
Abstract
Purpose
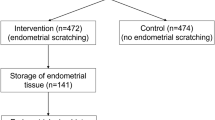
This prospective study investigates the correlation between vaginal microecology and pregnancy outcomes and explores their impact on endometrial microbiota composition during frozen embryo transfer (FET) cycles. Additionally, the impact of transvaginal Lactobacillus supplementation on reproductive outcomes in patients with previous failed cycles was assessed.
Methods
A total of 379 patients undergoing FET at a reproductive medicine center were categorized into clinical pregnancy (CP), miscarriage (MISC), and non-pregnant (NP) groups. Vaginal specimens were collected for microecological evaluation prior to embryo transfer. Endometrial microbiota samples were obtained during embryo transfer for 16S rRNA gene sequencing analysis to assess endometrial microbiota composition. Vaginal microecological indicators, including pH, Lactobacillus dominance, and leukocyte esterase activity, were measured. Transvaginal Lactobacillus supplementation was investigated in 60 patients with previous failed cycles.
Results
Vaginal microecology significantly correlated with pregnancy outcomes, with normal microecology associated with a higher clinical pregnancy rate. Vaginal pH and leukocyte esterase activity were significantly associated with clinical pregnancy. Furthermore, vaginal microecological differences significantly impacted endometrial microbiota composition. However, no significant differences were observed in endometrial microbiota composition among the CP, MISC, and NP groups. Notably, transvaginal Lactobacillus supplementation increased the clinical pregnancy rate without affecting the miscarriage rate.
Conclusion
This study highlights that normal vaginal microecology, characterized by lower pH and leukocyte esterase negativity, is associated with a higher likelihood of clinical pregnancy following FET. Importantly, vaginal microecological differences influence endometrial microbiota composition. Moreover, transvaginal Lactobacillus supplementation appears promising in improving clinical pregnancy rates in patients with previous failed cycles. These findings contribute to a better understanding of the interplay between vaginal and endometrial microbiota and offer potential interventions to enhance reproductive success in assisted reproductive technologies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Assisted reproductive technologies (ART) have significantly improved the management of infertility, offering hope to numerous couples worldwide. Among these technologies, frozen embryo transfer (FET) has emerged as a prominent approach due to its favorable outcomes, reduced risks, and increased success rates compared to fresh embryo transfer [1, 2]. Despite the progress in ART, the success of FET remains influenced by various factors, including the endometrial receptivity and microbiota, which play pivotal roles in the complex process of embryo implantation and early pregnancy establishment [3, 4].
In the context of reproductive health, the concept of vaginal microecology has gained increasing attention over the past decade. Traditional vaginal secretion testing methods have been limited by challenges such as precise timing of specimen collection, specimen quality, and the expertise of the examiner, resulting in relatively low accuracy and efficiency in diagnosing pathogenic infections and vaginitis. However, recent advancements in female vaginal microecological detection systems have demonstrated significant improvements, offering rapid, user-friendly, and comprehensive results, including clear morphological staining and functional assessments [5]. This enhanced approach enables a more accurate and comprehensive examination of pathogenic microorganisms, thereby providing valuable insights into the overall vaginal health.
In recent years, studies have indicated that vaginal microecological differences may exert substantial influence on endometrial microbiota, prompting further investigation into their potential impact on pregnancy outcomes in FET cycles. The establishment of a stable, Lactobacillus-dominated vaginal microbiota has been associated with a favorable reproductive environment, characterized by an acidic pH that inhibits harmful pathogens and supports embryonic development [6]. Conversely, vaginal dysbiosis, characterized by an imbalanced microbial composition, has been linked to adverse reproductive consequences, including infertility and an increased risk of preterm birth [7, 8].
In this study, we sought to investigate the correlation between vaginal microecological differences and pregnancy outcomes in FET cycles. Additionally, we aimed to examine the influence of vaginal microecological indicators on the composition of endometrial microbiota. Understanding these relationships could offer valuable insights into optimizing both vaginal and endometrial microecology for improved reproductive success in FET cycles, potentially enhancing the overall efficacy of ART procedures.
Materials and methods
Patient population
Patients who underwent FET in a hormone replacement therapy (HRT) cycle at the Reproductive Medicine Center of the Second Hospital of Chongqing Medical University between October 2020 and November 2021 were included in this study. For vaginal microecology analysis, a total of 379 patients met the inclusion and exclusion criteria. The inclusion criteria were as follows: non-smoking, aged between 20 and 40 years, having 2 good quality cleavage stage embryos, and having a normal uterus. The exclusion criteria were endometrial carcinoma, uterine adhesions, severe immune diseases, poorly controlled endocrine diseases, current reproductive tuberculosis (pelvic tuberculosis, endometrial tuberculosis), history of recurrent miscarriage and repeated embryo transfer failure, and reproductive tract infection with Neisseria gonorrhoeae, Chlamydia, Syphilis spirochetes, HPV, and HIV. No patients reported any symptoms in our study. Clinical pregnancy was defined as a intrauterine pregnancy up to 12 weeks of gestation. Miscarriage was defined as the loss of a pregnancy before the completion of 12 weeks of gestation.
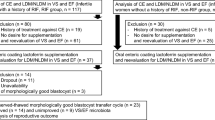
For investigating the impact of transvaginal Lactobacillus supplementation, we recruited 60 patients with previous failed cycles randomly assigned to control and treatment groups. Inclusion and exclusion criteria mirrored those mentioned earlier, excluding the history of recurrent miscarriage and repeated embryo transfer failure.
Vaginal secretion collection and microecological evaluation
Vaginal specimens were collected on the day of embryo transfer before the procedure. A sterile dry swab was used to gently rotate on the upper 1/3 of the lateral wall of the vagina collecting vaginal secretions for vaginal microecological assessment. Gram staining was performed to evaluate bacterial density, species of bacteria, dominant bacteria, leukocytes, and epithelial cells under a light microscope. Vaginal cleanliness and Nugent scores were determined following established protocols [5, 9].
Endometrial preparation and microbiota sampling
Endometrial microbiota sampling was performed during a hormone replacement therapy-frozen embryo transfer (HRT-FET) cycle. Prior to use, the transfer catheter, dish, and EP tube from the same lot number were tested for DNA contamination. After appropriate priming with oral estradiol (Femoston/estradiol, 1 mg bid) for 10–14 days, a trilaminar endometrium was achieved with a thickness ≥ 8 mm. When the appropriate hormonal status was confirmed, oral progesterone (Duphaston, 10 mg bid) was administered for 3 days. Before embryo transfer, the perineum was cleaned using cotton swabs soaked in iodophor solution while the patient was in the lithotomy position. A vaginal speculum was inserted, and vaginal secretions were removed using cotton swabs soaked in saline solution. Embryo transfer was performed with a double-lumen embryo transfer catheter (T-1731511, Pacific Contrast Scientific Instruments Co. Ltd., Jinan, Shandong, China) in an operating room with a ceiling air filtration system. To minimize the risk of cervicovaginal contamination, the outer sheath of the catheter was inserted into the endocervix without contacting the vaginal wall after removal of cervical mucus. Subsequently, the inner catheter containing the embryos at the top was inserted into the sheath and advanced into the uterine cavity. After the transfer, the inner catheter was re-sheathed, and both the sheath and catheter were withdrawn from the uterine cavity. The distal 1-cm portion of the inner catheter was then sterilely cut and placed in a DNA-free tube as described in a previous study [10]. The remaining transfer media served as a negative control.
16S rRNA gene amplification and sequencing
After cell lysis with Sodium Phosphate Buffer (Thermo Scientific, Waltham, MA, USA) and MT Buffer (Thermo Scientific), DNA extraction was performed using FastDNA® Spin Kit (MP Biomedicals, Santa Ana, CA, USA) according to the manufacturer’s instructions. To eliminate potential bacterial contamination during DNA processing and library preparation, one blank DNA extraction was processed as a background negative control for each batch of extractions. The V3-V4 region of the 16S rRNA gene was amplified via PCR using barcode-index primers 338F (5′-ACTCCTACGGGAGGCAGCAG-3′) and 806R (5′-GGACTACHVGGGTWTCTAAT-3′) using a TransStart FastPfu DNA polymerase (TransGen Biotech, Beijing, China) on a GeneAmp 9700 thermocycler (Applied Biosystems, Wakefield, RI, USA) as described previously [11]. The PCR amplification conditions were as follows: pre-denaturation at 95 °C for 3 min, followed by 30 cycles of denaturation at 95 °C for 30 s, annealing at 45 °C for 30 s, and extension at 72 °C for 45 s, with a final extension at 72 °C for 10 min.
Purification of amplified DNA products was performed using AxyPrep DNA Gel Extraction Kit. DNA sequences were read using Illumina’s MiSeq PE300. Quality control, sequence splicing, and noise reduction were carried out using the fastp, FLASH, and DADA2 plug-in in Qiime2, respectively. Species taxonomy analysis of ASVs (Amplicon Sequence Variants) was performed using the Naive Bayes classifier in Qiime2 based on the Silva 16S rRNA gene database (v 138).
Transvaginal Lactobacillus supplementation treatment
A live Lactobacillus capsule for vaginal use (Dingjunsheng, Inner Mongolia ShuangQi Pharmaceutical Co., Ltd.) was administered intravaginally for 30 consecutive days before the FET cycle initiation. The probiotic treatment with the live Lactobacillus capsule for women with gestational diabetes has been reported to improve maternal and infant health outcomes [12].
Statistical analysis
Statistical analysis was performed using R (version 4.0.0) and SPSS (version 24.0) software package (SPSS Inc., Chicago, IL, USA) to compare the differences between groups. Continuous variables were tested for normality, and parametric or non-parametric tests were used accordingly (Student’s t-test for normal distribution and Mann–Whitney U test for non-normal distribution). Continuous variables with normal distribution were presented as mean ± SD, while non-normally distributed continuous variables were expressed as median (25th percentile, 75th percentile). Categorical data were expressed as frequencies or percentages and compared between groups using the chi-square test. Differences were considered statistically significant at P < 0.05.
Results
Patients’ clinical characteristic
The study enrolled a total of 379 patients who underwent FET in a HRT cycle at the Reproductive Medicine Center of the Second Hospital of Chongqing Medical University. The patients’ mean age was 31.5 ± 3.8 years. The participants were categorized into three groups: clinical pregnancy group (CP group) (n = 194), miscarriage group (MISC group) (n = 39), and non-pregnant group (NP group) (n = 146). Comparison among the three groups revealed no statistically significant differences in baseline characteristics and cycle-associated parameters (P > 0.05, Table 1). Multivariate logistic regression was applied to assess the impact of patient characteristics and cycle-associated parameters on pregnancy outcomes, revealing no significant effects (P > 0.05, Table 2).
Correlation of vaginal microecological differences with pregnancy outcomes
To investigate the association between vaginal microecology and pregnancy outcomes, the microecological evaluations were compared among the CP, MISC, and NP groups. The chi-square test revealed a statistically significant correlation between vaginal microecology and pregnancy outcomes (χ2 = 17.344, P < 0.001, Table 3). Among the participants with normal vaginal microecology, 64.3% belonged to the CP group, 9.8% to the MISC group, and 25.9% to the NP group. In contrast, individuals with dysbiosis exhibited different proportions, with 43.2% in the CP group, 10.6% in the MISC group, and 46.2% in the NP group. The scoring values of vaginal microecological indicators were further analyzed (Table 4). Specifically, the vaginal pH was significantly lower in the CP group (53.6%) than in the MISC group (48.7%) and the NP group (33.6%) (P < 0.001). The leukocyte esterase negative rate was significantly better in the CP group (92.3%) and MISC group (94.9%) compared to the NP group (84.2%) (P = 0.03). Nevertheless, no significant differences were observed between the groups in terms of cleanliness degree, presence of pathogens, bacterial density, bacterial diversity, Lactobacillus-dominant microbiota, Nugent scores, Lactobacillus classification, catalase, and sialidase (P > 0.05).
Vaginal microecological indicators affect endometrial microbiota composition
In contrast to the previous work [3], our endometrial samples contained a low proportion of Lactobacillus (2.7%) (Fig. 1A). The top three predominant microbiota in the endometrial samples were Rhodococcus (23.7%), Pseudomonas (4.9%), and Achromobacter (4.1%). No statistically significant differences were found among the three groups in terms of endometrial microbiota composition (Fig. 1B, C) (P = 0.09). However, the abundance of Achromobacter was positively associated with clinical pregnancy, while the abundance of Romboutsia, Psychrobacter, Roseiflexaceae, and Chryseobacterium displayed negative correlations with clinical pregnancy (Fig. 1D). Fifteen microbiota including Nocardioides, Enterobacter, Roseiflexaceae, and Corynebacterium were associated with miscarriage (Fig. 1E).

Endometrial microbiota composition among clinical pregnancy (CP), miscarriage (MISC), and non-pregnant (NP) groups. A Pie chart for the microbial genera showing mean values of 10 most abundant genera in all endometrial samples. B Bar charts showing mean values of 10 most abundant genera. C Principal coordinate analysis (PCoA) plots indicating microbial similarity (P = 0.09) based on Bray–Curtis distances at the genus level. D Bar plots indicating the differences at the genus level between CP and NP groups using Student’s t-test (P < 0.05). E Bar plots indicating the differences at the genus level between CP and MISC groups using Student’s t test (P < 0.05)
Variance inflation factor analysis identified pH, LDM, Lactobacillus classification, catalase, and leukocyte esterase as the primary factors influencing endometrial microbiota composition (Table 5). Subsequently, using Bray–Curtis based dbRDA, we showed that microbial variation in endometrial samples was significantly explained by LDM (P = 0.01), Lactobacillus classification (P = 0.03), catalase (P = 0.008), and leukocyte esterase (P = 0.001) (Fig. 2A). Specifically, pH was correlated with the relative abundance of Lactobacillus and Bifidobacterium in the endometrial microbiota; Lactobacillus classification was related to the relative abundance of Rhizobiaceae, while leukocyte esterase was related to the relative abundance of Romboutsia and Roseiflexaceae (Fig. 2B).

Correlation between microbial composition and vaginal microecological indicators. A Distance-based redundancy analysis (db-RDA) triplot showing the association between microbiota variation and vaginal microecological indicators. B Heatmap of correlation between screened vaginal factors and endometrial microbiota. *P < 0.05, **P < 0.01
Transvaginal Lactobacillus supplementation improves pregnancy outcomes in patients with previous failed cycles
To investigate the impact of transvaginal Lactobacillus supplementation on reproductive outcomes, 60 patients with previous failed cycles were recruited, including 30 control patients and 30 patients with transvaginal Lactobacillus supplementation. The clinical characteristics of the participants are presented in Table 6. Transvaginal Lactobacillus supplementation significantly increased the clinical pregnancy rate, while the miscarriage rate showed no difference between the two groups (Table 7).
Discussion
In this prospective study, we aimed to explore the correlation between vaginal microecological differences and pregnancy outcomes in patients undergoing FET in an HRT cycle. Our results revealed that patients with normal vaginal microecology had a significantly higher frequency of clinical pregnancies compared to those with dysbiosis. The importance of a balanced and healthy vaginal microenvironment in supporting successful pregnancy outcomes has been recognized in previous studies [11, 13, 14]. Our findings support the notion that maintaining a stable and favorable vaginal microecology may be crucial for implantation and successful embryo development.
Interestingly, we observed that certain specific indicators of vaginal microecology were associated with clinical pregnancy. Notably, a lower vaginal pH was significantly associated with a higher rate of clinical pregnancies. A lower vaginal pH is indicative of a more acidic environment, which is considered beneficial for promoting the growth of Lactobacillus species. Lactobacilli, known for producing lactic acid, hydrogen peroxide, and bacteriocins, contribute to a healthy vaginal microenvironment by preventing the overgrowth of pathogenic microorganisms [15]. Our study found a higher proportion of Lactobacillus-dominant microbiota (LDM) in the clinical pregnancy group (60.3%) compared to the miscarriage (48.7%) and non-pregnant (50.0%) groups. Although a higher abundance of Lactobacillus has been associated with improved pregnancy outcomes [6], our results indicate a lack of a significant association between Lactobacillus dominance and pregnancy rates, raising questions about the role of endometrial biodiversity in fertility. Therefore, a comprehensive evaluation of fertility outcomes should consider the intricate interplay between vaginal microecology and endometrial microbiota, emphasizing the role of factors beyond Lactobacillus dominance in successful conception.
The genus Lactobacillus is dominated in endometrial microbiota in the majority of the uterine microbiome studies [3, 16,17,18,19]. A recent study also showed that women with a live birth within 12 months after a first failed IVF/ICSI cycle exhibited significantly higher Lactobacillus crispatus relative abundance compared to those without a live birth [20]. However, contrasting results in some studies revealed a low relative abundance of Lactobacillus in endometrial samples [21,22,23]. Our study also observed a low proportion of Lactobacillus in endometrial samples. Population-specific variations in microbiota composition, influenced by factors such as diet, geography, pollution, and genetics, could explain these differences [24]. As our study focused on IVF patients in Chongqing municipality, China, it is plausible that the method of microbiota sampling, regional and genetic variations may explain the distinct endometrial microbiota composition observed in our study. Therefore, it is essential to consider these factors when interpreting and generalizing our findings to other populations. While no significant differences were observed in the endometrial microbiota composition among the CP, MISC, and NP groups, further analysis revealed intriguing associations with specific bacterial abundances. Specifically, the abundance of Achromobacter displayed a positive correlation with clinical pregnancy, while the abundance of Romboutsia, Psychrobacter, Roseiflexaceae, and Chryseobacterium showed negative correlations. Several pathogenic microbiota including Nocardioides, Enterobacter, Roseiflexaceae, and Corynebacterium were associated with miscarriage. These findings provide insights into the complex interactions between vaginal and endometrial microecology, suggesting potential associations between specific bacterial taxa and reproductive outcomes.
In line with previous studies [15, 25], our variance inflation factor analysis highlighted the importance of pH, LDM, Lactobacillus classification, catalase, and leukocyte esterase as key factors influencing endometrial microbiota composition. Moreover, using Bray–Curtis based dbRDA, we demonstrated that microbial variation in endometrial fluids was significantly explained by LDM, Lactobacillus classification, catalase, and leukocyte esterase. We also revealed that the vaginal microecological indicators were associated with several specific endometrial microbiota. These results emphasize the intricate interplay between specific components of the vaginal and endometrial microecology, influencing overall reproductive success.
Interventions designed to enhance the vaginal microenvironment, such as Lactobacillus supplementation, have the potential to exert a positive influence on reproductive outcomes. Nevertheless, the impact of Lactobacillus supplementation on pregnancy outcomes is not consistent across studies [26]. Despite this, recent evidence suggests that introducing Lactobacillus into the vaginal milieu yields protective effects on the endometrium [27]. In our study, transvaginal Lactobacillus supplementation significantly increased the clinical pregnancy rate in patients with previous failed cycles, which aligns with some previous research [28]. The increase in the clinical pregnancy rate underscores the potential benefits of optimizing the vaginal microecology to create a more receptive endometrium for successful implantation and embryo development. Our study adds valuable insights into the practical application of interventions targeting the vaginal microbiota, offering a potential avenue for improving outcomes in patients with previous failed cycles.
Despite the valuable insights provided by our prospective study, certain limitations should be acknowledged. Firstly, the study’s specific patient population in Chongqing municipality, China, may limit the generalizability of the results to other regions or populations. Multicenter studies involving diverse patient cohorts and larger sample sizes are warranted to validate and extend our findings to a broader context. Secondly, the study focused on patients undergoing FET with HRT, potentially limiting the applicability of the findings to other infertility treatment modalities or natural conception. Lastly, while we collected comprehensive data on vaginal and endometrial microbiota, other factors such as lifestyle, diet, and hormonal profiles were not extensively explored. The influence of these variables on microbiota composition and pregnancy outcomes warrants further investigation.
Conclusion
In conclusion, our study not only highlights the association between normal vaginal microecology and a higher likelihood of clinical pregnancy following FET, but also introduces the positive impact of transvaginal Lactobacillus supplementation on reproductive outcomes in patients with previous failed cycles. Notably, normal vaginal microecology, characterized by lower pH and leukocyte esterase negativity, emerges as a key predictor of a higher likelihood of clinical pregnancy following FET. Moreover, our study demonstrated that vaginal microecological differences can influence the composition of the endometrial microbiota during FET cycles. These findings shed light on the intricate interactions between the vaginal and endometrial microenvironments and their potential impact on successful pregnancy outcomes. Further research is needed to explore the underlying mechanisms and clinical implications of these microbial interactions in the context of assisted reproductive technologies.
Data availability
The data and materials that support the findings of this study are available from the corresponding author on reasonable request.
References
Shi Y, Sun Y, Hao C, Zhang H, Wei D, Zhang Y, et al. Transfer of fresh versus frozen embryos in ovulatory women. N Engl J Med. 2018;378:2.
Roque M, Lattes K, Serra S, Sola I, Geber S, Carreras R, et al. Fresh embryo transfer versus frozen embryo transfer in in vitro fertilization cycles: a systematic review and meta-analysis. Fertil Steril. 2013;99:1.
Moreno I, Codoner FM, Vilella F, Valbuena D, Martinez-Blanch JF, Jimenez-Almazan J, et al. Evidence that the endometrial microbiota has an effect on implantation success or failure. Am J Obstet Gynecol. 2016;215:6.
Moreno I, Garcia-Grau I, Bau D, Perez-Villaroya D, Gonzalez-Monfort M, Vilella F, et al. The first glimpse of the endometrial microbiota in early pregnancy. Am J Obstet Gynecol. 2020;222:4.
Yue XA, Chen P, Tang Y, Wu X, Hu Z. The dynamic changes of vaginal microecosystem in patients with recurrent vulvovaginal candidiasis: a retrospective study of 800 patients. Arch Gynecol Obstet. 2015;292:6.
Baud A, Hillion KH, Plainvert C, Tessier V, Tazi A, Mandelbrot L, et al. Microbial diversity in the vaginal microbiota and its link to pregnancy outcomes. Sci Rep. 2023;13:1.
Gupta P, Singh MP, Goyal K. Diversity of vaginal microbiome in pregnancy: deciphering the obscurity. Front Public Health. 2020;8:326.
Wang L, Chen J, He L, Liu H, Liu Y, Luan Z, et al. Association between the vaginal and uterine microbiota and the risk of early embryonic arrest. Front Microbiol. 2023;14:1137869.
Nugent RP, Krohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991;29:2.
Franasiak JM, Werner MD, Juneau CR, Tao X, Landis J, Zhan Y, et al. Endometrial microbiome at the time of embryo transfer: next-generation sequencing of the 16S ribosomal subunit. J Assist Reprod Genet. 2016;33:1.
Fu M, Zhang X, Liang Y, Lin S, Qian W, Fan S. Alterations in vaginal microbiota and associated metabolome in women with recurrent implantation failure. mBio. 2020;11:3.
Okesene-Gafa KA, Moore AE, Jordan V, McCowan L, Crowther CA. Probiotic treatment for women with gestational diabetes to improve maternal and infant health and well-being. Cochrane Database Syst Rev. 2020;6:6.
Haahr T, Zacho J, Brauner M, Shathmigha K, Skov Jensen J, Humaidan P. Reproductive outcome of patients undergoing in vitro fertilisation treatment and diagnosed with bacterial vaginosis or abnormal vaginal microbiota: a systematic PRISMA review and meta-analysis. BJOG. 2019;126:2.
Haahr T, Jensen JS, Thomsen L, Duus L, Rygaard K, Humaidan P. Abnormal vaginal microbiota may be associated with poor reproductive outcomes: a prospective study in IVF patients. Hum Reprod. 2016;31:4.
Witkin SS, Mendes-Soares H, Linhares IM, Jayaram A, Ledger WJ, Forney LJ. Influence of vaginal bacteria and D- and L-lactic acid isomers on vaginal extracellular matrix metalloproteinase inducer: implications for protection against upper genital tract infections. mBio. 2013;4:4.
Moreno I, Garcia-Grau I, Perez-Villaroya D, Gonzalez-Monfort M, Bahceci M, Barrionuevo MJ, et al. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome. 2022;10:1.
Diaz-Martinez MDC, Bernabeu A, Lledo B, Carratala-Munuera C, Quesada JA, Lozano FM, et al. Impact of the vaginal and endometrial microbiome pattern on assisted reproduction outcomes. J Clin Med. 2021;10:18.
Ichiyama T, Kuroda K, Nagai Y, Urushiyama D, Ohno M, Yamaguchi T, et al. Analysis of vaginal and endometrial microbiota communities in infertile women with a history of repeated implantation failure. Reprod Med Biol. 2021;20:3.
Kitaya K, Nagai Y, Arai W, Sakuraba Y, Ishikawa T. Characterization of microbiota in endometrial fluid and vaginal secretions in infertile women with repeated implantation failure. Mediators Inflamm. 2019;2019:4893437.
Bui BN, van Hoogenhuijze N, Viveen M, Mol F, Teklenburg G, de Bruin JP, et al. The endometrial microbiota of women with or without a live birth within 12 months after a first failed IVF/ICSI cycle. Sci Rep. 2023;13:1.
Winters AD, Romero R, Gervasi MT, Gomez-Lopez N, Tran MR, Garcia-Flores V, et al. Does the endometrial cavity have a molecular microbial signature? Sci Rep. 2019;9:1.
Kyono K, Hashimoto T, Nagai Y, Sakuraba Y. Analysis of endometrial microbiota by 16S ribosomal RNA gene sequencing among infertile patients: a single-center pilot study. Reprod Med Biol. 2018;17:3.
Chen C, Song X, Wei W, Zhong H, Dai J, Lan Z, et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat Commun. 2017;8:1.
Gupta VK, Paul S, Dutta C. Geography, ethnicity or subsistence-specific variations in human microbiome composition and diversity. Front Microbiol. 2017;8:1162.
Borgdorff H, Tsivtsivadze E, Verhelst R, Marzorati M, Jurriaans S, Ndayisaba GF, et al. Lactobacillus-dominated cervicovaginal microbiota associated with reduced HIV/STI prevalence and genital HIV viral load in African women. ISME J. 2014;8:9.
Blancafort C, Llacer J. Can probiotics enhance fertility outcome? Capacity of probiotics as a single intervention to improve the feminine genital tract microbiota in non-symptomatic reproductive-aged women. Front Endocrinol (Lausanne). 2022;13:1081830.
Wang J, Li Z, Ma X, Du L, Jia Z, Cui X, et al. Translocation of vaginal microbiota is involved in impairment and protection of uterine health. Nat Commun. 2021;12:1.
Iwami N, Kawamata M, Ozawa N, Yamamoto T, Watanabe E, Mizuuchi M, et al. Therapeutic intervention based on gene sequencing analysis of microbial 16S ribosomal RNA of the intrauterine microbiome improves pregnancy outcomes in IVF patients: a prospective cohort study. J Assist Reprod Genet. 2023;40:1.
Acknowledgements
The authors express gratitude to Zhi Yuan, Chengguang Sun, and Hongliang Yi for collection and handling of endometrial microbiota samples.
Funding
This study was supported by the National Natural Science Foundation of China (82101710), Chongqing Medical Scientific Research Project (Joint Project of Chongqing Health Commission and Science and Technology Bureau, 2022QNXM023), Natural Science Foundation of Chongqing (cstc2021jcyj-msxmX0097), Strategic Collaborative Research Program of the Ferring Institute of Reproductive Medicine, Ferring Pharmaceuticals and Chinese Academy of Sciences (FIRMD200502), and the Kuanren Talents Program of the Second Affiliated Hospital of Chongqing Medical University.
Author information
Authors and Affiliations
Contributions
QW, LH, and SZ conceived and designed the study. HC, HZ, HZ, and SL recruited the patients. QW, HC, HZ, HZ, SL, JZ, and SZ performed the experiments. QW and SZ analyzed the data and created the figures. QW and SZ drafted and reviewed the manuscript. All authors read and approved the manuscript and all data were generated in-house and that no paper mill was used.
Corresponding authors
Ethics declarations
Ethical approval
Ethical approval for the study was obtained from the Ethics Committees of the Second Affiliated Hospital of Chongqing Medical University (2020–29).
Consent to participate
Written informed consent was obtained from all participants.
Consent for publication
Written informed consent for publication of their clinical details was obtained from the patients. The copies of the consent forms are available for review by the editor of this journal.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wei, Q., Chen, H., Zou, H. et al. Impact of vaginal microecological differences on pregnancy outcomes and endometrial microbiota in frozen embryo transfer cycles. J Assist Reprod Genet 41, 929–938 (2024). https://doi.org/10.1007/s10815-024-03066-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-024-03066-0