
Abstract
Between 2002 and 2017, concentrations of fine particulate matter (PM2.5) decreased 37% in the United States. Environmental economic theory generally assumes that environmental improvement is associated with a decrease in the marginal damage of emissions. In this case, the marginal damages of PM2.5 precursor emissions (NH3, NOX, primary PM2.5, and SO2) increased substantially. I calculate the change in the marginal damages of emissions between 2002 and 2017, finding increases, on average, of 30% for NH3, 46% for NOX, 61% for primary PM2.5, and 36% for SO2. The increase in marginal damages is especially large in the southeastern United States, with values more than double over this time period. The key factors that influence this change in marginal damages are the shape of the concentration-response (C-R) function that was adopted for these calculations between PM2.5 exposure and mortality (positive effect), the increase in the real value of a statistical life (positive effect), the increased population (positive effect), the aging of the population (positive effect), the decreased age-specific mortality rates (negative effect), and the geographic distribution of emissions (mixed effect). Between 32 and 65% of the increase in marginal damages is attributable to the shape of the C-R function and the decreased concentration of PM2.5. The C-R function adopted here indicates that the marginal effect of concentration reductions is higher at lower concentrations. Thus, at the lower PM2.5 concentrations resulting from improvements over 15 years, there would be a larger reduction in mortality from each additional unit of pollution reduction.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Air quality in the United States (US) has improved substantially since 2000, with fine particulate matter (PM2.5) concentrations reduced, on average, 37% (US Environmental Protection Agency 2022b). Corresponding to this improvement, emissions of all criteria air pollutants have decreased between 2000 and 2021, most notably with sulfur dioxide (SO2) and nitrogen oxides (NOX) declining by 89% and 66%, respectively (US Environmental Protection Agency 2022a). The benefits of these air quality improvements, in terms of improved health and reduced mortality, are enormous, and estimates from regulatory impact analyses from the Environmental Protection Agency (EPA) show that these benefits greatly outweigh the costs of pollution abatement (US EPA 2011, 2013).
In the traditional economic model of environmental degradation, the marginal benefits of abatement are declining as environmental quality improves, generally leading to an optimal environmental quality in which the marginal benefits equal the marginal costs of additional abatement. Following the improvements in air quality of the magnitude observed over the past 20 years, one may expect the marginal benefits today of additional pollution reductions to be much lower than in the past. Here, the change in the marginal benefits of abatement (or alternatively, the marginal damages of emissions) are calculated between 2002 and 2017 using air pollution modelling and concentration-response (C-R) functions from the epidemiological literature, and show, for a variety of reasons, that the marginal benefits of abatement were substantially higher in 2017 than they were 15 years prior when air quality was much worse. I explore and discuss the reasons why, using standard methods for calculating air pollution damages, that the marginal damages increased over time. If the marginal benefits of additional air pollution reductions are greater today than in the past, then it suggests that it may be optimal to achieve even more pollution reductions—potentially substantial reductions.
Our focus is on PM2.5 pollution, and the emission of those pollutants that contribute to PM2.5 concentrations. PM2.5 is composed of small solid particles and liquid droplets, less than 2.5 microns in diameter (US EPA 2021a). This fine particulate matter is distinguished from coarse particulate matter, less than 10 microns in diameter (PM10), in being able to travel much greater distances from the sources of emission and potentially penetrate more deeply into the lungs when inhaled, causing serious health effects (US EPA 2021a). Ambient exposure to PM2.5 is associated with several detrimental health effects, including premature mortality from ischemic heart disease, stroke, and upper respiratory tract infections (Krewski et al. 2009; Lepeule et al. 2012; Thurston et al. 2016; Burnett et al. 2018), and is estimated to be responsible for between 100,000–200,000 deaths in the US per year (Goodkind et al. 2019; Burnett et al. 2018).
The emission of several pollutants contributes to ambient PM2.5 concentrations. These pollutants can be either emitted as primary PM2.5 (emitted already in the form of fine particulate matter), or as other pollutants: SO2, NOX, ammonia (NH3) or volatile organic compounds (VOC), which form into secondary PM2.5 in the atmosphere. The ambient PM2.5 concentration combines primary and secondary PM2.5. Because the mechanism for regulating PM2.5 concentrations is at the sources of emissions of the contributing pollutants, the focus of the analysis is on the changes in the marginal damages of emissions over time of four pollutants (primary PM2.5, SO2, NOX, and NH3) that contribute to PM2.5 concentrations. Due to changes in the methodology of calculating quantities of emissions of VOCs over this time period, it is not possible to provide accurate calculations of the change in marginal damages of VOCs. Therefore, VOCs were excluded from the analysis.Footnote 1
Why have the marginal damage of emissions increased between 2002 and 2017? There are two key factors: (i) a positive shift in the marginal damage function due to demographic changes and increases in the value of mortality risk reductions, and (ii) a movement up along the marginal damage function resulting from concentration reductions and the relationship between PM2.5 and health effects.
The key demographic changes are to the total population of the US, the age distribution of the population, and the age-specific mortality rates. Between 2002 and 2017, the contiguous US adult population increased 16%. All else equal, the more people that are exposed to pollution, the larger the marginal damages per unit of emission. During this time period, the population got older on average, with a much larger share of the population represented by the oldest age groups. Studies suggest that older populations are at much higher risk of mortality from exposure to PM2.5 than younger populations (Burnett et al. 2018; Yin et al. 2021; Shumake et al. 2013). With an older, more pollution-vulnerable population, the marginal impact of emissions is larger. However, over this period, the age-group specific mortality rates decreased substantially, suggesting an overall healthier population, diminishing the effect of an older population.
Another factor leading to a shift in the marginal damages is that over time, with a wealthier population, one would expect the marginal willingness-to-pay for mortality risk reductions, the so-called value of a statistical life (VSL), to increase. An increased VSL is likely to contribute to a relatively small increase in the marginal damages of emissions.
These demographic and VSL changes led to a positive shift in the marginal damage function. As a simplified illustration of this effect, Fig. 1 demonstrates the marginal damages of a one-unit PM2.5 concentration change for the city of Charlotte, NC, which experienced a large population increase and a large PM2.5 concentration decrease. The blue line shows the marginal damages given 2002 conditions, and the red line shows the increased marginal damages after the demographic and VSL changes by 2017. This shift led to a 38% increase in the marginal damages (as shown by the vertical distance: \(\Delta M{D}^{\text{shift}}\)). Thus, if PM2.5 concentrations had remained constant at 2002 levels—approximately 14 µg m−3—marginal damages of PM2.5 would have increased 38% due to the demographic and VSL changes.

Marginal damage functions for Charlotte, NC example. The solid-blue curve represents the marginal damages of an additional unit of PM2.5 concentration exposure for the city, given 2002 conditions. The solid-red curve represents the marginal damages given 2017 conditions. The dashed blue lines show the PM2.5 concentration in 2002 and the mapping to marginal damages in 2002. The dashed red lines show the lower PM2.5 concentration in 2017 and the mapping to increased marginal damages in 2017. The vertical distance (ΔMDshift) represents the positive shift in the marginal damage function due to demographic and VSL changes. The vertical distance (ΔMDΔPM) represents the increased marginal damages in 2017 compared with 2002 due to the reduction in PM2.5 concentration (ΔPM) over this period
Our second factor, leading to the movement left and up the marginal damage function, is the result of the shape of the relationship between air pollution and mortality—i.e., the C-R function. The epidemiological research suggests that the relative risk of mortality from exposure to PM2.5 is concave (Krewski et al. 2009; Pope et al. 2011; Crouse et al. 2012; Burnett et al. 2014, 2018; Vodonos et al. 2018; Christidis et al. 2019). This relationship indicates that the marginal increase in the risk of mortality from exposure to more PM2.5 is higher at lower concentrations. This means that a one-unit reduction in PM2.5 to a population with relative clean air will save more lives than a similar reduction for a population with relatively dirty air. Thus, the population in 2017, with relatively cleaner air than in 2002, should exhibit more, not less, marginal benefit from an additional unit of pollution reduction.
The C-R function adopted for the present analysis is illustrated by the shape of the marginal damage functions in Fig. 1, which are declining with higher PM2.5 concentrations. In Fig. 1, and throughout this paper, I use the C-R function from Burnett et al. (2018) [also called the Global Exposure Mortality Model (GEMM)]. Figure 1 shows that along the 2017 marginal damage function (red curve), the marginal damages at the higher PM2.5 concentration in 2002 (14.2 µg m−3) are substantially lower than the marginal damages with the lower PM2.5 concentration in 2017 (7.8 µg m−3). By reducing the concentration by 45% in Charlotte, the marginal benefit of an additional unit of reduction increased by 36% (as shown by the vertical distance: \(\Delta M{D}^{\Delta PM}\)).
This effect illustrated for Charlotte, NC is representative of an effect experienced across the US between 2002 and 2017. This example is a simplification of the analysis by examining a single location and the exposure to PM2.5 concentrations, whereas the analysis that follows traces the pollution back to the sources of all emissions across the contiguous US. Using emission inventories between 2002 and 2017, air pollution modelling, and the GEMM C-R function, the marginal damages of emissions from all sources in the US over this period were calculated, identifying key trends and factors explaining the changes. Section 2 describes the methods used, Sect. 3 presents the results of the analysis, and Sect. 4 concludes.
2 Methods
2.1 Marginal damages
The primary indicator to be calculated are the marginal damages of emissions from a particular source of emissions. This is calculated for all sources of emissions in the contiguous US, for four pollutants, and for six different years of emission inventories (2002, 2005, 2008, 2011, 2014, and 2017). I start by deriving the marginal damage of emissions equation. The only health endpoint included is adult premature mortality. This is likely to result in an underestimate of the total damages from emissions, but only slightly, as other calculations of air pollution damages indicate that the damages from other health endpoints and environmental consequences of air pollution are small in comparison to premature mortality (Muller and Mendelsohn 2007).
Before calculating the marginal damages of emissions, we need to derive the total mortality (\({M}_{i}\)) in location \(i\), which is exposed to ambient PM2.5 concentrations (\({C}_{i}\)).
where \({p}_{i}\) is the population, and \({\lambda }_{i}\) is the mortality rate, which is some function of the ambient PM2.5 concentration.Footnote 2 The relationship that explains how the mortality rate changes with different PM2.5 concentrations is the C-R function or relative-risk (\(RR\)) function. Taking the observed mortality rate, \({\lambda }_{i}^{0}\), given the observed PM2.5 concentration, \({C}_{i}^{0}\), as the baseline risk (\(RR\) = 1), then the mortality rate at any other concentration, \({C}_{i}\), can be calculated as \({\lambda }_{i}\left({C}_{i}\right)={\lambda }_{i}^{0}\cdot RR\left({C}_{i}\right)\). Total mortality, in Eq. (1), becomes \({M}_{i}\left({C}_{i}\right)={p}_{i}\cdot {\lambda }_{i}^{0}\cdot RR\left({C}_{i}\right).\)
Next, the equation for the marginal increase in mortality from a one-unit increase in the PM2.5 concentration in location \(i\) is,
For this derivative (\(R{R}^{\prime}\)), I adopt an estimate from the epidemiological literature—the GEMM C-R function in Burnett et al. (2018). The GEMM is a series of meta-regressions using 15 independent individual-level cohort studies combined with an additional 26 relative-risk estimates from the literature of the C-R function between ambient PM2.5 and cause- and age-specific morality. Using the estimated GEMM functions, the change in the relative risk of mortality for any one-unit change in PM2.5 concentration is obtained.
The marginal mortality estimate can be converted into marginal damages at the baseline concentrations by multiplying by the VSL (\(V\))Footnote 3:
Equation (2) are the marginal damages of a change in PM2.5 concentration at any location. Next, is the equation for the marginal damages of emissions from a source. Any source of emissions is likely to impact many downwind locations. Therefore, the marginal damages of emissions of pollutant \(s\) from source \(j\) are the sum of the marginal damages of a concentration increase in all locations \(i\) shown in Eq. (2), weighted by the marginal increase in concentrations at \(i\) resulting from increased emissions at \(j\):
where \({\pi }_{ij}^{s}\) is the change in PM2.5 concentration in location \(i\) from a one-unit increase in emissions of pollutant \(s\) at source \(j\). The \({\pi }_{ij}^{s}\) coefficients come from the InMAP Source-Receptor Matrix (ISRM) in Goodkind et al. (2019). The ISRM uses a reduced form air-quality model, InMAP (Tessum et al. 2017), and isolates the impact of emissions from any particular source grid cell in the US to all possible locations. The ISRM uses variable-sized grid cells, with smaller grid cells in areas with higher population density. Marginal damages of emissions from every grid cell in the ISRM are calculated, and then emission sources are allocated to the corresponding grid cells in the ISRM.
2.2 Data
To calculate marginal damages, data on populations by age group, baseline (observed) mortality rates by age and cause, and observed PM2.5 concentrations were collected. Population data was collected at the Census tract level, in five-year age groups, and by race and ethnicity for the total population (Manson et al. 2021). Data was available for the years 2008, 2011, 2014 and 2017. It was unavailable for 2005 and 2002, and therefore population data from 2000 and 2008 was interpolated to estimate populations for 2002 and 2005.
Observed mortality rates were collected from the Centers for Disease Control and Prevention (CDC 2020). Data were collected for each year (2002, 2005, 2008, 2011, 2014, and 2017) by five-year age groups, at the state urbanization-category level. Data at the county level by age group was often unreliable, and therefore aggregating by urbanization category within a state was used. Six urbanization categories were combined into three groups: large metro (large central metro, large fringe metro), medium metro (medium metro, small metro), and non-metro (mircopolitan, noncore). These groupings exhibited substantially different age-specific mortality rates, and provided some degree of sub-state level heterogeneity in age-group mortality rates. The urbanization-group mortality rates were assigned to counties based on the county urbanization categorization (CDC 2017). Lastly, to get mortality rates for each grid cell, the mortality rate of the county within which the grid cell centroid resided was used. The mortality data included a subset of causes of death, rather than all causes. This was done to be consistent with the GEMM C-R function from Burnett et al. (2018), which examined the association between PM2.5 concentrations and deaths from non-communicable diseases plus lower-respiratory infections (NCD + LCI) (see Appendix for list of CDC codes included). The list of causes of death included in our analysis represented 87% of all deaths.
Annual average ground-level PM2.5 concentration data were collected from datasets using satellite measurements and calibrated with ground-level observations (van Donkelaar et al. 2021) for the years 2002, 2005, 2008, 2011, 2014, and 2017. The data were gridded at 0.1º × 0.1º across North America. These data were applied to the grid cells in the ISRM by taking the mean of the observations that were inside each ISRM grid cell.
2.3 VSL
For the main analysis, a uniform VSL was applied across all ages for the willingness to pay for changes in mortality risk. This uniform approach is commonly adopted in this literature and by the EPA in regulatory impact analyses. However, estimates of the VSL indicate that over time the value increases with income. The EPA estimates a triangular distribution of the income elasticity of the VSL with a mean of 0.49 (US EPA 2010). This mean value was applied to the real GDP per capita in the US over our study period (US Bureau of Economic Analysis 2022), to obtain VSL estimates for each year (in 2017$). The VSL increased by 10% (in real terms) from $9.17 million in 2002 to $10.08 million in 2017.
Estimates of the VSL are often derived from hedonic wage analyses, studying the relationship between compensation and the risk of death on the job of the working-age population. Studies of the risk of premature mortality related to air pollution exposure, find that the overwhelming majority of victims are older than the typical working-age adult. This raises the question if it is appropriate to apply the VSL derived by decisions of working-age adults to the generally older population harmed by air pollution. To illustrate the importance of age, the results are produced using a VSL uniformly applied to all populations—as is done by the EPA—as well as two alternative estimates of the VSL that are age adjusted.
The first age-adjusted VSL, which has intuitive appeal, is to apply a uniform value for each additional year of life expectancy (i.e., a uniform VSL-year or VSLY). In this approach, it is assumed that each year has equal value, on average, to individuals of any age, but the VSL is larger for younger individuals than older because they have more years of remaining life expectancy. With this measurement, the VSL at any age is equal to the discounted sum of the VSLY for the remaining years of life expectancy.
Evans and Smith (2006) note that “the conclusion that VSL declines with age has gained a status close to a professional consensus,” which would argue in favor of the age-adjusted VSL described above. Evans and Smith (2006), however, demonstrate that there is both theoretical and empirical evidence that suggest that an ever declining VSL over one’s lifetime may not be correct. This does not imply, however, that the VSL is necessarily uniform for all age groups. Aldy and Viscusi (2008) estimated this age-VSL relationship, and found an inverted-U shaped VSL across ages, perhaps reflecting the levels of consumption across the lifetime. This relationship rises from young to middle aged workers and then declines as workers reach retirement age.
These two age-adjusted VSL measurements (i.e., VSLY and inverted-U VSL) were applied to the results to understand the sensitivity of the conclusions to different VSL methodologies. I follow Robinson et al. (2021) who used the three VSL measurements described above. For the VSLY, a value of $432,000 is used for each year of additional life expectancy, along with the estimated life expectancy by age (Arias and Xu 2019). This produces a VSL equal to the uniform VSL of $10.08 million for a 40-year old individual using a 3% discount rate. For the inverted-U VSL, the cohort-adjusted VSL from Aldy and Viscusi (2008) was used and adjusted so that the VSL for a 40-year old is again equal to $10.08 million. A potential problem with the inverted-U VSL is that it stops at age 62. I use the age 62 estimated VSL for all older populations, again following Robinson et al. (2021). Each VSL measure, across age groups, is produced in Table 2 in the Appendix.
2.4 Emissions
US emissions data were downloaded from the National Emissions Inventory (NEI), which is compiled for every three years (2002, 2005, 2008, 2011, 2014, and 2017; US EPA 2021b). Emissions of primary PM2.5, SO2, NOX, NH3, and VOC were collected. Each year’s inventory is separated into point, non-point, on-road, and non-road sources. All emissions needed to be allocated to ISRM grid cells for the estimation of marginal damages. Every point source includes geographic locational information and were allocated to the grid cell it resided in. All other emission categories (non-point, on-road, and non-road) were summarized at the county level in the NEI. County emissions were allocated to ISRM grid cells proportionally to the population of the grid cells within that county. Point-source emissions were separated into three groups according to the release height of the emissions using the effective stack height. The heights are ground level or low stacks, middle stacks, and high stacks which affects the magnitude and spatial distribution of the air quality effects from emissions (see details of stack height allocation in Goodkind et al. 2019).
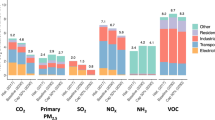
A summary of the emissions across all categories is shown in Table 1 (Table 3 in the Appendix shows summaries of emissions for each category). Emissions of SO2, mostly from point sources, dropped from 13.5 to 2.1 million metric tons from 2002 to 2017. NOX emissions, mostly from point and on-road sources, also dropped substantially from over 19 million metric tons to under 10 between 2002 to 2017. Emissions of VOC appears to have increased substantially over this period, but this is due to a change in the estimation methods of non-point VOC emissions in the NEI, not an actual observed increase in emissions. Therefore, VOCs were excluded from the analysis going forward.
2.5 C-R function
To make the marginal damage calculations, an appropriate C-R function was needed. To that end, the GEMM C-R functions were used relating NCD + LRI with PM2.5 concentrations (Burnett et al. 2018). Several reasons contributed to this choice over the other available options.
It was necessary to find a C-R function that related adult premature mortality with long-term exposure to PM2.5 air pollution. This endpoint makes up the vast majority of air pollution impacts in EPA calculations (US EPA 2011, 2013), and thus seems appropriate for understanding the changes in marginal damages over time. However, the bulk of the estimates of this relationship come from observational studies from the epidemiological literature. These estimates use sophisticated statistical methodologies and provide important associations, but perhaps lack the validity of causal-inference methodologies. Several strands of recent research have identified causal relationships between air pollution and adverse health and social effects (Currie and Walker 2011; Stafford 2015; Knittel et al. 2016; Burkhardt et al. 2019). These types of studies often rely upon infant health metrics as the endpoint due to more plausible claims of causality. These endpoints, however, are not suitable for this analysis.
Deryugina et al. (2019) found a causal relationship between air pollution and adult premature mortality, using wind direction as an instrument for pollution. This provides important validation of this relationship, but is not directly usable for the analysis here because it is silent on the shape of the air pollution/mortality relationship. The shape of the C-R function is vital for the analysis being conducted in the present paper, in being able to indicate how changes in PM2.5 concentrations affect the marginal damages of emissions. Several estimates from the epidemiological literature address the shape of the C-R function, with many finding a concave shape (Krewski et al. 2009; Pope et al. 2011; Crouse et al. 2012; Burnett et al. 2014; Vodonos et al. 2018; Christidis et al. 2019), with a steeper increase in mortality, per unit of PM2.5 increase, at low compared with high concentrations. A few papers in the economics literature also identified a concave shape of the air pollution C-R function—for example, Schlenker and Walker (2016) estimate the causal link between short-term variations in carbon monoxide and hospital admissions using airport congestion; and Gong et al. (2023) estimate the relationship between long-run exposure to PM2.5 and mortality in China using trade shocks as an instrumental variable. The GEMM is an ideal choice to understand the effect of a nonlinear C-R function as it is a meta regression of 41 separate studies, and uses a flexible functional form to let the data determine the shape of the C-R function.
The GEMM is a global estimate, mostly relying on studies from low-concentration countries in North America and Europe, but also including data from high-concentration countries, such as China (Burnett et al. 2018). There are a few major cohort studies based specifically on US populations (the American Cancer Society Study and the Harvard Six-Cities Study)—which are both included in the GEMM meta regression (Turner et al. 2016; Lepeule et al. 2012)—but estimates from these studies do not address the question of shape to the same degree as GEMM.
With the caveats that GEMM is based on associational, and not causal, studies, and is estimated for global populations, it was the best C-R function for the present analysis. While there is strong suggestive evidence that the C-R function is concave, this is not a settled question with definitive proof. The analysis provided here illustrates the effect on marginal damages from emissions as PM2.5 concentrations improve if we have a concave C-R function as found in GEMM.
The GEMM functions are stratified by five-year age groups for the adult population. The left panel of Fig. 2 illustrates the marginal relative risk [i.e., the change in the relative risk of mortality from a 1 µg m−3 increase in PM2.5 concentration—or the \(R{R}^{\prime}\left({C}_{i}\right)\) from Eq. (2)] for each age group. Two important features are evident from these functions. First, the marginal change in risk is much greater at lower concentrations than higher concentrations. Each function is relatively flat above approximately 13 µg m−3, and has a steep slope between 4 and 9 µg m−3. There is a two-fold greater risk reduction in going from a PM2.5 concentration of 5 to 4 µg m−3 than from going from 14 to 13 µg m−3. Second, the marginal relative-risk reduction is greater for younger compared with older populations. Thus, all else equal, an air quality improvement will provide a larger relative-risk reduction to younger populations. However, the absolute risk reductions are much larger for older populations who face substantially higher baseline risks of mortality, as is illustrated in the right panel of Fig. 2—the right panel shows the change in the mortality rate by age groups from a 1 µg m−3 increase in PM2.5 concentration, with substantially larger changes in the mortality rate for older populations compared with younger adults.

Left panel: Change in the GEMM relative-risk functions by five-year age groups. Each curve shows the change in the relative risk of mortality from a 1 µg m−3 increase in PM2.5 concentration. Right panel: Change in the mortality rate from NCD + LRI causes (per 100,000 population) for GEMM functions by five-year age groups. Each curve shows the change in the mortality rate from a 1 µg m−3 increase in PM2.5 concentration
2.6 Scenarios
In addition to calculating the changes in marginal damages over time, the factors that most influenced these changes were of interest. In particular, were how changes in the PM2.5 concentration, the VSL, the total population, the age distribution of the population, the age-specific mortality rates, and the location of emission sources each impact the marginal damages of emissions between 2002 and 2017.
To understand the effect of one of these factors, I see how the marginal damages in 2017 compare if one factor is held at 2002 levels. For example, with the VSL, this is easily accomplished by using the 2002 VSL value in the calculation for 2017 marginal damages. Then comparing the original 2017 marginal damages and these adjusted 2017 marginal damages (with the 2002 VSL), the effect of an increased VSL between 2002 and 2017 on the marginal damages was isolated. Similar methods were used to isolate the impact of the other factors involved. Most importantly, by isolating the effect of the change in the PM2.5 concentration, the importance of the shape of C-R function in increasing marginal damages as overall concentrations decline is demonstrated.
3 Results
3.1 Trends
To start, the trends in the factors that influence marginal damages are compared. Figure 3 shows that PM2.5 concentrations declined consistently between 2002 and 2017, falling 36% from a population-weighted average of 12.0 to 7.7 µg m−3. These trends were consistent across racial and ethnic groups, with 38% and 34% reductions for black and Hispanic populations, respectively. The decline in concentration exposure was greatest in those locations facing the worst air quality. The 95th percentile concentration exposure dropped 37% from 17.9 to 11.3 µg m−3, whereas the 5th percentile exposure dropped 22% from 7.0 to 5.5 µg m−3. Figure 4 shows that the largest PM2.5 concentration reductions between 2017 and 2002 were located in the eastern half of the country and California, with five to ten µg m−3 declines in the Rust Belt and states in the upper south (see Fig. 9 in the Appendix for PM2.5 concentration maps for years 2002, 2005, 2008, 2011, 2014, and 2017). Areas in Montana and the Pacific Northwest saw small concentration increases in 2017 (compared with 2002), potentially the result of abnormally bad wildfires in the region.

Population-weighted average PM2.5 concentration trends (µg m−3) for the total population and by racial and ethnic subpopulations

Change in PM2.5 concentration (µg m−3) between 2002 and 2017 (C2017 – C2002)
The adult population (defined here as 25 and older) in the contiguous US (which excludes Hawaii, Alaska, and Puerto Rico), increased 16% from 185 to 215 million between 2002 and 2017. However, the age distribution of the change was not uniform. The 25 to 49-year-old population grew just 0.3% over this time, whereas the 50 to 69-year-old population increased 44%, from 54 to 78 million, and the 70-and-over population increased 23%, from 26 to 32 million. All of these population factors increase the marginal damages, by having a larger population, and a larger share of the population in age groups that are more vulnerable to air pollution.
Despite the rising population in the older age groups, the mortality rates in these groups decreased over time. For younger adults, aged 25 to 39, the NCD + LRI mortality rate declined 4% between 2002 and 2017, for middle-aged adults (40 to 49-years-old) the mortality rate declined 16%, for the 50 to 69-year-old age group, the mortality rate declined 9%, and for the oldest age group, 70 and above, the mortality rate declined 17%. The lower the mortality rate, the less vulnerable the population is from exposure to air pollution. Also, mechanically, the calculation of marginal damages uses the baseline, or observed, mortality rates, and thus with a lower mortality rate the marginal damages are lower. It is important to distinguish the impact of the lower mortality rates across age groups. While the 40 to 49-year-old age group and the 70 and above age group showed similar percent reductions in the mortality rate, the mortality rate in the latter group is 30 times that of the former. Therefore, the effect on marginal damages is substantially more influenced by the reduced mortality rate in the oldest populations.
Trends in the other factors, including the spatial distribution of emissions and populations, are more difficult to quantify and must be inferred by the changes in the marginal damages. The overall trends in emissions by pollutant and the category of the source reveal a substantial change in the types of emissions contributing to PM2.5 concentrations. Point-source emissions of SO2 declined 84% from 11.4 to 1.9 million metric tons between 2002 and 2017. NOX emissions from point sources and on-road vehicles declined 63% and 56%, respectively, from 2002 to 2017. Primary PM2.5 emissions from non-point sources declined 28% over this period. Non-point emissions of NH3—which make up 95% of all NH3 emissions—increased 4% between 2002 and 2017. Between 2002 and 2017, substantial reductions from point and on-road sources occurred, but there were smaller reductions or increases in emissions from non-point sources. This resulted in a shift from SO2 and NOX being the overwhelming contributor to PM2.5 concentrations to primary PM2.5 and NH3 being major contributing pollutants.
3.2 Marginal damages
Mean marginal damages of emissions, shown in Fig. 5, in the US increased between 2002 and 2017 for primary PM2.5, SO2, NOX and NH3.Footnote 4 Primary PM2.5 marginal damages increased the most, on average, from $140,000 per ton to $227,000 per ton, a 61% increase. Mean marginal damages of NOX, SO2, and NH3 emissions increased 46%, 36%, and 30%, respectively, between 2002 and 2017.

Marginal damage distribution. Emission-weighted distribution of marginal damages per metric ton, in thousands of 2017$. The blue dot and red line represent the mean and median, respectively. The box represents the interquartile range, and the whiskers extend to the 10th and 90th percentiles
The marginal damages illustrated in Fig. 5 use the uniform VSL across ages. Using either of the age-adjusted VSL measurements substantially reduces marginal damages. For instance, calculating the mean marginal damages of primary PM2.5 emissions in 2017 with the always declining VSLY across ages, were 54% lower than the uniform VSL. The mean marginal damages of primary PM2.5 using the inverted-U VSL were 27% lower than the uniform VSL.
It is expected that the marginal damages are smaller with either of the age-adjusted VSLs, but for our purposes, the interest is in how the marginal damages changed between 2002 and 2017 using these three different VSL measures. Surprisingly, there was almost no difference in the change over time with any of the three VSL measures—that is, the ratio of the marginal damages between 2017 and 2002 was very similar across the uniform and the age-adjusted VSLs. Why was this so? There were substantial changes in the demographics of the US population, with a larger share of the population in the older age groups; however, there were also reductions in the baseline mortality rates, which offset some of the demographic changes. On net, from 2002 to 2017, this led to a slight increase in the share of air-pollution-related mortality in the oldest and middle-age groups, and a slight decrease in the share for the 70–79-year-old age group. The average age of an air-pollution-related death decreased ever so slightly from 73.71 to 73.67 between 2002 and 2017. Thus, using an age-adjusted VSL reduces marginal damages overall compared with a uniform VSL because the VSL is lower for the oldest age groups, but did not change the relative comparison of marginal damages between 2002 and 2017, which is the focus of our analysis. Therefore, the remaining results are all presented using the uniform VSL, noting that all values would be approximately proportionally deflated if an age-adjusted VSL were applied.
The change, spatially, in the marginal damages between 2002 and 2017 is shown in Fig. 6. The largest changes in overall magnitude were from emissions occurring generally near population centers and in the states in the upper south and the mid-Atlantic states. Figure 7 shows the relative changes in marginal damages by location between 2002 and 2017. The smallest relative changes occurred in the Pacific Northwest and the western states in the Midwest. In the states in the upper south, marginal damages doubled or more in many locations between 2002 and 2017.

Change in marginal damages of emissions (in thousands of 2017$ per metric ton) between 2002 and 2017. Each value represents the marginal damages in 2017 minus the marginal damages in 2002 at any particular location (MD2017 – MD2002). The displayed marginal damages are the effect of emissions at any particular location, not the location where the damages are occurring. The marginal damages are from ground-level sources for primary PM2.5, NH3 and NOX, and from high stacks for SO2

Ratio of marginal damages of emissions between 2017 and 2002. Each value represents the marginal damages in 2017 divided by the marginal damages in 2002 at any particular location (MD2017/MD2002). The displayed marginal damages are the effect of emissions at any particular location, not the location where the damages are occurring. The marginal damages are from ground-level sources for primary PM2.5, NH3 and NOX, and from high stacks for SO2
How were these increases in marginal damages affected by each of the key factors discussed above? To evaluate this, a series of counter-factual simulations were run in which all factors were held constant at 2017 levels except one which was set at 2002 levels. The isolated effect of each of these factors on the contribution to changes in mean marginal damages between 2002 and 2017 is illustrated in Fig. 8. To start, the effect of the decrease in PM2.5 concentrations between 2002 and 2017 were examined. With all other factors at 2017 levels (population, age distribution, mortality rates, VSL, and emissions), but PM2.5 concentrations at 2002 levels, the mean marginal damages of emissions were 21–23% less than the actual 2017 marginal damages. Thus, the 36% decrease in PM2.5 concentrations between 2002 and 2017, increased the marginal damages of emissions by approximately 22% (see teal bars in Fig. 8). This increase is the isolated effect of how lowered PM2.5 concentrations increased the marginal risk reduction of pollution abatement, as illustrated by the GEMM C-R response function in Fig. 2. Rather than reducing marginal damages of emissions as environmental quality improves substantially, our calculations here, when using the GEMM functions, indicates that the shape of the C-R function is an essential factor in increasing the marginal benefits of additional abatement.

Change in mean marginal damages by pollutant between 2002 and 2017, separated by contributing factor. Vertical black lines represent marginal damages (MD) in 2002 and 2017. The horizontal distance of colored blocks represents the change due to the specified factor: VSL (green), change in adult population totals and age distribution (yellow), change in PM2.5 concentration (teal), change in emission quantity and spatial distribution (pink), change in mortality rates (blue), all other unspecified factors (gray). Arrows pointing right (left) represent an increase (decrease) between 2002 and 2017 marginal damages due to the factor
Another important factor in the changes in marginal damages of emissions were the demographic trends. Simulating marginal damages with the total population and age distribution at 2002 levels, but all other factors at 2017 levels, led to a 19–22% reduction in marginal damages of emissions compared with the actual 2017 estimates. Thus, marginal damages would be approximately 20% lower than they were in 2017 if there were no changes in the population size or makeup since 2002 (see yellow bars in Fig. 8). This combines the effect of the 16% increase in the adult population and the larger share of the population over 50 years old. The growing population, with a larger share more vulnerable to the effects of air pollution, increases the marginal benefit of reducing additional emissions.
Along with the population changes, there were substantial reductions in the age-specific mortality rates. If five-year age-group mortality rates stayed at their elevated 2002 levels, but all other factors were kept at 2017 levels, the marginal damages of emissions would be 17–20% higher than the actual 2017 estimates. Without the substantial improvement in the adult population health between 2002 and 2017, marginal damages would be substantially higher in 2017 (see blue bars in Fig. 8). The population is somewhat less vulnerable to air pollution because of these reduced mortality rates, lessening the marginal benefit of additional emission reductions.
Rising mean income in the US led to an increased value of avoiding mortality risks. If the VSL had remained unchanged at the 2002 level, but all other factors were at 2017 levels, then the marginal damages would be 9% less than the actual 2017 estimates (see green bars in Fig. 8).
Lastly, the effect of the changes in the spatial distribution of emissions was isolated. When the quantity and spatial location of emissions were at 2002 levels, but all other factors were held at their 2017 levels, the effect is mixed on the marginal damages of emissions. Mean marginal damages of SO2, NH3, and NOX would be 16%, 14%, and 5% higher than the actual 2017 values if emissions remained unchanged at 2002 levels and locations. Thus, the spatial distribution of emissions of these three pollutants changed between 2002 and 2017 to make their marginal impact less harmful (see pink bars in Fig. 8). This is likely the result of disproportionate emission reductions from sources nearer to larger population centers. Conversely, the marginal damages of primary PM2.5 emissions were 11% less in this simulation compared with the actual 2017 values. This indicates that 2017 primary PM2.5 emission sources were more harmful due to the spatial distribution compared with emissions in 2002.
Overall, reduced PM2.5 concentrations, increased population with a larger share in the oldest age groups, and an increased VSL contributed to a 30–60% increase in the marginal damages of emissions.
4 Conclusion
Substantial progress was made in air quality in the US over the past several decades. Rather than see this issue as largely resolved, our analysis here indicate that there is ample opportunity to further improve health through air pollution reductions. In fact, a large part of this opportunity is attributable to the reduction in PM2.5 concentrations, as this raises the marginal risk reduction from additional improvements. The increased marginal damages raise the possibility that additional emission reductions could yield positive net benefits.
Even supposing that the marginal benefits of abatement exceeded marginal abatement costs for previous emission reductions, the marginal abatement costs could be many times greater for additional reductions. This may be especially true for abatement from large point sources of SO2 and NOX, which reduced an enormous share of their emissions in the past 20 years. However, other sources—such as agricultural emissions of NH3, and other pollutants from non-point sources—did not reduce emissions to nearly the same degree. While these sources may prove more difficult to regulate, there is the potential for large gains in welfare from a focus on reducing emissions from these sources.
Notes
While there are large quantities of VOC emissions, the marginal damages of VOCs are generally substantially lower per unit of mass than emissions of the other four pollutants, and thus make up a relatively small share of total damages from PM2.5 air pollution—by one estimate, VOC emissions were responsible for 11.6% of total PM2.5 air pollution damages in 2011 (Goodkind et al. 2019).
All populations and mortality rates are age-group specific, which is suppressed here for simplicity.
The baseline VSL measure used in this analysis is a uniform VSL applied to all populations. Two additional VSL measurements which are age adjusted were also evaluated.
All means are weighted by the quantity of emissions at each source.
References
Aldy JE, Viscusi WK (2008) Adjusting the value of a statistical life for age and cohort effects. Rev Econ Stat 90(3):573–581. https://doi.org/10.1162/rest.90.3.573
Arias E, Xu J (2019) United States Life Tables. Natl Health Stat Report 68(7):1–65
Burkhardt J, Bayham J, Wilson A, Carter E, Berman JD, O’Dell K, Ford B, Fischer EV, Pierce JR (2019) The effect of pollution on crime: Evidence from data on particulate matter and ozone. J Environ Econ Manag 98:102267. https://doi.org/10.1016/j.jeem.2019.102267
Burnett R, Chen H, Szyszkowicz M et al (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. P Natl Acad Sci USA 115:9592–9597. https://doi.org/10.1073/pnas.1803222115
Burnett RT, Pope CA III, Ezzati M et al (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Persp 122(4):397–403. https://doi.org/10.1289/ehp.1307049
Centers for Disease Control and Prevention, National Center for Health Statistics (2020) Underlying Cause of Death 1999–2019 on CDC WONDER Online Database. Data are from the Multiple Cause of Death Files, 1999–2019, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Accessed at http://wonder.cdc.gov/ucd-icd10.html on Nov 22, 2021
Centers for Disease Control and Prevention, National Center for Health Statistics (2017) NCHS Urban-Rural Classification Scheme for Counties. Accessed at https://www.cdc.gov/nchs/data_access/urban_rural.htm on April 11, 2023
Christidis T, Erickson AC, Pappin AJ et al (2019) Low concentrations of fine particle air pollution and mortality in the Canadian Community Health Survey cohort. Environ Health 18:84. https://doi.org/10.1186/s12940-019-0518-y
Crouse DL, Peters PA, van Donkelaar A et al (2012) Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ Health Persp 120(5):708–714. https://doi.org/10.1289/ehp.1104049
Currie J, Walker R (2011) Traffic congestion and infant health: Evidence from E-ZPass. Am Econ J-Appl Econ 3(1):65–90. https://doi.org/10.1257/app.3.1.65
Deryugina T, Heutel G, Miller NH, Molitor D, Reif J (2019) The mortality and medical costs of air pollution: Evidence from changes in wind direction. Am Econ Rev 109(12):4178–4219. https://doi.org/10.1257/aer.20180279
Evans MF, Smith VK (2006) Do we really understand the age-VSL relationship? Resour Energy Econ 28:242–261. https://doi.org/10.1016/j.reseneeco.2006.02.004
Gong Y, Li S, Sanders NJ, Shi G (2023) The mortality impact of fine particulate matter in China: Evidence from trade shocks. J Environ Econ Manag 117:102759. https://doi.org/10.1016/j.jeem.2022.102759
Goodkind AL, Tessum CW, Coggins JS, Hill JD, Marshall JD (2019) Fine-scale damage estimates of particulate matter air pollution reveal opportunities for location-specific mitigation of emissions. P Natl Acad Sci USA 116(18):8775–8780. https://doi.org/10.1073/pnas.1816102116
Knittel CR, Miller DL, Sanders NJ (2016) Caution, Drivers! Children present: Traffic, pollution, and infant health. Rev Econ Stat 98(2):350–366. https://doi.org/10.1162/REST_a_00548
Krewski D, Jerrett M, Burnett RT et al (2009) Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. Health Effects Institute, Boston 140:5–114
Lepeule J, Laden F, Dockery D, Schwartz J (2012) Chronic exposure to fine particles and mortality: An extended follow-up of the Harvard Six Cities Study from 1974 to 2009. Environ Health Persp 120(7):965–970. https://doi.org/10.1289/ehp.1104660
Manson S, Schroeder J, Van Riper D, Kugler T, Ruggles S (2021) IPUMS National Historical Geographic Information System: Version 16.0. IPUMS, Minneapolis. https://doi.org/10.18128/D050.V16.0
Muller NZ, Mendelsohn R (2007) Measuring the damages of air pollution in the United States. J Environ Econ Manag 54(1):1–14. https://doi.org/10.1016/j.jeem.2006.12.002
Pope CA III, Burnett RT, Turner MC, Cohen A, Krewski D, Jerrett M, Gapstur SM, Thun MJ (2011) Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: Shape of the exposure-response relationships. Environ Health Persp 119(11):1616–1621. https://doi.org/10.1289/ehp.1103639
Robinson LA, Sullivan R, Shogren JF (2021) Do the benefits of COVID-19 policies exceed the Costs? Exploring uncertainties in the age-VSL relationship. Risk Anal 41(5):761–770. https://doi.org/10.1111/risa.13561
Schlenker W, Walker WR (2016) Airports, air pollution, and contemporaneous health. Rev Econ Stud 83:768–809. https://doi.org/10.1093/restud/rdv043
Shumake KL, Sacks JD, Lee JS, Johns DO (2013) Susceptibility of older adults to health effects induced by ambient air pollutants regulated by the European Union and the United States. Aging Clin Exp Res 25:3–8. https://doi.org/10.1007/s40520-013-0001-5
Stafford TM (2015) Indoor air quality and academic performance. J Environ Econ Manag 70:34–50. https://doi.org/10.1016/j.jeem.2014.11.002
Tessum CW, Hill JD, Marshall JD (2017) InMAP: A model for air pollution interventions. PLoS ONE 12:e0176131. https://doi.org/10.1371/journal.pone.0176131
Thurston GD, Ahn J, Cromar KR, Shao Y, Reynolds HR, Jerrett M, Lim CC, Shanley R, Park Y, Hayes RB (2016) Ambient particulate matter air pollution exposure and mortality in the NIH-AARP Diet and Health cohort. Environ Health Persp 124(4):484–490. https://doi.org/10.1289/ehp.1509676
Turner MC, Jerrett M, Pope AC III et al (2016) Long-term ozone exposure and mortality in a large prospective study. Am J Resp Crit Care 193(10):1134–1142. https://doi.org/10.1164/rccm.201508-1633OC
US Bureau of Economic Analysis (2022) Real gross domestic product per capita [A939RX0Q048SBEA]. Retrieved from Federal Reserve Bank of St. Louis, June 8, 2022. https://fred.stlouisfed.org/series/A939RX0Q048SBEA
US Environmental Protection Agency (2022a) Air Pollutant Emission Trends Data. https://www.epa.gov/air-emissions-inventories/air-pollutant-emissions-trends-data
US Environmental Protection Agency (2022b) Particulate Matter (PM2.5) Trends. https://www.epa.gov/air-trends/particulate-matter-pm25-trends
US Environmental Protection Agency (2021a) Particulate Matter (PM) Basics. https://www.epa.gov/pm-pollution/particulate-matter-pm-basics#PM
US Environmental Protection Agency (2021b) 2017 National Emissions Inventory: January 2021 Update Release, Technical Support Document. Office of Air Quality Planning and Standards, Research Triangle Park EPA-454/R-21–001. https://www.epa.gov/air-emissions-inventories/national-emissions-inventory-nei
US Environmental Protection Agency (2013) Regulatory Impact Analysis for the Final Revisions to the National Ambient Air Quality Standards for Particulate Matter. Office of Air Quality Planning and Standards, Research Triangle Park EPA-452/R-12–005. https://www3.epa.gov/ttnecas1/regdata/RIAs/finalria.pdf
US Environmental Protection Agency (2011) Regulatory Impact Analysis for the Final Mercury and Air Toxics Standards. Office of Air Quality Planning and Standards, Research Triangle Park EPA-452/R-11–011. https://www3.epa.gov/ttnecas1/regdata/RIAs/matsriafinal.pdf
US Environmental Protection Agency (2010) Guidelines for Preparing Economic Analyses. National Center for Environmental Economics EPA-240/R-10–001. https://www.epa.gov/sites/default/files/2017-08/documents/ee-0568-50.pdf
van Donkelaar A, Hammer MS, Bindle L et al (2021) Monthly global estimates of fine particulate matter and their uncertainty. Environ Sci Technol 55(22):15287–15300. https://doi.org/10.1021/acs.est.1c05309
Vodonos A, Awad YA, Schwartz J (2018) The concentration-response between long-term PM2.5 exposure and mortality; A meta-regression approach. Environ Res 166:677–689. https://doi.org/10.1016/j.envres.2018.06.021
Yin H, Brauer M, Zhang J et al (2021) Population ageing and deaths attributa. Lancet Planet Health 5(6):E356–E367. https://doi.org/10.1016/S2542-5196(21)00131-5
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
1.1 CDC codes
The following items were included from ICD-10 113 cause list as a representation of non-communicable diseases plus lower-respiratory infections for use with the GEMM C-R function (CDC 2020).
-
Malignant neoplasms (C00-C97)
-
In situ neoplasms, benign neoplasms and neoplasms of uncertain or unknown behavior (D00-D48)
-
Anemias (D50-D64)
-
Diabetes mellitus (E10-E14)
-
Nutritional deficiencies (E40-E64)
-
Meningitis (G00,G03)
-
Parkinson disease (G20-G21)
-
Alzheimer disease (G30)
-
Major cardiovascular diseases (I00-I78); Other disorders of circulatory system (I80-I99)
-
Influenza and pneumonia (J09-J18)
-
Other acute lower respiratory infections (J20-J22,U04)
-
Chronic lower respiratory diseases (J40-J47)
-
Pneumoconioses and chemical effects (J60-J66,J68,U07.0)
-
Pneumonitis due to solids and liquids (J69)
-
Other diseases of respiratory system (J00-J06,J30- J39,J67,J70-J98)
-
Peptic ulcer (K25-K28)
-
Diseases of appendix (K35-K38)
-
Hernia (K40-K46)
-
Chronic liver disease and cirrhosis (K70,K73-K74)
-
Cholelithiasis and other disorders of gallbladder (K80-K82)
-
Nephritis, nephrotic syndrome and nephrosis (N00-N07,N17-N19,N25-N27)
-
Infections of kidney (N10-N12,N13.6,N15.1)
-
Hyperplasia of prostate (N40)
-
Inflammatory diseases of female pelvic organs (N70-N76)
-
All other diseases (Residual)
1.2 PM2.5 concentration maps

Source: van Donkelaar et al. (2021) and Author’s calculations
PM2.5 concentrations (µg m−3) by year.
1.3 VSL measurements
1.4 Emission totals by category
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Goodkind, A.L. Increased Marginal Damages of Air Emissions Following Improvements in Air Quality in the United States. Environ Resource Econ 87, 1761–1782 (2024). https://doi.org/10.1007/s10640-024-00871-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10640-024-00871-0