child in this age range parents were asked to select the child that they recently have been worrying about most (= target child). For mothers, the average age was M = 37.44 years (SD = 4.17) and for fathers M = 39.66 years (SD = 4.62), respectively. Ninety-two percent of the couples were married. Relationship duration ranged from 1 to 24 years (M = 13.35 years, SD = 5.10). The age of the target children averaged 6.52 years (SD = 2.69) in mothers’ reports and 6.69 years (SD = 2.98) in fathers’ reports. No significant differences were found in age, citizenship, education, income, marital status, duration of relationship, number of children, and age or gender of the target children between the three study groups.
Procedure
Participants were recruited by means of advertisements published in several Swiss newspapers. Eligible couples were randomly assigned to one of the three study groups (i.e., n = 50 to CCET, n = 50 to Triple P, n = 50 to the control group, respectively). Participants were asked to complete a set of questionnaires at four times: at pre-assessment (T1: 2 weeks prior to the treatment), at post-assessment (T2: 2 weeks after completion of the treatment), at 6-month follow-up (T3), and at 1-year follow-up (T4). In this study, only the data of T1 and T2 were included in the analyses because of two main reasons: First, in this study we were primarily interested in the process mechanisms of the treatments which accounted for the benefits in child behavioral problems and thus examined the two time points within which the interventions occurred exclusively. Second, inclusion of T3 and T4 data points would have dropped the power of the statistical analyses because of a reduced sample due to the attrition rate. All couples received an incentive of approximately $100 (US).
Treatments
Couples Coping Enhancement Training (CCET)
The CCET is an evidence-based relationship distress prevention program (Bodenmann and Shantinath 2004). In addition to the enhancement of constructive communication and problem-solving skills, CCET also addresses individual and dyadic coping skills. Several didactic elements are used in this training: short lectures with video examples, diagnostic assessments (e.g., evaluation of perceived stress level, individual coping, dyadic coping, communication), quizzes for determining the couple’s mastery of the training material, demonstrations of effective and ineffective problem-solving styles, video and live demonstrations by the workshop providers that model effective communication and dyadic coping skills, as well as supervision and feedback on the couple’s behaviors in exercises according to a ratio of one trainer per two couples.
In contrast to Triple P, the CCET is offered as a weekend workshop in a group format of 4–8 couples per workshop but it does not differ from Triple P concerning the overall duration (15 h). Similar to Triple P, it has a cognitive-behavioral orientation and requires homework after the session. Providers in the CCET group were accredited (advanced level graduate students in clinical psychology) who had successfully passed a written exam and an evaluation of a videotaped coaching of couples. Each provider received 30 h of training over a 4-day period and 20 h of group supervision before delivering the program. Both program providers (Triple P and CCET) were equally trained and there were no differences with regard to the quality of delivering the programs that might have influenced the treatment effects A high degree of standardization is achieved in both CCET as well as Triple P by means of a detailed and highly structured manual and close supervision of the trainers.
Triple P Positive Parenting Program
Triple P aims at preventing and reducing the incidence of psychological and behavioral problems in children by the enhancement of parenting skills (Sanders 1999). Triple P is a widely used and evidence-based parenting and family support system for all parents (universal prevention) as well as specific groups (selective prevention), or parents facing behavioral problems of their children (indicated prevention). Triple P incorporates five levels of intervention for parents of children aged 0–16 years. In this study, both parents (mothers and fathers) participated in Level 4 of Triple P exclusively which is offered as an 8-week preventive group program (Group Triple P) in Switzerland addressing parenting issues for all parents, independently of current problem behavior of their children. Hence, Level 4 group format in this study is not conceived as an intervention for parents with severe child problems (like in the original version of Triple P) but rather as a program for all parents willing to learn more about positive parenting. Group Triple P is used as a moderate intensity cost effective universal prevention program. In Switzerland, this kind of format is commonly used in the context of universal prevention.
Parents received four group sessions of parenting training per 2.5 h. Upon completion of the group sessions, parents were supported with four phone counselling sessions at home. For each phone consultation the couples could choose whether the mother, the father, or both parents together were involved in the calls. Parents also received a copy of the “Every Parent’s Group Workbook”(Sanders et al. 2003) containing the key learning principles of the program and exercises to be completed in the training and between sessions. The training involved 17 core child management strategies: 10 strategies were designed to promote children’s competence and development (e.g., praise, engaging activities, incidental teaching) and 7 strategies were designed to help parents manage children’s misbehavior (e.g., setting rules, logical consequences, time-out). The training aimed at enhancing the generalization and maintenance of parenting skills by teaching parents how to apply the skills to a broad range of child behaviors in both home and public settings. Parents were learned to set and monitor goals for behavior change and to enhance their skills in observing their child’s and their own behavior. Interactive training methods such as modeling, rehearsal, practice, and feedback were used to teach the parenting skills throughout the program within a self-regulatory framework. The program took 8 weeks to complete: 4 weeks of group sessions of 2.5 h duration each (enrolling 8–10 couples per workshop) and another 4 weeks of personal telephone contact subsequent to the group sessions (four individual consultations per approximately 15–30 min).
Measures
Relationship Quality
The quality of the couples’ relationship was measured by both partners’ reports on the German version of the Dyadic Adjustment Scale (Spanier 1976). This measure yields a general score of relationship satisfaction and quality including four main aspects: dyadic satisfaction, dyadic cohesion, dyadic consensus, and affectional expression. Thirty-two items (e.g., How often do you and your partner quarrel?; Do you kiss your mate?) are rated on different Likert scales ranging from 2-point to 7-point scales. The total score was used in this study which represents the sum of all items, ranging from 0 to 151. For the main path analyses we used a transformed scale to attain comparable variances with the other target variables, dividing the total scores by a constant of 30. Higher scores imply higher relationship quality. Good psychometric properties of the German scale have been shown (Dinkel and Balck 2006). In the current study, internal consistency for T1 and T2 were α = .86/.87 for mothers’ reports and α = .87/.86 for fathers’ reports.
Parenting
The short German version of the Parenting Scale (Naumann et al. 2010), originally developed by Arnold et al. (1993), was used to assess dysfunctional parenting behaviors. The parents rated the 13 items (e.g., If my child gets upset, I back down and give in; I raise my voice or yell) on a 7-point Likert scale. We used the total score in this study where higher scores reflect more dysfunctional parenting disciplines. The German version has good psychometric properties and a largely consistent factor structure to the American original (Naumann et al. 2010). Internal consistency for T1 and T2 were α = .75/.76 for mothers’ reports and α = .80/.84 for fathers’ reports, respectively.
Child Behavioral Problems
We used the German version of the Eyberg Child Behavior Inventory (Eyberg and Pincus 1999) to assess the parents’ perceptions of problem behaviors in children aged 2–16 years with 36 items (e.g., Refuses to go to bed on time; Acts defiant when told to do something). The parents rated how often the problem behavior occurs (intensity scale; rated on a 7-point Likert Scale) and whether the behavior is a significant problem (problem scale; rated on a dichotomous scale indicating yes or no). For the purpose of this study the intensity scale was used exclusively where higher scores reflect more child misbehavior. The German version was psychometrically validated recently (Heinrichs et al. 2014). In the current study, internal consistency for T1 and T2 were α = .88/.90 for mothers’ reports and α = .92/.91 for fathers’ reports, respectively.
Data Analysis
To test for mediating mechanisms, we conducted path analytical multigroup mediation models (see Fig. 1) separately for mothers and fathers. Including female and male variables into one model was not adequate, because the child problem behavior rated by both parents did not necessarily reflect the behavior of the same target child. The multigroup approach we used allows us to estimate model parameters and to test for differences in mediation processes between predefined groups simultaneously, as one model per group (CCET, Triple P, and control group) is calculated at the same time. More specifically, in this study, mediation processes are said to differ between groups when improved child behavioral problems (i.e., child behavioral problems after the treatment controlled for initial child behavior problems prior to the treatment) can be explained by a significant indirect effect via enhanced relationship quality (path k * p, see Fig. 1) or parenting (path o * q, see Fig. 1), respectively, from T1 to T2 in one treatment group, but not the other treatment group nor the control group. To test for distinct mediation effects per group, we compared two models. In Model 1, we allowed all paths that we assumed to differ between groups to vary; in Model 2, we deliberately constrained the respective paths to be equal across groups (see bold solid lines in Fig. 1). A significantly better model fit for Model 1 in comparison to Model 2 would provide support for our hypothesis that mediation effects differ between groups and should not be equalized. We reported multiple fit indices to indicate the degree to which the tested models fit the sample data. Beside the traditional Chi square discrepancy test, the relative Chi square index (χ 2/df) is presented whereby values below 3 are considered indicative of an acceptable fit (Field 2009). Additionally, the root mean square error of approximation (RMSEA; Browne and Cudeck 1993) and the comparative fit index (CFI; Bentler 1990) are reported. Values of the RMSEA less than or equal to .05 and values of the CFI of at least .95 indicate a good representation of the data. Analyses were conducted using Mplus 7 (Muthén and Muthén 1998–2012). Following recommendations of Shrout and Bolger (2002), the full information maximum likelihood estimation procedure (FIML) with bootstrap option (1000 samples) implemented in Mplus was used to estimate model parameters and corresponding standard errors.

Treatment effects from T1 to T2 mediated by relationship quality and parenting (Model 1). Fine solid lines represent correlations and paths that were held equal across groups. Dotted lines represent correlations and paths that vary freely without specific hypotheses to be different across groups. Bold solid lines represent paths that are hypothesized to be different across groups
Results
Means, standard deviations, and correlations among all target variables at T1 and T2 are listed in Table 1. T1 variables did not significantly differ between the study groups, except of males’ relationship quality, which was significantly lower in the CCET compared to the other groups (M CCET = 95.19; M Triple P = 101.19; M CG = 102.00; F(2/132) = 4.10, p = .019). In the overall sample, high levels in relationship quality were negatively linked to dysfunctional parenting for mothers and fathers and at both time points. Parenting at T1 was not significantly associated between gender. Relationship quality was linked to child behavior problems for fathers, but not for mothers. Dysfunctional parenting in mothers was related to mothers’ reports of child behavior problems and, accordingly, dysfunctional parenting in fathers was related to fathers’ reports of child behavior problems.
As described above, we tested two path-analytical models against each other within a multiple group approach (Muthén and Muthén 1998–2012). In the first constrained model (Model 1), all correlations and paths that were not assumed to vary across the three study groups were set equal across groups (see fine solid lines in Fig. 1). That is, we did not presume the correlations among the T1 variables (correlations a, b, and c) to differ across groups. Similarly, we did not expect the paths from T1 child behavioral problems on T2 variables (paths f, g, and h) or the paths from T1 relationship quality and T1 parenting to T2 child behavioral problems (paths e and i) to differ significantly between groups. When these paths were set equal across the three groups in Model 1, the model provided excellent fit to the data for mothers (χ 2(16) = 12.24, p = .728; χ 2/df = .77; RMSEA = .00; CFI = 1.00) and for fathers (χ 2(16) = 14.72, p = .545; χ 2/df = .92; RMSEA = .00; CFI = 1.00). A large proportion of the variance in T2 child behavioral problems were explained by the variables in Model 1, i.e., in the CCET group R 2 = .47 for mothers and R 2 = .57 for fathers; in the Triple P group R 2 = .54 for mothers and R 2 = .61 for fathers; and in the control group R 2 = .55 for mothers and R 2 = .47 for fathers, respectively.
To test the hypothesis that CCET reduces child misbehavior by enhancing the couples’ relationship quality while improved parenting mediates the benefits on child misbehavior in the Triple P group, we compared Model 1 to a second model (Model 2) in which we restricted specific paths. In Model 2, all those paths that we hypothesized to be different between the three study groups were set equal across groups (see bold solid lines in Fig. 1), above and beyond the paths which were set equal in Model 1. Namely, we constrained the paths from T1 relationship quality to T2 relationship quality (path k) and from T1 parenting to T2 parenting (path o) to be equal across groups. Likewise, we equalized T2 relationship quality and T2 parenting on T2 child behavioral problems (paths p and q). Concurrently to the direct paths, this approach resulted in equalized indirect paths from T1 relationship quality on T2 child behavioral problems by T2 relationship quality (indirect path k * p) and from T1 parenting on T2 child behavioral problems by T2 parenting (indirect path o * q). The remaining paths m and n, and the correlation d were allowed to vary freely between groups since they were not of primary interest with regard to the study hypotheses (see dotted solid lines in Fig. 1). In addition, we took into account the indirect effects that logically resulted out of the model set up (i.e., path m * q and path n * p). These indirect effects are also reported in Table 3 but were not our primary interest and thus were not included in our study hypotheses.
As expected, in comparison to Model 1, the more restricted Model 2 provided a significantly worse model fit for mothers (∆χ 2(∆df: 10) = 27.52; p = .002) and fathers (∆χ 2(∆df: 10) = 31.70; p < .001), respectively, suggesting that associations between the variables in question are not the same between groups and, hence, should not be set equal. Therefore, Model 1 was considered the final model for which parameter estimates of all coefficients are depicted in Table 2. Parameter estimates for the indirect effects of Model 1 across the study groups are listed separately in Table 3, that is, the indirect effects of T1 relationship quality and T1 parenting to T2 child behavioral problems by T2 relationship quality and T2 parenting controlled for T1 child behavioral problems. We first report the correlations and paths that were set equal across groups and detail the findings for each group afterwards. Regarding these group-specific paths, we will first report the results found for mothers and refer to the results for fathers subsequently. We use the term parenting conveniently throughout the report of the results but recall that higher scores imply higher levels in dysfunctional parenting.
Results Across Groups
Parameter estimates for correlations and paths coefficients that were set equal across groups are shown in Table 2. For mothers and fathers, T1 relationship quality and T1 parenting correlated significantly as well as T1 parenting and T1 child behavioral problems. There was a significant association between T1 relationship quality and T1 child behavioral problems, but only in fathers. T1 child behavioral problems were a strong predictor of T2 child behavioral problems in both genders.
Results for CCET
Parameter estimates for paths coefficients that were allowed to vary between groups according to our hypotheses are listed in Table 2 and the indirect effects are listed in Table 3. In mothers of the CCET group we found a significant link between parenting at T1 and T2 (β = .66, p < .001) (see Table 2). T1 relationship quality significantly predicted T2 relationship quality (β = .83, p < .001), which, in turn, predicted child behavioral problems at T2 (β = −.42, p = .014). Confirming our hypothesis, it is shown in Table 3 that T2 relationship quality mediated the effect of T1 relationship quality on T2 child behavioral problems (β = −.35, p = .024, CI95 = [−.65; −.05]). We did not find significant indirect effects via T2 parenting. These findings suggest that the enhancement of relationship quality rather than the enhancement of parenting accounted for the benefits in child adjustment reported by the mothers of the CCET group.
As shown in Table 2, in fathers of the CCET group there was a significant association between relationship quality at T1 and T2 (β = .75, p < .001). T1 parenting significantly predicted T2 parenting (β = .72, p < .001), which, in turn, was linked to child behavioral problems at T2 (β = .31, p = .026). Contradictory to our hypothesis, the effect of T1 parenting on T2 child behavioral problems was mediated by T2 parenting (β = .22, p = .020, CI95 = [.04; .41]) indicating that the benefits of the CCET on child adjustment reported by fathers were predominantly explained by the reduction of dysfunctional parenting (see Table 3). The indirect path from T1 relationship quality on T2 child behavioral problems via T2 relationship quality was only moderately significant (β = −.17, p = .086, CI95 = [−.36; .02]).
Results for Triple P
In mothers of the Triple P group T1 relationship quality significantly predicted T2 relationship quality (β = .69, p < .001) as shown in Table 2. T1 parenting predicted T2 parenting (β = .60, p < .001), which, in turn, was significantly linked to T2 child behavioral problems (β = .31, p = .044). As depicted in Table 3 in accordance to our hypothesis, T2 parenting (β = .18, p = .043, CI95 = [.01; .36]), but not T2 relationship quality (β = −.19, p = .234, CI95 = [−.03; .06]), mediated the effect of T1 parenting on T2 child behavioral problems. This indicates that the reduction of dysfunctional parenting explained the treatment effects on children’s behavioral problems rather than the enhancement of relationship quality in mothers of the Triple P group.
As depicted in Table 2, in fathers of the Triple P group T1 relationship quality significantly predicted T2 relationship quality (β = .88, p < .001) and T1 parenting was linked to T2 parenting (β = .83, p < .001). None of the indirect effects were significant for fathers in the Triple P group (see Table 3).
Results for the Control Group
As shown in Table 2, in mothers of the control group T1 and T2 relationship quality as well as T1 and T2 parenting were significantly associated (β = .86, p < .001 and β = .73, p < .001, respectively). There was no significant indirect effect for mothers in the control group (see Table 3).
In fathers of the control group T1 relationship quality significantly predicted T2 relationship quality (β = .76, p < .001) and T1 parenting was linked to T2 parenting (β = .53, p < .001) as shown in Table 2. None of the indirect effects were significant for fathers in the control group (see Table 3).
Discussion
The goal of this study was to compare the treatment mechanisms of an evidence-based relationship distress prevention program (CCET) with an evidence-based parenting program (Triple P) and a control group on children’s problem behaviors in 150 parents. The main study hypothesis that each program yields positive effects through specific mechanisms (either the improvement of relationship quality in case of CCET or the enhancement of parenting in case of Triple P) was confirmed in mothers. Our results indicate that the couple-focused program, CCET, enhanced mothers’ relationship quality, which, in turn, led to a significant reduction in mothers’ reports of child behavioral problems. The effect of the mothers’ relationship quality at pre-assessment on child behavioral problems 2 weeks after the treatment was mediated by the mothers’ relationship quality at post-assessment showing that the enhancement of relationship quality accounted for the benefits in child adjustment. On the other hand, as expected, improved maternal parenting mediated the treatment effects on child behavioral problems in mothers of the Triple P group. Thus in mothers both programs yielded expected results regarding the underlying mechanisms of effects of the two different prevention programs on child adjustment (enhanced relationship quality in CCET versus enhanced parenting in Triple P). Interestingly, there was a different pattern of results in fathers. CCET reduced dysfunctional parenting in fathers and this largely explained the reduction in child behavioral problems, a finding that does, at a first glance, not correspond to our hypothesis. Enhanced relationship quality only moderately mediated the treatment effects in fathers of the CCET group.
Our findings match previous research. Cowan et al. (2005) found that improved conflict communication explained the positive effects of the couple-focused program on children’s adaptation and positive parenting mediated the efficacy of the parenting training. These findings are consistent to the present results in mothers. Additionally, the results for the study by Cowan et al. (2005), in which couples who benefited from the couple-focused program showed also improved parenting, are consistent with our findings in men. There are several reasons that may help to explain the gender effects found in our research: We know from other studies (Sanders et al. 2000) that the efficacy of Triple P is usually higher in mothers than in fathers, as it was also the case in the original study of the current reanalysis (Bodenmann et al. 2008b). In many Western and European countries, mothers continue to hold the primary caregiving function for their children in most households. Given this traditional distribution of gender roles, it is plausible that mothers may be substantially more engaged in parenting skills trainings and their successful implementation at home than men. Furthermore, prior research found that mothers are better capable to compartmentalize their roles as parent and as spouse, leading to less spillover from the interparental to the parent–child relation (Cummings et al. 2004). Fathers are more susceptible to spillover effects; that is, couple conflict affects children’s wellbeing by undermining childrearing practices or interfering with sensitive parenting in fathers, disproportionally more than in mothers (Davies et al. 2009; Sturge-Apple et al. 2006). In positive terms, this weaker ability in males’ role compartmentalization could also explain why the couple-focused program reduced child behavior problems by paternal parenting in our study. When CCET fostered pair bonding, enhanced constructive conflict communication, and trained the mutual availability of the partners as a source of support, parenting of fathers might be less vulnerable to deterioration in the face of couple conflict. Additionally, since CCET explicitly focuses on reducing stress in couples by the enhancement of individual and dyadic coping skills, fathers may again benefit better in terms of parenting skills because this is an effective means of forestalling stress to impede positive parenting. It might be possible, and this hypothesis needs to be tested in a future study, that the CCET strengthened relationship quality and by this means positive, more consistent parenting that went along with better child outcome. Thus, a double mediation might be potentially the case in men.
Typically, interventions or prevention programs for couples aim to change relevant couple skills (such as communication, problem-solving, dyadic coping) by reducing destructive behaviors and increasing constructiveness between partners (Halford et al. 2003). Since the majority of these studies address couples in their middle age, it is likely that a considerable number of them have children (Cowan and Cowan 2002). Furthermore, the children’s well-being is frequently an important reason for parents to seek couple therapy (Doss et al. 2004). Against this backdrop, it seems astonishing that relatively little headway has been made to systematically examine whether couple-focused interventions also affect children’s adjustment and by which mechanisms these programs work. Earlier prospects emphasizing that impaired parenting is the exclusive way through which interparental conflict harms child well-being (e.g., Fauber et al. 1990) have become untenable given the preponderance of evidence showing that interparental conflict affects children also directly (Cummings and Davies 2010). That said, it seems that researchers increasingly acknowledge the significance of treating the interparental relationship in order to foster a healthy development for children. This study provides further evidence that children also benefit from couple-focused interventions for parents. The enhancement of the quality of the interparental relationship may yield benefits for child outcomes in its own right, that is, independent of parenting or potentially by indirectly also enhancing more consistent parenting between both partners. There is evidence accumulating that relationship education equal or enhance the efficacy of parenting trainings since relationship distress seems a considerable obstacle for the success of parenting and high relationship quality may vitally improve child adjustment by its positive effects on parenting (McCoy et al. 2013).
It is evident that parents who are satisfied in their close relationship and have sufficient communication skills may also benefit from these aspects in their parenting: They may define jointly parenting goals, and may show higher consistency and more congruent educational goals. There are programs emerging that address this goal explicitly. Growing research suggest that coparenting, that is, how parents cooperate in parenting, support each other in their parenting efforts, and manage conflict regarding child-rearing is an important predictor of family functioning and children’s well-being (McHale and Lindahl 2011). Hence, interventions focused on coparenting (in addition to parenting programs and CRE) is another potential means for the enhancement of family and child functioning and initial efficacy tests are promising (e.g., Feinberg et al. 2014; McHale et al. 2015). Although parenting programs have a primary focus on parenting skills, almost all of them emphasize the importance of the parents’ teamwork (i.e., coparenting) in raising children and this may be the potential leverage point for the reduction of child-related conflicts resulting from these programs. Moreover, some parenting programs integrate specific modules focused on the parents’ relationship adjunct to the original program when relationship distress is high. For instance, the Level 5 of Triple P (i.e., Enhanced Triple P, Pathways Triple P) offers intensive support for couples with serious problems focusing on the couples’ communication, conflict resolution and coping skills.
In sum, it may be wise to treat issues on parenting and the parents’ relationship functioning in clinical practice with children showing behavioral problems. Focusing on the child’s misbehavior distracts parents from their own relationship distress, which may lead to the neglect of addressing relationship problems in the treatment. Clinical work with children should also assess the quality of the parents’ relationship, since children are inevitably influenced by that relationship (Heinrichs and Prinz 2012). However, a major challenge for practitioners appears to gain an access to therapeutic progress in the parental relationship when parents seek therapy for their children. Particularly in cases of compulsory treatments (for example court mandated therapy after divorce) parents are usually not willing to work together in order to enhance positive communication and coparenting.
Several limitations of this study merit consideration. First, the most important weakness is that all study variables were assessed by self-report measures based on the parents’ perspectives exclusively. We thus have to acknowledge that effects may be inflated because of shared method variance. The inclusion of behavioral data on interparental behavior or parent–child interactions is clearly needed in potential replication. Moreover, family research without taking into account the children’s perception is inherently limited. However, the parents appear reliable informants on the target variables studied (i.e., interparental relationship, parenting, child behavioral problems). Second, since the primary interest of this report was to examine the process mechanisms which underlie the efficacy of the treatments we focused on the two time points prior to and 2 weeks after the completion of the intervention exclusively. Hence, we cannot draw from our analyses whether the mediational paths might also explain the treatment effects in the longer run. Third, since the interparental relationship precedes the parent-offspring relation it is enticing to consider relationship functioning and parenting as predictors of child adjustment, but the field would gain by more explicitly investigating the reciprocity between parents and children in family interactions. We considered this circumstance, at least, by allowing child behavior problems at T1 to be linked with the parents’ relationship quality and parenting skills at T1 and T2. Fourth, the participants constituted a universal prevention sample of couples without elevated child- or relationship-related problems. The generalizability of our results is thus limited. We cannot establish from our data how parenting or couple-focused approaches work in distressed couples and in families at risk for domestic violence or child abuse where the parents’ relationships are usually less stable and partners are less willing to attend to these programs.
Conclusion
The interparental relationship provides an important context for understanding child development. Research has begun to indicate that programs aimed at enhancing the parents’ relationship may be an effective way to prevent or treat child problems. With the above caveats in mind, the current study evidenced that a couple-focused intervention independently and differently reduced child behavior problems compared to a parenting training. Albeit this is an encouraging finding, it is urgently needed that couple-focused approaches are tested more frequently in their efficacy regarding child adjustment. Further replication and expansion of the present results help to illuminate how and why relationship education programs targeted towards helping parents to achieve satisfying relationships can contribute to children’s well-being. This is a seminal area of research because of its immanent potential to affect the health of many children.
References
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5(2), 137–144. doi:10.1037/1040-3590.5.2.137.
Barletta, J., & O’Mara, B. (2006). A review of the impact of marital conflict on child adjustment. Australian Journal of Guidance and Counselling, 16, 91–105. doi:10.1375/ajgc.16.1.91.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238–246. doi:10.1037/0033-2909.107.2.238.
Bodenmann, G. (1997). Dyadic coping—A systemic-transactional view of stress and coping among couples: Theory and empirical findings. European Review of Applied Psychology, 47, 137–140.
Bodenmann, G. (2005). Dyadic coping and its significance for marital functioning. In T. A. Revenson, K. Kayser, & G. Bodenmann (Eds.), Couples coping with stress: Emerging perspectives on dyadic coping (pp. 33–50). Washington, DC: American Psychological Association.
Bodenmann, G., Bradbury, T. N., & Pihet, S. (2008a). Relative contributions of treatment-related changes in communication skills and dyadic coping skills to the longitudinal course of marriage in the framework of marital distress prevention. Journal of Divorce and Remarriage, 50(1), 1–21. doi:10.1080/10502550802365391.
Bodenmann, G., Cina, A., Ledermann, T., & Sanders, M. R. (2008b). The efficacy of the Triple P-positive parenting program in improving parenting and child behavior: A comparison with two other treatment conditions. Behaviour Research and Therapy, 46(4), 411–427. doi:10.1016/j.brat.2008.01.001.
Bodenmann, G., & Shantinath, S. D. (2004). The Couples Coping Enhancement Training (CCET): A new approach to prevention of marital distress based upon stress and coping. Family Relations, 53(5), 477–484. doi:10.1111/j.0197-6664.2004.00056.x.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. Bollen & J. Long (Eds.), Testing structural equation models (pp. 136–162). Newbury Park, CA: Sage.
Cowan, P. A., & Cowan, C. P. (2002). Interventions as tests of family systems theories: Marital and family relationships in children’s development and psychopathology. Development and Psychopathology, 14(4), 731–759. doi:10.1017/S0954579402004054.
Cowan, P. A., & Cowan, C. P. (2014). Controversies in couple relationship education (CRE): Overlooked evidence and implications for research and policy. Psychology, Public Policy, and Law, 20(4), 361–383. doi:10.1037/law0000025.
Cowan, P. A., Cowan, C. P., Ablow, J. C., Johnson, V. K., & Measelle, J. R. (2005). The family context of parenting in children’s adaptation to elementary school. Mahwah, NJ: Erlbaum.
Cowan, C. P., Cowan, P. A., & Barry, J. (2011). Couples’ groups for parents of preschoolers: Ten-year outcomes of a randomized trial. Journal of Family Psychology, 25(2), 240–250. doi:10.1037/a0023003.
Cummings, E. M., & Davies, P. T. (2010). Marital conflict and children: An emotional security perspective. New York: The Guilford Press.
Cummings, E. M., Faircloth, W. B., Mitchell, P. M., Cummings, J. S., & Schermerhorn, A. C. (2008). Evaluating a brief prevention program for improving marital conflict in community families. Journal of Family Psychology, 22(2), 193–202. doi:10.1037/0893-3200.22.2.193.
Cummings, E. M., Goeke-Morey, M. C., & Raymond, J. (2004). Fathers in family context: Effects of marital quality and marital conflict. In M. E. Lamb (Ed.), The role of the father in child development (4th ed., pp. 196–221). New York: Wiley.
Dadds, M. R., Sanders, M. R., Behrens, B. C., & James, J. E. (1987a). Marital discord and child behavior problems: A description of family interactions during treatment. Journal of Clinical Child Psychology, 16(3), 192–203. doi:10.1207/s15374424jccp1603_3.
Dadds, M. R., Schwartz, S., & Sanders, M. R. (1987b). Marital discord and treatment outcome in behavioral treatment of child conduct disorders. Journal of Consulting and Clinical Psychology, 55(3), 396–403. doi:10.1037/0022-006X.55.3.396.
Davies, P. T., Sturge-Apple, M. L., Woitach, M. J., & Cummings, E. M. (2009). A process analysis of the transmission of distress from interparental conflict to parenting: Adult relationship security as an explanatory mechanism. Developmental Psychology, 45(6), 1761–1773. doi:10.1037/a0016426.
Dinkel, A., & Balck, F. (2006). Psychometrische Analyse der deutschen Dyadic Adjustment Scale. Zeitschrift für Psychologie/Journal of Psychology, 214(1), 1–9. doi:10.1026/0044-3409.214.1.1.
Doss, B. D., Simpson, L. E., & Christensen, A. (2004). Why do couples seek marital therapy? Professional Psychology: Research and Practice, 35(6), 608–614. doi:10.1037/0735-7028.35.6.608.
Dretzke, J., Frew, E., Davenport, C., Barlow, J., Stewart-Brown, S., Sandercock, J., et al. (2005). The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children. Health Technology Assessment, 9, 1–253.
El-Sheikh, M., & Cummings, E. M. (1995). Children’s responses to angry adult behavior as a function of experimentally manipulated exposure to resolved and unresolved conflict. Social Development, 4, 75–91. doi:10.1111/1467-9507.ep11635789.
Emery, R. E., Fincham, F. D., & Cummings, E. M. (1992). Parenting in context: Systemic thinking about parental conflict and its influence on children. Journal of Consulting and Clinical Psychology, 60(6), 909–912. doi:10.1037/0022-006X.60.6.909.
Eyberg, S. M., & Pincus, D. (1999). Eyberg child behavior inventory and sutter-eyberg student behavior inventory-revised: Professional manual. Odessa, FL: Psychological Assessment Resources.
Faircloth, W. B., Schermerhorn, A. C., Mitchell, P. M., Cummings, J. S., & Cummings, E. M. (2011). Testing the long-term efficacy of a prevention program for improving marital conflict in community families. Journal of Applied Developmental Psychology, 32(4), 189–197. doi:10.1016/j.appdev.2011.05.004.
Fauber, R., Forehand, R., Thomas, A. M., & Wierson, M. (1990). A mediational model of the impact of marital conflict on adolescent adjustment in intact and divorced families: The role of disrupted parenting. Child Development, 61(4), 1112–1123. doi:10.1111/1467-8624.ep9102040967.
Feinberg, M. E., Jones, D. E., Roettger, M. E., Solmeyer, A., & Hostetler, M. L. (2014). Long-term follow-up of a randomized trial of family foundations: Effects on children’s emotional, behavioral, and school adjustment. Journal of Family Psychology, 28(6), 821–831. doi:10.1037/fam0000037.
Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London: SAGE.
Fincham, F. D. (1998). Child development and marital relations. Child Development, 69(2), 543–574.
Gattis, K. S., Simpson, L. E., & Christensen, A. (2008). What about the kids? Parenting and child adjustment in the context of couple therapy. Journal of Family Psychology, 22(6), 833–842. doi:10.1037/a0013713.
Goeke-Morey, M. C., Cummings, E. M., Harold, G. T., & Shelton, K. H. (2003). Categories and continua of destructive and constructive marital conflict tactics from the perspective of US and Welsh children. Journal of Family Psychology, 17(3), 327–338. doi:10.1037/0893-3200.17.3.327.
Goeke-Morey, M. C., Cummings, E. M., & Papp, L. M. (2007). Children and marital conflict resolution: Implications for emotional security and adjustment. Journal of Family Psychology, 21(4), 744–753. doi:10.1037/0893-3200.21.4.744.
Griest, D. L., Forehand, R., Rogers, T., Breiner, J., Furey, W., & Williams, C. A. (1982). Effects of parent enhancement therapy on the treatment outcome and generalization of a parent training program. Behaviour Research and Therapy, 20(5), 429–436. doi:10.1016/0005-7967(82)90064-X.
Halford, W. K., & Bodenmann, G. (2013). Effects of relationship education on maintenance of couple relationship satisfaction. Clinical Psychology Review, 33(4), 512–525. doi:10.1016/j.cpr.2013.02.001.
Halford, W. K., Markman, H. J., Kline, G. H., & Stanley, S. M. (2003). Best practice in couple relationship education. Journal of Marital and Family Therapy, 29(3), 385–406. doi:10.1111/j.1752-0606.2003.tb01214.x.
Heinrichs, N., Bussing, R., Henrich, E., Schwarzer, G., & Briegel, W. (2014). Die Erfassung expansiven Verhaltens mit der deutschen Version des Eyberg Child Behavior Inventory (ECBI). Diagnostica, 60(4), 197–210. doi:10.1026/0012-1924/a000115.
Heinrichs, N., & Prinz, R. J. (2012). Families in trouble: Bridging the gaps among child, adult, and couple functioning. Clinical Child and Family Psychology Review, 15(1), 1–3. doi:10.1007/s10567-012-0113-z.
Ledermann, T., Bodenmann, G., & Cina, A. (2007). The efficacy of the Couples Coping Enhancement Training (CCET) in improving relationship quality. Journal of Social and Clinical Psychology, 26(8), 940–959. doi:10.1521/jscp.2007.26.8.940.
McCoy, K. P., Cummings, E. M., & Davies, P. T. (2009). Constructive and destructive marital conflict, emotional security and children’s prosocial behavior. Journal of Child Psychology and Psychiatry, 50(3), 270–279. doi:10.1111/j.1469-7610.2008.01945.x.
McCoy, K. P., George, M. R., Cummings, E. M., & Davies, P. T. (2013). Constructive and destructive marital conflict, parenting, and children’s school and social adjustment. Social Development, 22(4), 641–662. doi:10.1111/sode.12015.
McHale, J. P., & Lindahl, K. M. (2011). Coparenting: A conceptual and clinical examination of family systems (Vol. xii). Washington, DC: American Psychological Association.
McHale, J. P., Salman-Engin, S., & Coovert, M. D. (2015). Improvements in unmarried African American parents’ rapport, communication, and problem-solving following a prenatal coparenting intervention. Family Process,. doi:10.1111/famp.12147.
Minuchin, P. (1985). Families and individual development: Provocations from the field of family therapy. Child Development, 56(2), 289–302. doi:10.2307/1129720.
Muthén, L. K., & Muthén, B. O. (1998–2012). Mplus user’s guide (7th ed.). Los Angeles, CA: Muthén & Muthén.
Naumann, S., Bertram, H., Kuschel, A., Heinrichs, N., Hahlweg, K., & Döpfner, M. (2010). Der Erziehungsfragebogen (EFB): Ein Fragebogen zur Erfassung elterlicher Verhaltenstendenzen in schwierigen Erziehungssituationen. Diagnostica, 56(3), 144–157. doi:10.1026/0012-1924/a000018.
Nowak, C., & Heinrichs, N. (2008). A comprehensive meta-analysis of Triple P-Positive Parenting Program using hierarchical linear modeling: Effectiveness and moderating variables. Clinical Child and Family Psychology Review, 11(3), 114–144. doi:10.1007/s10567-008-0033-0.
Rhoades, K. A. (2008). Children’s responses to interparental conflict: A meta-analysis of their associations with child adjustment. Child Development, 79(6), 1942–1956. doi:10.1111/j.1467-8624.2008.01235.x.
Sanders, M. R. (1999). Triple P-Positive Parenting Program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children. Clinical Child and Family Psychology Review, 2(2), 71–90. doi:10.1023/A:1021843613840.
Sanders, M. R., Kirby, J. N., Tellegen, C. L., & Day, J. J. (2014). The Triple P-Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clinical Psychology Review, 34(4), 337–357. doi:10.1016/j.cpr.2014.04.003.
Sanders, M. R., Markie-Dadds, C., Tully, L. A., & Bor, W. (2000). The Triple P-Positive Parenting Program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology, 68(4), 624–640. doi:10.1037/0022-006X.68.4.624.
Sanders, M. R., Markie-Dadds, C., & Turner, K. M. T. (2003). Theoretical, scientific and clinical foundations of the Triple P-Positive Parenting Program: A population approach to the promotion of parenting competence. Parenting Research and Practice Monograph, 1, 1–24.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods, 7(4), 422–445. doi:10.1037/1082-989X.7.4.422.
Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar dyads. Journal of Marriage and Family, 38(1), 15–28. doi:10.2307/350547.
Sturge-Apple, M. L., Davies, P. T., & Cummings, E. M. (2006). Hostility and withdrawal in marital conflict: Effects on parental emotional unavailability and inconsistent discipline. Journal of Family Psychology, 20(2), 227–238. doi:10.1037/0893-3200.20.2.227.
Webster-Stratton, C. (1994). Advancing videotape parent training: A comparison study. Journal of Consulting and Clinical Psychology, 62(3), 583–593. doi:10.1037/0022-006X.62.3.583.
Zemp, M., Merrilees, C. E., & Bodenmann, G. (2014). How much positivity between parents is needed to buffer the impact of parental negativity on child adjustment? Family Relations, 63, 602–615. doi:10.1111/fare.12091.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zemp, M., Milek, A., Cummings, E.M. et al. How Couple- and Parenting-Focused Programs Affect Child Behavioral Problems: A Randomized Controlled Trial. J Child Fam Stud 25, 798–810 (2016). https://doi.org/10.1007/s10826-015-0260-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-015-0260-1