
Abstract
There is substantial comorbidity between autism spectrum disorder (ASD) and attention deficit/hyperactivity disorder (ADHD), and there are well-documented executive functioning (EF) deficits in both populations. An important question concerns whether EF deficits in children with ASD are related to severity of ASD, ADHD, or both. We examined ADHD and ASD symptoms in relation to ratings of EF in the home and classroom. The sample comprised 64 children (55 males) diagnosed with ASD (mean age = 9.26 years; mean FSIQ = 92). Analyses indicated that parent and teacher ratings of EF (except Shift and Emotional Control) were consistently related to ADHD symptom severity, but not to ASD severity. Thus, functioning in the domains of Shift and Emotional control appear relatively spared, whereas performance in all other EF was impaired in relation to ADHD symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
A substantial proportion of children with autism spectrum disorder (ASD) have symptoms of inattention, hyperactivity, and impulsivity that warrant a diagnosis of attention deficit/hyperactivity disorder (ADHD). A review by Leitner (2014) found prominent ADHD symptoms among 37–85% of individuals with ASD. Indeed, by late elementary school or early adolescence, the effects of comorbid psychiatric symptoms—such as ADHD—on individuals with ASD are often more problematic than core ASD symptoms (Loveland 2005; Mansour et al. 2017a, b; Pearson et al. 2006). Deficits in executive functioning (EF), including goal-directed behavior and inhibition, have long been implicated in ADHD (Barkley 1997; Sergeant et al. 2002). A number of studies have also found evidence of EF impairments in ASD (Demetriou et al. 2018; Granader et al. 2014; Ozonoff and Jensen 1999; Sergeant et al. 2002)—although in at least one previous study, approximately one-third of the adult ASD sample showed no EF impairment (Johnson et al. 2019).
Given that EF deficits are associated with ADHD, and that symptoms of ADHD often co-occur in children with ASD, children with ASD who also have significant ADHD symptoms (i.e., ASD+ADHD) may have a substantially higher risk for EF deficits. A prominent question is whether deficits in EF in children with ASD+ADHD are more closely related to their ASD or their ADHD symptoms. This is an important question that forms the rationale for this study. We hypothesize that if EF deficits are more closely associated with ADHD symptoms, as opposed to ASD symptoms, that it may be possible to treat these EF deficits with some of the same interventions that have been shown to be effective in ADHD such as stimulant medication. Although our group has found that cognitive task performance can be significantly improved by stimulant treatment in children with ASD and ADHD (Pearson et al. 2020), cognitive task performance does not always translate to real-work EF concerns (Ng et al. 2019; Van Eylen et al. 2015). EF deficits are related to real-world functional problems in ASD such as academic performance (John et al. 2018). Furthermore, they increase from childhood to late adolescence, (Rosenthal et al. 2013). If EF deficits are associated with ADHD symptoms that could be treated effectively with ADHD interventions, such treatment may result in real-world gains in the present (school) and in the future (job performance). The rationale for this study was to determine if ADHD symptoms were significantly related to EF deficits. If so, would ADHD treatments be indicated to treat EF deficits in some children with ASD (e.g., those who had significant ADHD symptoms) and perhaps not in other children with ASD (who do not have significant ADHD symptoms)?
It has been difficult to determine the contributions of ASD symptomatology and ADHD symptomatology to EF concerns because most studies examining EF deficits in ASD and ADHD samples compare EF profiles across different diagnostic groups (Craig et al. 2016). Semrud-Clikeman et al. (2010) studied EF in children with ASD, ADHD-C, ADHD-PI, and controls. They found that the number of ADHD symptoms and number of ASD symptoms accounted for significant proportions of the variance when all indices of the BRIEF were included in the model. However, ASD symptoms did not have a significant effect when EF indices were analyzed individually. A sizeable literature strongly suggests that children with either disorder, or both, exhibit weaknesses in aspects of EF as measured by laboratory-based cognitive tests (e.g., Corbett et al. 2009; Craig et al. 2016; Geurts et al. 2004; Goldberg et al. 2005; Happe et al. 2006). However, given that lab-based cognitive tasks may not capture real-world difficulties with planning, organization, and self-regulation (Ng et al. 2019; Van Eylen et al. 2015), many clinicians currently rely instead on rating scales indexing EF, such as the Behavioral Rating Inventory of Executive Function (BRIEF; Gioia et al. 2000a). EF deficits in ASD have also been demonstrated in studies using behavioral measures such as the BRIEF (e.g., Blijd-Hoogewys et al. 2014; Lawson et al. 2015; Rosenthal et al. 2013).
In summary, the literature suggests that EF deficits have consistently been found in children with ADHD and ASD. However, we are not aware of any previous study that has simultaneously examined the relative roles of ADHD and ASD symptoms in EF in the same children with ASD. Thus, it is not known if EF can be attributed primarily to severity of ADHD, to severity of ASD, or to some combination thereof. Furthermore, previous research has used only parent ratings of EF. Thus, it is also unknown what the relationship is between teacher ratings of EF and ADHD and ASD symptoms.
The objectives of this study were twofold: (1) to examine the contributions of parent-rated ADHD symptoms and ASD symptoms to ratings of EF deficits in the home, and (2) to examine the contributions of teacher-rated ADHD symptoms and ASD symptoms to EF deficits in the classroom.
Method
Procedure
This study was conducted as part of a larger investigation of ADHD symptoms in children with ASD. Participants were recruited from the general community via special education programs, special-needs schools, community clinics, ASD events, and parent advocacy groups. Parents who expressed interest in participation were asked to complete a phone screen interview with a master’s level psychologist, who administered the Social Communication Questionnaire (SCQ; Rutter et al. 2003a). Only children who scored ≥ 15 on the SCQ were invited to participate in the psychological assessment.
This study was approved by the institutional review board of the University of Texas Health Science Center at Houston. Consent from the parents and assent from the children (when appropriate) were obtained prior to commencing the study procedures. All participants included in the analyses met DSM-IV-TR criteria for Autistic Disorder, Asperger’s Disorder, or Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS). In addition, all participants met cutoff criteria on the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2001) and the Autism Diagnostic Interview-Revised (ADI-R; Rutter et al. 2003b). A diagnosis of ADHD was determined if participants met the DSM-IV-TR criteria for ADHD on a computerized clinical interview (DICA-IV; Reich et al. 1997), which was followed by a diagnostic interview conducted by a licensed psychologist (DAP). The diagnosis disregarded the DSM-IV-TR prohibition of diagnosing ADHD in the context of autism. Additionally, we gathered reports of impairment in multiple settings by the parents and teachers, and observation by the research team. Severity of ADHD symptoms was assessed using Conners’ Parent Rating Scale, Revised-Long (CPRS-R) and the Conners’ Teacher Rating Scale, Revised-Long ADHD Indexes (CTRS-R; Conners 1997). Final diagnoses were assigned following clinic observation by the study team, and case review by two licensed psychologists (DAP and KAL).
The primary caretaker for each child completed the parent report measures (e.g., Pearson et al. 2012). Teacher ratings were sent to subjects’ classrooms, and teachers mailed them back to the clinic. For children taking psychotropic medication, both parents and teachers were instructed, to the extent possible, to rate the child’s behavior when he or she was not taking medication.
Participants
As assessment of EF in children with intellectual disability can be exceptionally complex (Danielsson et al. 2012), participants were excluded from this EF study if they had an IQ below 70 (determined by the Stanford-Binet, 5th Edition [SB5; Roid 2003]). Participants were also excluded if English was not their primary language. The sample comprised 64 children (55 male) between the ages of 6 and 13 years old (mean age = 9.26), with a mean FSIQ of 92 (ranging from 70 to 116) on the SB5. Participants had an average mental age equivalent of 8.53 years (ranging from 4.83 to 15.0). Thirty-two participants (50% of the sample) had a diagnosis of Autism, 14 had a diagnosis of Asperger’s Disorder (21.9%), and 18 had a diagnosis of PDD-NOS (28.1%). Fifty-three of the participants (82.8% of the sample) met diagnostic criteria for ADHD in addition to ASD. Of the 53 participants who had ADHD, 37 had a combined presentation, 15 had Predominantly Inattentive type, and 1 had Predominantly Hyperactive/Impulsive type. Table 1 provides more details.
Twenty-six of the participants (40.63%) were taking psychotropic medications before the study. This included psychostimulants (31.25%), SSRIs and SNRIs (15.63%), atypical antipsychotics (10.94%), antihypertensives (4.69%), tricyclic antidepressants (3.13%), anticonvulsants (3.13%), antipsychotics (1.56%), mood stabilizers (1.56%), atomoxetine (1.56%), trazodone (1.56%), and central muscarinic antagonists (1.56%).
Measures
Stanford-Binet Intelligence Scale, 5th Edition (SB5)
The SB5 (Roid 2003) is normed for ages 2 through 80 years, and yields a measure of Full, Verbal, and Nonverbal IQ.
Diagnostic Interview for Children and Adolescents, 4th Edition-Parent Interview (DICA-IV)
The DICA-IV (Reich 2000; Reich et al. 1997) is a structured psychiatric interview that was administered to parents to assess major diagnostic categories of the DSM-IV. Importantly, the DICA-IV has been sensitive to psychiatric conditions in children with developmental disabilities (Pearson et al. 2013).
Social Communication Questionnaire, Lifetime (SCQ)
The SCQ (Rutter et al. 2003a) is a 40-item, parent-report questionnaire used to screen for ASD. Its score ranges from 0 to 40, with scores exceeding 15 indicating that a fuller work-up for ASD is needed.
Autism Diagnostic Observation Schedule (ADOS)
The ADOS (Lord et al. 2001) consists of a standard series of events, behavioral presses, and observations to determine presence of autism. It was used, in conjunction with the ADI-R (below), to diagnose ASD. The master’s level psychologist who administered the ADOS and the two supervising Ph.D.-level psychologists were all research-reliable on the ADOS (and the ADI-R). Most (59/64, or 92.2%) of the children in this project received Module 3, with one child (1.6%) receiving Module 2 and four children (6.3%) receiving Module 4.
Autism Diagnostic Interview, Revised (ADI-R)
The ADI-R (Rutter et al. 2003b), a 93-item, semi-structured interview assessing current and historical symptoms of ASD, was administered to primary caregivers. It is based on both DSM-IV and ICD-10 criteria for autism and has demonstrated good reliability and construct validity (Rutter et al. 2003b). The ADI-R yields scores on each of the three major domains [(a) reciprocal social interaction; (b) communication and language; and (c) restricted, repetitive, and interests]. The ADI-R total score was the measure of ASD symptom severity. Lefort-Besnard et al. (2020) have shown that the ADI-R is a reliable predictor of ASD symptom severity.
Conners’ Parent Rating Scale, Revised (CPRS-R)
The CPRS-R is widely used to assess ADHD and other behavioral/emotional issues (e.g., oppositional behavior, social problems) in the home setting. The CPRS-R is normed for children ages 3–17 years. The ADHD Index from the CPRS-R (Conners 1997) was used to assess ADHD severity. The ADHD Index from the CPRS-R is a 12-item scale. Internal consistency estimates range from .89 to .94 (Conners 1997).
Conners’ Teacher Rating Scale, Revised (CTRS-R)
The CTRS-R was completed by teachers to assess ADHD, behavioral, and emotional symptoms in the classroom setting (Conners 1997). The CTRS-R ADHD Index was the teacher measure of ADHD severity in the classroom. The ADHD Index from the CTRS-R is a 12-item scale. Internal consistency estimates range from .85 to .96 (Conners 1997).
Behavior Rating Inventory of Executive Function (BRIEF), Parent and Teacher Forms
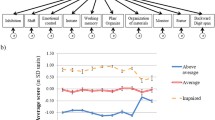
The BRIEF-Parent (BRIEF-P) and BRIEF-Teacher (BRIEF-T) (Gioia et al. 2000b) are widely used rating scales assessing executive functioning. They use age-based norms for individuals ages 5–18 years. They provide eight subscales of EF (Gioia et al. 2000b; psychometric properties are presented as parent/teacher): 1. Inhibit—ability to control impulses (Parent = 10 items/Teacher = 10 items, Parent α = .91/Teacher α = .96), 2. Shift—free movement from one situation or context to another (8/10 items, α = .81/.91), 3. Emotional Control—regulation of emotional responses (10/9 items, α = .89/.93), 4. Initiate—initiation of tasks/activities (8/7 items, α = .80/.90), 5. Working Memory—ability to hold information mentally (10/10 items, α = .89/.93), 6. Plan/Organize—set goals and create appropriate steps for future plans (12/10 items, α = .90/.91), 7. Organization of Materials—orderliness of play/work space and materials (6/7 items, α = .87/.92), and 8. Monitor—evaluate effects of behavior on others (8/10 items, α = .83/.90). The clinical scales form two broad indexes, Behavioral Regulation (BRI; α = .94/.97) and Metacognition (MI; α = .96/.98), and an overall score, the Global Executive Composite (GEC; α = .97/.98). Parents and teachers rated subjects on the BRIEF-Parent Form (BRIEF-P) and BRIEF-Teacher Form (BRIEF-T), respectively. Means, and standard deviations for the measure of ASD severity (ADI-R total score), parent and teacher measures of ADHD severity (CPRS-R and CTRS-R ADHD Indices), and parent and teacher BRIEF scores are presented in Table 2. Correlations among these variables are presented in Table 3.
Results
Multiple linear regressions were used to assess the association between parent and teacher ratings of EF and parent- and teacher-rated ADHD and ASD symptomology (determined by the ADI-R). The ADHD Index from the CPRS-R was used to estimate severity of ADHD at home, and the ADHD Index from the CTRS-R was used to estimate ADHD severity at school. ASD severity was estimated using the ADI-R Total Score (sum of domain scores). We assessed possible violations of normality of residuals visually using q–q plots and histograms. The residuals for BRIEF showed no meaningful deviation from normality. The variance inflation factor (VIF), a measure of the amount of multicollinearity in a set of multiple regression variables, was low (1.0–1.15), indicating that multicollinearity was not a concern.
Regression results for parent ratings of EF are presented in Table 4, where R2 represents the proportion of variation in the EF scales predicted by the overall model (i.e., combined ASD and ADHD symptom severity), t is the value used to test the significance (i.e., p ≤ .001) of each individual variable’s (i.e., symptom severities) prediction of EF scales. sr2 is the proportion of variance explained by each measure of symptom severity, after controlling for the other. Because of the large number of comparisons involving EF, we set alpha at p = .002 using a Bonferroni Correction. Among parent ratings comparing ADHD and EF indexes on the BRIEF-P, the ADHD index predicted outcomes on all except the Shift and Emotional Control, and Organization of Materials subscales (see Table 4). Interestingly, even the combined effects of ASD and ADHD symptom severity did not significantly account for variability in these three subscales. As seen in Table 4, the proportion of variance explained by ADHD severity, after controlling for ASD severity, ranged from 23 to 53%. Conversely, incremental variance explained by ASD severity was negligible and nonsignificant across all subscales: sr2 < 1% for all BRIEF-P indices and subscales. This is further illustrated in the partial regression plots of Fig. 1. In this figure, the residuals of parent ratings of general, broad based executive functioning (as measured by the BRIEF GEC) are plotted against the residuals of ASD and ADHD severity after removing the linear effects of the other predictor (see Velleman and Welsch 1981). Note that the variable means were added to the residuals for ease of interpretation. From these plots, a clear positive relationship between ADHD symptom severity and EF deficits emerged, whereas there was no relationship between EF and ASD symptoms.

Partial regression plots: parent ratings of BRIEF Global vs. ASD (N.S.) (a) and BRIEF Global vs. ADHD severity (p < 0.001) (b). ADHD severity measured by the CPRS-R ADHD index. ASD severity measured by the ADI-R sum of domain scores. GEC global executive composite
Similar results were found for teacher ratings (see Table 5). Whereas the ADHD index generally predicted BRIEF Teacher ratings (p < .001), ASD severity did not. Once again, the Shift (p = .05; sr2 = 7%) and the Emotional Control subscales (p = .07, sr2 = 6%) were not predicted by ADHD severity. Unlike the case with parent ratings, Organization of Materials was significantly predicted by ADHD severity. Neither Shift nor Emotional Control was significantly predicted by the overall model (i.e., variance explained by combined ASD and ADHD symptom severity). Of variables showing a significant relationship between ADHD and EF, incremental variance explained by ADHD severity ranged from 19 to 36% (see Table 5). Figure 2 displays the partial regression plot of teacher ratings of EF and the predictors, ASD and ADHD severity. Similar to parent ratings, teacher ratings showed a strong positive relationship between EF and ADHD severity, and no relationship between EF and ASD severity.

Partial regression plots of teacher ratings of BRIEF Global vs. ASD (N.S.) (a) and BRIEF Global vs. ADHD severity (p < .001) (b). ADHD severity measured by the CTRS-R ADHD index. ASD severity measured by the ADI-R sum of domain scores. GEC global executive composite
Discussion
To our knowledge, this study is the first to examine EF problems and their relationship with ASD and ADHD symptom severity using both parent and teacher behavior ratings. Thus, we were able to examine EF problems within our sample across environments. In addition, this study was unique by exploring deficits within our ASD sample rather than between children with ASD and other conditions. The benefit of this approach is that it reflected the high comorbidity of ADHD symptoms in children with ASD and included children with a range of ADHD severity in the analyses. Further, it provided insights into what was contributing to problematic EF deficits in children with ASD because we could control for one set of symptoms while examining the relative contribution of the other.
Our analyses found that ASD severity was not significantly related to any parent or teacher ratings of EF. This is inconsistent with previous research, although at least one previous study demonstrated no EF impairment in a substantial proportion (35.8%) of adults with ASD (Johnson et al. 2019). Studies examining differences in EF presentations across diagnostic groups have consistently documented both broad-based EF deficits compared with typically developing children and deficits in shift/flexibility which distinguish children with ASD from other developmental disorders (Gioia et al. 2002; Hovik et al. 2017; Lawson et al. 2015; Semrud-Clikeman et al. 2010). Much of the previous literature utilized both diagnostic group differences and compared proportions of their samples with clinically significant scores, rather than relative severity. However, our findings strongly suggest that the relationship between ADHD symptoms and EF is linear and thus the relationship between them is captured better with dimensional, rather than categorical, measurement. It should also be noted that although all of our children had ASD, there was a wide range of ASD severity in our sample. We conducted an analysis of the dispersion of scores participants received on the ADI-R; and this analysis revealed a range of 23–65 (SD = 10.98). Thus, there was sufficient variability in ASD severity to capture meaningful relationships if they existed.
Because we realize that the ADI-R has not been used extensively as a dimensional measure, we also conducted analyses in which we substituted the SCQ for the ADI-R Total Score as a measurement of ASD symptom severity. The results replicated our results using the ADI-R across parent and teacher ratings of EF. This finding suggests that our results were not an artifact of the difference in type of measurement (i.e., ADI-R total score versus SCQ score).
In terms of ADHD severity, we found that parent ratings were related to EF in the home for all measures except the BRIEF-P Shift, Emotional Control, and Organization of Materials subscales. Similarly, teacher ratings of the severity of ADHD symptoms were related to impaired EF in the classroom for all but two BRIEF-T subscales (i.e., Shift and Emotional Control). Our findings are thus consistent with previous research on EF in school-aged children diagnosed with ADHD. This has found that children with ADHD typically present with broad-based EF deficits, particularly inhibition and EF skills subsumed under Metacognition, but excluding the Shift and Emotional Control subscales (Gioia et al. 2002). Visual examination of Shift and Emotional Control scores revealed good dispersion of scores within our sample. This indicates that the lack of any relationship for Shift and Emotional Control with ADHD symptoms was not simply due to a lack of variability in scores. Thus, unlike other areas of EF, increased severity of ADHD symptoms was not characterized by increased problems with flexibility and not related to difficulty with emotional control. Our findings demonstrated remarkably consistent results across parent and teacher ratings. However, the relationship between Organization of Materials and ADHD severity was not replicated across parent and teacher ratings. Only teacher ratings showed that increased ADHD severity predicted poorer orderliness of workspace and materials. This relationship between ADHD and organization is consistent with previous research on parent (Gioia et al. 2002; Hovik et al. 2017; and Semrud-Clikeman et al. 2010) and teacher (Alloway et al. 2009) ratings of EF. The fact that it was not found for parent ratings may indicate that the types of organizational skills most relevant and sensitive to such a relationship are more cognitive in nature. Whereas parents may monitor their children’s organization in work, play, and storage spaces this may be qualitatively different from teacher perceptions of organizing cognitive tasks.
One issue that arises in this study relates to the possibility that the associations between EF and ADHD severity were due to “source variance” or common-method variance, a phenomenon in which relationships are due to the measurement method rather than to true relationships among the variables under study (Podsakoff et al. 2003). Indeed, the sources of data in this study were parents and teachers in all instances. However, it is important to bear in mind that the pattern of outcomes was completely different between the ADHD severity comparisons and the ASD severity outcomes, arguing against common-method variance as the explanation. There was consistency between parents and teachers for significance on 10 of 11 EF scales where ADHD severity was the outcome of interest (missing complete agreement on only Organization of Materials, which was significant for teachers but barely missed our .002 Bonferonni correction level). Thus, we suggest that the consistently positive outcomes between informants for ADHD severity on the one hand and the consistently negative outcomes for ASD severity on the other is compelling evidence that source variance does not account for the findings.
It is also interesting to note that EF deficits were related to ADHD symptoms—and that EF deficits have been successfully treated using stimulant medication in children with ADHD who do not have ASD (Everett et al. 1991; Gau and Shang 2010; Hale et al. 2011; Kempton et al. 1999; Rapoport et al. 1980; Tannock et al. 1995; van Stralen et al. 2020; Vance et al. 2003). As EF deficits are closely tied to ADHD symptoms in children with ASD, stimulant treatment may prove effective in treating EF deficits in children with ASD who also have significant ADHD symptoms. Cognitive performance (inattention, inhibition), and behavioral measures related to inattention, can be effectively treated in children with ASD+ADHD (Howes et al. 2018; Pearson et al. 2013; Pearson et al. 2020; Sturman et al. 2017). It is possible that stimulant treatment can also improve EF in the domains tapped by the BRIEF-P and BRIEF-T. Thus, the potential enhancement of EF via stimulant intervention is an area that deserves investigation—especially given that EF deficits significantly undermine a child’s ability to function in day-to-day life—and that these impairments increase from childhood to late adolescence, when older adolescents/young adults with ASD are preparing to enter the job market.
Limitations
As our participants only included children with full-scale IQs greater than or equal to 70, these results may not generalize to children with ASD and accompanying intellectual impairment. We also realize that most of our sample of children with ASD had ADHD, and that it would have been optimal if we could have recruited an equal number of children with ASD who did not have ADHD. Although we originally hoped to recruit two equal-sized groups of children (one with ASD+ADHD, and another with ASD but without ADHD), as recruitment proceeded, we found that it was very difficult to locate children in the latter group—a finding that reflects the growing knowledge regarding the high comorbidity between ASD and ADHD. This issue clearly warrants further exploration in future studies with larger samples.
Further, as is typical with ASD research, our sample was mostly male and largely Caucasian. Therefore, our results may not generalize to samples that are more diverse. Further, the females in the study showed little variability in diagnosis and presentation; all were diagnosed with ADHD. However, our data analytic techniques did not examine ADHD as a group diagnosis, but analyzed ADHD symptom severity across the entire sample.
Future researchers should consider examining whether intervention for ADHD (e.g., medication) not only improves EF, but whether enhanced EF in children with ASD leads to improvement in social skills, adaptive behavior, achievement, and other psychopathology. This could provide important information for the treatment of school-aged children with ASD.
Conclusion
Our results suggest that most BRIEF subscales show a correspondence between ADHD severity and EF. However, Shift and Emotional Control seem to be unrelated to either ASD or ADHD symptom severity, both at home and at school. Further research is needed to verify this pattern. If the relationships found here hold true, intervention which effectively targets ADHD symptoms may be helpful for improving EF skills in children with ASD. Future studies should explore possible intervention techniques that would be helpful for children with ASD who have significant ADHD symptoms.
References
Alloway, T. P., Gathercole, S. E., Holmes, J., Place, M., Elliott, J. G., & Hilton, K. (2009). The diagnostic utility of behavioral checklists in identifying children with ADHD and children with working memory deficits. Child Psychiatry and Human Development, 40(3), 353–366. https://doi.org/10.1007/s10578-009-0131-3.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121(1), 65. https://doi.org/10.1037/0033-2909.121.1.65.
Blijd-Hoogewys, E. M. A., Bezemer, M. L., & van Geert, P. L. C. (2014). Executive functioning in children with ASD: An analysis of the BRIEF. Journal of Autism and Developmental Disabilities, 44, 3089–3100. https://doi.org/10.1007/s10803-014-2176-9.
Conners, C. K. (1997). Conners’ Parent Rating Scale-Revised (L). North Tonawanda, NY: Multi-Health Systems.
Corbett, B. A., Constantine, L. J., Hendren, R., Rocke, D., & Ozonoff, S. (2009). Examining executive functioning in children with autism spectrum disorder, attention deficit hyperactivity disorder and typical development. Psychiatry Research, 166(2–3), 210–222. https://doi.org/10.1016/j.psychres.2008.02.005.
Craig, F., Margari, F., Legrottaglie, A. R., Palumbi, R., De Giambattista, C., & Margari, L. (2016). A review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiatric Disease and Treatment, 12, 1191–1202. https://doi.org/10.2147/NDT.S104620.
Danielsson, H., Henry, L., Messer, D., & Rönnberg, J. (2012). Strengths and weaknesses in executive functioning in children with intellectual disability. Journal of Research in Developmental Disabilities, 2(33), 600–607. https://doi.org/10.1016/j.ridd.2011.11.004.
Demetriou, E. A., Lampit, A., Quintana, D. S., Naismith, S. L., Song, Y. J. C., Pye, J. E., et al. (2018). Autism spectrum disorders: A meta-analysis of executive function. Molecular Psychiatry, 23, 1198–1204. https://doi.org/10.1038/mp.2017.75.
Everett, J., Thomas, J., Cote, F., Levesque, J., & Michaud, D. (1991). Cognitive effects of psychostimulant medication in hyperactive children. Child Psychiatry and Human Development, 22(2), 79–87. https://doi.org/10.1007/BF00707786.
Gau, S. S. F., & Shang, C. Y. (2010). Improvement of executive functions in boys with attention deficit hyperactivity disorder: An open-label follow-up study with once-daily atomoxetine. International Journal of Neuropsychopharmacology, 13(2), 243–256. https://doi.org/10.1017/S1461145709990836.
Geurts, H. M., Verté, S., Oosterlaan, J., Roeyers, H., & Sergeant, J. A. (2004). How specific are executive functioning deficits in attention deficit hyperactivity disorder and autism? Journal of Child Psychology and Psychiatry, 45(4), 836–854. https://doi.org/10.1111/j.1469-7610.2004.00276.x.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000a). TEST REVIEW behavior rating inventory of executive function. Child Neuropsychology, 6, 235–238. https://doi.org/10.1076/chin.6.3.235.3152.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000b). BRIEF Behavior rating inventory of executive function: Professional manual. Lutz: Psychological Assessment Resources.
Gioia, G. A., Isquith, P. K., Kenworthy, L., & Barton, R. M. (2002). Profiles of everyday executive function in acquired and developmental disorders. Child Neuropsychology, 8(2), 121–137. https://doi.org/10.1076/chin.8.2.121.8727.
Goldberg, M. C., Mostofsky, S. H., Cutting, L. E., Mahone, E. M., Astor, B. C., Denckla, M. B., et al. (2005). Subtle executive impairment in children with autism and children with ADHD. Journal of Autism and Developmental Disorders, 35(3), 279–293. https://doi.org/10.1007/s10803-005-3291-4.
Granader, Y., Wallace, G. L., Hardey, K. K., Yerys, B. E., Lawson, R. A., Rosenthal, M., et al. (2014). Characterizing the factor structure of parent reported executive function in autism spectrum disorders: The impact of cognitive inflexibility. Journal of Autism and Developmental Disorder, 44(12), 3056–3062. https://doi.org/10.1007/s10803-014-2169-8.
Hale, J. B., Reddy, L. A., Semrud-Clikeman, M., Hain, L. A., Whitaker, J., Morley, J., et al. (2011). Executive impairment determines ADHD medication response: Implications for academic achievement. Journal of Learning Disabilities, 44(2), 196–212. https://doi.org/10.1177/0022219410391191.
Happe, F., Booth, R., Charlton, R., & Hughes, C. (2006). Executive function deficits in autism spectrum disorders and attention-deficit/hyperactivity disorder: Examining profiles across domains and ages. Brain and Cognition, 61(1), 25–39. https://doi.org/10.1016/j.bandc.2006.03.004.
Hovik, K. T., Egeland, J., Isquith, P. K., Gioia, G., Skogli, E. W., Andersen, P. N., et al. (2017). Distinct patterns of everyday executive function problems distinguish children with Tourette syndrome from children with ADHD or autism spectrum disorders. Journal of Attention Disorders, 21(10), 811–823. https://doi.org/10.1177/1087054714550336.
Howes, O. D., Rogdaki, M., Findon, J. L., Wichers, R. H., Charman, T., King, B. H., et al. (2018). Autism spectrum disorder: Consensus guidelines on assessment, treatment, and research from the British Association for Psychopharmacology. Journal of Psychopharmacology, 32(1), 3–29. https://doi.org/10.1177/0269881117741766.
John, T. S., Dawson, G., & Estes, A. (2018). Brief report: Executive function as a predictor of academic achievement in school-age children with ASD. Journal of Autism and Developmental Disabilities, 48(1), 276–283. https://doi.org/10.1007/s10803-017-3296-9.
Johnson, K., Murray, K., Spain, D., Walker, I., & Russell, A. (2019). Executive function: Cognition and behaviour in adults with autism spectrum disorders (ASD). Journal of Autism and Developmental Disorders, 49(10), 4181–4192. https://doi.org/10.1007/s10803-019-04133-7.
Kempton, S., Vance, A., Maruff, P., Luk, E., Costin, J., & Pantelis, C. (1999). Executive function and attention deficit hyperactivity disorder: Stimulant medication and better executive function performance in children. Psychological Medicine, 29(3), 527–538. https://doi.org/10.1017/S0033291799008338.
Lawson, R. A., Papadakis, A. A., Higginson, C. I., Barnett, J. E., Wills, M. C., Strang, J. F., et al. (2015). Everyday executive function impairments predict comorbid psychopathology in autism spectrum and attention deficit hyperactivity disorders. Neuropsychology, 29(3), 445. https://doi.org/10.1037/neu0000145.
Lefort-Besnard, J., Vogeley, K., Schilbach, L., Varoquaux, G., Thirion, B., Dumas, G., et al. (2020). Patterns of autism symptoms: Hidden structure in the ADOS and ADI-R instruments. Translational Psychiatry, 10, 257. https://doi.org/10.1038/s41398-020-00946-8.
Leitner, Y. (2014). The co-occurrence of autism and attention deficit hyperactivity disorder in children—What do we know? Frontiers in Human Neuroscience, 8, 268. https://doi.org/10.3389/fnhum.2014.00268.
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (2001). Autism Diagnostic Observation Schedule-WPS Edition (ADOS-WPS). Los Angeles: Western Psychological Services.
Loveland, K. (2005). Social-emotional impairment and self-regulation in autism spectrum disorders. In J. Nadel & D. Muir (Eds.), Typical and impaired emotional development (pp. 365–382). Oxford: Oxford University Press.
Mansour, R., Dovi, A. T., Lane, D. M., Loveland, K. A., & Pearson, D. A. (2017a). ADHD severity as it relates to comorbid psychiatric symptomatology in children with autism spectrum disorders (ASD). Research in Developmental Disabilities, 60, 52–64.
Mansour, R, Ward A. R., Lane, D. M, Loveland, K. A, Aman, M. G., Jerger, S., et al. ADHD Severity as a predictor of cognitive task performance in children with autism spectrum disorder. Research in Developmental Disabilities (in press).
Ng, R., Heinrich, K., & Hodges, E. K. (2019). Brief report: Neuropsychological testing and informant-ratings of children with autism spectrum disorder, attention-deficit/hyperactivity disorder, or comorbid diagnosis. Journal of Autism and Developmental Disorders, 49, 2589–2596. https://doi.org/10.1007/s10803-019-03986-2.
Ozonoff, S., & Jensen, J. (1999). Brief report: Specific executive function profiles in three neurodevelopmental disorders. Journal of Autism Developmental Disorders, 29, 171–177. https://doi.org/10.1023/A:1023052913110.
Pearson, D. A., Aman, M. G., Arnold , L. E., Lane, D. M., Loveland, K. A., Santos, C. W., et al. (2012). High concordance of parent and teacher ADHD ratings in medicated and unmedicated children with autism spectrum disorders. Journal of Child and Adolescent Psychopharmacology, 22, 284–291. https://doi.org/10.1089/cap.2011.0067.
Pearson, D. A., Loveland, K. A., Lachar, D., Lane, D. M., Reddoch, S. L., Mansour, R., et al. ( (2006). A comparison of behavioral and emotional functioning in children and adolescents with autistic disorder and PDD-NOS. Child Neuropsychology, 12, 321–333. https://doi.org/10.1080/09297040600646847.
Pearson, D. A., Santos, C. W., Aman, M. G., Arnold, L. E., Casat, C. D., Mansour, R., et al. (2013). Effects of extended release methylphenidate treatment on ratings of attention-deficit/hyperactivity disorder (ADHD) and associated behavior in children with autism spectrum disorders and ADHD symptoms. Journal of Child and Adolescent Psychopharmacology, 23(5), 337–351. https://doi.org/10.1089/cap.2012.0096.
Pearson, D. A., Santos, C. W., Aman, M. G., Arnold, L. E., Lane, D. M., Loveland, K. A., et al. (2020). Effects of extended release methylphenidate treatment on cognitive task performance in children with autism spectrum disorder and ADHD. Journal of Child and Adolescent Psychopharmacology, 30(7), 414–426. https://doi.org/10.1089/cap.2020.0004
Podsakoff, P. M., MacKenzie, S. B., Lee, J.-Y., & Podsakoff, N. P. (October 2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology., 88(5), 879–903. https://doi.org/10.1037/0021-9010.88.5.879.
Rapoport, J. L., Buchsbaum, M. S., Weingartner, H., Zahn, T. P., Ludlow, C., & Mikkelsen, E. J. (1980). Dextroamphetamine: Its cognitive and behavioral effects in normal and hyperactive boys and normal men. Archives of General Psychiatry, 37(8), 933–943. https://doi.org/10.1001/archpsyc.1980.01780210091010.
Reich, W. (2000). Diagnostic interview for children and adolescents (DICA). Journal of the American Academy of Child & Adolescent Psychiatry, 39(1), 59–66. https://doi.org/10.1097/00004583-200001000-00017.
Reich, W., Welner, Z., & Herjanic, B. (1997). Diagnostic interview for children and adolescents-IV (DICA-IV). New York: Multi-Health Systems Incorporated.
Roid, G. H. (2003). Stanford-Binet Intelligence Scales, fifth edition (SB:V). Itasca: Riverside Publishing.
Rosenthal, M., Wallace, G. L., Lawson, R., Will, M. C., Dixon, E., Yerys, B. F., et al. (2013). Impairments in real world executive function increase from childhood to adolescence in autism spectrum disorders. Neuropsychology, 27(1), 13–18. https://doi.org/10.1037/a0031299.
Rutter, M., Bailey, A., & Lord, C. (2003a). Manual for the social communication questionnaire. Los Angeles: Psychological Services.
Rutter, M., Le Couteur, A., & Lord, C. (2003b). ADI-R: Autism diagnostic interview revised. Manual. Los Angeles: Western Psychological Services.
Semrud-Clikeman, M., Walkowiak, J., Wilkinson, A., & Butcher, B. (2010). Executive functioning in children with Asperger syndrome, ADHD-combined type, ADHD-predominately inattentive type, and controls. Journal of Autism and Developmental Disorders, 40(8), 1017–1027. https://doi.org/10.1007/s10803-010-0951-9.
Sergeant, J. A., Geurts, H., & Oosterlaan, J. (2002). How specific is a deficit of executive functioning for attention-deficit/hyperactivity disorder? Behavioral Brain Research, 130, 3–28. https://doi.org/10.1016/S0166-4328(01)00430-2.
Sturman, N., Deckx, L., & van Driel, M. L. (2017). Methylphenidate for children and adolescents with autism spectrum disorder. Cochrane Database of Systematic Reviews, 11(11), CD011144. https://doi.org/10.1002/14651858.CD011144.pub2.
Tannock, R., Ickowicz, A., & Schachar, R. (1995). Differential effects of methylphenidate on working memory in ADHD children with and without comorbid anxiety. Journal of the American Academy of Child & Adolescent Psychiatry, 34(7), 886–896. https://doi.org/10.1097/00004583-199507000-00012.
Van Eylen, L., Boets, B., Steyaert, J., Wagemans, J., & Noems, I. (2015). Executive functioning in autism spectrum disorders: Influence of task and sample characteristics and relation to symptom severity. European Child and Adolescent Psychiatry, 24(11), 1399–1417. https://doi.org/10.1007/s00787-015-0689-1.
van Stralen, J. P. M. (2020). A controlled trial of extended-release guanfacine and psychostimulants on executive function and ADHD. Journal of Attention Disorders, 24(2), 318–325. https://doi.org/10.1177/1087054717751197.
Vance, A. L., Maruff, P., & Barnett, R. (2003). Attention deficit hyperactivity disorder, combined type: Better executive function performance with longer-term psychostimulant medication. Australian & New Zealand Journal of Psychiatry, 37(5), 570–576. https://doi.org/10.1046/j.1440-1614.2003.01238.x.
Velleman, P. F., & Welsch, R. E. (1981). Efficient computing of regression diagnostics. The American Statistician, 35, 234–242.
Acknowledgments
This study was funded by Grant Number MH072263 from the National Institute of Mental Health (NIMH). Preliminary versions of this paper were presented at the American Academy of Child and Adolescent Psychiatry (AACAP) 56th Annual Meeting in Chicago, IL, October 30, 2008 and at the 8th Annual International Meeting for Autism Research (IMFAR) in Chicago, IL, May 7, 2009. The authors wish to express their appreciation to the children, parents, and teachers who participated in this study.
Author information
Authors and Affiliations
Contributions
All authors were involved in writing this manuscript. Drs. Pearson, Aman, and Loveland were involved in the conceptualization and methodology of the project. Dr. Pearson, Dr. Loveland, and Ms. Mansour were involved in investigation (i.e., conducting the research, collecting the data). Dr. Lane, Dr. Lee, Dr. Ward, and Ms. Mansour were involved in data analysis and visualization (preparation of figures). Dr. Pearson was responsible for project administration and funding acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Dr. Pearson has received travel reimbursement and research support from Curemark LLC; research support from Biomarin and Novartis, and has served as a consultant to Curemark LLC. Ms. Mansour have received research support from Curemark LLC. Dr. Aman has received research contracts, consulted with, served on advisory boards, or done investigator training for J & J Pharmaceuticals; Ovid Therapeutics; Hoffmann-La Roche; Supernus Pharmaceuticals, and Zynerba Pharmaceuticals. He receives royalties from Slosson Educational Publications. The other authors report no biomedical financial interests or potential conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lee, R.R., Ward, A.R., Lane, D.M. et al. Executive Function in Autism: Association with ADHD and ASD Symptoms. J Autism Dev Disord 53, 688–700 (2023). https://doi.org/10.1007/s10803-020-04852-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04852-2