
Abstract
This study aimed to evaluate Promoting Reciprocal Relationships with Flexibility, Coaching, and Teaching (PRRFCT Match), a parent-mediated naturalistic developmental behavioral intervention package. An expansion from an earlier pilot study (see Kunze et al., 2021), PRRFCT Match incorporates virtual coaching between a novice coach and parent to implement evidence-based, applied behavior analytic (ABA) techniques during play to increase engagement and decrease unengaged behavior exhibited by their young child with developmental delays (26–50 months old). Ten parent-child dyads were matched with a coach in this concurrent multiple baseline design across participants. Simulating the clinical training level of a novice early interventionist, nine graduate student clinicians received training as coaches on PRRFCT Match implementation and weekly supervision by a research team member. All aspects of training and intervention were delivered virtually. A visual analysis of the data combined with Tau-U revealed a strong basic effect between clinician coaching and parent strategy use. For child participants, a visual analysis and Tau-U results suggest that most increased engagement and decreased their unengaged behavior during the intervention. High variability, overlap, and high engagement at baseline are discussed. This study shows promise for the PRRFCT Match intervention package. The ABA technologies mediated by parents during play increased child engagement and decreased unengagement for most participants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Developmental delays and differences (DD) in young children may affect their social engagement and play behaviors, impacting parent-child relationships and the family system more broadly (Crnic et al., 2017). Research shows that early intervention (EI) can maximize developmental gains by increasing learning opportunities during the period of early childhood, birth to 3 years of age, which is characterized by rapid brain development (Division for Early Childhood, 2014; Individuals with Disabilities Education Improvement Act of, 2004, 2004; Odom & Wolery, 2003). EI can support a child’s development and the family system as a whole, ultimately increasing the likelihood of long-term success in school and community (Guralnick, 1997).
Dyadic Connection of the Parent and Child
The theoretical focus of EI is to identify the ecological system (e.g., parent-child dyads, extended family, and community connections; Bronfenbrenner, 1979) to promote a network of supports. As such, evidence-based EI targets specific aspects of child development (e.g., speech-language therapy to promote communication) and the family system (e.g., behavior interventions to promote caregiver-child interactions). This comprehensive approach to EI is essential for families with children with DD and autism, given the complexities of the parenting role. Parenting a young child with DD often involves managing challenging behaviors, which commonly co-occur with communication and adaptive delays, increasing parenting stress and negatively impacting their mental health (Estes et al., 2009; Oono et al., 2013). EI has been effective in reducing challenging behaviors in young children with DD; however, emerging evidence suggests that targeting child behavior alone may be insufficient for supporting overall family well-being and dyadic relationships (McIntyre & Kunze, 2021; Schwartzman et al., 2022).
Given that family well-being is likely nuanced and highly individual, it is imperative that EI is flexible and family-centered (i.e., including parents in the selection of interventions and goals). Family-centered EI considers family priorities and the impact of intervention participation on the family system. Additionally, these interventions are designed to support the overall functioning of the family (Estes et al., 2019). Aligned with family-centered EI, dyadic interventions, such as parent-mediated approaches, focus on building parents’ capacity to use behavior-changing strategies during meaningful daily routines effectively. Evidence suggests that dyadic parent-mediated, family-centered EI may decrease early social, emotional, and behavioral problems while increasing child social engagement within the family system (McIntyre & Kunze, 2021).
Parent-Mediated Naturalistic Developmental Behavioral Interventions
Family-centered, parent-mediated interventions (PMI) are increasingly used for young children with DD, given the additive benefits of supporting the parent, child, and dyadic interaction (Beaudoin et al., 2014). Such interventions consider parents’ pivotal role as their child’s first teacher by preparing parents to use evidence-based strategies with their children. Evidence-based PMI protocols share core methods for delivering content to parents and teaching parents to interact with their child to support their development. Adult learning approaches for teaching parents intervention implementation include coaching, video modeling, guided practice with feedback, written materials, and collaborative planning of activities to practice target skills (Lorio et al., 2020; Rush & Shelden, 2011).
Parent-mediated naturalistic developmental behavioral interventions (NDBIs), which combine behavioral and developmental perspective approaches (e.g., natural reinforcement in the primary environment, following the child’s lead), have demonstrated effectiveness in decreasing child-challenging behaviors and improving parent-child dyadic relationship (i.e., reciprocity and attachment), which is vital for family well-being and overall functioning (e.g., Project ImPACT, Ingersoll et al., 2017; JASPER, Kasari et al., 2010). Variation in intervention components is necessary to meet the needs of each child and caregiver, and such individualization results in complex protocols that require an experienced skill set to be delivered effectively. The unforeseen outcome of such complexity is the need for highly trained, seasoned professionals to deliver such intervention packages. However, EI providers often do not have the time to attend lengthy training nor the capacity to implement complicated interventions (Bruder et al., 2021; Griffith et al., 2023). This speaks to the need for less complex yet highly effective intervention packages and protocols tailored to novice interventionists’ skill sets with potential for inclusion in pre-service training (Ingersoll et al., 2023).
Virtual Coaching in Parent-Mediated Interventions
Given the effects of the novel coronavirus (COVID-19) on face-to-face intervention, virtual (smartphone, computer, or tablet) delivery of interventions became an invaluable tool for linking families with state-of-the-art therapy while reducing potential physical and psychological barriers (e.g., distance, scheduling, time constraints, stigma, and health risks; Newman, 2004; Nicholl et al., 2017; Ruskin et al., 2004; Tate & Zabinski, 2004). Virtual coaching is an interaction between an interventionist (i.e., coach) and a caregiver or parent who uses technology to communicate. The coach can observe interactions between the caregiver and child to provide support and feedback. This method of intervention delivery from a distance can address shortages of professionals caused by the client’s geographical isolation and the costs involved in provider or family travel (Delaigue et al., 2014; Simacek et al., 2017). Widespread shelter-at-home mandates during the COVID-19 pandemic forced many services to move online, and these virtual interventions enabled services to continue from a distance (Rodriguez, 2020).
Although no longer mandated, families have found the benefits of virtual interventions vast, and many have chosen to continue or supplement support services this way (Kunze et al., 2023). Virtual coaching of PMI for young children has increased in practice, and research on efficacy has been evolving in EI for over a decade. Meadan and colleagues (2016) described the importance of coaching partnered with parent training, suggesting the two are necessary for parents to effectively implement strategies during play or routine that will result in behavior change. In a randomized control trial by Lindgren et al. (2020), PMI using behavior consultation via telehealth (i.e., virtual coaching; telepractice) resulted in a 98% decrease in child-challenging behavior as compared to participants who continued with their current interventions (e.g., treatment as usual). More recently, research has targeted the fidelity and nuanced coach characteristics in the effectiveness of coaching parents to deliver interventions with their child. In a study by Pellecchia et al. (2023), results suggest that coaches who focused on collaboration with parents during their virtual intervention sessions were also successful in giving feedback to the parents, which increased parent’s use of strategies and improved child behavior.
PRRFCT Match Intervention Package
Promoting Reciprocal Relationships with Flexibility, Coaching, and Teaching (PRRFCT Match) intervention package expands evidence-based intervention options for young children with and at risk for DD and their caregivers. The current study tested the impact of this parent-mediated NDBI on the increase of reciprocal engagement between parent and child. Parent engagement is defined by strategy use as taught during intervention sessions. Child engagement is defined as a child’s action involving their parent in play, such as showing, giving, or receiving an object, verbally interacting, playing physically, or showing affection (e.g., hugging, cuddling). Unique to this study was the intent to train novice graduate-student coaches using a brief yet effective coach training to deliver the intervention package in response to the extended length and high complexity of other training protocols. Additionally, PRRFCT Match was prepared, delivered, and analyzed explicitly using virtual means. No components of this intervention package used an in-person component. This mode of delivery tested the flexibility and effectiveness of the training protocol and virtual intervention delivery, to ultimately reach providers and families despite geographic location.
This project expands a pilot study, Coaching via Telehealth: Parent-Mediated Intervention for Young Children on the Waitlist for an Autism Diagnosis (Kunze et al., 2021). The results from the pilot revealed a strong basic effect between the researcher-led intervention package, parent strategy use, and an increase in flexible child behavior for children suspected of autism. Participants rated the intervention as highly effective and usable. In PRRFCT Match, the intervention was modified to a more scalable and applicable package that can be used with a broader diagnostic category (e.g., developmental delay), wider age group of children (i.e., 24–50 months), and measurement of child play behavior as engaged or unengaged as a reflection of reciprocity during playtime between parent and child. Graduate students were trained to deliver PRRFCT Match, simulating the clinical training exhibited by entry-level early interventionists and the ease of training pre-service providers. Using a single-case experimental design (SCED), we aimed to examine the effects of PRRFCT Match, as coached by graduate students in EI and related fields, to increase child engagement during parent-child play in relation to each parent’s use of the intervention strategies, ultimately decreasing periods of non-engagement. Parent-child dyads were paired with a graduate student coach who delivered intervention education via virtual sessions. The following research questions (RQ) were tested. RQ 1- Is there a functional relation between the PRRFCT Match intervention and increases in the number of strategies the parent uses? RQ 2- Is there a functional relation between the parent-implemented intervention strategies and increases in child engagement during play?
Methods
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the University of Oregon (protocol #STUDY00000353 and 12/2021). Informed consent was obtained from all subjects involved in this study.
Participants
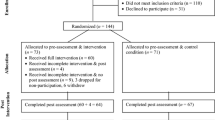
Eleven parent–child dyads (11 parents, 11 children) participated in this single-case experimental design study, and 10 completed the study and are included in the analysis here. Participant 11 dropped after baseline session 2 (data available upon request) due to limited time. Virtual flyers were posted on social media outlets of early intervention websites to recruit families with young children experiencing DD. Qualifying children (a) were between 18 and 60 months old at the time of consent, (b) demonstrated challenging inflexible behaviors, as reported by parents during intake and assessments, and (c) had a diagnosis or delay per parent report. Parents had (a) guardianship of the participating child, (b) lived in the same household as the participating child, (c) had access to an Internet-capable device with Bluetooth™ connectivity, (d) had Wi-Fi access, and (e) were willing to participate in all phases of the intervention. Table 1 summarizes child characteristics, including age, diagnosis, therapies, and sex. Table 2 summarizes parent demographics.
Setting and Materials
All assessment and intervention sessions occurred between the parent and research staff through virtual communication. All training and meetings among research staff also occurred through virtual communication. Coaches and researchers were either in a private university office or their home office during sessions and meetings. Parents selected a play space appropriate for child-parent interaction (e.g., outdoor play space, living room, child bedroom).
Coaches used a laptop with an internal video camera and speakers to conduct intervention sessions. Each parent used a tablet, laptop, or smartphone with a web camera and internal speaker. The coach assisted parents with camera placement and equipment usage during the first session- prior to baseline 1 data collection. Each device was connected through the family’s wireless, password-protected internet network, and encrypted audio-visual communication (i.e., Zoom, a video conferencing software), using 128-bit encryption that meets the requirements of the Health Insurance Portability and Accountability Act of 1996 (HIPPA), Pub. L. 104–191, 42 USC. §§ 1320 d et seq. Sessions were recorded for data collection using Zoom and stored in the University of Oregon secure cloud-based and HIPPA-compliant OneDrive and Dropbox. The project used numbers instead of names for all the information it collected and analyzed, and the data was stored in password-protected Dropbox files separate from other study data. Data will be stored for up to 5 years.
Educational materials and instructions for each intervention session were packaged in a shared virtual folder (Dropbox) post-baseline. A link to the folder was emailed to the parent by their coach before each session. Post-baseline materials included a handout of toys, activity ideas, and descriptions of types of play (e.g., flexible and inflexible). Intervention materials for parents included a PowerPoint overview, a sample video, and a reference sheet specific to the strategy introduced in that session. Parent practice was optional; a parent practice log was provided as a self-monitoring tool.
Researcher Roles
Nine graduate students participated as coaches in the study. Three coaches were pursuing a master’s degree in early intervention and six in school psychology. All coaches had experience working with children with developmental differences, with minimal experience working with parents. None of the coaches had experience coaching parents via virtual communication (i.e., Zoom) or specialized training in behavior analysis. Lead coaches, who supervised and assisted in training the coaches, were either BCBA, BCBA-D, or PhD with behavior analytic experience and knowledge. The principal investigator (PI) and first author was responsible for the overall study implementation and holds a PhD and BCBA-D.
Virtual Coach Training
Coach training included three 1-hour virtual sessions between the coaches, PI, and lead coaches. Coaches were trained on the study purpose and timeline, ABA strategies, and coaching components (see Kunze et al., 2021) for details on coaching components). Video examples were used in the training to demonstrate problem-solving and positive coaching exemplars. Coaches reached at least 90% correct on a knowledge assessment following the training sessions and prior to beginning coaching sessions. The coaches completed a Google doc designating their clinical interests, previous experience, and schedules. The PI reviewed the family intake and coach responses to match each coach with a dyad. Each coach was assigned a lead coach with whom they met weekly via Zoom or with an email check-in to discuss participant progress, receive feedback on recorded coaching sessions, and answer questions regarding intervention implementation. Each lead coach supervised between 1 and 4 coaches.
Advisory Board
We used a partner-driven process based on the Community Engagement Research model (CEnR; Isler & Corbie-Smith, 2012). The CEnR model ensures that project outcomes are grounded in the needs and preferences of those who will use it—parents of children with DD, neurodivergent young adults, community mental health providers, and EI providers. An advisory board was formed to guide the project. It included five members: a parent and their autistic adolescent child, a higher education professor with extensive clinical experience working with families and children with DD, an EI program director, and an EI provider. The advisory board met with the PI an average of 2 times (range 1–3) in group or individual virtual meetings during the year-long study. Advisory board meeting topics included (1) an overview of the project and discussion of key actions and barriers, (2) recruitment and coach training, and (3) outcomes and discussion of dissemination. Advisory board members provided broad project support, including feedback on (a) family recruitment, (b) intervention components, (c) resources for families, and c) conceptualizations of the utility and usability of PRRFCT Match. Recommendations and adjustments were incorporated into the study. Advisory board members were paid an honorarium of $25.00 for each meeting.
Procedures
All meetings and intervention sessions occurred virtually (i.e., synchronous virtual communication). Coaches and parents met once per week for baseline (5–9 times) and intervention (10 times). The study had four phases: (1) intake, (2) baseline, (3) intervention, and (4) post-intervention. Phase descriptions are detailed in Table 3.
Phase 1: Intake
For consent, parents received an email describing the study and a link to consent electronically using the University of XXX’s Qualtrics system. Once consented, a link to complete demographic intake and assessments was provided.
Parent ratings of child behavior were completed pre- and post-intervention to inform individualized intervention goals and assess intervention outcomes. Child inflexibility and repetitive behavior were assessed using The Repetitive Behavior Scale for Early Childhood (RBS-EC; Wolff et al., 2016) and The Behavior Inflexibility Scale (BIS; Lecavalier et al., 2020). The BIS was used pre-intervention only due to questionable sensitivity for children under 2. Child adaptive behavior was assessed using The Vineland Adaptive Behavior Scale, 3rd Edition (Vineland-III, Sparrow et al., 2016).
The RBS-EC (Wolff et al., 2016) measured the frequency of a child’s repetitive behaviors (e.g., inflexibility and insistence on sameness) per parent rating of 34 items on a Likert-type scale between 0 (does not occur) and 4 (occurs many times per day). The RBS-EC is a standardized measure to discriminate between repetitive behaviors considered developmentally typical and barriers to engagement. This scale can be used for children from infancy to early school age and takes approximately ten minutes to complete.
Similarly, the BIS (Lecavalier et al., 2020) measured the presence and interference of a child’s inflexible behaviors per parent rating of 38 items on a Likert-type scale between 0 (not a problem) and 5 (severe problem). The BIS results in a uni-dimensional overall inflexibility factor, particularly sensitive to ‘higher-order’ inflexible behaviors, such as insistence on sameness, rather than repetitive motor behaviors. As the BIS was normed on children three and older with autism, it was used cautiously to determine the goodness of fit for the behavior measurement of toddler-aged children with autism or DD. Thus, it was used in pre-intervention only.
The Vineland-III (Sparrow et al., 2016) Interview Form measured the frequency of children’s adaptive behaviors per clinician rating during a 45-minute parent interview on a Likert-type scale between 0 (never) and 2 (usually). The Vineland-III results in an overall Adaptive Behavior Composite (ABC) and component domain standard scores (M = 100, SD = 15), including Communication (Receptive, Expressive, Written), Daily Living Skills (Personal, Domestic, Community), Socialization (Interpersonal Relationships, Play and Leisure, Coping Skills), and Motor Skills (Fine Motor, Gross Motor; ages 0–2 years only). The Vineland-III is norm-referenced for individuals from birth to 90 years old and widely used for individuals with DD and disabilities.
Parent ratings of parenting stress and self-efficacy were measured. The Parent Stress Index - Short Form, 4th Edition (PSI-4; Abidin, 2012) was given as a pre-and post-measure measure of parent stress over time. The PSI-4, a self-report measure, can identify levels of stress in a parent-child relationship and took approximately ten minutes to complete. Parent self-efficacy was measured at pre- and post-intervention time points using the Self-Efficacy for Parenting Tasks Index – Toddler Scale (SEPS; Coleman & Hildebrandt Karraker, 2003). This assessment measures efficacy by parent self-report across seven domains of parenting: emotional availability, nurturance, protection, discipline, play, teaching, and instrumental care (Coleman & Hildebrandt Karraker, 2003).
Pre- and post-measure data for parents and children and the Vineland-III are presented in Table 4. Target behaviors for each child were initially identified in Phase 2, pre-baseline, during a brief parent-coach discussion of RBR-EC and BIS results, and general parent concern as a barrier to interaction. A more in-depth discussion of target behaviors was conducted post-baseline to minimize contamination of baseline sessions. Target behaviors were identified by their high scores on assessments and discussions with parents. High assessment scores were behaviors that scored two or higher on the RBS-EC, designating that the behavior occurs several times a day, and scores of 3 or higher on the BIS, which designates that the behavior is a moderate problem. Target behaviors for each child are listed in Table 4; see table note for specific behaviors.
Phase 2: Pre-Baseline, Baseline, Post-Baseline
The pre-baseline was a virtual meeting between the parent and coach to briefly review the completed child assessments and identify the target inflexible challenging behaviors to decrease. Following this brief meeting, concurrent observations established baseline performance for each dyad (within one week of each other). During baseline probes, parents were asked to play with their child as they usually would using preferred toys. The coach did not provide any feedback to the parent during baseline. The baseline length was between 5 and 7 sessions and was pre-determined for each dyad, and they were placed in either group A or B. Stable low parent performance (e.g., responding at levels of 0–3 per session) in baseline was hypothesized based on pilot data. If the parent response were highly variable, the dyad would continue in the baseline phase until stable responding was observed (see Ledford & Zimmerman, 2023). Dyads met with their coach once a week, with at least four days between sessions. Baseline sessions included a 10-minute observation, resulting in one baseline data point per meeting. Once a dyad completed its pre-determined baseline length and the parent had stable responses, baseline data collection was complete. A post-baseline meeting allowed for a more in-depth behavior discussion, a summary of baseline sessions, and an intervention introduction. Parents were paid a $25.00 stipend upon completion of baseline.
Phase 3: Intervention
Phase 3 included ten intervention sessions, 30 min each. All intervention sessions began with dyad interaction play to provide one data point. Each parent chose the materials for each play session with the coach’s input. Behavioral analytic, evidence-based intervention strategies specifically used to increase reciprocity were taught to parents in the context of play (Division for Early Childhood, 2014; Dracobly et al., 2017; Silbaugh et al., 2021; Steinbrenner et al., 2020; Wong et al., 2015). The ABA strategies introduced were environmental arrangement (Steinbrenner et al., 2020; Zimmerman et al., 2017), modeling (Francis et al., 2020; Frey & Kaiser, 2011; Quigley et al., 2018; Sam & AFIRM Team, 2016; Titus Dieringer et al., 2017) and prompting (Francis et al., 2020; Frey & Kaiser, 2011; Quigley et al., 2018; Sam & AFIRM Team, 2015; Titus Dieringer et al., 2017) with time delay, differential reinforcement of alternative behaviors (Savage & AFIRM Team, 2017; Tucker et al., 1998), response interruption and redirection (RIRD; Tomaszewski et al., 2017), and avoiding prompt dependency (Cividini-Motta & Ahearn, 2013). These strategies were specifically chosen because they decreased challenging behavior and increased flexibility in the pilot research (Kunze et al., 2021). Revisions to the pilot curriculum included coaching on (a) environmental arrangement, (b) time delay, and (c) avoiding prompt dependency. Table 5 defines each strategy, shows when it was introduced, and examples the coach used with the parent.
Strategies were introduced in a graduated sequence, beginning with an antecedent strategy (i.e., environmental arrangement), then the least intrusive strategy (i.e., modeling), and graduating to more directive strategies, as necessary, based on the child’s play skill set and responsivity. Time delay and reinforcement were strategies embedded within the parent-child interaction. Figure 1 is an overview of a strategy sequence used.

Strategy sequence
Phase 4: Post-Intervention
In phase four, the PI and parent met for a post-intervention meeting. Parents provided feedback to the PI on the intervention package and were asked to complete the post-intervention assessments. Upon completion, participants were paid a $75.00 stipend.
Experimental Design and Response Measurement
The study design combined single-case research and multiple baseline design, with non-experimental data collection using pre- and post-measures. A multiple baseline design requires three or more participants, with staggered baseline lengths of at least five data points before the beginning of the intervention, to align with the What Works Clearinghouse standards for single-case research (Kratochwill et al., 2013). Intervention start times for dyads were staggered (i.e., following baseline data points 5, 6, and 7) once variability was stable across baseline data points for parent responding. An extended baseline beyond this would require participants to continue longer without intervention, which is a concern due to potentially high attrition with this vulnerable population.
The level, trend, overlap, and variability of the dependent measures within and across participants across all tiers of the multiple baseline design was analyzed to demonstrate behavior change (Gast et al., 2014; Kratochwill et al., 2013). Visual inspection of graphed data provided valuable information related to intervention effects. As results showed clinically significant change based on visual analysis, a non-overlap estimator, Tau-U, was used (Parker et al., 2011; Kratochwill et al., 2013). Tau-U is a method for measuring data non-overlap between two phases (A and B) to determine the within-case effect size. It is a “distribution-free” nonparametric technique with a statistical power of 91–95%. Tau-U follows the “S” sampling distribution (as does Mann-Whitney U and Kendall’s Rank Correlation), so p-values and confidence intervals are available. Tau-U controlled for within phase trend, serial dependence in the data, and consistency in logic with single-case visual analysis. To calculate Tau-U and the single-case effect size calculator (Version 0.5), a web application was used and retrieved from https://jepusto.shinyapps.io/SCD-effect-sizes/ (Pustejovsky & Swan, 2018). The results were interpreted using a score of 0.65 or lower to indicate a weak functional relation; 0.66–0.92 indicated a medium to high relation and a strong relation of 0.93 or higher. A calculation of the standard mean difference will determine the between-case effect size for multiple baselines across a smaller number of participants (as in most single-case designs). To calculate the standard mean difference effect size, the single-case effect size calculator web application was used and retrieved from https://jepusto.shinyapps.io/scdhlm/ (Pustejovsky, 2020). The results were interpreted using a score below or above zero to indicate behavior change due to intervention.
Data Collection Procedures and Measures for Dependent Variables
Child engagement (i.e., engaged, unengaged, or un-codable) was coded per 5s interval during the 10-minute play between child and parent. The child was coded as engaged if they responded to or initiated interaction with the parent for 2 of the 5 s in the interval. Interaction initiation and responsivity were defined as a child’s action that involved the parent, such as showing, giving, or receiving an object, verbally interacting, playing physically, or showing affection (e.g., hugging, cuddling). The child was considered unengaged if they (1) did not initiate or respond to the parent verbally, physically, or with an object (showing or giving) or (2) demonstrated perseverative or self-stimulatory play and could not be interrupted to engage with the parent. The interval was marked as un-codable if the child left the play space or the interaction could not be clearly viewed. For each parent, the dependent variable was their correct use of intervention strategy sequences, as measured by the frequency of completed sequences during each 10-minute play session. Both parent and child behaviors were measured across the baseline and intervention phases.
Fidelity
For coach and intervention procedural fidelity, all sessions were recorded and coded using checklists developed by the first and second authors. Coach and intervention procedural fidelity was coded by the coach using a fidelity checklist (available upon request). Additionally, the PI or lead coach assessed fidelity for the first four intervention sessions and 30% of the sessions after that for each coach. Coach and intervention procedural fidelity was above 90% with no consistent error patterns. No coaches needed to be retrained due to low fidelity.
Inter-Observer Agreement
Inter-observer agreement (IOA) data for dependent variables (i.e., child behavior and parent strategy use) was collected for 33% of session videos asynchronously across dyads. Point-by-point IOA was calculated by subtracting disagreements from agreements, dividing by the possible outcomes, and multiplying by 100 to get a percentage for child behavior and parent strategy use. The PI and second author completed reliability data, reviewed disagreements, discussed discrepancies, and reached an agreement. IOA for parent strategy use averaged 95% (range 88–100%), and for child behavior averaged 85% (range 78–90%).
Social Validity
Social validity measures assess the appropriateness of the intervention strategies for each parent in the study. The Treatment Acceptability Rating Form-Revised (TARF-R; Reimers et al., 1992) can determine parents’ acceptability of an intervention (e.g., time commitment, cost, effectiveness, and understanding). The parent responded with 1 (strongly disagree) to 5 (strongly agree) for each item. Open-ended interview questions allowed for additional feedback, as seen as appropriate by each participant. Parent participants evaluated the social validity of the intervention and telepractice procedures. The modified TARF-R to assess the acceptability of the intervention is available by request from the first author.
Parents were asked to complete the TARF-R (Reimers et al., 1992) post-intervention to assess the parent-participant response to the intervention package components’ acceptability, efficacy, discomfort, and usability. Scores of treatment acceptability averaged 4.8 (range 4.0–5.0), and for effectiveness averaged 4.7 (range 4.0–5.0), where five was the highest possible for acceptability and effectiveness. Scores on the discomfort of the treatment package averaged 1.5 (range 1–2), where 1 is no discomfort. Table 6 shows the usability feedback for each strategy.
Post-intervention, a social validity assessment specific to the virtual delivery mode was also given. Scores for acceptability of delivery mode averaged 4.9 (range 4.0–5.0), with 5.0 as the highest rating, which is highly acceptable. Scores on the effectiveness of virtual meetings were 4.9 (range 4.0–5.0), with 5.0 as highly effective. Scores for the usability of materials and meeting format averaged 4.9 (range 4.0–5.0), with 5.0 representing virtual meetings as a highly usable format. Preference for virtual meetings compared to face-to-face averaged a 4.0 (range 1.0–5.0), with 5.0 representing a preference for face-to-face meetings over virtual meetings.
Results
Child Data
Figure 2 displays the results of multiple-baseline single-case data, which indicates a potential functional relation between the intervention and the child’s engagement during play. Researchers systematically manipulated the intervention and engaged in three attempts to demonstrate the effect of PRRFCT Match for participants in both Panels A and B.

Number of child’s engaged and unengaged intervals during play sessions
According to visual analyses of Panel A, compared to baseline data, increases in level and upward trends for engaged intervals are observed for Child 1, 2, 3, and 4 during the intervention phases, accompanied by decreases in level and downward trends for unengaged intervals, which suggests the intervention resulted in solid improvements for these four participants. An upward baseline trend and a large amount of overlap between phases for engaged intervals were observed for Child 5; additionally, unengaged intervals followed a downward trend during the baseline phase. All participants except Child 5 exhibited immediate increases in engaged intervals and decreases in unengaged intervals after introducing the intervention. A strong functional relation between the intervention and the child’s engagement was demonstrated for all participants except Child 5.
Based on visual inspection of data lines in Panel B, upward baseline trends with overlap at times between phases for engaged intervals were exhibited for child participants 6 and 8, indicating the intervention’s effectiveness was weak for these participants. Child 7, on the other hand, exhibited an evident increase in level for engaged intervals and a significant decrease for unengaged intervals after the intervention was in place. Minimal overlapping data points were observed between phases, suggesting the intervention effectively improves the quality of engagement for child 7. High variability in the baseline for children 9 and 10 carried forward to high overlap in the intervention phase, although an increase in engaged behavior is visible. A decrease in unengaged behavior for child nine is demonstrated, suggesting the intervention was successful for this participant for both unengaged and engaged behaviors. Due to the high overlap for Child 10, the outcomes are less conclusive, although engaged behavior occurs at a higher rate than unengaged behavior in the intervention phase.
Parent Data
Figure 3 displays the results of multiple-based single-case data for parent strategy use. Visual inspection for both panels indicates an evident, strong functional relation between PRRFCT Match and parents’ implementation of strategy sequences. Before the intervention, all parents engaged in low levels of proper strategy use; large increases in level and upward trends were exhibited for all parents during the intervention phases, accompanied by immediate improvements after the intervention was introduced and minimal overlapping data points between phases.

Number of parents’ correct strategy sequences during play sessions
Tau-U Data
Tau-U analyses measured the percentage of non-overlapping data between baseline and intervention phases. Results of Tau-U for each child and across all children were displayed in Table 7. For Panel A, Tau-U results for Child 5 are 0.43, p = .29, and − 0.64, p = .06, indicating a non-existent effect. The weighted Tau-U across the remaining four children is 0.82 (p < .001) and − 0.77 (p < .001), indicating the intervention is effective in increasing engagement and reducing unengagement during play routines for Child 1, Child 2, Child 3, and Child 4. For Panel B, Tau-U results suggest the intervention is only effective in increasing engagement for Child 7, Tau U: 0.68, p < .05, and has an impact in reducing un-engagement for Child 7 and Child 10, weighted Tau-U: − 0.64, p < .001.
Table 8 displays the results of Tau-U for parents’ strategy use. For Panel A and Panel B, the weighted Tau-Us across all parents are 0.89 (p < .01) and 0.93 (p < .01), which confirmed that parent coaching led to large increases in the implementation of intervention strategies for all parents.
Between-Case Effect Sizes
Between-case effect sizes (Pustejovsky et al., 2020) are displayed in Table 9. For the child’s engagement, the intervention effect is statistically significant and large in magnitude (g = 0.91, sg = 0.18). Regarding the child’s un-engagement, the intervention effectively reduced time spent unengaged with parents during play routines (g = − 0.84, sg = 0.17). For parents’ strategy use, the parent coaching is highly effective and generates large increases in the utilization of evidence-based practices (g = 1.27, sg = 0.26).
Nonexperimental Results
To explore whether PRRFCT Match positively impacts the child’s repetitive behavior, parenting stress, and parenting self-efficacy, a series of paired-sample t-test analyses were conducted (Table 10). Results suggest that although therapeutic effects were demonstrated by changes in raw scores in all three outcome measures, no statistically significant differences were observed after the intervention (t = 0.08, p = .94; t = 1.13, p = .29; t = − 0.83, p = .22).
Discussion
This SCED study aimed to determine the (a) effectiveness of coaching on parent’s use of the PRRFCT Match intervention strategies (RQ1) and (b) the impact of the parent-mediated intervention on child engagement during play (RQ2) for ten parent-child dyads as coached by novice student clinicians via virtual early intervention. In comparing the outcomes from the current study with the pilot data from Kunze and colleagues (2021), parent outcomes (RQ1) were successful in both trials, and child behavior change (RQ2) was found to be greater in the past research. Notable differences between the current and pilot study and implications for future research and practice are discussed here.
Additionally, non-experimental data using pre- and post-measures of child challenging behavior, parent stress, and parent self-efficacy were measured. While such measures clarify the characteristics and behaviors of participants, changes between pre- and post-timepoints of assessment were not significant in either study. This is expected as the primary outcomes were measured in RQ1 and RQ2 specifically, yet monitoring child-challenging behavior, parent stress, and parent self-efficacy to ensure no dramatic increases or decreases occurred due to participation in this intervention package is important. No significant outcomes here are likely due to the short duration of the intervention.
Parent Outcomes
RQ 1
PRRFCT Match intervention and increases in the number of strategies.
In answering RQ 1, results demonstrated improvement across all parents in using the intervention strategies during play sessions with their child. Increases in parent strategy use were immediate for most participants or occurred within the first three sessions for parents requiring more time to practice implementing what they had learned. As described in the pilot study (Kunze et al., 2021), parent strategy use was found to moderate child engagement and increase flexible play. It should be noted that significant changes in both parent and child behaviors occurred in sessions 10–15 of the pilot study, and the current study ended at session 10. This abbreviated package of ten sessions instead of 15 may have interrupted the opportunity for child engagement to increase further.
As recommended in the discussion of the pilot study research, avoiding prompt dependency was a specific topic for a coaching session in the present study. Additionally, the order of strategies from least to most support was revisited in each coaching session to support child-led interactions rather than opportunities for prompt dependent learning. Purposefully including coaching to avoid prompt dependency and least to most prompting may have resulted in a more naturally occurring, albeit slower-paced, behavior change.
Nonexperimental results of parent behavior included parent stress and self-efficacy. Differences between pre- and post-scores were not significant, which is expected due to the minimum time between tests and the light-touch nature of the intervention package. However, stress scores slightly decreased, and parental self-efficacy slightly increased on average, which is the desired direction for parent outcomes.
Child Outcomes
RQ 2
Parent-implemented intervention strategies and increases in child engagement.
For RQ 2, the results of child responses show variability across participants. Children 5, 6, and 8 showed no significant behavior change due to the intervention. Children 5 and 8 exhibited high levels of engaging behavior with lower levels of unengaged behavior at baseline, which remained constant through the intervention. Child 6 also had more engaged than unengaged behavior in baseline; however, it is difficult to draw conclusions from this participant’s performance due to high variability. Such participants may benefit from parent coaching on graduated play experiences where parents provide more complex social engagement opportunities (e.g., peer and sibling play) to encourage increased social development. All other child participants (i.e., 1, 2, 3, 4, 7, 9, and 10) demonstrated a decrease in unengaged behaviors during play with the participating parent in intervention, with most of this group (i.e., 1, 2, 3, 4, 7) also increasing their interactive engagement. Slower-to-respond participants, such as 1 and 4, may have benefitted from more direct parent coaching during intervention sessions (Barnett et al., 2017). The variation in responses may suggest that coaches should be prepared to exercise a broad skill set of behavioral interventions and adult learning techniques, allowing them to better address individual needs within each intervention session (Meadan et al., 2023). It should be noted that the variation in child outcomes is greater here than in pilot results, possibly due to the broader age and developmental ranges included in the current study.
Nonexperimental results of child behavior included challenging behavior as measured by the repetitive behavior scale reported by parents on pre- and post-measures. As expected, pre- and post-scores were not significant, partly due to the narrow window between the two assessment time points and the nature of the assessment, which is not designed to measure behavior change over time but rather provide a summary of current behavioral repertoire. Nonetheless, parents did report a decrease in the frequency of challenging behaviors between baseline and post-intervention.
Social Validity
As found in the pilot research, the parent participants rated the acceptability and efficacy of the PRRFCT Match as highly favorable. Parents also believed little to no discomfort was experienced by their children as participants in the intervention. Feedback on preferred strategy varied across participants. While some parents preferred environmental arrangement and modeling combined with prompting, others commented that RIRD was the most impactful strategy. This is a different outcome from the pilot research, where only one parent used RIRD once during intervention sessions. Another interesting outcome is the low use of reinforcement and the comment on the difficulty in identifying reinforcers despite the focus on verbal praise as a natural reinforcer during play exchanges. A mid-point social validity measure was not offered in the current study, and if it had been, it may have highlighted some areas needing further training.
Implications for Future Research and Practice
Four themes that should be considered in future research using PRRFCT Match and PMI in general have emerged. Considerations include (a) the number of intervention sessions, (b) variation in participant characteristics, (c) intervention individualization, and (d) the coach’s skill set, which are discussed here.
Number of Intervention Sessions
The current study included ten intervention sessions versus the pilot study, where 15 intervention sessions were implemented. While ten sessions were enough for the parents to learn and demonstrate the strategies in play with their child, some children had minimal change. Additional sessions, up to 5 more per dyad, may have resulted in more significant behavior change for the child participants. However, dosage alone would likely not be enough to increase already high levels of engagement, as seen for some participants. In a recent literature review by Frick et al. (2023), the authors point out that it is common for EI research to describe dosage as the number of times the child participated in the intervention (e.g., hours per month). Nevertheless, dosage should include an intervention’s frequency, content, and intensity. Because the correlation between additional sessions and positive child outcomes was demonstrated in the pilot study, it is recommended that future research using PRRFCT Match include 15 sessions rather than 10. However, further analysis of intervention adjustments for the content of parent-child interactions (e.g., what strategies are used and how frequently), intensity (e.g., introducing both straightforward and complex play scenarios to challenge play repertoire), as well as dosage (e.g., number of trials), should be considered (Frick et al., 2023).
Variation in Participant Characteristics
In the pilot data, child ages ranged from 18 to 35 months and children were on a waitlist for an autism diagnosis. Additionally, pilot families were (a) under-served (i.e., their child received minimal therapeutic and educational support), (b) lived in rural communities, or (c) under-resourced (see Kunze et al., 2021 for descriptions). In contrast, the children in this study varied in age, ranging from 26 to 50 months, and were more broadly described as having various developmental delays. Families were not limited to under-served, rural, or under-resourced. A consistent inclusion criterion across the two studies was that parents were not receiving other parent training at the time of the study. The current dyads had high levels of parent education (bachelor’s degree or above), more therapeutic and educational support for their child, and lived in urban and rural locations. Despite broadening the inclusion criteria, parent outcomes were similar in both studies, yet the child data differed. Future research should consider grouping participants to analyze more homogeneous groups. While the type and dosage of outside therapy were not tracked beyond intake, it is recommended that it be done in future studies. Such considerations may benefit in understanding complementary interventions and identifying barriers that may prevent behavior change.
Intervention Individualization
Data suggests that the intervention strategies taught to the parents supported engagement in dyad interaction (e.g., child behavior remained high for engagement). However, the intensity of the intervention strategies did not graduate in complexity specific to the child’s performance. For instance, the coaching during sessions 1–5 of the PRRFCT Match intervention was identical for each dyad. This was necessary to teach the parent participants strategies for engaging with their child during play (see baseline performance in Fig. 3). However, children with higher levels of engagement at baseline may have benefitted from a more individualized package for sessions 5–10 and beyond. Because the focus of the intervention package was dyad responsivity as measured through the child’s engagement (or lack of engagement) with the parent, it is important to note that the children with insignificant outcomes were high engagers despite their parent’s interactions with them. There are several possibilities for this. Confounding variables (e.g., amount of other therapeutic services, length of school day, learning histories) may have already solidified a competent play skill set in the child’s repertoire. Child age, differing diagnosis, and level of adaptive skills (see Table 4) are also likely contributors to the high performance at baseline. For example, three child participants with high baseline engagement and insignificant behavior change (i.e., 5, 6, and 8) were among the oldest children in the sample. Considering that some child participants may have benefitted from a more complex play scenario or be challenged with less skilled play partners (i.e., sibling or peer) lays the foundation for an intervention package with multiple pathways: one focusing on early learners and another for those considered to be a savvier play partner.
Play materials and activity choices should also be considered. While the pilot study participants were provided with a set of toys, participants in the current study were encouraged to use toys already in their homes. As such, the choice of toys, activity difficulty, and behavioral definitions (i.e., engaged versus unengaged) should be revised to match the level of the learner and the context of the play activity. For example, child 8, whose engagement was high in both baseline and intervention, may benefit from pretend play rather than object play, allowing for open-ended exchanges and the development of executive functions (White et al., 2021). Early learners, who in this study made slow progress (i.e., participants 2 and 4), may benefit from turn-taking (e.g., ball rolling) and concrete toy use (e.g., shape sorter) to practice additional opportunities for engagement with their parent (Campbell et al., 2016). Future research should consider additional analysis of the child’s present level of performance during play with parents and peers.
Coach Skill Set
The coach training in the current study comprised teaching each coach the intervention strategies (modeling, prompting, time delay, etc.) and how to interact with parents during each virtual session. A variation between coaching in the pilot study and this replication was the skill set of the coaches. All pilot coaching was done by a PhD, BCBA-D with over 25 years in the field of early intervention. However, in the current study, the coaches were novice graduate student clinicians with little experience working with parents or early intervention. While further investigation into coaching behavior is necessary, it is possible that additional training may have prepared coaches to support the parent in pivoting from early to advanced learner behaviors during sessions more easily through reflection and feedback. This is a similar finding in a study on coaching practices by Meadan et al. (2018), where reflection and feedback were found to be lacking in coaches’ implementation of intervention sessions despite the research consensus of its importance. PRRFCT Match coaches completed fidelity checklists stating that reflection and feedback occurred in each session; however, the investigation into the individualization of these components per participating family warrants further exploration. Such analysis should consider each child’s response to intervention, coach behavior during feedback and reflection, and parent implementation of strategies and play responsivity.
Limitations
Several limitations to this study should be considered for future research and next steps. First, the coach’s behavior fidelity was measured with a coaching checklist and video checks. Further analysis of individualized coaching should be considered to understand better-nuanced coach behaviors in support of or as barriers to child and parent progress. Such coach behaviors can be operationally defined and measured with more detailed fidelity checklists (see Meadan et al., 2023). Second, while the participating families were racially and geographically diverse, the socioeconomic and educational levels were high. This creates a concern in generalization across the overall US population. Additionally, diversity for child and parent participants should be considered for future studies. Specifically, considering variations in primary language, cultural variations, and gender of both child and parents could be addressed with a larger sample size. Third, the researchers did not control for other therapeutic influences that may impact a child’s performance. Thus, receiving therapeutic services (e.g., behavior therapy and educational programming) was not an exclusionary factor. While this was a purposeful decision, as stopping therapeutic support to participate in research is disruptive to families, external influences likely impacted child outcomes and were not controlled for. However, participating parents were asked not to seek out or receive parent education beyond PRRFCT Match during their time of participation in the study. Fourth, while parent practice and logs were recommended, it is unknown if and to what extent parents did practice, as no parent logs were returned to the coaches. Replications should measure parent practice as it is likely that practice outside of the intervention sessions would influence outcomes. Finally, conclusions from non-significant findings are cautioned. While pre- and post-measures may provide interesting participant information, using the outcomes to describe relationships between the intervention and participant performance is unfounded.
Conclusion
High-quality community-delivered EI positively impacts children’s developmental trajectory (Nahmias et al., 2019). PRRFCT Match expands the current evidence base of interventions for young children with DD and their caregivers. Outcomes revealed that the PRRFCT Match training protocol successfully trained novice coaches to deliver an intervention package effectively, responding to the limited usability of other more complex training protocols. Additionally, PRRFCT Match was prepared, delivered, and analyzed explicitly using virtual means, broadening coach training and delivery opportunities despite geographic location. The flexibility of training, delivery, and usability of the PRRFCT Match intervention package suggests practical applicability to a diverse pool of children, families, and professionals. Future studies will focus on under-served EI systems and families, which may be most impactful in practice, as these populations are often overlooked in research.
References
Barnett, M. L., Niec, L. N., Peer, S. O., Jent, J. F., Weinstein, A., Gisbert, P., & Simpson, S. (2017). Successful therapist–parent coaching: How in vivo feedback relates to parent engagement in parent–child interaction therapy. Journal of Clinical Child & Adolescent Psychology, 46(6), 895–902. https://doi.org/10.1080/15374416.2015.1063428
Beaudoin, A. J., Sébire, G., & Couture, M. (2014). Parent training interventions for toddlers with autism spectrum disorder. Autism Research and Treatment, 2014, 1–15. https://doi.org/10.1155/2014/839890
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
Bruder, M. B., Gundler, D., Stayton, V., & Kemp, P. (2021). The early Childhood Personnel Center: Building capacity to improve outcomes for infants and young children with disabilities and their families. Infants & Young Children, 34(2), 69–82. https://doi.org/10.1097/IYC.0000000000000191
Campbell, S. B., Leezenbaum, N. B., Mahoney, A. S., Moore, E. L., & Brownell, C. A. (2016). Pretend play and social engagement in toddlers at high and low genetic risk for autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(7), 2305–2316. https://doi.org/10.1007/s10803-016-2764-y
Cividini-Motta, C., & Ahearn, W. H. (2013). Effects of two variations of differential reinforcement on prompt dependency. Journal of Applied Behavior Analysis, 46(3), 640–650. https://doi.org/10.1002/jaba.67
Coleman, P. K., & Hildebrandt Karraker, K. (2003). Maternal self-efficacy beliefs, competence in parenting, and toddlers’ behavior and developmental status. Infant Mental Health Journal, 24(2), 126–148. https://doi.org/10.1002/imhj.10048
Crnic, K. A., Neece, C. L., McIntyre, L. L., Blacher, J., & Baker, B. L. (2017). Intellectual disability and developmental risk: Promoting intervention to improve child and family well-being. Child Development, 88(2), 436–445. https://doi.org/10.1111/cdev.12740
Davis, C. A., & Fox, J. (1999). Evaluating environmental arrangement as setting events: Review and implications for measurement. Journal of Behavioral Education, 9(2), 77–96. https://doi.org/10.1023/A:1022884816219
Delaigue, S., Morand, J. J., Olson, D., Wootton, R., & Bonnardot, L. (2014). Teledermatology in low-resource settings: The MSF experience with a multilingual tele-expertise platform. Front Public Health, 2, 233. https://doi.org/10.3389/fpubh.2014.00233
Division for Early Childhood (2014). DEC recommended practices in early intervention/early childhood special education. http://www.dec-sped.org/recommendedpractices
Dracobly, J. D., Dozier, C. L., Briggs, A. M., & Juanico, J. F. (2017). An analysis of procedures that affect response variability. Journal of Applied Behavior Analysis, 50(3), 600–621. https://doi.org/10.1002/jaba.392
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X. H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism, 13(4), 375–387. https://doi.org/10.1177/1362361309105658
Estes, A., Swain, D. M., & MacDuffie, K. E. (2019). The effects of early autism intervention on parents and family adaptive functioning. Pediatric Medicine, 2. https://doi.org/10.21037/pm.2019.05.05
Francis, R., Winchester, C., Barton, E. E., Ledford, J. R., & Velez, M. (2020). Using progressive time delay to increase levels of peer imitation during play with preschoolers with disabilities. American Journal on Intellectual and Developmental Disabilities, 125(3), 186–199. https://doi.org/10.1352/1944-7558-125.3.186
Frey, J. R., & Kaiser, A. P. (2011). The use of play expansions to increase the diversity and complexity of object play in young children with disabilities. Topics in Early Childhood Special Education, 31(2), 99–111. https://doi.org/10.1177/0271121410378758
Frick, T. A., Schnitz, A. G., Cosand, K., Horn, E. M., & Zimmerman, K. N. (2023). Dosage reporting in early intervention literature: A systematic review. Topics in Early Childhood Special Education, 43(1), 5–16. https://doi.org/10.1177/02711214231159603
Gast, D. L., Lloyd, B. P., & Ledford, J. (2014). Multiple baseline and multiple probe designs. In D. L. Gast, & J. R. Ledford (Eds.), Single Case Research Methodology Applications in Special Education and behavioral sciences (2nd ed., pp. 252–296). Routledge.
Griffith, S. F., Magariño, L. S., Martínez Pedraza, F. D., Frazier, S. L., Berkovits, M. D., & Bagner, D. M. (2023). Surveying early intervention providers to identify opportunities for workforce support to strengthen family-centered care. Infants & Young Children, 36(4), 314–332. https://doi.org/10.1097/IYC.0000000000000247
Guralnick, M. J. (1997). Effectiveness of early intervention for vulnerable children: A developmental perspective. American Journal on Mental Retardation, 102(4), 319–345. https://doi.org/10.1352/0895-8017(1998)102<0319:EOEIFV>2.0.CO;2
Individuals with Disabilities Education Improvement Act of 2004 (2004). P.L. 108–446, 20 U.S.C. $ 1400 et seqhttps://www.copyright.gov/legislation/pl108-446.pdf
Ingersoll, B. R., Wainer, A. L., Berger, N. I., & Walton, K. M. (2017). Efficacy of low intensity, therapist-implemented project ImPACT for increasing social communication skills in young children with ASD. Developmental Neurorehabilitation, 20(8), 502–510. https://doi.org/10.1080/17518423.2016.1278054
Ingersoll, B., Douglas, S. N., Brodhead, M. T., Barber, A., & Kaczmarek, L. A. (2023). Interdisciplinary competencies for implementing NDBIs with young children with autism and other social communication challenges. Journal of Early Intervention, 1–17. https://doi.org/10.1177/105381512312189
Isler, M. R., & Corbie-Smith, G. (2012). Practical steps to community engaged research: From inputs to outcomes. The Journal of Law Medicine & Ethics, 40(4), 904–914.
Kasari, C., Gulsrud, A., Wong, C., Kwon, S., & Locke, J. (2010). Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders, 40, 1045–1056.
Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2013). Single-case intervention research design standards. Remedial and Special Education, 34(1), 26–38. https://doi.org/10.1177/0741932512452794
Kunze, M. G., Machalicek, W., Wei, Q., & St Joseph, S. (2021). Coaching via telehealth: Caregiver-mediated interventions for young children on the waitlist for an autism diagnosis using single-case design. Journal of Clinical Medicine, 10(8), 1654. https://doi.org/10.3390/jcm10081654
Kunze, M., Gomez, D., Glenn, E., Todis, B., Riddle, I., Karns, K., Glang, A., & McIntyre, L. L. (2023). Parenting young children with developmental disabilities: Exploring mothers’ experiences during the COVID-19 pandemic. Journal of Childhood Education & Society, 4(2), 156–175. https://doi.org/10.37291/2717638X.202342264
Lecavalier, L., Bodfish, J., Harrop, C., Whitten, A., Jones, D., Pritchett, J., Faldowski, R., & Boyd, B. (2020). Development of the behavioral inflexibility scale for children with autism spectrum disorder and other developmental disabilities. Autism Research, 13(3), 489–499. https://doi.org/10.1002/aur.2257
Ledford, J. R., & Zimmerman, K. N. (2023). Rethinking Rigor in multiple baseline and multiple probe designs. Remedial and Special Education, 44(2), 154–167. https://doi.org/10.1177/07419325221102539
Lindgren, S., Wacker, D., Schieltz, K., Suess, A., Pelzel, K., Kopelman, T., Lee, J., Romani, P., & O’Brien, M. (2020). A randomized controlled trial of functional communication training via telehealth for young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(12), 4449–4462. https://doi.org/10.1007/s10803-020-04451-1
Lorio, C. M., Romano, M., Woods, J. J., & Brown, J. (2020). A review of problem solving and reflection as caregiver coaching strategies in early intervention. Infants & Young Children, 33(1), 35–70. https://doi.org/10.1097/iyc.0000000000000156
McIntyre, L. L., & Kunze, M. (2021). Family-focused interventions as prevention and early intervention of behavioral problems in children with autism spectrum disorder. In International Review of Research in Developmental Disabilities (Vol. 61, pp. 159–191). https://doi.org/10.1016/bs.irrdd.2021.07.007
Meadan, H., Snodgrass, M. R., Meyer, L. E., Fisher, K. W., Chung, M. Y., & Halle, J. W. (2016). Internet-based parent-implemented intervention for young children with autism: A pilot study. Journal of Early Intervention, 38(1), 3–23. https://doi.org/10.1177/1053815116630327
Meadan, H., Douglas, S. N., Kammes, R., & Schraml-Block, K. (2018). I’m a different coach with every family: Early interventionists’ beliefs and practices. Infants & Young Children, 31(3), 200–214. https://doi.org/10.1097/IYC.0000000000000118
Meadan, H., Lee, J. D., Sands, M. M., Chung, M. Y., & Garcia-Grau, P. (2023). The coaching fidelity scale; development and evaluation of an observational measure of coaching fidelity. Infants & Young Children, 36(1), 37–52. https://doi.org/10.1097/IYC.0000000000000231
Nahmias, A. S., Pellecchia, M., Stahmer, A. C., & Mandell, D. S. (2019). Effectiveness of community-based early intervention for children with autism spectrum disorder: A meta‐analysis. Journal of Child Psychology and Psychiatry, 60(11), 1200–1209. https://doi.org/10.1111/jcpp.13073
Newman, M. G. (2004). Technology in psychotherapy: An introduction. 60(2), 141–145. https://doi.org/10.1002/jclp.10240
Nicholl, H., Tracey, C., Begley, T., King, C., & Lynch, A. M. (2017). Internet use by parents of children with rare conditions: Findings from a study on parents’ web information needs. Journal of Medical Internet Research, 19(2), e51. https://doi.org/10.2196/jmir.5834
Odom, S. L., & Wolery, M. (2003). A unified theory of practice in early intervention/early childhood special education: Evidence-based practices. Journal of Special Education, 37(3), 164–173. https://doi.org/10.1177/00224669030370030601
Oono, I. P., Honey, E. J., & McConachie, H. (2013). Parent-mediated early intervention for young children with autism spectrum disorders (ASD). Evidence-Based Child Health: A Cochrane Review Journal, 8(6), 2380–2479. https://doi.org/10.1002/ebch.1952
Parker, R. J., Vannest, K. J., & Davis, J. L. (2011). Effect size in single-case research: S review of nine nonoverlap techniques. Behavior Modification, 35(4), 303–322.
Pellecchia, M., Mandell, D. S., Beidas, R. S., Dunst, C. J., Tomczuk, L., Newman, J., Zeigler, L., & Stahmer, A. C. (2023). Parent coaching in early intervention for autism spectrum disorder: A brief report. Journal of Early Intervention, 45(2), 185–197. https://doi.org/10.1177/10538151221095860
Pustejovsky, J. E., & Swan, D. M. (2018). Single-case effect size calculator (Version 0.5) Web application. https://jepusto.shinyapps.io/SCD-effect-sizes/
Pustejovsky, J., Chen, M., & Hamilton, B. (2020). SCDHLM: A web-based calculator for between-case standardized mean differences (0.5. 2) [Web application].
Quigley, J., Griffith, A. K., & Kates-McElrath, K. (2018). A comparison of modeling, prompting, and a multi-component intervention for teaching play skills to children with developmental disabilities. Behavior Analysis in Practice, 11(4), 315–326. https://doi.org/10.1007/s40617-018-0225-0
Reimers, T. M., Wacker, D. P., Cooper, L. J., & De Raad, A. (1992). Acceptability of behavioral treatments for children: Analog and naturalistic evaluations by parents. School Psychology Review, 21(4), 628–643. https://doi.org/10.1080/02796015.1992.12087371
Rodriguez, K. A. (2020). Maintaining treatment integrity in the face of crisis: A treatment selection model for transitioning direct ABA services to telehealth. Behavior Analysis in Practice, 13(2), 291–298. https://doi.org/10.1007/s40617-020-00429-8
Rush, D. D., & Shelden, M. L. L. (2011). The early childhood coaching handbook. Brookes Publishing Company.
Ruskin, P. E., Silver-Aylaian, M., Kling, M. A., Reed, S. A., Bradham, D. D., Hebel, J. R., Barrett, D., Knowles, F. 3rd, & Hauser, P. (2004). Treatment outcomes in depression: Comparison of remote treatment through telepsychiatry to in-person treatment. American Journal of Psychiatry, 161(8), 1471–1476. https://doi.org/10.1176/appi.ajp.161.8.1471
Sam, A., & AFIRM Team. (2015). Prompting. National Professional Development Center on Autism Spectrum Disorder, FPG Child Development Center, University of North Carolina. https://afirm.fpg.unc.edu/prompting
Sam, A., & AFIRM Team. (2016). Modeling. National Professional Development Center on Autism Spectrum Disorder, FPG Child Development Center, University of North Carolina. https://afirm.fpg.unc.edu/modeling
Savage, M. N., & AFIRM Team. (2017). &. Differential Reinforcement. National Professional Development Center on Autism Spectrum Disorder, FPG Child Development Center, University of North Carolina. http://afirm.fpg.unc.edu/differential-reinforcement
Schwartzman, J. M., Millan, M. E., & Gengoux, G. W. (2022). Predictors of self-reported resilience in parents of autistic children. Research in Autism Spectrum Disorders, 94, 101954. https://doi.org/10.1016/j.rasd.2022.101954
Silbaugh, B. C., Murray, C., Kelly, M. P., & Healy, O. (2021). A systematic synthesis of lag schedule research in individuals with autism and other populations. Review Journal of Autism and Developmental Disorders, 8(1), 92–107. https://doi.org/10.1007/s40489-020-00202-1
Simacek, J., Dimian, A. F., & McComas, J. J. (2017). Communication intervention for young children with severe neurodevelopmental disabilities via telehealth. Journal of Autism and Developmental Disorders, 47(3), 744–767. https://doi.org/10.1007/s10803-016-3006-z
Sparrow, S. S., Aaulnier, C. A., Cicchetti, D. V., & Doll, E. A. (2016). Vineland III: Vineland adaptive behavior scales, Manual (3rd ed.). Pearson Assessments.
Steinbrenner, J. R., Hume, K., Odom, S. L., Morin, K. L., Nowell, S. W., Tomaszewski, B., Szendrey, S., McIntyre, N. S., Yücesoy-Özkan, S., & Savage, M. N. (2020). Evidence-based practices for children, youth, and young adults with autism. The University of North Carolina at Chapel Hill, Frank Porter Graham Child Development Institute, National Clearinghouse on Autism Evidence and Practice Review Team. https://files.eric.ed.gov/fulltext/ED609029.pdf
Tate, D. F., & Zabinski, M. F. (2004). Computer and internet applications for psychological treatment: Update for clinicians. Journal of Clinical Psychology, 60(2), 209–220. https://doi.org/10.1002/jclp.10247
Titus Dieringer, S., Zoder-Martell, K., Porretta, D. L., Bricker, A., & Kabazie, J. (2017). Increasing physical activity in children with autism through music, prompting, and modeling. Psychology in the Schools, 54(4), 421–432. https://doi.org/10.1002/pits.22003
Tomaszewski, B., Regan, T., & AFIRM Team. (2017). &. Response interruption and redirection. National Professional Development Center on Autism Spectrum Disorder, FPG Child Development Center, University of North Carolina. https://afirm.fpg.unc.edu/response-interruption-and-redirection
Tucker, M., Sigafoos, J., & Bushell, H. (1998). Use of noncontingent reinforcement in the treatment of challenging behavior: A review and clinical guide. Behavior Modification, 22(4), 529–547.
White, R. E., Thibodeau-Nielsen, R. B., Palermo, F., & Mikulski, A. M. (2021). Engagement in social pretend play predicts preschoolers’ executive function gains across the school year. Early Childhood Research Quarterly, 56, 103–113. https://doi.org/10.1016/j.ecresq.2021.03.005
Wolff, J. J., Boyd, B. A., & Elison, J. T. (2016). A quantitative measure of restricted and repetitive behaviors for early childhood. Journal of Neurodevelopmental Disorders, 8(1), 27. https://doi.org/10.1186/s11689-016-9161-x
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. Journal of Autism and Developmental Disorders, 45(7), 1951–1966. https://doi.org/10.1007/s10803-014-2351-z
Zimmerman, K. N., Ledford, J. R., & Barton, E. E. (2017). Using visual activity schedules for young children with challenging behavior. Journal of Early Intervention, 39(4), 339–358. https://doi.org/10.1177/1053815117725693
Funding
The contents of this study and manuscript were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90SFGE0033). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this presentation do not necessarily represent the policy of NIDILRR, ACL, or HHS, and you should not assume endorsement by the Federal Government.
Author information
Authors and Affiliations
Contributions
Conceptualization- Megan Kunze; Methodology-Megan Kunze; Formal Analysis and Investigation-Megan Kunze and Qi Wei; Writing-all authors; Writing review and editing- Megan Kunze, Qi Wei, Alexis Bacon-Yates, Emily Pompan, Hannah Lockwood; Funding acquisition-Megan Kunze; Resources- Megan Kunze, Qi Wei, Emily Pompan; Supervision- Megan Kunze.
Corresponding author
Ethics declarations
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the University of Oregon.
Competing Interests
Authors have no financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kunze, M., Wei, Q., Bacon-Yates, A. et al. Promoting Reciprocal Relationships with Flexibility, Coaching, and Teaching (PRRFCT Match): A Virtual Parent-Mediated Intervention Package for Young Children with Developmental Disabilities. J Autism Dev Disord (2024). https://doi.org/10.1007/s10803-024-06386-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s10803-024-06386-3