
Abstract
The aim of this article is to evaluate the clinical utility of cardiac injury biomarkers in paediatric age. In December 2015, a literature search was performed (PubMed access to MEDLINE citations; http://www.ncbi.nlm.nih.gov/PubMed/). The search strategy included the following medical subject headings and text terms for the key words: “cardiac injury biomarkers”, “creatine kinase-MB”, “myoglobin”, “troponin”, “children”, “neonate/s”, “newborn/s”, “infant/s” and echocardiography. In the paediatric population, troponins show a good correlation with the extent of myocardial damage following cardiac surgery and cardiotoxic medication and can be used as predictors of subsequent cardiac recovery and mortality. Elevation of cardiac injury biomarkers may also have diagnostic value in cases when cardiac contusion or pericarditis is suspected. Cardiac injury biomarkers are very sensitive markers for the detection of myocardial injury and have been studied in healthy newborns, after tocolysis, intrauterine growth restriction, respiratory distress and asphyxia. The proportion of newborns with elevated troponin was higher than that in ill infants, children, and adolescents and in healthy adults, suggesting that myocardial injury, although clinically occult, is common in this young age group. Results suggest that significant elevation of cord troponin is an excellent early predictor of severity of hypoxic-ischaemic encephalopathy and mortality in term infants. Cardiac biomarkers may also benefit centres without on-site echocardiography with evidence showing good correlation with echo-derived markers of myocardial function. Further studies are needed to better clarify the role of cardiac biomarkers in paediatric age and their correlation with echocardiographic parameters.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
CK-MB, myoglobin and cardiac troponins I and T are cardiac injury biomarkers widely used in the management of adult patients [1, 2]. Interest in these cardiac biomarkers in the management of children has increased; however, there are no current guidelines for their routine use.
Creatine kinase (CK) is a dimeric enzyme, which occurs in four different forms: a mitochondrial isoenzyme and the cytosolic isoenzymes CK-MM (muscle type), CK-BB (brain type) and CK-MB (heart type). CK and its isoenzymes are used for the diagnosis and follow-up of myocardial infarct and muscle dystrophy. Myoglobin is a cytoplasmic protein in striated cardiac and skeletal musculature. It serves to transport oxygen within the myocytes and as an oxygen reservoir. It passes rapidly into the circulation after damage to the myocytes.
The cardiac sarcomere is built of contractile proteins (actin, myosin and tropomyosin) and the troponin complex (Fig. 1). The troponin complex regulates the interaction of the thin (actin and tropomyosin) and thick (myosin) filaments in the striated muscle in response to the concentration of intracellular calcium [3]. Ebashi et al. [4] found that troponin is the Ca2+ receptive protein and proposed the molecular mechanism of regulation of contraction and relaxation. The troponin complex is composed of three subunits called troponin I (affects myosin–actin interactions), T (binds troponin to tropomyosin) and C (binds divalent calcium ions) [5]. Foetal heart contains two troponin I isoforms: the adult troponin I and an isoform similar to the one found in adult slow-twitch skeletal muscle. The latter, that is predominant in the foetus, is replaced with maturation, so that at birth, only adult troponin I is detectable [6].

Schematic representation of the cardiac myofibrillar thin filament. Cardiac troponins exist in a bound form and in a free cytosolic pool and are released from the cardiomyocyte as complexes or as free protein (acknowledge to Servier Medical Art-Image bank)
The kinetics of troponins released in the blood are close to that of creatine kinase-MB (CK-MB), but the return to normal is observed after long periods of time [7]. Activities of total CK and its isoform are usually significantly elevated in patients with myocardial or with skeletal muscle injury as well as in those with renal failure. CK-MB may be expressed in up to 20 % of total CK activity in human skeletal muscle and therefore is not 100 % specific for the heart. Sobki et al. [8] demonstrated cardiac troponins had 100 % sensitivity and negative predictive value, for myocardial injury, as compared with 92 and 96 % for CK activity and 96 and 97 % for creatine kinase-mass. The cardiac troponins are predominantly myofibril bound with only approximately 5–8 % of both troponin I and troponin T being unbound in the cytosol. Cytosolic troponin is released first. In the case of demand ischaemia, the elevation of troponin is relatively smaller and with shorter circulation half-time than seen with necrosis [9].
Troponins appear in blood in 2–4 h after an insult, and peak in about 12 h and then remain elevated for 7–10 days. Positive levels of troponin I may result from reversible membrane damage, not necessarily from cell death [10]. Proposed mechanisms leading to troponin release in heart failure are cardiomyocyte damage caused by inflammatory cytokines or oxidative stress, subendocardial ischaemia, apoptosis and neurohumoral activation [10, 11]. Troponin I was found to be a very sensitive and specific marker of cardiac injury [12–14]. Cardiac troponin I had the highest specificity and positive predictive value (99 and 98 %) as compared with cardiac troponin T (96 and 93 %), creatine kinase-mass (92 and 86 %) and creatine kinase activity (89 and 80 %) [8]. The diagnostic value of troponin I is similar to troponin T, but compared with troponin T has the advantage of not being influenced by renal failure [15]. Troponin I is considered the gold standard for detecting myocardial injury [16]. Myoglobin is a cytoplasmic protein in cardiac and skeletal muscle, and it passes rapidly into circulation after damage to the myocytes [17, 18].
Aims
The aim of this article is to evaluate the clinical utility of cardiac injury biomarkers (creatine kinase-MB, myoglobin and troponin) in paediatric age by reviewing of published studies concerning the diagnostic accuracy, management and prognostic relevance of cardiac injury biomarkers. Was also reviewed the correlation of cardiac injury biomarkers with echocardiographic function parameters.
Methods
In December 2015, a literature search was performed (PubMed access to MEDLINE citations; http://www.ncbi.nlm.nih.gov/PubMed/). The search strategy included the following medical subject headings and text terms for the key words: “cardiac injury biomarkers”, “creatine kinase-MB”, “myoglobin”, “troponin”, “children”, “neonate/s”, “newborn/s”, “infant/s” and “echocardiography”. The search strategy was limited to articles concerning children (<18 years) that were published in the English language. Data were extracted on age, gender, type of clinical condition, cardiac injury biomarkers assay method and cardiac function parameters evaluated by echocardiography.
Results and discussion
There is growing interest in the use of cardiac injury biomarkers. Elevations in these biomarkers reflect myocardial injury; they do not indicate its mechanism [1, 19]. Troponin is released into the circulation in response to ischaemic and non-ischaemic cardiac injury [20]. Troponin has been reported in association with sepsis, septic shock, and systemic inflammatory response syndrome, hypotension or hypovolemia, acute and chronic heart failure and tachyarrhythmias. These clinical settings indicate that demand ischaemia, which refers to a mismatch between myocardial oxygen demand and supply in the absence of flow-limiting epicardial stenosis of coronary arteries, may induce troponin elevation in the circulation. Simultaneously, myocardial oxygen delivery may be decreased by reduced coronary perfusion because of tachycardia and decreased oxygen delivery to the heart [21].
Cardiac injury biomarkers in children
In recent years, there is growing interest in the use of troponin I in paediatrics and its value in assessing cardiac injury in children [22–24]. Reference values for troponin I (Table 1), CK-MB (Table 2) and myoglobin (Table 3) in children and newborns have been published [25–27].
In the paediatric population, troponins show a good correlation with the extent of myocardial damage following cardiac surgery and cardiotoxic medication and can be used as predictors of subsequent cardiac recovery and mortality. They may serve as a useful adjunct in the assessment of the magnitude of myocardial injury in respiratory distress syndrome and asphyxia. Elevation of troponin I may also have diagnostic value in cases when cardiac contusion is suspected. They may also benefit centres without on-site echocardiography with some evidence showing good correlation with echo-derived markers of myocardial function.
Shah et al. conducted a single-site, cross-sectional observational study of 29 children, single-ventricle patients. Troponin I was not associated with clinical heart failure [28]. Troponin I has also been studied in children with left-to-right shunt-induced myocardial injury [21, 29]. Troponin I levels in children with atrial and ventricular septal defects were significantly higher than those in healthy children and correlated with invasive ratio of pulmonary to systemic arterial pressure [29]. Sugimoto et al. suggest that volume overload can cause myocardial injury by increasing the oxygen demand of the myocardium, which also results in relative hypoperfusion of the myocardium [29, 30]. In another study of children with congenital heart defects (CHD) with pressure or volume overload, the pressure gradient at the site of coarctation site or stenotic valve was higher in those with positive troponin I and resolved 6 months after treatment [31]. The same group evaluated troponin I and natriuretic peptides in children with hypoplastic left heart syndrome (HLHS) and found that troponin I release is common before Norwood and Glenn operations; then during the treatment protocol for HLHS, troponin I release resolves and serum levels of natriuretic peptides decrease. This may reflect a reduction in volume overload of the right ventricle during the surgical treatment [10]. Levels of troponin I and natriuretic peptides showed no correlation with oxygen saturation or haemoglobin concentration [10].
Hirsch et al. found that troponin I values are usually less than 2.0 ng/mL in the absence of discernible myocardial damage in a wide variety of different paediatric conditions. This finding was consistent in infants and children with hemodynamically stable cyanotic and acyanotic congenital, and non-acute acquired heart disease. Moderate elevation of troponin I (<8.0 ng/mL) is rare in a paediatric population, except in critically ill patients [22]. The significance of moderate elevation of troponin I seen in newborns who are critically ill is uncertain. It is possible that small degrees of myocardial damage associated with these elevations do increase risk and may have long-term sequelae. Nevertheless, further prospective study is needed to clarify this issue, and to determine whether elevation of troponin I above a threshold level has significance as a prognostic factor [22]. Liesemer et al. [32] evaluated troponin I in children with chest pain, trauma, overdose/poisoning, syncope or palpitations and found that regardless of the diagnosis, elevated troponin I was predictive of longer hospitalizations, being mechanically ventilated, and death, suggesting a diagnostic and prognostic role of troponin in a variety of clinical scenarios in paediatric patients. The predictive value of the troponin I assay was strongest in the trauma and overdose or poisoning subgroups. In patients with sepsis, elevated troponin I levels were predictive of increased duration of hospitalization and mechanical ventilation. However, in paediatric patients with chest pain, in the absence of fever and/or abnormal ECG results, serum troponin assays are of little diagnostic or prognostic value [32].
Preoperative and perioperative elevations of troponin I are usually considered predictors of mortality and morbidity in infants and children [15, 33]. Immer et al. [15] calculated a positive predictive value of 100 % and a negative predictive value of 93 % of perioperative complications when troponin I value exceeds 35 ng/mL during the first 24 post-operative hours. Troponin above 100 ng/mL was associated with higher mortality [15, 34, 35]. Imura et al. [36] showed that a peak post-operative troponin I concentration is weakly, but significantly, correlated with clinical outcome (duration of inotropic support, intubation and ICU stay) in this population. In paediatric cardiac surgery patients, troponin I has also been shown to predict adverse post-operative outcomes [15, 33]. Bottio et al. [35] evaluated troponin in the post-operative period in newborns and children and concluded that troponin I was a specific and sensitive marker of myocardial injury after cardiac surgery and it might predict early-hospital outcomes but it lost the prognostic significance in the long term. Bojan et al. [37] suggest that routine monitoring of troponin I after surgery for CHD was not useful in patients less than 1 year old (except for a subgroup of procedures as arterial switch, truncus arteriosus repair, HLHS procedures or anomalous origin of the left coronary artery arising from the pulmonary artery repair). In another study, a troponin level greater than 100 ng/mL after bypass did not predict death or a severe cardiovascular event in the very young [38]. Troponin is not only a necrotic marker, but a dynamic marker of myocardial damage. Thus, the clinical relevance of increased troponin levels in patients with CHD before and after surgery should be studied further [21].
Cardiac injury biomarkers in newborns
Cardiac troponins are very sensitive markers for the detection of myocardial injury and have been studied in healthy newborns, after tocolysis, intrauterine growth restriction, respiratory distress syndrome and asphyxia. Reference values for myoglobin [18, 39], CK-MB [23], cardiac troponins T and I in healthy newborns have been published [12, 18, 23, 26, 27]. Despite that, very little is known about its role in newborns [40].
Lipshultz et al. evaluated the frequency of elevations in markers of myocardial injury in the umbilical cord and neonatal serum samples from 32 otherwise healthy newborns. The proportion of newborns with elevated troponin was higher than that in ill infants, children and adolescents and in healthy adults, suggesting that myocardial injury, although clinically occult, is common in this young age group [39]. It remains unclear whether the increased levels represent normal neonatal values associated with physiologic myocardial remodelling, occult myocardial injury, or both and whether these may be associated with morbidity [39].
Troponin concentrations peak during second to fourth post-natal days [39, 41–43]. Bader et al. measured the serum troponin I concentrations on the third day of life in normal newborns. There was a borderline significant trend for higher troponin I in preterm infants. No significant correlation was found between the mode of delivery, gestational age and birth weight and troponin I concentrations [12]. The number of newborns with troponin I >1.8 ng/mL was significantly higher after delivery by caesarean section, compared to vaginal delivery. No other significant associations were found between troponin I and perinatal or neonatal parameters [12]. Quivers et al. [24] also found a higher level of troponin I in preterm infants; the levels decreased significantly with increasing gestational age and birth weight. The CK-MB levels did not exhibit a significant difference between the preterm and term infant group when assessed for the effects of gestational age or birth weight [24]. The higher troponin I found during the first 3 months of life is interpreted by the authors as indicative of programed cell death, or apoptosis [24, 44]. Troponin I levels were elevated in critically ill patients without a comparable rise in CK-MB. Neither troponin I nor CK-MB levels were significantly different between preterm survivors and non-survivors [24]. Unlike Bader et al. and Quivers et al., Hirsch et al. did find that a significant elevation in troponin I in a paediatric intensive-care setting may be an indicator of poor outcome [22]. In a study by Lipshultz et al. [39], measures of myocardial injury were associated with longer hospitalization.
Troponins may be used as a useful adjunct in the assessment of the magnitude of myocardial injury in respiratory distress syndrome and asphyxia [41, 45, 46]. Birth asphyxia is defined as a severe disturbance of oxygen supply to the foetus, which develops during birth. The diagnosis is confirmed by a severe metabolic acidosis in the umbilical cord, a persistent low Apgar was well as functional disturbances as a result of hypoxic damage in various organs including central nervous system and heart [46]. Troponin I has been used to detect myocardial compromise in newborns with hypoxia and asphyxia [47–49]. Troponin was also useful for monitoring myocardial injury in infants of diabetic mothers; an elevated troponin I in infants of diabetic mothers with respiratory distress was a good predictor for hypertrophic cardiomyopathy and/or left ventricular dysfunction [50] and life-threatening respiratory or hemodynamic distress [51]. Troponin I was significantly higher in the asphyxiated newborns who died compared to the group of asphyxiated newborns that survived; the cut-off value was 0.135 ng/mL with a sensibility of 0.85 and a specificity of 0.74 [52]. Troponin I in the cord blood was predictive of severity of hypoxic-ischaemic encephalopathy and mortality in term infants [48]. In another group of newborns with asphyxia, troponin was elevated both in hypothermia and normothermia groups and no differences were found for troponin I concentrations between both groups [53]. In asphyxiated newborns, CK-MB was significantly increased compared with the control subjects [18, 52, 54]. However, in other studies, CK-MB levels in infants with myocardial injury were not higher than in infants without myocardial injury [55, 56]. There was no significant difference in CK-MB mass concentrations between asphyxiated infants with and without complications [55].
The use of troponin in the neonatal unit remains a research tool. More work is needed to explore their prognostic role and monitoring response to treatment following cardioprotective strategies. In preterm infants, the effect of inotropes on myocardial function needs further study and troponin may form an integral part of this research [41].
Cardiac injury biomarkers in the cord blood
There is evidence that cord blood can be used for early detection of neonatal cardiovascular disease [57, 58]. It was previously reported that troponin I does not cross the placenta; thus, increases in cord blood biomarkers can be attributed to foetal production [47, 59]. Was also reported that umbilical cord blood troponin I, CK-MB levels and myoglobin levels correlated with one another [39].
Troponin levels did not correlate with gestational age, birth weight, Apgar scores or gender [26, 39, 42]. Kocylowski et al. [18] found that in the umbilical cord blood (umbilical vein), myoglobin, troponin T, CK and CK-MB were statistically significantly higher in spontaneous vs caesarean section, reflecting some kind of heart strain in normal birth. There was an increase with gestational age for CK and CK-MB [18]. CK and CK-MB were just significantly different between males and females. There was only a weak correlation between birth weight and CK, CK-MB, myoglobin and troponin T [18]. There was a statistically significantly higher CK, troponin T and myoglobin in the artery versus vein [18]. Baum et al. investigated the distribution of troponin I in cord blood of healthy newborns. Compared to the adult values, the newborn upper limit was doubled for troponin I. No statistically significant differences were found between males and females for troponin I. A significant difference was found for troponin I between natural childbirth and caesarean section [27, 39, 41]. Trevisanuto et al. measured and compared cardiac troponin I, cardiac troponin T and CK-MB concentrations in the umbilical cord blood of healthy term infants and investigated the relationship between maternal and neonatal troponin values at birth, concluding that these cardiac regulatory proteins are of neonatal origin and are not influenced by maternal levels. In newborns, there was no significant correlation between CK-MB levels and troponin I concentrations. Furthermore, levels of troponin I and T were not significantly correlated with gestational age, birth weight and Apgar score at 5 min [26].
In healthy newborns, low levels of troponin I were reported [22, 26] by Trevisanuto et al. and Hirsch et al., while Soldin et al. [23] reported 33 % of neonatal patients with troponin I levels >0.1 ng/mL. These differing results could be due to differences in post-natal age and clinical characteristics of the study population; however, the most important reason is probably the different immunoassay methods used for troponin I determination, making it practically impossible to compare the data from these studies [26].
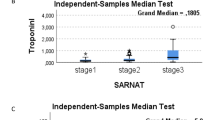
Turker et al. tested the hypothesis that cardiac troponin I is also an early predictor of severity of cerebral damage and mortality in intrauterine hypoxia. Venous and arterial cord blood samples were collected at delivery from 54 consecutive newborns with hypoxic-ischaemic encephalopathy and from 50 consecutive healthy controls. Arterial blood gas analysis was performed, and levels of troponin I, CK and CK-MB in venous cord blood were measured. The same serum parameters were also measured on the 3rd and 7th day of life. Infants with hypoxia had a significantly higher cord blood troponin I levels than controls. Cord blood and 3rd and 7th day serum troponin I values showed a significant increase with severity of hypoxic-ischaemic encephalopathy. In non-survivors cord blood, troponin I levels were significantly higher than the survivors. Receiver-operator curve analysis revealed cord troponin I as the most sensitive factor for predicting early death. Cord blood troponin I of 4.6 ng/mL was identified as the optimal cut-off level for predicting serious risk of early mortality. The results suggest that significant elevation of cord troponin is an excellent early predictor of severity of hypoxic-ischaemic encephalopathy and mortality in term infants [48]. Umbilical cord troponin I was not different between hospitalized newborns versus non-hospitalized newborns in a study by Usluer et al. [40].
Kocylowski et al., evaluated cardiac injury biomarkers in foetuses, ten of which had cardiac defects, plotted against normal ranges, and troponin T was only increased in 2/10. In troponin T, CK, CK-MB and myoglobin, there were no significant differences from normal. These changes were independent from umbilical cord blood pH at birth [18].
Troponin I concentration in the cord blood of newborns with neonatal lupus was not different from unaffected patients. Also, no significant associations were identified between troponin I and extranodal disease, post-natal outcomes or severity score [58]. The authors speculate that necrosis of tissue that precedes cardiomyocyte calcification occurs only during the target gestational age of disease onset, and troponin I levels may normalize by the time of childbirth. Alternatively, the troponin I assay used may not have been sufficiently sensitive to detect smaller differences due to heart failure or myocarditis that novel high-sensitivity tests would potentially discern [58, 60]. This might also be explained by the antibodies causing cardiomyocyte apoptosis, a controlled way of cell death, that may not lead to a substantial release of cardiomyocyte proteins [61].
In multiple gestations, troponins T and I and CK-MB were not increased in twins at birth and were not different between the first- and the second-born twin [62]. In intrauterine growth restriction that implies foetal hypoxia, resulting in flow redistribution and sparing of vital organs, no differences in troponin I levels were observed between the appropriate-for-gestational-age and intrauterine growth restriction groups [63]. Increase in troponin T but not in CK and CK-MB was found in the umbilical cord blood in intrauterine growth restriction [18].
Further research is necessary before cardiac injury biomarkers can be used in clinical practice in this age group [64, 65].
Cardiac biomarkers and echocardiographic parameters in newborns
Wei et al. evaluated the left ventricular function of newborns with asphyxia. Left ventricular ejection fraction and fractional shortening of the severe asphyxia group at 24 h were significantly lower than those at later time points and significantly lower than those of the mild asphyxia and control groups. Stroke volume was not significantly different among the three groups. TDI S′ was a more sensitive indicator of left ventricular systolic function than left ventricular ejection fraction, fractional shortening or stroke volume. S′ wave of asphyxia groups was significantly lower than that of control group. Troponin I values of the severe asphyxia group were remarkably higher than those of mild asphyxia and control groups. S′ showed a better correlation (negatively) with troponin I, than with fractional shortening, indicating that S′ is a better parameter than fractional shortening to reflect ischaemic change of left ventricle after asphyxia [49]. Matter et al. [66] correlated S′ mitral and tricuspid velocities in full-term newborns and controls. Mitral and tricuspid S′ were lower in asphyxiated newborns. Troponin T was higher in asphyxiated newborns and correlated positively with left ventricular Tei index and right ventricular Tei index and negatively with the mitral and tricuspid S′ velocities. Fractional shortening did not correlate with troponin T [66]. Troponin T was predictive of death, while the echocardiographic parameters evaluated were not [66]. Simovic et al. [52] found a significant correlation between troponin I concentration and ejection fraction and fractional shortening in patients with perinatal asphyxia, while no correlations were found between troponin I and echocardiographic measurements in perinatal asphyxia in other studies [53, 66]. In the asphyxiated population, troponin T levels were markedly raised and correlated with a decline in cardiac output [67]. Troponin T of asphyxiated infants with low ejection fraction <60 % was significantly higher at 12 and 24 h than those with normal ejection fraction [55].
Left ventricular contractility as assessed by ejection fraction and percentage shortening was higher in newborns of diabetic mother compared with the controls. This finding could reflect myocardial compromise or an increase in the ventricular workload [50, 68].
In preterm infants, plasma concentrations of troponin T measured in infants <1500 g at 12 h of age were correlated with simultaneous echocardiographic measures of myocardial function and output. There was a significant inverse correlation between troponin T and echocardiographic markers of myocardial function and stroke volume. Measurement of levels in the first hours of life may provide useful information regarding myocardial function and volume loading [69].
Clark et al. found a negative correlation between troponin T and fractional shortening measured on day one in newborns with respiratory distress. There was no statistically significant correlation between left ventricle output and troponin T [45]. Troponin T levels in newborns with CHD did not correlate with left ventricular ejection fraction [70]. Only hemodynamic significance evaluated by echocardiography influenced the troponin levels [70]. In a study by Bottio et al. [35] of newborns and children after cardiac surgery, when troponin I exceeded 35 ng/mL, at echocardiogram, a severely depressed left ventricular ejection fraction was evident. Patients with troponin I >35 ng/mL and cardiac dysfunction at discharge showed complete recovery at 12-month follow-up. Authors speculate that cardiac remodelling might also appear after devastating myocardial damage [35, 71].
Conclusions
In the paediatric population, cardiac biomarkers show a good correlation with the extent of myocardial damage following cardiac surgery and cardiotoxic medication and can be used as predictors of subsequent cardiac recovery and mortality. Elevation of cardiac injury biomarkers may also have diagnostic value in cases when cardiac contusion or pericarditis is suspected. Results suggest that significant elevation of cord troponin is an excellent early predictor of severity of hypoxic-ischaemic encephalopathy and mortality in term infants. However, different immunoassay methods used for cardiac biomarkers determination make it difficult to compare the data from different studies. Additionally, cardiac biomarkers are not stand-alone tests and should be used as an integrated approach and in the clinical context. Cardiac biomarkers may also benefit centres without on-site echocardiography with evidence showing good correlation with echo-derived markers of myocardial function. Further studies are needed to better clarify the role of cardiac biomarkers in paediatric age and their correlation with echocardiographic parameters.
References
Thygesen K, Alpert JS, White HD, Joint ESCAAHAWHFTFftRoMI (2007) Universal definition of myocardial infarction. J Am Coll Cardiol 50(22):2173–2195. doi:10.1016/j.jacc.2007.09.011
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, Writing Group on the Joint ESCAAHAWHFTFftUDoMI, Thygesen K, Alpert JS, White HD, Jaffe AS, Katus HA, Apple FS, Lindahl B, Morrow DA, Chaitman BA, Clemmensen PM, Johanson P, Hod H, Underwood R, Bax JJ, Bonow RO, Pinto F, Gibbons RJ, Fox KA, Atar D, Newby LK, Galvani M, Hamm CW, Uretsky BF, Steg PG, Wijns W, Bassand JP, Menasche P, Ravkilde J, Ohman EM, Antman EM, Wallentin LC, Armstrong PW, Simoons ML, Januzzi JL, Nieminen MS, Gheorghiade M, Filippatos G, Luepker RV, Fortmann SP, Rosamond WD, Levy D, Wood D, Smith SC, Hu D, Lopez-Sendon JL, Robertson RM, Weaver D, Tendera M, Bove AA, Parkhomenko AN, Vasilieva EJ, Mendis S, Guidelines ESCCfP (2012) Third universal definition of myocardial infarction. Eur Heart J 33(20):2551–2567. doi:10.1093/eurheartj/ehs184
Coudrey L (1998) The troponins. Arch Intern Med 158(11):1173–1180
Ebashi S, Ebashi F (1964) A new protein component participating in the superprecipitation of myosin B. J Biochem 55:604–613
Ebashi S, Ebashi F (1964) A new protein factor promoting contraction of actomyosin. Nature 203:645–646
Sasse S, Brand NJ, Kyprianou P, Dhoot GK, Wade R, Arai M, Periasamy M, Yacoub MH, Barton PJ (1993) Troponin I gene expression during human cardiac development and in end-stage heart failure. Circ Res 72(5):932–938
Sarko J, Pollack CV Jr (2002) Cardiac troponins. J Emerg Med 23(1):57–65
Sobki SH, Saadeddin SM, Habbab MA (2000) Cardiac markers used in the detection of myocardial injury. http://www.ncbi.nlm.nih.gov/pubmed/11376361. Accessed 21 Sept
Hickman PE, Potter JM, Aroney C, Koerbin G, Southcott E, Wu AH, Roberts MS (2010) Cardiac troponin may be released by ischemia alone, without necrosis. Clin Chim Acta 411(5–6):318–323. doi:10.1016/j.cca.2009.12.009
Eerola A, Poutanen T, Savukoski T, Pettersson K, Sairanen H, Jokinen E, Pihkala J (2014) Cardiac troponin I, cardiac troponin-specific autoantibodies and natriuretic peptides in children with hypoplastic left heart syndrome. Interact CardioVasc Thorac Surg 18(1):80–85. doi:10.1093/icvts/ivt430
Kociol RD, Pang PS, Gheorghiade M, Fonarow GC, O’Connor CM, Felker GM (2010) Troponin elevation in heart failure prevalence, mechanisms, and clinical implications. J Am Coll Cardiol 56(14):1071–1078. doi:10.1016/j.jacc.2010.06.016
Bader D, Kugelman A, Lanir A, Tamir A, Mula E, Riskin A (2006) Cardiac troponin I serum concentrations in newborns: a study and review of the literature. Clin Chim Acta 371(1–2):61–65. doi:10.1016/j.cca.2006.02.018
Wu AH, Apple FS, Gibler WB, Jesse RL, Warshaw MM, Valdes R Jr (1999) National Academy of Clinical Biochemistry Standards of Laboratory Practice: recommendations for the use of cardiac markers in coronary artery diseases. Clin Chem 45(7):1104–1121
Antman EM, Tanasijevic MJ, Thompson B, Schactman M, McCabe CH, Cannon CP, Fischer GA, Fung AY, Thompson C, Wybenga D, Braunwald E (1996) Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 335(18):1342–1349. doi:10.1056/NEJM199610313351802
Immer FF, Stocker F, Seiler AM, Pfammatter JP, Bachmann D, Printzen G, Carrel T (1999) Troponin-I for prediction of early postoperative course after pediatric cardiac surgery. J Am Coll Cardiol 33(6):1719–1723
Bodor GS, Porterfield D, Voss EM, Smith S, Apple FS (1995) Cardiac troponin-I is not expressed in fetal and healthy or diseased adult human skeletal muscle tissue. Clin Chem 41(12 Pt 1):1710–1715
Mair J, Morandell D, Genser N, Lechleitner P, Dienstl F, Puschendorf B (1995) Equivalent early sensitivities of myoglobin, creatine kinase MB mass, creatine kinase isoform ratios, and cardiac troponins I and T for acute myocardial infarction. Clin Chem 41(9):1266–1272
Kocylowski RD, Dubiel M, Gudmundsson S, Sieg I, Fritzer E, Alkasi O, Breborowicz GH, von Kaisenberg CS (2009) Biochemical tissue-specific injury markers of the heart and brain in postpartum cord blood. Am J Obstet Gynecol 200(3):273.e1–273.e25. doi:10.1016/j.ajog.2008.10.009
Jaffe AS, Ravkilde J, Roberts R, Naslund U, Apple FS, Galvani M, Katus H (2000) It’s time for a change to a troponin standard. Circulation 102(11):1216–1220
Suleiman MS, Lucchetti V, Caputo M, Angelini GD (1999) Short periods of regional ischaemia and reperfusion provoke release of troponin I from the human hearts. Clin Chim Acta 284(1):25–30
Kogaki S (2011) Highly sensitive cardiac troponin-I in congenital heart disease. Circ J 75(9):2056–2057
Hirsch R, Landt Y, Porter S, Canter CE, Jaffe AS, Ladenson JH, Grant JW, Landt M (1997) Cardiac troponin I in pediatrics: normal values and potential use in the assessment of cardiac injury. J Pediatr 130(6):872–877
Soldin SJ, Murthy JN, Agarwalla PK, Ojeifo O, Chea J (1999) Pediatric reference ranges for creatine kinase, CKMB, Troponin I, iron, and cortisol. Clin Biochem 32(1):77–80
Quivers ES, Murthy JN, Soldin SJ (1999) The effect of gestational age, birth weight, and disease on troponin I and creatine kinase MB in the first year of life. Clin Biochem 32(6):419–421
Bailey D, Colantonio D, Kyriakopoulou L, Cohen AH, Chan MK, Armbruster D, Adeli K (2013) Marked biological variance in endocrine and biochemical markers in childhood: establishment of pediatric reference intervals using healthy community children from the CALIPER cohort. Clin Chem 59(9):1393–1405. doi:10.1373/clinchem.2013.204222
Trevisanuto D, Pitton M, Altinier S, Zaninotto M, Plebani M, Zanardo V (2003) Cardiac troponin I, cardiac troponin T and creatine kinase MB concentrations in umbilical cord blood of healthy term neonates. Acta Paediatr 92(12):1463–1467
Baum H, Hinze A, Bartels P, Neumeier D (2004) Reference values for cardiac troponins T and I in healthy neonates. Clin Biochem 37(12):1079–1082. doi:10.1016/j.clinbiochem.2004.08.003
Shah A, Feraco AM, Harmon C, Tacy T, Fineman JR, Bernstein HS (2009) Usefulness of various plasma biomarkers for diagnosis of heart failure in children with single ventricle physiology. Am J Cardiol 104(9):1280–1284. doi:10.1016/j.amjcard.2009.06.046
Sugimoto M, Ota K, Kajihama A, Nakau K, Manabe H, Kajino H (2011) Volume overload and pressure overload due to left-to-right shunt-induced myocardial injury. Evaluation using a highly sensitive cardiac troponin-I assay in children with congenital heart disease. Circ J 75(9):2213–2219
Korff S, Katus HA, Giannitsis E (2006) Differential diagnosis of elevated troponins. Heart 92(7):987–993. doi:10.1136/hrt.2005.071282
Eerola A, Jokinen EO, Savukoski TI, Pettersson KS, Poutanen T, Pihkala JI (2013) Cardiac troponin I in congenital heart defects with pressure or volume overload. Scand Cardiovasc J 47(3):154–159. doi:10.3109/14017431.2012.751506
Liesemer K, Casper TC, Korgenski K, Menon SC (2012) Use and misuse of serum troponin assays in pediatric practice. Am J Cardiol 110(2):284–289. doi:10.1016/j.amjcard.2012.03.020
Montgomery VL, Sullivan JE, Buchino JJ (2000) Prognostic value of pre- and postoperative cardiac troponin I measurement in children having cardiac surgery. Pediatr Dev Pathol 3(1):53–60
Taggart DP, Hadjinikolas L, Hooper J, Albert J, Kemp M, Hue D, Yacoub M, Lincoln JC (1997) Effects of age and ischemic times on biochemical evidence of myocardial injury after pediatric cardiac operations. J Thorac Cardiovasc Surg 113(4):728–735
Bottio T, Vida V, Padalino M, Gerosa G, Stellin G (2006) Early and long-term prognostic value of Troponin-I after cardiac surgery in newborns and children. Eur J Cardiothorac Surg 30(2):250–255. doi:10.1016/j.ejcts.2006.05.001
Imura H, Modi P, Pawade A, Parry AJ, Suleiman MS, Angelini GD, Caputo M (2002) Cardiac troponin I in neonates undergoing the arterial switch operation. Ann Thorac Surg 74(6):1998–2002
Bojan M, Peperstraete H, Lilot M, Vicca S, Pouard P, Vouhe P (2012) Early elevation of cardiac troponin I is predictive of short-term outcome in neonates and infants with coronary anomalies or reduced ventricular mass undergoing cardiac surgery. J Thorac Cardiovasc Surg 144(6):1436–1444. doi:10.1016/j.jtcvs.2012.05.034
Gupta-Malhotra M, Kern JH, Flynn PA, Schiller MS, Quaegebeur JM, Friedman DM (2013) Cardiac troponin I after cardiopulmonary bypass in infants in comparison with older children. Cardiol Young 23(3):431–435. doi:10.1017/S1047951112001163
Lipshultz SE, Simbre VC 2nd, Hart S, Rifai N, Lipsitz SR, Reubens L, Sinkin RA (2008) Frequency of elevations in markers of cardiomyocyte damage in otherwise healthy newborns. Am J Cardiol 102(6):761–766. doi:10.1016/j.amjcard.2008.04.057
Usluer H, Turker G, Gokalp AS (2012) Value of homocysteine levels, troponin I, and score for neonatal acute physiology and perinatal extension II as early predictors of morbidity. Pediatr Int 54(1):104–110
El-Khuffash AF, Molloy EJ (2008) Serum troponin in neonatal intensive care. Neonatology 94(1):1–7. doi:10.1159/000112540
Araujo K, da Silva J, Sanudo A, Kopelman B (2004) Plasma concentrations of cardiac troponin I in newborn infants. Clin Chem 50(9):1717–1718. doi:10.1373/clinchem.2004.033472
Turker G, Babaoglu K, Duman C, Gokalp A, Zengin E, Arisoy AE (2004) The effect of blood gas and Apgar score on cord blood cardiac troponin I. J Matern Fetal Neonatal Med 16(5):315–319. doi:10.1080/14767050400017991
Kajstura J, Mansukhani M, Cheng W, Reiss K, Krajewski S, Reed JC, Quaini F, Sonnenblick EH, Anversa P (1995) Programmed cell death and expression of the protooncogene bcl-2 in myocytes during postnatal maturation of the heart. Exp Cell Res 219(1):110–121. doi:10.1006/excr.1995.1211
Clark SJ, Newland P, Yoxall CW, Subhedar NV (2006) Sequential cardiac troponin T following delivery and its relationship with myocardial performance in neonates with respiratory distress syndrome. Eur J Pediatr 165(2):87–93. doi:10.1007/s00431-005-0001-3
Correale M, Nunno L, Ieva R, Rinaldi M, Maffei G, Magaldi R, Di Biase M (2009) Troponin in newborns and pediatric patients. Cardiovasc Hematol Agents Med Chem 7(4):270–278
Trevisanuto D, Doglioni N, Altinier S, Zaninotto M, Plebani M, Zanardo V (2009) Cardiac troponin I at birth is of fetal-neonatal origin. Arch Dis Child Fetal Neonatal Ed 94(6):F464–F466. doi:10.1136/adc.2008.145987
Turker G, Babaoglu K, Gokalp AS, Sarper N, Zengin E, Arisoy AE (2004) Cord blood cardiac troponin I as an early predictor of short-term outcome in perinatal hypoxia. Biol Neonate 86(2):131–137. doi:10.1159/000079068
Wei Y, Xu J, Xu T, Fan J, Tao S (2009) Left ventricular systolic function of newborns with asphyxia evaluated by tissue Doppler imaging. Pediatr Cardiol 30(6):741–746. doi:10.1007/s00246-009-9421-6
Korraa A, Ezzat MH, Bastawy M, Aly H, El-Mazary AA, Abd El-Aziz L (2012) Cardiac troponin I levels and its relation to echocardiographic findings in infants of diabetic mothers. Ital J Pediatr 38:39. doi:10.1186/1824-7288-38-39
Oran B, Cam L, Baspinar O, Baysal T, Reisli I, Peru H, Karaaslan S, Koc H, Gurbilek M (2003) Cardiac troponin-I in the serum of infants of diabetic mothers. Cardiol Young 13(3):248–252
Simovic AM, Prijic SM, Knezevic JB, Igrutinovic ZR, Vujic AJ, Kosutic J (2014) Predictive value of biochemical, echocardiographic and electrocardiographic markers in non-surviving and surviving asphyxiated full-term newborns. Turk J Pediatr 56(3):243–249
Vijlbrief DC, Benders MJ, Kemperman H, van Bel F, de Vries WB (2012) Cardiac biomarkers as indicators of hemodynamic adaptation during postasphyxial hypothermia treatment. Neonatology 102(4):243–248. doi:10.1159/000339117
Szymankiewicz M, Matuszczak-Wleklak M, Vidyasagar D, Gadzinowski J (2006) Retrospective diagnosis of hypoxic myocardial injury in premature newborns. J Perinat Med 34(3):220–225. doi:10.1515/JPM.2006.040
Boo NY, Hafidz H, Nawawi HM, Cheah FC, Fadzil YJ, Abdul-Aziz BB, Ismail Z (2005) Comparison of serum cardiac troponin T and creatine kinase MB isoenzyme mass concentrations in asphyxiated term infants during the first 48 h of life. J Paediatr Child Health 41(7):331–337. doi:10.1111/j.1440-1754.2005.00626.x
Sadoh WE, Eregie CO, Nwaneri DU, Sadoh AE (2014) The diagnostic value of both troponin T and creatinine kinase isoenzyme (CK-MB) in detecting combined renal and myocardial injuries in asphyxiated infants. PLoS One 9(3):e91338. doi:10.1371/journal.pone.0091338
Llurba E, Sanchez O, Ferrer Q, Nicolaides KH, Ruiz A, Dominguez C, Sanchez-de-Toledo J, Garcia-Garcia B, Soro G, Arevalo S, Goya M, Suy A, Perez-Hoyos S, Alijotas-Reig J, Carreras E, Cabero L (2014) Maternal and foetal angiogenic imbalance in congenital heart defects. Eur Heart J 35(11):701–707. doi:10.1093/eurheartj/eht389
Saxena A, Izmirly PM, Han SW, Briassouli P, Rivera TL, Zhong H, Friedman DM, Clancy RM, Buyon JP (2015) Serum biomarkers of inflammation, fibrosis, and cardiac function in facilitating diagnosis, prognosis, and treatment of anti-SSA/Ro-associated cardiac neonatal lupus. J Am Coll Cardiol 66(8):930–939. doi:10.1016/j.jacc.2015.06.1088
Fleming SM, O’Gorman T, Finn J, Grimes H, Daly K, Morrison JJ (2000) Cardiac troponin I in pre-eclampsia and gestational hypertension. BJOG 107(11):1417–1420
Mahajan VS, Jarolim P (2011) How to interpret elevated cardiac troponin levels. Circulation 124(21):2350–2354. doi:10.1161/CIRCULATIONAHA.111.023697
Sliwa K, Hilfiker-Kleiner D (2015) Cord blood samples: a less explored tool in early diagnosis of neonatal cardiovascular disease. J Am Coll Cardiol 66(8):940–942. doi:10.1016/j.jacc.2015.07.001
Trevisanuto D, Pitton M, Doglioni N, Altinier S, Zaninotto M, Plebani M, Zanardo V (2004) Cord blood cardiac troponin T and troponin I levels in multiple-gestation neonates. Biol Neonate 85(4):269–272. doi:10.1159/000076365
Iacovidou N, Boutsikou M, Gourgiotis D, Briana DD, Baka S, Vraila VM, Kontara L, Hassiakos D, Malamitsi-Puchner A (2007) Perinatal changes of cardiac troponin-I in normal and intrauterine growth-restricted pregnancies. Mediat Inflamm 2007:53921. doi:10.1155/2007/53921
Vijlbrief DC, Benders MJ, Kemperman H, van Bel F, de Vries WB (2012) Use of cardiac biomarkers in neonatology. Pediatr Res 72(4):337–343. doi:10.1038/pr.2012.88
Gaze DC, Collinson PO (2005) Cardiac troponin I should be interpreted with caution in paediatric neonatal patients. Concerning Turker et al.: ‘Cord blood cardiac troponin I as an early predictor of short-term outcome in perinatal hypoxia’. Biol Neonate 87(1):19. doi:10.1159/000080890
Matter M, Abdel-Hady H, Attia G, Hafez M, Seliem W, Al-Arman M (2010) Myocardial performance in asphyxiated full-term infants assessed by Doppler tissue imaging. Pediatr Cardiol 31(5):634–642. doi:10.1007/s00246-010-9661-5
Sehgal A, Wong F, Mehta S (2012) Reduced cardiac output and its correlation with coronary blood flow and troponin in asphyxiated infants treated with therapeutic hypothermia. Eur J Pediatr 171(10):1511–1517. doi:10.1007/s00431-012-1764-y
Kozak-Barany A, Jokinen E, Kero P, Tuominen J, Ronnemaa T, Valimaki I (2004) Impaired left ventricular diastolic function in newborn infants of mothers with pregestational or gestational diabetes with good glycemic control. Early Hum Dev 77(1–2):13–22. doi:10.1016/j.earlhumdev.2003.11.006
El-Khuffash A, Davis PG, Walsh K, Molloy EJ (2008) Cardiac troponin T and N-terminal-pro-B type natriuretic peptide reflect myocardial function in preterm infants. J Perinatol 28(7):482–486. doi:10.1038/jp.2008.21
Tarkowska A, Furmaga-Jablonska W (2012) The evaluation of diagnostic role of cardiac troponin T (cTnT) in newborns with heart defects. Sci World J 2012:682538. doi:10.1100/2012/682538
Korbling M, Estrov Z (2003) Adult stem cells for tissue repair—a new therapeutic concept? N Engl J Med 349(6):570–582. doi:10.1056/NEJMra022361
Engin Y, Ustun Y, Kurtay G (2002) Cardiac troponin I levels in umbilical cord blood. Int J Gynaecol Obstet 77(3):239–241
McAuliffe F, Mears K, Fleming S, Grimes H, Morrison JJ (2004) Fetal cardiac troponin I in relation to intrapartum events and umbilical artery pH. Am J Perinatol 21(3):147–152. doi:10.1055/s-2004-823775
Acknowledgments
We would like to Servier Medical Art-Image bank, used to create the Fig. 1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Neves, A.L., Henriques-Coelho, T., Leite-Moreira, A. et al. Cardiac injury biomarkers in paediatric age: Are we there yet?. Heart Fail Rev 21, 771–781 (2016). https://doi.org/10.1007/s10741-016-9567-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-016-9567-2