
Abstract
The objective of this study was to identify subgroups of toddlers with DSM-5 ASD based on core ASD symptoms using a person-based analytical framework. This is a retrospective study of 500 toddlers (mean age 26 months, 79% male) with DSM-5 ASD. Data were analyzed using latent class analyses in which profiles were formed based on ASD symptomatology. Social communication (SC) symptoms favored a three-class solution, while restricted/repetitive behaviors (RRBs) favored a two-class solution. Classes with higher consistency of SC deficits were younger, with lower developmental functioning. The class with more RRBs was older, with higher functioning. If confirmed in other populations, these classes may more precisely characterize subgroups within the heterogeneous group of toddlers at time of ASD diagnosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder marked by deficits in social communication and the presence of restricted and repetitive behaviors (American Psychiatric Association 2013). Children with ASD are phenotypically heterogeneous at the time of diagnosis, and this is particularly true in toddlers (Chawarska et al. 2009; Estes et al. 2015; Guthrie et al. 2013; Kim et al. 2016; Munson et al. 2008; Stevens et al. 2000; Zwaigenbaum et al. 2013). While, by definition, all toddlers with ASD must exhibit impairments in social communication and demonstrate restricted and repetitive behaviors, the severity with which these core ASD symptoms manifest is variable (Georgiades et al. 2013; Wiggins et al. 2012). Toddlers with ASD display a range of cognitive, language, and adaptive functioning strengths or challenges. Furthermore, children with ASD demonstrate heterogeneous developmental trajectories. While some studies suggest that level of functioning in certain domains at diagnosis might predict a child’s trajectory or rate of improvement over time, correlations between presenting characteristics and trajectories or outcomes have not been consistently demonstrated across studies. (Anderson et al. 2014; Fountain et al. 2012; Kim et al. 2018; Catherine Lord et al. 2012a, b; Moulton et al. 2016; Szatmari et al. 2015). Thus far, it has not been determined whether there are subgroups of children within the broader autism spectrum that can be identified at time of diagnosis, and whether subgroup membership may allow clinicians to tailor treatments more precisely, inform families regarding potential developmental trajectory, and predict outcomes. Recent studies suggest diagnostic stability as early as 14 months of age (Pierce et al. 2019). Thus, there is an even greater imperative to better understand the ways in which ASD presents in this very young age group.
Previous attempts to identify subgroups of young children with ASD have typically combined cognitive, language, and adaptive functioning along with core ASD symptoms (Ben-Itzchak et al. 2014; Bitsika et al. 2008; Chawarska et al. 2009; Estes et al. 2015; Harris and Handleman 2000; Kim et al. 2016, 2018; Moulton et al. 2016). This approach is in part due to the difficulty in quantifying core ASD symptom severity, particularly in young children, as seen in the study by Kim et al. (2018). This study identified four “trajectory clusters” of core ASD symptoms and found that the symptom trajectory of given item-level behaviors from the Autism Diagnostic Observation Schedule (ADOS), such as “unusual eye contact” or “response to name,” did not always align with the trajectory of the overall severity score using the ADOS Calibrated Severity Score (CSS) (Kim et al. 2018). Additionally, the CSS for social affect (SA) had a different trajectory than that of the CSS for restricted/repetitive behaviors (RRB), with the CSS-SA improving while the CSS-RRB remained relatively stable. This suggests that global scores that include both SA and RRB symptom domains together may not capture individual symptom trajectories over time, and that the two domains themselves (SA and RRB) may not follow the same trajectory (Kim et al. 2018). Other domains of functioning were not closely correlated with core symptoms, as language improved for many children across clusters while CSS scores either improved, remained stable, or even worsened (Kim et al. 2018). Finally, “trajectory clusters” that remained stable, worsened, or improved all had a relatively similar proportion of children receiving high intensity intervention. The authors commented on the intra-individual variability in item-level core symptoms even within the clusters, observations that call for further research into the heterogeneity of core symptom severity within ASD (Kim et al. 2018). Szatmari and colleagues also described divergence in developmental trajectories of autism core symptom severity and adaptive functioning in a cohort of young children (Szatmari et al. 2015).
Most published literature on toddlers with ASD has focused on a broader definition of autism, as was defined in the previous Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). With the shift to the new fifth edition of the DSM (DSM-5), diagnostic criteria for ASD were condensed from three domains into two (social communication and restricted and repetitive behaviors) with children needing to meet a higher number of symptom criteria for diagnosis (American Psychiatric Association 2000, 2013). Studies that have compared children who met DSM-IV but not DSM-5 criteria have reported that those children who did not meet criteria for a DSM-5 diagnosis had higher adaptive or cognitive skills and less severe core symptoms, or were diagnosed with pervasive developmental disorder, not otherwise specified via DSM-IV (Gibbs et al. 2012; Jashar et al. 2016). Prior work has also suggested that the change in criteria could disproportionately impact toddlers, who may be less likely to meet the more stringent DSM-5 criteria compared to older children (Barton et al. 2013; Gibbs et al. 2012; Harstad et al. 2015). For example, certain “higher order” behaviors such as cognitive rigidity may not emerge until later ages (Wiggins 2012).
Given the recent diagnostic criteria changes and the increasingly younger age at which ASD is diagnosed, there is a need to more fully understand the heterogeneity of DSM-5 ASD core symptoms at time of diagnosis, particularly among toddlers. Identification of subgroups based on core ASD symptoms will also inform future work assessing stability of diagnosis, developmental trajectories and functional outcomes, with the ultimate goal of predicting trajectory and outcomes based on characteristics that can be observed at the time of a clinical diagnosis. Thus, our objectives are (1) to describe the presenting developmental profiles (a term encompassing cognitive, language, and adaptive functioning) and core ASD symptoms of toddlers diagnosed with ASD via DSM-5 criteria; (2) to use latent class analyses (LCA) to determine if phenotypic subgroups of core ASD symptoms can be identified at diagnosis; and (3) to evaluate whether cognitive, language, motor, and adaptive functioning levels vary across latent classes based on core ASD symptom subgroups.
Method
Study Setting and Participants
We conducted a retrospective chart review of 500 toddlers, ages 18 to 36 months, with a diagnosis of ASD made at a single, tertiary academic medical center that provides diagnostic services for children with neurodevelopmental disorders, including ASD. Children are referred to this center by their primary care pediatrician, early childhood intervention provider, or parent based on concern for delayed or atypical development. All new referrals are automatically triaged to an interdisciplinary team assessment unless previous psychological testing has been completed, in which case a single specialty consultation with a Developmental-Behavioral Pediatrician (DBP) is scheduled. In the team assessments, a DBP obtains a medical and developmental history from the parent in a semi-structured format consisting of a standardized written intake form prior to the visit and an interview on the day of the assessment that is uniform in its core components across providers. The DBP clinician also conducts a complete physical exam. A clinical child psychologist assesses developmental functioning through standardized cognitive, language, and adaptive measures, and administers the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) to assess for symptoms of ASD (Lord et al. 2012a, b). The majority of the sample received the Toddler Module (Toddler N = 387, 77.4%; Module 1 N = 69, 13.8%; Module 2 N = 6, 1.2%; or module not documented in the record N = 38, 7.6%). The Bayley Scales of Infant and Toddler Development, Third Edition was used to assess cognitive, language, and motor function (Bayley 2006). The Vineland Adaptive Behavior Scales, Second or Third Editions were used to assess adaptive function (Sparrow and Cicchetti 2005; Sparrow and Cichetti 2016). All components of both the DBP and psychologist portions of the assessment are compiled and documented together in the medical record in a uniform format that is utilized by all clinicians within the center. Records from July 1, 2013 until May 1, 2016 were reviewed as these dates corresponded with a clinic-wide implementation of a checklist to ensure ASD diagnoses were being made with fidelity to the new DSM-5 criteria (Harstad et al. 2015). Only 5 children were excluded from this study because they were seen by a single clinician rather than a team assessment. We identified participants via an electronic medical record search based on a billing code that signified a team consultation visit (99245 AND 96118 or 96119) and an ICD-9 or 10 code for a new diagnosis of ASD (F84.0, F84.9, or F84.5 or 299.0, 299.8, or 299.9). Participants were only included if they had a documented DSM-5 diagnosis of ASD made during the team assessment. The study was approved by the Boston Children’s Hospital Institutional Review Board with a waiver of informed consent.
Data Collection Procedures
We created a data abstraction form and revised it through subsequent data abstraction trials. We abstracted demographic characteristics available from the medical record, including sex, race, ethnicity, primary language, maternal level of education, and participant address. Variables that are typically combined into a composite measure to best estimate socioeconomic status (SES), such as maternal level of education, were not uniformly documented in the records and therefore could not be abstracted for all participants. Thus, we estimated household income via Census data based on participant’s zip code. We abstracted cognitive, language, motor, and adaptive standard scores (SS) from the Bayley and/or Vineland Scales.
In order to precisely abstract information about core ASD symptoms, we created a data dictionary of descriptions of core ASD symptoms based upon prior studies utilizing this clinical language approach and analogous to the coding used by the Centers for Disease Control in the ongoing ASD symptoms monitoring program (Barbaresi et al. 2005). The goal of the CDC coding is to determine whether or not a child has symptoms sufficient to meet diagnostic criteria for ASD. In contrast, among our subjects with a DSM-5 diagnosis of ASD, our objective was to assess for phenotypic subgroups based on core ASD symptoms. The data abstraction protocol included selected behaviors and symptoms that mapped directly to the DSM-5 criteria. In addition, we included behaviors that are elicited by tasks on the ADOS, which is routinely administered to individuals seen in the team assessments.
With regard to ASD core symptoms, our clinicians provide narrative descriptions of the ADOS within the clinical document but do not provide numeric scores. We were unable to retrieve specific score documentation from the original protocols. We used a systematic approach to abstract ASD symptoms from the medical record with the following steps: first the standardized ADOS-2 assessment from the psychological test results documented in the medical record, second from data documented by the physician or psychologist in the behavioral observations section of the clinical note, and finally from the physician-documented parent history section of the clinical note. Documentation of core ASD symptom behaviors were most often available in the ADOS account within the record; therefore, this served as the richest source of information regarding core ASD symptoms. When unavailable in the ADOS account, data abstraction progressed to other portions of the clinical document as noted above.
Documentation regarding consistency/frequency of social communication behaviors was available for all participants. Social communication behaviors were coded as consistent (participant used the social communication behavior regularly, did not meet ASD criteria), inconsistent (the participant used the behavior but not at the frequency expected, met ASD criteria), or absent (the participant did not demonstrate the social communication behavior during the observation, met ASD criteria). For analytic purposes, each social communication behavior was treated as a categorical variable for which possible choices were: absent (coded as 2); inconsistent (coded as 1); consistent (coded as 0); or not mentioned. For RRBs, documentation in the medical record was also available for all participants. Unlike social communication behaviors, information describing the frequency and consistency with which RRBs occurred was not available in the medical record; thus, each RRB was abstracted and coded as a dichotomous variable for which the possible codes were: present, met ASD criteria (coded as 1); absent/not mentioned, did not meet ASD criteria (coded as 0). Thus, for both core ASD symptom domains, scores greater than 0 indicated that the participant manifested a behavior consistent with the diagnostic criteria for ASD.
We double coded data abstraction for the first 20 participants and utilized discrepancies to further define variables and revise the data abstraction form. These pilot efforts led to the creation of an abstractor’s dictionary that clarified variable definitions. Two reviewers (H.H.; C.L.) recorded data in the RedCap tool for online data collection (Harris et al. 2009). We double coded 10% of the cases, and all of the double coded cases achieved > 96% inter-rater reliability. A third reviewer (E.H.) arbitrated discrepancies in coding.
Statistical Analyses
To describe the sample, we used frequencies and percentages to present demographics and the presence of core ASD symptom behaviors. We used mean standard scores from the Bayley and/or Vineland with standard deviations to present the developmental profiles (cognitive, language, motor and adaptive functioning).
We conducted latent class analyses (LCA) to evaluate for the presence of latent subgroups that describe core ASD symptoms. An attempt was made to conduct an LCA using all core ASD symptom behaviors as indicators in a single model to determine if subgroups emerged based on core symptom severity. This resulted in a model without optimal fit (see results below), suggesting that core symptoms represent distinct latent variables. Thus, separate LCAs were conducted within each core symptom domain (i.e., social communication and RRBs). For each LCA, we estimated a series of models with an increasing number of potential classes. We evaluated model preference using several inferential and information criteria but relied more heavily on: (a) the Bayesian Information Criterion (BIC), (b) the cmPK, and, (c) the Lo-Mendell-Rubin likelihood ratio (LR) test. (Bozdogan 1987; Masyn 2013; Nylund et al. 2007).
To compare cognitive, language, motor, and adaptive functioning across the classes we used a one-way analysis of variance (ANOVA), using the Tukey honestly significant difference post hoc procedure. We further adjusted for the presence of multiple comparisons using the Bonferroni correction. We conducted a power analysis and determined that 160 participants would suffice to properly define and differentiate at least 3 distinct classes of individuals with 6 predictors each. Thus, 500 participants yielded ample power for this study.
Results
Demographics
The average age of participants was 26.0 months (SD: 5.3 months) and 79.2% (N = 396) were male. 13% were premature (less than 37 weeks gestational age) and 58.4% were privately insured. The majority of participants (47.2%) had an estimated median household income classified in the upper class based on regional data, with the next largest percentage (35.8%) in the moderate class. Table 1 represents baseline characteristics of the cohort.
Developmental Profiles
14 participants were not administered the Bayley Scales as a cognitive and language measure (13 were administered the Differential Ability Scales-II and 1 was administered the Mullen Scales of Early Learning). 12 participants did not have results from the Vineland, but rather the Adaptive Behavior Assessment System, Third Edition. Participants who did not have results from the Bayley Scales and/or the Vineland were excluded from the relevant analyses. The included sample had low average cognitive (mean SS = 80.6) and motor functioning (mean SS = 78.9), with language functioning being below average (mean SS = 63.1) on the Bayley Scales (Table 2). The adaptive behavior composite score on the Vineland Adaptive Behavior Scales was in the moderately low range (mean SS = 74.8; Table 2).
All participants had core ASD symptom data available. In our sample, the most frequently observed social communication deficits included lack of symbolic play (68.4%), lack of a distal point (59.4%), and lack of ability to follow a gaze (58.6%). While some of these behaviors (e.g., lack of a distal point) are often highlighted as red flags for ASD, others are less commonly highlighted or included during screening, perhaps due to the difficulty in identifying those skills (e.g., lack of symbolic play). Participants were more likely to be able to demonstrate some degree of eye contact (only 3.6% were documented to have a total lack of eye contact), although eye contact was most commonly termed “inconsistent.” Among RRB criteria, motor stereotypies (84.0%) and repetitive object use (84.0%) were the most commonly documented behaviors. Sensory seeking behaviors (72.4%) and atypical visual regard (71.8%) were also noted in the majority of participants. Frequencies at which core ASD symptoms were reported are presented in Tables 3 and 4.
Phenotypic Subgroups Based on Latent Class Analyses of Core ASD Symptom Severity
An LCA incorporating all core ASD symptoms, including both social communication behaviors and RRBs was attempted. Among 5 competing models, the class enumeration process resulted in a 3-class model; however, this model accommodated the social criteria well, but forced the behavioral criteria into three groups that clearly showed misfit, as a 2-class solution was most descriptive for them. This misfit was evident using a test of differences in loglikelihood contrasting the 3-class solution describing social communication with the combined model [χ2(61) = 4644.6, p < 0.001] but also the 2-class RRB solution against the combined model [χ2(96) = 6892.3, p < 0.001]. Thus, the decision was made to conduct separate analyses for each core ASD symptom domain.
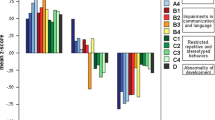
In the LCA of social communication symptoms, 5 different classes were considered and a 3-class model provided optimal model fit as the BIC had its smallest value (i.e. 8868.8) and the cmPK pointed to the preference of the 3-class model (Table 5). By use of the loglikelihood and the Vuong-Lo-Mendell-Rubin test, the improvement in loglikelihood when moving from a 3-class to a 4-class model was not significant (p = 0.34). Thus, for reasons of parsimony, the 3-class model was the preferred choice. To address class separation, a series of Wald tests were employed and tested threshold-level differences across classes on each of the 14 behaviors. Results indicated that all tests were significant at p < 0.001 (see Table S1 in Supplementary Material). We defined the latent classes based on a mean coded core symptom score that was derived from the coding outlined in the methods (each social communication behavior was coded as absent (2); inconsistent(1); or consistent(0); Fig. 1). Class 1 (N = 155, 31.0%) represented participants showing the least consistency in demonstrating social communication behaviors (i.e., greatest degree of consistency of social communication deficits). Class 2 (N = 219, 43.8%) demonstrated moderate consistency of social communication behaviors and contained the largest percentage of participants. Class 3 (N = 126, 25.2%) represented participants who showed the highest degree of consistency in the use of social communication skills. Classes were differentiated across all social communication behaviors, including eye contact (see Table S1 in supplementary material). This finding emerged despite the fact that in the available data children were rarely documented to have “absent” eye contact and similarly very rarely was eye contact documented to be “consistent,” thus limiting the variability for that specific social communication skill. Demonstration of a distal point and imitation are behaviors that differentiate Class 3 from Classes 1 and 2. In other words, participants in Class 3 showed more consistent use of these social communication skills than participants in other classes.

Optimal latent class solution for classifying social communication deficits. The scaling on the y-axis pertains to the following coding: skill being absent (coded as 2, met ASD criteria); inconsistent (coded as 1, met ASD criteria); consistent (coded as 0, did not meet ASD criteria)
In the LCA of RRB symptoms, a 2-class model provided optimal model fit (Table 5). The difference in log likelihoods when moving from a 2-class to a 3-class model was significant (p = 0.02) but that was likely an artifact of excessive power levels due to the large sample size. As is seen in Fig. 2, Class 1 exhibited more RRB behaviors (N = 315, 63.0%). Class 2 demonstrated fewer behaviors (N = 185, 37.0%). Participants in both latent classes demonstrated a relatively high probability of stereotypies and sensory interests. Class separation was noted mainly in the following behaviors: echolalia, repetitive use of objects, ritualized behavior, extreme distress with change, fixated interests, and to a lesser degree by atypical visual regard (using a one-tailed test) (see Supplementary Material Table S2).

Optimal latent class solution for classifying restrictive/repetitive behaviors. The scaling on the y-axis pertains to the following coding: present, met ASD criteria (coded as 1); absent/not mentioned, did not meet ASD criteria (coded as 0). Given that these skills represent DSM based criteria for ASD identification, the estimates in the figure show the probability that a given class meets these criteria. For example, in the severe RRB class the probability of children having self-injurious behavior was 20% but the probability of meeting the repetitive behavior criterion was over 95% (i.e., 95% of the children in this class had repetitive behaviors)
Relationship of Demographic Characteristics and Developmental Profiles to Latent Classes
We evaluated how developmental domains (cognitive, language, motor, and adaptive), along with demographic variables (sex, age, and income) related to the core ASD symptom latent classes. Scores were treated as continuous variables; mean scores were determined for each of the latent classes and were compared across classes using Pearson chi square tests. Bayley Cognitive SS were used, excluding 14 participants with missing data due to use of another measure as noted above. Due to variability in medical record documentation of Bayley Language or Motor SS, the Vineland Communication SS and Vineland Motor SS were used, respectively, to compare functioning in these two domains. In order to ensure that this decision to use the Vineland scores in place of Bayley scores was justified, we ran correlation analyses between scores from the Vineland and Bayley scales which demonstrated a high correlation in both the language and motor domains, specifically r = 0.743, p < 0.001 between the language measures and r = 0.560, p < 0.001 between the motor measures, suggesting strong convergence. The Vineland was also used for social and global adaptive functioning comparisons.
For the social communication classes, there was a statistically significant relationship between cognitive scores and class membership (mean SS = 91.1 in Class 3, SS = 81.2 in Class 2, and SS = 71.7 in Class 1). All other domains of developmental functioning (Vineland Communication, Daily Living and Adaptive Composite) followed a similar pattern (Table 6). Significant differences between social communication classes emerged for age, with Class 3 having a higher proportion of older participants (mean 28.0 months) while Class 1 had the highest proportion of younger participants (mean 24.4 months). There were no significant differences across the three latent classes for sex or median household income. Interestingly, despite observing a null effect in the relationship between sex and social communication class membership, we identified a trend suggesting a higher proportion of females in Class 1 (p = 0.08 using a one-tailed test). The chi-square test may have failed to exceed conventional levels of significance due to low power as there were cells with 18 individuals, when the expected frequencies assumption required 26 individuals per cell.
For the RRB 2-class model, there also was a statistically significant relationship between cognitive score and class membership, but in the opposite direction (mean SS = 82.0 in Class 1 and mean SS = 78.2 in Class 2). Again, this relationship held true across other domains of developmental functioning except for Vineland Socialization and Motor skills, for which there was no statistically significant difference. (see Table 7). Of note, we found smaller differences in mean scores for function across the RBB classes as compared to the social communication classes. These smaller differences may not be clinically apparent. Among demographic variables, Class 2 (lower number of behaviors demonstrated) consisted of younger individuals and fewer males compared to Class 1 (higher number of behaviors demonstrated). For income, there was no statistically significant difference between classes.
Discussion
We describe a sample of toddlers with a DSM-5 diagnosis of ASD and utilize clinically observable core ASD symptoms to demonstrate the existence of latent classes of ASD symptomatology. Mean Bayley Scales cognitive standard scores for the entire sample were similar to those in samples of toddlers with a DSM-IV diagnosis, and mean scores on the Vineland Adaptive Behavior Scales demonstrated a pattern seen in toddlers with a DSM-IV diagnosis, specifically motor > daily living > socialization > communication skills (Jashar et al. 2016; Long et al. 2011; Yang et al. 2016). Latent classes of ASD symptom demonstration were constructed from clinician-observed behaviors documented during the clinical encounter. Social communication (SC) behaviors favored a three-class model while restricted/repetitive behaviors (RRB) favored a two-class model. Classes with a higher degree of consistently demonstrating SC deficits were younger, and had lower developmental functioning. The class with a higher number of restricted/repetitive behaviors was older, with higher developmental functioning.
Previous studies that have sought to subgroup children with ASD have often combined core symptoms and developmental functioning in models and have included children of all ages. Additionally, attempts to quantify core ASD symptoms have used various methods, from global scores (Social Communication Questionnaire, ADOS Total Severity Scores) to a more qualitative description of core symptom behaviors, with the latter being less common (Georgiades et al. 2013; Kim et al. 2018; Kim et al. 2016; Wiggins et al. 2012, 2017). In this study, we sought to better understand the heterogeneity in presentation, specifically for the toddler age group, at diagnosis with DSM-5 ASD via latent class analyses that were based solely on core ASD symptom behaviors observable in clinical practice. These analyses based on core ASD symptoms among toddlers are unique to date in the literature, and as such, we cannot directly compare our results to prior studies that use different variables in their models. Despite the inability to draw direct comparisons, we do note differences and similarities to other studies using latent class analysis or a similar methodology to assess for subgroups of toddlers with ASD.
Many previous studies are in DSM-IV defined populations, but in a study utilizing DSM-5 diagnostic criteria, Georgiades and colleagues used factor mixture modeling in a cohort of over 300 preschoolers with ASD (Georgiades et al. 2013). Items from the Autism Diagnostic Interview-Revised (ADI-R) that correlated with DSM-5 criteria were used as indicators to reveal three classes of severity across both core symptom domains (Georgiades et al. 2013). Similar to Georgiades, we demonstrated three classes of social communication symptoms differentiated by consistency with which social behaviors were demonstrated. However, in our sample, the RRBs best fit a two class model. Interestingly, within Georgiades’ results, two of the three classes appear to overlap for specific RRBs, including stereotypies, repetitive object use, and sensory symptoms (Georgiades et al. 2013). Additionally, Georgiades and colleagues highlight that the gradient of severity in their three classes did not follow the same pattern for the different core symptom domains (SC and RRBs), leading the authors to suggest treating these domains as “independent spectra that together make up the overall compound ASD phenotype” (Georgiades et al. 2013). Furthermore, a subset of their cohort was re-evaluated at age 6 years, at which time 2 classes provided the best statistical fit to the RRB data (Georgiades et al. 2014). Additional studies support the view that the social communication and RRB domains are different constructs and should be considered separately when quantifying severity of ASD symptoms (Kang et al. 2019; Kim et al. 2019; Mandy and Skuse 2008).
Wiggins and colleagues used composite scores from the ADOS for the social communication domain while using discrete items from the ADI-R to capture the RRB core symptoms in their latent class model (2017). They also included domains of functioning and co-occurring behavioral conditions as variables. Their model revealed four classes: mild language delay with cognitive rigidity, mild language delay and motor delay with dysregulation, general developmental delay, and significant developmental delay with repetitive motor behaviors (Wiggins et al. 2017). As multiple variables beyond core symptoms were used in this model, we are unable to make direct comparisons to our sample. Social communication behaviors did not appear to play a prominent role in characterizing their latent classes. Some RRBs did distinguish amongst classes (cognitive rigidity), while others (sensory symptoms) were exhibited frequently across classes, a finding consistent with our results (Wiggins et al. 2017).
In our study, cognitive, language, adaptive, and motor functioning varied significantly across the classes. Classes with more consistent deficits in social communication had a greater percentage of participants with lower developmental functioning, similar to results obtained by Georgiades (2013). In fact, the mean cognitive score for participants in Class 1 was at the borderline range for developmental delay, while the mean cognitive score for participants in Class 3 was within the low end of the average range. Similarly, communication and global adaptive scores were notably different between the groups, with participants in Class 1 having a mean score in the low range, below the clinical cut off for delay, and participants in Class 3 having a mean score just below the average or adequate range on the Vineland Scales. Prior studies have suggested a higher degree of social communication deficits in children with lower language and/or cognitive functioning or have found that children with lower developmental functioning may be more likely to demonstrate atypical or delayed social communication development compared to children of the same chronological age (Charman et al. 1998; Gotham et al. 2012; Landry and Loveland 1988; Catherine Lord and Pickles 1996; Thurm et al. 2019; Trillingsgaard et al. 2005; Ventola et al. 2007).
For RBB classes, subjects in RBB Class 1 had higher developmental functioning. This contrasts with the findings for SC classes, where subjects in Class I had lower developmental functioning. Prior research suggests that individuals with lower developmental functioning demonstrate high levels of repetitive sensory and motor behaviors, while other RRBs related to “insistence on sameness” are considered “higher order” in that they may require higher language or cognitive functioning in order to be manifested (Cuccaro et al. 2003; Szatmari et al. 2006). In their latent class analysis of toddlers, Wiggins and colleagues also demonstrated higher language functioning to be associated with increased cognitive rigidity (Wiggins et al. 2017). In our study, the RRBs that best discriminated between the two subgroups (echolalia, repetitive object use, ritualized behavior, fixated interests and extreme distress with change) are consistent with this conceptualization that a higher level of developmental functioning may be necessary in order to manifest certain RRBs.
Age varied across the core ASD symptom classes. In the social communication domain, there was a greater proportion of younger participants in Class 1. Children who do not manifest social communication skills or only do so inconsistently are more severely affected and thus likely to be identified at younger ages. In contrast, children who demonstrate a higher frequency of attempts at social communication behaviors may be identified later as their deficits are not as apparent until expectations or demands for social communication increase. In contrast, for the RRB domain, there was a greater portion of older participants in Class 1. This is consistent with other studies describing the emergence of more RRBs with age (Charman et al. 2005; Guthrie et al. 2013; Richler et al. 2007; Szatmari et al. 2006; Wiggins et al. 2017).
We identified a higher percentage of males in the RRB Class 1 (i.e., the class with more RRBs). This finding is aligned with previous literature documenting more RRBs in males compared to females. (Frazier et al. 2014; Mandy et al. 2012; Szatmari et al. 2012; Tillmann et al. 2018). It has been suggested that females may demonstrate a more subtle presentation of restricted interests or express them in a more socially oriented manner when compared to males (McFayden et al. 2019). While there was not a statistically significant difference in sex among the social communication classes, there was a trend toward a higher number of females in Class 1 (i.e., the class defined by the lowest frequency of use of social communication skills). This finding is consistent with a body of literature that has reported either no differences in social communication deficit severity between sexes or lower social communication skills in females compared to males presenting at young ages (Carter et al. 2007; Lawson et al. 2018; Ros‐Demarize et al. 2020).
There are several limitations that should be noted when interpreting the findings of this study. We used retrospective data which is limited to information that was documented in the medical record. As described in the Method section, behaviors used to construct our latent classes were derived from narrative accounts within the medical records, mostly from the narrative descriptions of behaviors observed during administration of the ADOS in one clinical evaluation session. It is possible that behavior documented during ADOS administration or other portions of the clinical encounter were not indicative of a child’s typical behavioral functioning. Assessments were not administered in a research setting, although all psychologists were clinically reliable on the ADOS. Clinicians routinely documented social communication behaviors in terms of consistency (consistent, inconsistent, absent) but did not routinely document RRBs in this manner, only noting if the RRB was present or absent. Thus, there is less nuanced information for RRB symptomatology compared to social communication symptomatology. Numeric scores on the ADOS were not available for our retrospective study and therefore could not be incorporated into our analyses. However, prior studies have more often noted challenges with using ADOS numeric scores as a means to assess severity (Kim et al. 2018). Future work would ideally include both observable item level features and ADOS numeric scores to assess this relationship. The sample comes from a single tertiary care center. However, in our region, all children with concern for ASD are referred to a tertiary center in order to access government funded intensive intervention services. Thus, we believe our sample is representative of our region. While a Bayley Scales cognitive score was obtained for almost all participants, direct motor and language scores via the Bayley Scales were variably obtained based on provider preference, requiring Vineland parent report to be used for comparison of motor and language functioning across the latent classes. We are reassured by the high correlation between these tests when both were used. Finally, subtypes identified in this study via data generated statistical methods depended on the variables available to us for analysis. It will be important to assess for these classes of core ASD symptoms in other study populations, and to follow them longitudinally to determine individuals’ trajectories and responses to treatment in order to explore whether these classes may reflect ASD core symptom severity.
Our study’s strengths include a large sample size and the use of observable, core ASD symptom behaviors to identify two sets of latent classes, one for social communication and the other for restricted and repetitive behaviors. Our findings share many important similarities with prior studies based on DSM-IV ASD among toddlers; however, unlike other studies that combined both core symptoms and other developmental functioning measures, we sought to phenotypically subgroup toddlers solely using core symptom behaviors that were clinically observed at a diagnostic evaluation using the newer DSM-5 criteria. As children are diagnosed with ASD at younger and younger ages, the ability to understand the patterns with which young children display these core ASD symptom behaviors will be important, as broader global scores might not fully capture emerging symptoms in this population. Our study suggests that appreciable, distinct classes based on core ASD symptoms may exist within the broad, heterogeneous ASD phenotype, even at the time of diagnosis in toddlers. It will be important to attempt to replicate these findings in other populations, and to evaluate the extent to which class membership may be correlated with developmental trajectories and outcomes for toddlers receiving an ASD diagnosis. Additionally, our findings suggest that there are correlations between core ASD symptom profiles and functioning in other developmental domains that are distinct in directionality depending on the ASD symptom domain (social communication or restricted/repetitive behaviors). These findings also require replication in future studies across more diverse populations, but if consistent, could be a beginning step in better understanding ASD’s heterogeneity. Further analysis of core symptom behaviors and their role as predictors of diagnosis and/or response to therapy is also an area worth exploration, particularly for specific behaviors that discriminate between sub-groups of toddlers with ASD. If the latent classes from our study prove to be associated with different developmental trajectories, response to treatment, and functional outcomes, there is potential to better counsel and support parents at the time of diagnosis and ultimately, to individualize therapeutic recommendations.
Conclusions
Latent class analyses of observable core symptom behaviors in a large cohort of toddlers with DSM-5 ASD revealed meaningful latent classes in each core ASD symptom domain, offering a potential approach to understanding the heterogeneity of core ASD symptoms at the time of diagnosis. In our sample, social communication core symptoms fit a three class model. The classes with absent to less consistent use of social communication behaviors were younger in age, and had a greater percentage of participants with lower cognitive, language, motor, and adaptive functioning. Restricted and repetitive behavior core symptoms were best understood with a two class model. In this case, the class demonstrating a greater number of restricted and repetitive behaviors were older in age, had a higher percentage of males, and had a greater percentage of participants with higher cognitive, language, motor and adaptive functioning. If confirmed in other populations, these classes may more precisely characterize subgroups within the heterogeneous group of toddlers at time of ASD diagnosis.
Change history
08 March 2021
A Correction to this paper has been published: https://doi.org/10.1007/s10803-021-04954-5
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, D.C.: American Psychiatric Association. https://doi.org/10.1176/appi.books.9780890423349.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, D.C.: American Psychiatric Association. https://doi.org/10.1176/appi.books.9780890425596.744053.
Anderson, D. K., Liang, J. W., & Lord, C. (2014). Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. Journal of Child Psychology and Psychiatry, 55(5), 485–494. https://doi.org/10.1111/jcpp.12178.
Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Weaver, A. L., & Jacobsen, S. J. (2005). The incidence of autism in Olmsted County, Minnesota, 1976–1997: Results from a population-based study. Archives of Pediatrics and Adolescent Medicine. https://doi.org/10.1001/archpedi.159.1.37.
Barton, M. L., Robins, D. L., Jashar, D., Brennan, L., & Fein, D. (2013). Sensitivity and specificity of proposed DSM-5 criteria for autism spectrum disorder in toddlers. Journal of Autism and Developmental Disorders, 43(5), 1184–1195. https://doi.org/10.1007/s10803-013-1817-8.
Bayley, N. (2006). Bayley Scales of infant and toddler development, third edition: Administration manual. J Psychoeduc Assess. https://doi.org/10.1177/0734282906297199.
Ben-Itzchak, E., Watson, L. R., & Zachor, D. A. (2014). Cognitive ability is associated with different outcome trajectories in autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(9), 2221–2229. https://doi.org/10.1007/s10803-014-2091-0.
Bitsika, V., Sharpley, C. F., & Orapeleng, S. (2008). An exploratory analysis of the use of cognitive, adaptive and behavioural indices for cluster analysis of ASD subgroups. Journal of Intellectual Disability Research, 52(11), 973–985. https://doi.org/10.1111/j.1365-2788.2008.01123.
Bozdogan, H. (1987). Model selection and Akaike’s Information Criterion (AIC): The general theory and its analytical extensions. Psychometrika, 52, 345–370. https://doi.org/10.1007/BF02294361.
Carter, A. S., Black, D. O., Tewani, S., Connolly, C. E., Kadlec, M. B., & Tager-Flusberg, H. (2007). Sex differences in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(1), 86–97. https://doi.org/10.1007/s10803-006-0331-7.
Charman, T., Swettenham, J., Baron-Cohen, S., Cox, A., Baird, G., & Drew, A. (1998). An experimental investigation of socialcognitive abilities in infants with autism: Clinical implications. Infant Mental Health Journal, 19(2), 260–275. https://doi.org/10.1002/(SICI)1097-0355(199822)19:2%3c260::AID-IMHJ12%3e3.0.CO;2-W.
Charman, T., Taylor, E., Drew, A., Cockerill, H., Brown, J. A., & Baird, G. (2005). Outcome at 7 years of children diagnosed with autism at age 2: Predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. Journal of Child Psychology and Psychiatry and Allied Disciplines. https://doi.org/10.1111/j.1469-7610.2004.00377.
Chawarska, K., Klin, A., Paul, R., Macari, S., & Volkmar, F. (2009). A prospective study of toddlers with ASD: Short-term diagnostic and cognitive outcomes. Journal of Child Psychology and Psychiatry and Allied Disciplines, 50(10), 1235–1245. https://doi.org/10.1111/j.1469-7610.2009.02101.
Cuccaro, M. L., Shao, Y., Grubber, J., Slifer, M., Wolpert, C. M., Donnelly, S. L., … Pericak-Vance, M. A. (2003). Factor analysis of restricted and repetitive behaviors in autism using the autism diagnostic interview-R. Child Psychiatry and Human Development, 34(1), 3–17.https://doi.org/10.1023/A:1025321707947.
Estes, A., Zwaigenbaum, L., Gu, H., St John, T., Paterson, S., Elison, J. T., … Piven, J. (2015). Behavioral, cognitive, and adaptive development in infants with autism spectrum disorder in the first 2 years of life. Journal of Neurodevelopmental Disorders, 7(1), 24.https://doi.org/10.1186/s11689-015-9117-6.
Fountain, C., Winter, A. S., & Bearman, P. S. (2012). Six developmental trajectories characterize children with autism. Pediatrics, 129(5), e1112–e1120. https://doi.org/10.1542/peds.2011-1601.
Frazier, T. W., Georgiades, S., Bishop, S. L., & Hardan, A. Y. (2014). Behavioral and cognitive characteristics of females and males with autism in the simons simplex collection. Journal of the American Academy of Child and Adolescent Psychiatry, 153(3), 329–340. https://doi.org/10.1016/j.dcn.2011.01.002.The.
Georgiades, S., Boyle, M., Szatmari, P., Hanna, S., Duku, E., Zwaigenbaum, L., … Thompson, A. (2014). Modeling the phenotypic architecture of autism symptoms from time of diagnosis to age 6. Journal of Autism and Developmental Disorders, 44(12), 3045–3055.https://doi.org/10.1007/s10803-014-2167-x.
Georgiades, S., Szatmari, P., Boyle, M., Hanna, S., Duku, E., Zwaigenbaum, L., … Thompson, A. (2013). Investigating phenotypic heterogeneity in children with autism spectrum disorder: A factor mixture modeling approach. Journal of Child Psychology and Psychiatry and Allied Disciplines, 54(2), 206–215.https://doi.org/10.1111/j.1469-7610.2012.02588.
Gibbs, V., Aldridge, F., Chandler, F., Witzlsperger, E., & Smith, K. (2012). Brief report: an exploratory study comparing diagnostic outcomes for autism spectrum disorders under DSM-IV-TR with the proposed DSM-5 revision. Journal of Autism and Developmental Disorders, 42(8), 1750–1756. https://doi.org/10.1007/s10803-012-1560-6.
Gotham, K., Pickles, A., & Lord, C. (2012). Trajectories of autism severity in children using standardized ADOS scores. Pediatrics, 130(5), 1278. https://doi.org/10.1542/peds.2011-3668.
Guthrie, W., Swineford, L. B., Nottke, C., & Wetherby, A. M. (2013). Early diagnosis of autism spectrum disorder: stability and change in clinical diagnosis and symptom presentation. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54(5), 582–590. https://doi.org/10.1111/jcpp.12008.
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. https://doi.org/10.1016/j.jbi.2008.08.010.
Harris, S. L., & Handleman, J. S. (2000). Age and IQ at intake as predictors of placement for young children with autism: a four- to six-year follow-up. Journal of Autism and Developmental Disorders, 30(2), 137–142. https://doi.org/10.1023/a:1005459606120.
Harstad, E. B., Fogler, J., Sideridis, G., Weas, S., Mauras, C., & Barbaresi, W. J. (2015). Comparing diagnostic outcomes of autism spectrum disorder using DSM-IV-TR and DSM-5 criteria. Journal of Autism and Developmental Disorders, 45(5), 1437–1450. https://doi.org/10.1007/s10803-014-2306-4.
Jashar, D. T., Brennan, L. A., Barton, M. L., & Fein, D. (2016). Cognitive and adaptive skills in toddlers who meet criteria for autism in DSM-IV but not DSM-5. Journal of Autism and Developmental Disorders, 46(12), 3667–3677. https://doi.org/10.1007/s10803-016-2901-7.
Kang, E., Gadow, K. D., & Lerner, M. D. (2019). Atypical communication characteristics, differential diagnosis, and the autism spectrum disorder phenotype in youth. Journal of Clinical Child & Adolescent Psychology, 49(2), 1–13. https://doi.org/10.1080/15374416.2018.1539912.
Kim, H., Keifer, C., Rodriguez-Seijas, C., Eaton, N., Lerner, M., & Gadow, K. (2019). Quantifying the optimal structure of the autism phenotype: A comprehensive comparison of dimensional, categorical, and hybrid models. Journal of the American Academy of Child and Adolescent Psychiatry, 58(9), 876-886.e2. https://doi.org/10.1016/j.jaac.2018.09.431.
Kim, S. H., Bal, V. H., Benrey, N., Choi, Y. B., Guthrie, W., Colombi, C., & Lord, C. (2018). Variability in autism symptom trajectories using repeated observations from 14 to 36 months of age. Journal of the American Academy of Child and Adolescent Psychiatry, 57(11), 837–848.e2. https://doi.org/10.1016/j.jaac.2018.05.026.
Kim, S. H., Macari, S., Koller, J., & Chawarska, K. (2016). Examining the phenotypic heterogeneity of early autism spectrum disorder: Subtypes and short-term outcomes. Journal of Child Psychology and Psychiatry and Allied Disciplines, 57(1), 93–102. https://doi.org/10.1111/jcpp.12448.
Landry, S. H., & Loveland, K. A. (1988). Communication behaviors in autism and developmental language delay. Journal of Child Psychology and Psychiatry. https://doi.org/10.1111/j.1469-7610.1988.tb01884.
Lawson, L. P., Joshi, R., Barbaro, J., & Dissanayake, C. (2018). Gender differences during toddlerhood in autism spectrum disorder: A prospective community-based longitudinal follow-up study. Journal of Autism and Developmental Disorders, 48(8), 2619–2628. https://doi.org/10.1007/s10803-018-3516-y.
Long, C., Gurka, M. J., & Blackman, J. (2011). Cognitive skills of young children with and without autism spectrum disorder using the BSID-III. Autism Research and Treatment, 2011, 1–7. https://doi.org/10.1155/2011/759289.
Lord, C., Luyster, R., Guthrie, W., & Pickles, A. (2012b). Patterns of developmental trajectories in toddlers with autism spectrum disorder. Journal of Consulting and Clinical Psychology, 80(3), 477–489. https://doi.org/10.1037/a0027214.
Lord, C., & Pickles, A. (1996). Language behaviors level and nonverbal social-communicative in autistic and language-delayed children. Journal of the American Academy of Child & Adolescent Psychiatry. https://doi.org/10.1097/00004583-199611000-00024.
Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012a). Autism diagnostic observation schedule, second edition (ADOS-2) manual (Part I): Modules 1–4. Firenze: Giunti OS.
Mandy, W., Chilvers, R., Chowdhury, U., Salter, G., Seigal, A., & Skuse, D. (2012). Sex differences in autism spectrum disorder: Evidence from a large sample of children and adolescents. Journal of Autism and Developmental Disorders, 42(7), 1304–1313. https://doi.org/10.1007/s10803-011-1356-0.
Mandy, W. P. L., & Skuse, D. H. (2008). Research Review: What is the association between the social-communication element of autism and repetitive interests, behaviours and activities? Journal of Child Psychology and Psychiatry and Allied Disciplines, 49(8), 795–808. https://doi.org/10.1111/j.1469-7610.2008.01911.
Masyn, K. E. (2013). Latent Class analysis and finite mixture modeling. In T.D. Little (Ed.). In The oxford handbook of quantitative methods: Vol 2: Statistical Analysis: Oxford University Press. Retrieved 17 Jun. 2020, from https://www.oxfordhandbooks.com/view/https://doi.org/10.1093/oxfordhb/9780199934898.001.0001/oxfordhb-9780199934898-e-025.
McFayden, T. C., Albright, J., Muskett, A. E., & Scarpa, A. (2019). Brief report: Sex differences in ASD diagnosis—A brief report on restricted interests and repetitive behaviors. Journal of Autism and Developmental Disorders, 49(4), 1693–1699. https://doi.org/10.1007/s10803-018-3838-9.
Moulton, E., Barton, M. L., Robins, D. L., Abrams, D. N., & Fein, D. A. (2016). Early characteristics of children with ASD who demonstrate optimal progress between age two and four. Journal of Autism and Developmental Disorders, 46(6), 2160–2173. https://doi.org/10.1016/j.coviro.2015.09.001.
Munson, J., Dawson, G., Sterling, L., Beauchaine, T., Zhou, A., Koehler, E., … Abbott, R. (2008). Evidence for latent classes of IQ in young children with autism spectrum disorder. American Journal on Mental Retardation, 113(6), 439–452.https://doi.org/10.1352/2008.113:439-452.
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Structural equation modeling: A multidisciplinary journal deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling, 14(4), 535–569. https://doi.org/10.1080/10705510701575396.
Pierce, K., Gazestani, V. H., Bacon, E., Barnes, C. C., Cha, D., Nalabolu, S., … Courchesne, E. (2019). Evaluation of the diagnostic stability of the early autism spectrum disorder phenotype in the general population starting at 12 months. JAMA Pediatrics, 173(6), 578–587.https://doi.org/10.1001/jamapediatrics.2019.0624.
Richler, J., Bishop, S. L., Kleinke, J. R., & Lord, C. (2007). Restricted and repetitive behaviors in young children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(1), 73–85. https://doi.org/10.1007/s10803-006-0332-6.
Ros‐Demarize, R., Bradley, C., Kanne, S. M., Warren, Z., Boan, A., Lajonchere, C., … Carpenter, L. A. (2020). ASD symptoms in toddlers and preschoolers: An examination of sex differences. Autism Research, 13(1), 157–166.https://doi.org/10.1002/aur.2241.
Sparrow, S. S., Cicchetti, D. V., & Balla, D. A. (2005). Vineland-II adaptive behavior scales, second edition. San Antonio: PsychCorp.
Sparrow, S. S., & Cichetti, D. V. (2016). Vineland adaptive behavior scales, third edition (Vineland-3) manual. San Antonio: PsychCorp.
Stevens, M. C., Fein, D. A., Dunn, M., Allen, D., Waterhouse, L. H., Feinstein, C., & Rapin, I. (2000). Subgroups of children with autism by cluster analysis: A longitudinal examination. Journal of the American Academy of Child and Adolescent Psychiatry, 39(3), 346–352. https://doi.org/10.1097/00004583-200003000-00017.
Szatmari, P., Georgiades, S., Bryson, S., Zwaigenbaum, L., Roberts, W., Mahoney, W., … Tuff, L. (2006). Investigating the structure of the restricted, repetitive behaviours and interests domain of autism. Journal of Child Psychology and Psychiatry and Allied Disciplines, 47(6), 582–590.https://doi.org/10.1111/j.1469-7610.2005.01537.
Szatmari, P., Liu, X. Q., Goldberg, J., Zwaigenbaum, L., Paterson, A. D., Woodbury-Smith, M., … Thompson, A. (2012). Sex differences in repetitive stereotyped behaviors in autism: Implications for genetic liability. American Journal of Medical Genetics, Part B: Neuropsychiatric Genetics, 159 B(1), 5–12. https://doi.org/10.1002/ajmg.b.31238.
Szatmari, P., Georgiades, S., Duku, E., Bennett, T. A., Bryson, S., Fombonne, E., … Pathways in ASD Study Team. (2015). Developmental trajectories of symptom severity and adaptive functioning in an inception cohort of preschool children with autism spectrum disorder. JAMA Psychiatry, 72(3), 276–283. https://doi.org/10.1001/jamapsychiatry.2014.2463.
Thurm, A., Farmer, C., Salzman, E., Lord, C., & Bishop, S. (2019). State of the field: Differentiating intellectual disability from autism spectrum disorder. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2019.00526.
Tillmann, J., Ashwood, K., Absoud, M., Bölte, S., Bonnet-Brilhault, F., Buitelaar, J. K., … Charman, T. (2018). Evaluating sex and age differences in ADI-R and ADOS scores in a large European multi-site sample of individuals with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(7), 2490–2505.https://doi.org/10.1007/s10803-018-3510-4.
Trillingsgaard, A., Sørensen, E. U., Němec, G., & Jørgensen, M. (2005). What distinguishes autism spectrum disorders from other developmental disorders before the age of four years? European Child and Adolescent Psychiatry. https://doi.org/10.1007/s00787-005-0433-3.
Ventola, P., Kleinman, J., Pandey, J., Wilson, L., Esser, E., Boorstein, H., … Fein, D. (2007). Differentiating between autism spectrum disorders and other developmental disabilities in children who failed a screening instrument for ASD. Journal of Autism and Developmental Disorders, 37(3), 425–436.https://doi.org/10.1007/s10803-006-0177-z.
Wiggins, L. D., Robins, D. L., Adamson, L. B., Bakeman, R., & Henrich, C. C. (2012). Support for a dimensional view of autism spectrum disorders in toddlers. Journal of Autism and Developmental Disorders, 42(2), 191–200. https://doi.org/10.1007/s10803-011-1230-0.
Wiggins, L. D., Tian, L. H., Levy, S. E., Rice, C., Lee, L. C., Schieve, L., … Thompson, W. (2017). Homogeneous subgroups of young children with autism improve phenotypic characterization in the study to explore early development. Journal of Autism and Developmental Disorders, 47(11), 3634–3645.https://doi.org/10.1007/s10803-017-3280-4.
Yang, S., Paynter, J. M., & Gilmore, L. (2016). Vineland adaptive behavior scales: II profile of young children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(1), 64–73. https://doi.org/10.1007/s10803-015-2543-1.
Zwaigenbaum, L., Bryson, S., & Garon, N. (2013). Early identification of autism spectrum disorders. Behavioural Brain Research, 251, 133–146. https://doi.org/10.1016/j.bbr.2013.04.004.
Acknowledgments
All phases of this study were supported by the Palmer Family Fund for Autism Research. Study data were collected and managed using REDCap electronic data capture tools hosted at Boston Children’s Hospital. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. In light of the use of RedCap for this project, this publication was supported by NIH/NCRR Colorado CTSI Grant Number UL1 RR025780. Its contents are the authors’ sole responsibility and do not necessarily represent official NIH views.
Author information
Authors and Affiliations
Contributions
HKH, GDS, WJB, and EH contributed to the study conception and design. HKH and CL contributed to data collection. EH oversaw data collection and review. GDS performed statistical analyses. The first draft of the manuscript was written by HKH and GDS, WJB, and EH provided significant edits on subsequent revised versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Harris, H.K., Lee, C., Sideridis, G.D. et al. Identifying Subgroups of Toddlers with DSM-5 Autism Spectrum Disorder Based on Core Symptoms. J Autism Dev Disord 51, 4471–4485 (2021). https://doi.org/10.1007/s10803-021-04879-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-04879-z