
Abstract
Individuals with autism are at heightened risk for experiencing suicidality compared to those without autism. Despite this, it is unknown what tools are used to assess suicide risk in research and clinical practice among children and youth with autism. This systematic review examined tools commonly used to measure suicidality in children and youth with and without autism spectrum disorder. Four databases were searched. We identified five tools (C-SSRS, PSS, SITBI, SIQ-JR, BSS) commonly used with youth in the general population; however, we did not identify any tools that were commonly used autistic children and youth. Results highlight the lack of available tools utilized to measure suicidality in autistic children and youth. We propose a framework to facilitate research to fill this gap.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Suicidality (suicidal thoughts and behaviours) is exceptionally common and often overlooked in individuals with autism spectrum disorder (ASD), affecting upwards of 66% of individuals (Cassidy et al. 2014, 2018a, b; Cassidy and Rodgers 2017). Importantly, individuals with ASD are more likely to die by suicide, with the risk of death by suicide being seven times higher in individuals with ASD than the general population (Hirvikoski et al. 2016). Currently, no commonly used or validated suicide risk assessment measures exist for adults with ASD (Cassidy et al. 2018a, b), which can result in inappropriate and ineffective diagnosis (Au-Yeung et al. 2018). Untreated suicidal behaviour can lead to crisis (White et al. 2012), emergency room visits (Durbin et al. 2018), and inpatient hospitalizations along with significant and lifelong mental health difficulties (Leyfer et al. 2006), decreased quality of life for the youth and their family, and a heavy financial burden for individuals, government, and wider society. Not only are valid instruments necessary for clinical practice, they are essential for future research studies aiming to better understand and prevent suicide in autistic people. This includes identifying risk and protective factors, determining accurate prevalence rates, and evaluating the effectiveness of intervention approaches and prevention strategies of suicidality in this vulnerable population.
ASD is a neurodevelopmental disorder that is characterized by difficulties in social communication and repetitive and rigid behaviour (American Psychiatric Association, APA 2013). In addition to these core symptoms, individuals with ASD often experience many secondary conditions, including intellectual disability, sensory difficulties, deficits in academic and daily functioning, and most importantly, individuals with ASD often experience co-occurring psychiatric disorders. For example, approximately 70% of youth with ASD experience mental health issues (Lever and Geurts 2016), with 40–50% of adolescents with ASD meeting diagnostic criteria for two or more psychiatric conditions (Reaven and Wainer 2015). Internalizing mental health issues, such as anxiety and depression, are the most common. Mental health issues in youth with neurodevelopmental disorders (NDDs) can cause debilitating distress and significantly interfere with children’s daily functioning and quality of life (Baraskewich and McMorris 2019).
In the last decade, it has become alarmingly apparent that individuals with ASD experience suicidal thoughts and behaviours far more than the general population. Estimates of suicidality in children and youth with ASD have ranged from 10.9 to 50%, depending on the type of assessment measure used (Segers and Rawana 2014). Individuals with ASD comprise 7–15% of suicidal patients in the general population (Sharpley et al. 2016). Similar rates of suicidality have been found in children and youth with ASD based on parent reports (Horowitz et al. 2017) and diagnostic interviews with youth (Demirkaya and Tutkunkardaz 2016). Approximately 14% of caregivers of children and youth with ASD reported that their child ‘sometimes’ to ‘very often’ experienced suicidal ideation or behaviour, which was substantially more than children without ASD (Dickerson Mayes et al. 2013). Most importantly, suicidality is not only extremely prevalent in children and youth with ASD, but suicidality was identified as a significant contributor to premature mortality in adults with ASD (Hirvikoski et al. 2016).
Little is known about why suicidal behaviour occurs for a sizable proportion of individuals with ASD (66% reporting suicidal ideation and 35% have attempted suicide; Cassidy et al. 2014). Emerging research suggests that individuals with ASD exhibit risk factors for suicidal behaviour that are inherent to their diagnosis (impulsivity, deficits in executive functioning; Baraskewich and McMorris 2019; Chen et al. 2017), as well as risk factors that pertain to the general population (e.g., presence of co-occurring mental health issues, peer victimization, and adverse childhood experiences; Cassidy et al. 2018a, b; Horowitz et al. 2017). More specifically, there is overwhelming evidence to suggest that the presence of mental health issues is a significant risk factor for suicidality in adults with ASD (Cassidy et al. 2014; Dickerson Mayes et al. 2013; Horowitz et al. 2017; Kato et al. 2013). Similarly, physical or sexual abuse, mood dysregulation, impulsivity, and peer victimization have also been shown to be predictive of suicidal behaviour (Agosti et al. 2011; Dickerson Mayes et al. 2013). Suicidal behaviour is also related to IQ, with those individuals with higher IQs experiencing more suicidal behaviours (e.g., Segers and Rawana 2014).
Although it is well established that suicidality is alarmingly common in children and youth with ASD, to date, it is unknown if assessment tools created for children and youth in the general population, are valid and reliable for use in children and youth with ASD. Recently, using three databases, Cassidy et al. (2018a, b) conducted a systematic review to identify valid and reliable tools that assess for suicidality in adults with and without ASD. A robust research tool (COSMIN) was utilized to synthesize the evidence, efficacy, and utility of each measure. Three commonly used assessment measures with strong psychometric properties were identified through their systematic search: The Suicide Behaviour Questionnaire-Revised (SBQ-R), the Beck Scale for Suicidal Ideation (BSS), and the Columbia Suicide Severity Rating Scale (C-SSRS). Additionally, they identified only one measure, the C-SSRS that has moderate evidence in support of predicting future suicide attempts in research and clinical practice in non-autistic adults. While a number of studies have explored suicidality in adults with ASD, none have utilized a validated tool, and no tool has yet been developed to assess suicidality in autistic adults. These researchers highlight the need for future research to examine the measurement properties of these robust tools developed for the general population, in individuals with ASD.
While Cassidy et al. (2018b) found that no tool has been validated for use in autistic adults most of the existing tools had moderate support for psychometric properties. To date, it is unknown if this is the case in autistic children and youth, that is, it is plausible that the tools designed for children and youth in the general population will have the same utility and psychometric properties in autistic children and youth. However, it is also quite possible that given developmental difficulties often associated with ASD, such as alexithymia, difficulties in executive function, and self-awareness of mental states and emotions, that existing tools may need to be adapted for use in autistic children and youth to ensure we are accurately assessing for suicidal thoughts and behaviours.
Lack of evidence and gaps in knowledge are significant barriers to accurately assessing for risk of suicide in individuals with ASD (Horowitz et al. 2017). Individuals with ASD have been systematically excluded from studies examining the validity of suicide risk screening measures, due to cognitive limitations and difficulties with awareness (Horowitz et al. 2017). Similarly, it is unknown how suicidal thoughts are expressed in this population, and how they may be similar or different from individuals without ASD (Horowitz et al. 2017). Lastly, deficits inherent to autistic individuals, such as communication challenges, impulsivity, dysfunctional emotional awareness (alexithymia), differentiating special interests on topics of morbidity from reliable thoughts of death, and challenges in understanding the finality of death, make effectively and accurately detecting suicide extremely challenging (Cassidy and Rodgers 2017). Taken together, it is unknown how to accurately assess and determine the degree of risk in this vulnerable population.
The present study aimed to extend Cassidy et al.’s (2018a, b) study of suicidality in adults with ASD to systematically examine the suicide assessment tools used in research or clinical practice with children and youth. Specifically, we aimed to: (1) identify measures commonly used to assess suicidality in children and youth in the general population, as well as in children and youth with ASD; and (2) provide recommendations for further research in this area. Identifying valid assessment tools is essential for treating suicidal ideation and behaviours, as well as preventing premature death in children and youth with ASD. Further, it is essential to identify valid assessment tools for use in future research studies aimed at understanding underlying mechanisms, exploring sensitivity to change in intervention studies, and in the development of prevention approaches.
Methods
Literature Search
A systematic literature search was conducted using the following bibliographic databases: PsycINFO, Medline, Embase, and Web of Knowledge. The Cochrane Library was also searched to confirm that no other systematic reviews of the current study topic existed. Each search was carried out from inception until May 20, 2019 using relevant controlled vocabulary and key terms related to suicidality measures used with children and youth under the age of 21. Dates were not restricted for the purpose of this study in order to ensure that all possible tools to assess suicidal thoughts and behaviours in children and youth within both populations of interest were included. Searches were carried out for (1) children and youth with ASD, and (2) the general population of children and youth. The terms for each search strategy are included in Table 1.
Selection Criteria
Across all databases, searches were restricted to articles written in the English language and published in peer-reviewed journals. We focused on studies utilizing tools to assess both the prevalence of suicidality and suicide-related outcomes (e.g., treatment and intervention) among children and youth. Tools specifically assessing suicidality among children and youth, including assessment of suicidal intent, were operationalized clinically in accordance with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (APA 2013) and the International Classification of Diseases and Related Health Problems (ICD-11, World Health Organization 2018). In order to capture information related to indicators of risk for suicide such as frequency, intensity, and duration of current and lifetime symptoms, included studies were required to focus on a tool specifically assessing risk for suicidality, rather than self-harm or non-suicidal self-injury (NSSI) more broadly, for three reasons. First, this approach was utilized to be consistent with previous similar reviews (Cassidy et al. 2018a, b), in which studies were only included if they utilized tools with suicide-related items or adapted subscales from a larger measure were excluded. Second, while self-harm and non-suicidal self-injury (NSSI) are commonly seen in individuals with ASD, currently the nature of this self-harm is conceptualized as being fundamentally different than self-injury or NSSI than what is seen in the general population. For example, self-injurious behaviour, such as head banging and biting the self are common behaviours exhibited by some autistic individuals. These symptoms are often conceptualized as a repetitive rigid behaviour, or a way for autistic individuals to self-stimulate, whereas NSSI, such as cutting or burning, are understood to function as a way to cope with overwhelming emotions. Given the infancy of the existing literature, risk assessment tools have yet to make this distinction, thus making it challenging to delineate the differences between these two ‘types’ of self-injury. Lastly, no research has explored whether persons with ASD who present with self-injurious behaviour are experiencing suicidal thoughts or behaviours (Hannon and Taylor 2013).
General Population Selection Criteria
To ensure that the tools used were likely to be appropriate for use in a pediatric or adolescent population, studies were included if data from children and youth (i.e., under 21 years of age) comprised at least 50% of the total sample. Age of the sample was determined by examining the range of participant ages and ensuring that they fell within our criteria. If the study included participants over the age of 21, the study was included if the mean age of the sample was lower than 21. Although studies that involved an ASD comparison group were not included in the general population search, they were considered for inclusion in the ASD search. Some studies assessed for suicidality in a unique population (e.g., LGBTQ youth, juvenile offenders, trauma victims, etc.). These articles were included with the caveat that the prevalence of suicidality tends to be higher in these populations (e.g., Haas et al. 2011; Krysinska and Lester 2010; Teplin et al. 2017). We also chose to include studies that recruited from a psychiatric sample (e.g., patients currently receiving treatment for a mental health issue), but excluded studies that focused on groups with a particular condition (e.g., persons with co-occurring intellectual disability, patients being treated for psychosis, etc.) to ensure the tool would likely be useful for assessing suicidality in the general population rather than in those comprising a specific diagnostic category.
ASD Population Selection Criteria
The current study focused on literature pertaining to children and youth with a primary diagnosis of ASD, or acceptable equivalent to ASD [e.g., pervasive developmental disorder (PDD) or Asperger syndrome (AS)]. Diagnostic codes consistent with previous versions of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR, APA 2000) or International Classification of Diseases and Related Health Problems (ICD 9 or 10) were included. Additionally, studies were included if data from the ASD population of children and youth, without any co-occurring conditions, comprised at least 50% of the sample with an ASD (or equivalent) diagnosis.
Data Extraction
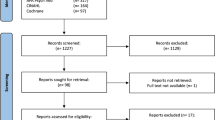
The electronic search was conducted independently by two authors (S.H. and K.H.), and supplemented by a manual review of reference lists from eligible publications and relevant reviews. Data pertaining to population characteristics, tools used, study type, and domains captured were recorded. A full-text review of the articles was then conducted by two authors (S.H. and K.H.), and any ambiguous articles were then discussed with a third author (C.M.) in order to reach consensus prior to analysis. From these selected articles, the authors examined the tools used in each study to assess for suicidality. Given that the primary objective of the current study was to identify commonly used tools, if a tool was used only once, it was eliminated from further discussion. “Commonly used” was operationalized as at least two (or more) reported uses evident in the literature. This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al. 2009). Figure 1 outlines the study selection process, and reasons for study inclusion and exclusion, for the purpose of this review.

PRISMA diagram results. Suicidality among children and youth with and without autism spectrum disorder: a systematic review of existing risk assessment tools
Results
Search Results
Children and Youth in the General Population
The search for studies utilizing tools to assess for suicidality in children and youth in the general population identified 1021 articles (after duplicates removed). After screening article titles and abstracts, 90 were selected for full-text review. Further examination of these articles revealed a total of 15 that met our selection criteria. Characteristics of these studies are provided in Table 2.
Of note, the majority of the studies screened and excluded from the final list of articles did not meet our inclusion criteria as they used a single-item to assess for suicidality. Many of these were items taken from tools that assess/screen for general psychopathology [e.g., the Youth Self-Report Questionnaire (YSR; Achenbach 1991a), Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS; Kaufman et al. 1997), Child Behaviour Checklist (CBCL; Achenbach 1991b), and the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID; Sheehan et al. 2010), etc.] or specific mental health disorders, such as depression [Children’s Depression Inventory (CDI; Kovacs 2010)]. In accordance with a similar search strategy used in previous studies (Wigham and McConachie 2014), these were excluded in order to focus on measures of broader conceptualizations of suicidality that simply cannot be captured by a single item or subscale (e.g., severity and frequency of suicidal thoughts and behaviours, suicide risk, etc.).
Nearly 6000 (N = 5766) participants were included in the general population studies reviewed, with sample sizes ranging from 36 (Czyz et al. 2019) to 1588 (Francesca-Pedrero et al. 2018). All studies, with the exception of one that focused on a sample of juvenile offenders (Penn et al. 2003), included more females than males (see Table 2). All studies examined adolescents and young adults with age ranges between 12 and 19 years of age. No studies examined suicidality in children younger than 12.
Sample characteristics varied substantially in terms of where participants were recruited. Five studies (Czyz et al. 2019; Kennard et al. 2018; McCauley et al. 2018; Malagama et al. 2018; Posner et al. 2011) recruited adolescents that were hospitalized or admitted into psychiatric treatment due to recent suicide attempt, suicidal ideation, or high suicide risk. Five studies (Glenn et al. 2016, 2019; Ordaz et al. 2018; Stewart et al. 2017; Vergara et al. 2019) gathered their participants from adolescents currently receiving inpatient or outpatient treatment for a mental health disorder, including mood and anxiety disorders. Four studies (Horvath et al. 2018; Kahn et al. 2015; Francesca-Pedrero et al. 2018; Muehlenkamp and Gutierrez 2004) utilized community samples (e.g. high school students), and one study utilized a sample of juvenile offenders admitted to a correctional facility (Penn et al. 2003).
Ten different tools were used to assess suicidality in the selected general population studies. Six of these were clinician-administered interviews. These included the Columbia-Suicide Severity Rating Scale (C-SSRS; Posner et al. 2011), the Paykel Suicide Scale (PSS; Paykel et al. 1974), the Self-Injurious Thoughts and Behaviors Interview (SITBI; Nock et al. 2007), the Adolescent Suicide Assessment Protocol-20 (ASAP-20; Fremouw et al. 2009), the Scale for Suicidal Ideation (SSI; Beck et al. 1999), and the Suicide Attempt Self-Injury Interview (SASII; Linehan et al. 2006). The remaining four tools identified were self-report questionnaires. These included the Suicidal Ideation Questionnaire-Junior High Version (SIQ-JR; Reynolds 1988), the Multi-Attitude Suicide Tendency Scale (MAST; Orbach et al. 1991), the Spectrum of Suicidal Behavior Scale (SSBS; Pfeffer 1986), and Beck’s Scale for Suicidal Ideation (BSS; Beck et al. 1979). Five of these 10 tools, including the ASAP-20, SASII, MAST, SSBS, and SSI, were not considered to be commonly used according to our operational definition (i.e., utilized in two or more studies); and were therefore eliminated from further consideration. Consequently, five tools (C-SSRS, PSS, SITBI, SIQ-JR, SSI) were considered for the purpose of the present study.
Children and Youth with ASD
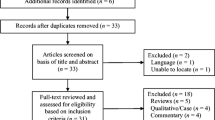
The search for studies utilizing tools to assess for suicidality in children and youth with ASD identified a total of 672 articles. After screening article titles and abstracts for relevance, six were selected for full-text review. Of these, two met inclusion criteria. While the general population search identified studies that assessed for suicidality using only a single item, the ASD search often identified articles that didn’t assess for suicidality at all. Many looked at self-injurious behaviours (e.g. head banging), which were not specified to include thoughts and behaviours related to a wish to end one’s life. Similar to the general population search, several studies also utilized items or subscales from broader measures of mental health or created their own items for the purposes of their study with no evidence of reliability or validity.
The sample sizes of the two selected studies were considerably smaller, with a combined total of 65 participants (n = 10; Demirkaya and Tutkunkardaz 2016 and n = 55; Shtayermman 2008). Approximately 90% of both samples were male. Shtayermman (2008) recruited adolescents with Asperger’s syndrome and their parent(s) to participate in the study through websites and snowball sampling. The age range of their sample was not reported but participants had a mean age of 19.7 (SD = 3.0). Demirkaya and Tutkunkardaz (2016) recruited autistic adolescents aged 7–20 years (M = 13.56, SD = 2.9) without co-occurring intellectual disability through an autism clinic. Characteristics of these studies are summarized in Table 3. These studies used the Eskin’s Suicide Screening Questionnaire (1995) and the SIQ (Reynolds 1988) as tools to measure suicidality among their samples. Both of these tools are self-report questionnaires. As each of these tools were only used once in the ASD population, they did not meet our commonly used criteria and were not considered further.
Tools Commonly Used
Our search did not identify any tools that are commonly used to assess for suicidality in autistic children or youth. A similar search in the general population of children and youth revealed five tools that measure suicidality used in two or more studies. General characteristics of these tools are summarized in Table 4, and evidence of their psychometric properties (as described in previous literature) is presented in Table 5.
Discussion
Suicidal thoughts and behaviours (STBs) are increasingly common in children and youth, and evidence is emerging to suggest that autistic children and youth are at a heightened risk for experiencing suicidality, yet suicidality in this population often goes undetected due to inadequate measurement (Horowitz et al. 2017). Despite the pressing need for tools to assess for suicidality in children and youth with ASD, results of the current review highlight the extremely limited number of available measures, and more importantly, the lack of studies determining the validity of such measures for this population. These results underscore the critical need to identify or develop tools that can accurately assess for STBs in children and youth with ASD. Furthermore, research is needed in order to distinguish between self-injury, that commonly serves a self-stimulatory function among individuals with ASD, versus NSSI and suicidality. Currently, we run the risk of inaccurately attributing such behaviours to restrictive repetitive behaviours common among individuals with ASD, without accurately considering suicidality.
While the nonexistence of validated measures for children and youth with ASD is unsurprising given the research on adults with ASD and suicidality (see Cassidy et al. 2018b), unfortunately measures developed for general population children and youth provide a limited framework for adaptation to the ASD population. Our search yielded only five common measures with evidence in support of their validity for assessing suicidality in children and youth without ASD, despite our liberal criteria for common-use measures (used in more than one study). Information on the psychometric properties of these measures was limited and much of the available evidence is from studies conducted by authors of the measures, with little to no independent validation studies. This lack of independently validated studies on common measures of suicidality in children and youth highlights a broader issue in the field; it is unclear whether the measures being used to assess for suicidality in children and youth are valid or reliable.
Broadly, the measures identified in our search mostly involved single-informant (i.e., self- or caregiver-report) interviews; however, best practice in the assessment of many childhood mental health concerns involves gathering information from multiple informants (e.g., self, caregivers, teachers; Srinath et al. 2019). Although previous literature suggests parent–child agreement on measures of suicidality is generally poor (Prinstein and Nock 2003), reliance on a single-informant may provide a limited scope of contextual factors that may be necessary for determining level of risk and safety planning. The SITBI is the only measure identified within our search that explicitly states it can be administered through interviews with adolescents, as well as their parents (Nock et al. 2007).
Based on the available evidence, the measures included also varied in their methods and ability to discriminate high vs. low risk of suicide. The C-SSRS, SITBI, and BSS measure multiple dimensions of suicidality (e.g., ideation and behaviours), though none of the measures assess a wide combination of dimensions of suicidal ideation (i.e., passive ideation, active ideation, intent, method, plan; US Food and Drug Administration 2012). The C-SSRS provides one of the most comprehensive assessments of ideation of the measures included, though this measure has been criticized for its narrow measurement of ideation (see Giddens et al. 2014). The limited range of suicidality assessed across the five studies included is particularly troubling given the field’s current limited understanding of the relationship between the various dimensions of ideation and suicide behaviours (Miranda et al. 2014). Consequently, is it unknown how accurate the available measures are at detecting suicidality in children and youth.
Assessment of Suicidality in Children and Youth with ASD
Robust assessment of suicidality in children and youth without ASD is complex and challenging. The unique difficulties inherent to ASD pose additional barriers to understanding and gathering accurate information on suicidal ideation, as well as risk for suicidal behaviour and/or attempts. Children and youth with ASD often experience alexithymia and difficulties with communication of their emotions to others (Schauder et al. 2015) in addition to a myriad of other difficulties in social, academic, and cognitive functioning, which may make assessment challenging. While such difficulties are not strictly limited to the assessment of suicidality in children and youth with ASD, new ASD-specific measures are beginning to emerge to screen for other mental health concerns (e.g., The Anxiety Scale for Children-ASD: ASC–ASD; Rodgers et al. 2016; Autism Spectrum Disorders-Comorbid for Children: ASD-CC; Matson and Wilkins 2008). Considering the unique difficulties individuals with ASD experience, even the most robust, well-validated scales for the general population may not be applicable, valid, or have clinical utility for autistic individuals. Whether to adapt tools developed for the general population or develop new tools specifically for the ASD population is also controversial among ASD self-advocates. However, given that up to 50% of children and youth with ASD may experience suicidality, we assert that there is an urgent need to determine if existing risk tools can accurately assess and detect suicidality in children and youth with ASD. Further, we emphasize the need for additional research in this field focusing on adapting, developing and validating risk assessment tools that can accurately identify suicidal ideation and behaviour in autistic children and youth. We present our findings as a necessary call to action for the research community, and propose the following framework to facilitate future research that could fill this substantial gap in existing research and clinical practice.
Predicting Risk for Death by Suicide
The present findings highlight that assessing for risk or predicting if a child or youth is likely to attempt death by suicide continues to represent a major hurdle for the field. At present, there are few evidence-based assessment tools available in the general population that can guide clinician decisions on predicting future suicide (Roos et al. 2013). Without such tools, this difficult decision relies on the expertise of the individual clinician, which in the general population and children with ASD, can vary quite drastically. Predicting death by suicide is particularly challenging, as acutely suicidal individuals are inherently driven to deny any suicidal thoughts and behaviours. Because the majority of existing measures are self-report, this tendency to minimize suicidal symptoms can make accurately assessing for risk extremely difficult for clinicians. Additionally, Roos et al. (2013) highlight the limitations of existing evidence examining the validity of risk assessment tools, including: (a) the overwhelming focus on factors that predict suicide attempts versus death; (b) examining the validity of one item on a tool versus the whole measure; (c) the correlational nature of much of the research examining risk factors for suicide; and (d) most scales are based on a compilation of risk factors that may or may not be helpful for all individuals who die by suicide (Large et al. 2011). In light of these flaws, many experts suggest that deeming existing risk assessment tools as evidence-based is quite premature, and that existing tools may not have clinical utility, despite being used in clinical settings. While existing tools might be helpful to guide clinician questions, Roos et al. (2013) highlight that clinicians and researchers should consider alternatives to the conventional risk factors checklists (e.g., cognitive risk assessments) or develop composite measures that include a multitude of approaches to assessing for risk, as this would be both of clinical utility and potentially have stronger predictive power than the existing tools.
A Framework for Future Research
Step 1. Validation Studies of Existing Tools
The current review highlights a lack of evidence to support the utility of existing risk assessment tools commonly being used to assess STBs in autistic children and youth. While we were unable to determine from the literature reviewed whether existing tools are valid in this population, we were similarly unable to find evidence that they are not valid; simply more research needed. A reasonable starting point for future research would be to examine the validity and psychometric properties of the five commonly used tools used to measure suicidality in the general population (identified here as the C-SSRS, SITBI, SIQ-JR, PSS, and BSS) in children and youth with ASD. From this, we can either confirm that there is an existing tool that can be used in this population with some confidence of reliability and validity, or establish that further tool development is needed.
Step 2. Tool Adaptation and Development
Through future research in this area, a robust general population measure of suicidality may (or may not) emerge as being a promising candidate for adaptation based on its psychometric properties in an ASD population. Rodgers et al.’s (2016) adaptation of the Revised Child Anxiety and Depression Scale (RCADS) to produce the Anxiety Scale for Children-ASD serves as an example for how this step may be undertaken. In this study, the wording of the RCADS was modified based on interviews with caregivers of children with ASD about their interpretation of the items. Additionally, new items were written that better captured the unique presentation of anxiety in ASD. Consistent with this approach, the content validity of existing suicidality measures could be explored through interviewing autistic children and youth and their caregivers about their interpretation of the specific measure items. Cognitive interviewing and focus groups could then help to inform the modification of items to enhance their clarity and relevance. However, it is possible that, despite modifications, tools developed for the general population will not demonstrate adequate reliability and validity when used with autistic children and youth. Consequently, new tools may need to be developed to capture the unique experience of suicidality in this population.
Based on the information provided related to psychometric properties and characteristics of the measures identified within the current study, at this time, no single measure stands out as a template that can be used as a guide for developing ASD-specific tools. Rather, a combination of characteristics from a number of measures may be most beneficial. Here we will present suggestions for the development of ASD-specific tools.
First, gathering both child/youth and caregiver reports is critical for determining level of risk; given the difficulties with social communication many persons with ASD experience, gathering information from multiple sources may help attenuate under-reporting from a single source. With regards to administration, whether questionnaire-based self- or caregiver-report or interview format is more beneficial for detecting mental health issues in children and youth with ASD is unclear (e.g., Keith et al. 2019; Mazefsky et al. 2011). Therefore, a measure with both open and closed ended questions that can incorporate both self-report questions and follow-up interview questions may be beneficial.
Regardless of the administration method, questions should be presented clearly and concisely with limited use of abstract, hypothetical, or ambiguous language (e.g., “What is the likelihood that you will have thoughts of suicide again in the future?”). In addition to gathering information on level of suicidality, gathering information on the child/youth’s restricted or repetitive patterns of behaviour and interests is critical. Understanding whether the child or youth is experiencing suicidality or whether they have circumscribed interests around topics such as death, heaven, or violence may help to inform level of risk. Lastly, but most importantly, the development or adaptation of measures of suicidality must involve autistic self-advocates or persons with lived experience in order to best understand the true nature and extent of their experiences.
Families of children with ASD and/or youth with ASD themselves are able to provide critical insight into what content and language will most effectively capture suicidality in this population. If developing a new tool, researchers could first identify emerging themes related to the characterization or identification of suicidality from interviews with individuals or families. From these themes, content for a scale could be devised and items could be selected. Cognitive interviews could then evaluate participant’s perceived ability to complete the scale/measure without bias (i.e., bias due to lack of understanding, their preferred response not being an option on the scale, etc.). Participants would have the opportunity to suggest alternative wording, response options, or formats that would limit bias. Finally, the psychometric properties (e.g., reliability and validity) of the tool would be assessed.
Strengths and Limitations
This is the first study, to our knowledge, to systematically review existing literature on tools used to assess for suicide in children and youth in the general population, as well as individuals with ASD. A major strength of this study was our comprehensive and exhaustive search strategy, as well as how we operationalized ‘commonly used’. Although the present findings fill a major gap in existing knowledge related to assessing for suicidality in autistic children and youth, we did not utilize a rigorous assessment tool, such as the COSMIN checklist, to adjudicate and report the psychometric properties of specific measures. Consequently, the present findings should be interpreted with some caution, as we did not take a systematic approach to analyzing the psychometric properties of each measure, but rather described the properties that were identified in previous research. Lastly, while we employed a comprehensive search strategy, it is also possible that we may not have discovered all relevant studies that assess the measurement properties of the tools identified.
Conclusion
Children and youth with ASD are at heightened risk for experiencing suicidality. Deficits that are inherent to ASD, such as communication difficulties, alexithymia, and special interests related to death, make validly assessing for suicidality challenging. Consistent with studies completed in adults with ASD (Cassidy et al. 2018a, b), findings from our study demonstrate that no tools currently exists that can accurately assess for suicide in children and youth with ASD, nor predict future suicidal behaviour and attempts. Consequently, these findings highlight the urgent need for future research to examine the psychometric properties of existing tools developed for the general population (e.g., C-SSRS, SIJ-Q) in children and youth with ASD to determine whether they accurately detect suicidality, to understand mechanisms of risk, and to accurately determine prevalence of STBs in this population. Additionally, it is important for future research to determine how to adapt existing tool for use in this population.
Identifying suicide risk accurately is essential for clinical practice, as untreated individuals with ASD who are suicidal can lead to negative outcomes (e.g., hospitalizations, visits to the emergency department, and poor quality of life), and most importantly, are more likely to complete suicide. Moreover, it is imperative that as a field we move to identifying and/or adapting valid existing measures or developing new measures to facilitate generalizable and clinically meaningful research to further understand and prevent suicidality in autistic children and youth.
References
Achenbach, T. M. (1991a). Manual for the Youth Self-Report and 1991 profile. Department of Psychiatry, Burlington, VT: University of Vermont.
Achenbach, T. M. (1991b). Manual for the Child Behavior Checklist/4-18 and 1991 Profile. Department of Psychiatry, Burlington, VT: University of Vermont.
Agosti, V., Chen, Y., & Levin, F. R. (2011). Does attention deficit hyperactivity disorder increase the risk of suicide attempts? Journal of Affective Disorders, 133(3), 595–599.
American Psychological Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
American Psychological Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Au-Yeung, S. K., Bradley, L., Robertson, A. E., Shaw, R., Baron-Cohen, S., & Cassidy, S. (2018). Experience of mental health diagnosis and perceived misdiagnosis in autistic, possibly autistic and non-autistic adults. Autism, 23(6), 1508–1518.
Baraskewich, J., & McMorris, C. (2019). Internalizing mental health issues in individuals with neurodevelopmental disorders: Implications for practitioners. Current Developmental Disorders Reports, 6(1), 1–8.
Barzilay, S., Feldman, D., Snir, A., Apter, A., Carli, V., Hoven, C.W., C. Wasserman, Sarchiapone, M., & Wasserman, D. (2015). The interpersonal theory of suicide and adolescent suicidal behaviour. Journal of Affective Disorders, 183, 68–74.
Beck, A. T., Brown, G. K., Steer, R. A., Dahlsgaard, K. K., & Grisham, J. R. (1999). Suicide ideation at its worst point: A predictor of eventual suicide in psychiatric outpatients. Suicide and Life Threatening Behaviour, 29(1), 1–9.
Beck, A. T., Kovacs, M., & Weissman, A. (1979). Assessment of suicidal intention: The Scale for Suicide Ideation. Journal of Consulting and Clinical Psychology, 47, 343–352.
Beck, A., Steer, R., & Ranieri, W. (1988). Scale for Suicidal Ideation: Psychometric properties of a self-report version. Journal of Clinical Psychology, 44, 499–505.
Cassidy, S. A., Bradley, L., Bowen, E., Wigham, S., & Rodgers, J. (2018a). Measurement properties of tools used to assess depression in adults with and without autism spectrum conditions: A systematic review. Autism Research, 11(5), 738–754.
Cassidy, S., Bradley, L., Bowen, E., Wigham, S., & Rodgers, J. (2018b). Measurement properties of tools used to assess suicidality in autistic and general population adults: A systematic review. Clinical Psychology Review, 62, 56–70.
Cassidy, S., Bradley, P., Robinson, J., Allison, C., McHugh, M., & Baron-Cohen, S. (2014). Suicidal ideation and suicide plans or attempts in adults with Asperger’s syndrome attending a specialist diagnostic clinic: A clinical cohort study. The Lancet Psychiatry, 1(2), 142–147.
Cassidy, S., & Rodgers, J. (2017). Understanding and prevention of suicide in autism. The Lancet Psychiatry, 4(6), 11.
Chen, M. H., Pan, T. L., Lan, W. H., Hsu, J. W., Huang, K. L., Su, T. P., et al. (2017). Risk of suicide attempts among adolescents and young adults with autism spectrum disorder: A nationwide longitudinal follow-up study. Journal of Clinical Psychiatry, 78(9), 1174–1179.…
Czyz, E. K., King, C. A., & Bierman, B. J. (2019). Motivational interviewing-enhanced safety planning for adolescents at high suicide risk: A pilot randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 48(2), 250–262.
Demirkaya, S. K., & Tutkunkardaz, M. D. (2016). Mukaddes NM (2016) Assessment of suicidality in children and adolescents with diagnosis of high functioning autism spectrum disorder in a Turkish clinical sample. Neuropsychiatric Disease and Treatment, 12, 2921–2926.
Dickerson Mayes, S. D., Gorman, A. A., Hillwig-Garcia, J., & Syed, E. (2013). Suicide ideation and attempts in children with autism. Research in Autism Spectrum Disorders, 7(1), 109–119.
Durbin, A., Balogh, R., Lin, E., Wilton, A., & Lunsky, Y. (2018). Emergency department use: Common presenting issues and continuity of care for individuals with and without intellectual and developmental disabilities. Journal on Autism and Other Developmental Disabilities, 48(10), 3542–3550.
Eskin, M. (1995). Suicidal behavior as related to social support and assertive-ness among Swedish and Turkish high school students: A cross-cultural investigation. Journal of Clinical Psychology, 51(2), 158–172.
Francesca-Pedrero, E., Inchausti, F., Perez-Albeniz, A., & Ortuno-Sierra, J. (2018). Validation of the Prodromal Questionnaire-Brief in a representative sample of adolescents: Internal structure, norms, reliability, and links with psychopathology. International Journal of Methods in Psychiatry Research, 27(4), e1740.
Fremouw, W. L., Strunk, J. M., Tyner, E. A., & Musick, H. (2009). Adolescent Suicide Assessment Protocol. West Virginia Suicide Council.
Giddens, J. M., Sheehan, K. H., & Sheehan, D. V. (2014). The Columbia-Suicide Severity Rating Scale: Has the “gold standard” become a liability? Innovations in Clinical Neuroscience, 11(9–10), 66–80.
Glenn, C. R., Lanzillo, E. C., Esposito, E. C., Santee, A. C., Nock, M. K., & Auerbach, R. P. (2016). Examining the course of suicidal and nonsuicidal self-injurious thoughts and behaviours in outpatient and inpatient adolescents. Journal of Abnormal Child Psychology, 45, 971–983.
Glenn, C. R., Millner, A. J., Esposito, E. C., Porter, A. C., & Nock, M. K. (2019). Implicit identification with death predicts suicidal thoughts and behaviour in adolescents. Journal of Clinical Child and Adolescent Psychology, 48(2), 263–272.
Haas, A. P., Eliason, M., Mays, V. M., Mathy, R. M., Cochran, S. D., A’Augelli, A. R., ..., Clayton, P. J. (2011). Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations. Journal of Homosexuality, 58(1), 10–51.
Hannon, G., & Taylor, E. P. (2013). Suicidal behaviour in adolescents and young adults with ASD: Findings from a systematic review. Clinical Psychology Review, 33(8), 1197–1204. https://doi.org/10.1016/j.cpr.2013.10.003.
Hirvikoski, T., Mittendorfer-Rutz, E., Boman, M., Larsson, H., Lichtenstein, P., & Bolte, S. (2016). Premature mortality in autism spectrum disorder. British Journal of Psychiatry, 208(3), 232–238.
Horowitz, L. M., Thurm, A., Farmer, C., Mazefsky, C., Lanzillo, E., Bridge, J. A., ..., Siegel, M. (2017). Talking about death or suicide: Prevalence and clinical correlates in youth with autism spectrum disorder in the psychiatric inpatient setting. Journal of Autism and Developmental Disorders, 48(11), 3702–3710.
Horvath, L. O., Balini, M., Ferenczi-Dallos, G., Farkas, L., Gadoros, J., Gyori, D., ..., Balazs, J. (2018). Direct self-injurious behaviour (D-SIB) and life events among vocational school and high school students. International Journal of Environmental Research and Public Health, 15, 1068–1081.
Kahn, J., Tubiana, A., Chen, R. F., Carli, V., Wasserman, C., Hoven, C., ..., Wasserman, D. (2015). Important variables when screening for students at suicidal risk: Findings from the French cohort of the SEYLE Study. International Journal of Environmental Research and Public Health, 12, 12277–12290.
Kato, K., Mikami, K., Akama, F., Yamada, Y., Maehara, M., Kimoto, K., ..., Matsumoto, H. (2013). Clinical features of suicide attempts in adults with autism spectrum disorders. General Hospital Psychiatry, 35, 50–53.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., et al. (1997). Schedule for affective disorders and schizophrenia for school-age children-resent and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child and Adolescent Psychiatry, 36(7), 980–988.…
Keane, E. M., Dick, R. W., Bechtold, D. W., & Manson, S. M. (1996). Predictive and concurrent validity of the Suicidal Ideation Questionnaire among American Indian adolescents. Journal of Abnormal Child Psychology, 24, 735–747.
Keith, J. M., Jamieson, J. P., & Bennetto, L. (2019). The importance of adolescent self-report in autism spectrum disorder: Integration of questionnaire and autonomic measures. Journal of Abnormal Child Psychology, 47(4), 741–754.
Kennard, B. D., Goldstein, T., Foxwell, A. A., McMakin, D. L., Wolfe, K., Biernesser, C., ..., Brent, D. (2018). As Safe as possible (ASAP): A brief app-supported inpatient intervention to prevent postdischarge suicidal behaviour in hospitalized, suicidal adolescents. American Journal of Psychiatry, 179(9), 864–872.
Kovacs, M. (2010). Children’s Depression inventory 2nd Edition (CDI-2). North Tonowanda, NY: Multi-Health Systems, Inc.
Krysinska, K., & Lester, D. (2010). Post-traumatic stress disorder and suicide risk: A systematic review. Archives of Suicide Research, 14(1), 1–23.
Large, M., Sharma, S., Cannon, E., Ryan, C., & Nielssen, O. (2011). Risk factors for suicide within a year of discharge from psychiatric hospital: A systematic meta-analysis. Australian and New Zealand Journal of Psychiatry, 45(8), 619–628.
Lever, A. G., & Geurts, H. M. (2016). Psychiatric co-occurring symptoms and disorders in young, middle-aged, and older adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(6), 1916–1930.
Leyfer, O. T., Folstein, S. E., Bacalman, S., Davis, N. O., Dinh, E., Morgan, J., ..., Lainhart, J. E. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of Autism and Developmental Disorders, 36, 849–861.
Linehan, M. M., Comtois, K. A., Brown, M. Z., Heard, H. L., & Wagner, A. (2006). Suicide Attempt Self-Injury Interview (SASII): Development, reliability, and validity of a scale to assess suicide attempts and intentional self-injury. Psychological Assessment, 18(3), 303–312.
Malagama, A. S., Tennakoon, S., & Abeyasinghe, D. R. R. (2018). Validation of Adolescent Suicide Assessment Protocol (ASAP-20) to Sri-Lankan adolescents. Asian Journal of Psychiatry, 33(2018), 11–17.
Matson, J. L., & Wilkins, J. (2008). Reliability of the autism spectrum disorders-comorbid for children (ASD-CC). Journal of Developmental and Physical Disabilities, 20(4), 327–336.
Mazefsky, C. A., Kao, J., & Oswald, D. P. (2011). Preliminary evidence suggesting caution in the use of psychiatric self-report measures with adolescents with high-functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 5(1), 164–174.
McCauley, E., Berk, M. S., Asarnow, J. R., Adrian, M., Cohen, J., Korslund, K., ..., Linehan, M. M. (2018). Efficacy of dialectical behaviour therapy for adolescents at high risk for suicide: A randomized clinical trial. JAMA Psychiatry, 75(8), 776–785.
Miranda, R., Ortin, A., Scott, M., & Shaffer, D. (2014). Characteristics of suicidal ideation that predict the transition to future suicide attempts in adolescents. J Child Psychology and Psychiatry, 55, 1288–1296.
Muehlenkamp, J. J., & Gutierrez, P. M. (2004). An investigation of differences between self-injurious behaviour and suicide attempts in a sample of adolescents. Suicide and Life-Threatening Behaviour, 34(1), 12–23.
Nock, M. K., Holmberg, E. B., Photos, V. I., & Michel, B. D. (2007). Self-Injurious Thoughts and Behaviors Interview: Development, reliability, and validity in an adolescent sample. Psychological Assessment, 19(3), 309–317.
Orbach, L., Milstein, L., Har-Even, D., Apter, A., Tyano, S., & Elizur, A. (1991). A multi-attitude suicide tendency scale for adolescents. Psychological Assessment, 3, 398–404.
Ordaz, S. J., Goyer, M. S., Ho, T. C., Singh, M. K., & Gotlib, I. H. (2018). Network basis of suicidal ideation in depressed adolescents. Journal of Affective Disorders, 226, 92–99.
Paykel, E. S., Myers, J. K., Lindenthal, J. J., & Tanner, J. (1974). Suicidal findings in the general population: A prevalence study. The British Journal of Psychiatry, 124(582), 460–469.
Penn, J. V., Esposito, C. L., Schaeffer, L. E., Pritz, G. K., & Spirito, A. (2003). Suicide attempts and self-mutilative behaviour in a juvenile correctional facility. Journal of the American Academy of Child and Adolescent Child Psychiatry, 42(7), 762–769.
Pfeffer, C. R. (1986). The suicidal child. New York: Guilford.
Pinto, A., McCoy, K. J. M., & Whisman, M. A. (1997). Suicidal ideation in adolescents: Psychometric properties of the Suicidal Ideation Questionnaire in a Clinical Sample. Psychological Assessment, 9, 63–66.
Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., ..., Mann, J. J. (2011). The Columbia-Suicide Severity Rating Scale: Validity and internal consistency findings from three multisite studies with adolescents and adults. American Journal of Psychiatry, 168, 1266–1277.
Prinstein, M. J., & Nock, M. K. (2003). Parents under-report children’s suicide ideation and attempts. Evidence Based Mental Health, 6(1), 12.
Reaven, J., & Wainer, A. L. (2015). Children and adolescents with ASD and co-occurring psychiatric conditions: Current trends in intervention. In R. M. Hodapp & D. J. Fidler (Eds.), International review of research in developmental disabilities (pp. 45–90). New York: Academic.
Reynolds, W. M. (1988). SIQ. Psychological Assessment Resources, Odessa, FL: Suicidal Ideation Questionnaire.
Reynolds, W. M., & Mazza, J. J. (1999). Assessment of suicidal ideation in inner-city children and young adolescents: Reliability and validity of the Suicidal Ideation Questionnaire-JR. School Psychology Review, 28(1), 17–30.
Rodgers, J., Wigham, S., McConachie, H., Freeston, M., Honey, E., & Parr, J. R. (2016). Development of the anxiety scale for children with autism spectrum disorder (ASC–ASD). Autism Research, 9(11), 1205–1215.
Roos, L., Sareen, J., & Bolton, J. M. (2013). Suicide risk assessment tools, predictive validity findings and utility today: Time for a revamp? Neuropsychiatry, 3(5), 483–495.
Rudd, M. D., Dahm, P. F., & Rajab, M. H. (1993). Diagnostic comorbidity in persons with suicidal ideation and behaviour. American Journal of Psychiatry, 150, 928–934.
Schauder, K. B., Mash, L. E., Bryant, L. K., & Cascio, C. J. (2015). Interoceptive ability and body awareness in autism spectrum disorder. Journal of Experimental Child Psychology, 131, 193–200. https://doi.org/10.1016/j.jecp.2014.11.002.
Segers, M., & Rawana, J. (2014). What do we know about suicidality in autism spectrum disorders? A systematic review. Autism Research, 7(4), 507–521.
Sharpley, C. F., Bitsika, V., Andronicos, N. M., & Agnew, L. L. (2016). Further evidence of HPA-axis dysregulation and its correlation with depression in autism spectrum disorder: Data from girls. Physiology and Behaviour, 16, 110–117.
Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Janavs, J., Bannon, Y., Rogers, J. E., ..., Wilkinson, B. (2010). Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). Journal of Clinical Psychiatry, 71, 313–326.
Shtayermman, O. (2008). Suicidal ideation and comorbid disorders in adolescents and young adults diagnosed with Asperger’s syndrome: A population at risk. Journal of Human Behaviour in the Social Environment, 18(3), 301–328.
Srinath, S., Jacob, P., Sharma, E., & Gautam, A. (2019). Clinical practice guidelines for assessment of children and adolescents. Indian Journal of Psychiatry, 61(Suppl 2), 158–175. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_580_18.
Steer, R. A., Kumar, F., & Beck, A. T. (1993). Self-reported suicidal ideation in adolescent psychiatric inpatients. Journal of Consulting and Clinical Psychology, 61, 1096–1099.
Stewart, J. G., Esposito, E. C., Glenn, C. R., Gilman, S. E., Pidgeon, B., Gold, J., et al. (2017). Adolescent self-injurers: Comparing non-ideators, suicide ideators, and suicide attempters. Journal of Psychiatric Research, 84, 105–112.
Teplin, L. A., Stokes, M. L., McCoy, K. P., Abram, K. M., & Byck, G. R. (2017). Suicidal ideation and behaviour in youth in the juvenile justice system: A review of the literature. Journal of Correctional Health Care, 21(3), 222–242.
US Food and Drug Administration. (2012). Guidance for industry: Suicidality: Prospective assessment of occurrence in clinical trials, draft guidance. Rockville, MD: US Department of Health and Human Services.
Vergara, G. A., Stewart, J. G., Cosby, E. A., Lincoln, S. H., & Auerbach, R. P. (2019). Non-suicidal self-injury and suicide in depressed adolescents: Impact of peer victimization and bullying. Journal of Affective Disorders, 245, 744–749.
White, S. E., McMorris, C. A., Weiss, J., & Lunsky, Y. (2012). The experience of crisis in families of individuals with autism spectrum disorder across the lifespan. Journal of Child and Family Studies, 21, 457–465.
Wigham, S., & McConachie, H. (2014). Systematic review of the properties of tools used to measure outcomes in anxiety intervention studies for children with autism spectrum disorders. PLoS ONE, 9(1), e85268.
World Health Organization. (2018). International statistical classification of diseases and related health problems (11th Revision). https://icd.who.int/browse11/l-m/en.
Acknowledgments
Special thanks to Panth Shah and Hangsel Sanguino for their help in preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. The literature search and data extraction was completed by SJH and KH. The first draft of the manuscript was written by SJH, KH CAM, and JB. SC edited and commented on the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
We have no potential conflicts of interest to disclose.
Informed Consent
As our research was a synthesis of existing literature, we did not have contact with human participants, and therefor informed consent was not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Howe, S.J., Hewitt, K., Baraskewich, J. et al. Suicidality Among Children and Youth With and Without Autism Spectrum Disorder: A Systematic Review of Existing Risk Assessment Tools. J Autism Dev Disord 50, 3462–3476 (2020). https://doi.org/10.1007/s10803-020-04394-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04394-7