
Abstract
Purpose
To assess whether live birth rates (LBR) and maternal/neonatal complications differed following single fresh and frozen-warmed blastocyst transfer.
Methods
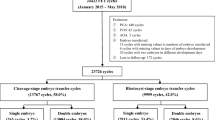
The present retrospective observational study analyzed 4,613 single embryo transfers (SET) (646 fresh and 3,967 frozen) from January 1, 2014, to December 31, 2018. Fresh embryo transfer at blastocyst stage was considered according to the age of the patient and her prognosis. In case of the risk of ovarian hyperstimulation syndrome, premature progesterone rise, non-optimal endometrial growth, or supernumerary embryos, cryopreservation with subsequent frozen embryo transfer (FET) was indicated.
Results
No differences in LBR were recorded. Fresh embryo transfers yielded an increase both in neonatal complications OR 2.15 (95% CI 1.20–3.86, p 0.010), with a higher prevalence of singletons weighting below the 5th percentile (p 0.013) and of intrauterine growth retardation (p 0.015), as well as maternal complications, with a higher placenta previa occurrence OR 3.58 (95% CI 1.54–8.28, p 0.003), compared to FET.
Conclusion
LBR appears not to be affected by the transfer procedure preferred. Fresh embryo transfer is associated with higher risk of neonatal complications (specifically a higher prevalence of singletons weighting below the 5th percentile and of intrauterine growth retardation) and placenta previa. Reflecting on the increased practice of ART procedures, it is imperative to understand whether a transfer procedure yields less complications than the other and if it is time to switch to a “freeze-all” procedure as standard practice.
Trial registration: Clinical Trial Registration Number: NCT04310761. Date of registration: March 17, 2020, retrospectively registered.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Embryo cryopreservation has become a recognized tool in assisted reproductive technology (ART), performed to protect women’s health, cryopreserve supernumerary embryos, and avoid further ovarian stimulation cycles if the fresh transfer is not successful [1]. The benefits of this procedure are many: it minimizes the risks of ovarian hyperstimulation syndrome (OHSS) [2, 3] and multiple pregnancy [4, 5] and maximizes cumulative live birth rate (CLBR) [6]. Additionally, cryopreservation allows to postpone embryo transfer when the endometrial preparation is suboptimal [7] or in case of premature progesterone rise. Moreover, cryopreservation has also been extended to cycles with pre-implantation genetic diagnosis/screening [8, 9].
Therefore, cryopreserving embryos gives the couple the opportunity of performing further transfers undergoing only a single controlled ovarian stimulation (COS) and oocyte retrieval with good clinical outcomes while maximizing CLBR [10].
Previous studies that analyzed different pregnancy outcomes comparing fresh and frozen single blastocyst transfers have shown for the latter increased maternal risks of placenta accreta and pregnancy-induced hypertension [11], and lower risks of placenta previa and placental abruption [12]. With regard to neonatal complications, literature reports for frozen transfers an increase in the rate of large for gestational age (LGA) [13] and a lower risk of very preterm birth, small for gestational age (SGA), and perinatal mortality [12].
Despite the increased use of frozen embryo (ET) transfer procedure, literature still lacks concrete up-to-date evidence to whether one procedure is superior to another. As a matter of fact, the large-scale study by Ishihara et al. [11], which analyzes different single ET procedures from 2008 to 2010, concludes that with the continuous improvement in ART techniques, it is important to provide new and more recent data on the topic.
The present study purpose, therefore, was to assess whether live birth rate (LBR) and maternal/neonatal complications differed following single fresh and frozen-warmed blastocyst transfers. In addition, our study intended to analyze transfers performed only in a single center in order to reduce any bias given by different operators’ dexterity or centers’ equipment. Moreover, by analyzing only single blastocyst transfers, and thus reducing any bias from twin pregnancies, our study provides further relevant information and evidence on the present still open debate.
Materials and methods
Study design and population
A single-center retrospective study was conducted at a University affiliated, tertiary care referral ART center. The focus of the study were single fresh and warmed day-five blastocyst transfers between January 1, 2014, and December 31, 2018.
To minimize the selection bias, the following exclusion criteria were considered: oocyte or sperm donation cycles and embryos subjected to pre-implantation genetic testing (PGT). No age limitations were considered. Only single embryo transfers (SETs) were included in both arms to reduce the bias due to twin pregnancies. Maternal and neonatal outcomes in these pregnancies, over the same period of time, were compared, corrected for the common covariates.
Interventions
In fresh cycles, the internal protocol between 2014 and 2018 established the usage of SET in good prognosis patients [14]. SET was chosen according to the age of the patient (< 35 years of age) and favorable factors, such as first cycle of in vitro fertilization, previous live birth (either natural or following ART), evidence of morphological good quality embryos, and supernumerary good quality embryos to allow cryopreservation [14]. The male partner’s infertility status was also considered, such as age, sperm quality, quantity, and source of spermatozoa. If the clinical presentation was feasible, after 5 days in culture, patients underwent fresh embryo transfer.
Cryopreservation with frozen embryo transfer (FET) was performed in women at risk of OHSS, premature progesterone rise, non-optimal endometrial growth, or in case of supernumerary embryos. Embryo transfer procedure relies on endometrial synchronization, and three main protocols were available: natural cycles (NC-FET), modified natural cycle (mNC-FET), and artificial replacement (AR-FET) [15].
ET procedure was carried out in a surgical theatre via transabdominal ultrasound scan (US) guidance and the use of a soft intrauterine catheter, following a pre-determined and standardized direct pre-load technique [16].
Patients’ follow-up
Clinical pregnancy was defined according to the ASRM/ESHRE definition as a pregnancy diagnosed by ultrasonographic visualization of one or more gestational sacs or definitive clinical signs of pregnancy; in addition to intra-uterine pregnancy, this definition includes clinically documented ectopic pregnancies. Delivery is defined as the complete expulsion or extraction of one or more fetuses, after at least 22 completed weeks of gestational age, irrespective of whether they are live births or stillbirths. Live birth rate was considered the complete expulsion or extraction from a woman of a product of fertilization, after 22 completed weeks of gestational age, which, after such separation, breathes or shows any other evidence of life, such as heartbeat, umbilical cord pulsation, or definite movement of voluntary muscles, irrespective of whether the umbilical cord has been cut or the placenta is attached, expressed per 100 ETs [17]. Twin delivery represents two live births [17].
Patient’s follow-up is performed by dedicated personnel which includes physicians and clinical psychologists, supported by the fetal-maternal staff throughout the pregnancy, generally with a 30- to 90-day interval. This data and those regarding pregnancy outcome, from delivery up to the end of the perinatal period (28 days after delivery), are reported in a dedicated section of the center’s internal database. This reduces the possibility of bias in data recording, but also any potential clinical interference.
Main outcomes
The main outcome of this study was the live birth rate (LBR). Secondary outcomes were neonatal and maternal complications.
Investigated neonatal complications included stillbirth, neonatal death, intrauterine growth restriction (IUGR), prematurity, macrosomia, and fetal malformations. In addition, the birth weight percentile per gestational week was calculated [18].
Maternal complications were gestational diabetes; pre-eclampsia; hypertensive disorders; threatened preterm labor (i.e., progression of cervical dilation and ripening caused by regular uterine contractions occurring before 37 weeks of pregnancy, which may result in preterm birth) or miscarriage; oligohydramnios; placenta previa; placenta abruption; premature rupture of the membranes; endocrine, autoimmune, or infectious disorders; and the rate of urgent Cesarean (C-) sections.
The analysis was corrected for the following covariates: maternal age and paternal age at induction, maternal body mass index (BMI), smoking history, years of infertility, primary or secondary infertility, ovarian reserve expressed as follicular stimulating hormone (FSH), anti-Müllerian hormone (AMH), and antral follicular count (AFC), and indication to treatment.
Ethical approval
Internal Ethical Committee approved the study design on April 7, 2020, and the protocol was registered in ClinicalTrials.gov (ID NCT04310761) prior to any data extraction and statistical analysis. Patients who underwent ART cycles had consented in writing that their medical records could be used for research purposes if their anonymity was ensured and protected.
All the relevant data for the study were collected using an exclusive internal web-based database, as already described in a previous study [19].
Statistical methods
Results were expressed as mean ± SD (standard deviation) or median (interquartile range (IQR)) or percentage, as appropriate. All variables were analyzed by univariate logistic regression, and variables with a p value less than 0.2 were then submitted to multivariate logistic regression analysis, to identify factors associated to outcome. Results of the logistic regression analysis were expressed as odds ratio (OR) and 95% confidence interval (CI).
All analyses were made with Stata 15.0 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC). Statistical significance was established at p < 0.05.
Results
Patient characteristics
During the 5-year period, a total of 4,613 single day-five blastocyst transfers were performed, among which 646 (14%) were fresh and 3,967 (86%) frozen transfers. As reported in Table 1, which displays the baseline characteristics of the embryo transfer population, significant differences existed between the two groups under investigation in maternal and paternal ages, infertility duration, ovarian reserve (expressed as AMH, AFC, FSH), and two specific indications to treatment: male and unexplained infertility. Mean female age at induction was 34.90 ± 3.97 for fresh and 35.97 ± 4.12 for frozen (p < 0.001) ETs. Regarding indication to treatment, male infertility accounted for 230 (35.6%) for fresh and 1,593 (40.2%) for frozen transfers (p 0.028), and unexplained infertility was recorded as 110 (17.0%) for fresh and 508 (12.8%) for frozen (p 0.003). Considering FET, the following transfer protocols were used: ART-ET 22.0%, NC-ET 15.2%, and mNC-ET 62.7%.
Live birth rate and other outcomes
The main outcome of the study is shown in Table 2: the live birth rate was 30.7%, 32.2% for fresh, and 30.5% for frozen ETs (p 0.382).
Out of 4,613 transfers, 2,047 (44.4%) clinical pregnancies were recorded. Biochemical pregnancies were not included in the analysis in accordance with the study protocol; these were 167.
Evolutive pregnancies were 1,653, of which 1,632 (86.8%) were single pregnancies, and 21(1.1%) twin pregnancies. Of these, 1,416 resulted in a live born neonate and 7 in stillbirth. The total number of abortions was 435 (23.1%); specific causes are shown in Table 2. Patients lost to follow-up were 4 (0.2%).
For both neonatal and maternal complications, complications were considered one if one or more complications occurred in a single neonate and woman, respectively.
Neonatal complications
For singleton pregnancies with delivery (n = 1,399) the highest prevalence of complication (5.4%) was observed upon fresh ET, compared to 2.6% for frozen ET (p 0.041), as shown in Table 3.
The mean birth weight (grams) was 3,183 ± 520 and 3,282 ± 526 for fresh ET and frozen ET, respectively (p 0.001). In addition, the 95th and 5th birth weight percentile per gestational week was calculated following the work of Nicolaides et al. of 2018 [18]. Notably, fresh ET resulted in a higher prevalence of singletons weighting below the 5th percentile, 12.9% compared to 7.4% in the frozen ET subgroup (p 0.013). The twin population (n = 17) was also analyzed, but no statistically relevant data were recorded concerning both neonatal and maternal complications in the two transfer groups. Investigating the single neonatal complications, a higher rate of intrauterine growth delay was reported by the fresh ET procedure subgroup: 3.3% versus 1.1% in FET (p 0.015).
Univariate and multivariate logistic regressions were performed to determine the relationship between the variables investigated and overall neonatal complications in fresh ET and frozen ET groups, as demonstrated by Table 4. Endometriosis and “other indication to treatment” were not included in the regression analysis since we had a recorded value of 0, and via the Fisher analysis, the p value was not statistically significant. In addition, only FSH was considered a variable for the assessment of female infertility as there is a strict correlation with the other two variables AMH and AFC.
The regression showed that the fresh ET procedure itself had a direct impact on the occurrence of the complications, with an OR of 2.15 (95% CI 1.20–3.86, p 0.010). p-values of less than 0.2 were then subjected to multivariate logistic regression analysis, confirming this result.
Maternal complications
As for maternal complications, a total of 501 (35.8%) and 10 (58.8%) were recorded in the group of singleton pregnancies with delivery (n = 1,399) and twin pregnancies with delivery (n = 17), respectively. No significant differences were observed between the two transfer procedure subgroups.
When single complications were analyzed, a higher prevalence of placenta previa was reported following fresh ET: 4.3% compared to 1.2% in FET (OR 3.58, 95% CI 1.54–8.28, p 0.003).
The same regression analyses were performed for the maternal complications (Table 5). Of statistical significance were maternal BMI and FSH (OR 1.05, 95% CI 1.01–1.09, p = 0.010 and OR 1.05, 95% CI 1.00–1.10, p = 0.035, respectively). Of interest was primary infertility, which was very close to reaching statistical significance: p 0.052. Multivariate logistic regression analysis further showed the significant impact of BMI, FSH, and primary infertility on maternal complications (OR 1.06 (95% CI 1.02–1.10) p = 0.004; OR 1.06 (95% CI 1.01–1.11) p = 0.019; and OR 1.3 (95% CI 1.02–1.69) p = 0.033, respectively).
Discussion
Our retrospective study shows that the LBR per total transfer was 30.7%, specifically 32.2% for the fresh ET procedure and 30.5% for frozen ET. Our study confirms the statement by Roy et al. that apparently there seems to be no statistical difference between the two transfer procedures (p 0.382) [20]. As for complications, fresh embryo transfers yielded an increase both in neonatal complications OR 2.15 (95% CI 1.20–3.86, p 0.010), with a higher prevalence of singletons weighting below the 5th percentile (p 0.013) and of intrauterine growth retardation (p 0.015), as well as maternal complications, with a higher placenta previa occurrence OR 3.58 (95% CI 1.54–8.28, p 0.003), compared to FET.
Research has suggested that singleton pregnancies after ARTs are associated with higher risks of obstetric and perinatal complications when compared with singleton pregnancies after spontaneous conception [21]. Understanding which procedure contributes to the greatest risk has now become mandatory. In fact, since the first successful live birth reported following frozen ET in 1984 [22], there has been an unsolved dilemma regarding which transfer procedure yields better neonatal and maternal outcomes, and if one has a higher pregnancy and LBR compared to another. As a matter of fact, the goal that an infertile couple seeks from ART procedures is a healthy, live born neonate. There have been multiple reports trying to solve this ongoing dilemma, without reaching a conclusive solution, with a handful of reports suggesting that warmed-thawed transfers yield an equivalent, or even higher pregnancy rate ([20, 23,24,25]. According to Aflatoonian et al., LBR resulted to be lower after FET [23]. Furthermore, it has been proved by Boomsma et al. that controlled ovarian stimulation (COS) causes direct and significant alterations on the endometrial milieu encountered by the embryo being transferred [26]. Thus, these deleterious effects on endometrial receptivity, and therefore on embryo implantation, during fresh-embryo transfer, could be avoided by exploiting natural cycle or artificial replacement cycles in frozen embryo transfer [27].
Considering that secondary outcomes of this study were the prevalence of both neonatal and maternal outcomes and that the factors that have an impact on the onset of obstetric complications in ART have been deeply investigated in the literature [28] and are still under debate, we decided to perform an analysis focusing on which, if any, individual complication had an association with the type of transfer procedure performed.
Our findings support the existing literature in that neonatal complications are more frequent in fresh ET than in frozen ET, with an OR of 2.15 (95% CI 1.20–3.86, p 0.01). Analyzing each single complication as a separate entity, this study revealed a higher prevalence of delay in intrauterine fetal growth in the fresh transfer procedure: 3.3% against 1.1% prevalence in frozen (p 0.019). Singletons born from the frozen ET had a statistically significant higher birthweight, on average 100 g heavier. But, despite this finding, only 6 newborns in singleton pregnancies appeared to be macrosomic (0.4% of all the live births). This could be explained by a higher prevalence of diabetes in the frozen population, i.e., 80 (6.6%), as compared to 8 (3.8%) in the fresh group. Nevertheless, this difference in weight does not appear to be of great clinical concern, considering also that only 3.7% of neonates had a birthweight above the 95th percentile.
In our study we performed a sub-analysis on the prevalence of neonatal complications in singleton and twin pregnancies. Despite only single embryo transfers were enrolled in this study, the overall twin delivery rate was 1.2%, 2.9% for fresh and 0.9% for FET. Despite only 17 twin pregnancies with delivery were recorded, a higher prevalence of complications occurred in this subgroup, 29.4% compared to only 3.0% in the singleton pregnancies. Indeed, of note is the potential impact of twin pregnancies on the total number of neonatal complications recorded. As a matter of fact, it is well known that multiple gestation pregnancies tend to have a more complicated clinical course than singleton pregnancies [29], and our results could have been influenced by their occurrence.
This finding could be explained by what Vega et al. reported [30] in a recent study. Vega et al. argue that there are three main causes responsible for twinning in SET:
-
1.
Zygotic splitting, which it is known to have a 1.3% prevalence in SET [31]
-
2.
Concomitant spontaneous conception
-
3.
Errors at the time of transfer (both in clinical and laboratory procedures)
While it is not possible to calculate the rate of the latter, Vega stated that concomitant spontaneous conception could be accounted for especially in the unexplained infertility subpopulation. It is possible, in fact, that this subpopulation, with the help of ART procedures such as controlled ovarian stimulation, could be able to spontaneously conceive, after sexual intercourse, thus leading to two embryos implanting and to a dizygotic twin pregnancy. Our data seems to agree, in our investigation, that unexplained infertility was the reason of 618 indications to treatment, for all cycles, 110 (17.0%) in the fresh ET and 508 (12.8%) in the frozen ET population, with a significant difference of p 0.003. Another cause could be an elevated BMI, which could lead to the incomplete oocyte retrieval, leading to the possibility of being spontaneously fertilized. This last finding was not confirmed in our population. On this regard, in our dataset of born twins, the monochorionic pregnancies were 11, and the dichorionic ones were 6. A total of 16 couples of twins were the same sex, and only one couple had different sex. No test for zygosity was performed.
Maternal complications
Maternal complications were first analyzed as a whole, showing no significant differences. When analyzed one by one however, a higher prevalence of placenta previa was observed in the fresh ET (4.29%), compared to 1.24% of the FET group (p 0.003). Our finding is in accordance with the literature that reports frozen ET having a lower risk of placenta previa compared to fresh [12]. Furthermore, upon univariate and multivariate logistic regression analyses, our study demonstrates that BMI, FSH levels, and primary infertility directly affect the rate of maternal complications.
Saunders et al., in 1988, was the first to state that infertility per se is an independent risk factor for subsequent problems during pregnancy [32, 33]. The comprehensive review of the literature on this topic, published by Palomba et al., states that “the level of evidence seems to be sufficient to suggest a direct relationship between infertility, subfertility factors and many adverse obstetric and neonatal outcomes” [32]. Our investigation showed an OR of 1.32 (95% CI 1.02–1.69) upon multivariate logistic regression analysis, regarding primary infertility. Remarkably, neither an increase in maternal nor paternal age seemed to have an effect on maternal complications, while it is well known that both have multiple adverse effects on pregnancy outcome and infertility [34, 35] even though maternal age seems to impact more spontaneous conception than ART-related pregnancies [36]. Another peculiar finding was the influence of high levels of FSH on the incidence of maternal complications, but since this was beyond the scope of the study, we decided not to investigate it further.
The primary strength of this study was the large number of single embryo transfers (n = 4,613) available for analysis and the length of the study period, i.e., 5 years. In addition, being the investigation focused solely on a single center, there are no confounding factors related to different procedures used by different centers nor on the method with which data were recorded and extrapolated. Furthermore, via the use of a dedicated phoning system, both embryo transfer and pregnancy follow-up could easily be guaranteed. Indeed, we only recorded a total of 4 patients lost to follow-up. Regarding possible study limitations, surely worth of mention is the retrospective design of the study. A further limitation of our study could be the design that did not consider a control arm of spontaneous conception and/or no history of infertility patients to compare neonatal and maternal complication rates with. It could have been important to perform such analysis on the very same population, but our university-affiliated tertiary care could not account on a physiological population, since it treats only infertile couples. Moreover, some data could have erroneously been recorded, despite the fact that data were retrieved from the center’s exclusive internal web-based database.
Conclusions
In conclusion, this single-center study focusing on LBR and maternal and neonatal outcomes after elective day-five single ET showed that single FET had a lower risk of neonatal complications and lower prevalence of placenta previa and of IUGR compared to single fresh ET when analyzed together. Indeed, fresh transfer has a higher neonatal complication rate compared to the frozen procedure.
Our study would appear to agree with the literature reporting that FET seems to be a safer option than a fresh transfer, certainly regarding the fetal counterpart. We found no difference in the LBR, which can still be taken as a positive outcome considering the incoherent data in the literature regarding this parameter. Further research is imperative to safely decide whether a “freeze-all” strategy, independent of the patients’ profile, should be implemented and whether it would be superior, in terms of live birth rate and outcomes, compared to a fresh transfer.
Data availability
Data and supplementary materials are available under request.
Code availability
Only under request.
References
Levi Setti PE, Albani E, Cesana A, Novara PV, Zannoni E, Baggiani AM, et al. Italian Constitutional Court modifications of a restrictive assisted reproduction technology law significantly improve pregnancy rate. Hum Reprod. 2011;26:376–81.
Gera PS, Tatpati LL, Allemand MC, Wentworth MA, Coddington CC. Ovarian hyperstimulation syndrome: steps to maximize success and minimize effect for assisted reproductive outcome. Fertil Steril. 2010;94:173–8.
D’Angelo A, Amso NN. Embryo freezing for preventing ovarian hyperstimulation syndrome: a Cochrane review. Hum Reprod. 2002;17:2787–94.
Martikainen H, Tiitinen A, Tomás C, Tapanainen J, Orava M, Tuomivaara L, et al. One versus two embryo transfer after IVF and ICSI: a randomized study. Hum Reprod. 2001;16:1900–3.
Veleva Z, Karinen P, Tomás C, Tapanainen JS, Martikainen H. Elective single embryo transfer with cryopreservation improves the outcome and diminishes the costs of IVF/ICSI. Hum Reprod. 2009;24:1632–9.
Malizia BA, Hacker MR, Penzias AS. Cumulative live-birth rates after in vitro fertilization. N Engl J Med. 2009;360:236–43.
El-Toukhy T, Coomarasamy A, Khairy M, Sunkara K, Seed P, Khalaf Y, et al. The relationship between endometrial thickness and outcome of medicated frozen embryo replacement cycles. Fertil Steril. 2008;89:832–9.
Ubaldi FM, Cimadomo D, Capalbo A, Vaiarelli A, Buffo L, Trabucco E, et al. Preimplantation genetic diagnosis for aneuploidy testing in women older than 44 years: a multicenter experience. Fertil Steril. 2017;107:1173–80.
Sacchi L, Albani E, Cesana A, Smeraldi A, Parini V, Fabiani M et al. Preimplantation genetic testing for aneuploidy improves clinical, gestational, and neonatal outcomes in advanced maternal age patients without compromising cumulative live-birth rate. J Assist Reprod Genet. 2019.
Scaravelli G, Levi-Setti PE, Livi C, La Sala G, Ubaldi FM, Greco E, et al. Contribution of cryopreservation to the cumulative live birth rate: a large multicentric cycle-based data analysis from the Italian National Registry. J Assist Reprod Genet. 2019;36:2287–95.
Ishihara O, Araki R, Kuwahara A, Itakura A, Saito H, Adamson GD. Impact of frozen-thawed single-blastocyst transfer on maternal and neonatal outcome: an analysis of 277,042 single-embryo transfer cycles from 2008 to 2010 in Japan. Fertil Steril. 2014;101:128–33.
Sha T, Yin X, Cheng W, Massey IY. Pregnancy-related complications and perinatal outcomes resulting from transfer of cryopreserved versus fresh embryos in vitro fertilization: a meta-analysis. Fertil Steril. 2018;109:330-42.e9.
Zhang J, Wang Y, Liu H, Mao X, Chen Q, Fan Y, et al. Effect of in vitro culture period on birth weight after vitrified-warmed transfer cycles: analysis of 4,201 singleton newborns. Fertil Steril. 2019;111:97–104.
Practice Committee of the American Society for Reproductive Medicine, Practice Committee of the Society for Assisted Reproductive Technology. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril. 2017;107:901–3.
Levi Setti PE, Cirillo F, De Cesare R, Morenghi E, Canevisio V, Ronchetti C, et al. Seven years of vitrified blastocyst transfers: comparison of 3 preparation protocols at a single ART center. Front Endocrinol (Lausanne). 2020;11:346.
Levi Setti PE, Albani E, Cavagna M, Bulletti C, Colombo GV, Negri L. The impact of embryo transfer on implantation–a review. Placenta. 2003;24 Suppl B:S20-6.
Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil Steril. 2017;108:393–406.
Nicolaides KH, Wright D, Syngelaki A, Wright A, Akolekar R. Fetal Medicine Foundation fetal and neonatal population weight charts. Ultrasound Obstet Gynecol. 2018;52:44–51.
Levi-Setti PE, Cirillo F, Scolaro V, Morenghi E, Heilbron F, Girardello D, et al. Appraisal of clinical complications after 23,827 oocyte retrievals in a large assisted reproductive technology program. Fertil Steril. 2018;109:1038-43.e1.
Roy TK, Bradley CK, Bowman MC, McArthur SJ. Single-embryo transfer of vitrified-warmed blastocysts yields equivalent live-birth rates and improved neonatal outcomes compared with fresh transfers. Fertil Steril. 2014;101:1294–301.
Pandey S, Shetty A, Hamilton M, Bhattacharya S, Maheshwari A. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: a systematic review and meta-analysis. Hum Reprod Update. 2012;18:485–503.
Zeilmaker GH, Alberda AT, van Gent I, Rijkmans CM, Drogendijk AC. Two pregnancies following transfer of intact frozen-thawed embryos. Fertil Steril. 1984;42:293–6.
Aflatoonian A, Mansoori Moghaddam F, Mashayekhy M, Mohamadian F. Comparison of early pregnancy and neonatal outcomes after frozen and fresh embryo transfer in ART cycles. J Assist Reprod Genet. 2010;27:695–700.
Zhu D, Zhang J, Cao S, Heng BC, Huang M, Ling X, et al. Vitrified-warmed blastocyst transfer cycles yield higher pregnancy and implantation rates compared with fresh blastocyst transfer cycles–time for a new embryo transfer strategy? Fertil Steril. 2011;95:1691–5.
Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C, Thomas S. Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: a prospective randomized trial comparing fresh and frozen-thawed embryo transfers in high responders. Fertil Steril. 2011;96:516–8.
Boomsma CM, Kavelaars A, Eijkemans MJ, Fauser BC, Heijnen CJ, Macklon NS. Ovarian stimulation for in vitro fertilization alters the intrauterine cytokine, chemokine, and growth factor milieu encountered by the embryo. Fertil Steril. 2010;94:1764–8.
Dieamant FC, Petersen CG, Mauri AL, Comar V, Mattila M, Vagnini LD, et al. Fresh embryos versus freeze-all embryos - transfer strategies: nuances of a meta-analysis. JBRA Assist Reprod. 2017;21:260–72.
Berntsen S, Söderström-Anttila V, Wennerholm UB, Laivuori H, Loft A, Oldereid NB, et al. The health of children conceived by ART: 'the chicken or the egg?' Hum Reprod Update. 2019;25:137–58.
Herruzo AJ, Martínez L, Biel E, Robles R, Rosales MA, Miranda JA. Perinatal morbidity and mortality in twin pregnancies. Int J Gynaecol Obstet. 1991;36:17–22.
Vega M, Zaghi S, Buyuk E, Jindal S. Not all twins are monozygotic after elective single embryo transfer: analysis of 32,600 elective single embryo transfer cycles as reported to the Society for Assisted Reproductive Technology. Fertil Steril. 2018;109:118–22.
Ikemoto Y, Kuroda K, Ochiai A, Yamashita S, Ikuma S, Nojiri S, et al. Prevalence and risk factors of zygotic splitting after 937 848 single embryo transfer cycles. Hum Reprod. 2018;33:1984–91.
Palomba S, Santagni S, Gibbins K, La Sala GB, Silver RM. Pregnancy complications in spontaneous and assisted conceptions of women with infertility and subfertility factors. A comprehensive review. Reprod Biomed Online. 2016;33:612–28.
Saunders DM, Mathews M, Lancaster PA. The Australian Register: current research and future role. A preliminary report. Ann N Y Acad Sci. 1988;541:7–21.
Pinheiro RL, Areia AL, Mota Pinto A, Donato H. Advanced maternal age: adverse outcomes of pregnancy, a meta-analysis. Acta Med Port. 2019;32:219–26.
Brandt JS, Cruz Ithier MA, Rosen T, Ashkinadze E. Advanced paternal age, infertility, and reproductive risks: A review of the literature. Prenat Diagn. 2019;39:81–7.
Wennberg AL, Opdahl S, Bergh C, Aaris Henningsen AK, Gissler M, Romundstad LB, et al. Effect of maternal age on maternal and neonatal outcomes after assisted reproductive technology. Fertil Steril. 2016;106:1142-9.e14.
Acknowledgements
The authors thank all the embryologists and gynecologists working in Humanitas Fertility Center, Rozzano, Milan, Italy.
Author information
Authors and Affiliations
Contributions
FC and PELS were involved in the study concept and design. LG, IP, and EM contributed to the acquisition of data. FC and EM analyzed data. LG and FC wrote the manuscript and had a primary responsibility for final content. FC and EM supervised the analysis. CR and AB contributed to bibliography updating and critically revised the manuscript and helped for data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Internal Ethical Committee approved the study design on April 7, 2020. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to participate and for publication
Patients who underwent ART cycles had consented in writing that their medical records could be used for research purposes and publication if their anonymity was ensured and protected.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Cirillo, F., Grilli, L., Ronchetti, C. et al. Retrospective comparison of pregnancy outcomes of fresh and frozen-warmed single blastocyst transfer: a 5-year single-center experience. J Assist Reprod Genet 39, 201–209 (2022). https://doi.org/10.1007/s10815-021-02362-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-021-02362-3