
Abstract
Type 2 diabetes is a multifactorial disorder coupled with impaired glucose tolerance, diminished insulin sensitivity and hyperlipidemia. Incessant hyperglycemia and hyperlipidemia led a towering risk to develop cardiovascular hitches with end-stage renal failure. Leaves of Nyctanthes arbor-tristis L. (NAT) (family: Oleaceae) is traditionally used by tribes of Assam for various ailments without proper scientific validation and appropriate mechanism of action for its activity. Hence, we aimed to evaluate the mechanism involved in the hypoglycemic and hypolipidemic effects of NAT leaves in high-fat diet (HFD)–streptozotocin (STZ)-induced diabetic rats. Male Sprague–Dawley rats were fed with in-house prepared high-fat diet (HFD) for a period of 4 weeks to create insulin resistance. Streptozotocin was injected intraperitoneally to these rats to cause β-cell destructions to create a model of type 2 diabetes. Our results have shown that NAT extract has a dose-dependent hypoglycemic and hypolipidemic activity in controlling the early biochemical parameters of kidney and lipids. Moreover, the extract has anti-oxidant and anti-inflammatory activities which were more pronounced at a dose of 400 mg/kg body weight. NAT treatment group also restored the normal architecture of the kidney and aorta tissue. GC–MS data analysis revealed the presence of several active compounds which are directly or indirectly responsible for its anti-diabetic and anti-hyperlipidemic activity. The apparent mechanism of NAT for its nephroprotection may be due to the suppression of hyperglycemia-mediated oxidative stress and amelioration of inflammatory cascades allied with NF-kB activation.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is an endocrine-related metabolic disorder where there is a persistent augment in blood glucose level (hyperglycemia) with impairments in insulin secretion, action or both (Ahmed et al. 2016). Diabetes has now become a major global saddle today affecting mostly the developing countries. As of 2015, India has become the diabetic hub with 69.2 million diabetic people and is ranked second in the world (Unnikrishnan et al. 2016). If the problem is not resolved, then India will become a land with 87 million diabetic people by 2030, making it the ‘Diabetic Capital of the World’ (Shaw et al. 2010). Continuous increase in blood glucose levels can lead to serious microvascular and macrovascular complications including retinopathy, neuropathy, and nephropathy, of which diabetic nephropathy (DN) accounts for nearly 40% of total new cases in both Asian and Western countries and is common among the patients with type 2 diabetes (Borgohain et al. 2017a).
Diabetic nephropathy (DN) is the preeminent root of end-stage renal disease (ESRD) characterized by microalbuminuria and increased blood pressure with the decline glomerular filtration rate (GFR), and is prevalent amidst type 2 diabetic patients (Cooper et al. 1998). Before the inception of microalbuminuria, a string of renal dysfunction occurs initially including renal hyperfiltration and hyperperfusion causing an increased capillary permeability (Mishra et al. 2010). In the latter stage of the progression of the disease, ultrastructural changes are seen in the kidney such as glomerular basement membrane thickening, devaluation in glomerular space, tubular expansion, leukocyte accumulation, and annihilation of proximal tubule cells (Sheetz and King, 2002). Hence, early control of blood glucose level becomes very much essential to prevent morbidity and mortality among the diabetic patients.
Long-term diabetes also contributes to boost low-density lipoprotein (LDL) cholesterol (CL) and decrease high-density lipoprotein cholesterol levels (HDL) that cause lipid dsyregulation (Jayashankar et al. 2015). This leads to an exponential growth in atherosclerotic coronary heart diseases (CHD) in diabetic patients and an increase in mortality and morbidity worldwide. Thus, it is imperative to check not only blood glucose levels, but also snaffle blood lipid levels to have beneficial therapeutic effects.
Prevailing medication for diabetes with synthetic hypoglycemic agents do have detrimental effects such as abnormal hypoglycemia, gastrointestinal abnormalities, lactic acidosis and hepatotoxicity (Fu et al. 2012). Moreover, diminution of response after prolonged use of these medicines is also a big concern (Agrawal and Pal, 2013). Despite tremendous improvements in medical science, there still lacks a single effective group of anti-diabetic drugs which also possess hypolipidemic properties. Therefore, hunt for an intact, superior and competent hypoglycemic agent always remains a challenged having low cost with minimal adverse effects. Plant formulations have gained its popularity due to minimum toxicity, easy accessibility, and ready availability with multiple molecular targets.
Nyctanthes arbor-tristis L. (family: Oleaceae), frequently known as night-flowering Jasmine (English) or sewali (in Assamese) is one of the eminent medicinal floras found in the Northeastern part of India. Its leaf extract reported with antibacterial, analgesic, anti-inflammatory (Saxena et al. 1987), anti-oxidant (Dasgupta and De 2007) and anticancer activities (Dinamani and Rao 2009). The literature survey also proves that the plant has anti-diabetic activity (Sharma and Pooja 2011) but this study only got struck up at the preliminary phytoscreening level with limited scientific data and required a more precise study. Hence, the current study was designed to scrutinize the mechanism involved in the hypoglycemic and hypolipidemic effects of ethanolic extract of tender leaves from N. arbor-tristis (L.) in albino rats which could achieve criterion evidence for improvement of novel therapy with minimal toxicity and high potency.
Materials and methods
Drug and chemicals
Streptozotocin (cat. no. S0130) and Glibenclamide (cat. no. G0639) were procured from Sigma-Aldrich (St. Louis, MO, USA). SD check glucometer was acquired from SD biosensor Inc. Korea. Superoxide dismutase (SOD) kit and catalase kit was purchased from Sigma-Aldrich (Steinheim, Germany). Rat insulin level (RAB09041) estimation was done with a commercial kit obtained from Sigma-Aldrich. ELISA kit for the determination of IL-6 (KRC0061) and TNF-α (KRC3011) was obtained from Life Technologies, and IL-1β (cat. no. RAB0278) was acquired from Sigma-Aldrich St. Louis USA. ELISA kits for rat NF-κB p65 kit (cat. no. QY-E11354) were procured from Qayee Bio Shanghai, China.
Plant materials
Leaves of N. arbor-tristis (NAT) were collected from Noonmati area (26.18°N 91.80°E.) district Kamrup, India during the month of January–February. Authentication of the plant was done by Curator Dr. Ganesh Sharma Department of Botany from Gauhati University, Guwahati. A voucher specimen with the same Acc no. 18200 dt. 16-9-2016 was deposited in the herbarium of Botanical Survey of India and preserved for further reference.
Method of extraction
Fresh leaves were separated from the other plant washed thoroughly and dried under shade. The dried leaves were grounded into coarse powder using a mechanical grinder. About 200 g of the coarse powder material was soaked in ethanol (500 ml) for 4 days under occasional shaking in a rotatory shaker. The extracts were filtered through Whatman filter paper (125 mm), and then concentrated by rotary evaporator at 40 °C for complete dryness. The percentage yield of N. arbor-tristis was 20.25% (w/w) with respect to the original dried powder.
GC–MS analysis of the extract
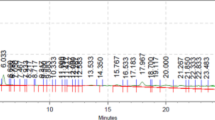
The ethanolic leaf extract of NAT was analyzed for the presence of phytocompounds by GC–MS (Shimadzu QP-2010 Plus with Thermal Desorption System TD 20). The bioactive compounds were predicted by their retention time (RT), peak area percentage (%), MW, molecular formula, and their biological activities with the help of PubChem compound (NCBI), WILEY8 and NIST11 libraries.
Animal selection and ethical permission
Sprague–Dawley (SD) rats weighing 200–250 g were accessed from the central animal facility (CAF) of the institute (Gauhati Medical College, Guwahati). The study was endorsed by Institutional Animal Ethics Committee (IEAC) (approval no. MC/05/2015/50), Gauhati Medical College, Guwahati (CPCSEA No.351;3/1/2001). The animals were housed in a group of six per cage in standard polycarbonate cage with standard environment conditions (24 ± 1 °C; humidity 65 ± 5%; reversed 12-h light/dark cycle).
Acute toxicity tests
The acute toxicity study was implemented according to OECD guidelines 425. Animals were fasted overnight prior to dosing and the dose was computed in accordance with the body weight. Following the period of fasting, the first animal was dosed at 175 mg/kg body weight with the extract by an oral gavage. The animal was inspected for mortality for 48 h and then a second animal was dosed at 550 mg/kg body weight by gavage. Again after 48 h of the second dosing, a third animal was dosed at 2000 mg/kg and observed further for the next 48 h for mortality. All the above animals were checked for complete observation period of 14 days. The animals were found to be alive at 2000 mg/kg. Hence, 1/20th, 1/10th and 1/5th, i.e., 100, 200 and 400 mg/kg were taken up for the further study.
Oral glucose tolerance test (OGTT)
OGTT were performed in overnight fasted rats as described by Kumar et al. (2013). Briefly, the rats were treated with three doses of the extract, i.e., 100 mg, 200 mg and 400 mg/kg body weight. After 30 min of administration of different doses of NAT extract and glibenclamide, the animals were challenged with an oral glucose load (2 g/kg body weight). Blood was withdrawn from the tail vein at 0-, 30-, 60-, 120- and 240-min interval and blood glucose levels were measured by the SD check glucometer. Results obtained from OGTT will be taken as a reference to select the dose for long-term effects of NAT on diabetic rats.
Induction of type 2 diabetes in rats
SD rats were obtained from CAF and allowed to acclimatize for 2 weeks in the laboratory environment. Six rats were segregated as normal control group fed on in-house normal pellet diet. The other rats were fed on high-fat diet (HFD) consisting of 12% lard oil, 18% sugar, 70% normal diet for 4 weeks to create insulin resistance. Streptozotocin (STZ) was prepared freshly by dissolving in citrate buffer (0.1 M, pH 4.5), and injected i.p. to the animals at dose a of 40 mg/kg body weight to create mild β-cell destruction (Srinivasan et al. 2005). Animals having blood glucose level higher than ≥ 200 mg/dl are contemplated as diabetic and used for further studies.
Animal grouping and experimental design
Diabetes was confirmed after 72 hours of dosing and the rats were divided into four groups from Group II to V with animals (n = 6) except in diabetic standard group (n = 12, where 6 animals were treated with glibenclamide). Group I serves as normal control. The treatment was given once a day for the next 28 days by oral route through an oral gavage.
Group I: normal control group—received normal saline in the dose of 10 ml/kg body weight.
Group II: diabetic control group—received normal saline in the dose of 10 ml/kg body weight.
Group III: diabetic test—received ethanolic extract of N. arbor-tristis 200 mg/kg body weight.
Group IV: diabetic test—received ethanolic extract of N. arbor-tristis 400 mg/kg body weight.
Group V: diabetic standard group—received glibenclamide at a dose of 10 mg/kg body weight.
Estimation of blood glucose, insulin level and other biochemical parameters
Blood glucose was estimated on every 7th day using SD CHECK GOLD blood glucose monitoring system. On the 29th day, animals were fasted overnight and killed by cervical dislocation. Blood was collected and serum and plasma both were separated for various biochemical estimation. Plasma and serum were used for the estimation of insulin, blood urea nitrogen (BUN), creatinine, triglycerides (TG), total cholesterol (TC) and high-density lipoprotein (HDL) using semi-auto-analyzer (IDEXX vet test analyzer). Low-density lipoprotein (LDL) and very low density lipoprotein (VLDL) cholesterol were calculated using the following formula:
Estimation of anti-oxidant parameters in the kidney tissues
Animals were dissected and kidney tissues were excised out carefully quickly and washed with ice-cold normal phosphate-buffered saline (PBS), pH 7.2, to remove other debris. Tissues were dried with a tissue paper and weight was taken. Finally, the tissues were cut into smaller pieces with a sharp surgical blade and homogenized by a glass homogenizer in ice-cold PBS. The solution was then centrifuged at 20,000 rpm for 10 min at 4 °C. The supernatant was collected snap frozen and stored in − 80 °C until further use.
Measurement of total protein
Total protein estimation in the kidney samples was done according to the method described by Lowry et al. (Lowry et al. 1951) using standard bovine serum albumin (BSA).
Measurement of superoxide dismutase
SOD levels were quantified using SOD assay kit obtained from Sigma-Aldrich, St. Louis, MO, USA. Absorbance was measured at 440 nm using SpectraMax i3x multi-mode microplate reader (Molecular Devices).
Measurement of lipid peroxidation
Lipid peroxidation (LPO) was estimated in agreement with the method described by Wright et al. (Wright et al. 1981) with slender modification. Results were expressed as nmoles of MDA formed per milligram of protein using molar extension coefficient 1.56 × 10 s M−1 cm−1.
Measurement of catalase
Catalase estimation was done by commercially available kit from Sigma-Aldrich. Data were expressed as μmol of H2O2 consumed/min (mg of protein).
Measurement of glutathione reductase
The reaction mixture consisting of 1.0 ml 10% PMS was mixed with 1.0 ml of 4% sulphosalicylic acid and then incubated for 1 h at 4 °C. Briefly, the reaction mixture having a total volume of 3 ml consists of 0.4 ml of tissue supernatant, 2.2 ml of phosphate buffer 0.1 M, pH 7.4, and 0.4 ml DTNB (4 mg/ml). The yellow color developed was instantly recorded at 412 nm on a SpectraMax i3× Multi-Mode Microplate Reader (Molecular Devices). The reduced glutathione concentration was measured as nmol GSH conjugates per mg of protein.
Estimation of NF-κB and other inflammatory cytokine levels in serum samples
NF-κB and other inflammatory cytokine levels (IL-1β, TNF-α, IL-6) were estimated by commercially available enzyme-linked immunosorbent assay (ELISA) kits. The method involves construction of a standard curve and the concentrations of test samples were obtained.
Western blot analysis
40 μg of protein samples (kidney) was mixed with an equal volume of 2× Laemmli buffer, boiled for 5 min at 95 °C, cooled, loaded on each lane of 10% polyacrylamide gel and separated by SDS-PAGE using Bio-rad electrophoresis unit (Mini-PROTEAN Tetra Cell). Proteins were transferred to polyvinylidene difluoride (PVDF) membrane using Trans-Blot® Turbo™ Transfer System (Bio-rad). The membranes were blocked with 3% bovine serum and incubated overnight at 4 °C with primary antibodies: NF-κB p65 (CST, cat. no. 3034), phosphoNF-κB p65 (CST cat no. 3033S), IκBα (CST cat. no. 4812S), phospho-IκBα (CST cat. no. 2859S). β-Actin antibody (CST cat. no. 4967S) was used as an internal control. The membranes were then washed with TBST solution gently and subsequently incubated with appropriate secondary antibodies (anti-rabbit IgG, HRP-linked 7074S) for 1 h. The bands were visualized by a Fusion Fx chemiluminescence-17-200255 (Vilber Lourmat) using ECL (Bio-Rad catalog no. 1705061) reagent. The densitometric analysis was performed using NIH Image J analysis software.
Histopathological studies
Paraffin sections of the kidney and aorta tissues were prepared, cut with a microtome (Theromo scientific microme HM325) and stained with hematoxylin and eosin (H&E) for the assessment of histopathological changes. Finally, the slides were observed under a Leica microscope (DM750 M) by a pathologist without prior awareness of the groups at 40X magnification.
Statistics
All the experimental results were expressed as mean ± SEM (n = 6). Comparisons between different groups were done using one-way analysis of variance (ANOVA) followed by multiple comparisons by Tukey’s test where appropriate. Two-way ANOVA followed by Bonferroni post test was used to analyze body weight and OGTT among different groups. Statistical analysis was performed using Graph Pad Prism 5.0 software (San Diego, CA, USA). A value of p < 0.05 is considered to be statistically significant.
Results and discussion
Type 2 diabetes (T2D) is a multifactorial disorder, strongly associated with obesity, impaired glucose tolerance, dwindled insulin sensitivity and dyslipidemia. Continuous hyperglycemia and hyperlipidemia led to a high risk to develop cardiovascular complications with end-stage renal failure (Lender and Sysko, 2006). So to combat such situations, a multi-targeted approach controlling the plasma insulin level as well as the high lipid level is obligatory. This has led to sustained efforts to scrutinize the potency of novel curative substances from natural origin that may be utilized as a substitute remedy for diabetes mellitus and its complications.
GC–MS data analysis
The ethanolic extract of NAT was injected in GC–MS and the compounds get separated according to their retention time. Among 81 compounds, those that were characterized and identified as the top 10 compounds according to their prevalence and activity were stated in this report (Table 1). Presence of stigmast-5-en-3-ol in the extract has anti-diabetic activity by promoting glucose uptake in a dose-dependent manner under insulin-resistant condition (Sujatha et al. 2010). Moreover, our extract contains octadecanoic acid/stearic acid which has excellent hypolipidemic activity by lowering the LDL cholesterol and apo-B significantly (Bonanome and Grundy, 1988). 2-Hexadecen-1-ol, 3,7,11,15-tetramethyl 2-hexadecen-1-ol (Phytol) is one of the components of the extract which has anti-oxidant activity and also acts as an agonist of retinoid X-receptor (RXR) (Kitareewan et al. 1996). Squalene present in the extract has the ability to reduce cholesterol and triglyceride levels and also act as an anti-oxidant (Amarowicz 2009). Stigmasterol present in the extract has hypoglycemic and cholesterol-lowering properties (Batta et al. 2006). The presence of various bioactive compounds in the extract of NAT justifies that the leaves have anti-oxidant, anti-diabetic and anti-lipidemic activities and hence the plant can be recommended as a plant of phytopharmaceutical importance.
Effect of NAT extracts on oral glucose tolerance test (OGTT)
Glucose feeding to normal fasting rats increases serum glucose levels from 60 min and reverted back to normal at 240 min. The acute effect of diverse doses of NAT leaf extract, feeded 30 min prior to glucose loading, results in significant reduction of blood glucose at 200 mg (154 ± 7.19 mg/dl) (p < 0.05) and 400 mg (152 ± 3.94 mg/dl) (p < 0.01) per kg body weight as shown in Fig. 1. At 120 min, 400 mg (117.67 ± 2.90 mg/dl) (p < 0.05) of the extract produces significant rebate in the blood glucose level compared to normal control. 100 mg/kg body weight of the extract does not produce any significant reduction in the blood glucose level; hence, the dose was not selected for further study (Fig. 1). Considering the aforementioned points, the ethanolic extract was further screened for its anti-diabetic, anti-hyperlipidemic anti-oxidant and anti-inflammatory activities.

Effect of different doses of Nyctanthes arbor-tristis (NAT) on fasting plasma glucose in oral glucose tolerance test (OGTT). Statistical significance was determined by two-way ANOVA followed by Bonferroni post test, where *p < 0.05, **p < 0.01, ***p < 0.001. “a” represents time point 60 min when compared with glucose control; “b” represents time point 120 min when compared with glucose control
Effect of NAT extracts on blood glucose and plasma insulin level
Insulin resistance with HFD and β-cell abnormality by STZ leads to a disparity between insulin sensitivity and internal glucose load causing importunate hyperglycemia in diabetic rats (Saha et al. 2018). HFD–STZ-induced diabetic rats show a significant gain in the blood glucose level when compared with the normal control group right from the 72 h of STZ injection (0 day) (451.7 ± 20.35 mg/dl) (p < 0.001) until the end of the study (28th day) (420.0 ± 22.40 mg/dl) (p < 0.001). Treatment with ethanolic extract of NAT at the dose of 200 mg and 400 mg/kg body weight significantly ameliorates the increase in the blood glucose level from 21st day (354.2 ± 22.07) (p < 0.05) in case of 200 mg extract and 14th day (345.4 ± 20.55) (p < 0.05) for 400 mg extract until completion of the study when compared with HFD–STZ-induced diabetic group showing its anti-diabetic activity (Table 2).
Figure 2 expresses the effect of ethanolic extract of NAT on plasma insulin of control and treated animals. Plasma insulin level was seen to be diminished in the diabetic rats as the peripheral tissue lacks insulin-sensitizing property. Both the doses have the ability to restore the plasma insulin level at a rate of 30.69 and 40.34%, respectively, versus the HFD–STZ-induced diabetic group. The hyperinsulinemia activity of the extract may be probably due to the restoration of insulin resistance and β-cell function.

Effect of NAT extract on plasma insulin levels of HFD–STZ-induced diabetic rats. All values were as mean ± SEM (n = 6). Statistical significance was determined by one-way ANOVA followed by Tukeys’s post hoc test, where *p < 0.05, **p < 0.01, ***p < 0.001, “a” represents normal control vs HFD–STZ-induced diabetic group, “b” represents 200 mg/kg of the extract vs HFD–STZ-induced diabetic group, “c” represents 400 mg of the extract vs HFD–STZ-induced diabetic group and “d” represents glibenclamide (10 mg/kg) vs HFD–STZ-induced diabetic group
Effect of NAT extracts on renal dysfunction
Persistent hyperglycemia, generation of free radicals and inflammatory cytokines play a key role in mesangial cell proliferation which is the main perpetrator behind the pathogenesis of DN. Highly inflamed kidney was seen in case of HFD–STZ-induced diabetic rats which causes an increase in the kidney dry weight (1.86 ± 0.03) (p < 0.001) when compared with normal rats. Moreover, the nephrotoxicity markers such as BUN (221.70 ± 4.41 mg/dl) and creatinine (8.68 ± 0.17 mg/dl) were significantly increased (p < 0.001) in the serum of HFD–STZ-induced diabetic rats. Treatment with ethanolic extract of NAT at both the doses for 28 days significantly ameliorates these inflated parameters when compared with diabetic rats asserts its nephroprotective activity (Table 3).
Effects of NAT extracts on serum lipid profile
Dyslipidemia is one of the hallmarks of type 2 diabetes with coronary artery disease (CAD) being the most widespread cause of death. Hyperlipidemia is often linked with altered levels of high-density lipoprotein (HDL), TC (total cholesterol), TG (triglyceride), VLDL (very low density lipoprotein) and LDL (low-density lipoprotein) in the blood (Castelli et al. 1977). Table 4 represents the lipid profile of the different experimental animals. Compared with the normal group rats, the HFD–STZ diabetic group rats have significant increase levels in the serum of TC (88%) (p < 0.001), TG (38%) (p < 0.01), VLDL (38.1%) (p < 0.01) and LDL (472.15%) (p < 0.001) with decease in the level of beneficial lipoprotein HDL (42%) (p < 0.001). However, the lipid profiles decreases significantly such as TC (36.3%) (p < 0.001), TG (21.6%) (p < 0.05), VLDL (21.6%) (p < 0.05) and LDL(60.3%) (p < 0.001) in the group treated with ethanolic extract of NAT at a dose of 400 mg/kg body weight when compared with HFD–STZ-induced diabetic rats. Moreover, the level of HDL (43.1%) (p < 0.05) also increases indicating that the extract has good anti-lipidemic activity. Atherogenic index (AI) and coronary index (CI) serve as an important index for developing CAD in the future with high-fat diet consumption. Our data shows an increase in the level of both the index in the HFD–STZ group indicating the animals are more prone to artery diseases in the future. Moreover, upon NAT treatment, the TC to HDL ratio, as a measure of Framingham’s coronary risk index (CI), is markedly reduced in the present study.
Effect of NAT extracts on oxidative stress in diabetic kidney
Precedent preclinical and clinical studies revealed the involvement of hyperglycemia- mediated oxidative stress in the pathophysiology of DN. Oxidative stress occurs when the reactive oxygen species (ROS) predominates the internal anti-oxidant defence of our body causing oxidation of various tissue biomolecules such as DNA, protein modifications, lipids, and carbohydrates (Borgohain et al. 2017b). HFD–STZ-induced diabetic rats show a significant elevated of MDA (marker of lipid peroxidation) (27.54 ± 1.38) (p < 0.001), along with decline in the level of SOD (5.45 ± 0.41) (p < 0.001), catalase (19.26 ± 2.16) (p < 0.001), reduced glutathione (49.48 ± 3.03) (p < 0.001), and glutathione reductase (24.75 ± 1.26) (p < 0.001) when compared with normal control group and is summarized in Table 5. Ethanolic extract of NAT at a dose of 400 mg/kg body weight significantly lowers the elevated level of MDA (13.17 ± 1.21) (p < 0.001) and elevates the level of enzymatic SOD (16.72 ± 0.79) (p < 0.001), catalase (55.50 ± 3.15) (p < 0.001), non-enzymatic anti-oxidant, reduced glutathione (93.58 ± 3.11) (p < 0.001), and glutathione reductase (39.14 ± 2.35) (p < 0.001) when compared with HFD–STZ-induced diabetic rat kidneys showing its anti-oxidant property (Table 5).
Effect of NAT extracts on the inflammatory cytokine levels
Inflammatory pathways have emerged as one of the major culprits in the pathogenesis of diverse renal disorders including DN. Among them tumor necrosis factor-α (TNF-α) is a major pleiotropic inflammatory cytokine which causes direct renal cell injury in the glomerular and tubular regions leading to an alternation of glomerular filtration, tubular permeability and reabsorption (Campion et al. 2017). IL-1β promotes the synthesis of PGE2 causing aberrant changes in the glomerular hemodynamics along with mesangial cell proliferation (Duran-Salgado and Rubio-Guerra, 2014). In the HFD–STZ-induced diabetic rats, there was a significant increase in the levels of IL-1β (202.70 ± 5.51) (p < 0.001), IL-6 (71.88 ± 2.69) (p < 0.001) and TNF-α (238.93 ± 6.55) (p < 0.001) in the kidney tissues when compared with normal control rats. Treatment with ethanolic extract of NAT for 28 days significantly restores the elevated levels of IL-1β (175.59 ± 3.85) (p < 0.05), IL-6 (55.99 ± 4.16) (p < 0.05) and TNF-α (207.96 ± 6.08) (p < 0.01) when compared to HFD–STZ-induced diabetic group (Fig. 3). The data prove that ethanolic extract of NAT has a dose-dependent inhibitory activity in combating the cytokine levels showing its anti-inflammatory activity which in turn might be responsible for its nephroprotective activity.

Effect of NAT extract on IL-1β, IL-6, TNF-α, and NF-κB levels in the kidneys of HFD–STZ-induced diabetic rats. All values were as mean ± SEM (n = 6). Statistical significance was determined by one-way ANOVA followed by Tukeys’s post hoc test, where *p < 0.05, **p < 0.01, ***p < 0.001, “a” represents normal control vs HFD–STZ-induced diabetic group, “b” represents 200 mg/kg of the extract vs HFD–STZ-induced diabetic group, “c” represents 400 mg of the extract vs HFD–STZ-induced diabetic group and “d” represents glibenclamide (10 mg/kg) vs HFD–STZ-induced diabetic group
Effect of NAT extracts on NF-kBp65 pathway activation
Canonical NF-κB signaling is an important transcription factor which is responsible for the release of plethora of cytokines and has been shown to be exacerbated in the glomeruli and renal tubes of patients suffering from DN (Mezzano et al. 2004). Generally, NF-κB remains in the cytosol in its dormant state forming heterodimers with its subunit IκBα which is an inhibitory protein. Once activated, free NF-κBp65 gets dissociated and translocates to the nucleus where it binds to its specific sequence and results in transcription of many pro-inflammatory cytokines such as TNF-α, IL-6, and IL-1β (Mundhe et al. 2015). To explore whether NF-κB signaling pathway is constitutively activated in HFD–STZ-induced diabetic rats and protection of NAT extract, the concentration of free NF-kBp65 and expression of its phosphorylated form and its endogenous subunits, i.e., IκBα were explored and measured by ELISA and immunoblots.
In our study, diabetic groups’ animal shows an increased expression of phospho-form of NF-κBp65 unit proving its nuclear translocation. NAT-treated rats showed significant low levels of renal NF-kBp65 (91.91 ± 5.56) (p < 0.001) (ELISA) (Fig. 3D) and increased expression of its phospho-form (immunoblots). Moreover, there was a decreased expression of pIκBα form in the NAT-treated rats showing its nuclear translocation inhibitory activity and exerting its anti-inflammatory activity (Fig. 4).

The expression of NF-κBp65, p NF-κBp65, IkBa, and pIkBa in the presence or absence of NAT extract in HFD–STZ diabetic rats was assessed by western blotting, and the quantified comparisons of relative densities are shown. All values were as mean ± SEM (n = 6). Statistical significance was determined by one-way ANOVA followed by Tukeys’s post hoc test, where *p < 0.05, **p < 0.01, ***p < 0.001, “a” represents normal control vs HFD–STZ-induced diabetic group, “b” represents 200 mg/kg of the extract vs HFD–STZ-induced diabetic group, “c” represents 400 mg/kg of the extract vs HFD–STZ-induced diabetic group and “d” represents glibenclamide (10 mg/kg) vs HFD–STZ-induced diabetic group
Effect on kidney histopathology
Kidney slides stained with hematoxylin–eosin (H&E) of control, diabetic and treatment groups under a microscope (40× magnifications) are shown in Fig. 5. Figure 5a depicts renal microphotographs of a control rat (black arrows), showing normal glomerular architecture, adequate capsular spaces and intact renal tubules with less leucocytes infiltration. Figure 5b depicts renal microphotographs of diabetic rats where complete loss of normal glomerular architecture showing detachment of basement membrane, glomerular space reduction and thickening, tubular damage, and leucocyte infiltration with large vacuolization was observed. Figure 5c represents microphotographs of kidney treated with the extract at a dose of 100 mg/kg body weight showing no improvement in the renal architecture. Figure 5d represents microphotographs of kidney treated with the extract at a dose of 200 mg/kg body weight showing mild improvement with somewhat less vacuolization, less leucocyte infiltration and necrosis. Figure 5e represents microphotographs of kidney treated with the extract of NAT at a dose of 400 mg/kg body weight showing much improvement in glomerular architecture and tubulointerstitial lesions with less vacuolization and low leucocyte infiltration as compared to diabetic group. Figure 5f represents the kidney section of diabetic rats treated with standard commercially available anti-diabetic drug, i.e., glibenclamide displayed minimum grading of glomerulus and tubulointerstitial lesions.

Photomicrographs of hematoxylin and eosin-stained kidney sections of experimental groups 40×. i Control, ii HFD + STZ-induced diabetic control, iii diabetic + MEPF100, iv diabetic + MEPF200, v diabetic + MEPF400 and vi GLB10. a Normal control group with normal architecture of the kidney tissue. b Diabetic kidney treated with HFD + STZ, where (black arrow) glomerular space reduction, (red arrow) lobulated glomeruli, (green arrow) leucocyte infiltration, (yellow arrow) large vacuolization, (blue arrow) tubular dilation. c Kidney tissue treated with the extract at a dose of 100 mg/kg body weight which failed to show any nephroprotection. d Kidney sections treated with a dose of 200 mg/kg body weight showing somewhat less vacuolization and nephritic damage. e Kidney of rats treated with 400 mg/kg body weight showing much improved glomeruli and tubules with less leucocyte infiltration and necrosis. f Kidney of rats treated with glibenclamide at a dose of 10 mg/kg body weight showing less lesion and treated glomeruli
Effect on aorta histopathology
Aorta tissues were also dissected out for histological evaluation by hematoxylin–eosin (H&E) staining under a microscope (40× magnifications) as depicted in Fig. 6. Microphotographs of the aorta of the normal control group showed a normal architecture with intact endothelial lining and solid vessel wall (Fig. 6a). There was no deposition of fat cells or foam cells in this group. Microphotographs of the aorta of the HFD + STZ (diabetic group) in Fig. 6b show deposition of abundant fat cells or foam cells and disruption of the endothelial lining with loss in its architecture. Figure 6c, d represents microphotographs of aorta tissue treated with the extract at a dose of 100 and 200 mg/kg body weight showing no improvement in the aorta architecture. Figure 6e represents microphotographs of aorta tissue treated with the extract at a dose of 400 mg/kg showing maximum improvement with less deposition of fat cells and regaining of the aortal architecture. Figure 6f represents microphotographs of aorta tissue treated with glibenclamide in which these changes were minimum to negligent when compared with HFD + STZ (diabetic) group.

Photomicrographs of hematoxylin and eosin-stained aorta sections of experimental groups 40×. i Control, ii HFD + STZ-induced diabetic control, iii diabetic + MEPF100, iv diabetic + MEPF200, v diabetic + MEPF400 and vi GLB10. a The aorta of the normal control group showed a normal architecture with intact endothelial lining and compact vessel wall. There was no deposition of fat cells or foam cells in this group. b Aorta of HFD + STZ-induced diabetic group showing (red arrow) deposition of abundant fat cells or foam cells and (black arrow) disruption of the endothelial lining. c Aorta treated with 100 mg of the extract with no improvement. d Aorta treated with 200 mg of the extract with a mild improvement. e Aorta of rat treated with 400 mg/kg of NAT showing much improvement of the endothelial lining and vessel wall
Conclusion
The present study was the first of its kind to provide a scientific basis of an ethnopharmacological claim of NAT leaf extract activity. Our results show that NAT has a dose-dependent hypoglycemic and hypolipidemic activity in halting the early stages of DN. The plausible mechanism for its protection may be due to suppression of hyperglycemia-mediated oxidative stress and embarrassment of inflammatory cascades associated with NF-κB activation. However, due to the numerous active molecules in NAT extract that exerts biological activities, further study is essential to clarify the other probable mechanism which elucidates its anti-diabetic and anti-hyperlipidemic activity.
References
Agrawal J, Pal A (2013) Nyctanthes arbor-tristis Linn—a critical ethnopharmacological review. J Ethnopharmacol 146:645–658
Ahmed S, Mundhe N, Borgohain M, Chowdhury L, Kwatra M, Bolshette N, Ahmed A, Lahkar M (2016) Diosmin modulates the NF-kB signal transduction pathways and downregulation of various oxidative stress markers in alloxan-induced diabetic nephropathy. Inflammation 39:1783–1797
Amarowicz R (2009) Squalene: a natural antioxidant? Eur J Lipid Sci Technol 111:411–412
Batta AK, Xu G, Honda A, Miyazaki T, Salen G (2006) Stigmasterol reduces plasma cholesterol levels and inhibits hepatic synthesis and intestinal absorption in the rat. Metab, Clin Exp 55:292–299
Bonanome A, Grundy SM (1988) Effect of dietary stearic acid on plasma cholesterol and lipoprotein levels. N Engl J Med 318:1244–1248
Borgohain MP, Chowdhury L, Ahmed S, Bolshette N, Devasani K, Das TJ, Mohapatra A, Lahkar M (2017a) Renoprotective and antioxidative effects of methanolic Paederia foetida leaf extract on experimental diabetic nephropathy in rats. J Ethnopharmacol 198:451–459
Borgohain MP, Lahkar M, Ahmed S, Chowdhury L, Kumar S, Pant R, Choubey A (2017b) Small molecule inhibiting nuclear factor-kB ameliorates oxidative stress and suppresses renal inflammation in early stage of Alloxan-induced diabetic nephropathy in rat. Basic Clin Pharmacol Toxicol 120:442–449
Campion CG, Sanchez-Ferras O, Batchu SN (2017) Potential role of serum and urinary biomarkers in diagnosis and prognosis of diabetic nephropathy. Can J Kidney Health Dis 4:2054358117705371
Castelli WP, Doyle JT, Gordon Hames CG, Hjortland MC, Hulley SB, Kagan A, Zukel WJ (1977) HDL cholesterol and other lipids in coronary heart disease. The cooperative lipoprotein phenotyping study. Circulation 55:767–772
Cooper ME, Gilbert RE, Epstein M (1998) Pathophysiology of diabetic nephropathy. Metabolism 47:3–6
Dasgupta N, De B (2007) Antioxidant activity of some leafy vegetables of India: a comparative study. Food Chem 101:471–474
Dinamani M, Rao AR (2009) Chemoprevention of DMBA induced skin tumorigenesis in Swiss albino mice: a study with Nyctanthes arbor-tristis leaf extract. Bioscan 4:295–299
Duran-Salgado MB, Rubio-Guerra AF (2014) Diabetic nephropathy and inflammation. World J Diabetes 5:393
Fu J, Fu J, Yuan J, Zhang N, Gao B, Fu G, Tu Y, Zhang Y (2012) Anti-diabetic activities of Acanthopanax senticosus polysaccharide (ASP) in combination with metformin. Int J Biol Macromol 50:619–623
Jayashankar CA, Andrews HP, Vijayasarathi Pinnelli VB, Shashidharan B, Nithin Kumar HN, Vemulapalli S (2015) Serum uric acid and low-density lipoprotein cholesterol levels are independent predictors of coronary artery disease in Asian Indian patients with type 2 diabetes mellitus. J Nat Sci Biol Med 7:161–165
Kitareewan S, Burka LT, Tomer KB, Parker CE, Deterding LJ, Stevens RD, Forman BM, Mais DE, Heyman RA, McMorris T (1996) Phytol metabolites are circulating dietary factors that activate the nuclear receptor RXR. Mol Biol Cell 7:1153–1166
Kumar V, Ahmed D, Gupta PS, Anwar F, Mujeeb M (2013) Anti-diabetic, anti-oxidant and anti-hyperlipidemic activities of Melastoma malabathricum Linn. leaves in streptozotocin induced diabetic rats. BMC Complement Altern Med 13:222
Lender D, Sysko K (2006) The metabolic syndrome and cardiometabolic risk: scope of the problem and current standard of care. Pharmacotherapy 26:3S–12S
Lowry OH, Rosebrough NJ, Farr AL, Randall RJ (1951) Protein measurement with the Folin phenol reagent. J Biol Chem 193:265–275
Mezzano S, Aros C, Droguett A, Burgos ME, Ardiles L, Flores C, Schneider H, Ruiz-Ortega M, Egido J (2004) NF-kB activation and overexpression of regulated genes in human diabetic nephropathy. Nephrol Dial Transplant 19:2505–2512
Mishra A, Bhatti R, Singh A, Singh Ishar MP (2010) Ameliorative effect of the cinnamon oil from Cinnamomum zeylanicum upon early stage diabetic nephropathy. Planta Med 76:412–417
Mundhe NA, Kumar P, Ahmed S, Jamdade V, Mundhe S, Lahkar M (2015) Nordihydroguaiaretic acid ameliorates cisplatin induced nephrotoxicity and potentiates its anti-tumor activity in DMBA induced breast cancer in female Sprague—Dawley rats. Int Immunopharmacol 28:634–642
Saha MR, Dey P, Sarkar I, De Sarker D, Haldar B, Chaudhuri TK, Sen A (2018) Acacia nilotica leaf improves insulin resistance and hyperglycemia associated acute hepatic injury and nephrotoxicity by improving systemic antioxidant status in diabetic mice. J Ethnopharmacol 210:275–286
Saxena RS, Gupta B, Saxena KK, Srivastava VK, Prasad DN (1987) Analgesic, antipyretic and ulcerogenic activity of Nyctanthes arbor-tristis leaf extract. J Ethnopharmacol 19:193–200
Sharma V, Pooja MA (2011) Hypoglycemic activity of methanolic extracts of Nyctanthes arbor-tristis linn. root in alloxan induced diabetic rats. Int J Pharm Pharm Sci 3:210–212
Shaw JE, Sicree RA, Zimmet PZ (2010) Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 87:4–14
Sheetz MJ, King GL (2002) Molecular understanding of hyperglycemia’s adverse effects for diabetic complications. JAMA 288:2579–2588
Srinivasan K, Viswanad B, Asrat L, Kaul CL, Ramarao P (2005) Combination of high-fat diet-fed and low-dose streptozotocin-treated rat: a model for type 2 diabetes and pharmacological screening. Pharmacol Res 52:313–320
Sujatha S, Anand S, Sangeetha KN, Shilpa K, Lakshmi J, Balakrishnan A, Lakshmi BS (2010) Biological evaluation of (3β)-STIGMAST-5-EN-3-OL as potent anti-diabetic agent in regulating glucose transport using in vitro model. Int J Diabetes Mellitus 2:101–109
Unnikrishnan R, Anjana RM, Mohan V (2016) Diabetes mellitus and its complications in India. Nat Rev Endocrinol 12:357–370
Wright J, Colby H, Miles P (1981) Cytosolic factors which affect microsomal lipid peroxidation in lung and liver. Arch Biochem Biophys 206:296–304
Acknowledgments
This research was supported by the National Institute of Pharmaceutical Education and Research (NIPER)-Guwahati, under the aegis of Department of Pharmaceuticals, Ministry of Chemicals and Fertilizers, Government of India. The authors acknowledge Institutional Biotech Hub (IBT hub), NIPER-Guwahati, for providing necessary facilities and equipment’s to carry out this work. The authors also acknowledge the Advanced Instrumentation Research Facility, Jawaharlal Nehru University (JNU), New Delhi, for helping with GC–MS data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interests.
Rights and permissions
About this article

Cite this article
Mousum, S.A., Ahmed, S., Gawali, B. et al. Nyctanthes arbor-tristis leaf extract ameliorates hyperlipidemia- and hyperglycemia-associated nephrotoxicity by improving anti-oxidant and anti-inflammatory status in high-fat diet–streptozotocin-induced diabetic rats. Inflammopharmacol 26, 1415–1428 (2018). https://doi.org/10.1007/s10787-018-0497-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10787-018-0497-6