
Abstract
Aim
In this retrospective cohort study, we evaluated the significance of liver volume in the prediction of hepatocellular carcinoma (HCC) in 277 chronic hepatitis C (CHC) patients who received dynamic computed tomography (CT) during surveillance.
Methods
Liver volumes were measured on portal venous phase of CT images by using ImageJ software. Liver volume index, a ratio of the standard liver volume expected by weight and height to the measured liver volume, was calculated to adjust for normal variations. The cohort was randomly divided to derivation (n = 100) and validation sets (n = 177) for the generation of a liver volume-based Cox prediction model and validation of a liver volume-based nomogram, respectively.
Results
The liver volume index was independent of weight or height, and it predicted further development of HCC (hazard ratio [HR] 16.30, 95% CI 6.70–39.62; p < 0.001). Liver cirrhosis, gamma-glutamyl transferase, and liver volume index were independent predictors of HCC, and nomogram-based prediction score from these three parameters identified high-risk patients at the cutoff of 110 in both derivation (p < 0.001) and validation cohort (p < 0.001).
Conclusion
Liver volume-based prediction model stratifies the risk of developing HCC in CHC patients whose initial dynamic CT study gave negative results.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hepatitis C virus (HCV) infection poses global health threat: over 142 million people are infected with HCV and the prevalence has increased by 18% over the last decade [1]. Hepatocellular carcinoma (HCC) is one of the most serious complications of HCV infection. The age-adjusted annual mortality of HCV-associated HCC is 2.6 per 100,000 globally [2]. Antiviral therapy for chronic hepatitis C (CHC) can reduce the risk of HCC [3], but a significant number of patients still develop HCC after achieving sustained virologic response (SVR) [4,5,6]. Therefore, surveillance for HCC is an important issue in the management of CHC.
Current guidelines recommend ultrasonography (US) with or without alpha-fetoprotein (AFP) as a surveillance tool for HCC detection in CHC patients [7,8,9,10,11]. Contrast-enhanced dynamic imaging studies such as computed tomography (CT) or magnetic resonance imaging (MRI) are indicated as a recall procedure if surveillance tests reveal suspicious nodule(s) and/or elevated tumor marker levels. Dynamic imaging studies are also indicated if advanced cirrhotic change limits adequate ultrasonographic evaluation [11]. Patients who get a negative result from the dynamic imaging may still have increased risk of HCC and warrant enhanced surveillance [7, 10], but it is not well defined how these patients should be followed.
Liver volume shrinks as chronic liver diseases progress, and it correlates with hepatic functional reserve in normal and pathologic states [12,13,14,15]. Computed tomography (CT) volumetry accurately measures liver volume [16,17,18], and CT-measured liver volumetry has been used in the preoperative planning [15, 17, 19]. Since CT volumetry can be obtained retrospectively on the scans performed during HCC surveillance, we sought to assess the prognostic significance of CT liver volumetry in CHC patients in whom the screening tests for HCC gave abnormal results and yet dynamic CT imaging did not reveal HCC.
Methods
Study Population
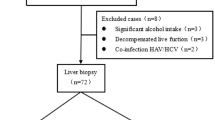
This retrospective cohort study enrolled all consecutive CHC patients who visited a tertiary referral center in South Korea between May 2003 and February 2016 and received regular surveillance for HCC for longer than 6 months (Fig. 1). Exclusion criteria were (1) diagnosis of HCC and other malignancies before or within 6 months after initial surveillance, (2) decompensated liver disease, i.e., Child–Pugh class B or C, and (3) HBV or HIV co-infection. CHC was diagnosed by positive tests for anti-HCV antibody and detection of serum HCV RNA. The presence of cirrhosis was diagnosed by histology, by imaging studies showing regenerative hepatic nodules and/or liver surface undulation or by endoscopy showing esophageal varices. HCC was diagnosed histologically or radiologically [20]. All patients were evaluated with biochemical and virologic blood tests at 3–6 months of interval. Surveillance abdominal ultrasonography was performed at 6–12 months of interval. Contrast-enhanced multidetector CT (MDCT) was performed when surveillance test results triggered recall procedures [10, 21]. MDCT was also performed in patients for whom US examination was considered inadequate for the detection of possible small HCC [10, 22].

Flowchart of the study population. *HCC surveillance is reimbursed by National Health Insurance Service in Korea in CHC patient aged > 40 or with cirrhosis. †Patients were recommended for liver CT if liver US showed new nodule(s), serum AFP elevated or liver US examination was considered inadequate for the detection of possible small HCC due to advanced cirrhotic change
This study has been approved by the institutional review board of Seoul National University Bundang Hospital (IRB Number: B-1706-401-101). Clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki [23]. The requirement for informed consent was waived by the IRBs due to the retrospective nature of the study and the anonymous analysis of the data.
Measurement of Liver Volume
Liver volume was measured on portal venous phase contrast-enhanced MDCT images as previously reported [24]. Briefly, each cross-sectional area of individual liver slices in transverse plane images was measured by using Image J (Research Services Branch, National Institute of Mental Health, Maryland, USA; http://imagej.nih.gov/ij). The liver boundaries were semi-automatically determined using the Versatile Wand Tool (https://imagej.nih.gov/ij/plugins/versatile-wand-tool/index.html) to enhance consistency of measurement. The inferior vena cava and gallbladder were excluded from volume measurement, but the intrahepatic portal veins enclosed by hepatic parenchyma were included in the measured areas. The calculated area of the liver was integrated over the hepatic vertical span. Since body build may affect liver volume [14, 24, 25], normal variance was adjusted for standardized liver volume by calculating the “liver volume index” as previously reported [14]:
where formula liver volume, i.e., standardized liver volume = 893.485 × body surface area (BSA)—439.169 (ml) [25] and (BSA = 0.007184 × (weight in kg)0.425 × (height in cm)0.725) [26]. Thus, decreased liver volume is expressed as increased volume index.
Statistical Analysis
The data collection and analysis followed the guideline of Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) [27]. The statistical analyses were performed using STATA version 14 (College Station, Texas) and R 3.3.2 (http://www.r-project.org/). Student’s t test and Kruskal–Wallis rank test were used for continuous variables, and Chi-square test was used for categorical variables. The associations between continuous variables were tested using Spearman rank correlation. The cumulative HCC risk was analyzed using Kaplan–Meier curves, and differences in curves were tested using the log-rank test. Cox proportional hazard analysis was used to identify the independent predictors of HCC risk. Nomogram for HCC prediction was developed using the risksetROC package of R [28]. Analysis of time-dependent ROC with calculation of integrated AUC and p value was performed by survcomp package of R [29].
Results
Baseline Characteristics and Incidence of HCC During Follow-Up
During the study period, 1121 CHC patients received regular HCC surveillance. After excluding 29 patients as defined in Fig. 1, recall procedure, i.e., dynamic CT imaging, was indicated in 650 patients, among whom 381 patients received liver CT scans. HCC cases were also excluded if detected within 6 months from screening (n = 104), and finally, 277 patients were included in this study. Baseline characteristics are summarized in Table 1. The median follow-up duration was 46 months (range: 6–167 months), during which 44 patients developed HCC with the incidence of 2.53 per 1000 person-years (Supplementary Fig. 1). In patients whose histologic data were available (n = 80), 3.6%, 9.1%, 16.7%, and 45.8% developed HCC in F1, F2, F3, and F4 fibrosis, respectively.
Liver Volume Profiles in CHC
Liver volume was associated with various parameters: age, weight, height, sex, liver cirrhosis, diabetes, platelet count, prothrombin time, and FIB-4 (Supplementary Table). The liver volume index, the estimated-to-measured liver volume ratio, also showed significant association with functional parameters, but contrary to the liver volume, did not depend on weight or height. In patients whose histologic data were available, the liver volume index was not significantly different across the variable stage of fibrosis (p = 0.635, Supplementary Fig. 2).
Liver Volume as an Independent Predictor of HCC
Previous observational studies identified several predictors of HCV-associated HCC such as age, cirrhosis, thrombocytopenia, and elevated GGT levels [30,31,32,33]. Our univariate Cox analysis also found these factors as significant predictors of HCC, along with diabetes, elevated baseline alpha-fetoprotein (AFP), prolonged prothrombin time, and significant fibrosis. Liver volume index was also predictive of further development of HCC (hazard ratio [HR] 16.30, 95% CI 6.70–39.62; p < 0.001). Multivariate analysis also confirmed that liver volume index was an independent predictor of HCC, along with liver cirrhosis and high GGT levels (Table 2). Liver volume index remained significant when subgroups were analyzed for cirrhosis and non-cirrhosis (Supplementary Table 2 and 3). These findings indicate that liver volume index has an independent prognostic value regardless of the presence of liver cirrhosis, i.e., the volume index can further stratify HCC risks in both cirrhotic and non-cirrhotic CHC patients. Sensitivity analysis also demonstrated that the live volume index is a powerful predictor of HCC, independent of various clinical and laboratory parameters (Fig. 2).

Sensitivity analysis of liver volume index hazard ratio for predicting HCC. Hazard ratio of liver volume index for HCC maintained significance across major clinical and laboratory parameters
Liver Volume-Based Prediction Model Differentiate Risk of HCC
Finally, we tried to verify the predictive power of liver volume index by building a prediction model using the independent predictors. For internal validation, the study population was divided randomly into derivation (n = 100) and validation (n = 177) cohort. A nomogram was built from the derivation cohort based on the presence of cirrhosis, GGT, and liver volume index to generate liver volume score for the prediction of HCC (Fig. 3). Discrimination analysis showed that the liver volume score significantly differentiated the HCC at the cutoff of 110, in both the derivation and validation cohort (p < 0.001, respectively) (Fig. 4). Two cutoffs at the nomogram point 80 and 120 were also able to discriminate medium- and high-risk from low-risk group for HCC development (Supplementary Fig. 3).

Nomogram from multivariable Cox regression analysis for risk of HCC in derivation cohort. Total risk scores are calculated by summing up points of the three parameters (Points axis). Are summed to get the total points (Total Points axis). The 2-, 4-, and 6-yr predicted probability for HCC are obtained from the corresponding total points

Discrimination of HCC probability by volume score-based nomogram. The nomogram-based liver volume score model differentiated the HCC risk at the cutoff off 110 in both derivation (a) and validation (b) cohort
Discussion
In this study, we found that decreased liver volume was independent predictor of HCC in CHC patients in addition to the classic predictors such as cirrhosis and GGT [32, 34,35,36,37,38]. Degree of hepatic fibrosis reliably stratifies the risk of HCC in CHC [35, 36, 39], but the staging of fibrosis needs liver biopsy which is invasive and prone to sampling error [40, 41]. LSM has been emerged as an attractive surrogate marker of fibrosis stage, but the role of LSM as a risk predictor for HCC has not been unequivocally validated [42,43,44,45]. Since advanced liver disease is frequently associated with decreased liver volume, it is plausible that liver volumetry may predict the risk for HCC. However, this assumption has not been quantitatively demonstrated in CHC.
Our analysis revealed that liver volume correlated with several demographic, clinical, and laboratory parameters (Supplementary Table). After adjustment by body surface area, liver volume index shows correlations only with age, presence of cirrhosis, HCV RNA levels, platelet counts, prothrombin time, and FIB-4. These relationships suggest that adjusted liver volume reflects the stage of liver fibrosis. Interestingly, however, there was wide overlap of volume index over various stages of fibrosis (Supplementary Fig. 2), indicating that stage of hepatic fibrosis may not be the sole determinant of volume index. This finding also suggests that additional mechanism(s) other that the degree of hepatic fibrosis may also contribute to the prognostic power of liver volume index. The result of the sensitivity analysis which showed that liver volume index remained significant across all subgroups may also support this hypothesize, but further validating studies will be necessary.
In predicting of HCV-associated HCC, several models have been built based on combinations of risk factors: age [32, 34, 37, 38], sex [33, 38], alcohol [32], presence of cirrhosis [34], platelet counts [32, 37, 38], alpha-fetoprotein [37, 38], liver enzymes [32,33,34, 37], and virologic parameters [32, 34]. Among them, only a few models included both non-cirrhotic and cirrhotic CHC patients [34,35,36]. Since HCV-associated HCC can develop without cirrhosis [46, 47], our liver volume-based prediction model may be versatile for clinical applications regardless of the presence of cirrhosis.
One of our major findings is that liver volume was an independent predictor of HCC in both cirrhotic and non-cirrhotic patients (Fig. 3 and Supplementary Table 2 and 3). We do not have mechanistic explanations, but small volume may induce active proliferation of hepatic progenitor cells which could increase oncogenic potential. Further studies are needed for the relation between small liver volume and risk of HCC.
Manual tracing of the hepatic boundary has been considered the gold standard for liver volumetry [16, 48]. In this study, liver volume was measured by free software Image J with a plug-in for semi-automatic boundary detection to minimize the measurement errors and to enhance the efficiency of measurement [24]. Semi-automatic measurements show comparable accuracy and precision [17], and we have also found that our method shows good reproducibility in chronic hepatitis B [24]. Technical accessibility of our method may enable clinical implementation of live volumetry without additional resources.
It is an interesting finding that GGT remained significant in our prediction model. GGT has been associated with adverse outcomes [49] including HCC [32] in chronic HCV infection. Supplementary Table 1 shows inverse relation between GGT levels and liver volume. We do not have definite explanation for the significance of GGT in HCC prediction and the inverse relation with liver volume at this moment. Although current alcohol history did not predict the risk (Table 2), it may be postulated that the GGT might represent alcohol consumption amount in the past, which might affect liver volume and the risk of HCC. However, this hypothesis needs further validation.
There are several limitations in this study. First, the cohort was built from patients from single institution. We adopted split-sample validation and bootstrapping iterations to ascertain internal validity and to minimize over-fitting of the volume-based model [27]. However, external validation is needed as discussed above. Moreover, since our cohort was built retrospectively, there is a potential risk for selection bias. Although we assessed the medical records of all consecutive patients eligible for this study, prospective cohort study may be needed to resolve this issue. Second, our cohort is limited to Korean population, limiting racial generalizability. Third, our prediction model was based on patients with liver CT imaging performed during surveillance, so that our patients may have more severe disease compared to general CHC population and therefore have increased HCC. Therefore, application of our results needs to be limited to CHC patients who receive liver CT as a recall procedure for abnormal HCC screening, and liver CT cannot be recommended for a prognostic purpose when screening tests do not indicate liver CT. Moreover, our study population was heterogeneous in terms of the LI-RADS category [50]. Majority of patients with abnormal US findings corresponded to LI_RADS US-3, but some received CT evaluation due to visualization score C (data not shown). We were not able to determine the exact LI_RADS category because the US results had been reported before the implementation of standardized reporting system. Further studies will be needed to determine the baseline LI-RADS status on the prognostic significance of our data. Fourth, our patients were heterogeneous with respect to the history of DAA therapy. However, SVR was not a significant predictor of HCC in our model, and sensitivity analysis showed that volume index was significant irrespective of SVR. Finally, only limited number of patients received transient elastography in our cohort (data not shown), so that comparison between liver volumetry and LSM was not done in our analysis. Further study would be needed to compare the performance between liver volume and LSM in predicting the fibrosis stage and risk of HCV-associated HCC.
In conclusion, decreased liver volume is an independent predictor of HCC risk in CHC whose initial dynamic CT study gave negative results, and liver volume-based prediction model stratifies the risk of developing HCC in these patients.
References
Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1545–1602. https://doi.org/10.1016/S0140-6736(16)31678-6.
Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1459–1544. https://doi.org/10.1016/S0140-6736(16)31012-1.
Bang CS, Song IH. Impact of antiviral therapy on hepatocellular carcinoma and mortality in patients with chronic hepatitis C: systematic review and meta-analysis. BMC Gastroenterol. 2017;17:46. https://doi.org/10.1186/s12876-017-0606-9.
Conti F, Buonfiglioli F, Scuteri A, et al. Early occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals. J Hepatol. 2016;65:727–733. https://doi.org/10.1016/j.jhep.2016.06.015.
Cheung MCM, Walker AJ, Hudson BE, et al. Outcomes after successful direct-acting antiviral therapy for patients with chronic hepatitis C and decompensated cirrhosis. J Hepatol. 2016;65:741–747. https://doi.org/10.1016/j.jhep.2016.06.019.
Lee HW. Nonzero risk of hepatocellular carcinoma even after sustained virological response. Gut Liver. 2016;10:661–662. https://doi.org/10.5009/gnl16340.
Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11:317–370. https://doi.org/10.1007/s12072-017-9799-9.
Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358–380. https://doi.org/10.1002/hep.29086.
Korean Liver Cancer A, National Cancer C. 2018 Korean Liver Cancer Association-National Cancer Center Korea practice guidelines for the management of hepatocellular carcinoma. Gut Liver. 2019;13:227–299. https://doi.org/10.5009/,gnl19024.
Kokudo N, Takemura N, Hasegawa K, et al. Clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol Res. 2019;49:1109–1113. https://doi.org/10.1111/hepr.13411.
European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. https://doi.org/10.1016/j.jhep.2018.03.019.
Ozaki K, Matsui O, Kobayashi S, et al. Selective atrophy of the middle hepatic venous drainage area in hepatitis C-related cirrhotic liver: morphometric study by using multidetector CT. Radiology. 2010;257:705–714. https://doi.org/10.1148/radiol.10100468.
Ito K, Mitchell DG, Hann HW, et al. Viral-induced cirrhosis: grading of severity using MR imaging. AJR. 1999;173:591–596. https://doi.org/10.2214/ajr.173.3.10470885.
Zhou XP, Lu T, Wei YG, Chen XZ. Liver volume variation in patients with virus-induced cirrhosis: findings on MDCT. AJR. 2007;189:W153–159. https://doi.org/10.2214/AJR.07.2181.
Kubota K, Makuuchi M, Kusaka K, et al. Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology. 1997;26:1176–1181. https://doi.org/10.1053/jhep.1997.v26.pm0009362359.
Suzuki K, Epstein ML, Kohlbrenner R, et al. Quantitative radiology: automated CT liver volumetry compared with interactive volumetry and manual volumetry. AJR. 2011;197:W706–712. https://doi.org/10.2214/AJR.10.5958.
Lim MC, Tan CH, Cai J, Zheng J, Kow AW. CT volumetry of the liver: where does it stand in clinical practice? Clin Radiol. 2014;69:887–895. https://doi.org/10.1016/j.crad.2013.12.021.
D’Onofrio M, De Robertis R, Demozzi E, Crosara S, Canestrini S, Pozzi Mucelli R. Liver volumetry: is imaging reliable? Personal experience and review of the literature. World J Radiol. 2014;6:62–71. https://doi.org/10.4329/wjr.v6.i4.62.
Higashiyama H, Yamaguchi T, Mori K, et al. Graft size assessment by preoperative computed tomography in living related partial liver transplantation. Br J Surg. 1993;80:489–492.
Bruix J, Sherman M, American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–1022. https://doi.org/10.1002/hep.24199.
Korean Liver Cancer Study G, National Cancer Center K. 2014 KLCSG-NCC Korea practice guideline for the management of hepatocellular carcinoma. Gut Liver. 2015;9:267–317. https://doi.org/10.5009/gnl14460.
Kudo M, Matsui O, Izumi N, et al. JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the Liver Cancer Study Group of Japan. Liver Cancer. 2014;3:458–468. https://doi.org/10.1159/000343875.
World Medical A. World Medical Association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194. https://doi.org/10.1001/jama.2013.281053.
Lee CS, Jung YJ, Kim SS, et al. Liver volume-based prediction model stratifies risks for hepatocellular carcinoma in chronic hepatitis B patients on surveillance. PLoS ONE. 2018;13:e0190261. https://doi.org/10.1371/journal.pone.0190261.
Um EH, Hwang S, Song GW, et al. Calculation of standard liver volume in Korean adults with analysis of confounding variables. Korean J Hepatobiliary Pancreat Surg. 2015;19:133–138. https://doi.org/10.14701/kjhbps.2015.19.4.133.
Du Bois D, Du Bois EF. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition. 1989;5:303–311. (discussion 312-303).
Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. Ann Intern Med. 2015;162:55–63. https://doi.org/10.7326/M14-0697.
Heagerty PJ, Zheng Y. Survival model predictive accuracy and ROC curves. Biometrics. 2005;61:92–105. https://doi.org/10.1111/j.0006-341X.2005.030814.x.
Schroder MS, Culhane AC, Quackenbush J, Haibe-Kains B. Survcomp: an R/Bioconductor package for performance assessment and comparison of survival models. Bioinformatics. 2011;27:3206–3208. https://doi.org/10.1093/bioinformatics/btr511.
Kanwal F, Kramer JR, Asch SM, Cao Y, Li L, El-Serag HB. Long-term risk of hepatocellular carcinoma in HCV patients treated with direct acting antiviral agents. Hepatology. 2019;. https://doi.org/10.1002/hep.30823.
Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155:1436–1450e1436. https://doi.org/10.1053/j.gastro.2018.07.015.
Ganne-Carrie N, Layese R, Bourcier V, et al. Nomogram for individualized prediction of hepatocellular carcinoma occurrence in hepatitis C virus cirrhosis (ANRS CO12 CirVir). Hepatology. 2016;64:1136–1147. https://doi.org/10.1002/hep.28702.
van der Meer AJ, Hansen BE, Fattovich G, et al. Reliable prediction of clinical outcome in patients with chronic HCV infection and compensated advanced hepatic fibrosis: a validated model using objective and readily available clinical parameters. Gut. 2015;64:322–331. https://doi.org/10.1136/gutjnl-2013-305357.
Lee MH, Lu SN, Yuan Y, et al. Development and validation of a clinical scoring system for predicting risk of HCC in asymptomatic individuals seropositive for anti-HCV antibodies. PLoS ONE. 2014;9:e94760. https://doi.org/10.1371/journal.pone.0094760.
Chang KC, Hung CH, Lu SN, et al. A novel predictive score for hepatocellular carcinoma development in patients with chronic hepatitis C after sustained response to pegylated interferon and ribavirin combination therapy. J Antimicrob Chemother. 2012;67:2766–2772. https://doi.org/10.1093/jac/dks269.
Chang KC, Wu YY, Hung CH, et al. Clinical-guide risk prediction of hepatocellular carcinoma development in chronic hepatitis C patients after interferon-based therapy. Br J Cancer. 2013;109:2481–2488. https://doi.org/10.1038/bjc.2013.564.
El-Serag HB, Kanwal F, Davila JA, Kramer J, Richardson P. A new laboratory-based algorithm to predict development of hepatocellular carcinoma in patients with hepatitis C and cirrhosis. Gastroenterology. 2014;146:1249–1255e1241. https://doi.org/10.1053/j.gastro.2014.01.045.
Ikeda K, Arase Y, Saitoh S, et al. Prediction model of hepatocarcinogenesis for patients with hepatitis C virus-related cirrhosis. Validation with internal and external cohorts. J Hepatol. 2006;44:1089–1097. https://doi.org/10.1016/j.jhep.2006.02.008.
Yoshida H, Shiratori Y, Moriyama M, et al. Interferon therapy reduces the risk for hepatocellular carcinoma: national surveillance program of cirrhotic and noncirrhotic patients with chronic hepatitis C in Japan. IHIT Study Group. Inhibition of hepatocarcinogenesis by interferon therapy. Ann Intern Med. 1999;131:174–181.
Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am J Gastroenterol. 2002;97:2614–2618. https://doi.org/10.1111/j.1572-0241.2002.06038.x.
Bedossa P, Carrat F. Liver biopsy: the best, not the gold standard. J Hepatol. 2009;50:1–3. https://doi.org/10.1016/j.jhep.2008.10.014.
Masuzaki R, Tateishi R, Yoshida H, et al. Prospective risk assessment for hepatocellular carcinoma development in patients with chronic hepatitis C by transient elastography. Hepatology. 2009;49:1954–1961. https://doi.org/10.1002/hep.22870.
Wang JH, Yen YH, Yao CC, et al. Liver stiffness-based score in hepatoma risk assessment for chronic hepatitis C patients after successful antiviral therapy. Liver Int. 2016;36:1793–1799. https://doi.org/10.1111/liv.13179.
Sultanik P, Kramer L, Soudan D, et al. The relationship between liver stiffness measurement and outcome in patients with chronic hepatitis C and cirrhosis: a retrospective longitudinal hospital study. Aliment Pharmacol Therap. 2016;44:505–513. https://doi.org/10.1111/apt.13722.
Adler M, Larocca L, Trovato FM, Marcinkowski H, Pasha Y, Taylor-Robinson SD. Evaluating the risk of hepatocellular carcinoma in patients with prominently elevated liver stiffness measurements by FibroScan: a multicentre study. HPB (Oxford). 2016;18:678–683. https://doi.org/10.1016/j.hpb.2016.05.005.
De Mitri MS, Poussin K, Baccarini P, et al. HCV-associated liver cancer without cirrhosis. Lancet. 1995;345:413–415.
el-Refaie A, Savage K, Bhattacharya S, et al. HCV-associated hepatocellular carcinoma without cirrhosis. J Hepatol. 1996;24:277–285.
Suzuki K, Kohlbrenner R, Epstein ML, Obajuluwa AM, Xu J, Hori M. Computer-aided measurement of liver volumes in CT by means of geodesic active contour segmentation coupled with level-set algorithms. Med Phys. 2010;37:2159–2166. https://doi.org/10.1118/1.3395579.
Everhart JE, Wright EC. Association of gamma-glutamyl transferase (GGT) activity with treatment and clinical outcomes in chronic hepatitis C (HCV). Hepatology. 2013;57:1725–1733. https://doi.org/10.1002/hep.26203.
Rodgers SK, Fetzer DT, Gabriel H, et al. Role of US LI-RADS in the LI-RADS algorithm. Radiographics. 2019;39:690–708. https://doi.org/10.1148/rg.2019180158.
Acknowledgments
All authors have no competing interests or other interests that might be perceived to influence the results and/or discussion reported in this paper. This work was supported by a National Research Foundation of Korea (NRF) Grant to J-W Kim, funded by the Korean Government (2017R1D1A1B03031483). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
JWK designed the study, analyzed the data, and drafted the manuscript. NK collected and analyzed the data and revised the manuscript. JWC, ESJ, and SHJ collected the data, participated in the study design, and revised the manuscript.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Fig.
1. Cumulative incidence of HCC during the study period (TIFF 674 kb)
Supplementary Fig.
2. Liver volume index with respect to stage of hepatic fibrosis. P value was calculated by Kruskal–Wallis rank test (TIFF 637 kb)
Supplementary Fig.
3. Discrimination of HCC probability by volume score-based nomogram. The nomogram-based liver volume score model differentiated the low-, medium-, and high-HCC risk at the cutoff off 80 and 120 in both derivation and validation cohort (TIFF 828 kb)
Rights and permissions
About this article

Cite this article
Kang, N., Chung, J.W., Jang, E.S. et al. Computed Tomography-Measured Liver Volume Predicts the Risk of Hepatocellular Carcinoma Development in Chronic Hepatitis C Patients. Dig Dis Sci 66, 4536–4544 (2021). https://doi.org/10.1007/s10620-020-06762-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06762-w