
Abstract
Metastasis remains the principal trigger for relapse and mortality across diverse cancer types. Circulating tumor cells (CTCs), which originate from the primary tumor or its metastatic sites, traverse the vascular system, serving as precursors in cancer recurrence and metastasis. Nevertheless, before CTCs can establish themselves in the distant parenchyma, they must overcome significant challenges present within the circulatory system, including hydrodynamic shear stress (HSS), oxidative damage, anoikis, and immune surveillance. Recently, there has been a growing body of compelling evidence suggesting that a specific subset of CTCs can persist within the bloodstream, but the precise mechanisms of their survival remain largely elusive. This review aims to present an outline of the survival challenges encountered by CTCs and to summarize the recent advancements in understanding the underlying survival mechanisms, suggesting their implications for cancer treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Despite significant advancements in cancer diagnostics and therapeutics, the formidable challenge of metastasis continues to cast a shadow over prognoses. The metastatic cascade is a complex, multistage process involving the journey of cancer cells from primary tumors to remote metastatic sites. This intricate process begins with detachment from the primary tumor, followed by invasion into the stroma, entry into the bloodstream, extravasation, and eventual colonization of distant niches [1]. These steps play a pivotal role in determining disease outcomes.
One of the key stages in the metastatic cascade involves the release of circulating tumor cells (CTCs) into the bloodstream. These CTCs, first observed by T. R. Ashworth in 1896 [2], embark on a perilous voyage throughout the host body. While the bloodstream serves as a transportation route for CTCs, their ability to successfully establish metastatic colonies is hampered by hydrodynamic shear stress (HSS). An additional challenge encountered by CTCs is anoikis, a programmed cell death triggered by cell detachment from the correct extracellular matrix (ECM) [3], resulting in significant attrition of CTCs. Both HSS and ECM detachment can elevate intracellular reactive oxygen species (ROS) levels, rendering CTCs susceptible to oxidative damage. Furthermore, immune cells, including natural killer (NK) cells and cytotoxic T lymphocytes (CTLs), attack and eliminate CTCs, increasing the difficulty of survival. These challenges are illustrated and discussed in detail in this review.
In recent years, accumulating research has elucidated the mechanisms enabling CTCs to survive in the bloodstream, including resistance to HSS, maintenance of redox balance, acquisition of anoikis resistance, and evasion of immune surveillance. Nonetheless, a more in-depth understanding of these underlying mechanisms is imperative and requires further investigation.
In this review, we present an overview of the latest advancements in understanding the survival mechanisms of CTCs and explore their implications for cancer treatment. A comprehensive understanding of CTC survival has the potential to unveil novel therapeutic interventions. Such insights hold the potential to pave the way for innovative strategies aimed at enhancing the prognosis and treatment of metastatic cancers.
2 The biology of CTCs
The genomic signatures of CTCs exhibit significant variations across different cancer types and are distinct from those of primary tumors. Copy number aberrations (CNAs) refer to deletions or amplifications of chromosomes or genes in somatic cells. Identifying CNAs in CTCs facilitates the analysis and tracking of cancer profiles as tumors evolve, providing valuable insights into the molecular dynamics of cancer progression. In breast cancer, researchers have identified a recurrent gain signature in CTCs primarily involving genes associated with tumor aggressiveness, which was present at low frequencies in primary tumors [4]. Similarly, a study on epithelial ovarian cancer revealed that 17 somatic mutations were detected restrictively in captured CTCs but not in the corresponding tumor samples [5]. In a study involving patients with recurrent breast cancer with liver metastasis, CNAs of isolated CTCs shared nearly 82% of gain/loss regions with recurrent liver metastases [6]. In the context of melanoma research, a remarkable concordance in single-nucleotide polymorphism (SNP) profiles exceeding 90% was observed between paired CTCs and their corresponding tumor metastases [7]. Additionally, recurring CNAs were also noted in systemic metastatic melanomas. In summary, the concordance of genomic signatures in CTCs and metastases suggests the presence of a mechanism through which specific genomic alterations are transmitted from localized metastatic foci to CTCs, thereby perpetuating their influence on distantly situated systemic metastases. Notably, the mutation pattern of CTCs differs from that of primary tumors, indicating that aberrant genomic changes are unique to CTCs.
Transcriptome analysis revealed notable decreases in the expression of key oncogenes, including MKI67 (Ki-67), MYC (c-Myc), and CTNNB1 (β-catenin), in CTCs [8]. The decreased expression of MKI67 and MYC suggests a reduced proliferative capacity of CTCs, placing them in a state of dormancy. This dormancy of CTCs may explain the failure of cytotoxic chemotherapy regimens that target rapidly dividing cancer cells in patients with breast cancer [9]. Epithelial cell adhesion molecule (EpCAM) is employed for the identification and distinction of CTCs. The presence of EpCAM-positive CTCs is indicative of cancer metastasis and an unfavorable prognosis [10]. Furthermore, the expression of epithelial markers, with EPCAM (EpCAM) as a prominent example, are also downregulated in CTCs [8], particularly during epithelial-to-mesenchymal transition (EMT) (see below for details). These findings suggest a potential loss of the epithelial phenotype in CTCs, thus elucidating the low detection rate of CTCs and the need to incorporate mesenchymal markers such as vimentin for more effective CTC detection.
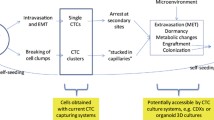
The EMT is a physiological process in the development of embryogenesis and is involved in tumor metastasis [11]. During EMT, epithelial cancer cells undergo a phenotypic transition to the mesenchymal phenotype. This transformation is driven by a group of EMT-related transcription factors, including the ZEB family (ZEB1 and ZEB2), the SNAIL family (SNAIL and Slug), and the TWIST family [12]. Interestingly, EMT is observed more frequently in CTCs than in primary tumors across various cancer types, including hepatocellular carcinoma (HCC), castration-resistant prostate cancer (CRPC), non-small cell lung cancer (NSCLC), and breast cancer [13,14,15]. In recent years, compelling evidence has highlighted the important role of EMT in cancer progression, which is correlated with unfavorable clinical outcomes [15,16,17,18]. Upon extravasation to metastatic sites, rather than EMT, a process called mesenchymal-to-epithelial transition (MET) occurs in mesenchymal CTCs [19]. Remarkably, the transition between EMT and MET is dynamic; MET is transient, and epithelial cancer cells continuously undergo EMT, thereby initiating the metastatic process anew [20].
A subset of CTCs gains a survival advantage in the blood circulation and exhibits self-renewal capabilities and the ability to induce tumor growth. These specialized CTCs are referred to as circulating tumor stem cells (CTSCs). The identification of CTSCs relies on the expression of specific cell surface markers, including CD44, CD133, and aldehyde dehydrogenase 1 (ALDH1) [21]. In patients with metastatic breast cancer, 35.2% of CTCs in the peripheral blood were characterized as CD44+/CD24−/low, and 17.7% were identified as ALDH1high/CD24−/low [22]. In addition, in the context of HCC, 71.4% of patients with HCC had CTCs that tested positive for CD44 [23]. These findings suggest that a significant proportion of CTCs in patients possess stemness properties.
Recent research has shown a strong correlation between stemness properties and the EMT process in CTCs. CD44+CD24−/low cancer stem cells can arise from CD44lowCD24+ human mammary epithelial cells following abnormal stimulation of the Ras/MAPK pathway driven by EMT induction [24]. Consistent with these findings, the Weinberg laboratory reported that EMT induction via Twist1 and Snail leads to the acquisition of mesenchymal traits and stemness characteristics in immortalized human mammary epithelial cells, thereby establishing a direct connection between EMT and the acquisition of characteristics resembling epithelial stem cells [25]. This dual phenotype of CTCs, characterized by both EMT and stemness properties, represents a subpopulation that exhibits resistance to chemotherapy and serves as an independent predictor of unfavorable prognosis in patients with metastatic breast cancer (Fig. 1) [26].

The biology of CTCs. CTCs are characterized by the distinctive genome and transcriptome signatures, as well as the presence of epithelial-to-mesenchymal transition (EMT) and stemness properties. (a) The mutation pattern of CTCs differs from that of primary tumors but is similar to that of metastatic lesions. (b) Oncogenes such as MKI67, MYC, and CTNNB1 are downregulated, along with the epithelial marker EPCAM. (c) During EMT, epithelial cancer cells undergo a phenotypic transition into the mesenchymal phenotype driven by the ZEB family, the SNAIL family, and the TWIST family. Conversely, MET, which is the process contrast to EMT, occurs in mesenchymal CTCs upon extravasation to metastatic sites. (d) CTSCs can be identified by specific cell surface markers including CD44, CD133, and ALDH1. CTCs can acquire stemness properties through EMT. CNAs, copy number aberrations; MET, mesenchymal-to-epithelial transition; ALDH1, aldehyde dehydrogenase 1; CTSCs, circulating tumor stem cells
3 Survival challenges encountered by CTCs in the blood circulation
While serving as a transportation route, the bloodstream strikingly compromises the viability of CTCs due to the presence of HSS. The average HSS levels in arterial flow range from 4 to 30 Dyn cm–2; in venous circulation, they span from 1 to 4 Dyn cm–2; and within capillaries, they range from 10 to 20 Dyn cm–2 [27]. Within arteries and capillaries, CTCs experience deformation caused by considerable shear stress, resulting in cellular fragmentation and subsequent death. However, cellular fragmentation can be a double-edged sword as it can facilitate metastasis. In a mouse lung metastasis visualization experiment, pioneer metastatic B16F10 melanoma cells shed microparticles which are actually cellular fragments with preserved metabolic motility driven by shear stress [28]. These microparticles are ingested by myeloid lineage cells, including neutrophils, monocytes, and macrophages, consequently priming an early prometastatic niche for future metastasis. An HSS of 12 Dyn cm–2 induces G2/M arrest in cancer cells, whereas under static conditions, cancer cells tend to exhibit G0/G1 arrest [29]. Furthermore, when subjected to HSS ranging from 15 to 30 Dyn cm–2, the production of ROS within CTCs increases, leading to mitochondrial damage and the induction of apoptosis [30]. Conversely, lower HSS levels (5 Dyn cm–2) do not have such an impact. Under conditions of extremely high HSS, specifically 60 Dyn cm–2 (common during intense exercise), necrosis occurs in more than 90% of CTCs within the initial 4 h of circulation [31]. When confronted with challenges from HSS, only 40–60% of metastatic cells manage to withstand the disruptive forces of the bloodstream, demonstrating the inefficiency of the metastatic process [32]. HSS also impacts CTC clustering. According to an in vitro study of triple-negative breast cancer cells, even low shear stress (2 Dyn/cm2) can cause the dissociation of CTC clusters, and with increasing shear stress (5 Dyn/cm2 or 20 Dyn/cm2), the reduction in cluster size is more significant [33]. High levels of HSS in the blood flow impede the survival of CTCs, whereas low levels of HSS in the interstitial fluid facilitate cell migration. Shear stress in the interstitial fluid increases the expression of αvβ3 integrins, thereby initiating downstream signaling and leading to elevated levels of MMP-9, which enhances the migratory capacity of PC3 prostate cancer cells [34]. In addition, the mechanosensitive ion channel Piezo1 is upregulated by shear stress in the interstitial fluid, subsequently activating Src and YAP, ultimately resulting in enhanced motility and increased migration speed in PC3 cells [35].
CTCs encounter elevated levels of oxidative stress from multiple sources, including HSS, abundant oxygen within the bloodstream [36], and ECM detachment [37]. Oxidative stress is characterized by an excess of ROS which have a short lifespan and strong reactivity. Generally, high ROS levels trigger apoptosis through various pathways: (1) the intrinsic pathway mediated by mitochondria, (2) the extrinsic pathway involving death receptors, and (3) the endoplasmic reticulum (ER) stress-related pathway. Among these pathways, mitochondria play a central role in triggering apoptosis. Mechanistically, the accumulation of ROS initiates the mitochondrial apoptotic pathway by damaging mitochondrial DNA (mtDNA), disrupting the permeability of the mitochondrial membrane, releasing cytochrome c into the cytosol, and activating caspase 3 via caspase 9 mediation [38]. ROS can also directly cause harm to nuclear DNA to activate the intrinsic mitochondrial pathway, consequently initiating apoptosis in CTCs [39]. Moreover, within a blood environment abundant in both oxygen and iron, ROS can induce ferroptosis in CTCs, which is a regulated form of cell death triggered by iron-dependent lipid peroxidation (LPO) [40].
The term “anoikis”, derived from the Greek word for homelessness, refers to programmed cell death induced by the absence of correct connections either between cells or between cells and the ECM [3]. Despite its distinct characterization, anoikis fundamentally represents an apoptotic mechanism. The correct adhesion of a cell to ECM proteins plays a crucial role in determining whether the cell is properly positioned. Integrins mediate cellular attachment to the ECM, leading to the activation of intracellular signaling molecules that support cell survival. Focal adhesion kinase (FAK) is an essential integrin signaling component that is engaged within focal adhesions upon cell–ECM contact [41]. FAK exerts influence on various essential cellular processes, including the phosphatidylinositol 3-kinase (PI3K)/AKT signaling pathway and the MAPK pathway. After detachment from the ECM, CTCs are effectively removed by anoikis, as they are displaced cells. Therefore, anoikis functions as a fundamental mechanism that disrupts the reattachment of CTCs to distant metastatic organs [3]. The elimination of CTCs by anoikis involves both extrinsic and intrinsic apoptotic pathways, as previously discussed for ROS. Briefly, in the extrinsic pathway, cell surface death receptors, such as Fas (CD95/APO-1), are stimulated by corresponding ligands such as TNF-α. This stimulation leads to caspase 8 activation via Fas-associated protein with death domain (FADD), ultimately resulting in anoikis via caspase 3 activation [42]. In the intrinsic apoptotic pathway, initiation occurs at the mitochondrial membrane, where proapoptotic proteins such as Bax create pores in the outer mitochondrial membrane. This action leads to the release of substances such as cytochrome c, which assemble into the apoptosome complex to activate caspase 9. Subsequently, caspase 3 is activated, ultimately leading to anoikis.
CTCs can be eliminated by immune surveillance mediated by various leukocyte populations. This process encompasses both innate surveillance carried out by NK cells and macrophages and adaptive surveillance conducted by T‑helper cells and cytotoxic T cells [43]. The elimination of CTCs by different types of immune cells blocks the establishment of distant metastases. NK cells, which are the principal members of the innate lymphoid cell family, contribute to protection against certain viruses and tumor cells through cytotoxicity mediated by IFN-γ, granzymes, and perforin [44]. Major histocompatibility complex class I (MHC I) expression on the tumor cell surface decreases to escape MHC class I-restricted elimination by CD8 + T cells [45]. NK cells, as alternative immune defense agents, eliminate tumor cells with MHC I deficiency [46, 47]. Compared with primary tumor-derived cells, CTCs exhibit reduced MHC I expression in HCC [13], which can be targeted by NK cells. The number of CTCs in mice with perforin-deficient NK cells was 2.8 times greater than that in mice with normal NK cells [48]. Additionally, computational modeling demonstrated that perforin-dependent killing of NK cells effectively eliminated 80% of CTCs. Together with NK cells, macrophages have an impact on innate surveillance. After antitumor monoclonal antibody treatment, liver macrophages (Kupffer cells) can recognize and arrest CTCs, inducing antibody‑dependent phagocytosis of CTCs [49]. Most related studies have focused on the associations between CTCs and intratumoral, peritumoral, or stromal lymphocytes [50,51,52]. In these studies, antitumor immunity was suppressed and linked to worse outcomes. However, the influence of lymphocytes on regulating the viability of peripheral cancer cells has not been thoroughly investigated. This lack of exploration could be explained by the fact that adaptive surveillance exhibits delayed responsiveness and comparatively lower sensitivity than immediate and robust innate surveillance within the circulation. Before T‑helper cells and cytotoxic T cells can contact CTCs, NK cells and macrophages have already eliminated these “dangerous” cells. Indeed, a recent study reported that among multiple types of immunocytes, CTCs predominantly interact with NK cells in the blood circulation of patients with pancreatic ductal adenocarcinoma (PDAC) [53]. NK cells primarily perform antitumor functions in the blood circulation rather than in primary/metastatic lesions. The interaction between CTCs and NK cells was also confirmed in a mouse breast cancer model. NK cells selectively kill single CTCs, which have a low ability to inhibit NK cell activity due to the loss of cell–cell adhesion by EMT [54]. This selective killing leads to a more effective suppression of monoclonal metastasis compared with polyclonal metastasis formed by CTC clusters.
In summary, CTCs face several challenges during circulation in the blood. These challenges include the tearing forces exerted by HSS, oxidative damage resulting from ROS, anoikis triggered by ECM detachment, and elimination by immune cells (Fig. 2). Despite these formidable challenges, a minor proportion of CTCs persistently manage to endure within the bloodstream. Consequently, it is imperative to unravel the intricate mechanisms by which these CTCs sustain their survival while in circulation.

Survival challenges encountered by CTCs in the blood circulation. Four major challenges that CTCs confront in the blood circulation include the ripping forces from HSS, oxidative damage due to intracellular ROS, anoikis induced by cell detachment from ECM, and elimination by immune cells. (a) Different levels of HSS have different effects on cells. (b) High ROS levels trigger apoptosis through three pathways: (1) the intrinsic pathway mediated by mitochondria; (2) the extrinsic pathway involving death receptors; and (3) the pathway related to ER stress. Additionally, ROS can induce ferroptosis driven by LPO. (c) Anoikis involves both extrinsic and intrinsic apoptotic pathways that engage different apoptotic cascades. (d) CTCs can be eliminated through innate surveillance carried out by NK cells and macrophages (Kupffer cells), along with adaptive surveillance performed by T‑helper cells and cytotoxic T cells. HSS, hydrodynamic shear stress; ROS, reactive oxygen species; LPO, lipid peroxidation; ER, endoplasmic reticulum; NK, natural killer
4 Survival mechanisms of CTCs in the blood circulation
The ability of CTCs to withstand various challenges, including HSS, oxidative damage, anoikis, and immune surveillance, plays a crucial role in their adaptation and persistence within the bloodstream. These mechanisms collectively facilitate the survival of CTCs, ultimately contributing to their successful metastatic dissemination. Elucidation of these survival mechanisms not only expands our fundamental knowledge of cancer progression but also has potential implications for the development of targeted therapeutic interventions aimed at disrupting these mechanisms and preventing the metastatic spread of tumor cells.
4.1 Resisting HSS
The primary factor leading to cell death due to HSS is damage to the plasma membrane. The ability to either avoid such membrane damage or effectively restore the impaired plasma membrane determines the resistance of CTCs to HSS [55]. Additionally, elevated resistance to HSS-triggered apoptosis is linked to augmented cell stiffness and diminished cell fluidity. Following repeated exposure to HSS, the plasma membranes of CTCs become resistant to damage, which is dependent on extracellular calcium and rapid actin cytoskeleton dynamics [56]. Recent reports have indicated that CTCs activate the RhoA/actomyosin signaling axis to protect themselves from HSS-induced plasma membrane damage [57]. Furthermore, CTCs improve their biophysical properties through EMT as a survival strategy in the bloodstream. HSS promotes CTCs to undergo EMT and exhibit stemness properties [58]. This effect is a result of ROS/nitric oxide (NO) production coupled with the inhibition of the extracellular signal-related kinase (ERK)/glycogen synthase kinase (GSK) 3β pathway. These combined actions confer adaptability on epithelial tumor cells, allowing them to sustain their undifferentiated mesenchymal stem cell properties. As a result, CTCs endure within the peripheral blood circulation. Consistently, low HSS (2 Dyn cm–2) can induce EMT in renal cell carcinoma (RCC) cells via Yes-associated protein 1 (YAP1) activation and nuclear localization [59].
Regulation of the cell nucleus also contributes to HSS resistance. Nuclear lamins A and C play pivotal roles as essential structural elements, conferring resistance to death induced by HSS within the bloodstream on CTCs [60]. In addition, HSS can increase nuclear size via histone acetylation, which serves to protect CTCs from HSS-induced destruction [61].
Moreover, CTCs can aggregate into stable cell clusters within the bloodstream through E-cadherin and cortical actin-myosin dynamics to resist HSS [62]. The formation of CTC aggregates can also be induced by reactive cancer-associated fibroblasts (CAFs), along with soluble factors derived from these reactive CAFs, including CCL2, CCL7 and CXCL5 [63]. These soluble factors contribute to maintaining cell viability, ultimately resulting in CTC resistance to HSS. Similarly, the membrane damage triggered by HSS can stimulate the proliferation of colorectal CTC clusters through the ANXA1/PI3K/AKT signaling pathway [64]. In prostate cancer, macrophages can enhance the adhesion of CTCs, leading to the formation of protective cell clusters [65]. This phenomenon thereby supports the survival of CTCs during the crucial initial phases of metastasis.
In summary, maintaining cell membrane integrity, optimizing biophysical properties such as cell stiffness and fluidity, regulating the nucleus, and fostering cell aggregation collectively contribute to HSS resistance.
4.2 Maintenance of redox balance
Both HSS and chemotherapeutic drugs can elevate ROS levels in CTCs. In response to the oxidative damage primarily caused by ROS, CTCs have evolved their own protective mechanisms to maintain redox balance. Notably, CTCs can increase manganese superoxide dismutase (MnSOD) levels to scavenge the elevated primary free radical and superoxide anion production triggered by HSS in mitochondria [30]. This defense mechanism contributes to resistance against the chemotherapeutic agent doxorubicin (DOX), which similarly induces mitochondrial superoxide production in patients with breast cancer.
The metabolic switch confers a survival advantage to CTCs by reducing ROS generation. Colorectal CTCs upregulate the expression of atonal bHLH transcription factor 8 (ATOH8) in response to HSS [66]. This upregulation transcriptionally activates the glycolytic enzyme hexokinase 2 (HK2), which suppresses ROS production by promoting glycolysis. Intratumor hypoxia leads to the shedding of CTC clusters [67], which subsequently creates a hypoxic environment in the center of the cell clusters. This environment triggers hypoxia-inducible factor 1 alpha (Hif1α)-mediated mitophagy, a mechanism that eliminates dysfunctional mitochondria and reduces ROS production [68]. To adapt to hypoxia and mitochondrial defects, detached cell clusters induce a switch from mitochondrial oxidative phosphorylation to glycolysis, which is supported by reductive glutamine metabolism through cytosolic NAD + recycling, consequently preventing ROS accumulation.
Ferroptosis is a distinct form of cell death triggered by ROS, and the ability to resist ferroptosis is essential for the survival of CTCs. Sterol regulatory element-binding protein 2 (SREBP2), a regulator of lipogenesis, induces the transcription of transferrin (TF) in melanoma CTCs [69]. The increased intracellular TF sequesters iron, resulting in a reduction in labile free iron pools, which leads to decreased ROS levels and lipid peroxidation. These effects collectively confer resistance against ferroptosis on CTCs.
In conclusion, CTCs employ diverse strategies, involving increasing MnSOD levels; metabolic switching, including ATOH8-induced HK-2 activation and cell clustering; and SREBP2-mediated TF upregulation, to manage ROS levels and ensure survival.
4.3 Acquisition of anoikis resistance
A plethora of pro-survival signals are activated after detachment of the ECM. Midkine, a basic heparin-binding growth factor, confers resistance to anoikis on CTCs by activating its receptor anaplastic lymphoma kinase (ALK) on the PI3K/AKT/NF-κB/TrkB signaling pathway [70]. High serum midkine levels in patients with HCC compared with healthy individuals were significantly associated with both CTC counts and postoperative recurrence. Following matrix detachment, the antiapoptotic molecule alphaB-crystallin is activated through the inhibition of ERK signaling [71]. This process suppresses caspase activation and the initiation of anoikis triggered by matrix detachment. In addition, the adhesion of platelets reduces the anoikis of CTCs by promoting YAP1 dephosphorylation and translocation to the nucleus [72]. This action triggers the activation of a gene expression profile conducive to cell survival.
Cells that have detached from the ECM experience nutrient scarcity, which constrains their capacity for energy generation [37]. Glutamate can be converted to α-ketoglutarate (a-KG) by glutamate dehydrogenase 1 (GDH1) in the mitochondria [73]. ECM detachment induces the upregulation of GDH1 and subsequently promotes the production of a-KG, which can bind and activate calcium/calmodulin-dependent protein kinase kinase 2 (CamKK2) [74]. In liver kinase B1 (LKB1)-deficient lung cancer, CamKK2 substitutes for LKB1 to activate 5’AMP-activated protein kinase (AMPK). This activity contributes to the production of energy for anoikis resistance and metastatic promotion.
ROS play dual roles in anoikis resistance by either promoting or inhibiting this process. ROS generation effectively enables CTCs to prevent anoikis through various mechanisms. In the presence of low HSS (2 Dyn cm–2), the production of ROS and (•)NO increases the stabilization of caveolin-1 in suspended cancer cells by hindering ubiquitination and proteasomal degradation [75]. This increase in caveolin-1 enhances the capacity of cancer cells to resist anoikis. The enzyme NADPH oxidase 4 (NOX4) is responsible for generating ROS. NOX4-generated ROS upregulate epidermal growth factor receptor (EGFR), consequently promoting resistance to anoikis in lung [76] and gastric [77] cancers. The elimination of ROS via carnitine palmitoyl transferase 1 A (CPT1A) is also critical for anoikis resistance. CPT1A, a key rate-limiting enzyme of fatty acid oxidation (FAO), is prominently upregulated in several cancer types, including esophageal squamous cell carcinoma (ESCC), colorectal cancer (CRC), and high-grade serous ovarian cancer (HGSOC) [78,79,80]. Under detached culture conditions, CPT1A expression is induced by upregulation of the transcription factor ETV4 and downregulation of the ubiquitin enzyme RNF2 [78]. This coordinated mechanism leads to increased CPT1A expression at both the mRNA and protein levels. The induction of CPT1A maintains redox homeostasis by supplying reduced glutathione (GSH) for ROS elimination [78, 79] and sustains mitochondrial respiration by utilizing monounsaturated fatty acids (MUFAs) [80], thereby contributing to cancer cell protection against anoikis. Notably, the Warburg effect contributes to anoikis resistance in cancer cells by attenuating the excessive production of ROS, which are byproducts of oxidative metabolism. The Warburg effect, named after the discoverer Otto Warburg, refers to tumor cells’ preference for glycolysis over mitochondrial oxidative phosphorylation even under aerobic conditions [81]. This process is also known as aerobic glycolysis. Pyruvate dehydrogenase (PDH) converts pyruvate to acetyl coenzyme A (CoA), which subsequently enters the mitochondrial TCA cycle and undergoes oxidative phosphorylation. PDH can be inactivated by pyruvate dehydrogenase kinases (PDKs) through phosphorylation of the E1α subunit [82]. PDKs are significantly upregulated in different types of human cancer cells, resulting in decreased oxidative metabolism and reduced ROS levels through the inhibition of PDH activity. Consequently, inherent resistance to anoikis is observed in cancer cells [83]. The transcriptional upregulation of PDK1 by Hif1 in response to intratumoral hypoxia-induced metabolic adaptation leads to a shift from oxidative metabolism toward glycolysis and constrains ROS generation [84]. As mentioned above, cell clustering triggers hypoxia in CTCs, thereby activating Hif1. In detached glioma cell clusters, activation of Hif1-dependent transcription leads to upregulation of PDK1 expression, subsequently attenuating the levels of ROS and preventing anoikis [85]. Hif1 activity can be upregulated in a hypoxia-independent, ROS-dependent manner in response to oxidative stress, which in turn reduces cellular ROS levels by reprogramming glucose metabolism [86]. Hence, Hif1 can also be activated by detachment-induced ROS accumulation in glioma CTC clusters, enabling resistance to anoikis [85].
Cell aggregation enhances not only resistance to HSS but also anoikis resistance. Lipid rafts are specialized regions within cell membranes enriched with cholesterol, sphingolipids, and proteins [87]. The detachment of cells from the ECM disrupts these lipid rafts, ultimately triggering anoikis [88]. A recent study reported that CD44 acts as a mediator of CTC aggregation, preserving the structural integrity of lipid rafts following cell detachment [89]. This preservation of lipid rafts subsequently activates the Rac1–Pak2 signaling pathway, effectively preventing anoikis and facilitating metastasis in triple-negative breast cancer. In addition, NOX4 induces upregulation of the ECM component fibronectin, thereby promoting enhanced cell‒cell desmosomal interactions through desmoglein-2, desmocollin-2/3, and plakoglobin [90]. These augmented interactions facilitate the aggregation of CTCs, thus counteracting anoikis. The presence of fibronectin expression holds clinical significance as it is correlated with unfavorable survival outcomes among patients with cancer.
It should be noted that the tumor microenvironment (TME) also impacts CTC resistance to anoikis. Within the TME, the anoxic microenvironment and the Warburg effect contribute to the development of acidic conditions. Melanoma cells cultured under low-pH conditions (pH 6.7), whether for a short duration (24 h) or an extended period (at least 3 months), exhibit comparable characteristics of resistance to anoikis [91]. Subsequently, these cells survive after injection into the bloodstream in mice. Additionally, an acidic pH facilitates autocrine signaling of transforming growth factor-beta 2 (TGF-β2), leading to the accumulation of lipid droplets [92]. These droplets serve as energy reservoirs, enhancing the ability of cancer cells to resist anoikis and reinforcing their invasion.
In summary, CTCs exhibit resistance to anoikis through a range of mechanisms, encompassing the activation of prosurvival signals, energy production, ROS generation or elimination, cell aggregation, and adaptation to an acidic tumor microenvironment.
4.4 Evading immune surveillance
The immune system functions as the body’s defense mechanism against tumor progression, and the ability of CTCs to evade the immune surveillance plays a crucial role in determining their fate during the metastatic process. To escape immune surveillance, CTCs express molecules to protect themselves, such as Survivin, inhibitory immune checkpoints, including programmed death ligand 1 (PD-L1) and CD47 (acting as a “do not eat me” signal), and fibrinogen-like protein 1 (FGL1). Survivin, also known as BIRC5, is an apoptosis inhibitor that is expressed in cells undergoing active proliferation [93]. Survivin expression in cancer cells provides protection against NK cell cytotoxicity [94]. Survivin is widely expressed in CTCs in patients with breast cancer, gastric cancer, colorectal cancer, NSCLC, ESCC, and metastatic colorectal cancer (mCRC), indicating poor prognosis [95,96,97,98,99]. A negative correlation between Survivin expression in CTCs and immune cell (including lymphocytes, dendritic cells, and monocytes) infiltration in the circulation has been identified in patients with osteosarcoma, highlighting its pivotal role in immune evasion [100]. The presence of PD-L1 on cancer cells impaired the viability and function of T cells through inhibiting proliferation, impacting survival, and reducing cytokine production [101]. Mazel et al. first reported that the proportion of PD-L1 expression on CTCs was 68.8% in patients with breast cancer, with the proportions of CTCsPD−L1(+) ranging from 0.2 to 100% [102]. A recent systematic review and meta-analysis indicated that a correlation existed between PD-L1 expression on CTCs in the peripheral blood of patients with cancer and an unfavorable prognosis, characterized by shorter overall survival (OS) and progression-free survival (PFS) [103]. Another molecule, CD47, is overexpressed on CTCs and serves as an antiphagocytic factor, shielding cells from clearance by macrophages [8]. In metastatic breast cancer, CTCs coexpress both CD47 and PD-L1 are associated with a poor prognosis, highlighting the potential contributions of both innate and adaptive immune evasion mechanisms to the metastatic process [104]. The recently identified liver-secreted protein FGL1 has been recognized as a major functional ligand of lymphocyte-activation gene 3 (LAG-3). Upon binding to LAG-3, the activation of antigen-specific T cells is inhibited [105]. FGL1 + CTCs were detected in 36.7% of patients with HCC [106]. A greater percentage of these patients had advanced TNM stage, distant metastasis, poorer postoperative survival, and resistance to immunotherapy than did patients with FGL– CTCs, indicating the facilitating effect of FGL1 on tumor progression.
Furthermore, CTCs can induce apoptosis in Fas-positive T-helper cells via the Fas/FasL pathway, resulting in a loss of long-term antigen activation in CD8+ T cells and an ineffective antitumor cellular response [107]. Another crucial regulator in the immune evasion of CTCs is the immunosuppressive chemokine CCL5. CCL5 is upregulated within CTCs via the p38/MAX signaling pathway, which recruits Tregs to promote immune evasion and create a prometastatic microenvironment [108]. Tregs in turn secrete TGF-β1 to active the p38/MAX signaling pathway, thereby establishing a positive feedback loop of TGF-β1/p38/MAX/CCL5 signaling pathway.
Apart from the intrinsic adaptive mechanisms discussed above, CTCs also engage in collaborative interactions with other cells present in the bloodstream to evade immune surveillance. Several studies have highlighted the role of platelet activation in facilitating tumor dissemination by providing protection to CTCs from NK cells. NK cell-mediated lysis necessitates direct contact with the target cells, but platelet-forming microthrombi act as a physical barrier, preventing NK cell–CTC contact and thus allowing CTCs to evade NK cell-mediated elimination [109]. Furthermore, platelet coating results in the transfer of platelet-derived normal MHC class I onto the CTC surface, which can be recognized by NK cells via inhibitory killer immunoglobulin-like receptor (KIR), thus inhibiting the cytotoxicity of NK cells [110]. CTCs can engulf platelets and acquire the platelet-derived protein RGS18 during this process [53]. Subsequently, RGS18 activates the AKT/GSK3b/CREB signaling pathway, leading to the upregulation of HLA-E. The elevated levels of HLA-E interact with CD94-NKG2A on NK cells, forming an immune checkpoint pair that hampers immune surveillance against CTCs in circulation. In addition, neutrophils can protect CTCs from immune elimination by dampening NK cell function [111]. MDSCs are recognized for their robust ability to hinder T-cell responses through different mechanisms [112]. Adhesion to MDSCs acts as a defensive barrier for CTCs, providing them with sufficient protection to facilitate immune evasion [113].
In summary, CTCs express immunosuppressive molecules and interact with other cells to induce immune evasion for survival within the bloodstream (Fig. 3).

The survival mechanisms of CTCs in the blood circulation. Resisting to HSS, maintenance of redox balance, acquisition of anoikis resistance and escape immune surveillance contribute to the adaptation and survival of CTCs in the blood circulation. (a) HSS resistance in CTCs is acquired through maintenance of cell membrane integrity, optimization of biophysical properties such as cell stiffness and fluidity, regulation of the cell nucleus, and promotion of cell aggregation. (b) The expression of MnSOD and the metabolic switch mechanisms, including ATOH8-induced HK-2 activation and cell clustering, collectively contribute to constraining ROS levels. SREBP2-mediated TF upregulation confers resistance to ferroptosis on CTCs. (c) CTCs resist anoikis by activating pro-survival signals, producing energy, generating or eliminating ROS, aggregating, and adapting to an acidic tumor microenvironment. (d) CTCs express immunosuppressive molecules and interact with other cells to evade immune surveillance. HSS, hydrodynamic shear stress; ATOH8, Atonal bHLH transcription factor 8; MnSOD, manganese superoxide dismutase; ROS, reactive oxygen species; SREBP2, sterol-regulatory element binding protein 2; TF, Transferrin; TME, tumor microenvironment; PD-L1, regulator programmed death ligand 1; DCs, dendritic cells; Tregs, regulatory cells; MDSCs, myeloid-derived suppressor cells; NK, natural killer; FGL1, fibrinogen-like protein 1; LAG-3, lymphocyte-activation gene 3; MHC I, major histocompatibility complex class I; KIR, inhibitory killer immunoglobulin-like receptor
5 Therapy strategies targeting the survival mechanisms of CTCs
Considering that the majority of patient deaths result from metastasis rather than from the primary tumor, the identification of novel therapeutic targets for early-stage metastasis, particularly focusing on the survival mechanisms of CTCs, holds profound significance. Nonetheless, the pursuit of effective CTC treatments is limited by their scarcity, necessitating further therapeutic investigations. This section is dedicated to providing a comprehensive list of specific drugs that directly target CTCs, regardless of their clinical application (Table 1).
5.1 Restoring antitumor immunity
In recent years, a significant focus of antitumor immunotherapy has centered around the utilization of immune checkpoint inhibitors (ICIs) for treatment. The blockade of immune checkpoints is similar to the release of brakes on antitumor immunity, thereby activating the immune system to eliminate CTCs in the blood circulation. The key mediators in the immune escape of CTCs are PD-L1 and CD47, which act as “do not find me” and “do not eat me” signals, respectively. Immunotherapies targeting PD-1/PD-L1 (such as nivolumab, pembrolizumab, sintilimab and tislelizumab) have demonstrated enhanced therapeutic outcomes in patients with PD-L1-positive CTCs [114]. Individuals with PD-L1 expression on either tissue or CTCs exhibit notably improved median progression-free survival (mPFS) after immunotherapy compared with PD-L1-negative patients. The presence of PD-L1 on CTCs offers a valuable supplementary indicator of the potential efficacy of immunotherapy, aiding in the identification of patient subsets that could derive benefits from such treatment strategies. CD47 can bind to SIRPα on macrophages, transmitting inhibitory signals that dampen phagocytosis. Disrupting the interaction between CD47 and SIRPα promotes macrophage phagocytic activity, stimulates tumor-specific cytotoxic T cells, and triggers the elimination of tumor cells via antibody-dependent cell-mediated cytotoxicity (ADCC) facilitated by NK cells [115, 116]. When CD47 and PD-L1 blocking antibodies are combined, the proportions of T cells and NK cells in the bloodstream increase, impeding the immune escape of CTCs in vivo [117]. In addition, the newly discovered immune checkpoint pair HLA-E:CD94-NKG2A has emerged as a promising target for antitumor drugs. Blockade or knockdown of HLA-E:CD94-NKG2A prevents the metastasis of PDAC [53]. Notably, the effectiveness of NKG2A blockade diminishes when administrated three days after tumor inoculation, suggesting that disrupting HLA-E:CD94-NKG2A primarily affects CTCs in circulation rather than tumor cells already established in metastatic sites. As an exclusive inhibitory immune checkpoint for CTCs, HLA-E:CD94-NKG2A represents a highly promising therapeutic target.
The significant role of platelets in CTC survival has spurred intense interest in identifying agents with antiplatelet properties as potential therapeutic agents for antitumor purposes [118]. Li’s laboratory devised nanoparticles termed Ptx@AlbSNO that release nitric oxide (NO) in the tumor microenvironment [119]. These nanoparticles were engineered to codeliver the antiplatelet agent NO along with the chemotherapeutic agent paclitaxel (Ptx) directly to tumor tissue. The research findings indicated that Ptx@AlbSNO effectively impeded tumor-specific platelet activity, thereby hindering platelet adhesion around CTCs. Furthermore, this approach led to an increase in immune cell infiltration within the tumor microenvironment. This innovative strategy demonstrates the potential to simultaneously target platelet-related functions and bolster the immune response within tumors. Taking advantage of the adhesion of platelets to CTCs, some anticancer drugs can be delivered through platelet cell membrane nanovesicles. CD155, which is prominently expressed on the tumor cell surface, can impair antitumor immunity by binding to its coinhibitory receptor T-cell immunoreceptor with immunoglobulin and the ITIM domain (TIGIT), which is located on the surfaces of NK cells and T cells [120]. Notably, exposure of tumor cells to oxaliplatin (OXA) results in increased CD155 expression. Yu et al. introduced an innovative approach using O-TPNVs (OXA-loaded nanovesicles fused with TIGIT-expressing and platelet cell membranes) [121]. O-TPNVs interact with CTCs, releasing OXA to directly eliminate CTCs and upregulate CD155 expression. Simultaneously, TPNVs disrupt the CD155/TIGIT pathway to restore the activity of CD8 + T cells. This strategy presents a promising avenue for effectively targeting CTCs and revitalizing antitumor immune responses.
5.2 Induction of oxidative stress and ferroptosis
Blood circulation is an oxygen-rich environment, rendering CTCs susceptible to oxidative stress-induced apoptosis and ferroptosis. Therefore, targeting key molecules that maintain redox balance and inducing ferroptosis are more viable strategies for eliminating CTCs.
Several studies have provided evidence that administering antioxidant treatments, either in vitro or in vivo, results in increased survival of CTCs within the bloodstream, ultimately facilitating the progression of distant metastasis [36, 37, 69, 122,123,124]. This phenomenon contradicts the conventional acknowledgment that antioxidants fight cancer. Therefore, pro-oxidant therapies hold promise as potential strategies for cancer intervention. A multitude of drugs that directly or indirectly influence ROS accumulation have been employed in clinical settings for cancer treatment [125]. However, the clinical significance of these pro-oxidative drugs against CTCs has not been explored. Radiotherapy and chemotherapies (including procarbazine, paclitaxel, daunorubicin, doxorubicin (DOX), and cisplatin) exert their anticancer effects in part by inducing oxidative stress to eliminate cancer cells [126]. Given that HSS in the range of 15–30 Dyn cm–2 triggers ROS generation in CTCs [30], anticancer medications such as cisplatin and DOX, which generate ROS, exhibit synergistic effects with HSS against CTCs in lung, breast, and cervical cancers [127]. In contrast, drugs such as Taxol and etoposide, which do not lead to ROS generation, do not have such an impact. Consequently, pro-oxidant therapies offer an approach to enhancing the eradication of CTCs through HSS-generated ROS, thus effectively suppressing metastasis. Jinfukang, a traditional Chinese medicine prescription, is specifically employed for the treatment of lung cancer. Jinfukang can increase ROS levels and trigger apoptosis via DNA damage in circulating lung cancer cells [39]. The important role of the metabolic switch in CTC resistance to ROS has made this process a potential therapeutic target. Cell clustering induces a metabolic switch to glycolysis, and inhibition of this switch by replacing glucose with galactose (forcing cells to undergo mitochondrial oxidative phosphorylation) significantly restricts the growth of cell clusters and increases the level of ROS, leading to cell death induced by oxidative stress [68]. This impairment was also observed in vivo, as evidenced by a reduction in the formation of lung colonies subsequent to tail vein injection of detached cells cultured in galactose.
The ferroptosis inducer RAS-selective lethal-3 (RSL3), which targets the antioxidant enzyme glutathione peroxidase 4 (GPX4), is known to trigger ferroptosis in cancer cells both in vivo and in vitro [128]. CTCs lacking protective mechanisms, such as TF knockdown, are more sensitive to RSL3 [69]. Although ferroptosis inducers have not been administered as therapeutic agents against CTCs, they are attractive drug targets for cancer therapy, especially for CTCs that suffer considerable oxidative damage in high-oxygen and high-iron blood environments.
5.3 Reversal of anoikis resistance
The integrin/Src/FAK signaling pathway, which plays a role in protecting CTCs from anoikis under physiological conditions, represents a potential therapeutic target. For instance, Jinfukang has been shown to induce anoikis in CTCs by suppressing the integrin/Src signaling pathway in NSCLC [129]. The zinc finger transcription factor ZIC2 is upregulated and positively correlated with the CTC counts in patients with NSCLC [130]. Silencing ZIC2 abrogates anoikis resistance and inhibits metastasis in vitro through the transcriptional inhibition of Src. Small molecules targeting FAK can also be applied for cancer treatment. Six FAK inhibitors are currently undergoing clinical trials, demonstrating effective control of tumor growth and metastasis [131, 132]. However, the efficacy of FAK inhibitors in inducing anoikis initiation for the elimination of CTCs has not been extensively investigated.
Platelets can interact with CTCs to protect them from anoikis via YAP1 activation [72]. Preventing platelet adhesion to CTCs and inducing apoptosis are new strategies for cancer therapy. However, conventional antiplatelet drugs have the potential risk of causing bleeding. To address this side effect, Li et al. engineered platelets at the genetic level to express tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), a cytokine expressed on platelet surfaces and known for its ability to induce apoptosis specifically in tumor cells, with the goal of neutralizing CTCs, thereby attenuating metastasis [133]. This innovative strategy achieves the desired therapeutic outcome while avoiding the bleeding risks associated with traditional antiplatelet medications.
Inhibitors targeting enzymes involved in supporting CTC survival after detachment from the ECM can also offer a promising avenue for cancer treatment. GDH1, which contributes to anoikis resistance by facilitating energy production, can be targeted with the small-molecule inhibitor R162 to effectively abrogate anoikis resistance and suppress tumor metastasis [74]. Additionally, as CPT1A-induced FAO promotes anoikis resistance by maintaining redox homeostasis and mitochondrial respiration, inhibiting CPT1A or FAO can disrupt this adaptation in CTCs. Several studies have reported that suppressing CPT1A via pharmacologic inhibitors such as etomoxir and perhexiline or via knockdown promotes anoikis and reduces CTC viability, subsequently inhibiting tumor growth and metastasis in vivo [78,79,80].
Given that metabolic reprogramming enhances CTC survival, normalizing the oxidative metabolism of glucose in cancer cells contributes to restoring CTC anoikis. Glucose oxidation was stimulated by overexpressing PDHE1α or deleting PDK1 in MDA-MB-231 triple-negative metastatic breast cancer cells, which are highly dependent on glycolysis, thus reversing their inherent resistance to anoikis and reducing metastasis in vivo [83]. Consistent with these findings, re-expression of the mitochondrial pyruvate carrier (MPC) suppressed the Warburg effect, leading to an increase in pyruvate oxidation and a decrease in the growth of colon cancer cells in low-attachment culture and in vivo [134]. Moreover, knockdown of the PDK regulator Hif1α reverses glucose metabolism, resulting in cell death upon loss of the cell–matrix contact [85].
5.4 Sensitizing CTCs to HSS
Increased cell stiffness promotes CTC resistance to HSS, and the activation of β-adrenergic signaling can increase cell stiffness through the Ca2+/actin axis, promoting cell invasion and migration [135]. The β-blocker propranolol has been shown to suppress this adaptation in cell deformability both in vivo and in vitro [135,136,137]. Nevertheless, the specific effects of β-adrenergic signaling and the therapeutic potential of propranolol on CTCs remain unclear and require further research for clarification.
CTCs tend to form clusters as a strategy to resist HSS; thus, disrupting CTC clusters has been explored as a potential therapeutic strategy. FAK inhibitor 14 (FAK I-14) is a common chemotherapeutic agent known to weaken cell–cell adhesions. FAK-14 disrupts CTC clusters and reduces the overall resistance of CTCs to HSS, increasing their susceptibility to mechanical forces in the bloodstream [138]. Inhibitors of Na(+)/K(+) ATPase can also cause CTC clusters to dissociate into individual cells [139], subsequently reducing CTC resistance to HSS. Given the role of hypoxia in CTC aggregation, the reversal of tumor hypoxia through proangiogenic therapy can significantly impact CTC resistance to HSS. EphrinB2 is the ligand that activates the signaling of erythropoietin-producing hepatoma receptor B4 (EphB4), which plays a crucial role in ensuring normal and functional angiogenesis [140]. The administration of EphrinB2 has the potential to enhance tumor vascularization and reduce hypoxia within the tumor microenvironment. As a result, this treatment can lead to a decreased rate of shedding of CTC clusters and ultimately contribute to the suppression of metastasis [67].
6 Conclusions
The intricate interplay among the mechanisms discussed previously is crucial for the survival of CTCs in the blood circulation. However, some of these mechanisms operate in a reverse manner, leading to questions about the role of ROS in CTC survival. Specifically, it remains unclear whether ROS facilitate or hinder survival. This uncertainty highlights the need for further investigation, especially concerning the administration of antioxidants or pro-oxidants in antitumor therapy. The impact of ROS on cells is strongly dependent on intracellular ROS levels. The maintenance of a physiological concentration of ROS is necessary for cell survival. However, aberrant accumulation of ROS can stimulate cell proliferation, initiating the pathological conversion of physiological signaling networks and ultimately resulting in the malignant transformation of normal cells [125]. In this review, ROS levels were augmented by detachment from the ECM and elevated oxygen levels and HSS in the bloodstream. The modulation of ROS levels (either decreasing or increasing ROS levels) depends on the stage of cancer metastasis. Metastasis is a complex process governed by diverse regulatory mechanisms at various stages. In the initial phase of metastasis, ECM detachment leads to a rapid surge in ROS levels within cancer cells. To counteract oxidative damage and prevent anoikis, metabolism switches to maintain intracellular redox homeostasis. Following detachment from the ECM, cancer cells become susceptible to anoikis, thereby promoting the activation of NOX4 to enhance prosurvival signaling pathways, such as the EGFR pathway, through ROS generation. Once CTCs enter the blood circulation, the damage they suffer from HSS depends on their location. HSS ranging from 5 to 30 Dyn cm–2 in the arterial circulation produces high levels of ROS to induce apoptosis. In contrast, HSS of 2 Dyn cm–2 in the venous circulation may facilitate CTC survival through ROS generation. Therefore, dual strategies that promote ROS generation to specifically kill CTCs and eliminate aberrantly increased ROS to inhibit survival signaling activation are promising anticancer therapeutic approaches, despite their inherent complexity and contradiction. In conclusion, the effects of ROS on CTCs are intricately linked to the stage of metastasis, the levels of intracellular ROS, and the location of CTCs in circulation.
Generally, CTCs exhibit decreased oxidative metabolism to acquire a survival advantage; in this case, pyruvate is usually converted into lactate instead of fueling the TCA cycle in mitochondria. Consistently, the prometastatic transcription factor Hif1 functions in multiple ways to attenuate oxidative metabolism, including mitophagy and transcriptionally upregulating PDK1 expression. Although oxidative metabolism is greater in CTCs from patients with metastatic melanoma than in those from healthy donors, brain-metastatic melanoma CTC-derived clonal cells have reduced oxidative metabolism and increased glycolysis compared with low-metastatic MeWos cells, indicating the prometastasis feature of glycolysis [141]. These metabolic changes in cells are ultimately reflected in redox homeostasis, which results in ROS regulation at the center of metabolic reprogramming in CTCs. However, the role of oxidative metabolism is controversial as the mitochondrial biogenesis regulator peroxisome proliferator-activated receptor gamma, coactivator 1 alpha (PGC-1α) triggers oxidative phosphorylation in CTCs from a mouse model of breast cancer to facilitate metastasis [142]. In addition, CPT1A also maintains mitochondrial respiration as a strategy for supporting CTC survival against anoikis in ovarian cancer. These alterations act against the adaptive strategies of redox homeostasis utilized by CTCs. However, as we discussed above, the effects of ROS on CTCs are complex and depend on various factors. The effect of oxidative metabolism on CTCs relies on the stage of metastasis, the genetic background and the metabolic profile of the cancer cells, which vary widely. In addition to the metabolic adaptation mentioned above, proline metabolism tends to be catabolic in cancer cells that grow in spheroids, supporting cell growth and promoting lung metastasis [143].
In most cases, the survival mechanisms mentioned above cooperate synergistically to promote CTC survival. For instance, low HSS (2 Dyn cm–2) can trigger EMT in CTCs, enhancing their resistance to HSS, and increasing the stabilization of caveolin-1 in CTCs, thereby preventing anoikis. However, a comprehensive understanding of the intricate crosstalk among these mechanisms necessitates further investigation to identify the specific molecular alterations at certain stages of a particular cancer type, which is important in the development of individualized cancer therapies. Given the diversity of survival mechanisms exploited by CTCs, it is unlikely that there is a one-size-fits-all solution for cancer prevention and treatment based solely on the molecular phenotype/karyotype of CTCs.
Unfortunately, most of the survival mechanisms and corresponding therapies currently under consideration are based primarily on experimental or theoretical extrapolation. Due to the differences in genetic backgrounds, physiological characteristics, and microenvironments between primary tumor cells and CTCs, the efficacies of anticancer drugs can vary significantly on CTCs. Interestingly, there are cases where the levels of effectiveness of certain anticancer drugs are heightened in CTCs, particularly those that generate ROS, such as cisplatin and DOX. Therefore, it is imperative to explore and validate these findings in clinical trials. In conclusion, further studies will need to place strong emphasis on clinical applications, including the identification of therapeutic agents that are specifically effective against CTCs and the optimization of clinical treatment strategies.
Data availability
Not applicable.
References
Fares, J., et al. (2020). Molecular principles of metastasis: A hallmark of cancer revisited. Signal Transduction and Targeted Therapy, 5(1), 28.
Ashworth, T. R. (1869). A case of cancer in which cells similar to those in the tumors were seen in the blood after death. Australas Med J, 14, 146–149.
Taddei, M. L., et al. (2012). Anoikis: An emerging hallmark in health and diseases. The Journal of Pathology, 226(2), 380–393.
Kanwar, N., et al. (2015). Identification of genomic signatures in circulating tumor cells from breast cancer. International Journal of Cancer, 137(2), 332–344.
Chang, T. Y. (2021). Comparison of genetic profiling between primary tumor and circulating Tumor cells captured by Microfluidics in Epithelial Ovarian Cancer: Tumor Heterogeneity or Allele Dropout? Diagnostics (Basel) 11 (6).
Zou, L., et al. (2020). Genome–wide copy number analysis of circulating tumor cells in breast cancer patients with liver metastasis. Oncology Reports, 44(3), 1075–1093.
Chiu, C. G., et al. (2014). Genome-wide characterization of circulating tumor cells identifies novel prognostic genomic alterations in systemic melanoma metastasis. Clinical Chemistry, 60(6), 873–885.
Steinert, G., et al. (2014). Immune escape and survival mechanisms in circulating Tumor cells of Colorectal Cancer. Cancer Research, 74(6), 1694–1704.
Müller, V., et al. (2005). Circulating tumor cells in breast cancer: Correlation to bone marrow micrometastases, heterogeneous response to systemic therapy and low proliferative activity. Clinical Cancer Research, 11(10), 3678–3685.
Gires, O. A. O. Expression and function of epithelial cell adhesion molecule EpCAM: Where are we after 40 years? (1573–7233 (Electronic)).
Thiery, J. P. (2003). Epithelial–mesenchymal transitions in development and pathologies. Current Opinion in Cell Biology, 15(6), 740–746.
Huang, Y., et al. (2022). The molecular mechanisms and therapeutic strategies of EMT in tumor progression and metastasis. Journal of Hematology & Oncology, 15(1), 129.
Huaman, J. (2019). Fibronectin regulation of integrin B1 and SLUG in circulating Tumor cells. Cells 8 (6).
Lecharpentier, A., et al. (2011). Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer. British Journal of Cancer, 105(9), 1338–1341.
Yu, M., et al. (2013). Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science, 339(6119), 580–584.
Armstrong, A. J., et al. (2011). Circulating tumor cells from patients with advanced prostate and breast cancer display both epithelial and mesenchymal markers. Molecular Cancer Research, 9(8), 997–1007.
Kallergi, G., et al. (2011). Epithelial to mesenchymal transition markers expressed in circulating tumour cells of early and metastatic breast cancer patients. Breast Cancer Research, 13(3), R59.
Liu, X., et al. (2019). Epithelial-type systemic breast carcinoma cells with a restricted mesenchymal transition are a major source of metastasis. Science Advances, 5(6), eaav4275.
Chaffer, C. L., et al. (2006). Mesenchymal-to-epithelial transition facilitates bladder cancer metastasis: Role of fibroblast growth factor receptor-2. Cancer Research, 66(23), 11271–11278.
Yamamoto, M., et al. (2017). Intratumoral bidirectional transitions between epithelial and mesenchymal cells in triple-negative breast cancer. Cancer Science, 108(6), 1210–1222.
Yang, M. H., et al. (2015). Circulating cancer stem cells: The importance to select. Chinese Journal of Cancer Research, 27(5), 437–449.
Theodoropoulos, P. A., et al. (2010). Circulating tumor cells with a putative stem cell phenotype in peripheral blood of patients with breast cancer. Cancer Letters, 288(1), 99–106.
Wan, S., et al. (2019). New Labyrinth Microfluidic device detects circulating Tumor cells expressing Cancer stem cell marker and circulating Tumor Microemboli in Hepatocellular Carcinoma. Scientific Reports, 9(1), 18575.
Morel, A. P. (2008). Generation of breast cancer stem cells through epithelial-mesenchymal transition. PLoS One 3 (8), e2888.
Mani, S. A., et al. (2008). The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell, 133(4), 704–715.
Papadaki, M. A., et al. (2019). Circulating Tumor cells with stemness and Epithelial-To-Mesenchymal Transition Features Are Chemoresistant and Predictive of poor outcome in metastatic breast Cancer. Molecular Cancer Therapeutics, 18(2), 437–447.
Follain, G., et al. (2020). Fluids and their mechanics in tumour transit: Shaping metastasis. Nature Reviews Cancer, 20(2), 107–124.
Headley, M. B., et al. (2016). Visualization of immediate immune responses to pioneer metastatic cells in the lung. Nature, 531(7595), 513–517.
Chang, S. F., et al. (2008). Tumor cell cycle arrest induced by shear stress: Roles of integrins and smad. Proc Natl Acad Sci U S A, 105(10), 3927–3932.
Fu, A., et al. (2016). High expression of MnSOD promotes survival of circulating breast cancer cells and increases their resistance to doxorubicin. Oncotarget, 7(31), 50239–50257.
Regmi, S., et al. (2017). High Shear stresses under Exercise Condition destroy circulating Tumor cells in a Microfluidic System. Scientific Reports, 7, 39975.
Kienast, Y., et al. (2010). Real-time imaging reveals the single steps of brain metastasis formation. Nature Medicine, 16(1), 116–122.
Marrella, A. (2021). High blood flow shear stress values are associated with circulating tumor cells cluster disaggregation in a multi-channel microfluidic device. PLoS One 16 (1), e0245536.
Jasuja, H., et al. (2023). Interstitial fluid flow contributes to prostate cancer invasion and migration to bone; study conducted using a novel horizontal flow bioreactor. Biofabrication, 15(2), 025017.
Kim, O. H., et al. (2022). Fluid shear stress facilitates prostate cancer metastasis through Piezo1-Src-YAP axis. Life Sciences, 308, 120936.
Piskounova, E., et al. (2015). Oxidative stress inhibits distant metastasis by human melanoma cells. Nature, 527(7577), 186–191.
Schafer, Z. T., et al. (2009). Antioxidant and oncogene rescue of metabolic defects caused by loss of matrix attachment. Nature, 461(7260), 109–113.
Redza-Dutordoir, M., & Averill-Bates, D. A. (2016). Activation of apoptosis signalling pathways by reactive oxygen species. Biochimica Et Biophysica Acta, 1863(12), 2977–2992.
Que, Z., et al. (2019). Jingfukang induces anti-cancer activity through oxidative stress-mediated DNA damage in circulating human lung cancer cells. Bmc Complementary and Alternative Medicine, 19(1), 204.
Ubellacker, J. M., et al. (2020). Lymph protects metastasizing melanoma cells from ferroptosis. Nature, 585(7823), 113–118.
Paoli, P., et al. (2013). Anoikis molecular pathways and its role in cancer progression. Biochimica Et Biophysica Acta, 1833(12), 3481–3498.
Khan, S. U., et al. (2022). Understanding the cell survival mechanism of anoikis-resistant cancer cells during different steps of metastasis. Clinical & Experimental Metastasis, 39(5), 715–726.
Mohme, M., et al. (2017). Circulating and disseminated tumour cells - mechanisms of immune surveillance and escape. Nature Reviews. Clinical Oncology, 14(3), 155–167.
Vivier, E., et al. (2018). Innate lymphoid cells: 10 years on. Cell, 174(5), 1054–1066.
Cornel, A. M. (2020). MHC Class I Downregulation in Cancer: Underlying Mechanisms and Potential Targets for Cancer Immunotherapy. Cancers (Basel) 12 (7).
Kärre, K., et al. (1986). Selective rejection of H–2-deficient lymphoma variants suggests alternative immune defence strategy. Nature, 319(6055), 675–678.
Ljunggren, H. G., & Kärre, K. (1985). Host resistance directed selectively against H-2-deficient lymphoma variants. Analysis of the mechanism. Journal of Experimental Medicine, 162(6), 1745–1759.
Brodbeck, T., et al. (2014). Perforin-dependent direct cytotoxicity in natural killer cells induces considerable knockdown of spontaneous lung metastases and computer modelling-proven tumor cell dormancy in a HT29 human colon cancer xenograft mouse model. Molecular Cancer, 13, 244.
Gül, N., et al. (2014). Macrophages eliminate circulating tumor cells after monoclonal antibody therapy. J Clin Invest, 124(2), 812–823.
Xue, D., et al. (2018). Role of regulatory T cells and CD8(+) T lymphocytes in the dissemination of circulating tumor cells in primary invasive breast cancer. Oncol Lett, 16(3), 3045–3053.
Liu, J., et al. (2019). Increased stromal infiltrating lymphocytes are Associated with circulating Tumor cells and metastatic relapse in breast Cancer patients after Neoadjuvant Chemotherapy. Cancer Manag Res, 11, 10791–10800.
Smolkova, B., et al. (2020). Increased stromal infiltrating lymphocytes are Associated with the risk of Disease Progression in Mesenchymal circulating Tumor cell-positive primary breast Cancer patients. International Journal of Molecular Sciences, 21, 24.
Liu, X., et al. (2023). Immune checkpoint HLA-E:CD94-NKG2A mediates evasion of circulating tumor cells from NK cell surveillance. Cancer Cell, 41(2), 272–287. e9.
Lo, H. C., et al. (2020). Resistance to natural killer cell immunosurveillance confers a selective advantage to polyclonal metastasis. Nat Cancer, 1(7), 709–722.
Hope, J. M. (2021). Circulating prostate cancer cells have differential resistance to fluid shear stress-induced cell death. Journal of Cell Science 134 (4).
Barnes, J. M. (2012). Resistance to fluid shear stress is a conserved biophysical property of malignant cells. PLoS One 7 (12), e50973.
Moose, D. L., et al. (2020). Cancer cells resist Mechanical Destruction in circulation via RhoA/Actomyosin-Dependent mechano-adaptation. Cell Rep, 30(11), 3864–3874e6.
Choi, H. Y., et al. (2019). Hydrodynamic shear stress promotes epithelial-mesenchymal transition by downregulating ERK and GSK3β activities. Breast Cancer Research, 21(1), 6.
Chen, X., et al. (2022). YAP1 activation promotes epithelial-mesenchymal transition and cell survival of renal cell carcinoma cells under shear stress. Carcinogenesis, 43(4), 301–310.
Mitchell, M. J., et al. (2015). Lamin A/C deficiency reduces circulating tumor cell resistance to fluid shear stress. American Journal of Physiology. Cell Physiology, 309(11), C736–C746.
Xu, Z. (2022). Fluid shear stress regulates the survival of circulating tumor cells via nuclear expansion. Journal of Cell Science 135 (10).
Maeshiro, M., et al. (2021). Colonization of distant organs by tumor cells generating circulating homotypic clusters adaptive to fluid shear stress. Scientific Reports, 11(1), 6150.
Ortiz-Otero, N., et al. (2020). Cancer associated fibroblasts confer shear resistance to circulating tumor cells during prostate cancer metastatic progression. Oncotarget, 11(12), 1037–1050.
Hagihara, T., et al. (2019). Hydrodynamic stress stimulates growth of cell clusters via the ANXA1/PI3K/AKT axis in colorectal cancer. Scientific Reports, 9(1), 20027.
Osmulski, P. A., et al. (2021). Contacts with macrophages promote an aggressive Nanomechanical phenotype of circulating Tumor cells in prostate Cancer. Cancer Research, 81(15), 4110–4123.
Huang, Q., et al. (2020). Shear stress activates ATOH8 via autocrine VEGF promoting glycolysis dependent-survival of colorectal cancer cells in the circulation. Journal of Experimental & Clinical Cancer Research : Cr, 39(1), 25.
Donato, C., et al. (2020). Hypoxia triggers the intravasation of clustered circulating Tumor cells. Cell Rep, 32(10), 108105.
Labuschagne, C. F., et al. (2019). Cell clustering promotes a metabolic switch that supports metastatic colonization. Cell Metab, 30(4), 720–734e5.
Hong, X., et al. (2021). The Lipogenic Regulator SREBP2 induces transferrin in circulating Melanoma cells and suppresses ferroptosis. Cancer Discovery, 11(3), 678–695.
Sun, B., et al. (2017). Midkine promotes hepatocellular carcinoma metastasis by elevating anoikis resistance of circulating tumor cells. Oncotarget, 8(20), 32523–32535.
Malin, D., et al. (2015). ERK-regulated alphab-crystallin induction by matrix detachment inhibits anoikis and promotes lung metastasis in vivo. Oncogene, 34(45), 5626–5634.
Haemmerle, M., et al. (2017). Platelets reduce anoikis and promote metastasis by activating YAP1 signaling. Nature Communications, 8(1), 310.
Jin, L., et al. (2015). Glutamate dehydrogenase 1 signals through Antioxidant Glutathione Peroxidase 1 to regulate Redox Homeostasis and Tumor Growth. Cancer Cell, 27(2), 257–270.
Jin, L., et al. (2018). The PLAG1-GDH1 Axis promotes Anoikis Resistance and Tumor Metastasis through CamKK2-AMPK Signaling in LKB1-Deficient Lung Cancer. Molecular Cell, 69(1), 87–99e7.
Chen, X., et al. (2022). Shear stress enhances anoikis resistance of cancer cells through ROS and NO suppressed degeneration of Caveolin-1. Free Radical Biology and Medicine, 193(Pt 1), 95–107.
Kim, H., et al. (2017). Regulation of anoikis resistance by NADPH oxidase 4 and epidermal growth factor receptor. British Journal of Cancer, 116(3), 370–381.
Du, S., et al. (2018). NADPH oxidase 4 regulates anoikis resistance of gastric cancer cells through the generation of reactive oxygen species and the induction of EGFR. Cell Death and Disease, 9(10), 948.
Tian, T., et al. (2022). CPT1A promotes anoikis resistance in esophageal squamous cell carcinoma via redox homeostasis. Redox Biology, 58, 102544.
Wang, Y. N., et al. (2018). CPT1A-mediated fatty acid oxidation promotes colorectal cancer cell metastasis by inhibiting anoikis. Oncogene, 37(46), 6025–6040.
Sawyer, B. T., et al. (2020). Targeting fatty acid oxidation to promote Anoikis and inhibit ovarian Cancer progression. Molecular Cancer Research, 18(7), 1088–1098.
Koppenol, W. H., et al. (2011). Otto Warburg’s contributions to current concepts of cancer metabolism. Nature Reviews Cancer, 11(5), 325–337.
Stacpoole, P. W. (2017). Therapeutic targeting of the Pyruvate Dehydrogenase Complex/Pyruvate Dehydrogenase Kinase (PDC/PDK) Axis in Cancer. JNCI: Journal of the National Cancer Institute, 109, 11.
Kamarajugadda, S., et al. (2012). Glucose oxidation modulates anoikis and tumor metastasis. Molecular and Cellular Biology, 32(10), 1893–1907.
Kim, J., et al. (2006). HIF-1-mediated expression of pyruvate dehydrogenase kinase: A metabolic switch required for cellular adaptation to hypoxia. Cell Metabolism, 3(3), 177–185.
Maurer, G. D., et al. (2019). Loss of cell-matrix contact increases hypoxia-inducible factor-dependent transcriptional activity in glioma cells. Biochemical and Biophysical Research Communications, 515(1), 77–84.
Zhao, T. (2014). HIF-1-mediated metabolic reprogramming reduces ROS levels and facilitates the metastatic colonization of cancers in lungs. Scientific Reports 4 (1).
Lingwood, D., & Simons, K. (2010). Lipid rafts as a membrane-Organizing Principle. 327 (5961), 46–50.
del Pozo, M. A., et al. (2005). Phospho-caveolin-1 mediates integrin-regulated membrane domain internalization. Nature Cell Biology, 7(9), 901–908.
Li, D. (2023). Cell aggregation activates small GTPase Rac1 and induces CD44 cleavage by maintaining lipid raft integrity. Journal of Biological Chemistry 299 (12).
Han, H. J., et al. (2021). Fibronectin regulates anoikis resistance via cell aggregate formation. Cancer Letters, 508, 59–72.
Peppicelli, S. (2019). Anoikis Resistance as a Further Trait of Acidic-Adapted Melanoma Cells. J Oncol 2019, 8340926.
Corbet, C., et al. (2020). TGFβ2-induced formation of lipid droplets supports acidosis-driven EMT and the metastatic spreading of cancer cells. Nature Communications, 11(1), 454.
Wheatley, S. P., & Altieri, D. C. (2019). Survivin at a glance. Journal of Cell Science, 132, 7.
Végran, F., et al. (2013). Survivin-3B potentiates immune escape in cancer but also inhibits the toxicity of cancer chemotherapy. Cancer Research, 73(17), 5391–5401.
Yie, S. M. (2006). Detection of Survivin-expressing circulating cancer cells in the peripheral blood of breast cancer patients by a RT-PCR ELISA. Clinical & Experimental Metastasis 23 (5–6), 279 – 89.
Yie, S., et al. (2008). Detection of Survivin-expressing circulating Cancer cells (CCCs) in Peripheral blood of patients with gastric and colorectal Cancer reveals high risks of Relapse. Annals of Surgical Oncology, 15(11), 3073–3082.
Yie, S. M., et al. (2009). Clinical significance of detecting survivin-expressing circulating cancer cells in patients with non-small cell lung cancer. Lung Cancer, 63(2), 284–290.
Cao, M., et al. (2009). Detection of survivin-expressing circulating cancer cells in the peripheral blood of patients with esophageal squamous cell carcinoma and its clinical significance. Clinical & Experimental Metastasis, 26(7), 751–758.
Ning, Y., et al. (2015). Cytokeratin-20 and survivin-expressing circulating Tumor cells predict survival in metastatic colorectal Cancer patients by a combined immunomagnetic qRT-PCR Approach. Molecular Cancer Therapeutics, 14(10), 2401–2408.
Lu, J., et al. (2023). Association of survivin positive circulating tumor cell levels with immune escape and prognosis of osteosarcoma. Journal of Cancer Research and Clinical Oncology, 149(15), 13741–13751.
Sun, C., et al. (2018). Regulation and function of the PD-L1 checkpoint. Immunity, 48(3), 434–452.
Mazel, M., et al. (2015). Frequent expression of PD-L1 on circulating breast cancer cells. Molecular Oncology, 9(9), 1773–1782.
Kong, D., et al. (2021). Correlation between PD-L1 expression ON CTCs and prognosis of patients with cancer: A systematic review and meta-analysis. Oncoimmunology, 10(1), 1938476.
Papadaki, M. A. (2020). Clinical Relevance of Immune Checkpoints on Circulating Tumor Cells in Breast Cancer. Cancers (Basel) 12 (2).
Wang, J., et al. (2019). Fibrinogen-like protein 1 is a major Immune Inhibitory ligand of LAG-3. Cell, 176(1–2), 334–347e12.
Yan, Q., et al. (2022). Immune Checkpoint FGL1 expression of circulating Tumor cells is Associated with Poor Survival in Curatively Resected Hepatocellular Carcinoma. Frontiers in Oncology, 12, 810269.
Gruber, I., et al. (2013). Relationship between circulating tumor cells and peripheral T-cells in patients with primary breast cancer. Anticancer Research, 33(5), 2233–2238.
Sun, Y. F., et al. (2021). Dissecting spatial heterogeneity and the immune-evasion mechanism of CTCs by single-cell RNA-seq in hepatocellular carcinoma. Nature Communications, 12(1), 4091.
Palumbo, J. S., et al. (2005). Platelets and fibrin(ogen) increase metastatic potential by impeding natural killer cell-mediated elimination of tumor cells. Blood, 105(1), 178–185.
Placke, T., et al. (2012). Platelet-derived MHC class I confers a pseudonormal phenotype to cancer cells that subverts the antitumor reactivity of natural killer immune cells. Cancer Research, 72(2), 440–448.
Spiegel, A., et al. (2016). Neutrophils suppress intraluminal NK cell-mediated Tumor Cell Clearance and enhance extravasation of disseminated carcinoma cells. Cancer Discovery, 6(6), 630–649.
Gabrilovich, D. I., & Nagaraj, S. (2009). Myeloid-derived suppressor cells as regulators of the immune system. Nature Reviews Immunology, 9(3), 162–174.
Liu, Q., et al. (2016). Myeloid-derived suppressor cells (MDSC) facilitate distant metastasis of malignancies by shielding circulating tumor cells (CTC) from immune surveillance. Medical Hypotheses, 87, 34–39.
Zhou, Q., et al. (2023). Circulating tumor cells PD-L1 expression detection and correlation of therapeutic efficacy of immune checkpoint inhibition in advanced non-small-cell lung cancer. Thorac Cancer, 14(5), 470–478.
Murata, Y., et al. (2018). CD47-signal regulatory protein alpha signaling system and its application to cancer immunotherapy. Cancer Science, 109(8), 2349–2357.
Liu, Y., et al. (2023). Emerging phagocytosis checkpoints in cancer immunotherapy. Signal Transduct Target Ther, 8(1), 104.
Lian, S., et al. (2019). Dual blockage of both PD-L1 and CD47 enhances immunotherapy against circulating tumor cells. Scientific Reports, 9(1), 4532.
Mammadova-Bach, E., et al. (2015). Platelets in cancer. From basic research to therapeutic implications. Hamostaseologie, 35(4), 325–336.
Xu, Y., et al. (2020). Blockade of platelets using tumor-specific NO-Releasing nanoparticles prevents Tumor Metastasis and reverses Tumor Immunosuppression. Acs Nano, 14(8), 9780–9795.
Wang, D., et al. (2022). Role of CD155/TIGIT in Digestive cancers: Promising Cancer Target for Immunotherapy. Frontiers in Oncology, 12, 844260.
Yu, Y., et al. (2022). Engineered drug-loaded cellular membrane nanovesicles for efficient treatment of postsurgical cancer recurrence and metastasis. Science Advances, 8(49), eadd3599.
Wang, H., et al. (2016). NRF2 activation by antioxidant antidiabetic agents accelerates tumor metastasis. Science Translational Medicine, 8(334), 334ra51.
Sayin, V. I., et al. (2014). Antioxidants accelerate lung cancer progression in mice. Science Translational Medicine, 6(221), 221ra15.
Zheng, Y., et al. (2017). Expression of β-globin by cancer cells promotes cell survival during blood-borne dissemination. Nature Communications, 8, 14344.
Wang, Y., et al. (2021). The double-edged roles of ROS in cancer prevention and therapy. Theranostics, 11(10), 4839–4857.
Tasdogan, A., et al. (2021). Redox Regulation in Cancer cells during metastasis. Cancer Discovery, 11(11), 2682–2692.
Regmi, S., et al. (2018). Fluidic shear stress increases the anti-cancer effects of ROS-generating drugs in circulating tumor cells. Breast Cancer Research and Treatment, 172(2), 297–312.
Yang, W. S., et al. (2014). Regulation of Ferroptotic Cancer Cell death by GPX4. Cell, 156(1–2), 317–331.
Que, Z. J., et al. (2021). Jinfukang regulates integrin/Src pathway and anoikis mediating circulating lung cancer cells migration. Journal of Ethnopharmacology, 267, 113473.
Liu, A., et al. (2021). Silencing ZIC2 abrogates tumorigenesis and anoikis resistance of non-small cell lung cancer cells by inhibiting Src/FAK signaling. Mol Ther Oncolytics, 22, 195–208.
Pang, X. J., et al. (2021). Drug Discovery Targeting Focal Adhesion kinase (FAK) as a Promising Cancer Therapy. Molecules, 26, 14.
Spallarossa, A. (2022). The development of FAK inhibitors: A five-year update. International Journal of Molecular Sciences 23 (12).
Li, J., et al. (2016). Genetic engineering of platelets to neutralize circulating tumor cells. Journal of Controlled Release : Official Journal of the Controlled Release Society, 228, 38–47.
Schell, J. C., et al. (2014). A role for the mitochondrial pyruvate carrier as a Repressor of the Warburg effect and Colon cancer cell growth. Molecular Cell, 56(3), 400–413.
Kim, T. H., et al. (2016). Cancer cells become less deformable and more invasive with activation of beta-adrenergic signaling. Journal of Cell Science, 129(24), 4563–4575.
Sloan, E. K., et al. (2010). The sympathetic nervous system induces a metastatic switch in primary breast cancer. Cancer Research, 70(18), 7042–7052.
Le, C. P., et al. (2016). Chronic stress in mice remodels lymph vasculature to promote tumour cell dissemination. Nature Communications, 7, 10634.
Au, S. H., et al. (2016). Clusters of circulating tumor cells traverse capillary-sized vessels. Proc Natl Acad Sci U S A, 113(18), 4947–4952.
Gkountela, S., et al. (2019). Circulating Tumor Cell Clustering shapes DNA methylation to Enable Metastasis Seeding. Cell, 176(1–2), 98–112e14.
Du, E., et al. (2020). The critical role of the interplays of EphrinB2/EphB4 and VEGF in the induction of angiogenesis. Molecular Biology Reports, 47(6), 4681–4690.
Bowley, T. Y. (2023). Targeting Translation and the Cell Cycle Inversely Affects CTC Metabolism but Not Metastasis. Cancers (Basel) 15 (21).
LeBleu, V. S., et al. (2014). PGC-1α mediates mitochondrial biogenesis and oxidative phosphorylation in cancer cells to promote metastasis. Nature Cell Biology, 16(10), 992–1003.
Elia, I. (2017). Proline metabolism supports metastasis formation and could be inhibited to selectively target metastasizing cancer cells. Nature Communications 8 (1).
Acknowledgements
Figures were created with FigDraw (www.figdraw.com).
Funding
This research was supported by the National Natural Science Foundation of China (82073059, 82103364); the Sichuan Science and Technology Program (2022YFS0204); the Post-doctor Research Project, West China Hospital (2023HXBH127).
Author information
Authors and Affiliations
Contributions
F.B made contributions to the conception and design. S.Z and H.X wrote the manuscript. Y.D and H.H completed the figures. Q.T helped to revise the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare that there are no conflicts of interest regarding the publication of this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhou, S., Xu, H., Duan, Y. et al. Survival mechanisms of circulating tumor cells and their implications for cancer treatment. Cancer Metastasis Rev 43, 941–957 (2024). https://doi.org/10.1007/s10555-024-10178-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10555-024-10178-7