
Abstract
Type 2 diabetes mellitus (T2DM) is a risk factor that plays a major role in the onset of heart failure (HF) both directly, by impairing cardiac function, and indirectly, through associated diseases such as hypertension, coronary disease, renal dysfunction, obesity, and other metabolic disorders. In a population of HF patients, the presence of T2DM ranged from 20 to 40%, according to the population studied, risk factor characteristics, geographic area, and age, and it is associated with a worse prognosis. Finally, patients with HF, when compared with those without HF, show an increased risk for the onset of T2DM due to several mechanisms that predispose the HF patient to insulin resistance. Despite the epidemiological data confirmed the relationship between T2DM and HF, the exact prevalence of HF in T2DM comes from interventional trials rather than from observational registries aimed to prospectively evaluate the risk of HF occurrence in T2DM population. This review is focused on the vicious cycle linking HF and T2DM, from epidemiological data to prognostic implications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is a well-established risk factor for a wide range of cardiovascular (CV) events, including macrovascular and microvascular complications [1, 2]. The prevalence and incidence of diabetes mellitus, and type 2 DM (T2DM) in particular, in patients with heart failure (HF), and the related risks associated with this condition, have not been fully described in a contemporary population [3].
The recent advances in diabetic treatment further highlight the need for better understanding of the complex relationship between T2DM and HF. Subjects affected by T2DM have a higher incidence of HF and a worse outcome than non-diabetic people [4]. T2DM is associated with the onset of HF both directly and indirectly through associated CV risk factors and diseases.
In many studies, HF is considered a CV complication. However, up to now, few studies have directly analyzed the real impact of T2DM in HF, and most reports describe post hoc or retrospective data [5,6,7]. Altered glycemic status is often associated with other CV risk factors and metabolic disorders. Therefore, T2DM may accelerate coronary and systemic atherosclerosis, endothelial damage, autonomic dysfunction, and extracellular matrix collagen deposition [8]. In addition to these factors, diabetic cardiomyopathy [9, 10] represents another potential cause of HF development, independent of the presence of vascular disease. Additionally, HF may increase the incidence of T2DM, whose onset is associated with a worse outcome [11].
The aim of this review is to describe epidemiological aspects and potential causal factors that explain the dangerous relationship between T2DM and HF.
Diabetes in heart failure
Diabetes as potential HF risk factor
Altered glycemic status is often associated with other CV risk factors, such as hypertension, obesity, and dyslipidemia. These factors have been highlighted in the new definition of HF, and they represent initial risk factors for HF occurrence [12]. Therefore, T2DM per se, may accelerate coronary and systemic atherosclerosis, vascular alteration, autonomic dysfunction, and extracellular matrix collagen deposition [8]. This relationship may confound the risk assessment, and it is unclear how much the adverse outcome is directly due to glycemic dysfunction or linked to the higher risk burden. T2DM is also associated with an atherogenic lipid profile, high blood pressure, low-grade inflammation, renal disorder, and advanced glycation end products (AGEs), all of which increase CV risk [13, 14]. The altered endothelial function is associated with an adverse lipid profile and vascular inflammation, which produce pro-atherogenic signals (P selectin, vascular grow factors, transforming grow factor β) that are responsible for systemic vascular damage. Both arterial and cellular alterations lead to increased myocardial susceptibility, fibrosis, and collagen deposition, mediated by energetic substrate modification and altered intracellular signals. Among all patients affected by T2DM, about 90% are overweight, 70% are dyslipidemic, and almost 70% suffer from hypertension [7] (Fig. 1).

Traditional and emerging risk factors that explain the increased risk of adverse events in patients with HF and associated diabetes
In the trial EMPAREG OUTCOME, 65% of patients had a prior myocardial infarction or stroke, and 12%, 40%, 30%, and 18% were at low, intermediate, high, and very high cardiovascular risk according to TIMI Risk Score for Secondary Prevention [15]. In the DECLARE Study, more than 90% of patients had multiple risk factors for cardiovascular disease or had established atherosclerotic CV disease defined as evidence of ischemic heart disease, ischemic cerebrovascular disease, or peripheral artery disease [16]. In the previously published ORIGIN trial, 59% of diabetic patients had cardiovascular event, 35% MI, and 79% affected by hypertension [17]. Moreover, more than half took statins and 80% antihypertensive or diuretic agents. Finally, in a post hoc analysis of the LEADER trial comparing patients with and without HF, the distribution of CV drugs was similar independently on NYHA class and the CV risk profile was comparable in all subgroups [18]. Current findings could explain several gaps in evaluating the risk burden and related risk for HF in this setting.
As far as functional status and exercise capacity are concerned, T2DM is characterized by a reduced exercise tolerance, impaired quality of life, and poor life expectancy due to both CV and peripheral muscle alterations independently on the presence of HF. In the cross-sectional cohort study, T2DM was much more common in women than in men, and its prevalence increased linearly as patient age from 46 to 74 years [2]. In this population, HF risk was twofold and fivefold greater in diabetic men and women, respectively, compared to non-diabetic men and women. In a meta-analysis of several cardiovascular outcome trials in T2DM patients, the authors found that HF was one of the most frequent nonfatal CV events, second only to myocardial infarction, with a mean prevalence ranging from 13 to 30% [19]. The wide range reported is due to the heterogeneity in HF diagnosis, the broad HF definition used, the lack of HF subtypes recognition, poor differentiation between chronic stable HF and de novo episodes, and population characteristics. In the ARIC study evaluating baseline diabetic patients without evidence of cardiac dysfunction, incidence of HF was strictly related with the presence of coronary artery disease (CAD) and it increases for each 1% higher glycosylated hemoglobin (HbA1c): 1.17 for the non-CAD group and 1.20 (CI 1.04–1.40) for the CAD group [20]. Similarly, in the Reykjavik study, across 20 years of mean follow-up, HF was diagnosed in 3.2% of non-diabetic patients compared with 6.0 and 11.8% among those with glycemic alteration and T2DM, respectively [21]. More recently, it has been demonstrated that not only the T2DM presence but also the changes in HbA1c over time were independently associated with risk of incident HF among patients with T2DM [22].
Prevalence of T2DM in HF population and related risk
Over the last two decades, the prevalence of T2DM in HF patients has gradually increased from 12 to 22% in people 70 years or older [13, 23]. The current trend may be the result of the increased incidence of T2DM in the general population, improvement of diagnostic care, population aging, and prevention programs diffusion in industrialized countries [24]. An observational study reported that 12% of diabetic patients admitted to the hospital have HF, and those without HF had a 3.3% increased risk per year for disease developing [3].
In addition to these reports, few studies have directly analyzed the real impact of T2DM in HF, and most of the reports have described post hoc or retrospective data [5,6,7]. The more intriguing data come from the recent introduction of sodium glucose transport inhibitors (SGLT2-i), which have a positive effect on both CV- and HF-related events [25, 26].
In clinical trials, prevalence of T2DM in HF population varies according to the presence of chronic kidney disease (CKD), the coexistence of other CV diseases, and the duration of the glyco-metabolic disorder. In the observational Rotterdam study, 28% of diabetic patients had HFrEF, and 25% experienced HFpEF [27]. In the pilot ESC survey, 30% of HF diabetic patients had a preserved EF [28]. Moreover, a post hoc analysis from CHARM revealed that the prevalence of T2DM in HFrEF is 28.5% vs 28.3% in those with HFpEF [29]. T2DM prevalence also varies across race and lifestyle. In a cohort analysis from two different registries, HF-ACTION and ASIAN HF, the authors showed relevant differences with the lowest T2DM prevalence in Whites (29.3%), followed by Japanese/Koreans (34.1%), Blacks (35.9%), Chinese (42.3%), and Indians (44.2%); the highest prevalence is in Malays (51.9%) [30]. As previously reported, most of the patients with HF and preserved left ventricular ejection fraction (HFpEF) have glycaemic intolerance, increased body mass index, or other metabolic disorders [31, 32]. In addition to these factors, T2DM can be associated with diabetic cardiomyopathy by a direct damage on myocytes and endothelial cells due to an overexpression of end-glycosylated product, collagen deposition, and augmented inflammatory pathways. Diabetic cardiomyopathy type is distinguished for increased left ventricular (LV) mass and volume, impaired left ventricular LV filling, diastolic dysfunction, and reduced arterial compliance [9, 10]. Since T2DM is often associated with the above cited metabolic disorders, an emerging syndrome called metabolic cardiomyopathy is now acknowledged. This is the final expression of multiple metabolic and cellular disorders that lead to ventricular hypertrophy and stiffness, reduced arterial and ventricular compliance, and increased filling pressure and afterload [31,32,33].
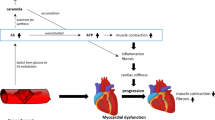
T2DM can affect myocardial structure and function by several mechanisms, among which the most important is related to insulin resistance of muscle, liver, and pancreatic cells. The lack of insulin response in these systems leads to systemic glucotoxicity, fatty acid lipotoxicity, accelerated lipolysis, increased renal glucose absorption, and reduced incretin levels from gastrointestinal tract. Of note, the cardiovascular damage may arise from different alterations including metabolic (lipogenesis and gluconeogenesis), renal (increasing Na and glucose resorption), myocardial (sarcomeric stiffness and fibrosis overexpression), endothelial (increased RAA activity vascular grow factors, reduced NO synthase), and inflammatory disorders (increased expression of interleukines facilitating thrombogenesis). The prevalence of each pathophysiological mechanism may explain the different HF pattern and cardiac structural adaptation. Behind these metabolic and energetic dysfunctions, patients with glycaemic associated metabolic disorders, and their conditions cannot be controlled with common antidiabetic drugs [34, 35]. Coronary artery disease, left ventricular hypertrophy, and CKD are common associated diseases that explain the worse outcome observed in these patients. Current overlapping makes difficult the distinction between cardiac structural abnormalities related to primitive diabetic damage or associated conditions.
HF prevalence and outcomes in the diabetic population
Several trials suggested T2DM begets HF and vice versa. The prevalence of HF in diabetic population is wide and it is related to HF definition and inclusion criteria that are often misleading [3, 4]. Of note, interventional trials demonstrated a mild reduction in CV events with glucose-lowering treatment if associated with other lifestyle modification and dietary programs, but the risk for HF remains increased [36, 37]. In a Scottish echocardiographic study, 71% of diabetic subjects experienced LV hypertrophy and 41% had diastolic dysfunction [38]. LV is associated with increased collagen expression and extracellular fibrotic expansion, leading to increasing cardiac stiffness, reduced longitudinal contraction, and increased vascular shear stress [39,40,41]. Notably, a retrospective analysis from diabetic patients with HFpEF showed increased LV thickness, left atrial enlargement, reduced quality of life associated with a higher rate hospitalization, and CV death, compared to non-diabetic subjects [42]. In this study, the authors observed a U-shaped trend in HbAc1, with the lowest risk of death in patients with moderate glucose control and higher risk in those with the optimal HbAc1 level; this suggests that simple reduction of glycemic levels is not the optimal treatment [43, 44].
A number of studies have also demonstrated the worse outcome of HF patients affected by T2DM. The increased all-cause mortality of HF patients affected by T2DM show some differences related to geographical area, population characteristics, and disease severity. In northern Europe and US registries, the prevalence of T2DM in HF patients is around 20%, whereas two studies conducted in different European countries reported a significant higher rate of T2DM in HF patients, despite lower body mass and younger age [28, 45,46,47]. Additionally, the prevalence of cardiac dysfunction and early stage of HF in asymptomatic diabetic patients ranges between 30 and 40%, and it is more prevalent in women and older subjects [48, 49]. Patients with T2DM have a 30% greater risk of requiring hospitalization for acute HF than do patients without T2DM. These patients experience a threefold greater risk of hospitalization for recurrent decompensation. The REACH study demonstrates an increased risk for hospitalization (HR 4.73) and a higher risk for CV mortality (HR 2.45) in patients with both HF and T2DM [50]. In the Swedish HF registry, absolute mortality is 48% in women with T2DM vs 40% in women without T2DM, and mortality rates in males are 43% and 35%, respectively [51]. Similarly, the Rotterdam study found that 17.5% of HF patients had T2DM and they revealed an increased risk for CV mortality during a mean 6.2 years follow-up (HR 3.19) [27]. In the post hoc analysis from CHARM, the adjusted HR for combined risk of mortality and hospitalization showed an increased HR both in HFrEF (1.64) and HFpEF (2.04) when compared to non-diabetic patients [29]. The more recent PARADIGM trial reveals that a consistent percentage of patients with T2DM (35%) have a higher risk of the primary composite outcome of HF hospitalization and cardiovascular mortality compared with those without a history of T2DM (HR 1.38) [52]. The long-term HFA registry [28] reveals higher cumulative rates of 1-year CV mortality (HR 1.28) and HF hospitalization (HR 1.37) independent of other risk factors. The mortality risk appears to be similarly independent of HF etiology and subtype. T2DM is associated with greater risk of CV mortality and HF hospitalization in subjects with HFpEF compared to those with HFrEF (HR 2.0 vs 1.6). The rates of adverse CV events per 1000 patients/years are 119 and 75 for diabetic and non-diabetic patients with low EF, respectively. For HFpEF, the rates are 58 and 31 for diabetic and non-diabetic patients, respectively [36]. In the I-PRESERVE study, hospitalization for HF occurred in 34% of diabetic patients vs 22% of those without diabetes, and diabetics had an increased HR mortality risk of 1.59 [53] (Table 1).
Finally, a meta-analysis including 12 trials with both acute and chronic HF patients and different EF thresholds confirms that T2DM is associated with increased risk of CV mortality (HR 1.34) and combined endpoint of mortality and HF hospitalization (HR 1.41) during a mean follow-up period of 3 years [54]. The increased risk of CV mortality is strictly related to baseline conditions and an increased CV risk burden. Most of these data come from HF registries, whereas studies in T2DM are often affected by several gaps making HF definition and occurrence inconsistent [55, 56]. The proportion of HF patients varied between 10 and 27% according with the criteria used to assess its presence. Most of studies reported NYHA class but did not HF treatment. Most of the trials included HF events among all the other MACE, without a pre-specified analysis. Finally, although the last studies considered the occurrence of HF hospitalization as event, they did not provide analyses about other end-points such as outpatients’ HF worsening or changes in their HF treatment [55, 56].
Additionally, patients with T2DM have worse NYHA class, reduced exercise tolerance, and peak oxygen uptake [57]. Finally, patients in the early stages of HF and LV dysfunction are more likely to progress to a symptomatic state compared to non-diabetics, and they experience higher congestion score and increased myocardial damage, as assessed by traditional laboratory screening (i.e., troponin and natriuretic peptides) [58, 59].
Heart failure leading to diabetes
The pathophysiological background underlying the greater incidence of T2DM in HF patients is complex and mainly related to the presence of insulin resistance in HF patients [60, 61], even in the absence of pathologically elevated fasting glucose plasma levels [62]. Insulin resistance is determined by different factors, including neuro-hormonal activation. In particular, sympathetic nervous system overactivity plays a key role in the development of insulin resistance [63, 64]. This could be due to the stimulation of alpha-adrenergic receptors by catecholamines, a process that causes vasoconstriction and hypoperfusion at the level of skeletal muscle and is responsible for reduced glucose uptake [64]. Catecholamine-mediated insulin resistance could be also related to increased oxidative stress [63], lipolysis, and availability of free fatty acids availability, as well as to reduced skeletal muscle glucose uptake, glucose metabolism, and increased hepatic gluconeogenesis [64].
The greater risk of new onset T2DM in HF patients could be also the result of overactivity of the renin–angiotensin–aldosterone system (RAAS). In particular, increased angiotensin II (AT2) levels could be responsible for skeletal muscle vasoconstriction, which is associated with reduced glucose delivery and insulin sensitivity [65]. Moreover, AT2 is able to promote fibrosis, inflammation, apoptosis, and β-cell death in the pancreas, thus affecting insulin production [65]. The negative metabolic effects of RAAS could be also mediated by increased serum aldosterone levels [66,67,68]. Aldosterone, by activating mineralocorticoid receptors (MRs), can alter insulin sensitivity at the level of peripheral tissue [69] and can also induce inflammation at the level of pancreatic β‐cells, thus affecting insulin secretion [70].
Aside from sympathetic nervous system and RAAS overactivity, an altered glucose metabolism could also be related to the reduced activity of the natriuretic peptides (NPs) system [71]. NPs counteract RAAS and SNA [72] by promoting natriuresis and diuresis, exerting an antifibrotic effect at the cardiac level, causing vasodilation, and inhibiting RAAS. Although NP serum levels increase with the progression of HF, the effectiveness of natriuretic peptides is reduced because of an altered target organ responsiveness, overactivation of RAAS and SNA, and decreased availability of biologically active natriuretic peptides [73]. In obese patients or in those with metabolic syndrome, increased NP clearance could be related to an increased removal of the peptides by adipose tissue [74]. It is worth noting that in the presence of low serum levels of NPs, an increased risk of new onset T2DM has been observed [75]. This is due to the favorable metabolic effects of natriuretic peptides, NPs which are responsible for improved insulin sensitivity, increased lipolysis of brown fat, lipid oxidation, reduced ghrelin secretion, and reduction of the inflammatory status [73]. This last condition is also among the main factors that predispose a patient to the new onset of T2DM in HF due to the effects of cytokines and the related oxidative stress in HF [76].
Among the factors leading to the new onset T2DM in HF patients, limited physical activity and its impact on insulin sensitivity is worth noting. Reduced daily activity could be the result of non-adherence to an advised lifestyle, or it could be the consequence of the severity of HF. In both cases, reduced skeletal muscle perfusion and hypoxia lead to insulin resistance. Moreover, the loss of muscle mass could lead to a vicious cycle of worse functional limitations and insulin sensitivity [60,61,62].
Epidemiological data also demonstrate a greater incidence of new onset T2DM in patients affected by HF. In the Kaiser Permanente Northwest group, among 58,056 non-diabetic adults aged ≥ 30 years, HF was independently associated with an increase in T2DM at an incidence rate of 48% (95% confidence interval, CI, 27–73%); i.e., the incidence in HF diabetic patients is 13.6/1000 persons per year vs 9.2/1000 persons per year in non-diabetics [11]. In the analysis of a Danish registry involving 104,522 HF subjects with a first HF hospitalization and a mean follow-up of 3.9 years, 10% of the patients were diagnosed with new onset of T2DM. The incidence rate ranged from 2 per 100 persons per year in the first years up to 3 per 100 persons per year after 5 years of follow-up. Patients with new onset of T2DM also show a higher risk of death (HR 1.47; 95% CI 1.42–1.52) [77]. The greater incidence of T2DM in HF patients is also observed among elderly patients [78]. Moreover, the worse the functional capacity [79, 80] or the greater body mass index [81], the higher the risk of new onset T2DM.
HF therapy, T2DM occurrence, and glycemic control
Currently, different classes of drugs are recommended in order to improve the prognosis of HF patients, especially those with HFrEF [82]. The drugs are able to modulate neuro-hormonal system activity, control heart rate, and solve congestion. All these classes of drugs have been studied in order to evaluate their effects on glucose metabolism (Fig. 2).

Pathophysiologic background leading to diabetes in heart failure patients and the influence of heart failure therapy on the risk of developing diabetes
Beta-blockers are the cornerstone of the therapeutic approach for HFrEF, because they counteract sympathetic nervous system overactivity and greatly improve patients’ prognosis. However, some studies have shown that the administration of beta-blockers could be associated with a worse glycemic status [83, 84]. The unfavorable metabolic effects are related to different mechanisms, such as the reduction of insulin secretion and insulin resistance [85]. Moreover, in the presence of a beta-blocker therapy, increased levels of catecholamines could activate alpha-adrenergic receptors and induce skeletal muscle vasoconstriction, leading to skeletal muscle hypoperfusion and reduction in glucose uptake [85]. This condition could be even more evident in therapies using a non-selective beta-blocker, due to the loss of beta-2 adrenergic receptor-mediated vasodilation [85]. However, beta-blockers are a heterogeneous class of drugs and the most recent ones, due to their ancillary actions, do not have the same unfavorable metabolic effects [86,87,88,89]. Carvedilol is a non-selective blocker of beta-adrenergic receptors and is also able to block alpha-adrenergic receptors, thus increasing skeletal muscle perfusion [88]. Moreover, carvedilol is able to reduce oxidative stress [88]. These mechanisms could explain the ability of carvedilol to exert a more favorable metabolic effect than metoprolol in the COMET trial [86]. In 2,298 patients without T2DM at baseline, a new onset T2DM was observed more frequently in the metoprolol group than in the carvedilol group (12.6 vs 10.3; HR: 0.78; 95%CI: 0.61–0.997; p: 0.048) [86]. Moreover, a greater incidence of diabetic events (diabetic coma, peripheral gangrene, diabetic foot, decreased glucose tolerance, or hyperglycemia) occurred in the metoprolol group (13 vs 10.6%; HR: 0.78; 95%CI: 0.61–0.99; p: 0.039). These results are further supported by the GEMINI trial, in which carvedilol and metoprolol effects in hypertensive diabetic patients were evaluated [88]. HbA1c increases with metoprolol but not with carvedilol, whereas insulin sensitivity improves with carvedilol but not metoprolol. Finally, the progression of microalbuminuria is less frequent with carvedilol. Nebivolol could have a more favorable metabolic profile [89]. Nebivolol is a selective beta-1 adrenergic receptor blocker which has, among other ancillary effects, nitric oxide-mediated vasodilatory and antioxidative properties [89]. Finally, bisoprolol has demonstrated to have a neutral effect on the glycemic control [90].
ACE inhibitors, angiotensin receptor blockers, and sacubitril/valsartan
Both angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) have been demonstrated to not only improve the prognosis in patients with HFrEF [91] but also to reduce the number of new onset T2DM cases [82,83,84,85,86,87,88,89,90,91,92,93]. These results are in line with previous studies of hypertensive patients that have demonstrated the ability of RAAS inhibitors to prevent T2DM [94, 95]. The mechanisms by which RAASi exert their protective effects against T2DM are not completely known. RAASi are responsible for vasodilatory effects, mediated by prostaglandin and nitric oxide pathways that lead to an improvement in skeletal muscle blood flow and glucose uptake [96]. ACEi could potentiate these effects by inhibiting the degradation of bradykinin [97]. Finally, the inhibition of AT2 vasoconstrictive effect in the pancreas increases islet blood flow, thus improving insulin release [98].
The favorable metabolic effects of valsartan are enhanced by the concomitant inhibition of neprilysin by sacubitril. Sacubitril/valsartan is able to further improve HFrEF prognosis when compared with enalapril [99], and it has been associated with better control of glycemic status [100] compared to enalapril. This effect could be caused by the inhibition of neprilysin and the increased availability of natriuretic peptides, which, as mentioned previously, improve metabolic status [71]. Moreover, it has been hypothesized that sacubitril, by inhibiting neprilysin, is also able to reduce the degradation of type 1 glucagon-like peptide (GLP1), thus further improving glycemic control [101].
Mineralcorticoid antagnists (MRA)
have demonstrated to improve outcome and are currently recommended to treat HFrEF patients [82]. A retrospective analysis from EPHESUS revealed that eplerenone reduces the risk of CV mortality by 17% in diabetic patients and the absolute risk reduction was much more significant in diabetic vs non diabetic subjects [102].
Although some concerns have been hypothesized about potential relation between MRA and increased incidence of T2DM, the EMPHASIS trial showed the eplerenone administration has neutral effects on new onset diabetes in HFrEF [103]. Moreover, in a TOCAT sub-analysis, in T2DM patients with LVEF ≥ 45%, the extracellular matrix deposition is overexpressed and the spironolactone treatment attenuates inflammatory and profibrotic biomarkers [104]. Overall, these findings demonstrate an optimal safety and additional positive effects of MRA in patients with both T2DM and HF.
Diuretics
In contrast to sacubitril/valsartan, thiazides and loop diuretic effects are unfavorable from a metabolic point of view [105,106,107] because they lead to impaired glucose tolerance, which is probably related to insulin resistance. This is a dose-dependent relationship that is reversible after diuretic withdrawal. The hyperglycemic effects could be related to hypokalemic effects [108] or to increased hepatic fat [109].
The association of loop diuretic dosage (furosemide equivalents) 90 days after discharge with risk of T2DM was evaluated in a Danish registry of 99,362 patients [110]. The study found that loop diuretic dosages are associated with an increased risk of developing T2DM in a dose-dependent manner. Concomitant use of renin-angiotensin system inhibitors attenuates the risk [110].
Ivabradine
In this case "Ivabradine" as indicated of persistence of a high sinus heart rate after uptitration of beta-blockers, the use of ivabradine is recommended in order to control heart rate [82]. In a group of patients with coronary artery disease, the administration of ivabradine was found to be associated with a reduction of fasting glucose levels and glycated hemoglobin [111]. These data support the possible neutral or favorable effect of ivabradine on glucose metabolism.
Conclusion
The data from experimental, observational, and randomized control trials clearly demonstrate the double link between T2DM and HF. Patients with T2DM present an increased risk of new onset of HF as well as HF-related events. On the other hand, HF patients present an increased risk of new onset T2DM. Both HF in T2DM and T2DM in HF are associated with a worse prognosis. These data are even more relevant considering the new therapeutic opportunities derived by the administration of SGLT2i [15, 16, 112,113,114].
Change history
04 September 2022
The original version of this paper was updated to add funding note.
References
Morrish JN, Wang S-L, Stevens KL, Fuller HJ, Keen H (2001) Mortality and causes of death in the WHO multinational study of vascular disease in diabetes. Diabetologia 44:S14–S21. https://doi.org/10.1007/pl00002934
Garcia MJ, McNamara PM, Gordon T, Kannel WB (1974) Morbidity and mortality in diabetics in the Framingham population. Sixteen year follow-up study Diabetes 23:105–111. https://doi.org/10.2337/diab.23.2.105
Nichols GA, Gullion CM, Koro CE, Ephross SA, Brown JB (2004) The incidence of congestive heart failure in type 2 diabetes: an update. Diabetes Care 27:1879–1884. https://doi.org/10.2337/diacare.27.8.1879
McMurray JJ, Gerstein HC, Holman RR, Pfeffer MA (2014) Heart failure: a cardiovascular outcome in diabetes that can no longer be ignored. Lancet Diabetes Endocrinol 2:843–851. https://doi.org/10.1016/S2213-8587(14)70031-2
Fitchett DH, Udell JA, Inzucchi SE (2017) Heart failure outcomes in clinical trials of glucose-lowering agents in patients with diabetes. Eur J Heart Fail 19:43–53. https://doi.org/10.1002/ejhf.633
Fitchett D, Butler J, van de Borne P et al (2018) Effects of empagliflozin on risk for cardiovascular death and heart failure hospitalization across the spectrum of heart failure risk in the EMPA-REG Outcome trial. Eur Heart J 39:363–370. https://doi.org/10.1093/eurheartj/ehx511
Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL, Goff DC Jr (2004) Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care 27:699–703. https://doi.org/10.2337/diacare.27.3.699
Duckworth W, Abraira C, Moritz T et al (2009) Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 360:129–39. https://doi.org/10.1056/NEJMoa0808431
Levelt E, Gulsin G, Neubauer S, McCann GP (2018) Mechanisms in endocrinology: Diabetic cardiomyopathy: pathophysiology and potential metabolic interventions state of the art review. Eur J Endocrinol 178:R127-R139. https://doi.org/10.1530/EJE-17-0724
Seferović PM, Paulus WJ (2015) Clinical diabetic cardiomyopathy: a two-faced disease with restrictive and dilated phenotypes. Eur Heart J 36:1718–27. https://doi.org/10.1093/eurheartj/ehv134
Nichols GA, Moler EJ (2011) Cardiovascular disease, heart failure, chronic kidney disease and depression independently increase the risk of incident diabetes. Diabetologia 54:523–526. https://doi.org/10.1093/eurheartj/ehv134
Bozkurt B, Coats AJS, Tsutsui H et al (2021) Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail 23:352–380. https://doi.org/10.1002/ejhf.2115
Rao Kondapally Seshasai S, Kaptoge S, Emerging TA, Collaboration RF et al (2011) Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med 364:829–841. https://doi.org/10.1056/NEJMoa1008862
Cosentino F, Grant PJ, Aboyans V et al (2020) 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 41:255–323. https://doi.org/10.1093/eurheartj/ehz486
Fitchett D, Inzucchi SE, Cannon CP et al (2019) Empagliflozin reduced mortality and hospitalization for heart failure across the spectrum of cardiovascular risk in the EMPA-REG OUTCOME trial. Circulation 139:1384–1395. https://doi.org/10.1161/CIRCULATIONAHA.118.037778
Kato ET, Silverman MG, Mosenzon O et al (2019) Effect of dapagliflozin on heart failure and mortality in type 2 diabetes mellitus. Circulation 139:2528–2536. https://doi.org/10.1161/CIRCULATIONAHA.119.040130
Gerstein H, Yusuf S, Riddle MC et al (2008) Rationale, design, and baseline characteristics for a large international trial of cardiovascular disease prevention in people with dysglycemia: the ORIGIN Trial (Outcome Reduction with an Initial Glargine Intervention). Am Heart J 155(26–32):32.e1–6. https://doi.org/10.1016/j.ahj.2007.09.009
Marso SP, Baeres FMM, Bain SC et al (2020) LEADER Trial Investigators. Effects of liraglutide on cardiovascular outcomes in patients with diabetes with or without heart failure. J Am Coll Cardiol 75:1128–1141. https://doi.org/10.1016/j.jacc.2019.12.063
Sacre JW, Magliano DJ, Shaw JE (2021) Heart failure hospitalisation relative to major atherosclerotic events in type 2 diabetes with versus without chronic kidney disease: a meta-analysis of cardiovascular outcomes trials. Diabetes Metab 47:101249. https://doi.org/10.1016/j.diabet.2021.101249
Pazin-Filho A, Kottgen A, Bertoni AG, Russell SD, Selvin E et al (2008) HbA 1c as a risk factor for heart failure in persons with diabetes: the Atherosclerosis Risk in Communities (ARIC) study. Diabetologia 51:2197–2204. https://doi.org/10.1007/s00125-008-1164-z
Thrainsdottir IS, Aspelund T, Thorgeirsson G et al (2005) The association between glucose abnormalities and heart failure in the population-based Reykjavik study. Diabetes Care 28:612–6. https://doi.org/10.2337/diacare.28.3.612
Segar MW, Patel KV, Vaduganathan M, Caughey MC, Butler J et al (2020) Association of long-term change and variability in glycemia with risk of incident heart failure among patients with type 2 diabetes: a secondary analysis of the ACCORD trial. Diabetes Care 43:1920–1928. https://doi.org/10.2337/dc19-2541
Echouffo-Tcheugui JB, Xu H, DeVore AD et al (2016) Temporal trends and factors associated with diabetes mellitus among patients hospitalized with heart failure: findings from Get With The Guidelines-Heart Failure registry. Am Heart J 182:9–20. https://doi.org/10.1016/j.ahj.2016.07.025
van Riet EE, Hoes AW, Wagenaar KP, Limburg A, Landman MA, Rutten FH (2016) Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail 18:242–252. https://doi.org/10.1002/ejhf.483
Savarese G, Sattar N, Januzzi J et al (2019) Empagliflozin is associated with a lower risk of post-acute heart failure rehospitalization and mortality. Circulation 139:1458–1460. https://doi.org/10.1161/CIRCULATIONAHA.118.038339
Jhund PS, Ponikowski P, Docherty KF et al (2021) Dapagliflozin and recurrent heart failure hospitalizations in heart failure with reduced ejection fraction: an analysis of DAPA-HF. Circulation 143:1962–1972. https://doi.org/10.1161/CIRCULATIONAHA.121.053659
Mosterd A, Cost B, Hoes AW, de Bruijne MC, Deckers JW, Hofman A, Grobbee DE (2001) The prognosis of heart failure in the general population: the Rotterdam Study. Eur Heart J 22:1318–27. https://doi.org/10.1053/euhj.2000.2533
Targher G, Dauriz M, Laroche C et al (2017) ESC-HFA HF Long-Term Registry investigators. In-hospital and 1-year mortality associated with diabetes in patients with acute heart failure: results from the ESC-HFA Heart Failure Long-Term Registry. Eur J Heart Fail 19:54–65. https://doi.org/10.1002/ejhf.679
MacDonald MR, Petrie MC, Varyani F et al (2008) Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J 29:1377–85. https://doi.org/10.1093/eurheartj/ehn153
Cooper LB, Yap J, Tay WT, Teng TK, MacDonald M, Anand IS, Sharma A, O’Connor CM, Kraus WE, Mentz RJ, Lam CS, HF-ACTION and ASIAN-HF Investigators. (2018) Multi-ethnic comparisons of diabetes in heart failure with reduced ejection fraction: insights from the HF-ACTION trial and the ASIAN-HF registry. Eur J Heart Fail 20(9):1281–1289. https://doi.org/10.1002/ejhf.1223
Gargiulo P, Marsico F, Renga F et al (2020) The metabolic syndrome in heart failure: insights to specific mechanisms. Heart Fail Rev 25:1–7. https://doi.org/10.1007/s10741-019-09838-6
Randhawa VK, Dhanvantari S, Connelly KA (2021) How diabetes and heart failure modulate each other and condition management. Can J Cardiol 37:595–608. https://doi.org/10.1016/j.cjca.2020.11.014
Frati G, Schirone L, Chimenti I et al (2017) An overview of the inflammatory signalling mechanisms in the myocardium underlying the development of diabetic cardiomyopathy. Cardiovasc Res 113:378–388. https://doi.org/10.1093/cvr/cvx011
Jia G, Hill MA, Sowers JR (2018) Diabetic cardiomyopathy: an update of mechanisms contributing to this clinical entity. Circ Res 122:624–638. https://doi.org/10.1161/CIRCRESAHA.117.311586
Evangelista I, Nuti R, Picchioni T, Dotta F, Palazzuoli A (2019) Molecular dysfunction and phenotypic derangement in diabetic cardiomyopathy. Int J Mol Sci 20:3264. https://doi.org/10.3390/ijms20133264
Kannel WB, Hjortland M, Castelli WP (1974) Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 34:29–34. https://doi.org/10.1016/0002-9149(74)90089-7
Kodama S, Fujihara K, Horikawa C et al (2020) Diabetes mellitus and risk of new-onset and recurrent heart failure: a systematic review and meta-analysis. ESC Heart Fail 7:2146–2174. https://doi.org/10.1002/ehf2.12782
Dawson A, Morris AD, Struthers AD (2005) The epidemiology of left ventricular hypertrophy in type 2 diabetes mellitus. Diabetologia 48:1971–9. https://doi.org/10.1007/s00125-005-1896-y
Struthers AD, Morris AD (2002) Screening for and treating left-ventricular abnormalities in diabetes mellitus: a new way of reducing cardiac deaths. Lancet 359:1430–2. https://doi.org/10.1016/S0140-6736(02)08358-7
Das SR, Drazner MH, Yancy CW, Stevenson LW, Gersh BJ, Dries DL (2004) Effects of diabetes mellitus and ischemic heart disease on the progression from asymptomatic left ventricular dysfunction to symptomatic heart failure: a retrospective analysis from the Studies of Left Ventricular Dysfunction (SOLVD) Prevention trial. Am Heart J 148:883–888. https://doi.org/10.1016/j.ahj.2004.04.019
Berg DD, Freedman BL, Bonaca MP et al (2021) Cardiovascular biomarkers and heart failure risk in stable patients with atherothrombotic disease: a nested biomarker study from TRA 2°P-TIMI 50. J Am Heart Assoc 10:e018673. https://doi.org/10.1161/JAHA.120.018673
Kristensen SL, Mogensen UM, Jhund PS et al (2017) Clinical and echocardiographic characteristics and cardiovascular outcomes according to diabetes status in patients with heart failure and preserved ejection fraction: a report from the I-Preserve Trial (Irbesartan in Heart Failure With Preserved Ejection Fraction). Circulation 135:724–735. https://doi.org/10.1161/CIRCULATIONAHA.116.024593
Paulus WJ, Dal Canto E (2018) Distinct myocardial targets for diabetes therapy in heart failure with preserved or reduced ejection fraction. JACC Heart Fail 6:1–7. https://doi.org/10.1016/j.jchf.2017.07.012
Seferović PM, Petrie MC, Filippatos GS et al (2018) Type 2 diabetes mellitus and heart failure: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 20:853–872. https://doi.org/10.1002/ejhf.1170
From AM, Leibson CL, Bursi F, Redfield MM, Weston SA, Jacobsen SJ, Rodeheffer RJ, Roger VL (2006) Diabetes in heart failure: prevalence and impact on outcome in the population. Am J Med 119:591–599. https://doi.org/10.1016/j.amjmed.2006.05.024
Dauriz M, Targher G, Temporelli PL, Lucci D, Gonzini L, Nicolosi GL, Marchioli R, Tognoni G, Latini R, Cosmi F, Tavazzi L, Maggioni AP, Investigators GISSI-HF (2017) Prognostic impact of diabetes and prediabetes on survival outcomes in patients with chronic heart failure: a post-hoc analysis of the GISSI-HF (Gruppo Italiano per lo Studio della Sopravvivenza nella Insufficienza Cardiaca-Heart Failure) Trial. J Am Heart Assoc 6:e005156. https://doi.org/10.1161/JAHA.116.005156
Kistorp C, Galatius S, Gustafsson F, Faber J, Corell P, Hildebrandt P (2005) Prevalence and characteristics of diabetic patients in a chronic heart failure population. Int J Cardiol 100(2):281–287. https://doi.org/10.1016/j.ijcard.2004.10.024
Aronow WS, Ahn C (1999) (1999) Incidence of heart failure in 2,737 older persons with and without diabetes mellitus. Chest 115:867–868. https://doi.org/10.1378/chest.115.3.867
Boonman-de Winter LJ, Rutten FH, Cramer MJ et al (2012) High prevalence of previously unknown heart failure and left ventricular dysfunction in patients with type 2 diabetes. Diabetologia 55:2154–2162. https://doi.org/10.1007/s00125-012-2579-0
Cavender MA, Steg PG, Smith SC Jr et al (2015) Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: outcomes at 4 years from the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Circulation 132:923–31. https://doi.org/10.1161/CIRCHEARTFAILURE.117.004646
Johansson I, Dahlström U, Edner M, Näsman P, Rydén L, Norhammar A (2015) Risk factors, treatment and prognosis in men and women with heart failure with and without diabetes. Heart 101:1139–48. https://doi.org/10.1136/heartjnl-2014-307131
Kristensen SL, Preiss D, Jhund PS et al (2016) Risk related to pre-diabetes mellitus and diabetes mellitus in heart failure with reduced ejection fraction: insights from prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial. Circ Heart Fail 9:e002560. https://doi.org/10.1161/CIRCHEARTFAILURE.115.002560
Komajda M, Carson PE, Hetzel S et al (2011) Factors associated with outcome in heart failure with preserved ejection fraction: findings from the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE). Circ Heart Fail 4:27–35. https://doi.org/10.1161/CIRCHEARTFAILURE.109.932996
Dauriz M, Mantovani A, Bonapace S et al (2017) Prognostic impact of diabetes on long-term survival outcomes in patients with heart failure: a meta-analysis. Diabetes Care 40:1597–1605. https://doi.org/10.2337/dc17-0697
Greene SJ, Vaduganathan M, Khan MS et al (2018) Prevalent and incident heart failure in cardiovascular outcome trials of patients with type 2 diabetes. J Am Coll Cardiol 71:1379–1390. https://doi.org/10.1016/j.jacc.2018.01.047
Dei Cas A, Khan SS, Butler J et al (2015) Impact of diabetes on epidemiology, treatment, and outcomes of patients with heart failure. JACC Heart Fail 3(2):136–145. https://doi.org/10.1016/j.jchf.2014.08.004 (PMID: 25660838)
Suskin N, McKelvie RS, Burns RJ et al (2000) Glucose and insulin abnormalities relate to functional capacity in patients with congestive heart failure. Eur Heart J 21:1368–1375
Banks AZ, Mentz RJ, Stebbins A et al (2016) Response to exercise training and outcomes in patients with heart failure and diabetes mellitus: insights from the HF-ACTION trial. J Card Fail 2016(22):485–491
Zelniker TA, Morrow DA, Mosenzon O et al (2021) Relationship between baseline cardiac biomarkers and cardiovascular death or hospitalization for heart failure with and without sodium-glucose co-transporter 2 inhibitor therapy in DECLARE-TIMI 58. Eur J Heart Fail 23:1026–1036. https://doi.org/10.1002/ejhf.2073
Swan JW, Walton C, Godsland IF, Clark AL, Coats AJ, Oliver MF (1994) Insulin resistance in chronic heart failure. Eur Heart J 15:1528–1532. https://doi.org/10.1016/s0735-1097(97)00185-x
Paolisso G, De Riu S, Marrazzo G, Verza M, Varricchio M, D’Onofrio F (1991) Insulin resistance and hyperinsulinemia in patients with chronic congestive heart failure. Metabolism 40:972–977. https://doi.org/10.1016/0026-0495(91)90075-8
Kostis JB, Sanders M (2005) The association of heart failure with insulin resistance and the development of type 2 diabetes. Am J Hypertens 18:731–737. https://doi.org/10.1016/j.amjhyper.2004.11.038
Palatini P, Julius S (1997) Association of tachycardia with morbidity and mortality: pathophysiological considerations. J Hum Hypertens 11(Suppl 1):S19–S27
Hayden MR, Tyagi SC (2003) Myocardial redox stress and remodeling in metabolic syndrome, type 2 diabetes mellitus, and congestive heart failure. Med Sci Monit 9:SR35–SR52
Jandeleit-Dahm KA, Tikellis C, Reid CM, Johnston CI, Cooper ME (2005) Why blockade of the renin-angiotensin system reduces the incidence of new-onset diabetes. J Hypertens 23:463–473. https://doi.org/10.1097/01.hjh.0000160198.05416.72
Briet M, Schiffrin EL (2011) The role of aldosterone in the metabolic syndrome. Curr Hypertens Rep 13:163–172. https://doi.org/10.1007/s11906-011-0182-2
Hitomi H, Kiyomoto H, Nishiyama A et al (2007) Aldosterone suppresses insulin signaling via the downregulation of insulin receptor substrate-1 in vascular smooth muscle cells. Hypertension 50:750–755. https://doi.org/10.1161/HYPERTENSIONAHA.107.093955
Buglioni A, Cannone V, Sangaralingham SJ et al (2015) Aldosterone predicts cardiovascular, renal, and metabolic disease in the general community: a 4-year follow-up. J Am Heart Assoc 4:e002505. https://doi.org/10.1161/JAHA.115.002505
Luther JM (2014) Effects of aldosterone on insulin sensitivity and secretion. Steroids 91:54–60. https://doi.org/10.1016/j.steroids.2014.08.016
Whaley-Connell A, Johnson MS, Sowers JR (2010) Aldosterone: role in the cardiometabolic syndrome and resistant hypertension. Prog Cardiovasc Dis 52:401–409. https://doi.org/10.1016/j.pcad.2009.12.004
Coué M, Moro C (2016) Natriuretic peptide control of energy balance and glucose homeostasis. Biochimie 124:84–91. https://doi.org/10.1016/j.biochi.2015.05.017
Buggey J, Mentz RJ, DeVore AD, Velazquez EJ (2015) Angiotensin receptor neprilysin inhibition in heart failure: mechanistic action and clinical impact. J Card Fail 21:741–750. https://doi.org/10.1016/j.cardfail.2015.07.008
Díez J (2017) Chronic heart failure as a state of reduced effectiveness of the natriuretic peptide system: implications for therapy. Eur J Heart Fail 19:167–176. https://doi.org/10.1002/ejhf.656
Wang TJ, Larson MG, Levy D et al (2004) Impact of obesity on plasma natriuretic peptide levels. Circulation 109;594e600. https://doi.org/10.1161/01.CIR.0000112582.16683.EA
Magnusson M, Jujic A, Hedblad B et al (2012) Low plasma level of atrial natriuretic peptide predicts development of diabetes: the prospective Malmo Diet and Cancer study. J Clin Endocrinol Metab 97:638–645. https://doi.org/10.1210/jc.2011-2425
Suthahar N, Meijers WC, Brouwers FP et al (2018) Heart failure and inflammation-related biomarkers as predictors of new-onset diabetes in the general population. Int J Cardiol 250:188–194. https://doi.org/10.1016/j.ijcard.2017.10.035
Zareini B, Rørth R, Holt A, Mogensen UM et al (2019) Heart failure and the prognostic impact and incidence of new-onset of diabetes mellitus: a nationwide cohort study. Cardiovasc Diabetol 18:79. https://doi.org/10.1186/s12933-019-0883-4
Amato L, Paolisso G, Cacciatore F et al (1997) Congestive heart failure predicts the development of non-insulin-dependent diabetes mellitus in the elderly. The Osservatorio Geriatrico Regione Campania Group. Diabetes Metab 23:213–218
Swan JW, Anker SD, Walton C et al (1997) Insulin resistance in chronic heart failure: relation to severity and etiology of heart failure. J Am Coll Cardiol 30:527–532. https://doi.org/10.1016/s0735-1097(97)00185-x
Tenenbaum A, Motro M, Fisman EZ, Leor J, Freimark D, Boyko V, Mandelzweig L, Adler Y, Sherer Y, Behar S (2003) Functional class in patients with heart failure is associated with the development of diabetes. Am J Med 114:271–275. https://doi.org/10.1016/s0002-9343(03)00392-9
Schmiegelow M, Andersson C, Olesen JB, Abildstrom SZ, Kober L, Torp-Pedersen C (2011) Body mass index is closely correlated to incident diabetes in patients with heart failure or myocardial infarction. Eur J Cardiovasc Prev Rehabil 18:305–311. https://doi.org/10.1177/1741826710389420
McDonagh TA, Metra M, Adamo M et al (2021) 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 42:3599–3726. https://doi.org/10.1093/eurheartj/ehab368
Dornhorst A, Powell SH, Pensky J (1985) Aggravation by propranolol of hyperglycaemic effect of hydrochlorothiazide in type II diabetics without alteration of insulin secretion. Lancet 1:123–126. https://doi.org/10.1016/s0140-6736(85)91900-2
Holzgreve H, Nakov R, Beck K et al (2003) Antihypertensive therapy with verapamil SR plus trandolapril versus atenolol plus chlorthalidone on glycemic control. Am J Hypertens 16:381–386. https://doi.org/10.1016/s0895-7061(03)00062-1
Pollare T, Lithell H, Selinus I, Berne C (1989) Sensitivity to insulin during treatment with atenolol and metoprolol: a randomised, double blind study of effects on carbohydrate and lipoprotein metabolism in hypertensive patients. BMJ 298:1152–1157. https://doi.org/10.1136/bmj.298.6681.1152
Torp-Pedersen C, Metra M, Charlesworth A et al (2007) Effects of metoprolol and carvedilol on pre-existing and new onset diabetes in patients with chronic heart failure: data from the Carvedilol Or Metoprolol European Trial (COMET). Heart 93:968–973. https://doi.org/10.1136/hrt.2006.092379
Ceriello A, Motz E (2004) Is oxidative stress the pathogenic mechanism underlying insulin resistance, diabetes, and cardiovascular disease? The common soil hypothesis revisited. Arterioscler Thromb Vasc Biol 24:816–823. https://doi.org/10.1161/01.ATV.0000122852.22604.78
Bakris GL, Fonseca V, Katholi RE et al (2004) Metabolic effects of carvedilol vs metoprolol in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 292:2227–2236. https://doi.org/10.1001/jama.292.18.2227
Marketou M, Gupta Y, Jain S, Vardas P (2017) Differential metabolic effects of beta-blockers: an updated systematic review of nebivolol. Curr Hypertens Rep 19:22. https://doi.org/10.1007/s11906-017-0716-3
Wai B, Kearney LG, Hare DL, Ord M, Burrell LM, Srivastava PM (2012) Beta blocker use in subjects with type 2 diabetes mellitus and systolic heart failure does not worsen glycaemic control. Cardiovasc Diabetol 11:14. https://doi.org/10.1186/1475-2840-11-14
Vermes E, Ducharme A, Bourassa MG, Lessard M, White M, Tardif JC, Dysfunction SOLV (2003) Enalapril reduces the incidence of diabetes in patients with chronic heart failure: insight from the Studies Of Left Ventricular Dysfunction (SOLVD). Circulation 107:1291–1296. https://doi.org/10.1161/01.cir.0000054611.89228.92
Yusuf S, Ostergren JB, Gerstein HC et al (2005) Candesartan in Heart Failure-Assessment of Reduction in Mortality and Morbidity Program Investigators. Effects of candesartan on the development of a new diagnosis of diabetes mellitus in patients with heart failure. Circulation 112:48–53. https://doi.org/10.1161/CIRCULATIONAHA.104.528166
Yusuf S, Gerstein H, Hoogwerf B et al (2001) Ramipril and the development of diabetes. JAMA 286:1882–1885. https://doi.org/10.1001/jama.286.15.1882
Hansson L, Lindholm LH, Niskanen L et al (1999) Effects of angiotensin converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trial. Lancet 353:611–616. https://doi.org/10.1016/s0140-6736(98)05012-0
Lindholm LH, Ibsen H, Borch-Johnsen K et al (2002) Risk of new-onset diabetes in the losartan intervention for endpoint reduction in hypertension study. J Hypertens 20:1879–1886. https://doi.org/10.1097/00004872-200209000-00035
Balon TW, Nadler JL (1997) Evidence that nitric oxide increases glucose transport in skeletal muscle. J Appl Physiol 82:359–363. https://doi.org/10.1152/jappl.1997.82.1.359
Tomiyama H, Kushiro T, Abeta H et al (1994) Kinins contribute to the improvement of insulin sensitivity during treatment with angiotensin converting enzyme inhibitor. Hypertension 23:450–455. https://doi.org/10.1161/01.hyp.23.4.450
Carlsson PO, Berne C, Jansson L (1998) Angiotensin II and the endocrine pancreas: effects on islet blood flow and insulin secretion in rats. Diabetologia 41:127–133. https://doi.org/10.1007/s001250050880
McMurray JJ, Packer M, Desai AS, for PARADIGM-HF Investigators and Committees. et al (2014) Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371:993–1004. https://doi.org/10.1056/NEJMoa1409077
Seferovic JP, Claggett B, Seidelmann SB et al (2017) Effect of sacubitril/valsartan versus enalapril on glycaemic control in patients with heart failure and diabetes: a post-hoc analysis from the PARADIGM-HF trial. Lancet Diabetes Endocrinol 5:333–340. https://doi.org/10.1016/S2213-8587(17)30087-6
Packer M (2018) Augmentation of glucagon-like peptide-1 receptor signalling by neprilysin inhibition: potential implications for patients with heart failure. Eur J Heart Fail 20:973–977. https://doi.org/10.1002/ejhf.1185
O’Keefe JH, Abuissa H, Pitt B (2008) Eplerenone improves prognosis in postmyocardial infarction diabetic patients with heart failure: results from EPHESUS. Diabetes Obes Metab 10:492–497. https://doi.org/10.1111/j.1463-1326.2007.00730.x
Preiss D, van Veldhuisen DJ, Sattar N, Krum H, Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B, Zannad F, McMurray JJ (2012) Eplerenone and new-onset diabetes in patients with mild heart failure: results from the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF). Eur J Heart Fail 14:909–915. https://doi.org/10.1093/eurjhf/hfs067
De Marco C, Claggett BL, de Denus S et al (2021) Impact of diabetes on serum biomarkers in heart failure with preserved ejection fraction: insights from the TOPCAT trial. ESC Heart Fail 8:1130–1138. https://doi.org/10.1002/ehf2.13153
Elliott WJ, Meyer PM (2007) Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis. Lancet 369:201–207. https://doi.org/10.1016/S0140-6736(07)60108-1
Ramsay LE, Yeo WW, Jackson PR (1992) Diabetes, impaired glucose tolerance and insulin resistance with diuretics. Eur Heart J 13 Suppl G:68–71. https://doi.org/10.1093/eurheartj/13.suppl_g.68
Dronavalli S, Bakris GL (2008) Mechanistic insights into diuretic-induced insulin resistance. Hypertension 52:1009–1011. https://doi.org/10.1161/HYPERTENSIONAHA.108.120923
Zillich AJ, Garg J, Basu S, Bakris GL, Carter BL (2006) Thiazide diuretics, potassium, and the development of diabetes: a quantitative review. Hypertension 48:219 –224. https://doi.org/10.1161/01.HYP.0000231552.10054.aa
Eriksson JW, Jansson P-A, Carlberg B et al (2008) Hydrochlorothiazide, but not candesartan, aggravates insulin resistance and causes visceral and hepatic fat accumulation: the Mechanisms for the Diabetes Preventing Effect of Candesartan Study. Hypertension 52:1030–1037. https://doi.org/10.1161/HYPERTENSIONAHA.108.119404
Demant MN, Gislason GH, Køber L, Vaag A, Torp-Pedersen C, Andersson C (2014) Association of heart failure severity with risk of diabetes: a Danish nationwide cohort study. Diabetologia 57:1595–1600. https://doi.org/10.1007/s00125-014-3259-z
Borer JS, Tardif JC (2010) Efficacy of ivabradine, a selective I(f) inhibitor, in patients with chronic stable angina pectoris and diabetes mellitus. Am J Cardiol 105:29–35. https://doi.org/10.1016/j.amjcard.2009.08.642
Packer M, Anker SD, Butler J et al (2020) Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med 383:1413–1424. https://doi.org/10.1056/NEJMoa2022190
Bhatt DL, Szarek M, Steg PG et al (2021) Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med 384:117–128. https://doi.org/10.1056/NEJMoa2030183
Anker SD, Butler J, Filippatos G et al (2021) Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 385:1451–1461. https://doi.org/10.1056/NEJMoa2107038
Funding
Open access funding provided by Università degli Studi di Trieste within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The manuscript does not contain clinical studies or patient data.
Conflict of interest
M. Iacoviello received honoraria as a consultant in advisory boards from AstraZeneca, Boehringer Ingelheim, Lilly, Merck Serono, Novartis, and Vifor Pharma. A. Palazzuoli received honoraria as a consultant from Menarini and Novartis.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Palazzuoli, A., Iacoviello, M. Diabetes leading to heart failure and heart failure leading to diabetes: epidemiological and clinical evidence. Heart Fail Rev 28, 585–596 (2023). https://doi.org/10.1007/s10741-022-10238-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-022-10238-6