
Abstract
This quantitative and qualitative study aimed to identify fungi isolated from patient beds at a reference hospital in Teresina, Piauí, Brazil, and evaluate the efficacy of 70 % ethanol and 1 % hypochlorite for removing the contamination. Thirty-eight beds were chosen at random and the collection was carried out in three situations: before and after disinfection with 70 % alcohol or hypochlorite 1 %. Each sample was inoculated onto Sabouraud dextrose agar containing chloramphenicol and incubated at room temperature to allow fungal growth. We identified 13 species belonging to the genera Aspergillus, Cladosporium, Alternaria, Rhizopus, Penicillium, and Candida. All of these species are pathogenic and can worsen the clinical condition of patients. The 1 % hypochlorite solution proved to be an efficient disinfectant against the fungi, but the same was not observed using 70 % ethanol. Based on these findings, we recommended that the use of 1 % hypochlorite during bed disinfection be added to the hospital biosafety protocol to reduce cross contamination and contribute to patient recovery.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hospital-acquired infections can be caused by both internal and external factors, and pathogenic microorganisms are commonly transmitted by patients, visitors, health professionals, and contaminated biological materials. In susceptible patients, such as children, the immunocompromised, and patients with chronic diseases, fungi play a significant role in both localized and disseminated infections (Rainer et al. 2001).
Nosocomial infections have a wide epidemiological distribution and are associated with increasingly high levels of morbidity and mortality. Multiple factors contribute to the development of hospital-acquired infections, including invasive procedures, indiscriminate use of antimicrobials, immunological and nutritional status of debilitated patients, and lack of compliance with biosafety standards, particularly in regard to the sanitation of the environment and inanimate objects (Okten et al. 2012). In the absence of strict hygiene practices, the hospital environment—including the air, water, and inanimate surfaces surrounding the patient—can transmit infection. Hospitals are responsible for maintaining proper hygiene and disinfection procedures to provide a biologically safe environment for patients, visitors, and hospital employees (Reynolds et al. 2012).
In an epidemiological study of the major nosocomial infections in Brazil from 2000 to 2014, fungi were, with 143 cases, the second most common cause of hospital-acquired infections (De Almeida et al. 2014). This number represents only the properly notified cases, suggesting that the actual number of fungal infections in Brazilian hospitals may be much larger.
Analysis of fungal contamination of hospital beds is particularly important because contamination of inanimate surfaces plays a prominent role in the fungal transmission chain. The objectives of this study were to identify fungi isolated from hospital beds in a reference hospital in Teresina, Piauí, Brazil, and evaluate the efficacy of disinfectants against these pathogenic microorganisms.
Materials and methods
This was a quantitative observational study. Data was gathered between October 2014 and March 2015 from a reference hospital in Teresina, Piauí, Brazil, which treats contagious infectious diseases.
The 38 beds were randomly chosen from various nursing wards after liberation of the patient from the hospital. Samples were collected in three situations: before disinfection, after disinfection with 70 % alcohol, and after disinfection with hypochlorite 1 %. For the collection of the samples in the three aforementioned situations, we used sterile swabs soaked in saline 0.85 %, rubbed on three areas of greatest contact with the patient beds (upper end, middle region, and lower end). Alcohol 70 % was applied to 19 beds by friction with gauze on the surfaces for collection. After a period of 5 min, new samples were collected to verify its effectiveness. In the other beds, the hypochlorite 1 % was applied and after 5 min, held the collection to verify its effectiveness. Then they were transported at room temperature to the research laboratory of the University Center UNINOVAFAPI.
Duplicate Sabouraud dextrose agar plates (HiMedia Laboratories, Mumbai, India) containing 0.05 g L−1 chloramphenicol (INLAB, São Paulo, Brazil) were inoculated with 100 μL of sample and then incubated at room temperature for 72 h to allow fungal growth. After growth of the filamentous fungi, microcultures were prepared to allow observation of fungal structures and carry out species identification (De Hoog et al. 2000). Putative yeast species were isolated on BBL CHROMagar Candida (BDDifco, NJ, USA). Candida species were identified by observing colony color and through additional biochemical testing. The absolute (N°) and relative (%) frequency was calculated using Microsoft Excel 2007.
Results
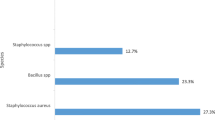
Filamentous fungi and yeast species were isolated from all 38 beds prior to disinfection. The most frequently observed species were Aspergillus niger (52.6 %), Penicillium citrinum (42.1 %), Aspergillus flavus (26.3 %), Cladosporium oxysporum (23.7 %), Cladosporium cladosporioides (18.4 %), Rhizopus oryzae (15.8 %), Aspergillus fumigatus (10.5 %), Curvularia lunata (7.9 %), and Candida tropicalis (7.9 %), as shown in Table 1.
After disinfection with 70 % alcohol, we observed the growth of the following colonies: A. flavus, A. niger, C. oxysporum, C. cladosporioides, R. oryzae, and P. citrinum. However, none were observed fungal colonies after the use of 1 % hypochlorite.
Discussion
Measures for containing infectious fungi inside health units rely on responsible practices by health professionals as well as all hospital users. Pathogens responsible for nosocomial infections may be carried by other patients, officials, professionals, and visitors, as well as inanimate objects and equipment that are in direct or indirect contact with the sick. Immunocompromised patients, those with nutritional deficiency, or patients subjected to invasive procedures are considered the most susceptible to nosocomial infection, particularly to contaminants in the air that are easily disseminated. Therefore, understanding the sources of infection in a hospital setting allows the implementation of effective prevention protocols (Cremesp 2010; Méheust et al. 2014).
According to the standard operating procedure (SOP) of the hospital, disinfection of beds should be performed soon after discharge, death, or patient transfer using three consecutive applications of 70 % alcohol by movements unidirectional rubbing for 15 s. Moreover, SOP guides the used rubber gloves by the operator must be washed and disinfected with 70 % alcohol after use.
All beds examined in the present study were contaminated with pathogenic fungi prior to disinfection. These findings suggest that the sanitation practices used by the hospital were insufficient, either as a result of inappropriate cleaning protocols or the selection of chemicals used for disinfection.
Studies of intensive therapy units in different countries that sampled incubators, beds, doors, doorknobs, windows, telephones, air conditioning apparatus, air, and stethoscopes found Penicillium, Cladosporium, Aspergillus, Alternaria, Curvalaria, Rhizopus, and Candida species, as well as other pathogenic and opportunistic species (Mobin and Salmito 2006; Cunha et al. 2011; Okten et al. 2012; Oviedo 2013; Santos et al. 2009). These findings show that, in addition to hospital beds, fungi are found on diverse surfaces in different medical units that house patients with weakened immune systems (Okten et al. 2012).
Fernando et al. (2013) examined the beds of patients with Candida in their bloodstreams in a private hospital located in São Paulo for the presence of fungi. They confirmed that 10 of the 25 beds examined were contaminated with Candida species, including Candida albicans, Candida parapsilosis, C. tropicalis, Candida orthopsilosis, and/or Candida glabrata. They also evaluated the effectiveness of disinfection of the beds with a solution of potassium monopersulfate and confirmed the presence of C. parapsilosis and Candida guilliermondii following disinfection with this solution. In contrast, Pereira et al. (2014) confirmed, after literature review, that sodium hypochlorite possesses sufficient antifungal activity to inhibit the growth of C. parapsilosis and C. guilliermondii, the species of Candida that were not inhibited by potassium monopersulfate in the previous study.
In the present study, we verified the growth of fungal colonies following disinfection using 70 % ethanol, suggesting that this cleaning agent is not a reliable disinfectant for use against fungi. However, we observed that none of the yeast species grew following disinfection with 1 % hypochlorite, consistent with the findings of Pereira et al. (2014). There was also no growth of filamentous fungi after treatment with this substance, suggesting that sodium hypochlorite is an efficient disinfectant for the removal of fungi.
The National Health Surveillance Agency (ANVISA) cleaning and disinfection manual indicates three specific products for disinfection of beds: 70 % ethanol, 0.02–1 % hypochlorite, and phenol (Brasil 2010; Ferreira et al. 2016). Ethanol (70 %) is a surface disinfectant used frequently by health units because of its easy application and low cost; however, it is not sufficient for effective elimination of microorganisms (Fernando et al. 2014; Ferreira et al. 2015; Ferreira et al. 2016; Peckham et al. 2016; Ribeiro et al. 2015). ANVISA guidelines require three applications of 70 % ethanol to achieve antimicrobial activity. However, a study has shown that following application of 70 % ethanol according to ANVISA guidelines, high levels of microbial contamination may still be present (Ferreira et al. 2016).
Fungi, particularly yeasts, can remain in hospital beds for long periods of time. Their presence can be related equally to aerial contamination (filamentous fungi) and contamination by the previous patient. Therefore, products used for disinfection must be carefully chosen and correctly applied (Pereira et al. 2014). Sodium hypochlorite is a far superior disinfectant to ethanol. Through the liberation of chlorine molecules, and with significant residual activity, sodium hypochlorite is highly toxic to pathogenic microorganisms when applied to inanimate surfaces. The inhibition of fungi, including species such as Candida, is almost instantaneous at high concentrations (30 s with 5.25 % hypochlorite) (Ferreira et al. 2015).
Conclusion
Our results confirmed that all of the beds examined were contaminated with pathogenic fungi prior to disinfection, which can further complicate the clinical picture of immunocompromised patients. We also found that 70 % ethanol did not satisfactorily disinfect beds in the evaluated hospital, and the use of the hypochlorite 1 % by unidirectional rubbing movements for 5 min after washing with water and detergent is a disinfection method efficient against fungi.
Therefore, this study reinforces the need to include 1 % hypochlorite treatment for disinfection of beds in the biosafety protocol of the hospital in this study, as well as in the ANVISA guidelines. This measure is essential to reduce cross contamination and thus promote safe recovery of the patient.
References
Brasil (2010). Agência Nacional de Vigilância Sanitária Segurança do paciente em serviços de saúde: limpeza e desinfecção de superfícies/Agência Nacional de Vigilância Sanitária. Brasília: Anvisa.
Conselho Regional de Medicina do Estado de São Paulo (CREMESP), Ministério Público do Estado de São Paulo (2010). O controle da infecção hospitalar no Estado de São Paulo. Conselho Regional de Medicina do Estado de São Paulo.
Cunha, M. A., Nery, A. F., Lima, F. P., Junior, J. D., Neto, J. M., Calado, N. B., Luz, K. G., & Milan, E. P. (2011). Rhinocerebral zygomycosis in a diabetic patient. Revista da Sociedade Brasileira de Medicina Tropical, 44(2), 257–259.
De Almeida, Z. G., & Farias, L. R. (2014). Epidemiological investigations of principal nosocomial infections in Brazil and identification of pathogens responsible: a bibliographic approach. Revista Brasileira de Pesquisa em Ciências da Saúde, 1(2), 49–53.
de Fernando, F. S. L., Ferreira, A. M., Colombo, T., Rigotti, M. A., Rubio, F. G., & Almeida, M. G. T. (2014). Álcool Etílico: análise da ação desinfetante sobre leveduras presentes em colchões hospitalares. Journal of Nursing UFPE, 8(5), 1273–1283.
De Hoog, G. S., Guarro, J., Gené, J., & Figueras, M. J. (2000). Atlas of clinical fungi (2nd ed.). Washington: ASM Press.
Fernando, F. S. L., Ferreira, A. M., Colombo, T. E., Rubio, F. G., & Almeida, M. T. G. (2013). Fungal contamination of hospital mattresses before and following cleaning and disinfection. Acta Paulista de Enfermagem, 26(5), 485–491.
Ferreira, A. M., de Andrade, D., Rigotti, M. A., de Almeida, M. T. G., Guerra, O. G., & Junior, A. G. S. (2015). Assessment of disinfection of hospital surfaces using different monitoring methods. Revista Latino-Americana de Enfermagem, 23(3), 466–474.
Ferreira, R. E. C., Neto, J. R., Antas, M. G. C., Sobrinho, C. R. W., & Peres, F. M. M. R. (2016). Eficácia de três substâncias desinfetantes na prática da radiologia odontológica. Revista Brasileira de Odontologia, 73(1), 14–19.
Méheust, D., Cann, P. L., Reboux, G., Millon, L., & Gangneux, J. P. (2014). Indoor fungal contamination: health risks and measurement methods in hospitals, homes and workplaces. Critical Reviews in Microbiology, 40(3), 248–260.
Mobin, M., & Salmito, M. D. A. (2006). Fungus microbiota in air conditioners in intensive care units in Teresina, Piauí. Revista da Sociedade Brasileira de Medicina Tropical, 3(6), 556–559.
Okten, S., & Ahmet, A. (2012). Airborne fungi and bacteria in indoor and outdoor environment of the pediatric unit of Edirne Government Hospital. Environmental Monitoring and Assessment, 184(3), 1739–1751.
Oviedo, M. S., Sturm, M. E., Reynoso, M. M., Chulze, S. N., & Ramirez, M. L. (2013). Toxigenia profile and AFLP variability of Alternaria alternata and Alternaria infectoria occurring on wheat. Brazilian Journal of Microbiology, 44(2), 447–455.
Peckham, D., Williams, K., Wynne, S., Denton, M., Pollard, K., Barton, R. (2016). Fungal contamination of nebuliser devices used by people with cystic fibrosis. Journal of Cystic Fibrosis, 15(1), 74–77.
Pereira, J. G., Zan, R. A., Jardin, C. F., & Meneguetti, D. U. O. (2014). Analysis of airborne fungi in a hospital in the town of Ariquemes, Rondônia, Western Amazon region, Brazil. Revista de Epidemiologia e Controle de Infecção, 4(1), 18–22.
Rainer, J., Peintner, U., & Pöder, R. (2001). Biodiversity and concentration of airborne fungi in a hospital environment. Mycopathologia, 149(2), 87–97.
Reynolds, K. A., Boone, S., Bright, K. R., & Gerba, C. P. (2012). Occurrence of household mold and efficacy of sodium hypochlorite disinfectant. Journal of Occupational and Environmental Hygiene, 9(11), 663–669.
Ribeiro, M. M., Neumann, V. A., Padoveze, M. C., & Graziano, K. U. (2015). Eficácia e efetividade do álcool na desinfecção de materiais semicríticos: revisão sistemática. Revista Latino-Americana de Enfermagem, 23(4), 741–752.
Santos LS, Bernardes RC, Magalhães LM, Siqueira FS, Khouri S (2009). Perfil de sensibilidade de amostras isoladas de casos de candidurias hospitalares aos antifúngicos convencionais. XIII Encontro Latino Americano de Iniciação Científica e IX Encontro Latino Americano de Pós-Graduação – Universidade do Vale do Paraíba.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
da Silva Aquino, I., Porto, J.C.S., da Silva, J.L. et al. Evaluation of disinfectants for elimination of fungal contamination of patient beds in a reference hospital in Piauí, Brazil. Environ Monit Assess 188, 644 (2016). https://doi.org/10.1007/s10661-016-5654-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-016-5654-z