
Abstract
Left ventricular (LV) geometric patterns aid clinicians in the diagnosis and prognostication of various cardiomyopathies. The aim of this study is to assess the accuracy and reproducibility of LV dimensions and wall thickness using deep learning (DL) models. A total of 30,080 unique studies were included; 24,013 studies were used to train a convolutional neural network model to automatically assess, at end-diastole, LV internal diameter (LVID), interventricular septal wall thickness (IVS), posterior wall thickness (PWT), and LV mass. The model was trained to select end-diastolic frames with the largest LVID and to identify four landmarks, marking the dimensions of LVID, IVS, and PWT using manually labeled landmarks as reference. The model was validated with 3,014 echocardiographic cines and the accuracy of the model was evaluated with a test set of 3,053 echocardiographic cines. The model accurately measured LVID, IVS, PWT, and LV mass compared to study report values with a mean relative error of 5.40%, 11.73%, 12.76%, and 13.93%, respectively. The 𝑅2 of the model for the LVID, IVS, PWT, and the LV mass was 0.88, 0.63, 0.50, and 0.87, respectively. The novel DL model developed in this study was accurate for LV dimension assessment without the need to select end-diastolic frames manually. DL automated measurements of IVS and PWT were less accurate with greater wall thickness. Validation studies in larger and more diverse populations are ongoing.
Graphical Abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Left ventricular (LV) geometric patterns provide clues in the diagnosis, management, and monitoring of cardiovascular diseases. Two-dimensional (2D) transthoracic echocardiography is an accessible and reliable imaging modality routinely used for the measurement of LV dimensions and wall thickness, which has been shown to predict prognosis in various cardiomyopathies [1,2,3,4,5]. Diagnostic accuracy of transthoracic echocardiogram interpretations by a novice interpreter is low, and an accurate assessment of LV geometry using echocardiography may be limited by the requirement of an experienced interpreter [6,7,8]. Further, these measurements have been shown to show significant interobserver and intraobserver variability [9]. Automation of echocardiographic interpretation using deep learning (DL) can potentially allow non-experts to assess LV dimensions and wall thickness with an accuracy comparable to experts while eliminating intraobserver variability, thus improving reproducibility [10]. As predictions made by DL models are subject to noise and inference errors, it is important to be able to represent uncertainty in the model’s predictions [11]. Previous DL models measuring LV dimensions lacked uncertainty quantification and required manual input of individual end-diastolic frames for data analysis, which limited their real-life applicability [12,13,14]. The aim of this study is to determine the accuracy and reproducibility of DL derived LV dimensions and wall thickness with incorporation of prediction uncertainty.
Methods
Study population
All transthoracic echocardiography studies of consecutive patients ≥ 18 years old from 01/01/2017 to 12/31/2021 at a single tertiary care center with annotations for the measurement of LV dimensions that were verified by level 3 echocardiographers were included in the development of the model. The echocardiographic cines were split in 80:10:10 proportions for training, validation, and testing respectively. The study was approved by the University of British Columbia Clinical Research Ethics Board.
Two-dimensional transthoracic echocardiography and preprocessing
Transthoracic echocardiogram studies were performed by certified academic sonographers using standard commercially available ultrasound systems E9 [GE Healthcare, Milwaukee, WI], EPIQ [Philips Medical Imaging, Andover, MA]), and iE33 [Philips Medical Imaging, Andover, MA]) and recorded on an image and information system (Syngo Dynamics [Siemens Medical Solutions, Ann Arbor, MI]). The distribution of the machines used for data acquisition was E9 (7%), iE33 (43%), and EPIQ (50%). Echocardiographic images were acquired, and measurements were performed offline in accordance with the recommendations of the American Society of Echocardiography [15]. End-diastolic frames were identified visually by frames with the greatest LV cavity. Left ventricular internal diameter (LVID) was measured at end-diastole in the LV minor axis plane at the level of mitral valve leaflet tips. The anteroseptal and inferolateral septal wall thickness were measured at end-diastole to assess the interventricular septum at end-diastole (IVS) and posterior wall thickness at end-diastole (PWT) respectively. LV mass was calculated using the Cube formula. All measurements were verified by a level 3 echocardiographer at our center. All annotations, on-screen texts, and identifications were removed, and the parasternal long axis (PLAX) videos were converted to multidimensional numeric arrays of pixels, which were resized to 224 × 224 while maintaining the aspect ratio, by adding pad pixels of 0 value while maintaining the beam in the center.
Deep learning model development and training
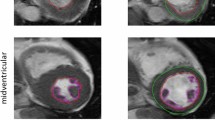
We developed and trained our convolutional neural network model using the open-source library Keras with TensorFlow backend in Python. We used a U-net architecture with skip connections. The downstream (first half of the U-net) consisted of four sets of two 2D-convolutional layers with three max-pooling layers in between and the upstream (second half of the U-net) consisted of two sets of two 2D-convolutional layers, with upsampling at the beginning of each set, followed by two output heads, each consisting of another upsampling layer, two 2D-convolutional layers, and a full connected layer with sigmoid activation function to generate binary segmentation map for that output head. The number of convolutional kernels started from 8 and increased to 64 by the end of the downstream section, and decreased from 32 to 8 in the upstream section. All 2D convolutional kernels had the kernel size of 3 × 3 pixels. The model was optimized for image segmentation to perform landmark detection. The model first identified the correct end-diastolic frames in the cine loops, then used the end-diastolic frames to train end-to-end a two-foci network, with one focus responsible for finding a pair of the landmarks at the septal endocardial border and the inferolateral wall endocardial border below the level of the mitral valve leaflet tips. The other focus was responsible for finding a pair of landmarks to identify the pericardium and right ventricular endocardial border for estimation of IVS and PWT respectively (Fig. 1).
The model selected the correct end-diastolic frames with the largest LVID to identify key landmarks for measuring the LV dimensions in each cine. LVID was measured for all the frames of a PLAX video, and the frame with the largest LVID measurement was used as the end-diastolic frame for further measurement (Fig. 2). Using manually labeled annotations as a reference, the model was trained to automatically measure the LVID, IVS, PWT, and LV mass. Each frame was processed individually, and no temporal information was used. Measurements of LVID, IVS, and PWT were done as a postprocessing step.

Architecture of the deep neural network framework

Frame-by-frame assessment of left ventricular internal diameter (LVID) in all frames of a parasternal long axis video using the deep neural network model
The model was validated with 10% of the total echocardiographic cines, which were also used to calibrate the prediction uncertainty. We then evaluated prediction uncertainty in all of the test sets. Prediction uncertainty was presented as a binary result, and an echocardiographic cine was discarded by the model if the model identified > 2 landmark locations per focus or was unable to generate predictions in five consecutive frames around the end-diastolic frames, or if the Z-score of uncertainties was > 1 based on our validation set. The accuracy of the model was evaluated with a test set from the remaining 10% of the echocardiographic cines, and the mean relative error and 𝑅2 scores were calculated.
The model was trained for 100 epochs, meaning that each training data was seen by the model 100 times. To prevent overfitting on or memorizing the training data, each image was augmented with random rotation (up to 10 degrees), horizontal and vertical shift (by 10% of the image resolution), and zooming in (to up to 90% of the image size). Each batch of input data at each training iteration consisted of 16 end-diastolic frames of 16 randomly selected echo cines. To optimize the model, DICE loss and binary cross-entropy loss were used as the error measures, with equal weight. These were applied on both output heads. The ADAM optimizer with the learning rate of 0.001 was used.
Statistical analysis
Statistical analyses were performed using SAS v9.4 (SAS Institute, Cary, North Carolina). Continuous variables were expressed as mean ± standard deviation. Categorical variables were expressed as numbers (percentages). Data was analyzed using two-way ANOVA, chi-square, and student’s t-test. A p-value of < 0.05 was taken to be significant.
Results
A total of 30,080 unique transthoracic echocardiographic cines from the parasternal long-axis (PLAX) view over a 5-year period were used to train, validate, and test a convolutional neural network model to automatically assess LV dimensions. A total of 24,013 unique studies were used to train the model, and the model was validated with 3,014 echocardiographic cines, which were also used to calibrate the prediction uncertainty. The accuracy of the model was evaluated with a test set of 3,053 echocardiographic cines (Fig. 3). We note that the training, validation, and test sets had mutually exclusive group of patients.

Echocardiographic cines distribution for the model development
In our test set of 3,053 echocardiographic cines, a total of 240 echocardiographic cines were discarded due to high uncertainty. Of the remaining 2813 echocardiographic cines, our model automatically measured the LVID, IVS, PWT, and LV mass with a mean percent error of 5.40%, 11.73%, 12.76%, and 13.93%, and with a mean absolute error of 2.4 mm, 1.1 mm, 1.2 mm, and 20.8 g respectively (Figs. 4 and 5).The 𝑅2 of the model for the LVID, IVS, PWT, and the LV mass was 0.88, 0.63, 0.50, and 0.87 respectively. Our model prediction on all of the measurements improved in its accuracy with prediction uncertainty, and the analysis of the rejected cases demonstrated poor model prediction (Table 1).

Scatter plot and regression of predicted left ventricular dimension measurement using deep neural network models

Blind-Altman plots for the mean percent error
Our model had similar mean percentage error compared to the state-of-the-art models in landmark detection of LVID, IVS, and PWT (Table 2). Model prediction for IVS and PWT were less accurate than LV mass and LVID, especially with very large LV wall thickness. Our model predictions were more accurate or at least similar to human interobserver variability between two independent expert readers using manual measurements (Table 3) [6]. On average, the model generated an output of 270 frames/second, processing each frame in 3.7ms.
We assessed our model’s accuracy of the classification model in predicting LV geometry pattern based on the 2015 ASE/EACVI guideline (Fig. 6) [15]. Our model was able to accurately categorize the LV geometry pattern with F1 scores of 0.73, 0.58, 0.62, and 0.44 (normal, concentric remodeling, eccentric hypertrophy, and concentric hypertrophy respectively).

Confusion matrix demonstrating the accuracy of the classification models in predicting the left ventricular geometry pattern based on the 2015 ASE/EACVI guidelines
Discussion
To the best of our knowledge, the dataset of 2D transthoracic echocardiography studies used for the development of this DL model for assessing LV dimension and wall thickness represented the largest of all datasets that have been used for similar development. The principal findings of this study are as follows: (1) the novel DL model was able to accurately assess the LV wall dimension; (2) the model was able to automatically estimate the LV wall thickness without manual selection of end-diastolic frames; and (3) DL automated measurements of IVS and PWT were less accurate with greater wall thickness.
Our DL model for automating LV dimensions from PLAX views compare favorably with the current state-of-the-art models. In practice, LV thickness is measured using an end-diastole frame that is identified manually by selecting the frame with the largest LV cavity. Previous DL models have required users to manually select end-diastolic frames to be inputted into the model, which limits the real-life applicability of automated LV wall dimension assessment. Previous DL models have been trained to select end-systolic and end-diastolic frames automatically, but have not been used to measure and report LV wall thickness [16,17,18,19,20,21,22]. The mean percentage error ranged between 5.40 and 13.93% for our model, which is well within the range of typical interobserver variability between expert clinicians, while eliminating intraobserver variability [9, 23, 24]. Our model contributes to the previous work in LV wall dimension measurements by making a truly autonomous model one step closer. Although our study selected PLAX videos specifically for assessment, our group has demonstrated that DL models can accurately classify 15 standard views in two-dimensional echocardiography, and that automated selection of PLAX video is feasible [25, 26].
Similar to previous work, our model was less accurate in estimating IVS and PWT when compared to LVID, especially in cases of greater wall thickness [13]. Several considerations are important. First, the measurements could have been overestimated by including the RV trabeculation, papillary muscles, or the sigmoid septum; however, our model generally underestimated the wall thickness as opposed to overestimation. It is possible that our model measured the septum at the tapered section, underestimating its true thickness. As well, the model had fewer images of markedly thickened walls to train on. One way of improving the accuracy of the model would be to include more images with very thick LV walls in the training set and to set a geographical limitation on the landmark detection to avoid the end of the septum where the tapering may occur.
This study was the first to incorporate prediction uncertainty in a DL model for assessing LV wall dimensions. Uncertainty quantification in artificial intelligence is important, as the model is able to convey to the users the level of confidence for its predictions and users can be apprised of any uncertainty of its predictions. However, there are no universally accepted parameters for the level of uncertainty in measurement of LV wall dimension by a DL model. Further studies are needed to demonstrate optimal uncertainty quantification for the measurement of LV dimensions.
This study adds to the growing body of research demonstrating the feasibility of DL models for complex echocardiographic assessments [27]. DL models can assess the quality of transthoracic echocardiograms, identify PLAX views from other standardized views, and automatically assess the LV wall from PLAX videos, but no one DL model has yet been developed that can comprehensively complete all theses tasks. Automation of LV wall dimension assessment from an undifferentiated set of echocardiographic videos would be of interest in future studies, as well as assessing the utility of DL models in the diagnosis and the management of various cardiomyopathies.
Study limitations
We acknowledge several limitations in our study. We used the manual measurements by trained sonographers as the ground truth label when developing our model, which are susceptible to human errors. Our model was trained from echocardiograms done at a single tertiary care center, limiting its generalizability. However, we included a large set of consecutive echocardiograms done in both inpatient and outpatient echocardiography labs at our tertiary care center that includes a diverse set of populations and pathologies. We only included echocardiographic studies of good quality for LV dimension and wall thickness. However, poor echocardiographic studies are unlikely to yield accurate LV wall dimensions, and our model’s prediction uncertainty would likely have discarded those studies. There is also uncertainty in how the model will perform with certain anatomic variations, such as basal septal hypertrophy or apical hypertrophy.
Conclusion
In this pilot study, we developed a novel DL model for automating the measurement of LV dimensions and wall thickness by 2D echocardiography. The model performed well for measurements of LVID and LV mass, and moderately for IVS and PWT. The accuracy appeared reduced with greater LV wall thickness.
Data availability
The data that support the findings of this study are available from the corresponding author (TT) upon reasonable request.
References
Kristen Av, Perz JB, Schonland SO et al (2007) Rapid Progression of Left Ventricular Wall Thickness predicts mortality in Cardiac Light-chain amyloidosis. J Heart Lung Transplantation 26:1313–1319. https://doi.org/10.1016/J.HEALUN.2007.09.014
Ghali JK, Liao Y, Cooper RS (1998) Influence of left ventricular geometric patterns on prognosis in patients with or without coronary artery disease. J Am Coll Cardiol 31:1635–1640. https://doi.org/10.1016/S0735-1097(98)00131-4
Olivotto I, Gistri R, Petrone P et al (2003) Maximum left ventricular thickness and risk of sudden death in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 41:315–321. https://doi.org/10.1016/S0735-1097(02)02713-4
Eguchi K, Ishikawa J, Hoshide S et al (2007) Differential impact of left ventricular mass and relative wall thickness on cardiovascular prognosis in diabetic and nondiabetic hypertensive subjects. Am Heart J 154. https://doi.org/10.1016/J.AHJ.2007.04.021. :79.e9-79.e15
Elliott PM, Gimeno Blanes JR, Mahon NG et al (2001) Relation between severity of left-ventricular hypertrophy and prognosis in patients with hypertrophic cardiomyopathy. Lancet 357:420–424. https://doi.org/10.1016/S0140-6736(00)04005-8
Nair P, Siu SC, Sloggett CE et al (2006) The assessment of technical and interpretative proficiency in echocardiography. J Am Soc Echocardiogr 19:924–931. https://doi.org/10.1016/J.ECHO.2006.01.015
Anderson DR, Blissett S, O’Sullivan P, Qasim A (2021) Differences in echocardiography interpretation techniques among trainees and expert readers. J Echocardiogr 19:222–231. https://doi.org/10.1007/S12574-021-00531-Y
Wiegers SE, Ryan T, Arrighi JA et al (2019) 2019 ACC/AHA/ASE Advanced Training Statement on Echocardiography (revision of the 2003 ACC/AHA clinical competence Statement on Echocardiography): a report of the ACC Competency Management Committee. J Am Coll Cardiol 74:377–402. https://doi.org/10.1016/J.JACC.2019.02.003
Foppa M, Duncan BB, Rohde LEP (2005) Echocardiography-based left ventricular mass estimation. How should we define hypertrophy? Cardiovasc Ultrasound 3:1–13. https://doi.org/10.1186/1476-7120-3-17/FIGURES/2
Davis A, Billick K, Horton K et al (2020) Artificial Intelligence and Echocardiography: a primer for Cardiac sonographers. J Am Soc Echocardiogr 33:1061. https://doi.org/10.1016/J.ECHO.2020.04.025
Abdar M, Pourpanah F, Hussain S et al (2021) A review of uncertainty quantification in deep learning: techniques, applications and challenges. Inform Fusion 76:243–297. https://doi.org/10.1016/j.inffus.2021.05.008
Sofka M, Milletari F, Jia J, Rothberg A (2017) Fully convolutional regression network for accurate detection of measurement points. Lecture Notes Comput Sci (Including Subser Lecture Notes Artif Intell Lecture Notes Bioinformatics) 10553 LNCS:258–266. https://doi.org/10.1007/978-3-319-67558-9_30/FIGURES/5
Gilbert A, Holden M, Eikvil L et al (2019) Automated left ventricle dimension measurement in 2D Cardiac Ultrasound via an Anatomically Meaningful CNN Approach. Lecture Notes Comput Sci (Including Subser Lecture Notes Artif Intell Lecture Notes Bioinformatics) 11798 LNCS:29–37. https://doi.org/10.1007/978-3-030-32875-7_4
Zhang J, Gajjala S, Agrawal P et al (2018) Fully automated echocardiogram interpretation in clinical practice: feasibility and diagnostic accuracy. Circulation 138:1623–1635. https://doi.org/10.1161/CIRCULATIONAHA.118.034338/FORMAT/EPUB
Lang RM, Badano LP, Victor MA et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28:1–39e14. https://doi.org/10.1016/j.echo.2014.10.003
Ghorbani A, Ouyang D, Abid A et al (2020) Deep learning interpretation of echocardiograms. Npj Digit Med 2020 3(1 3):1–10. https://doi.org/10.1038/s41746-019-0216-8
Salte IM, Østvik A, Smistad E et al (2021) Artificial Intelligence for Automatic Measurement of Left ventricular strain in Echocardiography. JACC Cardiovasc Imaging 14:1918–1928. https://doi.org/10.1016/J.JCMG.2021.04.018
Sirjani N, Moradi S, Oghli MG et al (2022) Automatic cardiac evaluations using a deep video object segmentation network. Insights Imaging 13. https://doi.org/10.1186/S13244-022-01212-9
Asch FM, Poilvert N, Abraham T et al (2019) Automated echocardiographic quantification of left ventricular ejection Fraction without volume measurements using a machine learning Algorithm Mimicking a Human Expert. Circ Cardiovasc Imaging 12. https://doi.org/10.1161/CIRCIMAGING.119.009303
Leclerc S, Smistad E, Pedrosa J et al (2019) Deep learning for Segmentation using an Open large-scale dataset in 2D Echocardiography. IEEE Trans Med Imaging 38:2198–2210. https://doi.org/10.1109/TMI.2019.2900516
Ouyang D, He B, Ghorbani A et al (2020) Video-based AI for beat-to-beat assessment of cardiac function. Nature 580:252–256. https://doi.org/10.1038/S41586-020-2145-8
Knackstedt C, Bekkers SCAM, Schummers G et al (2015) Fully automated Versus Standard Tracking of Left ventricular ejection fraction and longitudinal strain: the FAST-EFs Multicenter Study. J Am Coll Cardiol 66:1456–1466. https://doi.org/10.1016/J.JACC.2015.07.052
Selamet Tierney ES, Hollenbeck-Pringle D, Lee CK et al (2017) Reproducibility of left ventricular dimension Versus Area Versus volume measurements in Pediatric patients with dilated cardiomyopathy. https://doi.org/10.1161/CIRCIMAGING.116.006007. Circ Cardiovasc Imaging 10:
Lang RM, Addetia K, Miyoshi T et al (2021) Use of Machine Learning to improve echocardiographic image Interpretation Workflow: a disruptive paradigm change? J Am Soc Echocardiogr 34:443. https://doi.org/10.1016/J.ECHO.2020.11.017
van Woudenberg N, Liao Z, Abdi AH et al (2018) Quantitative echocardiography: real-time quality estimation and view classification implemented on a mobile android device. Lecture Notes Comput Sci (Including Subser Lecture Notes Artif Intell Lecture Notes Bioinformatics) 11042 LNCS:74–81. https://doi.org/10.1007/978-3-030-01045-4_9/FIGURES/6
Vaseli H, Liao Z, Abdi AH et al (2019) Designing lightweight deep learning models for echocardiography view classification. 10951:93–99. https://doi.org/10.1117/122512913
Abdi AH, Luong C, Tsang T et al (2017) Automatic Quality Assessment of echocardiograms using Convolutional neural networks: feasibility on the apical four-Chamber View. IEEE Trans Med Imaging 36:1221–1230. https://doi.org/10.1109/TMI.2017.2690836
Acknowledgements
We thank the Vancouver General Hospital and University of British Columbia Echo Lab and Artificial Intelligence Echo Core Lab staff for their significant contributions to this study.
Funding
This work is funded in part by the Canadian Institutes of Health Research (CIHR) and in part by the Natural Sciences and Engineering Research Council of Canada (NSERC).
Author information
Authors and Affiliations
Contributions
Conceptualization, study design, supervision, project administration, funding acquisition - T.T. and P.A. Data collection, data curation, investigation, writing - original draft, writing - review & editing, visualization, project administration - J.Y. Machine learning model development, software development, validation, formal analysis - H.V. and M.M. Writing - review & editing, supervision - C.L., M.T., D.Y., M.B., P.N., J.J., K.G.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yim, J., Mahdavi, M., Vaseli, H. et al. Assessment of left ventricular wall thickness and dimension: accuracy of a deep learning model with prediction uncertainty. Int J Cardiovasc Imaging (2024). https://doi.org/10.1007/s10554-024-03207-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10554-024-03207-7