
Abstract
Objectives
This study aimed to develop and validate a nomogram based on extracellular volume (ECV) derived from computed tomography (CT) for predicting post-hepatectomy liver failure (PHLF) in patients with resectable hepatocellular carcinoma (HCC).
Methods
A total of 202 patients with resectable HCC from two hospitals were enrolled and underwent multiphasic contrast-enhanced CT before surgery. One hundred twenty-one patients from our hospital and 81 patients from another hospital were assigned to the training cohort and the validation cohort, respectively. CT–derived ECV was measured using nonenhanced and equilibrium-phase-enhanced CT images. The nomogram was developed with independent predictors of PHLF. Predictive performance and calibration were assessed by receiver operator characteristic (ROC) analysis and Hosmer–Lemeshow test, respectively. The Delong test was used to compare the areas under the curve (AUCs).
Results
CT–derived ECV had a strong correlation with the postoperative pathological fibrosis stage of the background liver (p < 0.001, r = 0.591). The nomogram combining CT–derived ECV, serum albumin (Alb), and serum total bilirubin (Tbil) obtained higher AUCs than the albumin–bilirubin (ALBI) score for predicting PHLF in both the training cohort (0.828 vs. 0.708; p = 0.004) and the validation cohort (0.821 vs. 0.630; p < 0.001). The nomogram showed satisfactory goodness of fit for PHLF prediction in the training and validation cohorts (p = 0.621 and 0.697, respectively).
Conclusions
The nomogram contributes to the preoperative prediction of PHLF in patients with resectable HCC.
Key Points
• CT–derived ECV had a strong correlation with the postoperative pathological fibrosis stage of the background liver.
• CT–derived ECV was an independent predictor of PHLF in patients with resectable HCC.
• The nomogram based on CT–derived ECV showed a superior prediction efficacy than that of clinical models (including Child–Pugh stage, MELD score, and ALBI score).
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Liver resection is one of the radical treatment options for patients with resectable hepatocellular carcinoma (HCC) [1]. Post-hepatectomy liver failure (PHLF) is the most serious complication of liver resection, accounting for more than 50% of postoperative deaths [2,3,4,5]. Previous reports have shown that the incidence of PHLF after liver resection varies and ranges from 0.7 to 39.6% [6, 7]. The occurrence of PHLF is decided by both the quality and the quantity of remaining liver parenchyma [8]. Preoperative assessment of background liver function is essential for preventing the development of PHLF.
Several clinical models are commonly used for predicting PHLF in patients with resectable HCC, including Child–Pugh stage, Model for End-Stage Liver Disease (MELD) scoring system, and albumin–bilirubin (ALBI) score. Zou et al [9] determined that the ALBI score is an independent predictor of PHLF and showed superior predictive value over Child–Pugh stage and MELD score. Unfortunately, the predictive ability of the ALBI score is still unsatisfactory due to limited data.
Multiphasic contrast-enhanced computed tomography (CT) is a widely recommended modality for the preoperative assessment of HCC [10, 11]. The liver consists of three distinct spaces, including the intravascular space, intracellular space, and extravascular extracellular space. The expansion of extracellular volume (ECV), due to the deposition of collagen and matrix proteins, is the histopathologic feature of liver fibrosis [12]. Several studies [12,13,14,15,16,17] have indicated that ECV, which is calculated using nonenhanced and equilibrium-phase CT images, can predict the degree of liver fibrosis. HCC patients usually suffer from liver fibrosis and cirrhosis, which is associated with PHLF [2, 8, 18, 19]. However, whether CT–derived ECV can predict PHLF in patients with resectable HCC is unclear.
Nomogram [20], simple visualization of complex regression equation, has been widely used. It is considered to be evidence-based, personalized, and accurate risk assessment. In this study, we aimed to develop and validate a nomogram based on CT–derived ECV for predicting PHLF in patients with resectable HCC and to compare the preoperative prediction efficacy of this nomogram with that of clinical models (including Child–Pugh stage, MELD score, and ALBI score).
Materials and methods
Patients
This retrospective study was approved by the Institutional Review Board of the two participating hospitals. Informed consent was waived.
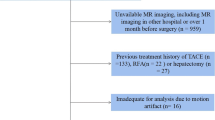
Between June 2013 and May 2021, 1150 consecutive patients who underwent liver resection with histopathologically proven HCC at Chongqing University Cancer Hospital were reviewed retrospectively. A total of 121 patients who met the inclusion criteria were enrolled and formed the training cohort for this study. From November 2019 to July 2021, the other 81 consecutive patients in Chongqing General Hospital with the same selection criteria were enrolled as an independent external validation cohort. The inclusion criteria were as follows: (1) patients with histopathologically confirmed HCC after hepatectomy, (2) patients with Child–Pugh stage (grade A or B) liver function before operation, and (3) patients who underwent multiphasic contrast-enhanced CT examination and serum marker testing within 2 weeks before operation. The exclusion criteria were patients with any antitumor therapy before surgery. None of these included patients were analyzed in another study, nor as a sub-cohort of another published study.
Collection of data
Preoperative laboratory data (including biochemical and coagulation markers) were recorded, including plasma levels of platelet (PLT) counts, alanine aminotransferase (ALT), aspartate aminotransferase (AST), albumin (Alb), creatinine (Cr), total bilirubin (Tbil), hematocrit (Hct), international normalized ratio (INR), prothrombin time (PT), and prothrombin activity (PTA). The following preoperative comorbidities were recorded: ascites, high blood pressure, diabetes mellitus, the presence of viral hepatitis, and liver cirrhosis. Surgical data were recorded, including operation time, hepatic inflow occlusion duration (the total time of occlusion of hepatic blood flow during hepatic resection), blood loss in surgery, blood transfusion, and hepatectomy (major or minor). Major hepatectomy was defined as resection of four or more liver segments, and minor hepatectomy was defined as resection of three or fewer liver segments [21]. All resected specimens were subjected to histopathological analysis, and fibrosis stage (S0–4) and the presence of steatosis in the background liver were recorded.
The MELD score and the ALBI score were calculated using the following formulas [9]: MELD score = 11.2 × ln (INR) + 9.57 × ln (Cr, mg/dL) + 3.78 × ln (Tbil, mg/dL) + 6.43 × etiology (0 for cholestatic and alcoholic, 1 for liver cirrhosis due to virus and other causes); ALBI score = 0.66 × log10 (Tbil [μmol/L]) − 0.085 × (Alb [g/L]).
According to the International Study Group of Liver Surgery (ISGLS) [4], PHLF was defined as hyperbilirubinemia (serum Tbil > 22 μmol/L or above preoperative value) and increased INR (INR > 1.5 or PTA < 50%) on or after postoperative day 5, except for observed biochemical and clinical changes due to other reasons.
CT examination protocol
Multiphasic contrast-enhanced CT was conducted for all patients using two CT scanners (SOMATOM Definition AS and SOMATOM DRIVE, Siemens Healthineers). The scanning range was from the lung base to the iliac crest. Nonenhanced images were acquired using the conventional helical scan mode. Contrast material (Ioversol, 320 mg/mL iodine, HENGRUI Medicine) was injected via antecubital venous injection at a rate of 3.0–3.5 mL/s for a total of 80–100 mL (1.5 mL/kg of body weight). Bolus tracking was used. Arterial phase scanning began 7 s after the trigger attenuation threshold (100 HU) reached the level of the supraceliac abdominal aorta. Portal phase scanning began at a delay of 30 s after arterial phase scanning, and the equilibrium phase (EP) began at a delay of 90 s after portal phase scanning. The scanning parameters were as follows: tube voltage = 120 kV, reference tube current = 180 mAs, increment collimation = 128 × 0.6 mm, pitch = 1.0, and rotation time = 0.5 s. The reconstruction parameters were as follows: thickness = 1.5 mm, increment = 1 mm, and soft-tissue convolution kernel (I31). CT images were reconstructed with projection-based material-decomposition software using a standard reconstruction kernel.
Imaging analysis
With the known clinical and surgery data, radiologist 1 (15 years of experience in abdominal CT imaging) drew the regions of interest (ROIs) on the nonenhanced images and EP images in the PACS (DJ HealthUnion Systems Corp version 2.0). For each patient, three anatomical cross sections were chosen, including the intrahepatic inferior vena cava confluence, portal hilum, and gallbladder fossa [15]. Handcrafted ROIs were drawn along the margins of the future remnant liver in the preoperative baseline images, taking care to avoid blood vessels and bile ducts. To minimize the difference in image acquisition time, circular ROIs were placed in the abdominal aorta on the same plane (Fig. S1). The CT values (HU) of the liver (HUliver) and the abdominal aorta (HUaorta) were measured. The ECV values of the background liver at the section of the intrahepatic inferior vena cava confluence (ECV1), portal hilum (ECV2), and gallbladder fossa (ECV3) were calculated using the following formula:
where ΔHU means the change in HU between EP and nonenhanced images. The mean value of ECV1, ECV2, and ECV3 was taken as the CT–derived ECV for the patient (ECV). The calculation process of the CT–derived ECV is also shown in Fig. S1.
To assess intraobserver and interobserver reliability of the CT–derived ECV, radiologist 1 and radiologist 2 (10 years of experience in abdominal CT imaging) drew ROIs at 4 weeks after the first assessment in the PACS in the same way.
Statistical analysis
All statistical analyses were performed using SPSS statistics version 25.0 (International Business Machines Corporation (IBM)). The Kolmogorov–Smirnov test was used to test whether the variable obeyed a normal distribution. Continuous variables are presented as the mean ± standard deviation (SD) or median and interquartile range. Categorical variables were summarized as counts and frequencies. Intraclass correlation coefficients (ICCs) and Bland–Altman plots were used to assess the intraobserver and interobserver reliability of the CT–derived ECV. Spearman’s rank correlation was used to assess the association between CT–derived ECV and the fibrosis stage of the background liver. To identify independent predictors for PHLF, we used univariate and multivariate analyses. For the univariate analysis, the Wilcoxon rank sum test or Student’s t test was used for continuous variables, and the χ2 test or Fisher’s exact test was used for categorical variables. Then, multivariate logistic regression analysis was performed to identify the independent variables for PHLF by using variables (p value < 0.05 in the univariate analyses). The β coefficients from the multivariate logistic regression analysis results were used to form the nomogram to assess the risk for PHLF using R software (version 3.6.2). The predictive performance of the nomogram and clinical models was assessed by receiver operator characteristic (ROC) analysis and nomogram, and the areas under the ROC curve (AUCs) were calculated. The Delong test was used to compare the AUCs. The Hosmer–Lemeshow test was used to assess the calibration of the model. A p value < 0.05 (two-tailed) was considered statistically significant.
Results
Characteristics of the study patients
The characteristics of the study patients in the training cohort and validation cohort are summarized in Table 1. The characteristics included the following categories: preoperative laboratory data, preoperative comorbidity, surgical data, histopathological data, and PHLF. In our study, 121 and 81 consecutive patients with resectable HCC were finally enrolled in the training and validation cohorts, respectively. In the training and validation cohorts, the incidences of PHLF were 39.67% (48/121) and 38.27% (31/81), respectively.
The intraobserver and interobserver reliability of the CT–derived ECV
The intraobserver and interobserver reliability of the CT–derived ECV were good in both the training and validation cohorts, with all ICC values greater than 0.80 (Table S1). The Bland–Altman plots of the CT–derived ECV showed good intraobserver and interobserver agreement in both the training and validation cohorts (Fig. S2). Therefore, the average value of ECV measured by the two radiologists was used for further analysis.
Correlation between CT–derived ECV and pathological fibrosis stage in background liver
Spearman correlation analysis revealed that CT–derived ECV had a strong correlation with the postoperative pathological fibrosis stage of the background liver (p < 0.001, r = 0.591; Fig. 1).

Scatterplot showed strong correlation between CT–derived ECV and the postoperative pathological fibrosis stage of the background liver (p < 0.001, r = 0.591). CT, computed tomography; ECV, extracellular volume
Independent predictors of post-hepatectomy liver failure in the training cohort
The univariate analyses of predictors for PHLF according to the ISGLS criteria in the training cohort are shown in Table 1. CT–derived ECV (28.02 vs. 25.67; p < 0.001), serum Tbil (14.94 μmol/L vs. 13.43 μmol/L; p = 0.013), and hepatic inflow occlusion duration (22.50 min vs. 0 min; p = 0.032) were higher in patients with PHLF than in patients without PHLF. Serum Alb (38.55 g/L ± 5.24 vs. 41.84 g/L ± 4.24; p < 0.001) was lower in patients with PHLF than in patients without PHLF. These four risk factors were accepted in the multivariate logistic regression analysis. With a method of input, CT–derived ECV (OR: 1.308, 95% CI: 1.139–1.502, p < 0.001), serum Alb (odds ratio [OR]: 0.855, 95% confidence interval [CI]: 0.771–0.949, p = 0.003), and serum Tbil (OR: 1.015, 95% CI: 1.000–1.030, p = 0.048) were independent predictors of PHLF (Table 2).
The median ALBI score of patients with PHLF was significantly higher than that of patients without PHLF (− 2.54 vs. − 2.73; p < 0.001). No significant differences in Child–Pugh stage or MELD score between patients with and without PHLF were found (both p > 0.05).
Development of the nomogram
These significant independent predictors were combined to form a nomogram for PHLF estimation in the training cohort (Fig. 2). The nomogram demonstrated good performance for PHLF prediction, with an AUC of 0.828 (95% CI: 0.756–0.901). The AUC of the nomogram for PHLF prediction was higher than that of the single predictor, including CT–derived ECV (AUC = 0.712), serum Alb (AUC = 0.680), serum Tbil (AUC = 0.595), and hepatic inflow occlusion duration (AUC = 0.645; Delong test: p = 0.008, p = 0.002, p < 0.001, and p < 0.001, respectively; Fig. 3). The importance ranking of these factors in the nomogram was CT–derived ECV > serum Alb > serum Tbil. Therefore, CT–derived ECV was the most crucial factor in the nomogram. The nomogram was well calibrated according to the Hosmer–Lemeshow test (p = 0.621) (Table 3 and Fig. 2).

The nomogram and calibration curve for prediction of PHLF in patients with resectable HCC. a The nomogram was developed by combined CT–derived ECV, serum Alb, and serum Tbil in the training cohort. The calibration curves of the nomogram in the training cohort (b) and validation cohort (c) showed a good consistency. PHLF, post-hepatectomy liver failure; HCC, hepatocellular carcinoma; CT, computed tomography; ECV, extracellular volume; Alb, albumin; Tbil, total bilirubin

Receiver operating characteristic (ROC) curve analyses of CT–derived ECV, serum Alb, serum Tbil, hepatic inflow occlusion duration, and the nomogram to predict PHLF. The nomogram showed the highest AUC value (0.828; 95% CI: 0.756–0.901) for PHLF prediction compared with CT–derived ECV, serum Alb, serum Tbil, and hepatic inflow occlusion duration (Delong test: all p < 0.05). PHLF, post-hepatectomy liver failure; Alb, albumin; Tbil, total bilirubin; CT, computed tomography; ECV, extracellular volume; AUC, areas under the curve
Comparison of predictive efficacy for PHLF between the nomogram and clinical models in the training cohort
The predictive power for PHLF prediction between the nomogram and clinical models was compared. There was no significant difference in Child–Pugh stage or MELD score between patients with and without PHLF (both p > 0.05). The AUC of the nomogram was significantly higher than that of the ALBI score (0.828, 95% CI: 0.756–0.901 vs. 0.708, 95% CI: 0.612–0.803; Delong test: p = 0.004) (Fig. 4). The cutoff value of the nomogram was 0.473, with a sensitivity of 68.8% and a specificity of 83.6% for predicting PHLF (Table 3).

Comparison of predictive power for PHLF between the nomogram and ALBI score. The AUCs of the nomogram were significantly higher than those of the ALBI score both in the training cohort (a) and validation cohort (b) (Delong test: p = 0.004, p < 0.001, respectively). PHLF, post-hepatectomy liver failure; ALBI, albumin-bilirubin; AUC, areas under the curve
Validation of the nomogram
For the purpose of validating the nomogram, we prepared a validation cohort from another hospital (n = 81) which met the inclusion and exclusion criteria (Table 1). In the validation cohort, the AUC of the nomogram was significantly higher than that of the ALBI score (0.821, 95% CI: 0.727–0.914 vs. 0.630, 95% CI: 0.516–0.735; Delong test: p < 0.001) (Fig. 4). According to the Hosmer–Lemeshow test, the nomogram showed good agreement between the prediction and actual observation (p = 0.697, Fig. 2). Two examples were given to illustrate the clinical application of the nomogram (Fig. S3).
Discussion
In our study, we developed and validated a nomogram for the prediction of PHLF in patients with resectable HCC. The nomogram integrated three independent factors, including CT–derived ECV, serum Alb, and serum Tbil. In addition, CT–derived ECV was the most crucial factor in the nomogram. The performance of the nomogram was superior to that of the clinical model with AUCs of 0.828 and 0.821 in the training and validation cohorts, respectively. The nomogram may be helpful for providing pretreatment consultation for patients who are suitable for hepatectomy.
We found that CT–derived ECV had a strong positive correlation with the postoperative pathological fibrosis stage of the background liver. The higher the ECV of the background liver, the more severe the liver fibrosis. Our results are consistent with those of previous studies showing that ECV was useful in estimating the liver fibrosis stage and the risk of liver-related events [12,13,14,15,16,17]. The histopathological mechanism of liver fibrosis is the expansion of extracellular volume due to the deposition of collagen and matrix proteins [12]. Based on these theories, we evaluated the efficacy of preoperative CT–derived ECV in predicting PHLF after hepatectomy for patients with HCC. CT–derived ECV as an independent and crucial predictor was integrated into the nomogram in our study. A higher ECV means a higher risk for PHLF in patients with resectable HCC.
Serum Alb and serum Tbil were both independent predictors for PHLF in our study, which was consistent with previous studies [20, 22, 23]. These two parameters are well-known indicators of liver function. In line with this, some previous studies have shown that impaired preoperative liver function and potential liver disease are important predictors of postoperative liver function impairment [24, 25]. In the present study, hepatic inflow occlusion duration, a factor in surgery, was identified as a significant predictor of PHLF by univariate analysis, while it was not included as a final independent predictor. The longer the hepatic inflow occlusion duration, the higher the risk for PHLF in HCC patients. During surgery, even though hepatic inflow occlusion is helpful in controlling bleeding, repeated hilar blocking and opening can lead to hepatic ischemia–reperfusion injury and thus increase the risk of PHLF. The reason why it was not included among the final independent predictors may be that the strong discrimination ability of the selected CT–derived ECV, serum Alb, and serum Tbil diminished the contribution of hepatic inflow occlusion duration in the final nomogram. Our result is different from that of a previous study by Shen et al [26]. Their study showed that hepatic inflow occlusion was not associated with PHLF in patients with HCC. The reasons may be that, on the one hand, hepatic inflow occlusion in their study was a categorical variable (yes/no), and the quantitative data in our study; on the other hand, the samples of the two studies are different in the present study; the ALBI score was an independent predictor of PHLF. This was in accordance with the study reported by Zou et al [9], which also showed that the ALBI score was a predictor of PHLF. The AUC of the ALBI score for PHLF prediction was 0.708 in our study, which was near the 0.745 published by Zou et al [9]. Zou et al also found that the MELD score and Child–Pugh stage could predict PHLF with AUCs of 0.649 and 0.665, respectively. However, our study demonstrated that the MELD score and Child–Pugh stage failed to predict PHLF. The following factors may explain the different results. First, the MELD score was determined based on serum INR, Cr, and Tbil according to the formula. Although serum Tbil was different between patients with and without PHLF in our study, the absence of differences in serum INR and Cr between patients with and without PHLF may lead to the failure of the MELD score to predict PHLF. Second, our study population consisted of patients with resectable HCC; thus, the preoperative baseline Child–Pugh stage of these patients was mostly grade A/B (grade A dominated). This may be one reason why the Child–Pugh stage did not show a significant difference in our study.
The performance of our nomogram was superior to the clinical models both in the training and validation cohorts (0.828 vs. 0.708, p = 0.004; 0.821 vs. 0.630, p < 0.001, respectively). The calibration curve showed that the predicted value of the nomogram was in good agreement with the actual observed. Shen et al [26] also constructed a nomogram in predicting PHLF with a C-index of 0.818 and 0.906 in the training and externally validated cohort, respectively. Their study included volumetric data (future liver remnant (FLR) ratio, spleen volume/FLR), the generation of these parameters needed the help of additional post-processing software, and the process was time consuming. Several studies [20, 27, 28] have shown that preoperative liver stiffness (LS) derived from ultrasound elastography imaging is a reliable predictor of PHLF. However, ultrasound-derived LS measurement requires not only well-trained operators but also other factors that must be controlled, such as abdominal obesity/body mass index [29], liver inflammatory activity, and adverse effects of abnormal bilirubin or transaminase [30, 31]. CT–derived ECV in our nomogram is easy to operate, has low requirements for operators, and has good reliability [17]. Meanwhile, our nomogram is a simple method, which does not add any additional examination to those already performed in routine.
This study still had several limitations. First, it was a retrospective study. Second, it was based on two centers in Chongqing, China, and the population sample was relatively limited. To further verify the clinical reliability and effectiveness of the proposed nomogram in this study, more centers and larger samples from different regions and countries are needed. Third, the proposed nomogram in this study was only compared with clinical models (including blood biochemical indices), and other indices (LS based on ultrasound, residual liver volume, and MR–based indices, among others) need to be added for further comparison and demonstration. Fourth, patients with PHLF were not further classified in detail (grade A/B/C) in this study. Due to the small number of cases, the data after classification and grouping were seriously unbalanced, and most patients were grade A or B.
Conclusions
The proposed novel nomogram, combined with CT–derived ECV, serum Alb, and serum Tbil, showed superior prediction of PHLF in patients with resectable HCC than the Child–Pugh stage, MELD score, and ALBI score. As a feasible and promising noninvasive tool, this nomogram may provide a new strategy for the preoperative prediction of PHLF.
Abbreviations
- Alb:
-
Albumin
- ALBI:
-
Albumin–bilirubin
- AUC:
-
Area under the curve
- CT:
-
Computed tomography
- ECV:
-
Extracellular volume
- EP:
-
Equilibrium phase
- HCC:
-
Hepatocellular carcinoma
- Hct:
-
Hematocrit
- ISGLS:
-
International Study Group of Liver Surgery
- MELD:
-
Model for End-Stage Liver Disease
- PHLF:
-
Post-hepatectomy liver failure
- ROC:
-
Receiver operator characteristic
- ROI:
-
Region of interest
- Tbil:
-
Total bilirubin
References
Dhir M, Melin AA, Douaiher J et al (2016) A review and update of treatment options and controversies in the management of hepatocellular carcinoma. Ann Surg 263:1112–1125
Farges O, Malassagne B, Flejou JF, Balzan S, Sauvanet A, Belghiti J (1999) Risk of major liver resection in patients with underlying chronic liver disease: a reappraisal. Ann Surg 229:210–215
Mullen JT, Ribero D, Reddy SK et al (2007) Hepatic insufficiency and mortality in 1,059 noncirrhotic patients undergoing major hepatectomy. J Am Coll Surg 204:854–862 discussion 862-854
Rahbari NN, Garden OJ, Padbury R et al (2011) Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 149:713–724
Gilg S, Sandstrom P, Rizell M et al (2018) The impact of post-hepatectomy liver failure on mortality: a population-based study. Scand J Gastroenterol 53:1335–1339
Soreide JA, Deshpande R (2021) Post hepatectomy liver failure (PHLF) - recent advances in prevention and clinical management. Eur J Surg Oncol 47:216–224
Tsujita Y, Sofue K, Komatsu S et al (2020) Prediction of post-hepatectomy liver failure using gadoxetic acid-enhanced magnetic resonance imaging for hepatocellular carcinoma with portal vein invasion. Eur J Radiol 130:109189
van den Broek MA, Olde Damink SW, Dejong CH et al (2008) Liver failure after partial hepatic resection: definition, pathophysiology, risk factors and treatment. Liver Int 28:767–780
Zou H, Yang X, Li QL, Zhou QX, Xiong L, Wen Y (2018) A comparative study of albumin-bilirubin score with Child-Pugh score, Model for End-Stage Liver Disease score and indocyanine green R15 in predicting posthepatectomy liver failure for hepatocellular carcinoma patients. Dig Dis 36:236–243
European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L (2018) EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 69:182–236
Korean Liver Cancer Association (KLCA); National Cancer Center (NCC), Goyang, Korea (2019) 2018 Korean Liver Cancer Association-National Cancer Center Korea practice guidelines for the management of hepatocellular carcinoma. Korean J Radiol 20:1042–1113
Varenika V, Fu Y, Maher JJ et al (2013) Hepatic fibrosis: evaluation with semiquantitative contrast-enhanced CT. Radiology 266:151–158
Bandula S, Punwani S, Rosenberg WM et al (2015) Equilibrium contrast-enhanced CT imaging to evaluate hepatic fibrosis: initial validation by comparison with histopathologic sampling. Radiology 275:136–143
Shinagawa Y, Sakamoto K, Sato K, Ito E, Urakawa H, Yoshimitsu K (2018) Usefulness of new subtraction algorithm in estimating degree of liver fibrosis by calculating extracellular volume fraction obtained from routine liver CT protocol equilibrium phase data: preliminary experience. Eur J Radiol 103:99–104
Bak S, Kim JE, Bae K et al (2020) Quantification of liver extracellular volume using dual-energy CT: utility for prediction of liver-related events in cirrhosis. Eur Radiol 30:5317–5326
Yoon JH, Lee JM, Kim JH et al (2021) Hepatic fibrosis grading with extracellular volume fraction from iodine mapping in spectral liver CT. Eur J Radiol 137:109604
Guo SL, Su LN, Zhai YN et al (2017) The clinical value of hepatic extracellular volume fraction using routine multiphasic contrast-enhanced liver CT for staging liver fibrosis. Clin Radiol 72:242–246
Zhang Z, Ouyang G, Wang P et al (2021) Safe standard remnant liver volume after hepatectomy in HCC patients in different stages of hepatic fibrosis. BMC Surg 21:57
Feng JW, Qu Z, Wu BQ, Sun DL, Jiang Y (2019) The preoperative fibrosis score 4 predicts posthepatectomy liver failure in patients with hepatocellular carcinoma. Ann Hepatol 18:701–707
Hu H, Han H, Han XK, Wang WP, Ding H (2018) Nomogram for individualised prediction of liver failure risk after hepatectomy in patients with resectable hepatocellular carcinoma: the evidence from ultrasound data. Eur Radiol 28:877–885
Reddy SK, Barbas AS, Turley RS et al (2011) A standard definition of major hepatectomy: resection of four or more liver segments. HPB (Oxford) 13:494–502
Motoyama H, Kobayashi A, Yokoyama T et al (2014) Liver failure after hepatocellular carcinoma surgery. Langenbecks Arch Surg 399:1047–1055
Kong FH, Miao XY, Zou H et al (2019) End-stage liver disease score and future liver remnant volume predict post-hepatectomy liver failure in hepatocellular carcinoma. World J Clin Cases 7:3734–3741
Kubota K, Makuuchi M, Kusaka K et al (1997) Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology 26:1176–1181
Yang T, Zhang J, Lu JH, Yang GS, Wu MC, Yu WF (2011) Risk factors influencing postoperative outcomes of major hepatic resection of hepatocellular carcinoma for patients with underlying liver diseases. World J Surg 35:2073–2082
Shen YN, Tang TY, Yao WY et al (2019) A nomogram for prediction of posthepatectomy liver failure in patients with hepatocellular carcinoma: a retrospective study. Medicine (Baltimore) 98:e18490
Cescon M, Colecchia A, Cucchetti A et al (2012) Value of transient elastography measured with FibroScan in predicting the outcome of hepatic resection for hepatocellular carcinoma. Ann Surg 256:706–712 discussion 712-703
Shen Y, Zhou C, Zhu G et al (2017) Liver stiffness assessed by shear wave elastography predicts postoperative liver failure in patients with hepatocellular carcinoma. J Gastrointest Surg 21:1471–1479
Castera L, Foucher J, Bernard PH et al (2010) Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology 51:828–835
Arena U, Vizzutti F, Corti G et al (2008) Acute viral hepatitis increases liver stiffness values measured by transient elastography. Hepatology 47:380–384
Liang XE, Chen YP, Zhang Q, Dai L, Zhu YF, Hou JL (2011) Dynamic evaluation of liver stiffness measurement to improve diagnostic accuracy of liver cirrhosis in patients with chronic hepatitis B acute exacerbation. J Viral Hepat 18:884–891
Acknowledgements
We would like thank all the participants of this study.
Funding
This study has received funding from the National Natural Science Foundation of China (Grant No. 82071883), the combination projects of medicine and engineering of the Fundamental Research Funds for the Central Universities in 2019 (Project No. 2019CDYGYB008), and the Chongqing key medical research project of a combination of science and medicine (Grant No. 2021MSXM077).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Jiuquan Zhang, from the Department of Radiology, Chongqing University Cancer Hospital & Chongqing Cancer Institute & Chongqing Cancer Hospital, Chongqing, People’s Republic of China, email: zhangjq_radiol@foxmail.com.
Conflict of interest
One of the authors (Xiaoyue Zhang) of this manuscript is an employee of Siemens Healthineers. The remaining authors declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approvals of the two participating hospitals were obtained.
Methodology
retrospective
diagnostic or prognostic study
multicenter study
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Figure S1.
Handcrafted ROIs diagram and calculation process of the CT-derived ECV. A 39-year-old man with HCC, underwent a major hepatectomy (resection of right lobe and caudate lobe of liver) and with a known of Hct value was 47%. In the preoperative baseline nonenhanced (A-C) and EP enhanced (D-F) images, handcrafted ROIs were drawn along the margins of the future remnant liver, and circular ROIs were drawn in the abdominal aorta on the same plane. ROIs were placed on three cross-sections, including intrahepatic inferior vena cava confluence (A, D), portal hilum (B, E) and gallbladder fossa (C, F). The ECV values of the section at intrahepatic inferior vena cava confluence (ECV1), portal hilum (ECV2) and gallbladder fossa (ECV3) were calculated by the formula shown in the figure, respectively. Then the CT-derived ECV for the patient (ECV = 33.00) was the mean value of ECV1, ECV2 and ECV3. ROI, region of interest; CT, computed tomography; ECV, extracellular volume; HCC, hepatocellular carcinoma; EP, equilibrium phase; Hct, hematocrit. (PNG 9760 kb)
Figure S2.
Bland–Altman plots of the CT-derived ECV differences measured by radiologist 1 with an interval of 4 weeks (A, C), and radiologist 1/2 (B, D). A/B and C/D were for the training and validation cohort, respectively. These Bland–Altman plots showed good agreement. CT, computed tomography; ECV, extracellular volume. (PNG 265 kb)
Figure S3.
Two examples of clinical application of our nomogram. (A) a 51-year-old man with resectable HCC, the point of CT-derived ECV (22.00), serum Alb (38.00 g/L) and serum Tbil (18.98 μmol/L) were indicated by orange dotted lines, then the total point of this patient was indicated by red dotted line, indicating that the risk of PHLF in this patient was much less than 35%. (B) a 64-year-old man with resectable HCC, the point of CT-derived ECV (27.01), serum Alb (33.61 g/L) and serum Tbil (131.13 μmol/L) were indicated by orange dotted lines, then the total point of this patient was indicated by red dotted line, indicating that the risk of PHLF in this patient was exceeded 85%. Therefore, this patient should consider a new strategy for clinical treatment. HCC, hepatocellular carcinoma; CT, computed tomography; ECV, extracellular volume; Alb, albumin; Tbil, total bilirubin; PHLF, post-hepatectomy liver failure. (PNG 543 kb)
ESM 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Peng, Y., Shen, H., Tang, H. et al. Nomogram based on CT–derived extracellular volume for the prediction of post-hepatectomy liver failure in patients with resectable hepatocellular carcinoma. Eur Radiol 32, 8529–8539 (2022). https://doi.org/10.1007/s00330-022-08917-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-022-08917-x