
Abstract
Investigate how novice drivers with autism spectrum disorder (ASD) differ from experienced drivers and whether virtual reality driving simulation training (VRDST) improves ASD driving performance. 51 novice ASD drivers (mean age 17.96 years, 78% male) were randomized to routine training (RT) or one of three types of VRDST (8–12 sessions). All participants followed DMV behind-the-wheel training guidelines for earning a driver’s license. Participants were assessed pre- and post-training for driving-specific executive function (EF) abilities and tactical driving skills. ASD drivers showed worse baseline EF and driving skills than experienced drivers. At post-assessment, VRDST significantly improved driving and EF performance over RT. This study demonstrated feasibility and potential efficacy of VRDST for novice ASD drivers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Virtual Reality Driving Simulation Training (VRDST)
Virtual reality driving simulation (VRDS), which involves real-time interaction with a driving console and a virtual world (see Fig. 1), offers a safe environment to assess and provide targeted interventions for individuals who are in the process of obtaining a driver’s license (Adler et al. 1995; Brooks et al. 2013; Hoffman et al. 2002). Applied to the needs of adolescents and young adults with an autism spectrum disorder (ASD), the use of VRDS training (VRDST) allows for repetition in a controlled and safe environment, naturalistic settings in a primarily visual world, modified scenarios to foster generalization of learned skills, an individualized approach, different modes of computer interaction, reduced boredom and fatigue, and the inclusion of eye-tracking (Bölte 2004; Parsons et al. 2004; Strickland 1997). The latter allows feedback about gaze, which provides potentially important training benefits because gaze patterns reflect drivers’ competence and gaze training increases competence (Malik et al. 2009; Pradhan et al. 2007).

Simulator displaying a road hazard (motorcyclist emerging from behind traffic) requiring a defensive maneuver
Virtual reality driving simulation training has already shown improvement in driving performance and successful prediction of future driving mishaps (collisions and citations for moving vehicle violations). For example, VRDST improved driving performance in elderly drivers (Casutt et al. 2014) and novice drivers learning to drive (Cox et al. 2009), and improved visual search for hazards in young novice drivers (Vlakveld et al. 2011). Furthermore, VRDST has proved useful with patient populations. For instance, VRDST improved driving performance in individuals recovering from stroke (Akinwuntan et al. 2005) and in military personnel recovering from traumatic brain injury (Cox et al. 2010). These military personnel also experienced a reduction in road rage and risky driving. Performance on VRDS can predict future driving mishaps of both novice drivers (Cox et al. 2015b) and senior drivers (Cox et al. 1999). Consequently, employment of VRDS holds promise in the identification of driving challenges specific to those with ASD and in training general driving skills and targeted ASD-specific driving challenges.
Driving with Autism Spectrum Disorder
Only a limited number of studies have used VRDS to assess driving skills in ASD participants. On-road studies have never been reported. This gap in the research is surprising given the critical role that motor vehicle driving plays in adolescent development and functional independence. For individuals with and without ASD, acquiring a driver’s license is associated with increased participation in full-time academic programs, plans to attend college, and a history of paid employment (Huang et al. 2012). A recent upsurge in research on motor vehicle driving for individuals with ASD reflects an improved understanding of this disorder’s lifetime course and changing functional impairments across development (Classen and Monahan 2013; Classen et al. 2013; Cox et al. 2012; Huang et al. 2012; Reimer et al. 2013; Sheppard et al. 2010). While many individuals with ASD have secured a driver’s license and are able to safely operate a motor vehicle, emerging research indicates that the acquisition of safe driving skills is often difficult for this population (Classen et al. 2013; Cox et al. 2012; Huang et al. 2012; Ross et al. 2015b). Therefore, individuals with ASD are less likely than their peers to acquire a driver’s license. If they do acquire a license, they obtain it significantly later (Cox et al. 2012; Daly et al. 2014).
Difficulties in learning to drive may be caused by the negative interference of characteristics that are often associated with ASD. For example, executive functioning difficulties (reflected in limited self-monitoring, creativity, mental flexibility, and planning abilities) could cause driving to be stressful and dangerous (Ross et al. 2015b). In support, executive functioning has been related to driving performance in adolescents and young adults with ASD (Cox et al. 2016). It has also been related to driving performance in other populations, such as neuro-typical adolescents and young adults (Lambert et al. 2014; Mäntylä et al. 2009; Ross et al. 2015a), the elderly (Aksan et al. 2012; Freund et al. 2008), and adults with ADHD (Reimer et al. 2006). Furthermore, executive functioning training has been shown to transfer to driving performance. For example, computer-based cognitive training was found to be predictive of improvements in motor vehicle collisions in elderly drivers (Ball et al. 2010; Cassavaugh and Kramer 2009).
In regard to hazard perception, it has been suggested that adolescents with ASD might be less likely to identify socially relevant road hazards, such as pedestrians (Sheppard et al. 2010). A subsequent study from the same group suggests a more general attentional process in which individuals with ASD may distribute and direct their attention differently to road hazards, indicating subtle orienting differences (Sheppard et al. 2016). Furthermore, they are less likely to monitor all relevant visual fields while driving (Reimer et al. 2013). An experimental study using eye-tracking technology found that when young male adults were distracted by a mobile phone, both the ASD and control groups increased their focus on the road ahead, therefore paying less attention to the overall driving environment, such as the surrounding traffic. The ASD group especially paid less attention to traffic (Reimer et al. 2013). A study from Wade et al. (2014) replicated these results. They found that the gaze from a group of adolescent ASD drivers was higher in the vertical direction and toward the right in the horizontal direction during simulated driving.
A few studies indicate that adolescents and young adults with ASD face additional difficulties when learning to drive. Adolescents with ASD have difficulties with shifting their attention, sequential task performance, and the integration and coordination of visuomotor responses. During simulated driving, they performed worse than healthy controls on lane maintenance, visual scanning, speed regulation, signaling, and adjusting to stimuli (Classen et al. 2013; Monahan et al. 2013).
To further complicate the matter, great variability is present among the ASD population. The relationship between ASD and driving might not always be negative, such as when a tendency for perfectionism could be considered beneficial when learning to drive (Ross et al. 2015b). Developing effective driver-training programs is critical to improving functional outcomes and promoting independence of adolescents and young adults with ASD.
There was no literature available on using VRDST to improve the driving performance of novice drivers diagnosed with ASD. Therefore, this study is the first to investigate how novice ASD drivers differ from “safe” drivers with respect to driving-specific measures of executive functioning (EF). VRDST options that move novice ASD drivers closer in performance to routine drivers were also explored.
Hypotheses Tested
This study investigated four main hypotheses. (1) Novice drivers with ASD will perform worse on general driving skills and working memory than experienced drivers. (2) VRDST will lead to improved general driving performance on a virtual reality driving simulator. (3) VRDST focused on driving-relevant EF will improve that ability. (4) VRDST can be enhanced by adding non-human automated feedback and/or eye-tracking feedback.
Methods
Overview
In this multi-center study, a total sample of 51 ASD individuals (U.Va.; n = 25, mean age = 17.83, 87.5% male, and U.I.; n = 26, mean age = 18.08, 73.1% male) were randomized to one of four conditions (Routine Training or one of three variations of VRDST) for 3 months. All participants had earned their learner’s permit but not their driver’s license. Driving-specific EF and general tactical assessments occurred at baseline and after 3 months of training.
Facilities
The commercially available Driver Guidance System (DGS-78) VRDS is a realistic driver’s cockpit with side- and rear-view mirrors. The driver’s view is projected onto a 2.44 m (8 ft) diameter, 210° curved screen (Fig. 1). Driving performance on this simulator can differentiate a number of groups, such as novice drivers with and without ASD (Cox et al. 2016), and drivers with corrected vs. uncorrected astigmatism (Cox et al. 2015a). Simulator performance also predicted future driving mishaps during the first 6 months of independent driving (Cox et al. 2015b). Finally, training on the simulator improved on-road driving of neuro-typical novice drivers (Cox et al. 2009).
This VRDS has two assessment capabilities: driving-specific executive functioning (EF) abilities and general tactical skills (Cox et al. 2016). EF tests were modeled after traditional neuropsychological tests, e.g., dual tasking, response inhibition, and working memory (see Table 1 [Table 1 located between next paragraph and paragraph beginning “Tactical testing”] for a description). Tests included driving-relevant stimuli, responses, and context. This allowed for enhancement of ecological validity. All tests used the same environment, thus reducing re-adaptation from one test to another. The participant drove down the middle lane of a three-lane highway with the simulator maintaining a constant distance from a lead car at 56.33 km/h (35 mph). To equate task instructions, all participants heard the same instructions, delivered at the same point in the task by the simulator’s synthetic voice. Details of this testing method have been published previously (Cox et al. 2016, 2015a).
All three EF abilities tested have been previously linked to driving (Cascio et al. 2014; Cassavaugh and Kramer 2009; Cox et al. 2016; Ross et al. 2014, 2015a). Dual tasking refers to the simultaneous execution of tasks. Response inhibition assesses the ability to suppress the processing, activation, or expression of information (or action) that would otherwise interfere with the attainment of a desired cognitive or behavioral goal (Dempster 1992; Hofmann et al. 2012). Working memory is a limited capacity system responsible for the temporary storage, rehearsal, updating, and mental manipulation of information for use in guiding behavior (Baddeley 2007). The working memory test was a complex span task modeled after the automated operation span task (Conway et al. 2005; Unsworth et al. 2005) and provided an index of overall working memory function. All of the EF tests placed demands on the same stimulus modality – vision. An EF composite score was created from the primary variables of all three tests (see Table 1). Scores were first converted to z-scores to allow a common metric and then were summed. Thus, the composite score was an overall reflection of EF driving abilities. A composite score of “0” was average, while a negative composite score was below average.
Tactical testing followed the framework from Michon (1985) that involved maneuvering a vehicle while negotiating different road and traffic environments and situations (Dickerson and Bédard 2014). It is analogous to an on-road test of driving skills, but performed in a safe, reliable, yet challenging virtual world. The tactical test involved driving on a standardized route that included 4.2 km (2.6 mi) of rural, 6.4 km (4 mi) of highway, and 3.2 km (2 mi) of urban roads. Drivers negotiated realistic roads with anticipated and unanticipated signal, traffic, and hazard demands. To avoid practice effects, a different tactical course was used for the pre- and post-assessments, but both were similar in mileage and degree of challenge.
Fifteen tactical variables, which included swerving, rolling stops, speeding, and collisions, were monitored throughout the routes and contributed to a tactical driving composite score (see Table 2 [Table 2 located after this paragraph and before Driver Training heading]; Cox et al. 2015b, 2016). Variable selection was based on a previous assessment of the relationship between variables and crash history of neuro-typical experienced drivers, as well as prior experience with patient groups that involved the selection of variables that readily distinguished between groups while being related to traffic safety. The tactical composite score was calculated similarly to the EF composite score but incorporated tactical variables. Past research has demonstrated the usefulness of a tactical composite score as a valid overall measure of driving performance. For example, tactical composite scores predicted future driving collisions of seniors (Cox et al. 1999), differentiated drivers with and without ADHD (Cox et al. 2000), and predicted on-road driving performance (Cox et al. 2010) and future driving mishaps of novice drivers during their first 6 months of independent driving (Cox et al. 2015a, b). The tactical composite score was the primary VRDS outcome variable.
Driver Training
Routine training (RT) involved giving participating families the state-specific DMV training manual and instructing them to follow the training program detailed in the manual. This included a tracking sheet to document supervised on-road driving experience.
Standard VRDST involved a minimum of eight and a maximum of twelve 1-hour sessions, depending on how quickly the participant progressed through the VRDST modules (see Table 3 for average number of sessions) [Table 3 located before Comparison Group heading, a few pages down, after the paragraph beginning “Requiring a learner’s permit…”]. Within a training session, the focus alternated between EF driving deficits identified during the baseline assessment and tactical driving skills. Training was a mastery-based program, meaning a participant did not progress to a subsequent stage of training until mastering the earlier training module. During each session, the trainer would first “get behind the wheel” to demonstrate the task to the participant, and then monitor participant performance while providing continual positive verbal feedback. The training stages were as follows:
-
1.
Reviewing pre-assessment, identifying deficits
-
2.
Maintaining lane position on straight roads, curvy roads, and in turns
-
3.
Braking, stopping, and speed maintenance
-
4.
Refining lane and speed maintenance with executive functioning tests
-
5.
First generalization of skills on a rural and urban route with no traffic
-
6.
Use of mirrors and turn signals
-
7.
Hazard detection
-
8.
Multi-tasking
-
9.
Navigating traffic
-
10.
Second generalization of skills on a rural and urban route with traffic
To ensure treatment fidelity across sites and trainers, a structured trainer manual was developed that detailed each step of the training procedure. This manual is available upon request.
Automated VRDST was identical to Standard VRDST, only the simulator’s computerized voice provided real-time auditory feedback (e.g., “too fast”, “did not stop”, “wide turn”, “tailgating”) instead of the trainer when the participant transgressed tactical thresholds. The variables for which thresholds were set included:
-
Driving too fast (for specific road segments [e.g., open road with no instructions to change lane or other deceleration instructions] and against a normative population)
-
Driving too slow (for specific road segment and against a normative population)
-
Swerving
-
Rolling stops
-
Missed stops
-
Not using turn signals (lane change and turning)
-
Position in lane (for specific road segment and against a normative population)
-
Turning too wide (for specific road segment and against a normative population)
-
Turning too tight (for specific road segment and against a normative population)
-
Tailgating
-
Bumps and crashes
Eye-tracking VRDST incorporated eye-tracking (Mobile Eye XG, Applied Science Laboratories; Bedford, MA) into Standard VRDST in various ways. First, a member of the research team produced videos of the eye-view (three per module) while the driving tasks were performed. This largely replaced the trainer demonstration from Standard VRDST. These videos were produced using the eye-tracker. Two feedback options modeled exactly where the participant should look while driving (see Fig. 2). After viewing the model video, the participant wore the eye-tracker “glasses” during his/her drives, from which a video of their eye gaze during driving was produced for review (see Fig. 2). Once a segment was completed, the trainer and participant would review performance. This was particularly helpful around intersections. For example, the trainer could clearly see if a failure to stop occurred because the participant never scanned for a stop sign or checked the state of a stoplight, or because s/he had checked but either ignored or misinterpreted the signal.

Two types of eye-tracking feedback: driver view (top red dot) and aerial view (bottom red line). The thin horizontal bar above the dashboard represents the position of the integrated eye-tracker. (Color figure online)
Procedure
Assessment Phase
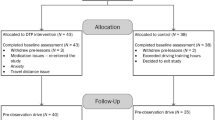
Interested adolescents and their parents came to the driving laboratory and were escorted to a private room where they were verbally informed about the study and consented/assented once all their questions were addressed. Informed consent was obtained from all participants in the study. Participants were then screened for inclusion/exclusion criteria. Parents completed a short demographic survey that included specific questions about their child’s diagnosis (including the presence of comorbid disorders such as depression or anxiety), the SRS-2, the BRIEF, and the BASC-2. Parent responses on the SRS-2 were used to confirm a diagnosis of ASD. A score greater than 1.5 standard deviations beyond the normative mean was required. While parents completed the questionnaires, participants were assessed on the VRDS with both EF and tactical tests. Post-assessment was identical to pre-assessment in terms of the VRDS testing, except a different tactical course was used for the pre- and post-assessments (see Fig. 3).

Study flow chart
Training Phase
In this exploratory quasi-experimental design, 28 participants were randomized to either Standard or Automated VRDST during the first year. This allowed for determination of the optimal training condition on which to add eye-tracking in the following year. Since Automated VRDST was not found to be superior to Standard VRDST, eye-tracking was added to Standard VRDST. During the second year, 23 participants were recruited and assigned to the RT group. After completing pre-assessment, 3 months of RT, and post-assessment, 18 of these 23 participants were subsequently crossed over to Eye-Tracking VRDST. The post-assessment of RT served as the pre-assessment for Eye-Tracking VRDST.
This design allowed identification of whether automated feedback was beneficial via analysis of the previous year’s data before moving on to the addition of eye-tracking. It also minimized the amount of time RT participants had to wait before receiving training, while controlling for season of training and on-road driving (summer). Participant recruitment took place during the spring of 2013 and 2014. Training took place during the summer and fall of each year because the availability of adolescents was highest then and the weather and road conditions were similar across sites.
Participants
This multi-center study recruited participants from the catchment areas surrounding the two sites through newspaper and internet advertisements, flyers, and public announcements. Participants had to meet the following inclusion criteria:
-
Diagnosed with ASD (including Asperger’s, Autistic Disorder, PDD, or PDD-NOS) by a licensed clinician
-
Parents’ rating of child was more than 1.5 standard deviations above the normative mean on screening questionnaires
-
Had a valid learner’s permit
-
Age 15.5–25 years
-
Able to operate the driving simulator without simulation sickness
-
Able to attend up to 14 study visits (two assessment visits, and up to 12 training sessions) in a 3-month period
-
Parent or legal guardian able and willing to provide in-car driving training at home
No participants were disallowed because of the following exclusion criteria:
-
Not able to understand written and spoken English
-
Diagnosis of intellectual disability (ID) or mental retardation (MR)
-
Brain injury
-
Diagnosed genetic disorder or chromosomal abnormality (e.g., Down Syndrome, Prader–Willi Syndrome, Fragile X, Angelman Syndrome)
-
Severe physical, medical, or psychiatric condition that impairs driving ability (e.g., muscular dystrophy, psychosis)
Requiring a learner’s permit assured basic levels of driving knowledge and intellectual capabilities. Requiring on-road training opportunities served multiple purposes, including allowing the transfer of training from the virtual to the physical world and partially satisfying the DMV requirements toward securing an independent driver’s license. Five participants dropped out of the study due to scheduling difficulties or family events. One participant dropped out due to simulation sickness. The study groups did not differ on demographic variables (Table 3).
Comparison Group
This study compared novice ASD drivers to DMV normative drivers in terms of magnitude of difference of ASD to normative data. DMV drivers were licensed, between the ages of 25 and 75 (N = 333, 73% male, mean age = 40.0 years), had come to the DMV for general business purposes (e.g., registering a car), and voluntarily drove the VRDS once for 60 min. The age range of 25–75 was taken as a conservative normative group because the accident rate per miles driven is relatively flat across this age range (Massie et al. 1995).
The ASD drivers were compared to this group rather than a neuro-typical novice driver group for several reasons. The comparison of ASD to neuro-typical novice drivers has previously been reported (Cox et al. 2016). It is very difficult to age match the ASD novice drivers to neuro-typical novice drivers because the ASD group is generally older than the neuro-typical novice driver. Neuro-typical novice drivers are a high-risk group and it is preferential to not have the ASD novice drivers emulate a high-risk group. Additionally, the ASD novice drivers have to “stack up” to routine safe drivers, and any deficits relative to this group need to be identified and significantly rectified before engaging in independent driving.
Results
Hypothesis 1: Novice Drivers with ASD Perform Worse on General Tactical Driving and Working Memory than Experienced Drivers
Using the DMV normative comparison group’s means (µ) and standard deviations (SD), z-scores were calculated for the individual EF and tactical variables. These were then summed into composite scores. Independent sample t-tests were executed. If the Levene’s test indicated that the variances were not equal, the corrected parameters were reported. In addition to testing the hypothesis, exploratory analyses were conducted on individual performance variables to indicate which ones differentiated ASD drivers from the normative sample and should be considered for use in future training programs.
Consistent with the hypothesis, ASD drivers performed worse than normative drivers in terms of overall tactical composite score (t = −4.54, p < 0.001) and EF composite score (t = −2.85, p < 0.01), (see Table 4) [Table 4 located between the end of this paragraph and Hypothesis 2 heading]. Exploratory analyses indicated that in terms of driving skills, ASD drivers performed worse on nearly every individual tactical driving variable. However, both groups had a similar number of rolling stops at stop signs and demonstrated similar control of the accelerator and speed variability. In terms of EF scores, ASD drivers performed worse on the number of correct responses for both dual tasking and response inhibition and the secondary variable of foot/leg reaction time during both dual tasking and response inhibition. ASD drivers did not differ in terms of primary or secondary measures of working memory.
Hypothesis 2: VRDST Leads to Better General Tactical Driving Performance
To evaluate the effects of VRDST on tactical driving performance, the pre- and post-assessment scores were transformed to z-scores based on the mean and standard deviation from the ASD group on both assessments and then summed to produce the tactical composite scores. Transformation to z-scores for the normative group was not possible because the unique post-assessment tactical drive differed from the pre-assessment drive and no DMV normative data existed for this drive. Using the composite scores, a 1 × 4 ANCOVA (between-subjects factor: group) determined the difference between the groups (RT, Standard, Automated, Eye-Tracking) on the post-assessment while controlling for baseline. The results were Bonferroni-corrected.
The general tactical composite score improved differentially across groups (F = 5.70, p < 0.010), and a significant covariate (F = 54.83, p < 0.001, β = 0.50) indicated that better baseline performance was associated with better post-assessment performance. Contrasts revealed that both Standard and Automated VRDST were superior to RT. Exploratory analyses indicated specific variable scores differed significantly across groups, albeit this differed per measure (see Table 5) [Table 5 located after this paragraph and before Hypothesis 3 heading]. In terms of overall performance, Standard and Automated VRDST were superior to RT, primarily due to better steering (less crossing the midline and swerving) and speed control (less tailgating, speeding, and reckless driving).
Hypothesis 3: VRDST Focusing on Driving-Relevant EF Improves that Ability
The same EF tests were used at both pre- and post-assessments, so z-score transformations were again based on the normative sample to investigate the group effect relative to the normative sample. Scores from participants who used double feet (i.e., right foot on accelerator and left foot on brake pedal) to respond or who performed poorly (>3 SD below mean) were replaced with “-3”. As with hypothesis 2, post-assessment scores for both primary and secondary variables were entered into 1 × 4 ANCOVAs with baseline scores serving as the covariate to determine whether post-assessment EF was related to baseline performance. Because there was no automated feedback during EF training, Standard and Automated VRDST subjects were combined into a single group. VRDST was not associated with greater improvement on EF than RT (F = 1.04, p = 0.36). A priori power analysis (Faul et al. 2007) demonstrated that a reasonably larger sample size would not find a significant effect.
A significant covariate (F = 17.13, p < 0.01, β = 0.50) indicated that better baseline performance was associated with better post-assessment performance. As Table 6 [located after this paragraph and before Hypothesis 4 heading] indicates, few group differences were found for the improvement of driving-relevant EF. Standard and Automated VRDST were superior to RT only when considering the secondary variable of working memory - arm/hand reaction time.
Hypothesis 4: VRDST can be Enhanced by Adding Automated Feedback and/or Eye-Tracking
There were no significant contrasts across the three VRDST groups. Only the Standard and Automated groups were significantly superior to RT on the tactical simulator tests. Additionally, Standard VRDST demonstrated the greatest improvement in both primary and secondary EF (see Table 6).
Discussion
As hypothesized, this study demonstrated that ASD novice drivers differed from experienced drivers without ASD on the tactical test, in which subjects drove through a virtual world while they negotiated routine and unanticipated traffic and road demands. This replicated findings that compared novice ASD to novice neuro-typical drivers (Cox et al. 2016). However, in the current study the tactical composite score of −29.71 for novice ASD drivers was nearly six standard deviations below normative data, which indicated that our ASD novice drivers were extremely deficient in general driving skills. Tactical skills are based heavily on driving experience (Dickerson and Bédard 2014) and predict future collisions of novice drivers (Cox et al. 2015b).
Given that EF typically does not mature until around age 25 (Lambert et al. 2014) and that ASD can be associated with deficits in EF (Ross et al. 2015b), it was hypothesized that our ASD sample would differ from our older and more experienced sample. The data did confirm such differences when a composite score of EF was considered. However, with a difference of less than one standard deviation, the current findings that novice ASD drivers differed from older and experienced drivers in terms of dual tasking and response inhibition may reflect maturation differences between the ASD and experienced driver groups rather than autism per se.
Standard and Automated VRDST differentially improved tactical performance relative to RT, which suggests that VRDST can improve basic driving skills. Two prior studies support the significance of this by demonstrating that tactical test composite scores both predicted future collisions of senior drivers (Cox et al. 1999) and future driving mishaps of newly licensed drivers (Cox et al. 2015b).
Eye-Tracking VRDST did not significantly improve tactical performance relative to RT, contrary to the Standard and Automated VRDST groups. This lack of significance may be due to the sometimes obtrusive or irritating nature of wearing eye-tracking glasses. This could be corrected in future studies by using dash-mounted eye trackers. It was not surprising that VRDST did not differentially improve EF since initial deficits in this parameter were minimal.
The very significant covariates for post-training assessments indicate that those who initially performed well performed better after training. This suggests that very poor baseline performance may identify a driving candidate who might not improve significantly in the short term. If follow-up research confirms this, then poor initial VRDS performance may suggest that further training might not be worth pursuing at this time, or that more intensive training either with VRDS or in-car methods may be needed.
While a pioneering effort, this study could have been improved in a variety of areas. A larger sample could have been recruited. Greater emphasis and documentation of on-road training during the 3-month training interval could have been encouraged and analyzed. A control group of neuro-typical drivers would have allowed for the differentiation of the effects of ASD from that of being a novice driver. Having normative data for the post-assessment tactical score would have allowed determination of how much training moved the ASD sample toward safer driver performance.
Despite these limitations, this initial simulation training study demonstrated the feasibility of VRDST for novice drivers with ASD and identified areas of future research. In addition to correcting the above issues, applying a fixed treatment protocol (e.g., eye-tracking) to all participants may have been counterproductive. For example, some participants apparently benefitted from eye-tracking feedback, while others did not have initial difficulty with gaze direction or duration. Some participants appreciated the computer-generated automated feedback while others preferred a human instructor because they found the computer voice aggravating and distracting, interfering with skill acquisition. Consistent with the training manual, where participants spend as little or as much time training on specific skills as needed, the use of eye-tracking and automated feedback could also be personalized. VRDST holds significant promise to aid individuals with ASD in improving tactical driving performance, but further research needs to focus on how best to generalize VRDST skills to real world driving.
References
Adler, L. A., Resnick, S., Kunz, M., & Devinsky, O. (1995). Open-label trial of venlafaxine in adults with attention deficit disorder. Psychopharmacology Bulletin, 31(4), 785–788.
Akinwuntan, A. E., Weerdt, W. D., Feys, H., Pauwels, J., Baten, G., Arno, P., et al. (2005). Effect of simulator training on driving after stroke: A randomized controlled trial. Neurology, 65, 843–850.
Aksan, N., Anderson, S. W., Dawson, J. D., Johnson, A. M., Uc, E. Y., & Rizzo, M. (2012). Cognitive functioning predicts driver safety on road tests 1 and 2 years later. Journal of the American Geriatrics Society, 60, 99–105. doi:10.1111/j.1532-5415.2011.03739.x.
Baddeley, A. (2007). Working memory, thought, and action. New York: Oxford University.
Ball, K., Edwards, J. D., Ross, L. A., & McGwin, G. (2010). Cognitive training decreases motor vehicle collision involvement of older drivers. Journal of the American Geriatrics Society, 58(11), 2107–2113. doi:10.1111/j.1532-5415.2010.03138.x.
Bölte, S. (2004). Computer-based intervention in autism spectrum disorders. In O. T. Ryaskin (Ed.), Focus on autism research (pp. 247–260). New York: Nova Science.
Brooks, J. O., Mossey, E., M., Collins, J. C., & Tyler, P. (2013). An exploratory investigation: are driving simulators appropriate to teach pre-driving skills to young adults with intellectual disabilities? British Journal of Learning Disabilities, 42(2), 204–213.
Cascio, C. N., Carp, J., OʼDonnell, M. B., Tinney, F. J., Bingham, R. C., Shope, J. T., & Falk, E. B. (2014). Buffering social influence: neural correlates of response inhibition predict driving safety in the presence of a peer. Journal of Cognitive Neuroscience, 27(1), 83–95.
Cassavaugh, N. D., & Kramer, A. F. (2009). Transfer of computer-based training to simulated driving in older adults. Applied Ergonomics, 40(5), 943–952.
Casutt, G., Theill, N., Martin, M., Keller, M., & Jäncke, L. (2014). The drive-wise project: driving simulator training increases real driving performance in healthy older drivers. Frontiers in Aging Neuroscience, 6(85). doi:10.3389/fnagi.2014.00085.
Classen, S., & Monahan, M. (2013). Evidence-based review on interventions and determinants of driving performance in teens with attention deficit hyperactivity disorder or autism spectrum disorder. Traffic Injury Prevention, 14(2), 188–193.
Classen, S., Monahan, M., & Hernandez, S. (2013). Indicators of simulated driving skills in adolescents with autism spectrum disorder. The Open Journal of Occupational Therapy, 4(2). Retrieved from http://scholarworks.wmich.edu/ojot/vol1/iss4/2.
Conway, A. A., Kane, M. J., Bunting, M. F., Hambrick, D. Z., Wilhelm, O., & Engle, R. W. (2005). Working memory span tasks: A methodological review and user’s guide. Psychonomic Bulletin and Review, 12(5), 769–786.
Cox, C. V., Wharam, R., Mouran, R., & Cox, D. J. (2009). Does virtual reality driving simulation training transfer to on-road driving in novice drivers? A pilot study. Chronicle of the American Driver and Traffic Safety Education Association, 57(1).
Cox, D. J., Banton, T., Record, S., & Grabman, J. H. (2015a). Does correcting astigmatism with toric contact lenses improve driving safety? A pilot study. Optometry and Vision Science, 92(4), 404–411.
Cox, D. J., Davis, M., Singh, H., Barbour, B., Nidiffer, D., Trudel, T., & Moncrief, R. (2010). Driving rehabilitation for military personnel recovering from traumatic brain injury using virtual reality driving simulation: A feasibility study. Military Medicine, 175(6), 411–416.
Cox, D. J., Merkel, R. L., Kovatchev, B., & Seward, R. (2000). Effect of stimulant medication on driving performance of young adults with attention-deficit hyperactivity disorder: A preliminary double-blind placebo controlled trial. The Journal of nervous and mental disease, 188(4), 230–234.
Cox, D. J., Moncrief, M., Rizzo, M., Fisher, D., Lambert, A., Thomas, S., et al. (2015b). Low hanging fruit: Use of virtual reality simulation in Department of Motor Vehicles to assess minimal competence of novice drivers. In Paper presented at international driving symposium on human factors in driving assessment, training, and vehicle design. Salt Lake City, UT.
Cox, D. J., Taylor, P., & Kovatchev, B. (1999). Driving simulation performance predicts future accidents among older drivers. Journal of the American Geriatrics Society, 47(3), 381–382.
Cox, N. B., Reeve, R. E., Cox, S. M., & Cox, D. J. (2012). Brief report: Driving and young adults with ASD: Parents’ experiences. Journal of Autism and Developmental Disorders, 42, 2257–2262.
Cox, S. M., Cox, D. J., Kofler, M. J., Moncrief, M. A., Johnson, R. J., Cain, S. A., & Reeve, R. E. (2016). Driving simulator performance in adolescents with autism spectrum disorder: The role of executive functions and basic motor skills. Journal of Autism and Developmental Disorders. doi:10.1007/s10803-015-2677-1.
Daly, B. P., Nicholls, E. G., Patrick, K. E., Brinckman, D. D., & Schultheis, M. T. (2014). Driving behaviors in adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44(12), 3119–3128. doi:10.1007/s10803-014-2166-y.
Dempster, F. N. (1992). The rise and fall of the inhibitory mechanism: Toward a unified theory of cognitive development and aging. Developmental Review, 12(1), 45–75.
Dickerson, A. E., & Bédard, M. (2014). Decision tool for clients with medical issues: A framework for identifying driving risk and potential to return to driving. Occupational Therapy In Health Care, 28(2), 94–202. doi:10.3109/07380577.2014.903357.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191.
Freund, B., Colgrove, L. A., Petrakos, D., & McLeod, R. (2008). In my car the brake is on the right: Pedal errors among older drivers. Accident Analysis and Prevention, 40, 403–409.
Hoffman, J. D., Lee, J. D., Brown, T. L., & McGehee, D. V. (2002). Comparison of driver braking responses in a high-fidelity simulator and on a test track. Transportation Research Record, 1803(1), 59–65.
Hofmann, W., Schmeichel, B. J., & Baddeley, A. D. (2012). Executive functions and self-regulation. Trends in Cognitive Sciences, 16(3), 174–180.
Huang, P., Kao, T., Curry, A. E., & Durbin, D. R. (2012). Factors associated with driving in teens with autism spectrum disorders. Journal of Developmental and Behavioral Pediatrics, 33, 70–74.
Lambert, A. E., Simons-Morton, B. G., Cain, S. A., Weisz, S., & Cox, D. J. (2014). Considerations of a dual-systems model of cognitive development and risky driving. Journal of Research on Adolescence, 24(3), 541–550.
Malik, H., Rakotonirainy, A., & Maire, F. (2009). Correlating eye gaze direction, depth and vehicle information on an interactive. 2009 Australasian Road Safety Research, Policing and Education Conference : Smarter, Safer Directions. Sydney: Sydney Convention and Exhibition Centre.
Mäntylä, T., Karlsson, M. J., & Marklund, M. (2009). Executive control functions in simulated driving. Applied Neuropsychology, 16, 11–18.
Massie, D. L., Campbell, K. L., & Williams, A. F. (1995). Traffic accident involvement rates by driver age and gender. Accident Analysis and Prevention, 27(1), 73–87.
Michon, J. A. (1985). A critical view of driver behaviour models: What do we know, what should we do? In L. Evans, & R. C. Schwing (Eds.), Human behaviour and traffic safety (pp. 485–524). New York: Plenum.
Monahan, M., Classen, S., & Helsel, P. V. (2013). Pre-driving evaluation of a teen with attention deficit hyperactivity disorder and autism spectrum disorder. Canadian Journal of Occupational Therapy, 80(1), 35–41. doi:10.1177/0008417412474221.
Parsons, S., Mitchell, P., & Leonard, A. (2004). The use and understanding of virtual environments by adolescents with autistic spectrum disorders. Journal of Autism and Developmental Disorders, 34(4), 449–466.
Pradhan, A., Pollatsek, A., & Fisher, D. L. (2007). Comparison of trained and untrained novice drivers’ gaze behavior in risky and non-risky scenarios. Proceedings of the fourth international driving symposium on human factors in driver assessment, training and vehicle design. Stevenson, Washington.
Reimer, B., Aleardi, M., Martin, J. M., Coughlin, J. F., & Biederman, J. (2006). Characterizing impaired driving in adults with attention-deficit/hyperactivity disorder: A controlled study. Journal of Clinical Psychiatry, 67(4), 567–574.
Reimer, B., Fried, R., Mehler, B., Joshi, G., Bolfek, A., Godfrey, K. M., & Biederman, J. (2013). Brief report: Examining driving behavior in young adults with high functioning autism spectrum disorders: A pilot study using a driving simulation paradigm. Journal of Autism and Developmental Disorders, 43, 2211–2217.
Ross, V., Jongen, E. M., Brijs, T., Brijs, K., Ruiter, R. A., & Wets, G. (2015a). The relation between cognitive control and risky driving in young novice drivers. Applied Neuropsychology, 22(1), 61–72. doi:10.1080/23279095.2013.838958.
Ross, V., Jongen, E. M., Vanvuchelen, M., Brijs, T., Brijs, K., & Wets, G. (2015b). Exploring the driving behavior of youth with an autism spectrum disorder: a driver instructor questionnaire. 8th international driving symposium on human factors in driver assessment, training and vehicle design. Salt Lake City.
Ross, V., Jongen, E. M., Wang, W., Brijs, T., Brijs, K., Ruiter, R. A., & Wets, G. (2014). Investigating the influence of working memory capacity when driving behavior is combined with cognitive load: An LCT study of young novice drivers. Accident Analysis and Prevention, 62, 377–387.
Sheppard, E., Ropar, D., Underwood, G., & van Loon, E. (2010). Brief report: Driving hazard perception in autism. Journal of Autism and Developmental Disorders, 40, 504–508.
Sheppard, E., Van Loon, E., Underwood, G., & Ropar, D. (2016). Attentional differences in a driving hazard perception task in adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 1–10.
Strickland, D. (1997). Virtual Reality for the Treatment of Autism. Virtual Reality in Neuro-Psycho-Physiology, 81–86.
Unsworth, N., Heitz, R. P., Schrock, J. C., & Engle, R. W. (2005). An automated version of the operation span task. Behavior Research Methods, 37(3), 498–505.
Vlakveld, W., Romoser, M. R., Mehranian, H., Diete, F., Pollatsek, A., & Fisher, D. L. (2011). Do crashes and near crashes in simulator-based training enhance novice drivers’ visual search for latent hazards? Transportation Research Record, 2265, 153–160.
Wade, J., Bian, D., Zhang, L., Swanson, A., Sarkar, M., Warren, Z., & Sarkar, N. (2014). Design of a Virtual Reality Driving Environment to Assess Performance of Teenagers with ASD. In Universal access in human-computer interaction. Universal access to information and knowledge (pp. 466–474). New York: Springer International Publishing.
Acknowledgments
This project was supported by grant #W81XWH-12-1-0608 from the U.S. Department of Defense. We are indebted to the assistance rendered by Sarah Cain, Addison Walker, Erin Thiemann, Roger Thompson, Paul Barnard, Kristin Lucas, Trevor Johnson, and Rachel Dyke in the execution of this study.
Author Contributions
DJC was the principle investigator, the overall director of the project, and the primary writer of the manuscript. TB was the co-investigator of the project and oversaw data collection at the University of Iowa. He reviewed and critiqued the manuscript. VR did the data analysis for this paper and contributed extensively to the literature review and Results section. MM performed all assessments and VRDST at the University of Virginia and was the overall data manager of the project. He also contributed to the data presentation in this manuscript. RS was the University of Iowa’s project coordinator and performed their VRDS assessments. She did extensive technical editing of the manuscript. GG and RR were the clinicians responsible for the diagnosis of the ASD participants at the University of Iowa and the University of Virginia, respectively. They actively contributed to subject recruitment and they reviewed and critiqued this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Daniel Cox has received grant funding from the Department of Defense, the National institutes of Health, Johnson & Johnson, Purdue Pharmaceuticals and DexCom. Timothy Brown has received grant funding from the Department of Defense, and has performed contractual work for the National Highway Traffic Safety Administration, the Federal Highway Administration, Toyota Motor Company, and the National Institutes of Health. Veerle Ross has received grant funding from the Marie-Marguerite Delacroux support fund. Gary Gaffney has received grant funding from the Department of Defense, and has performed contractual work for the National Highway Traffic Safety Administration, and the National Institutes of Health. Ron Reeve received grant funding from the Department of Defense. Matthew Moncrief and Rose Schmitt declare that they have no conflict of interest.
Ethical Approval
All procedures performed involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Statement of Principles defined under the Belmont Report. Each site received individual approval from their respective institutional review board.
Informed Consent
All participants either signed an assent form (parents signing a Consent form) or a Consent form if age 18 or older. Before signing, participant and parent were taken to a quiet room, the consent form was reviewed, then parent and participant were left alone to consider the consent form and sign it if in agreement.
Additional information
This is a follow-up to an earlier study: Cox SM, Cox DJ, Kofler MJ, Moncrief MA, Johnson RJ, Lambert AE, Cain S and Reeve RE. Driving simulator performance in adolescents with autism spectrum disorder: The role of executive functions and basic motor skills. Journal of Autism and Developmental Disorders. 46(4), 1379–1391. doi 10.1007/s10803-015-2677-1.
Rights and permissions
About this article

Cite this article
Cox, D.J., Brown, T., Ross, V. et al. Can Youth with Autism Spectrum Disorder Use Virtual Reality Driving Simulation Training to Evaluate and Improve Driving Performance? An Exploratory Study. J Autism Dev Disord 47, 2544–2555 (2017). https://doi.org/10.1007/s10803-017-3164-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-017-3164-7