
Abstract
This study examined the efficacy of the school-based Program for the Education and Enrichment of Relational Skills on the social functioning of young adults with autism and cognitive deficits. The program was administered bi-weekly at a private school for students with special needs. Students’ social etiquette knowledge, friendship engagement and teacher reported levels of their social functioning were assessed pre- and post-intervention. All participants experienced significantly improved knowledge of appropriate social etiquette. Further, students with cognitive deficits, but not those with autism, reported a significant increase in friendship engagement. Overall, the PEERS school curriculum benefited young adults with cognitive deficits, but the students with ASD experienced more challenges applying their new social skills outside of the program.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Individuals with Autism Spectrum Disorders (ASD), as well as those with non-comorbid intellectual disabilities (ID), experience a range of social and daily living challenges throughout adulthood (Orsmond et al. 2013; Tipton et al. 2013). There have been several social skills programs that aim to assist youth with ASD (see Camargo et al. 2014; Kaat and Lecavalier 2014; McMahon et al. 2013; Wong et al. 2015, for reviews). While these programs improved students’ social skills knowledge and on-task social performance, these methods were less effective when analyzing students’ actual social behaviors in real-life contexts (Gates et al. 2017).
The Program for the Education and Enrichment of Relational Skills (PEERS) was specifically designed to benefit individuals with ASD. As individuals with ASD experience challenges understanding and utilizing appropriate social etiquette (American Psychiatric Association 2013), the PEERS program provides developmentally-appropriate and generalizable instruction that has shown to improve their knowledge of appropriate social interactions, and more importantly, their application of the newly acquired social skills to their daily lives (Gonring et al. 2017; Laugeson et al. 2009, 2012; Schohl et al. 2014). However, most research on this program has focused on the clinical outpatient group model, but the school-based program (Laugeson 2014) has not been analyzed in as much depth (Laugeson et al. 2014). There has also been little research to date on group-based social skills programs in samples with young adults and those who possess lower intellectual functioning (Wong et al. 2015). As individuals with lower intellectual functioning also experience significant social deficits with respect to their initiation and maintenance of social relationships (Orsmond et al. 2013; Taheri et al. 2016), the PEERS program may also benefit this frequently overlooked population in the social intervention literature. To address these important gaps in the literature, the current study examined the effectiveness of the school-based PEERS program with a sample of young adults with ASD and those with cognitive deficits (CD).
Social Functioning and Neurodevelopmental Disorders
Individuals with neurodevelopmental disabilities, namely ASD and ID, generally have lower social skills and friendship quality (American Psychiatry Association 2013), which can greatly hinder their future interpersonal (Taheri et al. 2016), employment (Nord et al. 2016) and mental health (Marriage et al. 2009) outcomes. ASD is a neurodevelopmental disorder in which a child has persistent communication and social interaction deficits, and/or restricted or repetitive behavior patterns, across multiple settings (American Psychiatric Association 2013). Notably, individuals with ASD experience deficits with social-emotional reciprocity whereby they have difficulties initiating and maintaining conversations, as well as additional challenges sharing interests and engaging in back-and-forth conversations. Further, deficits in the use of nonverbal communicative behaviors that are effectively integrated with verbal communication, including culturally appropriate eye-contact, gestures, body language and personal space, are common in individuals with ASD. Restricted and repetitive patterns of behavior (e.g., stereotyped motor movements), interests and/or activities is an additional diagnostic criterion used to evaluate ASD. Overall, these social deficits and repetitive/restricted behaviors typically result in significant challenges understanding, developing and maintaining social relationships with others (American Psychiatric Association 2013). However, it is worth highlighting that ASD symptomology is examined across a spectrum, and thus, there is a broad range in the presence and severity of specific ASD symptoms across this population.
An intellectual disability (i.e., Intellectual Developmental Disorder) is typically diagnosed early in life when a child’s cognitive ability is determined to be at least two standard deviations below the population mean (American Psychiatric Association 2013; American Association on Intellectual and Developmental Disabilities 2017). Deficits in cognitive functioning limit an individual’s learning potential and abilities to demonstrate age-appropriate communication, reasoning and judgement in their daily lives. In addition to delayed cognitive ability, a child must also have considerable delays in adaptive functioning. Delays in adaptive functioning can limit a child’s abilities to communicate with others, develop applied academic skills, socialize, engage in leisure and self-directed activities, attain self-care and safety skills, and meet the general community standards of personal independence and social responsibility. Furthermore, an ID diagnosis ranges from mild, to moderate, to severe or profound, as a means of describing the severity of the cognitive and adaptive skill deficits (American Psychiatric Association 2013).
The social, emotional and behavioral difficulties in individuals with ASD are typically more severe compared to those with an ID (Brereton et al. 2006; Smith and Matson 2010). However, both populations experience communication and social deficits, namely lower initiation and maintenance of social relationships (Orsmond et al. 2013; Taheri et al. 2016), which can result in increased feelings of loneliness (Gilmore and Cuskelly 2014; Mazurek 2014), sadness and anxiety (Marriage et al. 2009). Both populations are also especially vulnerable to becoming victims of bullying (Zeedyk et al. 2014) and abuse (Jones et al. 2012; Mandell et al. 2005). Additionally, both populations have significantly more challenges finding meaningful and consistent employment compared to the general population (Nord et al. 2016). These social deficits, in addition to the cognitive and daily living limitations, often result in increased dependence on family members or community resources throughout adulthood for self-care, economic assistance and social support (Farley et al. 2018; Grey et al. 2015). Lastly, among those that do have friendships, these bonds are more likely to be characterized as being lower in quality, closeness, warmth and reciprocity compared to the general population (Orsmond et al. 2013; Tipton et al. 2013). To address these important concerns in the social functioning of adults with ASD and cognitive deficits (ID and borderline intellectual functioning), the current study evaluated the potential value of the PEERS school-based program for improving the social abilities and friendship acquisition of these two populations.
Program for the Education and Enrichment of Relational Skills (PEERS)
There have been several individual and group-based social skills interventions designed to improve the overall social functioning of children and youth with ASD (Camargo et al. 2014; Kaat and Lecavalier 2014; McMahon et al. 2013; Wong et al. 2015). Individual-focused interventions, such as techniques used in applied behavior analysis (ABA) therapy (e.g., reinforcement, extinction, video-modeling, scripting and social stories) have obtained positive results (see Granpeesheh et al. 2009; Wong et al. 2015, for reviews). While the PEERS program includes some evidence-based features of ABA (e.g., reinforcement and modelling), traditional ABA treatments with older students also possess some limitations. Notably, ABA treatments are often individual-focused, such that the student works one-on-one or in a small group setting with a therapist, teacher or mentor to eliminate undesirable behaviors and learn new social behaviors and skills. Individual-based interventions help to address the personal needs and capacities of a single client. However, given that individuals with ASD have difficulty transferring learned social skills into real life situations (Rao et al. 2008), recent social skills programs have focused on students receiving their social skills training in a larger group setting to assist with the generalization of their newly acquired skills (see Camargo et al. 2014 for a review).
Group-based social skills interventions in inclusive settings differ from individual-focused interventions because they enable youth to practice the socials skills being taught with similar-aged peers. Further, participating in social groups permits youth to learn from each other, find common interests, and potentially develop friendships (Camargo et al. 2014; Laugeson 2014). While several review papers highlight the many benefits of group-based social skills interventions for improving students’ social skills knowledge and behavior (e.g., Camargo et al. 2014; Kaat and Lecavalier 2014; McMahon et al. 2013), a recent meta-analysis by Gates et al. (2017) of 19 randomized control trial studies (from an initial search that produced 2620 articles) highlighted some limitations with these methods. The group-based methods were found to have significant and medium positive effects (g = 0.51, p < .01) overall, with these effects being largest for self-reports (g = 0.92) and task-based measures (g = 0.58). In contrast, the effects were small for parent (g = 0.47) and observe reports (g = 0.40), and the effects were non-significant for teacher reports. Therefore, the social skills groups were found to improve students’ social knowledge and task-based performance. Yet, their social skills outside of the groups did not improve to the same level, as determined by the small or non-significant effects on the parent, teacher and observer reports (Gates et al. 2017).
To address these challenges with existing social skills programs, the PEERS program includes one of the first published treatment manuals (Laugeson 2014; Laugeson and Frankel 2010) for helping practitioners, teachers and parents effectively improve the social functioning of children and teens with social deficits. Since ABA treatment methods are often tailored to the individual (Bailey and Burch 2017), much of this research has been dominated by cases studies (see Granpeesheh et al. 2009, for a review). As the PEERS curriculum is manual-based and is taught in a group setting, there have been a growing number of empirical studies with larger samples that have examined the specific benefits of this program with students diagnosed with ASD (e.g., Laugeson et al. 2009, 2012; Mandelberg et al. 2014; Schohl et al. 2014) and ADHD (Gardner et al. 2015; Gonring et al. 2017).
The original PEERS curriculum (Laugeson et al. 2009) incorporated teens and their parents participating in separate and concurrent outpatient group sessions with qualified instructors. The teen meetings focus on improving their social skills etiquette, such as developing appropriate and flexible conversation skills (e.g., peer entry and exiting skills), establishing friendship networks, and managing confrontations, teasing, bullying and bad reputations; refer to Table 1 for the corresponding topics used in the school-based model. At the same time, teens are provided with a safe setting to develop friendships with their developmentally-similar peers. Teens also receive a range of evidence-based strategies for teaching them the aforementioned social skills, including: (1) Short didactic teaching from a qualified instructor; (2) role-playing and behavioral rehearsals; (3) weekly socialization assignments and homework review that emphasize friendship development; and (4) behavior modeling, coaching and immediate social performance feedback. Given the importance of parents on fostering social development and friendship building throughout childhood and adolescence (Flynn et al. 2017), the parents meet concurrently whereby they are informed by an instructor about the weekly PEERS lesson, goals and homework tasks, along with how they can supervise the implementation and development of their child’s new social skills (Laugeson et al. 2009).
Research on the outpatient PEERS model has been very positive. Findings from several studies indicate that this program improved the social skills knowledge and friendship attainment of teens with ASD (e.g., Laugeson et al. 2009, 2012; Mandelberg et al. 2014; Schohl et al. 2014) and ADHD (Gardner et al. 2015; Gonring et al. 2017), along with significant improvements on observer reports of their social functioning and a decrease in autism symptomology and social anxiety.
The PEERS school-based curriculum was later developed as a means of helping students with ASD to not only improve their social skills knowledge and behavior, but to provide them with actual experiences to enable them to apply these skills to real-life settings (Laugeson 2014). While the instructional content is similar to the outpatient program format, the school-based PEERS model is a teacher-facilitated social skills class, which puts an emphasis on helping teens to make and keep friends in the school setting (Laugeson 2014). Parents are also sent summaries of the weekly lessons, goals and homework tasks, but there are no concurrent parent groups. To date, research on the school-based model is limited. In one of the few studies on the school model, Laugeson and colleagues (2014) found that middle school students with ASD in the active treatment group demonstrated significant improvements in social responsiveness (according to teacher reports) compared to the control group, along with an increase in self-reported hosted and invited get-togethers.
Given the paucity of research on the school-based PEERS program, the current study seeks to advance the prior PEERS and social skills intervention research in several ways. Firstly, the prior PEERS literature has typically included a sample of high functioning students with ASD (e.g., Laugeson et al. 2009, 2012, 2014; Schohl et al. 2014) or ADHD (Gardner et al. 2015; Gonring et al. 2017). However, individuals with CD, who do not have comorbid ASD, also experience social deficits that can greatly limit their independence at home (Grey et al. 2015) and future employment opportunities (Nord et al. 2016), as well as hinder the frequency and quality of their friendships (Tipton et al. 2013). Therefore, like individuals with ASD, it is necessary to examine the value of social skill programs with individuals with CD to further enhance their social and daily living functioning at home and in the community. The PEERS school-based program addresses many of the specific social challenges in both ASD and CD populations by providing them with instruction and practice for building their communication skills in different contexts (e.g., joining and exiting conversations, organizing hangouts, handling conflicts), as well as increasing their friendship building and maintenance skills. However, it is unclear whether this program in its current state can be effectively taught to individuals with lower verbal, nonverbal (e.g., memory and reasoning) and adaptive skills.
Secondly, in Wong et al. (2015) comprehensive review of 27 focused intervention practices, the majority of the 456 studies examined included a sample of students under the age of 15. Social skills programs for young adults is essential given that some youth with social deficits have not had access to any prior formalized social interventions (Wainer and Ingersoll 2015). Among those who have received intervention, the social skills needed during adulthood differ from those commonly practiced in childhood and adolescence. Notably, young adults have increased responsibilities and independence at home and in the community, whether it be developing the daily living social skills needed to live independently, seeking out and maintaining friendships/relationships outside of school, and pursuing and maintaining meaningful employment.
Thirdly, school-based social skills interventions permit students to directly apply the learned social knowledge into a setting wherein they are most likely to interact with others and develop friendships. While there has been considerable research on the original outpatient group PEERS model (e.g., Laugeson et al. 2009, 2012; Schohl et al. 2014; Yoo et al. 2014), there has been very little research that has specifically analyzed the benefits and limitations of the school-based PEERS model (Laugeson et al. 2014). As previously noted, there are several differences between the outpatient and school-based PEERS models, such as the fact that the school model is teacher facilitated, takes place in the school setting and includes no concurrent parent groups (Laugeson 2014).
To address these notable gaps in the social skill intervention literature, the current study examines the efficacy of the school-based PEERS program with young adults with ASD and/or cognitive deficits in a special education school environment. The present study can particularly benefit parents, teachers, school administrators and practitioners who are trying to improve the social functioning of young adults. More specifically, the PEERS school-based intervention can be a more cost-effective and practical way for students to improve their social abilities, given that this intervention takes place at school during the day (Laugeson 2014). Instead of receiving the intervention in a private and non-generalizable clinical setting from an unfamiliar instructor, students in the school program receive the evidence-based instruction from a teacher they know and trust in a setting wherein they are most likely to socialize with peers. As a result, students who experience challenges generalizing their social knowledge into their daily lives (Gates et al. 2017; Rao et al. 2008) may be more receptive to this school-based intervention as they are given opportunities to directly use the acquired social skills with peers at school.
Current Study
In the current study, 63 students with ASD or CD (ID or borderline intellectual functioning) were administered the 16-week PEERS school-based curriculum. To examine the efficacy of this intervention, pre-test and post-test measures of the students’ (1) knowledge of appropriate social etiquette in various social contexts (e.g., starting conversations, building friendships and handling conflicts), (2) socialization frequency, and (3) social functioning and severity of ASD symptoms (according to teacher reports) were obtained. Based on the prior research on the outpatient (e.g., Laugeson et al. 2009, 2012; Mandelberg et al. 2014; Schohl et al. 2014; Yoo et al. 2014) and school-based (Laugeson et al. 2014) PEERS models, the ASD and CD students were expected to demonstrate significant post-intervention improvements across the three measures used to examine their social skills knowledge, social functioning and socialization frequency.
Methods
Participants
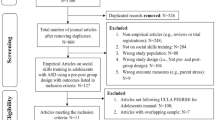
The original sample included 70 students with ASD and/or cognitive deficits between the ages of 15 and 21. However, 7 students were excluded from the final analyses because they did not attend any of the PEERS social skills meetings (n = 6), while one student changed schools during the study. The final sample included 63 students (77.8% male) between the ages of 16 and 21 (pre-test Mage = 18.70 years); this final sample was considerably larger than some of the other PEERS studies (e.g., Gardner et al. 2015; Mandelberg et al. 2014; Laugeson et al. 2012; Yoo et al. 2014). All students were recruited from a private school in a large metropolitan area (i.e., population greater than 3,000,000) that serviced students from the ages 4 to 21 who presented with a range of developmental difficulties, including ID and ASD. The young adults in this study attended a work-oriented training program, within the private school, whereby they developed specific applied academic, daily living and work skills needed during adulthood. Following ethics approval from this institution, parental consent was given for each student. All students who received parental consent also provided verbal assent to participate.
Students were separated into two groups for the analyses. The Autism Spectrum Disorder (ASD) group included students who presented with a diagnosis of ASD. The cognitive deficits (CD) group incorporated students who did not have an ASD diagnosis, but presented with other diagnoses and developmental challenges, including intellectual disabilities (mild and moderate) and learning disabilities. The cognitive functioning of all students in the CD group either fell in the intellectual disability (n = 26) or borderline ranges (n = 8). The level of cognitive functioning in the ASD group ranged from intellectual disability (n = 8) to borderline/low average (n = 21). Random assignment to these two groups was not required since participants were assigned to a group based on their prior diagnoses of a developmental disability (i.e., whether they were previously diagnosed with ASD or CD).
Measures
Intervention
Students attended two 45-min sessions a week over a period of 16-weeks that covered the material in the PEERS Curriculum for School-Based Professionals: Social Skills Training for Adolescents with Autism Spectrum Disorder (Laugeson 2014). This manual replaced the parent-focused model from the original treatment manual (Laugeson et al. 2009) with a more school-based, teacher-facilitated model. See Table 1 for an overview of the 16 session topics covered in the curriculum, along with the weekly homework assignments.
The 63 students were organized into four classroom instruction groups based on their age, with the groups having 11–18 students; each classroom group also included students from both the ASD and CD groups. For each PEERS lesson, a doctoral school psychology intern at the school served as the “instructor”, and the classroom teachers and teaching assistants served as the “coaches”. Since the PEERS school social skills program is designed to be run by school staff (e.g., educators, school counsellors) and other mental health professionals (e.g., psychologists, social workers and speech and language therapists), specific training beyond the detailed instructions and guides in the manual were not required. However, the doctoral school psychology student, who was being supervised by a licensed school psychologist, had several years of experience working with teens and young adults with developmental disabilities in clinical and school settings. The instructor was responsible for leading the two weekly PEERS sessions, as well as tracking student attendance, participation and homework completion. The same instructor was used to teach each classroom group to ensure that each student received the same instruction. The coaches participated in the role plays with the instructor, reminded the students of the PEERS homework tasks, encouraged student participation and sent home weekly summaries of the content being covered in the PEERS curriculum. Each lesson was taught according to the step-by-step outline in the PEERS manual. However, the instructor also used PowerPoint slides for each lesson to provide the students with additional visual information (step-by-step lists for each social behavior, videos and imagery) to further facilitate student engagement and comprehension of the material. Finally, students took home newsletters to their parents that summarized the social skills content and homework being covered that week in the PEERS curriculum.
The two weekly PEERS meetings included homework reviews, didactic lessons, role-play demonstrations and behavioral rehearsals. The instructor began the first weekly session by reviewing the homework from the previous week. These homework assignments were used to encourage students to practice the content from the weekly lessons in real-life situations; see Table 1 for the homework assignments for each week. In order to get credit for an assignment, students had to describe what they did in or outside school to fulfill the requirements for the homework. Next, the rules and steps of etiquette for each social behavior in the PEERS program were taught didactically by means of group discussions, videos, imagery and step-by-step lists. The instructor and coaches then modelled the social skills being taught, with the students later rehearsing the newly acquired social skills through structured socialization activities with each other. During the behavior rehearsals, the instructor and coaches provided the students with immediate feedback and recommendations.
Attendance and Level of Engagement
Student attendance and level of engagement was tracked for each PEERS lesson. Participation points were used to measure student engagement whereby each classroom group were encouraged to accumulate points through in-class participation and completing the homework assignments; the participation points for each classroom later went towards a large party at the end of the program. At the beginning of each weekly lesson, the instructor reminded the students about the end of program party, and the importance of completing the homework and participating in-class.
Pre- and Post-Test Measures
Students’ pre- and post-test social skill knowledge, frequency of social engagement, and the severity of their autism spectrum symptoms were evaluated to assess for potential treatment changes. The pre-test measures were completed 2 weeks before the start of the intervention, and the post-test measures were completed 2 weeks after the conclusion of the intervention. The following pre-test and post-test measures have been widely used by previous PEERS research (e.g., Laugeson et al. 2009, 2012, 2014) to examine for potential treatment changes.
First, the Test of Adolescent Social Skills Knowledge (TASSK; Laugeson and Frankel 2010) consisted of 30 multiple-choice questions that measured treatment changes in students’ knowledge of the social skills taught in the PEERS program. Higher scores on the TASSK reflected greater social skills knowledge. The coefficient alpha for this measure was 0.56, and this moderate level of consistency was deemed acceptable because of the large range of social skills topics examined on this measure (Laugeson et al. 2009). Second, the Quality of Socialization Questionnaire-Adolescent (QSQ-A; Laugeson and Frankel 2010), adapted from the Quality of Play Questionnaire (QPQ; Frankel and Mintz 2011), incorporated students’ self-reported number of hangouts (invited to or hosted) with their peers outside of school in the previous month, along with the names of the people who attended the hangouts. Higher QSQ-A scores indicated greater friendship involvement outside of school. Students completed the TASSK and QSQ-A questionnaires independently, but they were allowed to ask the instructor or coaches for assistance with reading and/or understanding the questions. The original QPQ questionnaire was developed following a factor analysis of 175 boys and girls (Laugeson et al. 2009). Nevertheless, since the students were only asked to report the number of hangouts they were invited to or hosted, there was no coefficient alpha provided by the questionnaire developer for these specific questions. Third, the classroom teachers completed the Social Responsiveness Scale—Second Edition (SRS-2): Adult (Relative/Other Report; Constantino and Gruber 2012) for each student in their class during the pre- and post-test phases of the study. The SRS-2 (adult version) is a 65-item rating scale that was used to evaluate the severity of autism spectrum symptoms as they occur in natural social settings. Higher SRS-2 scores suggested a higher number of social deficits and autism spectrum-related symptoms. The SRS-2 is a widely used clinical measure of ASD symptomology and social competency. In a recent review of the adult measure, Chan et al. (2017) found evidence of concurrent, convergent, predictive and discriminant validity of the SRS-2 factors.
Procedure
Two weeks prior to the start of the intervention, the students (TASSK and QSQ-A) and teachers (SRS-2) completed their respective pre-test measures. Afterwards, students attended two 45-min sessions a week for 16-weeks that covered the material in the PEERS curriculum. For each session, student attendance and engagement (in-class participation and homework completion) were recorded. Two-weeks following the conclusion of the PEERS curriculum, students and teachers completed the post-test measures.
Results
The statistical analyses and organization of the results is similar to recent PEERS studies with adolescents and young adults (Laugeson et al. 2015; McVey et al. 2016). As previously noted, the efficacy of the PEERS program was assessed by examining pre-test and post-test score differences across three outcome measures, namely TASSK test scores, self QSQ-A reports and teacher SRS-2 reports. First, preliminary analyses were conducted to examine outcome measure pre-test score differences between the CD and ASD groups, as well as to analyze the demographic (e.g., mean age and disability status) and program engagement (i.e., participation points and attendance) characteristics of the two groups. Second, pre- to post-test score comparisons on the three outcome measures were examined for the entire sample, with the data for the two treatment groups (CD and ASD) being combined for this analysis. Additionally, pre- to post-test comparisons on the outcome measures were conducted within the CD and ASD groups; thus, one comparison analysis only included participants in the CD group, and the second analysis only had participants in the ASD group. Third, pre- to post-test difference scores on the outcome measures were compared between the ASD and CD groups to determine if the groups differed in their response to the PEERS treatment.
Preliminary Results
Chi-Square analyses revealed no significant age or gender differences between the CD and ASD groups; however, as expected, the CD group included significantly more students with intellectual disabilities, χ2(1) = 15.06, p < .001 (see Table 2). Analyses were therefore collapsed across participant age and gender. With regards to the baseline measures, ANOVA analyses indicated significant group differences on the SRS-2 measures, which was expected. More specifically, the ASD group had significantly higher SRS-2 pre-test total scores than the CD group, F(1, 61) = 6.97, p = .01, including higher scores on the social awareness, social cognition, social communication, and restricted and repetitive behavior subscales (see Table 3). In contrast, there were no significant group differences on the TASSK and QSQ-A pre-test scores, as well as with the level of student engagement throughout the program. Overall, students attended an average of 66.6% of the PEERS weekly lessons, with no significant differences in the attendance rates between the ASD (64.9%) and CD (68.0%) groups. Students earned an average of 50.3% of the total participation points, with there being no significant differences between the ASD (47.8%) and CD (52.5%) groups. Lastly, there was no missing data for any of the pre-test or post-test variables. Table 2 provides the mean demographic characteristics of the CD and ASD groups, and Table 3 shows the mean dependent measure baseline scores (TASSK, QSQ-A and SRS-2 pre-test scores) and level of student engagement (attendance and participation points).
Within Group Outcome Comparisons
A one-way repeated measures ANOVA with a Greenhouse-Geisser correction was conducted to analyze differences on the TASSK, QSQ-A and SRS-2 (total) across the two time-points (pre-test vs. post-test) for the entire sample. TASSK scores differed significantly from pre-test to post-test, F(1, 62) = 135.69, p = .00, as students demonstrated significantly higher social skills knowledge on the post-test after completing the PEERS program. Conversely, SRS-2 (total) and QSQ-A scores for the total sample did not differ significantly from pre-test to post-test. Follow-up one-way repeated measures ANOVAs revealed no significant differences from pre-test to post-test on any of the SRS-2 subscales. Table 4 displays the mean pre-test and post-test TASSK, QSQ-A and SRS-2 scores for the entire sample.
Follow-up dependent measure t-tests (or paired sample t-tests) were conducted to analyze pre-to post-test score differences within the CD and ASD groups for each of the three outcome measures. Within the CD group, students performed significantly higher on the post-test TASSK measure (M = 19.29) when compared to their pre-test performance (M = 13.50), t(33) = − 8.96, p < .001. On the QSQ-A, the CD group also achieved a marginally significant increase in QSQ-A self-reported hang-outs from pre-test (M = 3.97) to post-test (M = 5.74), t(33) = − 1.98, p = .056. Within the ASD group, students scored significantly higher on the post-test TASSK measure (M = 19.17) than the pre-test (M = 14.31), t(28) = − 7.45, p < .001. Conversely, there were no significant pre- to post-test differences on the QSQ-A for the ASD group participants. Lastly, dependent measure t-tests revealed no significant pre-to post-test improvements on any of the SRS-2 scales within the ASD and CD groups.
Between Group Outcome Comparisons
To examine between group (CD vs. ASD) differences in participant response to the PEERS program, outcome measure scores were converted to difference scores (post-test minus pre-test score). A positive difference score indicated an improvement on the QSQ-A and TASSK, whereas a negative difference score signified an improvement on each of the SRS-2 subscales. There were no significant correlations found between the outcome measure differences scores according to student post-test age and program attendance percentage (see Table 5); nevertheless, TASSK difference scores were positively correlated with student engagement (participation and homework points) percentage (r = .32, p = .01).
A MANOVA analysis was conducted, with treatment group (CD versus ASD) as the independent variable and the outcome measure difference scores (QSQ-A, TASSK and SRS-2 total score) as the dependent variables. Overall, there were no statistically significant discrepancies in outcome measure difference scores between the two treatment groups, F (3, 59) = 2.27, p = .09; Wilk’s Λ = 0.90, partial η2 = 0.10. However, follow-up univariate ANOVA’s indicated significant discrepancies between treatment groups with respect to the QSQ-A differences scores, F (1, 61) = 4.40, p = .04. More specifically, students in the CD group had a greater increase in the number of hangouts they organized and/or were invited to from pre-test to post-test (M difference = 1.77, SD = 5.20) compared to the ASD group (M difference = − 1.07, SD = 5.52). Finally, findings from a second MANOVA indicated that there were no statistically significant discrepancies between treatment groups in difference scores on any of the SRS-2 subscales, F (5, 57) = 0.49, p = .79; Wilk’s Λ = 0.96, partial η2 = 0.04. Table 6 displays the mean pre-test versus post-test difference scores on the SRS-2, TASSK and QSQ-A for the CD and ASD groups.
Discussion
Group-based social skills interventions, particularly those that take place in a generalizable social setting (Laugeson et al. 2014), can be effective for improving the social functioning, knowledge and behaviors of children and youth (Camargo et al. 2014; Kaat and Lecavalier 2014; McMahon et al. 2013). The school-based PEERS curriculum (Laugeson 2014) also has the potential to be very effective, given that it is based on the successful outpatient PEERS model (e.g., Laugeson et al. 2009, 2012; Mandelberg et al. 2014; Schohl et al. 2014). While it expands on the outpatient model by being teacher-facilitated and takes place in the school environment, little research to date has specifically analyzed the potential benefits and limitations of this model (Laugeson et al. 2014). Further, there has been considerably less research on group-based interventions that are designed to improve the social functioning of young adults (Wong et al. 2015), and it is presently unclear whether the PEERS program can be used with individuals with lower intellectual functioning. Individuals with cognitive deficits also experience social deficits and challenges at home (Grey et al. 2015), and in the community and workplace (Nord et al. 2016); albeit at a lower severity to those with ASD (Brereton et al. 2006). Lastly, there is a need for more social intervention research with young adults, especially when considering that the social skills needed to function as an independent and mature adult in the community differ from those commonly practiced in child-based interventions. To address these gaps in the social intervention literature, the present study examined the efficacy of the school-based PEERS intervention with young adults who were diagnosed with ASD, and those with cognitive deficits.
The Current Findings
Overall, the current findings are both supported and contrasted by prior literature on the efficacy of the PEERS outpatient (Laugeson et al. 2012; Mandelberg et al. 2014; Schohl et al. 2014; Yoo et al. 2014) and school-based (Laugeson et al. 2014) programs with high functioning adolescents. In accordance with prior PEERS research, the one-way repeated measures ANOVA with a Greenhouse-Geisser correction, along with follow-up dependent measure t-tests, indicated that both the ASD and CD groups had significant increases in their TASSK social knowledge performance from pre-test to post-test. Thus, after participating in the 16-week school-based PEERS program, students demonstrated an improved knowledge of appropriate social and conversational etiquette, sportsmanship, and handling of negative peer interactions (e.g., teasing, arguments and bullying). Moreover, dependent measure t-tests revealed that students in the CD group demonstrated a marginally significant increase in post-test self-reported number of hangouts (invited and initiated) on the QSQ-A when compared to the pre-test. Conversely, there were no significant QSQ-A score improvements when analyzing just the ASD participants. Also, unexpectedly, there were no significant pre- to post-test treatment changes on the MANOVA and follow-up dependent measure t-test analyses for any of the SRS-2 teacher-reported subscales in both the ASD and CD groups (see Tables 4, 6).
The two unexpected findings, namely the lack of post-test improvements on the QSQ-A and SRS-2 for the ASD group, may have occurred for several reasons. First, results from the recent meta-analysis by Gates et al. (2017), which were consistent with prior studies (e.g., Rao et al. 2008), suggests that students with ASD have difficulty applying their enriched social knowledge, acquired in group social skill interventions, into real life settings. While there were large improvements to students’ social knowledge and task-based performance, there were much smaller positive effects for parent-, observer- and teacher-reports of the students’ actual social functioning (Gates et al. 2017). The current findings somewhat reinforce these concerns, as the students with ASD generally did not apply their increased social knowledge into real-life situations, at least according to their non-significant QSQ-A and SRS-2 post-test improvements. On the other hand, students with cognitive deficits responded more positively to the program given that they showed marginally significant improvements on the QSQ-A in their willingness to initiate and engage in social hangouts outside of school.
Second, it is worth highlighting that the lack of increase in SRS-2 post-test scores in the CD group is likely a result of the fact that they had low pre-test scores on this measure (M total score = 38.82; normal range); as a result, there was a low likelihood of any improvement on this measure to begin with. The ASD group also scored in the high-end of the normal range on the SRS-2 (M total score = 57.35), but their social functioning and ASD symptoms were rated as being significantly more severe than the CD group. The lower than expected pre-test SRS-2 scores may be a result of the fact that many of the students had attended the special education private school for several years, whereby they likely received more social skills training tailored to their developmental needs prior to this study compared to students with developmental disabilities in a general education setting. Further, the special education teachers, many of whom worked at this private school for several years, may have been comparing the social functioning of these students to their developmentally-similar classmates instead of the general population; thus, the severity of the students’ social deficits, especially for the ASD group, may have been diminished in the special educator teacher SRS-2 observations.
Third, whereas the current study included primarily young adults, the school-based PEERS curriculum (Laugeson 2014) was designed to mostly benefit adolescents under the age of 18. During data collection, the Program for the Education and Enrichment of Relational Skills for Young Adults (Laugeson and Frankel 2016) was published, which is an outpatient program specifically designed to help young adults (ages 18–35) develop and maintain friendships and romantic relationships. Results from pilot studies on this outpatient program have been very positive, as high-functioning ASD students demonstrated significant improvements in their social skill knowledge and applied social behaviors (Gantman et al. 2012; Laugeson et al. 2015; McVey et al. 2016).
The young adult program, while very similar to the school-based intervention in content, administration and structure (Laugeson and Frankel 2016), has a few unique features. In correspondence with the highly successful original teen outpatient program (Laugeson et al. 2009, 2012; Mandelberg et al. 2014; Schohl et al. 2014; Yoo et al. 2014), the young adult model includes concurrent parent information and support meetings (Laugeson and Frankel 2016). The increased parental involvement in the program, beyond the weekly content summary and homework newsletters in the school model, encourages parents to be more involved in their child’s social progress outside of school. By being well-informed about the specific skills being practiced each PEERS lesson, parents are better prepared to supervise their child’s social progress and provide effective and immediate social feedback. Heightened parental involvement would also likely increase students’ program attendance and completion of the important homework assignments. In the current study, students attended two-thirds (66.6%) of the instructional meetings and received 50.3% of participation points (i.e., in-class participation and homework completion). Based on prior PEERS literature (Laugeson et al. 2009, 2012, 2014; Mandelberg et al. 2014; Schohl et al. 2014; Yoo et al. 2014), it is likely that the expected increase in student attendance and engagement, proceeding from the improved parental involvement, could have resulted in higher post-test scores on the QSQ-A and SRS-2 measures for the ASD group in particular. At the same time, it is worth highlighting that the amount of program participation points achieved by the students in this study was not overly dissimilar to the 43.4% PEERS homework completion rate found in Yoo et al. (2014). Whereas, the other PEERS school-based study did not report the student engagement data (Laugeson et al. 2014).
Lastly, the young adult PEERS manual also covers some adult-specific topics that were not present in the school manual. For instance, participants in the young adult program receive three additional modules that discuss appropriate dating etiquette (Laugeson and Frankel 2016). Moreover, the teaching instruction and group discussions are more tailored to an adult audience. For these reasons, future research should utilize the young adult model to better understand the benefits of the PEERS intervention with the sample analyzed in this study.
Implications and Contributions
The findings from this study can inform parents, teachers, practitioners and school administrators who work with young adults with ASD and CD about the benefits and limitations of this school-based intervention. The current study was one of the first to analyze the efficacy of a school-based social skills intervention with teens and young adults. There is extensive literature available on the efficacy of individual and clinical-based interventions with young children with ASD (see Camargo et al. 2014; Granpeesheh et al. 2009; Wong et al. 2015, for reviews), particularly with respect to ABA therapeutic strategies. Nevertheless, many families have difficulty getting access to clinical therapy services (Jacobson and Mulick 2000; Parish et al. 2012; Sharpe and Baker 2007), whether that be due to financial, insurance, geographical (e.g., rural areas), time and/or educational (e.g., knowledge of available services) restraints. Specific social skills interventions that take place at school, such as the PEERS school-based model, can increase the accessibility of important and effective social skills training for students who do not have access to treatments outside of the school setting.
The current study was one of the few to examine whether a social skills intervention can be effectively implemented in a post-secondary vocational school setting. Vocational (or transitional) services and schools for young adults with disabilities have shown to be very beneficial for improving their future life (i.e., health, social and financial) and employment outcomes (e.g., Luecking et al. 2018). The students in this study, particularly those with CD, were able to directly apply their new social knowledge in both school and work settings. Furthermore, the current study utilized an instructor who had not received formalized PEERS training; although the primary instructor was a doctoral school psychology student who was being supervised by a licensed school psychologist. This generalizes to real school settings wherein the primary instructor of the PEERS program, (e.g., a teacher, guidance counselor or school psychologist), who likely had not received the formalized PEERS training, would utilize the manual to implement this intervention at their school.
Students with CD are often overlooked in the social skills literature. Notably, these students experience significant social challenges with respect to social communication, as well as with friendship initiation and maintenance (Orsmond et al. 2013; Taheri et al. 2016); these difficulties can result in increased feelings of loneliness and sadness, along with making them more vulnerable to mistreatment (e.g., bullying and abuse) by others (Jones et al. 2012; Zeedyk et al. 2014). Young adults are another relatively forgotten population in the social skills literature (Wong et al. 2015) who were included in this study. As previously noted, many students experiencing social deficits have not received the essential early social intervention (Wainer and Ingersoll 2015). At the same time, the social skills needed during adolescence and early adulthood differ compared to those used during childhood. By including teens and young adults with ASD or CD, the current study provides important information on the efficacy of a school-based intervention with these often overlooked populations. Our findings indicate that the PEERS intervention, which was initially designed for high-functioning children and teens with ASD, can also be effective for students with lower cognitive functioning. For this reason, students with CD, who often have not received the necessary social-skills intervention, can benefit from this accessible and generalizable treatment for improving their social knowledge and outcomes. Future research should examine whether other populations that experience social challenges can also benefit from this program, including those with ADHD (e.g., Gardner et al. 2015), conduct and oppositionality problems, as well as social anxiety.
From a theoretical standpoint, the current study provides further evidence that improving social knowledge alone does not necessarily result in increased social performance. While the ASD group achieved significantly higher social knowledge scores on the TASSK, this newly acquired knowledge did not result in improved social behaviors on the SRS-2 and increased friendship interactions; whereas, the students without ASD were better able to use their new skills to increase their social interactions outside of school. This finding reinforces the fact that students with ASD experience significant challenges with the important application component of skill building. Thus, social skills programs, such as PEERS, should ensure that the students are consistently applying their new skills outside of the program.
Concurrent parent meetings used in the clinical PEERS model, but absent in the school-model, is a potentially effective strategy for encouraging students to apply their new social knowledge outside of the program. These meetings help parents to be more cognizant of the specific skills being taught each week in the program. At the same time, these meetings encourage open discussion about potential solutions to the unique social problems each family is experiencing with their children. By engaging in these group talks, parents can learn from each other and develop social networks for themselves and their children that can continue after the program has concluded. Finally, parents are taught to be social coaches for their children to assist with the weekly socialization assignments, which in turn, increases the generalization of the social skills to natural social settings.
Previous PEERS research on the clinical model with children, teens and adults suggest that including these parent meetings can better encourage students with ASD to effectively apply their new social skills to their daily lives (Laugeson et al. 2009, 2012, 2014; Mandelberg et al. 2014; Schohl et al. 2014; Yoo et al. 2014). While they may be effective, these meetings may not be a feasible option for some schools due to time and resource restraints. Therefore, other methods for increasing parental involvement might include weekly email program summaries and homework reminders, in addition to the newsletters. Further, calling families of students with low homework completion can encourage these parents to help their children to practice the social skills at home. Finally, organizing a small number of parent meetings, such as during the standard parent-teacher meetings that take place each academic semester, may be more feasible than the weekly meetings for communicating directly with parents.
Directions for Future Research
There are other ways to expand and improve on the current methodology. Given that the current study took place in a school during school hours, it was not possible to acquire extensive data on each student’s social functioning in the home environment. Although parents were provided with weekly summaries for each PEERS lesson, the parents did not complete any of the pre-test or post-test measures due to ethical restrictions. Future research should therefore attempt to include parent measures to better understand changes in students’ social functioning outside of the school environment.
The current study modelled previous studies (e.g., Laugeson et al. 2009, 2012, 2014) by utilizing pre-test and post-test measures that evaluated the students’ social skills knowledge (TASSK; Laugeson and Frankel 2010), frequency of social engagement (QSQ-A; Laugeson and Frankel 2010,) and the severity of their social deficits and autism spectrum symptoms (SRS-2; Constantino and Gruber 2012). However, there are other indicators of social functioning that have been examined in previous PEERS research that were omitted from the current study due to time restraints, such as measures of students’ self-esteem and self-concept (e.g., Laugeson et al. 2014), behavior (e.g., Yoo et al. 2014), friendship quality (e.g., Gardner et al. 2015), and levels of social anxiety (e.g., Schohl et al. 2014). Additional measures of the students’ social functioning and emotional well-being would provide more detailed information on the overall efficacy of the PEERS program.
The current sample (N = 63) was considerably higher than other PEERS studies (e.g., Gardner et al. 2015; Mandelberg et al. 2014; Laugeson et al. 2012; Yoo et al. 2014), especially when considering the challenges associated with recruiting participants with specific clinical characteristics (i.e., those with ASD or CD). Nevertheless, a larger and more diverse sample would enable for a more in-depth examination of the benefits and limitations of this intervention. For example, having more female participants would permit for an examination of potential gender differences in the overall efficacy of the PEERS program, such as in the study by McVey et al. (2017). Further, including a more diverse sample of individuals with CD, such as those with severe IDs, would provide more information about whether PEERS can be used with those who possess severely limited verbal, nonverbal and adaptive skills.
The PEERS program includes a range of components that are based on evidenced-based ABA and cognitive behavioral therapy strategies (Laugeson and Park 2014), such as didactic social skills instruction, modelling, reinforcement, role-playing (good and bad), immediate performance feedback, concrete rules and steps, and socialization assignments that incorporate students applying their new social skills in a real-life setting. Prior research has assessed the benefits of each of these individual methods, but the PEERS program is one of the first published and manualized treatments (Laugeson 2014; Laugeson and Frankel 2010) that incorporates all these strategies together to provide children, teens and young adults with effective social skills instruction. The current study assessed the school-based PEERS program in its entirety. However, it was discovered that an important component of the clinical PEERS model that was absent in the school model (Laugeson and Frankel 2016), namely the weekly parent meetings, may have contributed to the lower improvements in ASD symptomology and friendship acquisition among those diagnosed with ASD. Thus, it was recommended that the school-based program increase parental involvement, in addition to the weekly newsletters, to ensure that the students are consistently practicing appropriate social interactions outside of school. For this reason, more research should be conducted that identifies which specific components of the PEERS treatment are the most effective and whether any additional modifications might be needed.
Conclusions
The current study was one of the first to examine the benefits and limitations of a school-based social skills group intervention, namely the PEERS school curriculum (Laugeson 2014), in groups of young adults with ASD and cognitive deficits. Pre- versus post-test comparisons indicated that the students in both the ASD and CD groups demonstrated significantly improved social skills knowledge on the TASSK assessment, especially for those with increased program participation and homework completion. Conversely there were no significant pre- to post-test improvements for both groups on the teacher SRS-2 observer report scores of the students’ social functioning and ASD symptom severity. However, these low SRS-2 post-test score improvements may have been a result of the already low SRS-2 pre-test scores, especially for the CD group. Lastly, there were no significant improvements on the QSQ-A measure of friendship participation for the ASD group. Nevertheless, the CD group did show a marginally significant increase in the number of hangouts they organized and/or were invited-to after completing the program.
Taken together, these findings suggest that students who possess low intellectual functioning can benefit from the PEERS school-based program, given their increased post-test social knowledge and participation in social interactions within the school setting. In contrast, the students with ASD did not show meaningful improvements in their application of their newly acquired social knowledge at school, which is a limitation highlighted in Gates et al. (2017) meta-analysis of group-based interventions for ASD populations. Based on recent findings (e.g., Laugeson et al. 2015; McVey et al. 2016), the new PEERS young adult curriculum (Laugeson and Frankel 2016) is likely more effective than the school-based model for improving the social functioning of young adults with ASD.
References
American Association on Intellectual and Developmental Disabilities. (2017). Definition of intellectual disability. http://aaidd.org/intellectual-disability/definition.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington: American Psychiatric Publishing.
Bailey, J. S., & Burch, M. R. (2017). Research methods in applied behavior analysis: Second edition. New York, NY: Routledge.
Brereton, A. V., Tonge, B. J., & Einfeld, S. L. (2006). Psychopathology in children and adolescents with autism compared to young people with intellectual disability. Journal of Autism and Developmental Disorders, 36(7), 863–870. https://doi.org/10.1007/s10803-006-0125-y.
Camargo, S. P. H., Rispoli, M., Ganz, J., Hong, E. R., Davis, H., & Mason, R. (2014). A review of the quality of behaviorally-based intervention research to improve social interaction skills of children with ASD in inclusive settings. Journal of Autism and Developmental Disorders, 44(9), 2096–2116. https://doi.org/10.1007/s10803-014-2060-7.
Chan, W., Smith, L. E., Hong, J., Greenberg, J. S., & Mailick, M. R. (2017). Validating the social responsiveness scale for adults with autism. Autism Research, 10(10), 1663–1671. https://doi.org/10.1002/aur.1813.
Constantino, J. N., & Gruber, C. P. (2012). Social responsiveness scale (SRS). Torrance: Western Psychological Services.
Cowan, R. J., & Allen, K. D. (2007). Using naturalistic procedures to enhance learning in individuals with autism: A focus on generalized teaching within the school setting. Psychology in the Schools, 44(7), 701–715. https://doi.org/10.1002/pits.20259.
Farley, M., Cottle, K. J., Bilder, D., Viskochil, J., Coon, H., & McMahon, W. (2018). Mid-life social outcomes for a population-based sample of adults with ASD. Autism Research, 11, 142–152. https://doi.org/10.1002/aur.1897.
Flynn, H. K., Felmlee, D. H., & Conger, R. D. (2017). The social context of adolescent friendships: Parents, peers, and romantic partners. Youth & Society, 49(5), 679–705. https://doi.org/10.1177/0044118X14559900.
Frankel, F., & Mintz, J. (2011). Maternal reports of play dates of clinic referred and community children. Journal of Child and Family Studies, 20, 623–630. https://doi.org/10.1007/s10826-010-9437-9.
Gantman, A., Kapp, S. K., Orenski, K., & Laugeson, E. A. (2012). Social skills training for young adults with high-functioning autism spectrum disorders: A randomized controlled pilot study. Journal of Autism and Developmental Disorders, 42(6), 1094–1103. https://doi.org/10.1007/s10803-011-1350-6.
Gardner, D. M., Gerdes, A. C., & Weinberger, K. (2015). Examination of a parent-assisted, friendship-building program for adolescents with ADHD. Journal of Attention Disorders. https://doi.org/10.1177/1087054715588188.
Gates, J. A., Kang, E., & Lerner, M. D. (2017). Efficacy of group social skills interventions for youth with autism spectrum disorder: A systematic review and meta-analysis. Clinical Psychology Review, 52, 164–181. https://doi.org/10.1016/j.cpr.2017.01.006.
Gilmore, L., & Cuskelly, M. (2014). Vulnerability to loneliness in people with intellectual disability: An explanatory model. Journal of Policy and Practice in Intellectual Disabilities, 11(3), 192–199. https://doi.org/10.1111/jppi.12089.
Gonring, K., Gerdes, A., & Denise, G. (2017). Program for the education and enrichment of relational skills: Parental outcomes with an ADHD sample. Child & Family Behavior Therapy, 39, 19–42. https://doi.org/10.1080/07317107.2016.1268003.
Granpeesheh, D., Tarbox, J., & Dixon, D. R. (2009). Applied behavior analytic interventions for children with autism: A description and review of treatment research. Annals of Clinical Psychiatry, 21(3), 162–173.
Grey, J. M., Griffith, G. M., Totsika, V., & Hastings, R. P. (2015). Families’ experiences of seeking out-of-home accommodation for their adult child with an intellectual disability. Journal of Policy and Practice in Intellectual Disabilities, 12, 47–57. https://doi.org/10.1111/jppi.12106.
Jacobson, J. W., & Mulick, J. A. (2000). System and cost research issues in treatments for people with autistic disorders. Journal of Autism and Developmental Disorders, 30(6), 585–593. https://doi.org/10.1023/A:1005691411255.
Jones, L., Bellis, M. A., Wood, S., Hughes, K., McCoy, E., Eckley, L., … Officer, A. (2012). Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. The Lancet, 380, 899–907. https://doi.org/10.1016/S0140-6736(12)60692-8.
Kaat, A. J., & Lecavalier, L. (2014). Group-based social skills treatment: A methodological review. Research in Autism Spectrum Disorders, 8, 15–24. https://doi.org/10.1016/j.rasd.2013.10.007.
Laugeson, E. A. (2014). The PEERS® curriculum for school-based professionals: Social skills training for adolescents with autism spectrum disorder. New York: Routledge.
Laugeson, E. A., Ellingsen, R., Sanderson, J., Tucci, L., & Bates, S. (2014). The ABC’s of teaching social skills to adolescents with autism spectrum disorder in the classroom: The UCLA PEERS® program. Journal of Autism and Developmental Disorders, 44, 2244–2256. https://doi.org/10.1007/s10803-014-2108-8.
Laugeson, E. A., & Frankel, F. (2010). Social skills for teenagers with developmental and autism spectrum disorder: The PEERS® treatment manual. New York: Routledge.
Laugeson, E. A., & Frankel, F. (2016). The PEERS treatment manual for young adults with autism spectrum disorder: Evidence-based social skills training. New York: Routledge.
Laugeson, E. A., Frankel, F., Gantman, A., Dillon, A. R., & Mogil, C. (2012). Evidence-based social skills training for adolescents with autism spectrum disorders: The UCLA PEERS® program. Journal of Autism and Developmental Disorders, 42, 1025–1036. https://doi.org/10.1007/s10803-011-1339-1.
Laugeson, E. A., Frankel, F., Mogil, C., & Dillon, A. R. (2009). Parent-assisted social skills training to improve friendships in teens with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 596–606. https://doi.org/10.1007/s10803-008-0664-5.
Laugeson, E. A., Gantman, A., Kapp, S. K., Orenski, K., & Ellingsen, R. (2015). A randomized controlled trial to improve social skills in young adults with autism spectrum disorder: The UCLA PEERS® program. Journal of Autism and Developmental Disorders, 45, 3978–3989. https://doi.org/10.1007/s10803-015-2504-8.
Laugeson, E. A., & Park, M. N. (2014). Using a CBT approach to teach social skills to adolescents with autism spectrum disorder and other social challenges: The PEERS® method. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 32, 84–97. https://doi.org/10.1007/s10942-014-0181-8.
Luecking, R. G., Fabian, E. S., Contreary, K., Honeycutt, T. C., & Luecking, D. M. (2018). Vocational rehabilitation outcomes for students participating in a model transition program. Rehabilitation Counseling Bulletin, 61(3), 154–163. https://doi.org/10.1177/0034355217713167.
Mandelberg, J., Laugeson, E. A., Cunningham, T. D., Ellingsen, R., Bates, S., & Frankel, F. (2014). Long-term treatment outcomes for parent-assisted social skills training for adolescents with autism spectrum disorders: The UCLA PEERS program. Journal of Mental Health Research in Intellectual Disabilities, 7, 45–73. https://doi.org/10.1080/19315864.2012.730600.
Mandell, D. S., Walrath, C. M., Manteuffel, B., Sgro, G., & Pinto-Martin, J. A. (2005). The prevalence and correlates of abuse among children with autism served in comprehensive community-based mental health settings. Child Abuse & Neglect, 29(12), 1359–1372. https://doi.org/10.1016/j.chiabu.2005.06.006.
Marriage, S., Wolverton, A., & Marriage, K. (2009). Autism spectrum disorder grown up: A chart review of adult functioning. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 18(4), 322–328.
Mazurek, M. O. (2014). Loneliness, friendship, and well-being in adults with autism spectrum disorders. Autism, 18(3), 223–232. https://doi.org/10.1177/1362361312474121.
McMahon, C. M., Lerner, M. D., & Britton, N. (2013). Group-based social skills interventions for adolescents with higher-functioning autism spectrum disorder: A review and looking to the future. Adolescent Health, Medicine and Therapeutics, 4, 23–38. https://doi.org/10.2147/AHMT.S25402.
McVey, A. J., Dolan, B. K., Willar, K. S., Pleiss, S., Karst, J. S., Casnar, C. L., … Van Hecke, A. V. (2016). A replication and extension of the PEERS for young adults social skills intervention: Examining effects on social skills and social anxiety in young adults with autism spectrum disorder. Journal of Autism and Developmental Disorders, 46, 3739–3754. https://doi.org/10.1007/s10803-016-2911-5.
McVey, A. J., Schiltz, H., Haendel, A., Dolan, B. K., Willar, K. S., Pleiss, S., … Van Hecke, A. V. (2017). Brief report: Does gender matter in intervention for ASD? Examining the impact of the PEERS social skills intervention on social behavior among females with ASD. Journal of Autism and Developmental Disorders, 47(7), 2282–2289. https://doi.org/10.1007/s10803-017-3121-5.
Nord, D. K., Stancliffe, R. J., Nye-Lengerman, K., & Hewitt, A. S. (2016). Employment in the community for people with and without autism: A comparative analysis. Research in Autism Spectrum Disorders, 24, 11–16. https://doi.org/10.1016/j.rasd.2015.12.013.
Orsmond, G. I., Shattuck, P. T., Cooper, B. P., Sterzing, P. R., & Anderson, K. A. (2013). Social participation among young adults with an autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(11), 2710–2719. https://doi.org/10.1007/s10803-013-1833-8.
Parish, S., Thomas, K., Rose, R., Kilany, M., & McConville, R. (2012). State insurance parity legislation for autism services and family financial burden. Intellectual and Developmental Disabilities, 50(3), 190–198. https://doi.org/10.1352/1934-9556-50.3.190.
Rao, P. A., Beidel, D. C., & Murray, M. J. (2008). Social skills interventions for children with Asperger’s syndrome or high-functioning autism: A review and recommendations. Journal of Autism and Developmental Disorders, 38(2), 353–361. https://doi.org/10.1007/s10803-007-0402-4.
Schohl, K. A., Van Hecke, A. V., Carson, A. M., Dolan, B., Karst, J., & Stevens, S. (2014). A replication and extension of the PEERS intervention: Examining effects on social skills and social anxiety in adolescents with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44, 532–545. https://doi.org/10.1007/s10803-013-1900-1.
Sharpe, D. L., & Baker, D. L. (2007). Financial issues associated with having a child with autism. Journal of Family and Economic Issues, 28(2), 247–264. https://doi.org/10.1007/s10834-007-9059-6.
Smith, K. R., & Matson, J. L. (2010). Social skills: Differences among adults with intellectual disabilities, co-morbid autism spectrum disorders and epilepsy. Research in Developmental Disabilities, 31(6), 1366–1372. https://doi.org/10.1016/j.ridd.2010.07.002.
Taheri, A., Perry, A., & Minnes, P. (2016). Examining the social participation of children and adolescents with Intellectual Disabilities and Autism Spectrum Disorder in relation to peers. Journal of Intellectual Disability Research, 60(5), 435–443. https://doi.org/10.1111/jir.12289.
Tipton, L. A., Christensen, L., & Blacher, J. (2013). Friendship quality in adolescents with and without an intellectual disability. Journal of Applied Research in Intellectual Disabilities, 26(6), 522–532. https://doi.org/10.1111/jar.12051.
Wainer, A. L., & Ingersoll, B. R. (2015). Increasing access to an ASD imitation intervention via a telehealth parent training program. Journal of Autism and Developmental Disorders, 45(12), 3877–3890. https://doi.org/10.1007/s10803-014-2186-7.
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., … Schultz, T. R. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. Journal of Autism and Developmental Disorders, 45(7), 1951–1966. https://doi.org/10.1007/s10803-014-2351-z.
Yoo, H. J., Bahn, G., Cho, I. H., Kim, E. K., Kim, J. H., Min, J. W., … Cho, S. (2014). A randomized controlled trial of the Korean version of the PEERS parent-assisted social skills training program for teens with ASD. Autism Research, 7, 145–161. https://doi.org/10.1002/aur.1354.
Zeedyk, S. M., Rodriguez, G., Tipton, L. A., Baker, B. L., & Blacher, J. (2014). Bullying of youth with autism spectrum disorder, intellectual disability, or typical development: Victim and parent perspectives. Research in Autism Spectrum Disorders, 8(9), 1173–1183. https://doi.org/10.1016/j.rasd.2014.06.001.
Acknowledgments
A special thank you to the many students, teachers and families who participated in this study. Finally, there were no personal or institutional conflicts of interest pertaining to the subject matter or materials discussed in this manuscript.
Author information
Authors and Affiliations
Contributions
Both authors contributed greatly to the completion of this manuscript. AC conceived the original idea for this study. AC and JW were both involved in the design and data collection of this study. JW interpreted the data and wrote the first full draft of the manuscript; JW consulted with AC during the writing of the first draft. Furthermore, AC and JW were both involved in the editing of this manuscript.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wyman, J., Claro, A. The UCLA PEERS School-Based Program: Treatment Outcomes for Improving Social Functioning in Adolescents and Young Adults with Autism Spectrum Disorder and Those with Cognitive Deficits. J Autism Dev Disord 50, 1907–1920 (2020). https://doi.org/10.1007/s10803-019-03943-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-019-03943-z