
Abstract
Purpose
Studies have demonstrated high implantation rates after trophectoderm biopsy of day 5 expanded blastocysts. However, biopsy of cleavage stage embryos may adversely affect embryo development and implantation. No studies have assessed the utility of day 5 morulae and early blastocyst biopsy. This study sought to better understand these slower embryos’ aneuploidy rates and implantation potential.
Methods
This was a retrospective review of all autologous IVF cycles utilizing PGS at a single academic infertility center.
Results
The biopsy of day 5 morulae and early blastocysts provided 22 % additional euploid blastocysts available for fresh day 6 transfer compared to day 5 biopsy of only expanded blastocysts. Aneuploidy did correlate with embryo stage on day 5, even after controlling for maternal age, with 16 % of morulae and 35 % of blastocysts being euploid. The majority (83 %) of euploid morulae progressed to the blastocyst stage by day 6. Experience transferring slower developing embryos is limited, but preliminary pregnancy and implantation rates appear similar to euploid embryos biopsied as expanded blastocysts.
Conclusions
The biopsy of all non-arrested embryos on day 5 provides genetic information for all blastocysts on day 6, increasing the pool of euploid blastocysts available for fresh transfer and avoiding the need to cryopreserve developmentally competent embryos without genetic information.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patients undergoing in vitro fertilization (IVF) have used pre-implantation genetic screening (PGS) to select euploid embryos for transfer, avoiding the transfer of aneuploid embryos which can be expected to fail to implant, implant and miscarry, or become a genetically abnormal pregnancy. While initial studies evaluating PGS using fluorescence in situ hybridization (FISH) with a day 3 biopsy failed to demonstrate a benefit of PGS on live birth rates [1, 2], recent trials using better aneuploidy screening methods and biopsy of later stage embryos have demonstrated an increase in implantation and live birth rates attributed to PGS [3, 4].
There are two commonly used approaches to utilizing PGS with a day 5 embryo biopsy: The first involves cryopreserving all embryos after biopsy, and transferring thawed embryos that were identified by PGS as euploid in subsequent thawed transfer cycles. Another approach aims for a fresh day 6 transfer. This also requires a trophectoderm biopsy on day 5 in order to have genetic information available for a fresh transfer the following day. While some groups have found a freeze all strategy to improve pregnancy and live birth rates [5], other centers have not yet observed any difference between fresh and frozen transfer outcomes [6], and fresh transfers do spare patients the financial costs and time incurred with waiting for a thawed transfer cycle.
Both strategies engage the question of what to do with embryos that have not yet reached the expanded blastocyst stage by the time of a day 5 biopsy. Many centers do not biopsy day 5 morulae or early blastocysts, limiting day 5 biopsy to only expanded or expanding blastocysts, and choosing to rather wait until day 6 to determine if subsequent development warrants day 6 biopsy and immediate cryopreservation of embryos that have not reached the expanded blastocyst stage on day 5 [7]. However, these slower but non-arrested embryos are frequently found to have progressed to blastocyst stage by the time of a day 6 transfer, and the inability to perform a day 5 biopsy on these embryos precludes the availability of genetic information by the time of a fresh day 6 transfer. Consequently these embryos are unavailable for fresh transfer and are frozen, potentially limiting the pool of euploid blastocysts available for transfer and unnecessarily subjecting both euploid and aneuploid blastocysts to freezing.
Biopsy of all non-arrested embryos on day 5 would provide timely genetic information on all embryos which are blastocysts at the time of a fresh day 6 transfer; however, the potential for day 5 morulae and early blastocysts to become a successful euploid pregnancy is unclear. Kroener et al. demonstrated that after a day 3 biopsy, day 5 morulae have a significantly higher overall aneuploidy rate than day 5 blastocysts [8]. However, the subset of day 5 morulae that became blastocysts on day 6—the most clinically important embryos—did not have any difference in aneuploidy rates compared to day 5 blastocysts, suggesting that the biopsy of day 5 morulae may be just as worthwhile as the biopsy of day 5 blastocysts when aiming for a fresh day 6 transfer. There have been inconsistent results regarding the implantation potential of day 5 non-blastocysts compared to day 5 blastocysts. While Shapiro et al. did demonstrate a higher implantation rate for embryos that are blastocysts by day 5 [9], these results were not consistent with other studies [10] and may have been confounded by the number of embryos transferred. Whether there are detrimental effects from biopsying morulae and early blastocysts on day 5 is also unknown. A recent randomized trial demonstrated a significant reduction in the implantation potential attributed to the biopsy of cleavage stage embryos on day 3 [3, 4], however no studies have evaluated the effects of biopsying morulae or early blastocysts on day 5.
This study’s objective was to assess the association with embryo stage at the time of day 5 biopsy with aneuploidy and subsequent development as well as provide additional information regarding the biopsy of day 5 morulae and early blastocysts when aiming for a fresh day 6 transfer with PGS.
Materials and methods
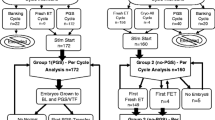
This was a retrospective review of all autologous IVF cycles with a day 5 PGS biopsy at a single academic infertility center between 2010 and 2014. Approval was obtained from the Stanford University Institutional Review Board (IRB-27769). Embryos were included if they were part of an autologous IVF cycle and had a biopsy for PGS on day 5 after fertilization. Only embryos from patients aged 30 to 45 were included. Only embryos with 24 chromosome analysis, and day 5 and day 6 development results available were included. Any cycles using previously cryopreserved oocytes were excluded. Embryos that were biopsied at cleavage stage were excluded.
Day 5 embryo stage was assessed once in the morning of the fifth day after fertilization (~115–120 h after fertilization). Embryos with any evidence of cavitation were considered blastocysts. Embryos with evidence of compaction but no cavitation on day 5 were considered morulae. All blastocysts were assessed using the Gardner grading scale, and blastocysts with a score of ≤2 were considered “early blastocysts”, while blastocysts with a score >2 were considered expanded blastocysts.
All embryos included were cultured according to our standard clinical practice: All embryos were group cultured until biopsy in SAGE sequential media under low oxygen conditions. All embryos underwent laser assisted hatching on day 3, and underwent biopsy 5 days (115–120 h) after fertilization. Day 5 morulae were placed in calcium magnesium free media until cell decompaction prior to biopsy and day 5 early blastocysts were placed directly in modified HDF media for biopsy. Biopsy was performed with laser assistance, and only peripheral cells were removed. Three to 5 cells were removed from day 5 early blastocysts, while only a single cell was removed from day 5 morulae.
Twenty-four chromosome screening was performed with either aCGH or SNP array by three PGS labs (IVIGEN/Blastogen, Reprogenetics, or Natera). Grading was performed by 1 of 5 embryologists. Charts were reviewed for embryo grade on day 5 and day 6, PGS results, and embryo fate (transfer, cryopreservation or discard). Subsequent transfer and pregnancy outcomes were recorded.
An additional retrospective chart review of all IVF cycles from January to December 2014 was used to identify a control group of day 5 non-blastocysts that were not biopsied on day 5, and had day 5 and day 6 embryo development or Gardner grade available. This cohort was used to conduct a preliminary assessment of the effect of morulae biopsy on subsequent embryo development.
Data was maintained on excel spreadsheets and the Stanford RedCap secure database, and initial statistical analysis was carried out using chi-square analysis, Fisher exact test, and ANOVA. A multivariable logistic regression was performed on SPSS software to create an odds ratio for the dependent variable of “euploid” based on the independent variables of maternal age at oocyte retrieval and whether or not the embryo was a blastocyst or morulae on day 5.
Results
There were 819 embryos, resulting from 142 IVF cycles and 113 different patients that were biopsied on day 5 during the study period and included in the study (Table 1). Eighty-one percent of the embryos were blastocysts at the time of day 5 biopsy and 19 % were day 5 morulae. Of the blastocysts biopsied on day 5, 24 % were early blastocysts. The mean patient age (37.5 vs. 37.7, p = NS) and mean baseline AMH values (2.79 vs. 2.86, p = NS) were similar between patients who had day 5 morulae and day 5 blastocysts biopsied.
Among the entire embryo population, Day 5 morulae had a significantly higher aneuploidy rate and no call rate (No call results are given when there is not sufficient genetic material to confidently make any conclusions regarding embryo ploidy) compared to embryos that were blastocysts on day 5 (Aneuploidy rate 84.5 vs. 64.6 %, p < 0.05; No call rate 5.9 vs. 2.6 %, p < 0.05). Using a multivariable logistic regression model to control for any confounding effects of maternal age, day 5 morulae still had a significantly lower likelihood of being euploid (OR 0.35 95 % CI(0.22, 0.55) than day 5 blastocysts (Table 2). This trend continued after stratifying patients by maternal age, reaching significance for all patients except those younger than 35 (Table 3). The age-related decline in euploid rates with increasing maternal age was steeper among day 5 morulae than day 5 blastocysts. Limiting analysis only to the day 5 morulae that progressed on day 6, the no call rate was 4.4 % and not significantly different than the no call rate among day 5 blastocysts. Among these day 5 morulae that progressed to blastocyst stage on day 6, there was still a trend of day 5 morulae having higher aneuploid rates than day 5 blastocysts, although this trend only reached significance among patients ages 35 to 40 (Table 4). The majority of day 5 morulae progressed to become blastocysts by day 6. Euploid day 5 morulae had a significantly higher rate of making blastocyst on day 6 compared to day 5 morulae that were aneuploid or had no results after PGS analysis (83.3 vs. 48.8 %, p < 0.05).
Among embryos with PGS results from a day 5 biopsy, the aneuploidy rate significantly decreased with increasing day 5 progression from morulae to early blastocysts to expanded blastocysts. (Table 5). Among aneuploid morulae, there was a higher number of chromosomes affected per embryo that subsequently arrested on day 5 compared to those aneuploid morulae that progressed to become day 6 blastocysts (5.3 vs. 3.1 affected chromosomes per embryo, p < 0.05).
To date there have been 6 former day 5 morulae transferred and 14 day 5 early blastocysts transferred. While 3 of the day 5 morulae and 5 of the day 5 early blastocysts were part of mixed transfers, also including a day 5 expanded blastocyst in the transfer, there were 4 single embryo transfers or transfers in which PGS gender results confirm which embryo implanted. Of these 4 transfers, 2 (50 %) former day 5 morulae implanted and led to a live birth and 1 (25 %) resulted in a biochemical pregnancy. There were 9 single embryo transfers of former day 5 early blastocysts. Five (55.6 %) of these resulted in a live birth or ongoing pregnancy, and 1 (11.1 %) resulted in a biochemical pregnancy.
In 2014, there were 141 day 5 morulae that were not biopsied as day 5 morulae. Sixty-one percent of these day 5 morulae progressed to become blastocysts on day 6. This progression rate was not significantly different to the observed progression rate of day 5 morulae that were biopsied as day 5 morulae (61.7 % vs 54.5 %, p = 0.21).
Discussion
Day 5 biopsy of all non-arrested embryos regardless of development stage provides the opportunity to have genetic information on all embryos eligible for transfer at the time of a fresh day 6 transfer. This study demonstrates that morulae and early blastocysts can be biopsied for PGS on day 5 in order to have genetic information available at the time of a fresh day 6 embryo transfer, be transferred and result in a successful pregnancy. While in this study aneuploidy rates of day 5 morulae and early blastocysts were significantly higher than embryos that were expanded blastocysts on day 5, there was a significant population of euploid day 5 morulae and early blastocysts that would be available for blastocyst transfer on day 6. These embryos would increase the pool of euploid blastocysts available for a fresh day 6 transfer. Additionally, the availability of genetic information on day 6 avoids the need to cryopreserve developmentally competent embryos without knowing whether they are euploid or not. This prevents subjecting euploid blastocysts that may be chosen for transfer to cryopreservation, and also avoids the labor, expense, and additional lab volume associated with cryopreserving aneuploid embryos.
Similar to a prior study [8] comparing the rate of embryo development with aneuploidy rates, this study did find that as a whole, slower developing embryos on day 5 had a higher aneuploidy rate compared with day 5 expanded blastocysts even after controlling for maternal age. Maternal age was controlled for in this study by both stratifying embryo cohorts by maternal age, and using a multivariable logistic regression model, with both analyses reaching similar conclusions. A prior regression analysis of our PGS data revealed that maternal age was the only IVF cycle parameter which significantly correlated with embryo euploid rates [11], prompting its inclusion in our model as the only independent variable other than day 5 embryo development. In contrast to Kroener’s findings, we observed that this difference in aneuploidy rates persisted between day 5 blastocysts and the subgroup of day 5 morulae that became blastocysts on day 6. This embryo subgroup is the most important population of day 5 morulae, as these are the embryos that would be considered for a fresh day 6 transfer. The difference in findings between studies may be attributable to the later day of biopsy in our study (Day 5) compared to theirs (Day 3), or the lower overall aneuploidy rate among day 5 blastocysts in our study. These findings are similar to a recent morphokinetic study that observed a delay in the initial compaction and blastulation among aneuploid embryos relative to euploid counterparts [12] but contrasts with a retrospective multicenter analysis that did not observe any significant difference in euploid or implantation rates between day 5 or day 6 blastocysts [7] and another morphokinetic study that did not find any correlation between aneuploid rates and the timing of initiation or completion of blastulation [13]. Due to the inconsistency of study results, a larger analysis with a diverse patient population and uniformity of chromosomal analysis is obviously needed. Although if euploid rates are similar between day 5 and day 6 blastocysts, this evidence would further support the practice of day 5 morulae biopsy for patients desiring a fresh Day 6 embryo transfer, assuming no harm to the embryo results from the morulae biopsy.
While we did observe a higher no call rate among day 5 morulae compared to day 5 blastocysts, this finding is less clinically relevant as when embryos that arrested on day 5—embryos that would not be considered for a fresh day 6 transfer or day 6 biopsy and cryopreservation—were excluded, the difference was not significantly different. Additionally, day 5 morulae with no call results from a day 5 biopsy that do not arrest can be re-biopsied on day 6 and then frozen, a practice similar to the traditional management of these slower developing embryos.
Despite a higher aneuploidy rate among slower developing embryos, any additional euploid embryo available for transfer is important from the perspective of the patient who may only need one euploid embryo to transfer. As the majority of day 5 morulae and early blastocysts will continue to progress, and many of these embryos that progress are euploid, these embryos have the potential to increase the pool of euploid embryos available for a fresh transfer. However, additional data is needed to provide reassurance that the biopsy of a day 5 morulae does not harm these slower embryos’ progression or implantation potential. Additionally, before widespread adoption of this practice, further analysis of Day 5 morulae determined to be aneuploid after a single cell morulae biopsy, is needed to confirm that PGS results from Day 5 morulae are not confounded by the mosaicism issues that plagued the clinical impact of PGS when cleavage stage embryos were biopsied on day 3 [14]. While this study was not designed to evaluate the safety of day 5 morulae or early blastocyst biopsy, the similar progression rates between biopsied and non-biopsied day 5 morulae, particularly among euploid morulae, is reassuring regarding the effects of the biopsy on subsequent embryo progression. Despite this initial reassurance, a prospective randomized trial comparing progression and implantation rates of non-biopsied day 5 morulae to biopsied day 5 morulae is needed to confirm these findings and ensure that the 16.7 % of euploid day 5 morulae that arrest on day 6 is not a consequence of the day 5 biopsy.
Another potential argument against the practice of day 5 biopsy of non-expanded blastocysts is the concern that biopsy of early blastocysts or day 5 morulae may impair the allocation of cells to the inner cell mass and other aspects of cavitation, or remove post-differentied cells destined to become the inner cell mass. However, only cells from the periphery of the embryo are biopsied, and evidence supporting the inside outside and cell polarity models of lineage specification [15] suggest that even if biopsy occurs after differentiation, these cells are destined to become trophectoderm and not inner cell mass. However while this theory and our limited initial implantation and pregnancy outcomes are reassuring, these results must be confirmed in a prospective trial.
The extremely limited experience with transfer of former day 5 morulae and early blastocysts prohibits any conclusions regarding the implantation potential of these embryos or any adverse effects on pregnancy outcomes resulting from the day 5 biopsy of these relatively slower developing embryos. Our initial experience and the observation of a similar live birth rate for biopsied former day 5 morulae and early blastocysts compared to our overall live birth rate after PGS biopsy and fresh transfer [6] is reassuring, but additional follow up is clearly needed for confirmation that the biopsy of less developed embryos on day 5 does not confer the same risk of impaired implantation observed after day 3 embryo biopsy in previous studies.
As cryopreservation techniques have improved over time, so have freeze-thaw survival rates. However, exposing euploid embryos that might otherwise be chosen for a fresh transfer to freezing does expose these embryos to the low possibility of reduced post-thaw viability, as well as potentially other less understood effects of freezing. Prior studies have demonstrated that post-thaw viability is higher among better quality embryos [16], and if these slower developing embryos are lower quality compared to day 5 expanded blastocysts, they may also be more vulnerable to any adverse effects of freezing.
The benefit of a freeze all strategy on pregnancy outcomes is currently under debate, and should frozen thawed embryo transfers eventually categorically prove to provide higher pregnancy rates with lower perinatal morbidity, our findings become less relevant. Fresh transfers do avoid the financial costs, increased cycle coordination, and temporal delay incurred as patients wait for a subsequent thawed transfer cycle. Most biopsied embryos were found to be aneuploid and have no potential to become a genetically normal pregnancy. Cryopreserving developmentally competent embryos without genetic information does not offer patients or providers information regarding how many of these embryos have the potential to become a normal pregnancy, and with the high aneuploidy rate observed, most cryopreservation and its associated costs are unnecessary. Additionally, while biopsy of all day 5 morulae leads to needless biopsy of the 40–45 % of day 5 morulae that will arrest on day 6, the cryopreservation—which is more time intensive than embryo biopsy—of aneuploid embryos creates needless labor and expense for embryology labs, and the increased volume of cryopreserved embryos takes up cryostorage space and increases the risk for laboratory error as embryologists are increasingly required to sort through goblets of carriers populated with a mix of euploid and aneuploid embryos.
Despite systematic classification of embryos by cavitation and Gardner grading, these are still subjective judgments that are vulnerable to inter-observer variability as well as the bias resulting from assisted hatching of all embryos destined for PGS biopsy which may have made it more difficult to distinguish between a non-expanded and an expanded blastocyst on day 5. The retrospective nature and the lack of a controlled comparison group of embryos to evaluate the effects of a day 5 biopsy on morulae and early blastocysts is another limitation. Future research will hopefully compare this cohort of embryos with embryos that are biopsied only after making blastocyst on day 6; however, while newer methods of PGS are drastically reducing the turnaround times for PGS analysis [17], at most centers currently, embryos biopsied on day 6 would not be available for a fresh day 6 transfer. Additionally, the embryos included in this study were analyzed by multiple labs and comprehensive chromosomal screening platforms, and variation between labs and screening methods may contribute to variations observed in our results.
Patients undergoing IVF with PGS need only one euploid embryo in order to proceed with an embryo transfer and have a chance to become pregnant with a genetically normal embryo. Much effort in IVF is spent trying to maximize the number of embryos available in order to increase the number of euploid embryos available to choose from. Patients aiming for a fresh day 6 transfer after PGS may increase the number of euploid blastocysts available for fresh transfer and also avoid the unnecessary task of cryopreserving aneuploid embryos by biopsying morulae and early blastocysts on day 5.
References
Northrop LE, Treff NR, Levy B, Scott Jr RT. SNP microarray-based 24 chromosome aneuploidy screening demonstrates that cleavage-stage FISH poorly predicts aneuploidy in embryos that develop to morphologically normal blastocysts. MHR: Basic Sci Reprod Med. 2010;16:590–600.
Fritz MA. Perspectives on the efficacy and indications for preimplantation genetic screening: where are we now? Hum Reprod. 2008;23:2617–21.
Scott Jr RT, Upham KM, Forman EJ, Hong KH, Scott KL, Taylor D, et al. Blastocyst biopsy with comprehensive chromosome screening and fresh embryo transfer significantly increases in vitro fertilization implantation and delivery rates: a randomized controlled trial. Fertil Steril. 2013;100:697–703.
Scott Jr RT, Upham KM, Forman EJ, Zhao T, Treff NR. Cleavage-stage biopsy significantly impairs human embryonic implantation potential while blastocyst biopsy does not: a randomized and paired clinical trial. Fertil Steril. 2013;100:624–30.
Roque M, Lattes K, Serra S, Sola I, Geber S, Carreras R, et al. Fresh embryo transfer versus frozen embryo transfer in in vitro fertilization cycles: a systematic review and meta-analysis. Fertil Steril. 2013;99:156–62.
Gustin SF, Zhao Q, Behr B, Lathi RB. Leveling the playing field – embryo transfers after trophectoderm biopsy have similar outcomes in fresh and frozen cycles. Fertil Steril. 2013;100:S194–5.
Capalbo A, Rienzi L, Cimadomo D, Maggiulli R, Elliot T, Wright G, et al. Correlation between standard blastocyst morphology, euploidy and implantation: an observational study in two centers involving 956 screened blastocysts. Hum Reprod. 2014;29:1173–81.
Kroener L, Ambartsumyan G, Briton-Jones C, Dumesic D, Surrey M, Munné S, et al. The effect of timing of embryonic progression on chromosomal abnormality. Fertil Steril. 2012;98:876–80.
Shapiro BS, Richter KS, Harris DC, Daneshmand ST. A comparison of day 5 and day 6 blastocyst transfers. Fertil Steril. 2001;75:1126–30.
Behr B, Gebhardt J, Lyon J, Milki A. Factors relating to a successful cryopreserved blastocyst transfer program. Fertil Steril. 2002;77:697–9.
Kort JD, Lathi RB, Zhao Q, Behr B, Baker VL. Are Anti-müllerian hormone levels predictive of aneuploidy rates? Fertil Steril. 2014;101(2 Supplement):e5–6.
Campbell A, Fishel S, Bowman N, Duffy S, Sedler M, Hickman CFL. Modelling a risk classification of aneuploidy in human embryos using non-invasive morphokinetics. Reprod BioMed Online. 2013;26:477–85.
Rienzi L, Capalbo A, Stoppa M, Romano S, Maggiulli R, Albricci L, et al. No evidence of association between blastocyst aneuploidy and morphokinetic assessment in a selected population of poor-prognosis patients: a longitudinal cohort study. Reprod Biomed Online. 2015;30(1):57–66.
Gonzalez-Merino E, Emiliani S, Vassart G, Den Bergh MV, Vannin AS, Abramowicz M, et al. Incidence of chromosomal mosaicism in human embryos at different developmental stages analyzed by fluorescence in situ hybridization. Genet Test. 2003;7:85–95.
Lorthongpanich T, Doris TPY, Limviphuvadh V, Knowles BB, Solter D. Developmental fate and lineage commitment of singled mouse blastomeres. Development. 2012;139:3722–31.
Tao J, Craig RH, Johnson M, Williams B, Lewis W, White J, et al. Cryopreservation of human embryos at the morula stage and outcomes after transfer. Fertil Steril. 2004;82:108–18.
Treff N, Tao X, Ferry K, Jing S, Taylor D, Scott RT. Development and validation of an accurate quantitative real-time polymerase chain reaction–based assay for human blastocyst comprehensive chromosomal aneuploidy screening. Fertil Steril. 2012;97(4):819–24.
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule Biopsy of day 5 morulae and early blastocysts may increase the pool of euploid blastocysts available for a fresh day 6 transfer and avoid unnecessary cryopreservation of aneuploid embryos.
Rights and permissions
About this article

Cite this article
Kort, J.D., Lathi, R.B., Brookfield, K. et al. Aneuploidy rates and blastocyst formation after biopsy of morulae and early blastocysts on day 5. J Assist Reprod Genet 32, 925–930 (2015). https://doi.org/10.1007/s10815-015-0475-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-015-0475-5