
Abstract
In this paper, we examine efficiency and total factor productivity for hospitals operating in China between the years of 2009–2016. Given reforms in China focusing on the hospital sector, it has been demonstrated that efficiency and productivity are important in meeting the overall objective of meeting more accessibility to hospital care for the population. Measuring an aggregate directional distance function is in itself a non-parametric approach, we report on the decomposition of hospital performance and found that between 2009 and 2010, technical inefficiency (using resources inefficiently) dominated overall inefficiency but beyond 2011–2016, mix inefficiency (misallocation of resources) was higher. Furthermore, an additive total factor productivity (TFP) indicator is proposed to capture contributions of individual provincial (or group) hospital performance to the total productivity gain. We also report that mix inefficiency had growth throughout this time period indicating a catching up in the correct mix of inputs. This finding is worth following as hospital reform in China also focuses on utilizing the right labor and capital mix in producing efficient care.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
China is the most populated country in the world with a history of a centralized government overseeing policies that cover a vast array of industries and services. One such service is the hospital system, in which the financing and production of hospital care with the setting of over policy under the auspices of the central government, with local governments responsible for the actual provision of hospital services. Public hospitals provide over 90% of all hospital services in China. Even though the system is dominated by public ownership, under reforms, the system has become more decentralized and privately run [1]. Blumenthal and Hsiao [2] noted that as the economy of China expanded, the health care system adopted some of the privatization strategies of the U.S., known widely for cost inflation and high health care costs. These authors argued that the efficiency of China’s health care system has declined attributed to barriers to access and hence the productivity of health care/hospital services [2]. The recommendation of these authors was that assessments of the inefficiencies of the health care system need to be addressed.
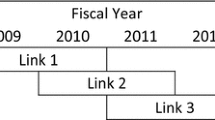
The overall objective of hospital reform from the central government’s perspective was access for the entire population to necessary hospital care [3]. Previously, Chinese hospitals operated from a centralized and bureaucratic system, but reforms were enacted to move away from this model to one that is operated from the regional/provincial level [4]. However, changes in financing to a more private payment scheme via insurance was expanded to substitute for direct government financing, but the implication was clear that increased efficiency was crucial to meet the increasing hospitalizations to meet access goals [3]. Moving away from supply side financing, it was the aim of reforms to increase the number of individuals who had health insurance that would aid in provider financing [4]. It was also suggested by Barber et al. [3] that the county level of government would increase its authority over hospital operations, indicating county-wide efficiency and productivity would be crucial information to where policy makers should focus their attention. Separating regulations from operations would be one such option, however, the central-planning structure included the decision-making process for human resource management [4]. It was hoped that public hospital reforms in the next five years will include more public hospital autonomy over resource use and increased efficiency [4]. The timeline for Chinese hospital reforms are given in Table 1.
Research in Chinese hospital reform has been performed to assess how changes have affected the system across the country. Zhang et al. [5] examined an experiment by the Chinese government to infuse resources into rural hospitals coupled with increases in fees paid by patients (rather than charging for pharmaceuticals which was one method of financing hospital care). Comparing Hubei Province with other rural areas, these authors found that overall hospital expenditures increased although pharmaceutical costs decrease. Therefore, combined with the findings by Barber et al., [3] public hospitals required to follow more profit maximization objectives to ensure adequate funding for staff and other hospital improvements.
Liu et al. [6] found existing inefficiency and inequity in resource use and that these issues were addressed via hospital price regulation. Even though prices for health services are set under guidelines, the country needs to better oversee the fee-for-service system (which accounts for 11% higher costs according to Gerdtham et al. [7] which includes a better understanding of the sources of inefficiency.
Hu et al. [1] contended that resources were not evenly distributed among the three regions of China – Eastern, Inland, and Western, and changes were necessary to better equate hospital care among these regions. However, noting efficiency differences were also required to better allocate resources for care and not to perpetuate inefficiencies. Inefficiency worries arose because of the movement toward a private health insurance type system [1]. Audibert et al. [8] echoed this concern about a misallocation of resources particularly as this inequitable portioning of resources affected township hospitals in rural China.
Because the current hospital system in China, even after reforms, still include centralized decision-making over regulations and operations, there still may exist prevalent inefficiencies that may be either county-wide, province-wide, or region- wise.
The General Office of the State Council [9] has issued policy reforms to better allocate resources to best meet the needs of the population. This policy fits in with previous findings in the literature that suggest China needs to address wasteful health care delivery [10], restructure the delivery of care [11] and further study in the sources of inefficiency would add in determining proper resource allocation [12]. Hence, the approach we present here adds to the policy decision making that is consistent with the central government’s objective of improving health care delivery and better efficiency among hospitals in providing necessary care limiting excessive waste.
In the next section of the paper literature review for hospital efficiency is summarized. Then we describe the methodological approach taken here followed by a description of the data. Results follow and we conclude with a summary and policy recommendation.
2 Literature review
In response to the growing concern of Chinese hospital inefficiency, which feeds into the inefficiency of the health care system as a whole, there has been a proliferation of analysis addressing sources and changes in inefficiency in the literature.
Using data envelopment analysis (DEA) and Malmquist approaches, several authors have reported their findings and policy suggestions. Ng [13] assesses China’s productive efficiency using the Malmquist approach, and found that the health care sector suffered from a productivity rather than an efficiency decline over 2002–2005 particularly for the coastal provinces. In his summary of the findings, he argued that economic development may induce better ways of using resources and as a result the changes in economic efficiency among coastal provinces were more diverse.
Ng [13] using DEA and the Malmquist index determined efficiency and technological change between 2004 and 2008. The findings reported that technological gains were offset by a regression of economic change. From these results, Ng [13] argued that hospital efficiency changes and economic development did not move in the same direction.
Hu et al. [1] performed DEA to assess the technical efficiency of hospitals operating in China. Using a Tobit secondary analysis, these authors found that technical efficiency varied greatly there was no statistically significant different between coastal and non-coastal region hospitals ceteris paribus, but that the New Rural Cooperative Medical System (NRCMS) which better allocated resources to rural area hospitals was effective in promoting accessibility. This is a relevant finding since access to services, as Blumenthal and Hsiao [2] argued would increase the productive use of resources.
Hu et al. [14] analyzed hospital efficiency at the provincial level since most of these hospitals are non-profit or public and are not susceptible to market forces such as cost minimization or profit maximization. Province level analysis was performed because the provincial governments are responsible for the provision of resources and hence provide an illustration for implications for the health authority within the province. Using time and regional differences, these authors found that accessibility and inequality of medical resources are widening and hence there was a geographical distribution of hospital efficiency scores using DEA. Further, non-coastal areas (Western and Inland Regions) were supported less resulting in higher inefficiency scores than the coastal areas which were afforded adequate resources and higher demand and access which is tied closely with efficiency. As an aside, the Western Region did catch up with the efficiency of the Eastern Region beginning in 2006 through 2008 but did not exceed the Eastern Region overall technical efficiency.
Wang et al. [15] assessed efficiency and productivity changes in county public hospitals after public hospital reform. These authors, using bootstrapping DEA and Malmquist Index approaches,Footnote 1 reported that overall productivity increased by 8.12% increase in Central China, 12.11% increase in Eastern China, and 11.58% increase in Western China. Along with the lower productivity growth in Central China, these authors also found lower efficiency scores and advised policy makers to focus on this area’s hospital for appropriate measures to improve efficiency. Even though there have been productivity increases, it has been reported in the literature that inefficiency still prevails in urban regions due to the wealthier population who can afford and have a reliance on hospital care [10] whereas the improvement of efficiency in rural areas under reform is attributed to greater access to services [14]. These findings corroborate Wang et al. [15] who suggest that even though there was productivity growth, there existed a higher degree of inefficiency over time. Li, Dong, and Liu [12] found that overall efficiency and productivity can only be improved with further positive technological change, technical change, and allocative efficiency.
In other studies, authors focused on specific regions and assessed efficiency in rural areas [8], Beijing [12] and Henan Province [14] Shenzhen city [17] and Northeast Asia [18, 19] reporting that inefficiencies exist attributed to quality changes and other economic changes. All these studies used DEA and/or the Malmquist Measures.
More recently, Boussemart et al. [20] used the Luenberger Productivity Indicator to assess Chinese hospitals. These authors found that the growth rate varied with time and geographical regions. Summarizing, productive growth was attributed to technological progress and efficiency changes were more varied corroborating the results of Ng [13]. Again, as other authors suggested in their work, rapid growth and various reforms were responsible for the varying levels of efficiency across regions.
The earlier research on Chinese hospital efficiency has focused on traditional DEA and Malmquist methods but advances in assessing total factor productivity have not been applied in this economic sector. However, there are several limitations of previous research on the total factor productivity (TFP) measures. First, in most of the literature, the input and/or output level of evaluated DMUs is employed as the objective direction in directional distance function. As each DMUs improve output level and/or reduce input level in terms of itself is not a common observation, and hence, the (in)efficiency scores obtained by objective function cannot be compared among DMUs. Policy and decision makers may not acquire enough, or clear economic interpretation based on such a setting.
Second, the TFP indices or indictors computed in the literature are often constructed by combinations of directional distance functions. As directions are different among DMUs, TFP indices or indictors are abstractly modelized to analyze economic performance. For a specific DMU, the evolution of TFP growth may make sense. However, to compare the productivity gain or loss from one DMU to another, or to analyze a group of DMUs, such results may not provide believable and effective empirical support.
Moreover, computing the TFP growth for a group of DMUs, the existing approach is usually to take the arithmetic average of group result. This approach assumes that there are only two DMUs analyzed, one that may have a small increase in its TFP growth of, for example, 1%, another DMU has a larger increase in TFP, of says 9%. Thus, the mean value is 5%. This approach, we argue, that the group result of TFP evolution obtained by an averaging method may be nonsensical.
In order to solve the above limitations, the main contribution of this paper is to propose an additive TFP indicator that allows to allocate productivity gain or loss among DMUs. Based on an aggregate directional distance function, the proposed specification allows us to compare (in)efficiency scores and TFP indicator among DMUs as a group. Therefore, policy and decision makers would obviously address the economic performance to a specific group and easily identify constraint factors in productivity change.
3 Methodology
Before proceeding to a description of the methodology section, we wish to reiterate how our approach improves on previous approaches that used the same direction and means to gauge productivity and efficiency. Whereas, there are many similarities in the non-parametric approaches used by others and our approach here, we will point out specifically where our variation can better identify sources of inefficiency.
3.1 Production technology and aggregate directional distance functions
First, we introduce the production technology that can be illustrated by the production set. Inputs X (N, number of inputs) can be used to produce outputs y (M, number of outputs). The production technology also meets some basic economic assumptions, such convexity, closedness, free disposability of inputs and outputs, and returns to scale, etc. (See detail in Hackman [21] and Li [22]). A general production technology can be defined in Eq. 1.
Decision making units (DMUs) represent the production unit in the production technology where is K number of provinces in China. The aggregate (total China) and individual (provincial) production technologies are defined as TAgg and Tk. In model specification, both assumptions of variable returns to scale (VRS) and constant returns to scale (CRS) are applied to estimate inefficiency scores. Following Ferrier et al. [23] and Boussemart et al. [22], the aggregate production technology has two representations related to individual ones under VRS and CRS cases. As shown in Eq. 2, the aggregate production technology is equivalent to the individual one under CRS, while the aggregate production technology is the summation of individual ones under VRS [22].
The distance function is the measurement that represents the production technology. Two types of distance functions have been widely used in literature: the Shephard approach and the directional distance approach. The latter one is proposed by Chambers et al. [24] and the direction vector can flexibly be set up. In contrast to the traditional setting of directional distance functions, the direction vector is defined as the aggregate value of inputs/outputs instead of evaluated at the individual DMU level. In this paper, efficiency composition is based on output-oriented aggregate directional distance functions and TFP estimation is depending on both input and output -oriented measures. So rather than assessing the individual DMU, using the aggregate value of inputs/outputs can be used to assess how to improve resource allocation and whether the source of the inefficiency is too many inputs or too few outputs. The general case of the direction vector and directional distance function can be defined in Eq. 3.
The inefficiency scores ϕ and δ represent the possible reduction of inputs or potential improvement of outputs in terms of aggregate inputs/outputs values respectively. For instance, a 1% inefficiency score for ϕ (δ) indicates that the evaluated DMU can reduce (expand) its inputs (outputs) level by 1% corresponding to total inputs (outputs) of the entire group of DMUs.
The unique direction setting is used as the basis for evaluating the potential improvement in the distance among observed DMUs and best practices. By comparing (in)efficiency scores, among DMUs, this will allow for a measure of group performance of selected DMUs. This is accomplished by aggregating individual DMU scores (this will be discussed in Section 2.2). Moreover, the TFP indicators constructed using this condition could be additive, thus a group TFP growth is the sum of individual TFP changes (this will be discussed in Section 2.3).
Alternatively, we also employ the traditional setting of directional distance functions as references to compare empirical results. The direction vector is usually defined as input/output value of evaluated DMU.
3.2 Efficiency decompositions
To measure potential improvement for the Chinese hospital sector, we employ an output-oriented aggregate directional distance function following the approach suggested by Boussemart et al. [25]. Based on the same unit of measurement, the inefficiency scores are additive that can be interpreted as how much the outputs level can be improved with a given level of inputs.
First, we attempt to analyze potential aggregate improvement for total Chinese hospitals by defining the Overall Inefficiency (OI) which is assessed under a VRS assumption as given in Eq. 4. This score is interpreted as the percentage of total hospital outputs that can be increased if all the hospitals within the provinces moved to the best practice production frontier.
The above OI is at an aggregate level that can be further decomposed. Second, the individual economic performance of each of the provinces is revealed by Technical Inefficiency (TI). This score is at an individual level which is the TI measures for the total sample given by the sum of individual TI. The catching up effect arises when there is a TI scores decrease over time.
Mix inefficiency (MI) measures the heterogeneity of input and output allocations among DMUs. For example, a misallocation in output mix may arise if we assume that service quality is equivalent but there is an inefficient price system among provinces, the use of inputs would be inefficient. Price differentials would lead to such a misallocation causing the customers (patients) prefer to choose cheaper service that leads to inefficiency in output allocation.
Scale inefficiency (SI) indicates the distance to the most productive scale size between the evaluated DMU and the production frontier. A decrease in SI indicates a possible improvement of evaluated DMU is approaching to optimal production scale. In Eq. 8, the SI is modelled in a combination of distance functions under VRS and CRS assumptions.
In general, OI is the sum of TI, MI, and SI. The summary of each efficiency components is represented in Table 2.
3.3 An additive Luenberger-Hicks-Moorsteen TFP indicator
Briec and Kerstens [26] introduced a Luenberger-Hicks-Moorsteen (LHM) TFP indicator. Kerstens et al. [27] (2018) further argue that this indicator is a better TFP measurement for an economic interpretation. In the work presented here, we employ both the input and output aggregate directional distance functions to measure the LHM TFP indicator. Following TFP defined by Briec and Kerstens [26] and aggregate directional distance functions suggested by Boussemart et al. [20], the additive LHM TFP indicator can be defined by merging productivity components in t and t + 1:
This TFP indicator is the mean of LHM components in t and t + 1.
The directional vectors for all elements of LHM TFP are obtained by using aggregate values of inputs/outputs as given in Eq. 3. Therefore, the individual TFP indicators are additive and a group TFP growth is the cumulative value of corresponding provinces that are homes to the hospitals being evaluated. From this approach, one can allocate productivity gain or loss among the DMUs. We argue that the traditional way of taking the arithmetic average value to obtain a group productivity change might not consider the size difference among DMUs leading to biased estimated values of productivity evolution trend. The proposed model given here can overcome this pitfall and the aggregate TFP growth is sum of individual productivity changes considering the most productive scale size which is an improvement over simple averaging.
Because of the common direction vector, the cumulative value of the TFP indicator can take on the summation of productivity changes in time dimension, but also in the provincial dimension. The total Chinese hospital TFP growths over period can be derived by cumulating provincial productivity gain (loss) in Eq. 12. Thus, individual contribution to total industry growth can be observed.
Alternatively, as the elements of TFP measure that constructed on the traditional distance functions, the TFP indicator at a group level is often defined as an arithmetic mean of individual TFP growths.
Finally, both parametric and nonparametric approaches can be applied to measure the distance functions. In this research, we select a nonparametric approach avoiding the need to prespecify the functional form of production technology. The detail format of DEA linear programs we applied is available from e.g. Ferrier et al. [23].
In Table 2 we present a summary of the measures used in this paper.
4 Data
To measure the contribution of each of the hospitals in the provinces and regions operating in China, we select a balanced provincial data of inputs and outputs at marco level from the National Bureau of Statistics of China [28]. The total sample contains 248 observations with 31 provinces over 2009–2016. Provinces can be grouped in three large areas depending on geographical and economic characters: the eastern region (with eleven relatively developed provinces: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, and Hainan), the inland region (with eight provinces: Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan), and the western region (with twelve relatively undeveloped provinces: Inner Mongolia, Guangxi, Sichuan, Chongqing, Guizhou, Yunnan, Tibet, Shannxi, Gansu, Qinhai, Ningxia, and Xinjiang).Footnote 2
Four inputs are used including the number of licensed (assistant) doctors, number of registered nurse, other technical staff, and number of beds in hospitals. The four outputs used here are emergency treatment in hospitals, other outpatients visits; the number of inpatients, and the number of surgeries per hospitals. The annual growth rates between the period of 2009–2016 of each the inputs and outputs are presented in Table 3.
One can observe that on the input side, except licensed doctors, other inputs in Western region have the fastest growth rates. On the output side, except emergency treatment, other outputs in Western region also have the fastest growth rates. This implies the backward region has been taken care by the recent healthcare reform in China.
5 Empirical results
One can observe the evolution of inefficiency scores for Chinese hospital system during 2009–2016 at the aggregate and regional levels in Table 4. At the aggregate level, the overall inefficiency is generally decreasing at −1.21% annual rate that can be decomposed into technical, mix and scale effects. This improvement in overall efficiency is mainly driven by the reduction in technical inefficiency that indicates a significant catching-up effect among the Chinese regional hospital sector. This catching-up effect is revealed by the growth rate of technical inefficiency that is decreasing at −0.81% annually and t-value is −9.30 based on the stochastic trend in Table 5. The inland region hospitals demonstrated the highest level of technical inefficiency, followed by the Western and Eastern regions respectively. Similar findings for the regions were likewise reported for the mix and scale effects, indicating that better allocation and size decisions need to be focused on the Inland region. At the regional level, we note that the improvement of Chinese hospital mainly arises in the inland and western regions. This indicates that these two regions benefited from the reform that happened in the sample period. Furthermore, the annual growth rates of technical inefficiency scores are −0.19%, −0.42%, and − 0.20% all negative in eastern, inland, and western regions respectively. This catching up effect among regions implies provinces attempted to improve their performance in order to get close to their benchmark.
Although the performance of mix effect is improving at the aggregate level in Chinese healthcare sector during 2009–2016, mix inefficiency scores in eastern region show a positive trend at 0.07%. This indicates the input/output mix used is leading to a misallocation resources or inefficient prices of healthcare inputs and outputs among regions.
For scale effect, the evolution of scale inefficiency score shows a negative trend (−0.18%) in inland region. This result may reveal that the provinces are improving their healthcare scale to the most productive scale size comparing to other areas.
We set the initial value of TFP indicator at a null level to create its cumulative change. The annual growth rate of cumulative TFP indicator is shown in Table 6. As this TFP indictor is additive, based on a common basis, we can allocate the contribution of each provincial units to the TFP growth for the Chinese hospital sector. The inland region contributes the most (43.86%) growth during the sample period. In detail, the hospitals operating in the Hubei and Shanxi provinces contribute more than 10%.
It can be seen in Table 7 that the aggregate DDF (by Eq. 3) is lower than the traditional DDF (by Eq. 4) which suggests that growth may be overestimated using the older approach. We also demonstrate that there is a wider range between the minimum and maximum scores in the traditional DDF that leads to more variation in the type of and source of inefficiency making it more difficult for assessing resource allocation decisions.
Contradictory results are observed in TFP estimation which indicates the sign of TFP change is opposite. This implies that different setting of direction vector also has significant impact on TFP measures. The suggestions or policy decisions may be influenced by bias results that should be taken care in the evaluation of economic performance.
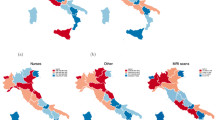
In Fig. 1, the evolution of cumulative TFP indicator is shown. The TFP gain during 2009–2016 was highest for Inland China, followed by Eastern China with Western China demonstrating the lowest TFP gains. Therefore, the proposed TFP measure allows to identify the contributions of TFP gains by allocating growth rates among regions. One can notice that the TFP growth in Chinese healthcare sector is noteworthy in 2009–2012 comparing to that in 2012–2016. The implemented policy reform may show slightly weak in the later stage.

Within each province, we report that Jiangsu hospitals demonstrated the highest TFP growth coupled with the largest proportion of total share of Province TFP growth (Table 6). For the Inland province, we report that Hubei had the greatest TFP growth along with the largest proportion of total share of total TFP growth. Finally, for the Western province Shanxi had both the highest TFP growth and the highest share by far for total TFP growth. However, for the Western Province, the range of TFP growth was −0.03 to 0.16%. Comparing this finding to the Inland Province performance wherein hospitals ranged from −0.08% to 0.28% and the Eastern Province −0.12% to 0.24%, it appears that TFP growth was lower, in general, to that of the other two provinces. Further, the Western Province, two hospitals had negative TFP growth compared to one county in the Inland Province. This is also indicative as to why the Inland Province had the continuously increasing growth of TFP. Interestingly, the hospitals in three of the counties in the Eastern Provinces demonstrated negative TFP growth but was balanced by the TFP growth in other counties.
6 Conclusion
Total factor productivity (TFP) indices and indicators measure the performance of decision-making units (DMUs) to produce the maximum outputs with the minimum inputs. In the literature, most methodologies evaluate the productivity growth for a specific production unit at an individual level. However, at an aggregate level, the traditional approach that takes the arithmetic average value for measuring a group productivity change may generate bias results and economic interpretations. Moreover, the contribution of each individual production units to the group TFP growth may not be clearly identified by previous approaches. In order to allocate productivity gain or loss among DMUs, in this paper we propose an additive and complete TFP measurement based on the Luenberger-Hicks-Moorsteen (LHM) approach. Here, the TFP indicator and aggregate distance functions are applied in an application to measure the economic performance of the Chinese hospital system at both the individual and group levels. The results indicate that the TFP growth of the Chinese hospital sector over the period 2009–2016 is driven by the hospitals operating in the inland region. Specifically we found that over the time frame of our analysis, the inland region demonstrated the most productivity growth of 1.07% as compared to the eastern region of 0.91% growth and the western region of 4.6%. Taken together, our findings demonstrate that China has had a healthy overall growth rate of 4.6%, but inefficiencies still exist. We found that when assessing inefficiency, the results were similar wherein the Inland region had the least inefficiency (recall that the negative sign designates less inefficiency) followed by the western region and finally the eastern region. Further decomposing the overall inefficiency measure, we note that the eastern region had the most inefficiency in terms of allocative inefficiency which corroborates other studies suggesting that urban areas of have too much technology in the hospitals. But, as far as scale inefficiency is concerned, we note that the hospitals in the eastern region do not have scale inefficiency, indicating they are the right size in terms of beds, but may not be using other inputs as effectively.
When compared to other studies, our findings contradict the results from Wang et al., [15] but this contrary finding may be attributed to the different methodological approaches wherein we apply the directional distance function rather than averaging used by the more traditional Malmquist approach applied by Wang et al. [15]. Furthermore, a significant catching up process has been detected among Chinese provincial healthcare sector.
To summarize, the impetus for this study is to update earlier studies in this area with more recent data as well as use a method that permits us to determine where, specifically, hospitals were not operating efficiently. The call for such as study comes from the literature in which authors claimed a misallocation of resources across China where in the non-coastal regions (Inland and Western) there were not as much resources allocated as compared to the Eastern Region. It was also argued that higher levels of demand and a breakdown of barriers of access would enhance efficiency and productivity.
As Ng [13] suggested in his work, hospitals suffered from productivity decline particularly in the coastal regions. This was contradicted by Hu et al. [1] who reported no statistically significant difference between coastal and non-coastal regions. Wang et al., [15] demonstrated that provincial differences in productivity did exist. Given these divergent findings, we add to the literature by employing a distance function approach using more recent data.
Unlike findings in other studies in this area, we found that Inland and Western regions were operating at efficiency levels below the Eastern region at statistically significant levels. Using the TFP analysis, we found that there was growth in the Inland region regions and that there was an increasing trend. However, these upward trends demonstrated that the learning curve of a more privatized, market approach to hospital care resulted in improved productivity.
Because we use the directional distance function, we can identify which provinces add the most to inefficiency at the regional level. Since policy making is at the regional levels, closer examination qualitatively why some locations have more inefficiency can be accomplished. The identify of provinces, will provide regional decision-makers to better meet the 2020 goal of better resource allocation.
We also assessed the TFP how China’s overall hospital performance improved over time. We could also ascertain which regions affect provincial TFP. This is a bottom-up approach which can be used to make allocative resources decisions. Given the increasing TFP in the Inland and Western Regions, we can surmise that rural hospital reforms may be achieving their objectives. Our findings follow the suggestion by Barber et al. [3] who wrote that the main goal for public hospitals is to maintain their social welfare function including accessible and affordable health care for the population. To ensure for such a goal to be achieved requires the efficient and productive use of resources in hospitals, and as such we have applied an appropriate method for government officials at all levels to assess hospital performance at either the provincial or county level. The findings reported here can also assist public hospital managers and more localized levels of government decision-making over the operations of hospitals to increase efficiency and productivity based on the best practices employed by other DMUs in the region. Ma, et al. [29] also acknowledge that reforms in China’s health care system have not fully met aspirations and calls for a system perspective for health services delivery. This matches the policies for better resource allocation, a topic we addressed here in this study. Further, the research here can be used to establish economic benchmarks along with pay for performance to increase efficiency and productivity in the hospital system [4]. Since health care reform has been predicted to become more decentralized with local government control, our findings can provide these policy makers regarding total factor productivity and the sources of total factor production that can be the focus of management, which is the future objective of hospital reform in China, rather than the allocation of resources at the centralized level that may not be able to account for local/regional/provincial nuances.
Another change that may affect resource allocation is the causes of death/disease. Gender differences also existed in health status within urban areas that were different than the gender differences in less populous areas [30]. According to a study on income differentials and health, the wealthier urban population was not considered healthier than the rural population [31]. The conclusion was derived from the finding that chronic disease dominated the course of illness in urban populations. China has also experienced rapid urbanization, and therefore new requirements for the health care system and hospitals for treating the associated health issues of an urbanized policy including pollution, obesity, and other chronic illnesses [31]. This finding corroborates the wish of the Chinese government to pursue more primary care/community health centers in urban areas since this is where effective treatment (prevention) occurs for treating chronic conditions. Again, this would require provincial decision making regarding resource allocation which we have supplied in the empirical section of this paper, specifically the findings of TFP growth, noting that the urban eastern region did not have the highest TFP growth rate.
Other future research would include using this same approach to determine which ownership form – non-profit or public has better performance. Closer examination of prices and resource allocation could also be assessed to determine the shadow prices for efficient pricing methods that can be provincially determined for better allocation of resources and payments that could be used to reduce barrier to access in less populated areas. Including measures of quality of care in outcomes would be included for future research to meet the Chinese policy of payment for performance [32]. Unfortunately, these data were not available.
Notes
As a reminder, the Malmquist approach uses inputs and outputs from multiple time periods comparing what could be produced using year 1’s inputs and compares this to year 2’s output. The index is analogous to traditional indices such as Paasche and Laspeyre, but instead of using prices and commodities of goods purchased, the Malmqusit approach uses inputs and outputs. For a further review, see (Färe, et al.s [16]).
We ignore the regions of Hong Kong, Macao and Taiwan in China due to data accessibility.
References
Hu H, Qi Q, Yang C (2012) Analysis of hospital technical efficiency: effect of health insurance reform. China Econ Rev 23(4):865–877
Blumenthal D, Hsiao W (2005) Privatization and its discontents – the evolving Chinese health care system. N Engl J Med 353(11):1165–1170
Barber S, Borowitz M, Bekedam H, Ma J (2014) The hospital of the future in China: China’s reform of public hospitals and trends from industrialized countries. Health Policy Plan 29(3):367–378
Liu G, Vortherms S, Hong X (2017) China’s health reform update. Annu Rev Public Health 38:431–448
Zhang Y, Ma Q, Chen Y, Goa H (2017) Effects of public hospital reform on inpatient expenditures in rural China. Health Econ 26(4):421–430
Liu X, Liu Y, Chen N (2000) The Chinese experience of hospital price regulation. Health Policy Plan 15(2):157–163
Gerdtham U, Sogaard J, Andersson G, Jonsson B (1992) An econometric analysis of health care expenditure: a cross-section study of the OECD countries. J Health Econ 11(1):63–84
Audibert M, Mathonnat J, Pelissier A, Huang H, Ma A (2013) Health insurance reform and efficiency of township hospitals in rural China: an analysis from survey data. China Econ Rev 27:326–338
China sets up new system to optimize medical resources. National Health Commission of the Peoples Republic of China (2015) http://en.nhc.gov.cn/2015-09/16/c_46816.htm
Yip W, Hsiao W (2008) The Chinese health system at a crossroads. Health Aff 27(2):460–468
Daemmich A (2013) The pollical economy of healthcare reform in China: negotiating public and private. Springer Plus 2:448–463
Li H, Dong S, Liu T (2014) Relative efficiency and productivity: a preliminary exploration of public hospitals in Beijing, China. BMJ Health Services Research 14:158–168
Ng. Y (2011) The productive efficiency of Chinese hospitals. China Econ Rev 22:428–439
Hu H, Qi Q, Yang C (2012) Evaluation of China’s regional hospital efficiency: DEA approach with undesirable output. J Oper Res Soc 63(6):715–725
Wang M, Fang H, Tao H, Cheng Z (2017) Bootstrapping data envelopment analysis of efficiency, and productivity of county hospitals in eastern, central, and Western China after public hospital reform. J Huazhong University Sci Technol 37(5):681–692
Färe R, Grosskopf S, Lindgren B, Roos P (1992) Productivity changes in Swedish pharmacies 1980-1989: a non-parametric Malmquist approach. J Prod Anal 3(1–2):85–101
Cheng Z, Tao H, Lin H, Lin X, Zhang R (2015) Technical efficiency and productivity of Chinese county hospitals: an exploratory study in Henan Province. BMJ Open Access 5:e007267. https://doi.org/10.1136/BMJOpen-2014-007267
Chu K, Zhang N, Chen Z (2015) The efficiency and its determinants for China’s medical care system: some policy implications for Northeast China. Sustainability 7(10):14092–14111
Yang, J., Zeng W. (2014). The tradeoff between efficiency and quality in the hospital production: some evidence from Shenzhen, China. China Econ Rev 31 166–184
Boussemart, J-P., Ferrier, G., Leleu, H., Shen, Z. (2018) An expanded decomposition of the Luenberger productivity indicator with an application to the Chinese healthcare sector. IESEG working paper
Hackman ST (2008) Production economics: integrating the microeconomic and engineering perspectives. Springer, Berlin
Li SK (1995) Relations between convexity and homogeneity in multi-output technologies. J Math Econ 24:311–318
Ferrier G, Leleu H, Valdmanis V (2010) The impact of CON regulation on hospital efficiency. Health Care Management Sci 83(1):84–100
Chambers R, Chung Y, Färe R (1996) Benefit and distance functions. J Econ Theory 70(2):407–419
Boussemart JP, Leleu H, Shen Z (2015) Environmental growth convergence among Chinese regions. China Econ Rev 34:1–18
Briec W, Kerstens K (2004) A Luenberger-Hicks-Moorsteen productivity indicator: its relation to the Hicks-Moorsteen productivity index and the Luenberger productivity indicator. Economic Theory 23:925–939
Kerstens K, Shen Z, Van de Woestyne I (2018) Comparing Luenberger and Luenberger-Hicks-Moorsteen productivity indicators: how well is total factor productivity approximated? Int J Prod Econ 195:311–318
National Bureau of Statistics of China (2017) http://www.stats.gov.cn/english/Statisticaldata/AnnualData/
Ma J, Lu M, Quan H (2008) From a national, centrally planned health system to a systems based on the market: lessons from China. Health Aff 27(4):937–948
Shi J, Liu M, Zhang Q, Lu M, Quan H (2008) Male and female adult population health status in China: a cross-sectional national survey. BMC Public Health 8:277–286
Gong P, Liang S, Carlton E, Jiang Q, Wu J, Wang L, Remais J (2012) Urbanisation and health in China. Lancet 379:843–851
Yu H (2015) Universal health insurance coverage for 1.3 billion people: what accounts for China’s success? Health Policy 119:1145–1152
Funding
There was no external funding received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There is no conflict of interest between the authors and other agencies or persons.
Ethical approval
This article does not contain any studies with human participants or animals performed.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shen, Z., Valdmanis, V. Identifying the contribution to hospital performance among Chinese regions by an aggregate directional distance function. Health Care Manag Sci 23, 142–152 (2020). https://doi.org/10.1007/s10729-019-09482-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10729-019-09482-4
Keywords
- China hospitals
- Aggregate directional distance function
- Additive Total factor productivity
- China hospital productivity