
Summary
Background Tipifarnib is an orally active, competitive inhibitor of farnesyltransferase which has shown encouraging signs of activity either alone or when combined with other agents. Clinical studies of tipifarnib in combination with anti-estrogen therapy have yielded disappointing results. In contrast, tipifarnib appears to be synergistic in combination with anthracycline based chemotherapy. Here we report the results of the first prospective phase II trial evaluating the efficacy of the novel combination of tipifarnib and gemcitabine in the treatment of metastatic breast cancer. Patients and Methods 30 postmenopausal women with metastatic breast cancer were treated on a 21-day cycle with tipifarnib 300 mg PO twice daily from days 1 through 14. Gemcitabine was administered intravenously at a dose of 1000 mg/m2 on days 1 and 8. Patients were treated until disease progression or unacceptable toxicity. Results There was one complete response and four partial responses yielding an objective response rate of 16.7%. Median progression-free survival and overall survival was 2.5 months (95% confidence interval: 1.6–5.7 months) and 13.1 months (95% confidence interval: 9.1–20.6 months), respectively. 40% of patients experienced grade 4 neutropenia in this study. Conclusion The combination of tipifarnib and gemcitabine is not well tolerated with high rates of myelosuppression and is not more effective than gemcitabine monotherapy in the treatment of metastatic breast cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tipifarnib is a non-peptidomimetic, orally active, competitive inhibitor of farnesyltransferase [1]. Inhibition of farnesyltransferase interferes with post-translational modification of Ras [2] and has been shown to inhibit tumor cell growth in multiple preclinical studies [1, 3,4,5,6,7,8,9]. Aberrant signaling in the Ras pathway secondary to enhanced upstream growth factor receptor activation has been implicated in the development human breast cancer [10]. It is therefore not surprising that tipifarnib has shown promising preclinical signs of activity in breast cancer, either alone [3, 5] or in combination with other agents including tamoxifen [7, 8], taxanes [4, 6] and novel agents like AKT inhibitors [9].
Encouraging signs of clinical activity were seen in a phase II study evaluating two different dosing schedules of tipifarnib in patients with advanced breast cancer [11]. However, clinical studies of tipifarnib in combination with other agents in breast cancer have brought mixed results. A phase II trial of tipifarnib plus fulvestrant in metastatic breast cancer reported a clinical benefit rate (CBR) of 48% in aromatase inhibitor resistant disease [12] which compared favorably with the 30–35% CBR reported with fulvestrant alone in prior studies [13,14,15,16]. However, the trial did not meet its primary end-point. Several other phase II studies evaluated the role of tipifarnib in advanced breast cancer in combination with anti-estrogen therapy [17, 18] or capecitabine [19] with disappointing results. In contrast, two phase I-II studies of tipifarnib with anthracycline based chemotherapy in locally advanced breast cancer showed promising signs of activity in the neoadjuvant setting [20, 21].
Gemcitabine is commonly used in metastatic breast cancer and has demonstrated activity either as a single agent [22, 23] or in combination with taxanes [24, 25], and preclinical studies have demonstrated that the combination of gemcitabine and farnesyltransferase inhibitors results in additive cytotoxicity [26,27,28]. Although not previously evaluated specifically in the setting of metastatic breast cancer, the combination of gemcitabine plus tipifarnib was previously shown to be tolerable in a phase I trial of patients with advanced malignancies [29] and a phase III trial in patients with advanced pancreatic cancer [30].
Based on this background and rationale, we conducted a single-institution prospective phase II study to determine the efficacy of the combination of tipifarnib and gemcitabine in patients with metastatic breast cancer.
Methods
Eligibility
Patients were eligible for the study if they were at least 18 years of age at the time of study enrollment and had histologically confirmed breast cancer with clinical evidence of metastatic disease.
There were no restrictions placed on prior treatment with hormonal therapies or trastuzumab. Patients could have received up to two prior lines of systemic chemotherapy for metastatic breast cancer. Concurrent bisphosphonate use was allowed in patients with bone metastases. Localized radiotherapy deemed not to influence the signal of the evaluable lesion was allowed prior to the initiation of therapy as long as recovery from myelosuppression was documented. Patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of two or better as well as adequate organ and marrow function.
Patients were excluded if they had prior treatment with a farnesyltransferase inhibitor or gemcitabine for metastatic breast cancer. Patients with metastatic disease involving the central nervous system (CNS) or symptomatic lymphangitic pulmonary metastases were excluded. Patients with grade 2 or greater peripheral neuropathy were also excluded from the study.
The protocol was reviewed by The University of Texas MD Anderson Cancer Center Institutional Review Board and all patients provided informed consent.
Study design and treatment
The primary objective of this single-institution prospective phase II trial was to evaluate the efficacy of the combination of gemcitabine and the farnesyltransferase inhibitor, tipifarnib (R115777) in patients with metastatic breast cancer. Treatment was administered over a 21-day cycle. For the first three patients, the starting dose of tipifarnib (R115777) was 300 mg twice daily from days 1 through 14. Gemcitabine was administered intravenously at a dose of 1000 mg/m2 on days 1 and 8. If one or no patient developed a dose limiting toxicity (DLT) in the first cycle of treatment, tipifarnib (R115777) 300 mg twice daily would be used for subsequent patients enrolled in the study.
For this study, DLTs were defined as any grade 3 or greater non-hematological toxicities not resolving by day 21 with the exception of grade 3 nausea or vomiting. Grade 4 nausea or vomiting which did not resolve by day 21 was considered a DLT. Grade 4 neutropenia or thrombocytopenia at day 21, grade 3 neutropenia with a documented infection and/or fever, and grade 3 thrombocytopenia with bleeding were also considered DLTs.
Evaluations before and during treatment consisted of a complete medical history, physical examinations, hematologic and metabolic profiles, relevant imaging studies and toxicity assessments. Patients remained on study until radiographic or clinical disease progression, unacceptable toxicity, or withdrawal of consent. All patients were provided with full supportive care during the study.
Safety monitoring and dose modifications
Patients were evaluated for toxicity while on study from the time of first treatment with tipifarnib (R115777). Severity was graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events (NCI CTCAE), version 3.0.
All patients were required to have an absolute neutrophil count (ANC) of 1500 cells/mm3 or greater, platelet count of 100,000/mm3 or greater, and resolution of non-hematological toxicities to grade 2 or less at the beginning of each cycle. Otherwise, treatment was held. If treatment was held for longer than 2 weeks, the dose of gemcitabine was reduced to the next dose level according to the protocol specified dose schedule. Patients requiring more than 2 dose reductions were removed from study.
Grade 2 thrombocytopenia and/or grade 3 neutropenia present on day 8 was an indication for a 50% dose reduction in gemcitabine. The day 8 dose of gemcitabine was held for grade 3 or greater thrombocytopenia and grade 4 neutropenia.
Grade 2 or greater pneumonitis thought to be related to gemcitabine was an indication for removal from protocol treatment.
Disease monitoring
All patients included in the study were evaluated for disease response or progression with appropriate cross sectional imaging studies at baseline and every six weeks. Complete response (CR), partial response (PR), stable disease (SD) and progressive disease (PD) were defined and assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.0. All CRs and PRs required confirmation by repeat assessments at least 4 weeks after the initial criteria for response was met. All responses were reviewed by an independent radiology expert at the time of study completion.
Statistical methods
The planned enrollment for this study was up to 45 patients. The sample size of 45 would have provided an estimate of the objective response rate (ORR) with a 90% credibility interval of width 0.22, assuming a targeted rate of 30%. The trial was monitored using a Bayesian method with cohorts of 15 patients each. Termination was to be recommended if there was strong evidence that the ORR was unlikely to be more than 30%. The first interim analysis was conducted after the first 15 patients were evaluated for response. If at least two responses were observed, accrual would continue. At the second interim analysis (30 patients), at least six objective responses were required for continued accrual. 95% confidence intervals for proportions were calculated using the exact binomial method. Progression-free survival (PFS) was defined as the time from study registration to disease progression or death from any cause, whichever occurred first. PFS data were censored at the time of removal from study. Overall survival (OS) was defined as the time from study registration to death from any cause. Information on vital status was collected following study completion through October 8, 2017 and was used in the determination of OS. For patients who had a confirmed objective response (PR or CR), duration of response was defined as the time from the initial documentation of response to the time of progression. Data on duration of response was censored at the time of study exit. Median PFS, OS and duration of response were estimated using the Kaplan-Meier method. All data were analyzed using STATA v14.0 (STATA, College Station, TX).
Results
Patients
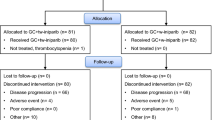
Thirty female patients were enrolled on this study from September 2005 through March 2007 and treated at The University of Texas MD Anderson Cancer Center. All patients received at least one dose of the study treatment and were considered evaluable for toxicity and response. Baseline patient characteristics are summarized in Table 1. The median age was 55.1 years (range 37.8–73.8 years). 60% (18/30) of patients had an ECOG performance status of 0. 50% (15/30) were white and 33% (10/30) were black. 70% (21/30) and 47% (14/30) of patients had received prior chemotherapy and hormonal therapy in the metastatic setting, respectively. A majority of patients (57%) had ER- and/or PR-positive disease and only 10% of patients had HER2-positive disease.
Efficacy
Accrual was terminated after the first 30 patients were enrolled because only five confirmed responses were observed. Patients who were already enrolled continued to receive therapy per protocol until progression, unacceptable toxicity or withdrawal of consent. Table 2 summarizes the outcomes of patients treated on this protocol. There was one confirmed CR and four patients had a confirmed PR, yielding an ORR of 16.7% (95% confidence interval [CI]: 5.6–34.7%). 23.3% (95% CI: 9.9–42.3%) of patients on this study had stable disease. The single patient with the confirmed CR had triple negative breast cancer. Among the four patients with confirmed PRs, two had ER-positive/HER2-negative breast cancer, one had ER-positive/HER2-positive breast cancer, and one had triple negative breast cancer. Table 3 summarizes the pretreatment characteristics of patients stratified by best overall response. 80% (4/5) of patients with confirmed responses (CR or PR) and 59% (13/22) of patients with a best response of SD or PD had ER- and/or PR-positive disease. 40% (2/5) of patients with confirmed responses (CR or PR) and 73% (16/22) of patients with a best response of SD or PD had received prior chemotherapy in the metastatic setting. The median PFS was 2.5 months (95% CI: 1.6–5.7 months, Fig. 1). The median OS was 13.1 months (95% CI: 9.1–20.6 months, Fig. 2). Among the 5 patients with confirmed objective responses (CR or PR), the median duration of response was 4.2 months (95% CI: 2.8-undefined months).

Kaplan-Meier Estimation of Progression-Free Survival (PFS). A Kaplan-Meier plot of PFS is shown. The median PFS for patients on this study was 2.5 months (95% confidence interval: 1.6–5.7 months)

Kaplan-Meier Estimation of Overall Survival (OS). A Kaplan-Meier plot of OS is shown. The median OS for patients on this study was 13.1 months (95% confidence interval: 9.1–20.6 months)
Toxicity
All 30 treated patients on this protocol were assessable for toxicity. There were no treatment related deaths. None of the first three patients developed a DLT. Table 4 summarizes the grade 2 and greater toxicities observed in this study thought to be possibly, probably or definitely related to the study treatment. Neutropenia was the most common grade 4 toxicity, occurring in 40% of treated patients. Other grade 4 toxicities included leukopenia (13%), thrombocytopenia (10%), anemia (3%) and hypokalemia (3%). Common grade 3 toxicities observed in this study include fatigue (57%), leukopenia (33%) and neutropenia (27%). Nausea was the most common grade 2 toxicity observed (63%).
Discussion
This is the first phase II trial to report on the combination of tipifarnib and gemcitabine in the treatment of metastatic breast cancer. The ORR in this study was 16.7%, which is not an improvement from the reported response rate of 16%–30% with gemcitabine monotherapy in patients with metastatic breast cancer [22, 31,32,33,34]. However, our reported response rate is slightly better compared to the 10–14% response rate reported in the single agent phase II study of tipifarnib [11] and the 9.5% response rate reported by a phase II study evaluating the combination of tipifarnib and capecitabine [19]. Additionally, we observed that 80% of patients with confirmed responses on this study had ER- and/or PR-positive disease. In contrast, only 59% of patients with a best response of SD or PD had ER- and/or PR-positive disease. Further, patients with confirmed responses in our study appeared less likely to have received prior treatment with chemotherapy in the metastatic setting (40% vs 73% in patients with a best response of SD or PD).
Although our reported ORR of 16.7% appears to be less favorable compared to two phase II trials evaluating the combination of tipifarnib and anti-estrogen therapy in the metastatic setting which reported response rates of 30–35.5% [12, 17], it is important to note that these trials were restricted to patients with ER- and/or PR-positive disease and either excluded patients who had received prior chemotherapy in the metastatic setting [12] or limited enrollment to patients who received one or less lines of chemotherapy [17]. In contrast, 43% of patients enrolled in our study had ER/PR-negative disease and 70% of patients in our study had received prior chemotherapy for metastatic disease, majority of whom received two prior lines of chemotherapy. Of note, preclinical studies showed that ER/PR-negative breast cancer cell lines (MDA-MB-231, MDA-MB-468) were less sensitive to tipifarnib-induced growth inhibition as compared to an ER/PR-positive breast cancer cell line (MCF-7) [9]. In clinical studies of metastatic breast cancer, response rates to gemcitabine appear to decrease with increasing number of lines of prior chemotherapy [23, 33]. Thus, we hypothesize that the comparatively lower response rate observed in our study was due, in part, to the inclusion of patients with ER/PR-negative disease and patients who were more heavily pre-treated. Although limited by small numbers, patients with confirmed responses in our study appeared more likely to have ER- and/or PR-positive disease and be less heavily pre-treated, further supporting our hypothesis. Interestingly, a phase II trial evaluating the combination of tipifarnib and tamoxifen, which included heavily pre-treated patients, reported an ORR of just 5% [18].
The combination of tipifarnib and gemcitabine resulted in significant myelosuppression with 40% of patients developing grade 4 neutropenia and 10% developing grade 4 thrombocytopenia. Myelosuppression was also the principal toxicity reported in the phase I study evaluating the combination of tipifarnib and gemcitabine [29]. However, only 18% of patients in the phase I study experienced grade 3 or grade 4 neutropenia likely because of the lower doses of tipifarnib used in patients enrolled in the earlier dose-escalation cohorts. In contrast, gemcitabine is well tolerated as a single agent in metastatic breast cancer with only 0–2% of patients experiencing grade 4 neutropenia, anemia or thrombocytopenia [22, 32].
There are several possible explanations for the low response rate observed in this study. First, tipifarnib might not be a suitable agent to use in combination with gemcitabine. The high rates of myelosuppression led to dose reductions and/or interruptions which may have affected the efficacy of the combination. Second, the inclusion of patients with ER- and/or PR-negative disease and heavily pre-treated patients in our study may have contributed to the lower response rate. Third, our heterogeneous patient cohort might have diluted the potential efficacy of the combination in specific subgroups of patients. Despite the lack of added efficacy achieved by combining tipifarnib with gemcitabine, tipifarnib has shown promise in the neoadjuvant setting in combination with anthracyclines and taxanes [20, 21, 35].
In conclusion, this phase II study suggests that the combination of tipifarnib and gemcitabine is not well tolerated with high rates of myelosuppression and is not more effective than gemcitabine monotherapy in the treatment of metastatic breast cancer. Combinations of tipifarnib with agents other than gemcitabine should be explored if supported by pre-clinical data.
References
End DW, Smets G, Todd AV, Applegate TL, Fuery CJ, Angibaud P, Venet M, Sanz G, Poignet H, Skrzat S, Devine A, Wouters W, Bowden C (2001) Characterization of the antitumor effects of the selective farnesyl protein transferase inhibitor R115777 in vivo and in vitro. Cancer Res 61(1):131–137
Kato K, Cox AD, Hisaka MM, Graham SM, Buss JE, Der CJ (1992) Isoprenoid addition to Ras protein is the critical modification for its membrane association and transforming activity. Proc Natl Acad Sci U S A 89(14):6403–6407
Kelland LR, Smith V, Valenti M, Patterson L, Clarke PA, Detre S, End D, Howes AJ, Dowsett M, Workman P, Johnston SR (2001) Preclinical antitumor activity and pharmacodynamic studies with the farnesyl protein transferase inhibitor R115777 in human breast cancer. Clin Cancer Res 7(11):3544–3550
Izbicka E, Campos D, Carrizales G, Patnaik A (2005) Biomarkers of anticancer activity of R115777 (Tipifarnib, Zarnestra) in human breast cancer models in vitro. Anticancer Res 25(5):3215–3223
Warnberg F, White D, Anderson E, Knox F, Clarke RB, Morris J, Bundred NJ (2006) Effect of a farnesyl transferase inhibitor (R115777) on ductal carcinoma in situ of the breast in a human xenograft model and on breast and ovarian cancer cell growth in vitro and in vivo. Breast Cancer Res 8(2):R21. https://doi.org/10.1186/bcr1395
Caraglia M, Giuberti G, Marra M, Di Gennaro E, Facchini G, Caponigro F, Iaffaioli R, Budillon A, Abbruzzese A (2005) Docetaxel induces p53-dependent apoptosis and synergizes with farnesyl transferase inhibitor r115777 in human epithelial cancer cells. Front Biosci 10:2566–2575
Dalenc F, Giamarchi C, Petit M, Poirot M, Favre G, Faye JC (2005) Farnesyl-transferase inhibitor R115,777 enhances tamoxifen inhibition of MCF-7 cell growth through estrogen receptor dependent and independent pathways. Breast Cancer Res 7(6):R1159–R1167. https://doi.org/10.1186/bcr1357
Martin LA, Head JE, Pancholi S, Salter J, Quinn E, Detre S, Kaye S, Howes A, Dowsett M, Johnston SR (2007) The farnesyltransferase inhibitor R115777 (tipifarnib) in combination with tamoxifen acts synergistically to inhibit MCF-7 breast cancer cell proliferation and cell cycle progression in vitro and in vivo. Mol Cancer Ther 6(9):2458–2467. https://doi.org/10.1158/1535-7163.MCT-06-0452
Balasis ME, Forinash KD, Chen YA, Fulp WJ, Coppola D, Hamilton AD, Cheng JQ, Sebti SM (2011) Combination of farnesyltransferase and Akt inhibitors is synergistic in breast cancer cells and causes significant breast tumor regression in ErbB2 transgenic mice. Clin Cancer Res 17(9):2852–2862. https://doi.org/10.1158/1078-0432.CCR-10-2544
Clark GJ, Der CJ (1995) Aberrant function of the Ras signal transduction pathway in human breast cancer. Breast Cancer Res Treat 35(1):133–144
Johnston SR, Hickish T, Ellis P, Houston S, Kelland L, Dowsett M, Salter J, Michiels B, Perez-Ruixo JJ, Palmer P, Howes A (2003) Phase II study of the efficacy and tolerability of two dosing regimens of the farnesyl transferase inhibitor, R115777, in advanced breast cancer. J Clin Oncol 21(13):2492–2499. https://doi.org/10.1200/JCO.2003.10.064
Li T, Christos PJ, Sparano JA, Hershman DL, Hoschander S, O'Brien K, Wright JJ, Vahdat LT (2009) Phase II trial of the farnesyltransferase inhibitor tipifarnib plus fulvestrant in hormone receptor-positive metastatic breast cancer: New York cancer consortium trial P6205. Ann Oncol 20(4):642–647. https://doi.org/10.1093/annonc/mdn689
Dodwell D, Vergote I (2005) A comparison of fulvestrant and the third-generation aromatase inhibitors in the second-line treatment of postmenopausal women with advanced breast cancer. Cancer Treat Rev 31(4):274–282. https://doi.org/10.1016/j.ctrv.2005.03.009
Ingle JN, Suman VJ, Rowland KM, Mirchandani D, Bernath AM, Camoriano JK, Fishkin PA, Nikcevich DA, Perez EA, North Central Cancer Treatment Group Trial N (2006) Fulvestrant in women with advanced breast cancer after progression on prior aromatase inhibitor therapy: north central cancer treatment group trial N0032. J Clin Oncol 24(7):1052–1056. https://doi.org/10.1200/JCO.2005.04.1053
Perey L, Paridaens R, Hawle H, Zaman K, Nole F, Wildiers H, Fiche M, Dietrich D, Clement P, Koberle D, Goldhirsch A, Thurlimann B (2007) Clinical benefit of fulvestrant in postmenopausal women with advanced breast cancer and primary or acquired resistance to aromatase inhibitors: final results of phase II Swiss Group for Clinical Cancer Research Trial (SAKK 21/00). Ann Oncol 18(1):64–69. https://doi.org/10.1093/annonc/mdl341
Chia S, Gradishar W, Mauriac L, Bines J, Amant F, Federico M, Fein L, Romieu G, Buzdar A, Robertson JF, Brufsky A, Possinger K, Rennie P, Sapunar F, Lowe E, Piccart M (2008) Double-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECT. J Clin Oncol 26(10):1664–1670. https://doi.org/10.1200/JCO.2007.13.5822
Johnston SR, Semiglazov VF, Manikhas GM, Spaeth D, Romieu G, Dodwell DJ, Wardley AM, Neven P, Bessems A, Park YC, De Porre PM, Perez Ruixo JJ, Howes AJ (2008) A phase II, randomized, blinded study of the farnesyltransferase inhibitor tipifarnib combined with letrozole in the treatment of advanced breast cancer after antiestrogen therapy. Breast Cancer Res Treat 110(2):327–335. https://doi.org/10.1007/s10549-007-9726-1
Dalenc F, Doisneau-Sixou SF, Allal BC, Marsili S, Lauwers-Cances V, Chaoui K, Schiltz O, Monsarrat B, Filleron T, Renee N, Malissein E, Meunier E, Favre G, Roche H (2010) Tipifarnib plus tamoxifen in tamoxifen-resistant metastatic breast cancer: a negative phase II and screening of potential therapeutic markers by proteomic analysis. Clin Cancer Res 16(4):1264–1271. https://doi.org/10.1158/1078-0432.CCR-09-1192
Li T, Guo M, Gradishar WJ, Sparano JA, Perez EA, Wang M, Sledge GW (2012) A phase II trial of capecitabine in combination with the farnesyltransferase inhibitor tipifarnib in patients with anthracycline-treated and taxane-resistant metastatic breast cancer: an eastern cooperative oncology group study (E1103). Breast Cancer Res Treat 134(1):345–352. https://doi.org/10.1007/s10549-012-2071-z
Andreopoulou E, Vigoda IS, Valero V, Hershman DL, Raptis G, Vahdat LT, Han HS, Wright JJ, Pellegrino CM, Cristofanilli M, Alvarez RH, Fehn K, Fineberg S, Sparano JA (2013) Phase I-II study of the farnesyl transferase inhibitor tipifarnib plus sequential weekly paclitaxel and doxorubicin-cyclophosphamide in HER2/neu-negative inflammatory carcinoma and non-inflammatory estrogen receptor-positive breast carcinoma. Breast Cancer Res Treat 141(3):429–435. https://doi.org/10.1007/s10549-013-2704-x
Sparano JA, Moulder S, Kazi A, Coppola D, Negassa A, Vahdat L, Li T, Pellegrino C, Fineberg S, Munster P, Malafa M, Lee D, Hoschander S, Hopkins U, Hershman D, Wright JJ, Kleer C, Merajver S, Sebti SM (2009) Phase II trial of tipifarnib plus neoadjuvant doxorubicin-cyclophosphamide in patients with clinical stage IIB-IIIC breast cancer. Clin Cancer Res 15(8):2942–2948. https://doi.org/10.1158/1078-0432.CCR-08-2658
Rha SY, Moon YH, Jeung HC, Kim YT, Sohn JH, Yang WI, Suh CO, Kim GE, Roh JK, Chung HC (2005) Gemcitabine monotherapy as salvage chemotherapy in heavily pretreated metastatic breast cancer. Breast Cancer Res Treat 90(3):215–221. https://doi.org/10.1007/s10549-004-2468-4
Blackstein M, Vogel CL, Ambinder R, Cowan J, Iglesias J, Melemed A (2002) Gemcitabine as first-line therapy in patients with metastatic breast cancer: a phase II trial. Oncology 62(1):2–8
Albain KS, Nag SM, Calderillo-Ruiz G, Jordaan JP, Llombart AC, Pluzanska A, Rolski J, Melemed AS, Reyes-Vidal JM, Sekhon JS, Simms L, O'Shaughnessy J (2008) Gemcitabine plus paclitaxel versus paclitaxel monotherapy in patients with metastatic breast cancer and prior anthracycline treatment. J Clin Oncol 26(24):3950–3957. https://doi.org/10.1200/JCO.2007.11.9362
Chan S, Romieu G, Huober J, Delozier T, Tubiana-Hulin M, Schneeweiss A, Lluch A, Llombart A, du Bois A, Kreienberg R, Mayordomo JI, Anton A, Harrison M, Jones A, Carrasco E, Vaury AT, Frimodt-Moller B, Fumoleau P (2009) Phase III study of gemcitabine plus docetaxel compared with capecitabine plus docetaxel for anthracycline-pretreated patients with metastatic breast cancer. J Clin Oncol 27(11):1753–1760. https://doi.org/10.1200/JCO.2007.15.8485
Siegel-Lakhai WS, Crul M, Zhang S, Sparidans RW, Pluim D, Howes A, Solanki B, Beijnen JH, Schellens JH (2005) Phase I and pharmacological study of the farnesyltransferase inhibitor tipifarnib (Zarnestra, R115777) in combination with gemcitabine and cisplatin in patients with advanced solid tumours. Br J Cancer 93(11):1222–1229. https://doi.org/10.1038/sj.bjc.6602850
Sun J, Blaskovich MA, Knowles D, Qian Y, Ohkanda J, Bailey RD, Hamilton AD, Sebti SM (1999) Antitumor efficacy of a novel class of non-thiol-containing peptidomimetic inhibitors of farnesyltransferase and geranylgeranyltransferase I: combination therapy with the cytotoxic agents cisplatin, Taxol, and gemcitabine. Cancer Res 59(19):4919–4926
Adjei AA, Davis JN, Bruzek LM, Erlichman C, Kaufmann SH (2001) Synergy of the protein farnesyltransferase inhibitor SCH66336 and cisplatin in human cancer cell lines. Clin Cancer Res 7(5):1438–1445
Patnaik A, Eckhardt SG, Izbicka E, Tolcher AA, Hammond LA, Takimoto CH, Schwartz G, McCreery H, Goetz A, Mori M, Terada K, Gentner L, Rybak ME, Richards H, Zhang S, Rowinsky EK (2003) A phase I, pharmacokinetic, and biological study of the farnesyltransferase inhibitor tipifarnib in combination with gemcitabine in patients with advanced malignancies. Clin Cancer Res 9(13):4761–4771
Van Cutsem E, van de Velde H, Karasek P, Oettle H, Vervenne WL, Szawlowski A, Schoffski P, Post S, Verslype C, Neumann H, Safran H, Humblet Y, Perez Ruixo J, Ma Y, Von Hoff D (2004) Phase III trial of gemcitabine plus tipifarnib compared with gemcitabine plus placebo in advanced pancreatic cancer. J Clin Oncol 22(8):1430–1438. https://doi.org/10.1200/JCO.2004.10.112
Schmid P, Akrivakis K, Flath B, Grosse Y, Sezer O, Mergenthaler HG, Possinger K (1999) Phase II trial of gemcitabine as prolonged infusion in metastatic breast cancer. Anti-Cancer Drugs 10(7):625–631
Spielmann M, Llombart-Cussac A, Kalla S, Espie M, Namer M, Ferrero JM, Dieras V, Fumoleau P, Cuvier C, Perrocheau G, Ponzio A, Kayitalire L, Pouillart P (2001) Single-agent gemcitabine is active in previously treated metastatic breast cancer. Oncology 60 (4):303-307. Doi:58524
Brodowicz T, Kostler WJ, Moslinger R, Tomek S, Vaclavik I, Herscovici V, Wiltschke C, Steger GG, Wein W, Seifert M, Kubista E, Zielinski CC (2000) Single-agent gemcitabine as second- and third-line treatment in metastatic breast cancer. Breast 9(6):338–342. https://doi.org/10.1054/brst.2000.0170
Park JY, Kim C, Sohn JH, Kim YT, Rha SY, Jang WI, Kim GE, Chung HC (2002) A phase II study of gemcitabine monotherapy in breast cancer patients refractory to anthracycline and Taxane. Cancer Res Treat 34(4):274–279. https://doi.org/10.4143/crt.2002.34.4.274
Sparano JA, Moulder S, Kazi A, Vahdat L, Li T, Pellegrino C, Munster P, Malafa M, Lee D, Hoschander S, Hopkins U, Hershman D, Wright JJ, Sebti SM (2006) Targeted inhibition of farnesyltransferase in locally advanced breast cancer: a phase I and II trial of tipifarnib plus dose-dense doxorubicin and cyclophosphamide. J Clin Oncol 24(19):3013–3018. https://doi.org/10.1200/JCO.2005.04.9114
Acknowledgments
This work was supported in part by the National Institutes of Health/National Cancer Institute (N01-CM-2011-00039). Tipifarnib was provided by the National Cancer Institute (NCI) under a Clinical Trials Agreement (CTA) with Johnson & Johnson Pharmaceutical Research and Development LLC.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of interest
The authors declare no relevant potential conflicts of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Yam, C., Murthy, R.K., Valero, V. et al. A phase II study of tipifarnib and gemcitabine in metastatic breast cancer. Invest New Drugs 36, 299–306 (2018). https://doi.org/10.1007/s10637-018-0564-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-018-0564-2