
Abstract
Background and Aims
Prior to the consensus guideline conference in 2007, eosinophilic esophagitis (EoE) was uncommon dominated by the fibrostenotic phenotype, but over the past decade has become a common cause of dysphagia with more inflammatory phenotypes diagnosed. We assessed the impact of guideline definitions on the characteristics of EoE phenotypes over the past 26 years at our institution.
Methods
We reviewed the electronic health record of 75 consecutive patients meeting guideline definition EoE from 1/1988 to 5/2014. We separated groups based on 5-year intervals of diagnosis and phenotype. For continuous data, results were summarized as mean difference and standard deviation with 95 % confidence intervals.
Results
Five groups based on 5-year intervals of diagnosis were identified: group 1—1988–1993 (n = 7), group 2—1994–1999 (n = 7), group 3—2000–2005 (n = 4), group 4—2006–2011 (n = 35), and group 5—2012–2014 (n = 22). Prior to 2000, all patients were diagnosed with fibrostenotic EoE. After the initial 2007 guideline conference, inflammatory EoE has predominated with only one-third diagnosed with fibrostenotic EoE. Prior to 2011, only two were diagnosed with PPI-REE. In the last 3 years, 8 out of 22 patients (32 %) had PPI-REE. Overall, 8 out of 10 (80 %) PPI-REE were the inflammatory phenotype. When comparing pre- (n = 18) and post (n = 57)-consensus definitions, there was a significant difference between age of diagnosis (30.710.2 vs. 41.3 ± 14.3; p = 0.001), age of symptom onset (18.4 +/15.2 vs. 32.4 ± 15.5), and initial esophageal diameter (10.5 ± 2.7 vs. 14.3 ± 4.2; p < 0.0001), respectively.
Conclusions
Fibrostenotic EoE has steadily decreased, and inflammatory EoE is now the most recognized form. Across our 26-year experience, there was a decrease in delay in diagnosis and severity of esophageal stricture. The pivotal change occurred around 2007 corresponding to the first EoE guideline emphasizing the impact and importance of early detection of disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The historical naming of eosinophilic esophagitis (EoE) has evolved from various aliases over the past several decades including ringed esophagus, corrugated esophagus, feline esophagus, small caliber esophagus, and congenital esophageal stenosis (CES) [1–6]. The term “eosinophilic esophagitis” was first reported into the literature in 1978 with most physicians at the time uncertain whether EoE represented a congenital disease or another form of GERD [7]. Case series thereafter began to differentiate EoE from other diseases and defined distinct characteristics of the disease. The histologic and phenotypic description of the disease was first described by Attwood [8] and later by Straumann [9]. As larger cohorts reported natural history data [10–14], consensus guideline definitions evolved [15, 16]. The first consensus guidelines published in 2007 distinguished gastroesophageal reflux disease (GERD) from EoE [15]. However, after Ngo et al. [17] reported a case series of three patients responding endoscopically and histologically to PPI therapy, a new form of the disease evolved, termed “PPI-responsive esophageal eosinophilia (PPI-REE).” According to the second EoE consensus statement published in 2011, “EoE is a clinicopathological diagnosis defined as symptoms related to esophageal dysfunction, >15 eosinophils per high-power field, eosinophilia that persists after a trial of PPI therapy, and exclusion of other secondary causes of esophageal eosinophilia” [16].
EoE is currently considered the most common cause of food impaction in young adult and adolescent patients, and second leading cause of chronic esophagitis behind GERD [16]. One prospectively collected study of patients undergoing endoscopy with routine esophageal biopsies reported over 40 % of subjects with dysphagia and 4 % without dysphagia meeting the current histologic definition of EoE (>15 eos/hpf) [18]. One recent review evaluates the previously published epidemiology studies of EoE and estimates the prevalence in the general population to range from 0.5 to 1 case/1,000 persons; the incidence was approximated at 1 out of 10,000 new cases per year and concluded the incidence to be outpacing the increases in recognition [19].
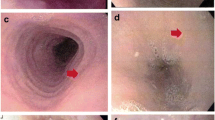
Endoscopically, the features of EoE are quite variable with at least two forms, an inflammatory and a fibrostenotic phenotype [20, 21]. Normal esophageal diameter, edema, whitish exudates, and linear furrows constitute the inflammatory phenotype, whereas fixed rings, narrowing, and esophageal strictures characterize the fibrostenotic phenotype [20–22]. Most patients present with mixed features of these two phenotypes endoscopically [23, 24].
Due to the scarcity in the literature of EoE case series detailing the clinical and phenotypic presentation over time, we retrospectively reviewed our database of EoE patients diagnosed over the past 26 years at the University of South Florida (USF) to assess the potential impact of guideline definitions on disease recognition and separation into inflammatory and fibrostenotic phenotypes.
Methods
Data
For this retrospective cohort study, Institutional Review Board approval was obtained from the University of South Florida (#00008547). All consecutive patients treated between 1988 and 2014 were included from a database of patients who met consensus definition of eosinophilic esophagitis at the University of South Florida Joy McCann Culverhouse Center for Swallowing Disorders in Tampa, Florida. This is a predominantly white patient population found in an urban area serving approximately 2 million people on the central west coast of Florida. All patients experienced the symptoms of esophageal dysfunction, >15 eos/hpf on esophageal biopsy, and did not respond to a 2-month trial of proton pump inhibitor [16]. In addition, other causes of esophageal eosinophilia were ruled out such as GERD, collagen vascular disease, autoimmune processes, or infections. All patients in this database were adults, 18 years or older when first seen in the Swallowing Center.
Data were extracted from patient charts through electronic medical records including patient encounters, endoscopy reports, and pathology records. Information included demographics (age, sex, race), past medical history, age of symptom onset, age of diagnosis, symptom presentation, and time of diagnosis. Delay in diagnosis was defined by subtracting the pre-diagnosis symptom from the time of EoE diagnosis.
Esophageal characteristics during endoscopy were recorded, i.e., edema, exudates, furrows, rings, and narrowing/strictures. As per our Swallowing Center protocols, all patients with any type of dysphagia undergo careful graduated esophageal dilation at their first endoscopy. Esophageal diameter was recorded using the smallest bougie with moderate resistance noted during either Maloney or Savory-Guilliard bougie dilation. We prefer to dilate our EoE patients with bougies rather than through-the-scope balloons and do not look for mucosal tears during or after the procedure. The passage of each dilator is graded for subjective resistance as 0—none, 1—minimal, 2—moderate, and 3—extensive resistance and recorded in the endoscopy record. We chose “moderate” resistance to estimate esophageal diameter realizing it may overestimate stricture size, but eliminates the mild resistance sometimes noted with passage over guide wires or from the bite block. Although subjective, we are confident this technique is more precise than gauging stricture size on the diameter of the endoscope alone.
Pathology reports were reviewed by one of two pathologists experienced with diagnosing EoE and recorded based on location and eosinophil counts (400×, area 0.4 mm2 per HPF) with the highest density for each biopsy used. Biopsies from patients prior to 2007 EoE guidelines were reviewed retrospectively and previously referenced [25].
Phenotype Definitions
The inflammatory phenotype was defined by an esophageal diameter >17 mm (smallest bougie with moderate resistance during dilation) and primary endoscopic characteristics of edema, furrows, or exudates [26]. In contrast, the fibrostenotic group had primarily rings/strictures on endoscopy and diameter <17 mm. The cut point for esophageal diameter was set at 17 mm as patients can normally eat a regular diet above this size [27]. PPI-REE was defined using 2011 guideline definitions as patients responding to a PPI dose of 20–40 mg once or twice daily for 8–12 weeks dependent on the patient and chosen PPI [16]. “Responders” were defined as <15 eos/hpf on esophageal biopsy after an 8- to 12-week PPI trial.
Statistical Analysis
The association between dependent and independent variables was assessed using either an independent t test in case of binary and continuous variable and Chi-square test for dichotomous variables comparing pre- and post-first EoE consensus conference diagnosed EoE. For continuous data, the results were summarized as mean difference (MD) and standard deviation (SD). For dichotomous data, results are summarized using odds ratio (OR) and 95 % confidence intervals (CI). The statistical significance was set at 5 %. All data analyses were performed using SPSS version 22.
Results
Population
Seventy-five adult patients met consensus guideline definition for EoE identified between January 1988 and May 2014. The population consisted of 73.3 % males (55/75) with a mean age of 44.2 years and mean age of diagnosis of 38.7 years. The average follow-up on our patients was 5.4 years. Twenty-four percent (18/75) of our patients were diagnosed prior to the first consensus conference meeting.
Patient Characteristics
Table 1 displays the patient characteristics broken into 5-year intervals over 26 years. Of note, there appears to be a linear increase in age of diagnosis with each 5-year increment in decade of diagnosis. In general, age of symptom onset occurred at a younger age in the earlier 5-year intervals compared to the post-consensus years: 14.2 years old (1988–1993) trending upward to 35.7 years old during the more recent time (2012–2014). Delay in diagnosis appeared to decrease overtime with an average delay of 14.2 years (1988–1993) compared to 7.4 years during the 2012–2014 time span. The diameter of the esophagus at the time of diagnosis was less narrowed by 2–3 mm in the more recent time span (2012–2014).
Impact of Consensus Guidelines
There were 18 patients diagnosed prior to the first consensus guideline published in 2007 versus 57 diagnosed subsequently (Table 2). There was a statistically significant change in age of symptom onset when comparing pre- and post-consensus guideline diagnosed patients 18.4 ± 15.2 versus 32.4 ± 15.5 MD 14.0 (95 % CI 5.5–22.4); p = 0.002), respectively. Similarly, age of diagnosis was also significantly different between the two groups 41.3 ± 14.3 versus 30.7 ± 10.2 MD 10.6 (95 % CI 4.4, 16.7; p = 0.001), respectively. Delay in diagnosis was longer in the pre-consensus group, although this did not reach statistical significance 12.3 ± 7.7 versus 8.2 ± 8.9 MD −4.1 (−8.5, 0.34; p = 0.07). The average esophageal diameter of patients diagnosed prior to 2006 was 10.5 ± 2.7 versus 14.3 ± 4.2 mm after recommendations MD 3.8 (95 % CI 2.1–5.5; p < 0.0001). Neither BMI nor eosinophil count/hpf (initial or highest count) appeared to change significantly after initial guidelines.
Evolution of Frequency of EoE Phenotypes and PPI-REE
Prior to 2000, all patients seen in our clinic were diagnosed with the fibrostenotic phenotype. The inflammatory phenotype increased from 25 % in year 2000–2005 to 45.7 % in year 2006–2011 after the initial guideline definitions.
Similarly, PPI-REE was not diagnosed prior to 2006, only appearing in a small percentage 8.6 % from 2006 to 2011 compared to 31.8 % after 2012 (see Fig. 1). The trend was statistically significant for all comparisons (p < 0.0001). Overall, 8 out of 10 (80 %) of PPI-REE were of the inflammatory phenotype.

Phenotype incidence at diagnosis separated in 5-year intervals
Discussion
The standard definition of a “Clinical Practice Guideline” was first described by Field and Lohr in 1990 as: “Systematically developed statements to assist practitioners and patient decisions about appropriate health care for specific circumstances.” [28] The purpose of guidelines was to help focus appropriate management, highlight the inappropriate variations in standard practices, and bring forth short comings in the existing literature to generate future research.
For eosinophilic esophagitis, the most problematic delay in forming initial diagnostic and treatment guidelines was the limited understanding, sparse recognition, and lack of uniform criteria to define the disease. The North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition held the First International Gastrointestinal Eosinophil Research Symposium in 2006 at Digestive Disease Week in Orlando, Florida. Later, in 2007, the first consensus recommendations were published, focusing on the clinical experiences of a multidisciplinary team of experts, both clinicians and scientists [15]. Since then, many large prospectively collected studies were published, as well as clinical drug trials strengthening the knowledge of a chronic progressive disease with limited treatment options. After the initial recommendations in 2007, three more guidelines were published based on well-designed prospective studies with fewer flaws and biases [16, 29, 30].
Isolated endoscopic case reports of patients with an EoE like syndrome were first reported as early as the 1960s and 1970s [7, 31, 32]. In 1989, Attwood et al. [33] published an abstract in Gut reporting on a group of 15 adults presenting with dysphagia and normal pH tests displaying markedly elevated eosinophil counts, which they named “esophageal asthma.” The histologic and phenotypic description of the disease was first described and published by Attwood et al. [8] in 1993 and later by Straumann et al. [9] in 1994. Straumann called this new disease “idiopathic EoE.”
As the primary esophageal center in Florida, we began to see along this same time line a similar group of patients (mostly white men) with complaints of debilitating dysphagia, frequent food impactions, and endoscopic findings characterized by multiple rings, generalized narrowing, and strictures. Dr H. Worth Boyce called these patients “congenital esophageal stenosis.” Their endoscopic/X-ray features resembled a known pediatric disease associated with fixed esophageal strictures and trachealization, the result of residual tracheobronchial tissue remaining in the esophagus from incomplete esophageal and tracheal separation [1]. During this period, biopsies were primarily obtained from the distal esophagus looking for BE and dysplasia and selectively from ringed/strictured areas. Our pathologists consistently read these biopsies as histology compatible with “reflux esophagitis” or “reflux esophagitis with eosinophilia.” [14, 25] Therefore, patients were treated like complicated GERD strictures with PPIs and esophageal dilation, as other options in adult patients were unknown with no guidelines.
We believe the key to early detection of EoE in adults evolved from the 2007 EoE guidelines where the histologic number of eosinophils required for diagnosis (>15 eosinophils/HPF) and multiple biopsies became a part of standard practice [15, 16]. Prior to this time, the common teaching was that eosinophils were a marker of severe GERD [34, 35]. This was based on the investigation published in 1982 by Winters et al. [36] showing in a cohort of patients undergoing esophageal pH testing that prolonged acid reflux correlated with the proximal extent of eosinophils.
Pediatric gastroenterologists began in the early 1990s to take random biopsies from the proximal and distal esophagus, recognizing that inflammatory diseases could be found despite normal appearance to the mucosa [11, 37]. Likely, this contributed to this earlier recognition of EoE than their adult colleagues [11, 12]. After the consensus guidelines in 2007, adult gastroenterologists began to follow the same practice, and simultaneously pathologists increasingly made the diagnosis of EoE. Our review at USF of biopsies from the pre-2006 era confirmed the histologic criteria for EoE in all our patients with “congenital esophageal stenosis” [14] and subsequently the delay in diagnosis decreased by over 4 years after the consensus guidelines (Table 2).
Many articles in the early 2000s began to focus on the clinicopathological characteristics of EoE. Endoscopic features associated with EoE were described including exudate, furrows, crepe paper esophagus, fixed rings, strictures, and narrowed caliber esophagus [38–40]. Subsequently, the features of EoE began to be described as two phenotypic forms: one with primary endoscopic features of esophageal edema, exudates, and linear furrows defining the inflammatory phenotype, and the second termed fibrostenotic, which was associated with esophageal strictures and fixed rings [20, 41].
At USF, we primarily recognized the fibrostenotic phenotype prior to 2005. This phenomenon may have been a referral bias as many physicians did not know how to treat these patients as well as the inflammatory features of EoE were poorly defined and probably confused with reflux esophagitis. However, the inflammatory phenotype evolved as a common presentation after the 2007 guidelines with recognition of these endoscopic features confirmed by multiple biopsies and histology. The inflammatory phenotype increased from 26 % in those diagnosed with EoE from 2000 to 2005 to around 46 % over the 2006–2011 time span with a reciprocal drop in the percentage of patients presenting with the fibrostenotic phenotype. As shown in Fig. 1, both trends were significant. This is similar to the experience at the University of North Carolina where unpublished data showed only 12 % of patients after 2011 were diagnosed with the fibrostenotic phenotype, 29 % inflammatory, and 59 % mixed compared to 2001 when the fibrostenotic form represented 50 % of cases [42].
Owing to the EoE guidelines, patients are now being recognized earlier with shorter delays in diagnosis. As shown in our 26-year experience, this had a major impact on the severity of esophageal strictures at presentation in our EoE patients. The average esophageal diameter was approximately 10 mm prior to the first consensus guidelines. Over the last 8 years, the average esophageal diameter significantly increased to over 14 mm, despite the degree of mucosal eosinophilia not significantly changing (Table 2). As first suggested by Schoepfer, early diagnosis and treatment interrupts the chronic sequela of eosinophilia inflammation with resulting subepithelial fibrosis [43].
The first consensus guidelines in 2007 distinguished GERD from EoE, but after Ngo et al. [17] first reported a case series of three patients responding endoscopically and histologically to PPI therapy in 2006, the coexisting relationship between the two diseases began to evolve. Several later studies confirmed the existence of patients with clinical symptoms of dysphagia and food impaction and eosinophilia responsive to PPI BID therapy highlighting this newly recognized form of EoE termed “PPI-responsive esophageal eosinophilia.” [44–46] Before 2006 at USF, these patients were given the diagnosis of GERD. Over the next 7 years, patients with PPI-REE tripled from 9 to 32 % after 2012. This is similar to the histologic remission rates currently reported in the literature after a trial of PPI therapy ranging between 33 and 61 % [18, 46–51].
Limitations of this study include the retrospective nature of this study, as well as the difficulty in separating true changes in the disease presentation of EoE (i.e., a shift from fibrostenotic to inflammatory) from changes related to different reporting of previously existing findings based on increased awareness and, potentially, on improved scope optics/imaging/technology. Strengths include a 26-year observation period of EoE and the steady change in phenotype over this time frame.
Conclusions
Before the consensus guideline recommendations in 2007, early detection of EoE prior to severe esophageal stricturing was uncommon. Over the past decade, EoE has become a common cause of dysphagia with the inflammatory disease predominating as the primary phenotype seen at the time of diagnosis. Treatments have improved, and one-third of patients experienced resolution of their eosinophilia with BID PPIs. Our study has assessed the impact of guideline definitions on EoE patients over the past 26 years at our institution and demonstrates the success of the immense research focused on a relatively new disease.
References
Morrow JB, Vargo JJ, Goldblum JR, et al. The ringed esophagus: histological features of GERD. Am J Gastroenterol. 2001;96:984–989.
Langdon DE. Corrugated ringed esophagus. Am J Gastroenterol. 1993;88:1461.
McKinley MJ, Eisner TD, Fisher ML, et al. Multiple rings of the esophagus associated with gastroesophageal reflux [case report]. Am J Gastroenterol. 1996;91:574–576.
Potter JW, Saeian K, Staff D, et al. Eosinophilic esophagitis in adults: an emerging problem with unique esophageal features. Gastrointest Endosc. 2004;59:355–361.
Rencken IO, Heyman MB, Perr HA, et al. Ringed esophagus (feline esophagus) in childhood. Pediatr Radiol. 1997;27:773–775.
Langdon DE. “Congenital” esophageal stenosis, corrugated ringed esophagus, and eosinophilic esophagitis. Am J Gastroenterol. 2000;95:2123–2124.
Landres RT, Kuster GG, Strum WB. Eosinophilic esophagitis in a patient with vigorous achalasia. Gastroenterology. 1978;74:1298–1301.
Attwood SE, Smyrk TC, Demeester TR, et al. Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome. Dig Dis Sci. 1993;38:109–116.
Straumann A, Spichtin HP, Bernoulli R, et al. Idiopathic eosinophilic esophagitis: a frequently overlooked disease with typical clinical aspects and discrete endoscopic findings. Schweiz Med Wochenschr. 1994;124:1419–1429.
Straumann A, Spichtin HP, Grize L, et al. Natural history of primary eosinophilic esophagitis: a follow-up of 30 adult patients for up to 11.5 years. Gastroenterology. 2003;125:1660–1669.
Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis: a 10-year experience in 381 children. Clin Gastroenterol Hepatol. 2005;3:1198–1206.
Assa’ad AH, Putnam PE, Collins MH, et al. Pediatric patients with eosinophilic esophagitis: an 8-year follow-up. J Allergy Clin Immunol. 2007;119:731–738.
Spergel JM, Brown-Whitehorn TF, Beausoleil JL, et al. 14 years of eosinophilic esophagitis: clinical features and prognosis. J Pediatr Gastroenterol Nutr. 2009;48:30–36.
Lipka S, Keshishian J, Boyce HW, et al. The natural history of steroid-naive eosinophilic esophagitis in adults treated with endoscopic dilation and proton pump inhibitor therapy over a mean duration of nearly 14 years. Gastrointest Endosc. 2014;80:592–598.
Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133:1342–1363.
Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3.e6–20.e6 (quiz 21–22).
Ngo P, Furuta GT, Antonioli DA, et al. Eosinophils in the esophagus–peptic or allergic eosinophilic esophagitis? Case series of three patients with esophageal eosinophilia. Am J Gastroenterol. 2006;101:1666–1670.
Dellon ES, Speck O, Woodward K, et al. Clinical and endoscopic characteristics do not reliably differentiate PPI-responsive esophageal eosinophilia and eosinophilic esophagitis in patients undergoing upper endoscopy: a prospective cohort study. Am J Gastroenterol. 2013;108:1854–1860.
Dellon ES. Epidemiology of eosinophilic esophagitis. Gastroenterol Clin North Am. 2014;43:201–218.
Bohm ME, Richter JE. Review article: oesophageal dilation in adults with eosinophilic oesophagitis. Aliment Pharmacol Ther. 2011;33:748–757.
Almansa C, Stark ME, DeVault KR, et al. S1071 Eosinophilic esophageal infiltration in PPI responsive versus steroid responsive patients: are there phenotypic differences? Gastroenterology. 2012;138:S-172.
Fox VL. Eosinophilic esophagitis: endoscopic findings. Gastrointest Endosc Clin N Am.. 2008;18:45–57. (viii).
Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3.e6–20.e6.
Straumann A, Aceves SS, Blanchard C, et al. Pediatric and adult eosinophilic esophagitis: similarities and differences. Allergy. 2012;67:477–490.
Keshishian J, Vrcel V, Boyce HW, et al. Eosinophilic esophagitis: a paradigm shift for pathology. J Clin Gastroenterol. 2014;48:607–612.
Hirano I, Moy N, Heckman MG, et al. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. 2013;62:489–495.
Goldschmid S, Boyce HW Jr, Brown JI, et al. A new objective measurement of esophageal lumen patency. Am J Gastroenterol. 1989;84:1255–1258.
Field MJ, Lohr K. Guidelines for Clinical Practice: From Development to Use. Washington, DC: Institute of Medicine, National Academy Press; 1992.
Dellon ES, Gonsalves N, Hirano I, et al. ACG clinical guideline: evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013;108:679–692. (quiz 693).
Papadopoulou A, Koletzko S, Heuschkel R, et al. Management guidelines of eosinophilic esophagitis in childhood. J Pediatr Gastroenterol Nutr. 2014;58:107–118.
Kelley ML Jr, Frazer JP. Symptomatic mid-esophageal webs. JAMA. 1966;197:143–146.
Shiflett DW, Gilliam JH, Wu WC, et al. Multiple esophageal webs. Gastroenterology. 1979;77:556–559.
Attwood SEST, Demeester TR. Eosinophilic asthma-episodic dysphagia with eosinophilic infiltrates. Gut. 1989;30:A1493.
Biller JA, Winter HS, Grand RJ, et al. Are endoscopic changes predictive of histologic esophagitis in children? J Pediatr. 1983;103:215–218.
Brown LF, Goldman H, Antonioli DA. Intraepithelial eosinophils in endoscopic biopsies of adults with reflux esophagitis. Am J Surg Pathol. 1984;8:899–905.
Winter HS, Madara JL, Stafford RJ, et al. Intraepithelial eosinophils: a new diagnostic criterion for reflux esophagitis. Gastroenterology. 1982;83:818–823.
Franciosi JP, Fiorino K, Ruchelli E, et al. Changing indications for upper endoscopy in children during a 20-year period. J Pediatr Gastroenterol Nutr. 2010;51:443–447.
Remedios M, Campbell C, Jones DM, et al. Eosinophilic esophagitis in adults: clinical, endoscopic, histologic findings, and response to treatment with fluticasone propionate. Gastrointest. Endosc. 2006;63:3–12.
Croese J, Fairley SK, Masson JW, et al. Clinical and endoscopic features of eosinophilic esophagitis in adults. Gastrointest. Endosc. 2003;58:516–522.
Aceves SS, Newbury RO, Dohil R, et al. Distinguishing eosinophilic esophagitis in pediatric patients: clinical, endoscopic, and histologic features of an emerging disorder. J Clin Gastroenterol. 2007;41:252–256. doi:10.1097/01.mcg.0000212639.52359.f1.
Almansa CSM, DeVault K, et al. Eosinophilic esophageal infiltration in PPI response versus steroid responsive patients: are there phenotypic differences? In: Proceedings from the Digestive Disease Week Annual Meeting; May 1–5, 2010; New Orleans, LA. Abstract S1071.
Dellon ES, Kim HP, McConville S, et al. Su1847 Decreasing frequency of the fibrostenotic phenotype of eosinophilic esophagitis: time trends over the past decade. Gastroenterology. 2012;144:S-490.
Schoepfer AM, Safroneeva E, Bussmann C, et al. Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time-dependent manner. Gastroenterology. 2013;145:1230.e1-2–1236.e1-2.
Dranove JE, Horn DS, Davis MA, et al. Predictors of response to proton pump inhibitor therapy among children with significant esophageal eosinophilia. J Pediatr. 2009;154:96–100.
Sayej WN, Patel R, Baker RD, et al. Treatment with high-dose proton pump inhibitors helps distinguish eosinophilic esophagitis from noneosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2009;49:393–399.
Peterson KA, Thomas KL, Hilden K, et al. Comparison of esomeprazole to aerosolized, swallowed fluticasone for eosinophilic esophagitis. Dig Dis Sci. 2010;55:1313–1319.
Molina-Infante J, Ferrando-Lamana L, Ripoll C, et al. Esophageal eosinophilic infiltration responds to proton pump inhibition in most adults. Clin Gastroenterol Hepatol. 2011;9:110–117.
Abe Y, Iijima K, Ohara S, et al. A Japanese case series of 12 patients with esophageal eosinophilia. J Gastroenterol. 2011;46:25–30.
Francis DL, Foxx-Orenstein A, Arora AS, et al. Results of ambulatory pH monitoring do not reliably predict response to therapy in patients with eosinophilic oesophagitis. Aliment Pharmacol Ther. 2012;35:300–307.
Fujiwara Y, Sugawa T, Tanaka F, et al. A multicenter study on the prevalence of eosinophilic esophagitis and PPI-responsive esophageal eosinophilic infiltration. Intern Med. 2012;51:3235–3239.
Moawad FJ, Veerappan GR, Dias JA, et al. Randomized controlled trial comparing aerosolized swallowed fluticasone to esomeprazole for esophageal eosinophilia. Am J Gastroenterol. 2013;108:366–372.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lipka, S., Boyce, H.W., Kumar, A. et al. The Changing Faces of Eosinophilic Esophagitis: The Impact of Consensus Guidelines at the University of South Florida. Dig Dis Sci 60, 1572–1578 (2015). https://doi.org/10.1007/s10620-014-3517-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3517-4