
Abstract
This paper exhibits the outline and advancement of a pervasive remote monitoring system for the Parkinson’s disease (PD) patients. The proposed system gathers various PD related information such as voice samples, gait information etc. and would empower in-home monitoring of early PD symptoms. We accomplished this objective by utilizing various wearable sensors technology, mobile computing system, Internet, cloud computing technologies. Such an incorporated framework guarantees the compelling and effective utilization of data gathered for evaluating early PD symptom’s as well as identifies critical PD severity levels. In particular, the proposed system can evaluate PD patients’ voice disorders or Dysphonia and thus enables doctors to detect patient’s PD symptoms or severity levels. Trial comes about demonstrate that our proposed system achieves very high accuracy for detecting PD symptoms as compared to existing approaches.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Parkinson sickness (PD) is a standout amongst the most ceaseless and dynamic neurodegenerative human malady. It is the most predominant development issue of the focal sensory system, and influences around 3% of the populace beyond 65 years old on the planet [1]. It is accounted for that in US, the PD is basic among people of 65 years or more seasoned at the rate of 160/100,000 people. Parkinson’s disease is traditionally characterized on impossible to miss engine disintegration signs as solid inflexibility, tremors very still, bradykinesia, hypokinesia/akinesia and postural unsteadiness. Patients may likewise experience the ill effects of rearranging of step, solidifying of walk, and Dysphonia [2].
To manage and treat PD effectively, current approach requires regular clinical visits of PD patients for assessment and close monitoring of PD symptoms [3]. Assessment is subjective and generally conducted by the physician during a patient visit. However, it is hard to keep track of differentiation of PD symptoms (e.g. decline or improvement) between clinic visits. In addition, more frequent clinic visits may increase the physical and economic burden for PD patients and their families. Therefore, there is a need for remote monitoring systems for PD patients that can deal with above issues and support continuous follow-up of the disease. There are some active efforts to monitor PD patients by analyzing physical activity data, mostly about gait performance (e.g. walking, turning, running etc.) and hand tremors at rest from wearable [4,5,6,7,8,9] and environmental sensors [10,11,12,13,14] and Smartphone applications [2, 15,16,17,18].
The major limitations of the above works to monitor PD patients is related to PD symptoms detection, measurement and analysis. Much of the time, these were finished by the utilization of regulated systems that require human mediation [6, 10,11,12,13,14,15,16]. Many investigations [15,16,17,18,19,20] featured the difficulties of managed strategies in genuine situations as far as Human predisposition amid demonstrate articulation (naming and preparing stages). Hence, inquire about into a non-obtrusive and self-sufficient framework to gauge PD side effects continuously while enhancing long haul execution is required.
Because of late improvements of a few innovative advances and new ideas, for example, Internet of Things, Body Sensor Networks (BSNs), distributed computing and minimal effort remote information correspondence frameworks, unavoidable wellbeing administrations are expanding drastically that screen indispensable signs and physiological signs, including electrocardiograms and electromyography, with a few being advertised [21,22,23,24,25,26,27,28,29,30]. With the coordinated sensors in present day cell phones ending up more intense and less expensive, the plausibility and exactness of utilizing cell phones to quantify different development related measurements have pulled in a great deal of research intrigue. With these innovation advancement, it is achievable and exceptionally encouraging to expand PD checking from discontinuous facility based appraisal to the locally situated condition by utilizing current cell phone and intense distributed computing.
This goal is not new, but the adoption of newly arrived technologies, would be a great step towards the development of an effective and efficient real-time PD-patient monitoring system. In this paper, we propose a sensor-cloud framework for designing and implementing a continuous, non-invasive and wireless monitoring system for the PD patients that can collect PD patients voice data and detect PD symptoms and severity levels about PD and would enable home-based assessment and monitoring. We evaluated five classification techniques- Decision tree, Random tree, SVM, Naïve Bayes and KNN to classify the patient’s voice samples offline and found that Decision Tree was able to provide better recognition rate. If the system finds positive results of recognition of PD symptoms, it notifies the doctor or caregiver automatically and thus help to get possible quick recommendations from the doctor. Our long haul objective is to increase current PD evaluation situated in the center setting to the locally established condition. furthermore, enable patients and specialists with a novel inescapable figuring framework for persistent checking and administration of PD.
2 Related works
Given the attributes of Parkinson’s sickness and its difficulties on ailment administration, outlining mobile instruments for remote observing of PD patients has pulled in a great deal of consideration as of late [6,7,8,9,10, 19, 21,22,23]. In a current report, Rodriguez-Molinero et al utilized a versatile inertial sensor to distinguish engine vacillations (on-off) in PD patients, and the outcome indicated high affectability and specificity [15]. Regarding stride, there are three essential estimations of step: (1) drive based estimation, (2) precise rate estimation, and (3) accelerometer estimation Several accelerometer-based estimation frameworks for wandering observing of step related indications in PD have been accounted for in solidifying of stride identification, stance and strolling speed estimation, and fall hazard estimation [2, 4, 9, 12, 15]. Salarian et al [20] utilized body-appended spinners to assess walk highlights and physical exercises identified with PD. Be that as it may, their investigation did not report any outcome about how to utilize the assessed highlights to identify and evaluate PD seriousness. Patel et al, [9] in Harvard therapeutic school, utilized wearable accelerometers to assess engine difficulties on people with PD, and endeavored to predicate the clinicians’ appraisals of illness indications seriousness. In any case, their approach required patients to join a few sensors at various areas and furthermore required a different control module to transmit and store information. The prerequisite of these additional settings puts an extra weight on clients and declines the ease of use of the framework.
In general, the problems with current methods limit their long-term effectiveness to support real-time processing, storing, analyzing, visualizing, knowledge discovery, decision making, summarizing and searching of a large volume of monitored PD-related data and provide seamless and ubiquitous access to processed information under context (e.g. location, ambient conditions, current physical activity) to different users such as PD patients, caregiver or clinics etc. for better management of PD.
With the quick advancement of sensor innovation, Internet of Things (IoT) distributed computing, and pervasive access to the Internet from cell phones, eHealth and versatile wellbeing have prodded the improvement of tele medicinal frameworks that screen indispensable signs and physiological signs, including electrocardiograms and electromyography [10, 13, 15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. Initially, the idea driving Clouds is to give a situation where equipment and programming could be conveyed on a bespoke way to clients and used as needs be to their solicitations. This is a vital distributed computing advantage as it permits the scaling of client assets on request (a procedure called versatility). In parallel, IoT relates clients and their shrewd gadgets alongside sensors utilized as a part of consistently activities (e.g., Smart telephones and wearable gadgets). Utilizing the IoT worldview, new open doors rising where different gadgets could offer to sensor-inserted social insurance new applications and administrations.
With the coordinated sensors in present day cell phones can quantify different development related measurements too Fontecha et al as of late revealed utilizing tri-axels accelerometers in cell phones to survey slightness in elderly individuals [18]. Liddle et al utilized the worldwide situating framework (GPS) sensor in cell phones to assess life space of individuals with PD [17]. Galan-Mercant and Cuesta-Vargas used the accelerometer and gyrator to gauge sit-to-stand pose change in elderly people [27]. As of late, Apple revealed its intend to set out on social insurance by discharging HealthKit APIs in iOS 8 in June 2014 (https://developer.apple.com/healthkit/). These give effective instruments and an interface for engineers to create applications to get to, oversee, and exchange data about wellbeing and prosperity with a wearable gadget.
In this paper, we consider utilizing the latest health-related technologies such as cloud computing, wearable sensors, Internet of Things etc. for an effective and efficient real-time PD-patient monitoring system. There is currently very few automated and intelligent technological system that can measure both PD patient’s healthcare status and physical motion or motor performance factors in a manner that is required for efficient PD management in order to reduce critical movement disability that may lead to sudden death of patients.
3 System overview
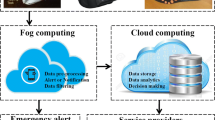
Our goal is to develop an integrated system that will engage and monitor the PD patients’ physical and mental condition, and also the performance of the PD patients’ with a view to reduce the number of attacks. The process of monitoring and data calculation can be divided into two parts. Unlike existing solutions that tackle one or two associated problems, our solution will address most problems and incorporate different aspects such as PD patient’s physical condition monitoring, PD patient’s information about hand resting tremor, walking, and turning and all other sorts of internal and external monitoring. It also includes accurate, effective and timely storage and processing of collected data, efficient data processing and providing accurate and authentic information to the respective users. The proposed technology can provide accurate assessment of physical and mental activity of the PD patient’s in order to assist in determining their level of PD severity for effective PD management. The collected data from the sensors can be huge and not maintainable for a single computer. In order to provide efficient data storage, analysis, and knowledge discovery and decision making process developments, we used a cloud computing environment, where several tens of computers can perform the computing and processing services in a distributed manner. The output of computation is provided to the respective users on demand, that is after the paying for the services and immediate feedback will be provided to the PD patients which will help them to self-monitor, whenever their performance degrades. Thus, the proposed architecture provides accurate assessment and continuous feedback mechanisms to detect PD severity estimation.
3.1 The architecture of proposed framework
Figure 1 presents the proposed sensor-cloud based system architecture of PD patients’ monitoring system. It consists of four major components- sensor devices, Smart phones, cloud services and service users. Different wearable sensors were deployed for monitoring the PD patients’ vital sign data and physical motion data for gait performance and tremor at rest measurements. We deploy ECG sensors, blood pressure sensors and body temperature sensors to measure vital sign data of the patients. We also deploy 3D accelerometer sensor for ambulatory monitoring of gait-related symptoms in PD such as freezing of gait, posture and walking speed estimation, and fall risk estimation.
The data collected by the sensors are sent to the smart phone device which locally stores the data for a short period of time and finally send the data along with the metadata to the cloud server through the mobile Internet or and/or Wi-Fi. The application at the cloud side preprocess the data, extract the important features from the sensor data and estimate the severity of the PD symptoms. Finally, the results are stored in the cloud database and also send back to the PD patients as a report for their monitoring.
The proposed system also maintains the users’ privacy as well as data security. It is done in various stages in the system, data collection, data transmission and cloud data storage scenario. While collecting the data, all data are stored in the mobile device in an encrypted format. Also in case of data transmission, encrypted data are transmitted to the cloud and only the authorized users can access it.

Proposed automated and intelligent PD monitoring system
In our proposed PD monitoring system, we are interested in voice samples of patients obtained by the smart phones. Here, the patient or caregivers can upload voice samples to the proposed sensor-cloud framework of PD. Then the uploaded voice signal will be transmitted to the cloud via the cloud manager. Finally, the decision of PD symptoms will be identified by the system.
3.2 Cloud-based data processing and analysis
The cloud some portion of the proposed system can perform different assignments, for example, store the voice information, pre-process the specimen information by utilizing clamor remover, and examine the information utilizing different grouping methods to recognize PD side effects. The patient associates with the authority over the cloud through the web using their shrewd phones. The cloud administrations are controlled by the cloud head or administrator. The cloud administrator performs different assignments, for example, apportioning virtual assets (VMs), checking and metering of VM assets while preparing and dissecting voice information for distinguishing PD side effects. There is an administration administrator that handles the operations of the VMs. The VMs contain different characterization systems that initially extricates different highlights from the voice tests, select ideal subset of the highlights for grouping lastly isolates the dataset as preparing dataset, test dataset and approval dataset to identify PD.
4 Performance evaluation
The goal of our proposed PD monitoring framework is to get the best results of PD symptoms detection by using various classification technique in cloud computing environment. Therefore, in our study, we used five classification techniques- Decision tree, Random tree, SVM, Naïve Bayes and KNN to Parkinson’s disease (PK) dataset.
4.1 Data source and simulation environment
The dataset used as a piece of PD revelation was taken from UCI machine learning store which was made by Max Little of the University of Oxford, and the voice were recorded by the National Center for Voice and Speech, Denver, Colorado [31]. This dataset is used to perceive or isolate PD patients from people without PD. The data includes 195 persistent vowel phonations from 31 male and female subjects ages moved from 46 to 85 years. 23 of them were resolved to have PD, and rest of them was strong. Among 147 PD vowel phonations and 48 sound vowel phonations, each subject supplies an ordinary of six phonations of the vowel with length of 1– 36 s [21]. The properties are recorded in Table 1. WEKA [32] Tool (Waikato Environment for Knowledge Analysis), was utilized for examination of information. In this examination, the Decision tree, Random tree, SVM, Naïve Bayes and KNN calculations are connected to PK informational index and the after effects of applying these systems are appeared in next area.
4.2 Experimental results
All of the classifiers (i.e. Decision tree, Random Tree, SVM, Naïve Bayes and KNN algorithm) were tested and compared for the given dataset. At first, we have used the Decision Tree classifier. The decision tree is created by selecting the best split at every node. To select the best attribute for the split, the information gain is computed at each node and the attributes are ranked accordingly. The Decision Tree algorithm J48 is then applied to the data set. The results are shown in Table 2.
Next, for Naïve Bayes, the attribute evaluator used is Gain Ratio and the search method used is Ranker method. The Naïve Bayes algorithm is applied to the data set and the results are shown in Table 3.
Next, the KNN algorithm is applied to the data set and the results are shown Table 4. Then, the random tree algorithm is applied to the data set and the results are shown Table 5.
Finally, SVM algorithm is applied to the data set and the results are shown Table 6.
Now, the evaluation measures used to compare the performance of the classifiers are Sensitivity, Specificity and Accuracy
-
(i)
Sensitivity = TP/P
-
(ii)
Specificity = TN/N
-
(iii)
Accuracy = (TP + TN)/(P + N)
where TP is true positives, TN is true negatives, P and T are actual positives and actual negatives respectively.

Comparison of prediction techniques
A good predictor must have high sensitivity, low specificity and high accuracy. The graph in Fig. 2 presents the predictor comparisons of the 5-classifiers. Decision tree has high sensitivity and accuracy and low specificity which ensures it can provide a good indicator for the accuracy of decisions tree in predicting PK disease from their voice signals.

Performance comparison (accuracy, sensitivity and specificity) plot of Decision tree and Bayes classifiers

Performance comparison (accuracy, sensitivity and specificity) plot of Decision tree and KNN classifiers

Performance comparison (accuracy, sensitivity and specificity) plot of Decision tree and random tree classifiers
Figures 3, 4, 5, and 6 compare all the remaining classifiers with decision tree. Moreover, the results show that KNN has highest accuracy as expected since KNN remembers all the instances. But when used for prediction the Decision Tree performs well when compared to other four methods for the given dataset.

Performance comparison (accuracy, sensitivity and specificity) plot of Decision tree and SVM classifiers
5 Conclusion
Parkinson’s infection (PD) is a standout amongst the most well-known neurodegenerative issue and influences more than 6.3 million individuals in everywhere throughout the world. Current PD administration requires normal clinical visits for evaluation and close checking of PD side effects. In any case, it is difficult to monitor separation of PD side effects (e.g. decrease or change) between center visits. What’s more, more incessant facility visits may expand the physical and monetary weight for PD patients and their families. Along these lines, as of late, remote checking of PD patients has pulled in a considerable measure of consideration and there are some dynamic endeavors exist in the writing. Be that as it may, much of the time the assessment of PD side effects was done in managed situations. Different works incorporated the programmed movement acknowledgment in particular snapshots of the day, e.g. evaluation of the stride execution and bradykinesia seriousness when the patient is strolling. We proposed a structure that can productively address the above issues and give the PD seriousness level estimation and help PD patients from sudden falls.
Change history
06 December 2022
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1007/s10586-022-03855-1
References
De Lau, L.M., Breteler, M.M.: Epidemiology of Parkinson’s disease. Lancet Neurol. 5(6), 525–35 (2006)
Rispens, S.M., van Schooten, K.S., Pijnappels, M., Daffertshofer, A., Beek, P.J., van Dieën, J.H.: Do extreme values of daily-life gait characteristics provide more information about fall risk than median values? JMIR Res. Protoc. 4(1), e4 (2015). https://doi.org/10.2196/resprot.3931
Cancela, J., Pastorino, M., Moreno, E., Waldmeyer, M.A.: A mobile monitoring tool for the automatic activity recognition and its application for Parkinson’s disease rehabilitation. In: World Congress on Medical Physics and Biomedical Engineering, June 7–12, 2015, Toronto, Canada, pp. 1457–1460. Springer, New York (2015)
Cancela, J., Pastorino, M., Arredondo, M.T., Nikita, K.S., Villagra, F., Pastor, M.A.: Feasibility study of a wearable system based on a wireless body area network for gait assessment in Parkinson’s disease patients. Sensors 14(3), 4618–4633 (2014)
Caldara, M., Comotti, D., Galizzi, M., Locatelli, P., Re, V., Alimonti, D., Poloni, M., Rizzetti, M.C.: A novel body sensor network for Parkinson’s disease patients rehabilitation assessment. In: 2014 11th International Conference on Wearable and Implantable Body Sensor Networks (BSN), pp. 81–86. IEEE (2014)
Patel, S., Chen, B.R., Buckley, T., Rednic, R., McClure, D., Tarsy, D., Shih, L., Dy, J., Welsh, M., Bonato, P.: Home monitoring of patients with Parkinson’s disease via wearable technology and a web-based application. In: 2010 Annual International Conference of the IEEE on Engineering in Medicine and Biology Society (EMBC), pp. 4411–4414. IEEE (2010)
Tzallas, A.T., Tsipouras, M.G., Rigas, G., Tsalikakis, D.G., Karvounis, E.C., Chondrogiorgi, M., Psomadellis, F., Cancela, J., Pastorino, M., Waldmeyer, M.T.A., Konitsiotis, S.: PERFORM: a system for monitoring, assessment and management of patients with Parkinson’s disease. Sensors 14(11), 21329–21357 (2014)
Chen, B.R., Patel, S., Buckley, T., Rednic, R., McClure, D.J., Shih, L., Tarsy, D., Welsh, M., Bonato, P.: A web-based system for home monitoring of patients with Parkinson’s disease using wearable sensors. IEEE Trans. Biomed. Eng. 58(3), 831–836 (2011)
Patel, S., Lorincz, K., Hughes, R., Huggins, N., Growdon, J., Standaert, D., et al.: Monitoring motor fluctuations in patients with Parkinson’s disease using wearable sensors. IEEE Trans. Inf. Technol. Biomed. 13(6), 864–873 (2009)
Bächlin, M., Plotnik, M., Roggen, D., Inbar, N., Giladi, N., Hausdorff, J., et al.: Parkinsons disease patients perspective on context aware wearable technology for auditive assistance. In: 2009 3rd International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth), pp. 1–8 (2009)
Cancela, J., Pansera, M., Arredondo, M.T., Estrada, J.J., Pastorino, M., PastorSanz, L., Villalar, J.L.: A comprehensive motor symptom monitoring and management system: the bradykinesia case. In: Conference of the IEEE Engineering in Medicine and Biology Society, vol. 2010, pp. 1008–1011 (2010)
Bonato, P., Sherrill, D.M., Standaert, D.G., Salles, S.S., Akay, M.: Data mining techniques to detect motor fluctuations in Parkinson’s disease. In Conference of the IEEE Engineering in Medicine and Biology Society, vol. 7, pp. 4766–4769 (2004)
Cunningham, L., Mason, S., Nugent, C., Moore, G., Finlay, D., Craig, D.: Homebased monitoring and assessment of Parkinson’s disease. IEEE Trans. Inf Technol. Biomed. 15(1), 47–53 (2011)
Keijsers Noël, L.W., Horstink Martin, W.I.M., Gielen Stan, C.A.M.: Ambulatory motor assessment in Parkinson’s disease. Mov. Disord. 21(1), 34–44 (2006)
Rodríguez-Molinero, A., Samà, A., Pérez-Martínez, D.A., López, C.P., Romagosa, J., Bayés, À., Sanz, P., Calopa, M., Gálvez-Barrón, C., de Mingo, E., Martín, D.R.: Validation of a portable device for mapping motor and gait disturbances in Parkinson’s disease. JMIR Mhealth Uhealth 3(1), e9 (2015). https://doi.org/10.2196/mhealth.3321
Pan, D., Dhall, R., Lieberman, A., Petitti, D.B.: A mobile cloud-based Parkinson’s disease assessment system for home-based monitoring. JMIR Mhealth Uhealth 3(1), e29 (2015). https://doi.org/10.2196/mhealth.3956
Liddle, J., Ireland, D., McBride, S.J., Brauer, S.G., Hall, L.M., Ding, H., Karunanithi, M., Hodges, P.W., Theodoros, D., Silburn, P.A., Chenery, H.J.: Measuring the lifespace of people with Parkinson’s disease using smartphones: proof of principle. JMIR Mhealth Uhealth 2(1), e13 (2014). https://doi.org/10.2196/mhealth.2799
Fontecha, J., Hervás, R., Bravo, J., Navarro, F.J.: A mobile and ubiquitous approach for supporting frailty assessment in elderly people. J. Med. Internet Res. 15(9), e197 (2013). https://doi.org/10.2196/jmir.2529
Eskofier, B.M., Lee, S.I., Baron, M., Simon, A., Martindale, C.F., Gaßner, H., Klucken, J.: An overview of smart shoes in the internet of health things: gait and mobility assessment in health promotion and disease monitoring. Appl. Sci. 7(10), 986 (2017)
Salarian, A., Russmann, H., Vingerhoets, F.J.G., Burkhard, P.R., Aminian, K., Wider, C.: Ambulatory monitoring of physical activities in patients with Parkinson’s disease. IEEE Trans. Biomed. Eng. 54(12), 2296–2299 (2007)
Al Mamun, K.A., Alhussein, M., Sailunaz, K., Islam, M.S.: Cloud based framework for Parkinson’s disease diagnosis and monitoring system for remote healthcare applications. Future Gener. Comput. Syst. 31(66), 36–47 (2017)
Tsiouris, K.M., Gatsios, D., Rigas, G., Miljkovic, D., Seljak, B.K., Bohanec, M., Arredondo, M.T., Antonini, A., Konitsiotis, S., Koutsouris, D.D., Fotiadis, D.I.: PD_Manager: an mHealth platform for Parkinson’s disease patient management. Healthc. Technol. Lett. 4(3), 102–108 (2017)
van den Noort, J.C., Verhagen, R., van Dijk, K.J., Veltink, P.H., Vos, M.C., de Bie, R.M., Bour, L.J., Heida, C.T.: Quantification of hand motor symptoms in Parkinson’s disease: A proof-of-principle study using inertial and force sensors. Ann. Biomed. Eng. 45(10), 2423–2436 (2017)
Lin, B.S., Chou, N.K., Chong, F.C., Chen, S.J.: RTWPMS: a realtime wireless physiological monitoring system. IEEE Trans. Inf. Technol. Biomed. 10(4), 647–656 (2006)
Jin, Z., Oresko, J., Huang, S., Cheng, A.C.: HeartToGo: a personalized medicine technology for cardiovascular disease prevention and detection. In: Proceedings of the IEEE/NIH LiSSA, Bethesda, 9 Apr 2009, pp. 80–83
Pantelopoulos, A., Bourbakis, N.: A survey on wearable sensorbased systems for health monitoring and prognosis. IEEE Trans. Syst. Man. Cybern. C 40(1), 1–12 (2010). https://doi.org/10.1109/TSMCC.2009.2032660
Galán-Mercant, A., Cuesta-Vargas, A.I.: Differences in trunk accelerometry between frail and nonfrail elderly persons in sit-to stand and stand-to-sit transitions based on a mobile inertial sensor. JMIR Mhealth Uhealth 1(2), e21 (2013). https://doi.org/10.2196/mhealth.2710
Almashaqbeh, G., Hayajneh, T., Vasilakos, A.V., Mohd, B.J.: QoS-aware health monitoring system using cloud-based WBANs. J. Med. Syst. 38(10), 121 (2014)
Hassanalieragh, M., Page, A., Soyata, T., Sharma, G., Aktas, M., Mateos, G., Kantarci, B., Andreescu, S. Health monitoring and management using Internet-of-Things (IoT) sensing with cloud-based processing: Opportunities and challenges. In: 2015 IEEE International Conference on Services Computing (SCC), pp. 285–292. IEEE (2015)
Almogren, A.: Developing a powerful and resilient smart body sensor network through hypercube interconnection. Int. J. Distrib. Sens. Netw. Article Number: 609715, Open Access (2015)
Asuncion, A., Newman, D.: UCI machine learning repository. School of Information and Computer Science, University of California, Irvine. http://mlearn.ics.uci.edu/MLRepository.html (2009)
Singhal, S., Jena, M.: A study on WEKA tool for data preprocessing, classification and clustering. Int. J. Innov. Technol. Explor. Eng. 2(6), 250–253 (2013)
Acknowledgements
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through research group no (RGP-1437-35).
Author information
Authors and Affiliations
Corresponding author
Additional information
This article has been retracted. Please see the retraction notice for more detail:https://doi.org/10.1007/s10586-017-1591-z
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Almogren, A. RETRACTED ARTICLE: An automated and intelligent Parkinson disease monitoring system using wearable computing and cloud technology. Cluster Comput 22 (Suppl 1), 2309–2316 (2019). https://doi.org/10.1007/s10586-017-1591-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10586-017-1591-z