
Abstract
Extant data suggest that the cognitive profiles of individuals with ASD may be characterized by variability, particularly in terms of verbal intellectual functioning (VIQ) and non-verbal intellectual functioning (NVIQ) discrepancies. The Differential Ability Scales, Second Edition (DAS-II) has limited data available on its use with youth with ASD. The current study examined data from 2,110 youth with ASD in order to characterize performance on the DAS-II and to investigate potential discrepancies between VIQ and NVIQ. A larger proportion of individuals in the ASD sample had significant discrepancies between VIQ and NVIQ when compared to the normative sample [early years sample χ2 (2) = 38.36; p < .001; school age sample χ2 (2) = 13.48; p < .01]. Clinical and research implications are discussed.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Given that there is no biological test for autism spectrum disorder (ASD), valid and reliable evaluation of behavioral symptoms, considered in relation to an individual’s level of cognitive functioning, is an important assessment component for accurate diagnosis (Filipek et al. 2000; Johnson and Myers 2007). However, extant research suggests that profile variability on tests of cognitive functioning is a commonly occurring finding in the ASD population. Consequently, the use of a global index of cognitive functioning [i.e., full scale intellectual quotient (FSIQ)] may be inappropriate when characterizing individuals and research samples [e.g., National Research Council (NRC), 2001a]. Furthermore, the cognitive profile variability and behavioral symptoms observed in individuals with ASD may be a result of information-processing deficits that are caused by genetic and neurological impairments (Klinger and Renner 2000). For example, there are indications that a significant discrepancy between nonverbal intellectual quotient (NVIQ) and verbal intellectual quotient (VIQ), in either direction, may be associated with more significant social-communication deficits (Black et al. 2009). Also, in the first study of its kind, Chapman et al. (2011) found that a significant discrepancy between NVIQ and VIQ was strongly associated with a region on chromosome 10, as well as a suggested link with chromosome 16. Thus, clarifying the frequency and degree of cognitive profile variability is important both at the individual level and in terms of defining phenotypic subgroups.
Interpretation of cognitive profile variability occurs at two levels; statistical significance and base-rate or probability of occurrence (Sattler 2008). A difference between scores may be considered statistically significant but is a common occurrence (i.e., does not occur in <10–15 % of the population) in the normative sample; thus, not clinically meaningful (Flanagan et al. 2013). Understanding what is “expected” in terms of cognitive profile variability is important to clinicians,-profile discrepancies at the level of the individual are potentially meaningful in terms of clinical interpretation (Sattler 2008) and subsequent recommendations for intervention.
Extant research suggests that individuals with ASD are more likely to have significant variation between NVIQ and VIQ on standardized measures of cognitive functioning when compared both to (a) the samples on which the tests were normed (Coolican et al. 2008; Joseph et al. 2002) and (b) children with other, non-ASD developmental disabilities (Kuschner et al. 2007). Using the Differential Ability Scales (DAS; Elliott 1991), the occurrence of NVIQ/VIQ discrepancies in preschool and school-age samples with ASD was found to be 26 and 32 % (respectively) higher than those in the normative samples (Joseph et al. 2002). Similarly, 45 % of individuals sampled evidenced statistically significant NVIQ/VIQ splits using the Stanford Binet—Intelligence Scales 5th Edition (SB5) (Coolican et al. 2008). Black et al. (2009) reported that, in a sample of 78 children with high-functioning autism FSIQ ≥70, 54 % had a significant VIQ/NVIQ discrepancy, which was a much higher proportion than expected based on the available norms. Other researchers found that the proportion of VIQ/NVIQ discrepancies in individuals with Asperger’s disorder was similar to that in the general population and in individuals with other developmental disabilities (Lennen et al. 2010; Semrud-Clikeman et al. 2010). In a recent investigation examining the Differential Ability Scales—Second Edition (DAS-II; Elliott 2007a), a higher proportion of youth with ASD had NVIQ > VIQ discrepancies; but, the proportion of individuals with NVIQ < VIQ was approximately the same as the normative sample (Ankenman et al. 2014).
Given the inconsistent findings about the proportion of children with ASD who demonstrate NVIQ/VIQ discrepancies, it is postulated that significant cognitive profile variability may be related to other factors such as age (Ankenman et al. 2014; Joseph et al. 2002; Lincoln et al. 1998; Siegel et al. 1996). For example, the proportion of individuals with significant discrepancies between NVIQ and VIQ may decrease with age (Lincoln et al. 1998) and the direction of NVIQ/VIQ discrepancies may change with age (Joseph et al. 2002). In a sample of children with ASD, Joseph et al. (2002) found that, at younger ages (i.e., those administered the preschool version of the original version of the DAS), 65 % of the sample had a statistically significant NVIQ > VIQ discrepancy; though, at older ages [i.e., those administered the school age (SA) version of the DAS], the proportion of NVIQ > VIQ: NVIQ < VIQ was approximately equal. Relatedly, rates of NVIQ/VIQ discrepancies may be greater in children younger than 6 years of age (Mayes and Calhoun 2003). However, more recently, Coolican et al. (2008) did not find any evidence that NVIQ/VIQ discrepancy patterns were related to age among their sample of 63 children with ASD. The results described above are summarized in Table 1.
Purpose
The aforementioned results, though inconclusive, indicate that individuals with ASD may have an increased likelihood of NVIQ/VIQ discrepancies when compared to normative samples (e.g., Joseph et al. 2002) and that such discrepancies are potentially related to other factors, including age. Significant cognitive-profile variability has the potential to be an informative phenotypic marker for individuals with ASD (Chapman et al. 2011); furthermore, understanding patterns of cognitive-profile variability is important at the individual level (i.e., for diagnosis and treatment planning); when matching samples for research and may even inform etiological research. The DAS-II (Elliott 2007a) also differs from the original DAS in several respects. In contrast to the DAS, the DAS-II is modeled on Cattell–Horn–Carroll (CHC) theory. Revisions have been made to administration, recording, and scoring procedures for multiple subtests, with content revised for 13 subtests (Elliott 2007b). Though base-rate discrepancy data for eight special groups are included in the DAS-II manual, there is no such information specific to individuals with ASD (Elliott 2007b).
To the authors’ knowledge, there is only one other published finding examining NVIQ/VIQ discrepancies in individuals with ASD on the DAS-II (Elliott 2007a) and that study collapsed the early years (EY) and SA samples (Ankenman et al. 2014). As described later in this manuscript, the DAS-II verbal and nonverbal clusters of the EY and SA clusters are comprised of different subtests assessing different narrow cognitive processing abilities. Collapsing scores in this way may mask important differences across the batteries and limits the clinical utility of the findings.
Much of the existing research has relied on what some studies have shown to be unreliable and perhaps artificial diagnostic categories (i.e., autistic disorder, Asperger’s disorder, or PDD-NOS; Lord et al. 2011). Rather than analyzing cognitive profile discrepancies based on diagnostic subtypes defined within the DSM-IV-TR, analyzing data from all individuals meeting diagnostic criteria for an ASD acknowledges the fact that assigning categorical diagnosis may mask the substantial heterogeneity within each ASD subtype and is consistent with the Diagnostic and Statistical Manual—Fifth Edition (DSM-5; 2013) guidelines.
Thus, the purpose of the current study was to (a) investigate the rate and type of occurrence of cognitive-profile variability in children and adolescents with ASD on the DAS-II, EY and SA versions; and (b) compare these base-rate occurrences to those from the normative samples. In addition to examining profiles on a recommended test of intellectual functioning (i.e., the DAS-II) that, to date, has minimal published research; the current study builds on the literature base in this area by utilizing a well characterized sample of youth with ASD that is large enough to investigate patterns across age groups.
Method
Participants
The sample was drawn from 2,110 children and adolescents between the ages of 4 and 18 who participated in the simons simplex collection (SSC) and were administered the DAS-II. The SSC is a multi-site, genetic research project in North America that included families with only one child with an ASD and no other first- through third-degree relatives with ASD or suspected ASD (i.e., simplex families; Fischbach and Lord 2010). In order to be included in the SSC, focal children necessarily met criteria for an ASD based on scores from standardized diagnostic instruments and clinical judgment. More specific information about how families were recruited into the SSC and the procedures for collecting data can be found in Fischbach and Lord (2010).
Children/adolescents with a confirmed diagnosis of ASD who were administered the DAS-II and obtained standard scores on all clusters and subtests were included in the current sample (N = 1,850). In the original DAS-II EY sample, 1,054 youth had NVIQ standard scores reported, while 1,103 had VIQ standard scores reported. The resulting DAS-II EY sample (i.e., with both NVIQ and VIQ standard scores reported on the EY form) consisted of 739 children with a mean age of 5.89 years (SD = 1.21 years, range 4.8–11 years). A majority of the sample (86.5 %) were male, non-Hispanic (90 %), and Caucasian (80.4 %). In the original DAS-II SA sample, 1,258 youth had NVIQ standard scores reported while 1,143 had VIQ standard scores reported. The resulting sample (i.e., standard scores were reported for both the VIQ and NVIQ on the SA form) consisted of 1,120 youth with a mean age of 11.02 (SD = 2.97, range 5.3–18 years). Similar to the EY sample, a majority of the sample was male (88.1 %), non-Hispanic (90.1 %), and Caucasian (83.25). The socio-economic statuses of the individuals in both samples were skewed toward higher incomes. Many parents of participating children had obtained at least a baccalaureate degree, with relatively large proportions also having obtained graduate education. Specific information regarding race, SES, and parent-education levels for both the EY and SA samples can be found in Table 2.
Measures
As part of their participation in the SSC, youth were administered several phenotypic measures, including the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2000), the Autism Diagnostic Interview-Revised (ADI-R: Rutter et al. 2003), and the DAS-II. Both the ADI-R and ADOS were administered by two different research-reliable examiners at each of the data-collection sites, and only those children who met diagnostic cutoffs on these instruments and received a clinical diagnosis of ASD were included in the SSC. Descriptive information for the EY and SA sample for each measured variable is presented in Table 3.
Differential Ability Scales: Second Edition (DAS-II)
The DAS-II (Elliott 2007a) assesses a range of cognitive abilities but there is minimal published research on its use in general and special populations. The original DAS was developed for the purpose of profile analysis of cognitive strengths and weaknesses, but it was recently revised to align with CHC theory of intelligence (Beran 2007). The DAS-II was standardized on a normative sample of 3,480 children aged 2 years, 6 months to 17 years, 11 months and consisted of an equal number of males and females (Beran 2007). The DAS-II demonstrated excellent reliability and validity across the standardization sample, regardless of age (Beran 2007).
There are two, overlapping forms: the early years battery [(EY) with normative data available for individuals between the ages of 2 years 6 months and 8 years 11 months] and the school age battery [(SA) with normative data available for individuals between the ages of 5 years 0 months and 17 years 11 months]. The EY battery consists of two versions, a lower level [(LL) for children between the ages of 2 years 6 months and 3 years 5 months] and an upper level [(EY: UL) with normative data available on children between the ages of 3 years 6 months and 8 years 11 months]. Both batteries provide a global measure of intellectual functioning—the General Conceptual Ability (GCA). In addition, the EY: UL and the SA provide the following three composite scores: verbal ability (VA), nonverbal reasoning ability (NVA), and spatial ability (SPA). The NVA and SPA composites together make up the Special Nonverbal Reasoning score. The GCA and all three composite scores are reported as comparable, standard scores.
For the purposes of the current study, the VA and NVA cluster scores were examined and were operationalized as the VIQ and NVIQ, respectively. These particular cluster scores (rather than all three available cluster scores) were selected so that previous findings using the DAS and other measures, which only included a measure of verbal and non-verbal reasoning, could be replicated as closely as possible. Depending on which battery of subtests is administered, the resulting VIQ and NVIQ cluster scores may be comprised of different subtest scores. For example, for subtests that comprise the NVIQ cluster, normative data is only available between 5 years 0 months and 17 years 11 months for the recall of designs and sequential and quantitative reasoning subtests; normative data is only available between 3 years 6 months and 8 years 11 months for the Copying subtest. Consequently, though the cluster scores can be considered to be measures of general non-verbal reasoning and verbal reasoning abilities, there may be differences in the specific cognitive processes assessed within each domain. For example, the Copying and Recall of Designs subtests both measure the broad ability of visual-spatial ability; however, the Copying subtest measures the narrow ability of visualization whereas the Recall of Designs subtest measures the narrow ability of visual memory. This was also a consideration in comparing patterns of scores on the NVIQ and VIQ clusters to other tests of intellectual functioning as well as the earlier edition of the DAS. Results were interpreted within the context of these limitations and examination of VIQ and NVIQ discrepancy patterns selected as a starting point with the knowledge that investigation of variability at the subtest level would likely be warranted in future studies.
Procedure
All data were extracted from a national database containing de-identified information. Data corresponding to the measures listed above were requested from the Simons Foundation Autism Research Initiative (SFARI) following institutional review board (IRB) approval from the first author’s institution. Informed consent was obtained from all participants prior to participation.
Not all of the children administered the DAS-II had standard scores reported. Depending on the child’s level of functioning, items may have been administered out of level (i.e., above the age range for which standard and/or t-scores are available). In addition, when scores were obtained that fell below the floor of the test, t-scores were not reported and, instead, ratio scores based on age equivalents were calculated. For clarity of interpretation, only those individuals with standard scores on all clusters and subtests were analyzed in the present study. The decision regarding which form of the DAS-II was administered (i.e., EY or SA) was made, first, based on age, and, second, based on whether the child obtained a raw score considered to represent a true standard score. Specifically, if a child obtained a standard score representing the floor, the standard score was only reported if the child had obtained at least a raw score of 3. Otherwise, the clinician dropped down to either the DAS-II EY form or to the Mullen Scales.
Data Analysis
Analyses were conducted using SPSS Version 19. Per the inclusion criteria described above, cases without standard scores reported were identified using descriptive analyses and removed using list wise deletion. Proportions of children with significant discrepancies in either direction (i.e., NVIQ > VIQ, or NVIQ < VIQ) were calculated and compared to the number of children with significant discrepancies in the normative sample. According to Dumont, et al. (2009), discrepancies of 13–16 points are significant at the .05 level and discrepancies above 17 points are significant at the .01 level. In addition, discrepancies of 16 points or greater occur in <15 % of the normative sample (i.e., are considered unusual occurrences) (Elliott 2007b). Using this criterion, discrepancies equal to or >16 points were considered significant in the current study. The sample was grouped based on whether individuals had one of the following three cognitive profiles: NVIQ > VIQ, NVIQ < VIQ or NVIQ ≈ VIQ (i.e., no statistically significant difference); frequencies of youth falling within each category are reported in Table 3. Group membership in the ASD sample for each group (i.e., EY and SA) was compared to that in the DAS-II normative sample using Chi square Goodness of Fit test.
Results
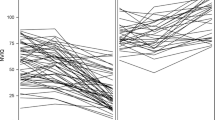
Distributions of VIQ and NVIQ in the combined sample, the EY sample, and the SA sample are presented in Figs. 1, 2 and 3, respectively. Expected and obtained proportions for the EY and SA samples are presented in Table 4. There was a significant difference between the expected and obtained proportions, across categories, for both samples: EY χ2 (2) = 125.69; p < .000; w = .46 (i.e., medium effect size); SA χ2 (2) = 172.67; p < .000; w = .39 (i.e., medium effect size) when compared to the normative sample. Compared to the normative sample, a significantly larger proportion of both the EY and SA samples had discrepancies in the VIQ > NVIQ and NVIQ > VIQ categories, with the exception of the VIQ > NVIQ category in the EY age group. In the VIQ > NVIQ EY category, there was a significantly smaller proportion of individuals with a discrepancy between VIQ and NVIQ (i.e., fewer individuals demonstrated higher VIQ scores than NVIQ scores than expected; 6 % obtained compared to 12 % expected). Compared to the normative sample, there were significantly fewer individuals than expected in both VIQ ≈ NVIQ categories (i.e., for the EY and the SA samples).

Verbal IQ as a function of non-verbal IQ: total sample

Verbal IQ as a function of non-verbal IQ: early years sample

Verbal IQ as a function of non-verbal IQ: school age sample
There was also a significant difference between observed and expected proportions, when comparing the EY to the SA sample χ2 (2) = 42.38, p < .001. Rates of discrepancies were found to be more evenly distributed in the SA sample. Specifically, the proportions in the SA group were more evenly split between VIQ > NVIQ (15 % and NVIQ > VIQ 20 %) than in the EY sample (VIQ > NVIQ = 6 %; NVIQ > VIQ = 32 %).
Discussion
The primary aims of the current study were to: (a) investigate cognitive variability in a sample of individuals with ASD and (b) compare cognitive-profile variability to that of the DAS-II normative sample. In individuals with ASD who were below 9 years of age, a total of 38 % of the sample had a significant VIQ/NVIQ discrepancy and in the SA sample, a total of 35 % had a significant discrepancy between VIQ/NVIQ. In both samples, the rate of VIQ/NVIQ discrepancy was significantly greater than expected when compared to the normative sample. These findings are consistent with some existing research (e.g., Black et al. 2009; Joseph et al. 2002; Kuschner et al. 2007) and demonstrate that there is significantly greater cognitive-profile variability in the current ASD sample than in a normative sample.
Previously reported VIQ/NVIQ discrepancy rates have ranged from 25 to 70 % depending on the sample, cognitive assessment measure, and how investigators define “discrepancy.” In an earlier study that examined the original version of the DAS, higher VIQ/NVIQ discrepancy rates were found when compared to the present study (EY = 56 %; SA = 62 %; Joseph et al. 2002). It is likely that the difference between the rates reported by Joseph et al. (2002) and the current findings are related to differences in sample characteristics and the use of the updated version of the DAS. To our knowledge, there is one other study investigating cognitive-profile variability using the DAS-II, and that work collapsed EY and SA samples (Ankenman et al. 2014). The authors found that, while there were higher than expected NVIQ > VIQ occurrences (compared to the normative sample), there were approximately equal numbers of individuals with NVIQ < VIQ. The difference between the current findings and those of Ankenman et al. (2014) is likely the result of the manner in which the samples were divided. Given that the subtests comprising the EY and SA samples differ, the current findings suggest that: (1) to fully understand cognitive profiles, it may be necessary to consider the specific cognitive processes being assessed and (2) when matching research samples using the DAS-II, it may be important to consider EY and SA samples separately.
Direction of VIQ/NVIQ discrepancy was also investigated and, interestingly, when compared to the normative group, significantly larger proportions of both the EY and SA samples had discrepancies in both the VIQ > NVIQ and the NVIQ > VIQ categories, with the exception of the VIQ > NVIQ in the EY age group. In that instance, there were a significantly smaller proportion of individuals with a significant discrepancy between VIQ and NVIQ. In addition, as found in research by Joseph et al. (2002), a significant difference in the proportion of individuals falling in the VIQ > NVIQ and NVIQ > VIQ across the two age groups was found, with rates of discrepancies being more evenly distributed in the SA sample. Specifically, the proportions in the SA group were more evenly split between VIQ > NVIQ (15 % and NVIQ > VIQ 20 %) than in the EY sample (VIQ > NVIQ = 6 %; NVIQ > VIQ = 32 %). However, the findings do not support previous reports that the gap between VIQ and NVIQ diminishes with age in this population (Mayes and Calhoun 2003). The relative proportion of children with no significant discrepancy between VIQ and NVIQ was consistent across groups (EY = 63 %; SA = 65 %).
Differences found across the EY and SA samples may have arisen for several reasons. Some existing research suggests that, in young children with ASD, VIQ scores tend to increase over time (Mayes and Calhoun 2003); thus, the differences found between the EY and SA samples may be a reflection of those changes. One of the key characteristics for many children with ASD is a delay in language development; thus, the fact that there are fewer children than expected with greater VIQ scores than NVIQ scores in the EY sample may reflect language delays for that particular group of children. Possibly, those in the school-age sample had more language and thus, better verbal reasoning skills. A more equal distribution was found across the NVIQ > VIQ and the VIQ > NVIQ groups in the SA sample. It is also plausible that the differences may be associated with changes in task demands across the two test batteries. Alternately, the differences may be an artifact of children in the school-age sample having more experience in test-taking situations. Regardless, the current findings highlight the importance of conducting re-evaluations over time to identify developmental changes in cognitive processes.
The current study supported the hypothesis that individuals with ASD exhibit significantly more profile variability (specifically VIQ/NVIQ discrepancies) when compared to the DAS-II normative sample. This has practical implications in several areas. The findings related to cognitive intra-profile variability described above are particularly relevant because some psychologists have argued that significant profile variability invalidates a global IQ score, and in the presence of significant profile scatter, the global-IQ score should not be interpreted (e.g., Flanagan and Kaufman 2004). Experts in the field have emphasized the importance of presenting a pattern of strengths and weaknesses rather than reporting misleading summary scores that are a meaningless average of discrepant scores (Klin et al. 2005). The findings from this study support that argument and suggest that, given the higher-than-expected number of individuals with significant discrepancies between clusters, it is particularly important to consider the appropriateness (or lack thereof) in interpreting a global-IQ score for individuals with ASD or characterizing level of functioning using a global IQ score. This is also consistent with the DSM-5 recommendation to consider both NVIQ and VIQ together with the diagnostic category when listing diagnostic specifiers (APA 2013).
Significant cognitive-profile variability renders replication of research findings (i.e., by matching sample characteristics) problematic because the profiles of two individuals with ASD who obtain a FSIQ of 80 may look remarkably different at the cluster or subtest level. The findings from the current study suggest that using a single global indicator of cognitive functioning (i.e., a full scale IQ score) to describe individuals with ASD may not be the best way to characterize a research sample. Furthermore, describing individuals as having “high-functioning autism” based on a single global score may not be appropriate if there are significant discrepancies between the cluster scores that comprise that global score. Differences in results from studies examining cognitive-profile variable also point out the value of considering which specific cognitive processes are being evaluated. Finally, the current findings suggest that, when matching samples evaluated using the DAS-II, it may be necessary to consider EY and SA samples separately.
Using more detailed description of research samples (both in terms of magnitude and direction of discrepancy) appears to be important in all types of ASD research but may be particularly important in genetic research. It is plausible that the patterns of cognitive-profile variability found in the present study (e.g., VIQ/NVIQ discrepancies) may be related to specific genetic differences. The first published study to investigate VIQ/NVIQ discrepancy as a phenotypic marker found a strong link to chromosome 10 and a suggested link to chromosome 16 (Chapman et al. 2011).
Limitations
Several limitations associated with the current study were identified. First, the current study was based on an extant database, inherently limiting the amount of control the investigators had over the collection of data. However, the SSC is acknowledged for its high-quality methodology, as well as the process for validation of the data, which minimizes concern over this potential limitation. Second, the proposed study was cross-sectional in nature, limiting causal inferences that can be made; it is not possible to determine cognitive changes across the lifespan of a child from these data.
There were characteristics of the sample which potentially limit the generalization of the findings. Specifically, families included in the SSC may not constitute a representative sample of the general population of children with ASD because of strict inclusion/exclusion criteria, the latter of which included the presence of significant birth complications, the presence of particular medical conditions in either the focal child with ASD or immediate family members, and the presence of significant learning disabilities or mental health conditions in siblings. Furthermore, because of cut-off requirements for inclusion in the SSC, the sample to date has been reported to have a higher-than-expected overall FSIQ (SS = 88). However, changes in minimum IQ requirements were implemented in the last 12 months of the study to ensure a more representative sample. Fourth, demographic analyses indicate that the SSC population (a) may not be proportionally representative of all ethnic groups and (b) appears to be skewed toward higher incomes. Clinicians should be mindful of the relatively homogenous nature of the current sample when using these results as a clinical reference.
Finally, in addition to variability across VIQ and NVIQ, there is some existing research documenting increased likelihood of significant variability at the subtest level in individuals with ASD (NRC 2001a). Analysis at the subtest level was beyond the scope of the proposed study and is therefore acknowledged as a potential limitation. The presence of significant subtest scatter within both the VIQ and NVIQ likely renders both cluster scores nonunitary, further influencing the interpretability of cluster scores (Joseph et al. 2002). Furthermore, as noted in the measures section of this manuscript, interpretation of differences in proportions of individuals with significant discrepancies between clusters (i.e., NVIQ and VIQ) across the EY and SA forms should be made with the understanding that there are some differences in the subtests comprising the cluster scores across the EY and SA forms.
Future Directions
As mentioned above, the current study neither investigated profile variability at the subtest level nor any potential relationships of intra profile variability at the subtest level with age or ASD symptoms. This is an important area for future research because, just as discrepancy scores between clusters have the potential to invalidate FSIQ scores, discrepancies between subtest scores have the potential to invalidate cluster scores. Also, analysis at the subtest level may help to further define any ASD subgroups and account for more statistical variance than analysis at the cluster-score level. Another potential area of investigation would involve reexamining the data to determine if or how overall level of functioning relates to profile discrepancies. As mentioned earlier, there is existing research suggesting that cognitive variability is independent of FSIQ; however, replication of those findings would add to the existing literature and potentially help to elucidate patterns of cognitive-profile variability in individuals with ASD.
The current study was cross-sectional in nature and, though differences were found between the EY and SA samples, because this was a between-subjects design (as opposed to a within-subject design), it limits the extent to which the findings can be generalized. Completing a similar study using a longitudinal design would provide further evidence along these lines.
Summary
The current study investigated cognitive-profile variability and base-rate occurrences of VIQ/NVIQ discrepancies in a large, well-characterized ASD sample. Findings supported some extant research and indicate that, using the DAS-II, individuals with ASD are more likely to have significant discrepancies between VIQ and NVIQ when compared to the normative sample; that those discrepancies may change over time; and that, when matching research samples using the DAS-II, it may be important to consider EY and SA samples separately. Findings add to the existing literature by addressing some of the methodological limitations of previous studies and emphasize the importance of understanding how cognitive-profile variability affects research samples, treatment and potentially, prognosis.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Association.
Ankenman, K., Elgin, J., Sullivan, K., Vincent, L., & Bernier, R. (2014). Nonverbal and verbal cognitive discrepancy profiles in autism spectrum disorders: Influence of age and gender. American Journal on Intellectual and Developmental Disabilities, 1, 84–99. doi:10.1352/1944-7558-119.1.84.
Beran, T. (2007). Review of the differential ability scales (2nd ed.). Canadian Journal of School Psychology, 22, 128–132. doi:10.1177/0829573507302967.
Black, D. O., Wallace, G. L., Sokoloff, J. L., & Kenworthy, L. (2009). Brief report: IQ split predicts social symptoms and communication abilities in high-functioning children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(11), 1613–1619.
Chapman, N. C., Estes, A., Munson, J., Bernier, R., Webb, S. J., Rothstein, J. H., et al. (2011). Genome-scan for IQ discrepancy in autism: evidence for loci on chromosomes 10 and 16. Human Genetics, 129, 59–70. doi:10.1007/s00439-010-0899-z.
Coolican, J., Bryson, S., & Zwaigenbaum, L. (2008). Brief report: Data on the Stanford–Binet intelligence scales (5th ed.) in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 38, 190–197. doi:10.1007/s10803-007-0368-2.
Dumont, R., Willis, J. O., & Elliott, C. D. (2009). Essentials of DAS-II assessment. Hoboken, NJ: Wiley.
Elliott, C. D. (1991). Differential Ability Scales (DAS). San Antonio, TX: Harcourt Assessment.
Elliott, C. D. (2007a). Differential Ability Scales—Second edition (DAS-II). San Antonio, TX: Harcourt Assessment.
Elliott, C. D. (2007b). Differential ability scales, 2nd edition: Introductory and technical handbook. San Antonio, TX: Harcourt Assessment.
Filipek, P., Accardo, P., Ashwal, S., Baranek, G., Cook, E., Dawson, G., et al. (2000). Practice parameter: Screening and diagnosis of autism: Report of the quality standards subcommittee of the American academy of neurology and the child neurology society. Neurology, 55, 468–479.
Fischbach, G. D., & Lord, C. (2010). The simons simplex collection: A resource for identification of autism genetic risk factors. Neuron, 68(2), 192–195.
Flanagan, D. P., Ortiz, S. O., & Alfonso, V. C. (2013). Essentials of psychological assessment: Essentials of cross battery assessment (3rd ed.). Hoboken, NJ: Wiley.
Flanagan, D. P., & Kaufman, A. S. (2004). Essentials of WISC-IV assessment. Hoboken, NJ: Wiley.
Johnson, C., & Myers, S. (2007). Identification and evaluation of children with autism spectrum disorders. American Academy of Pediatrics Policy, 120(5), 1183–1215. doi:10.1542/peds.2007-2361.
Joseph, R. M., Tager-Flusberg, H., & Lord, C. (2002). Cognitive profiles and social-communicative functioning in children with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 43(6), 807–821. doi:10.1111/1469-7610.00092.
Klin, A., Saulnier, C., Tsatsanis, K., & Volkmar, F. (2005). Clinical Evaluation in Autism Spectrum Disorders: Psychological Assessment within a Transdisciplinary Framework. In F. R. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders, vol 1: Assessment, interventions, and policy (3rd ed., pp. 772–798). Hoboken, NJ US: Wiley.
Klinger, L., & Renner, P. (2000). Performance-based measures in autism: Implications for diagnosis, early detection, and identification of cognitive profiles. Journal of Clinical Child Psychology, 29(4), 479–492. doi:10.1207/S15374424JCCP2904_3.
Kuschner, E. S., Bennetto, L., & Yost, K. (2007). Patterns of nonverbal cognitive functioning in young children with autism spectrum disorders. Journal of Autism and Developmental Disabilities, 37(5), 795–807. doi:10.1007/s10803-006-0209-8.
Lennen, D. T., Lamb, G. D., Dunagan, B. J., & Hall, T. A. (2010). Verbal prowess equals higher IQ: Implications for evaluating autism. Research in Autism Spectrum Disorders, 4(1), 95–101. doi:10.1016/j.rasd.2009.09.004.
Lincoln, A., Courchesne, E., Allen, M., Hanson, E., & Ene, M. (1998). Neurobiology of Asperger syndrome: Seven case studies and quantitative magnetic resonance imaging findings. In E. Schopler, G. Mesibov, & L. J. Kunce (Eds.), Asperger Syndrome or High-functioning Autism? (pp. 145–166). New York: Plenum.
Lord, C., Petkova, E., Hus, V., Gan, W., Lu, F., Martin, D. M., et al. (2011). A multisite study of the clinical diagnosis of different autism spectrum disorders. Archives of General Psychiatry,. doi:10.1001/archgenpsychiatry.2011.148.
Lord, C., Risi, S., Lambrecht, L., Cook, E., Leventhal, B., DiLavore, P., et al. (2000). The autism diagnostic observation schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30, 205–223. doi:10.1023/A:1005592401947.
Mayes, S., & Calhoun, S. L. (2003). Analysis of WISC-III, Stanford–Binet: IV, and academic achievement test scores in children with autism. Journal of Autism and Developmental Disorders, 33(3), 329–341. doi:10.1023/A:1024462719081.
National Research Council. (2001). Diagnosis, assessment, and prevalence. In C. Lord & J. P. McGee (Eds.), Educating children with autism (pp. 23–31). Washington, DC: National Academy Press.
Rutter, M., LeCouteur, A., & Lord, C. (2003). Autism Diagnostic Interview-Revised. Lutz, FL: PAR.
Sattler, J. M. (2008). Assessment of children: Cognitive applications (5th ed.). San Diego, CA: Author.
Semrud-Clikeman, M., Walkowiak, J., Wilkinson, A., & Christopher, G. (2010). Neuropsychological differences among children with Asperger syndrome, nonverbal learning disabilities, attention deficit disorder, and controls. Developmental Neuropsychology, 35(5), 582–600. doi:10.1080/875656412010494747.
Siegel, D., Minshew, N., & Goldstein, G. (1996). Wechsler IQ profiles in diagnosis of high-functioning autism. Journal of Autism and Developmental Disorders, 26, 389–406. doi:10.1007/BF02172825.
Acknowledgments
This research was supported by a grant from the Simons Foundation (SFARI SSC-15 to R. Goin-Kochel and A. Beaudet). We are grateful to all of the families at the participating SFARI Simplex Collection (SSC) sites, as well as the principal investigators (A. Beaudet, R. Bernier, J. Constantino, E. Cook, E. Fombonne, D. Geschwind, D. Grice, A. Klin, D. Ledbetter, C. Lord, C. Martin, D. Martin, R. Maxim, J. Miles, O. Ousley, B. Peterson, J. Piggot, C. Saulnier, M. State, W. Stone, J. Sutcliffe, C. Walsh, E. Wijsman). We appreciate obtaining access to phenotypic data on SFARI Base. Approved researchers can obtain the SSC population dataset described in this study (https://ordering.base.sfari.org/~browse_collection/archive[sfari_collection_v14]/ui:view()) by applying at https://base.sfari.org.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nowell, K.P., Schanding, G.T., Kanne, S.M. et al. Cognitive Profiles in Youth with Autism Spectrum Disorder: An Investigation of Base Rate Discrepancies using the Differential Ability Scales—Second Edition. J Autism Dev Disord 45, 1978–1988 (2015). https://doi.org/10.1007/s10803-014-2356-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2356-7