
Abstract
Racial discrimination is a documented risk factor for sexual risk behaviors among young Black men. Mechanisms of effect and protective processes remain to be investigated. This study examined the mediating effect of emotional distress, self-regulation, and substance use on the association between racial discrimination and sexual risk behaviors. Sexual risk behaviors included in this study were inconsistent condom use and sexual concurrency (sexual partnerships that overlap overtime). The protective effect of protective social ties was also investigated. A sample of 505 heterosexually active men aged 19–22 years were recruited and surveyed for 3 time points. Men answered questions on racial discrimination, sexual risk behaviors, emotional distress, self-regulation, and substance use. Mediation and moderation models were tested. Racial discrimination (T1) significantly and positively predicted emotional distress (T2). Emotional distress, substance use, and self-regulation partially mediated the association between racial discrimination and sexual risk behaviors. Protective social ties attenuated the effects of emotional distress on substance use and self-regulation. Racial discrimination is an important context for sexual risk behaviors. Minority stress may translate to sexual risk behavior through psychosocial mediators, such as emotional distress, self-regulation, and substance use. Protective social ties may buffer against emotional distress to reduce substance use and increase self-regulation. The findings of this study can provide new insights through the investigation of risk and protective processes that influence sexual risk behaviors among young Black men.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Once confined mainly to urban centers, HIV infection has become increasingly prevalent in small towns and rural communities, particularly among Blacks in the southern U.S. (Fleming, Lansky, Lee, & Nakashima, 2006; Hall, Li, & McKenna, 2005; Kann et al., 2016). The South accounts for more than one-third of all AIDS cases in the U.S., and infection among residents of rural areas is more likely to occur in the South than in other areas of the country (Kann et al., 2016). In 2016, 44% of new HIV diagnoses were among African-Americans living in the rural south (CDC, 2017). The majority of research on the behavioral factors associated with HIV-related behaviors in the rural South has focused on Black women, intravenous drug users, or Black men who have sex with men (Cohen et al., 2011; Hladik & McElrath, 2008; Sharp & Hahn, 2011). Recent research, however, suggests that heterosexual Black men, aged 20–25, also experience elevated risk. Black men comprise 15% of new HIV infections through heterosexual contact transmission in the U.S. (CDC, 2017). Moreover, approximately 24% of new HIV diagnoses among the total population of the U.S. were contracted through heterosexual contact compared with 3% in 1983 (Kann et al., 2016).
Transmission of HIV among heterosexual Black men is related to preventable risk behaviors including inconsistent use of contraceptives and sex with concurrent partners, particularly when partnerships overlap in time. When condoms are not used consistently and young men engage in sexual concurrency (sexual relationships that overlap across time), sexual pathogens can spread rapidly throughout the community; this is especially true when communities have high rates of sexually transmitted pathogens (Hallfors, Iritani, Miller, & Bauer, 2007). This is particularly true in rural communities, characterized by densely interconnected social networks and a restricted dating pool (Adimora, Schoenbach, & Doherty, 2007).
Racial discrimination is a pervasive stressor affecting the health risk behavior of African-American men (Ayala, Bingham, Kim, Wheeler, & Millett, 2012; Williams & Mohammed, 2009). Racial discrimination often refers to unfair treatment received because of one’s race by individuals from a dominant group in society (Williams & Mohammed, 2009). Racial discrimination may be overt and involve institutional practices such as denying service or creating barriers to employment (Williams & Mohammed, 2009). “Racial microstressors” refer to everyday experiences with racism that include being ignored, overlooked, or mistreated in ways that lead to feelings of demoralization and dehumanization (Sue et al., 2007). These experiences are often minimized and not considered serious enough to address, but their accumulation has significant consequences for mental and physical health. In fact, some research suggests that the accumulation of microstressors may have a greater impact on mental health than more overt and structural experiences of discriminatory behavior (Sue et al., 2008). Although the negative effects of everyday discrimination on Black men’s sexual health are increasingly well documented, few prospective studies have investigated the proximal, psychosocial mechanisms linking discrimination to risky sexual behavior (Bowleg et al., 2014; Roberts et al., 2012).
This study is informed by perspectives on minority stress and social ecological theory. Social ecological theory examines individual behaviors in the aspects of multiple levels of contextual influence. Ecological influences include intrapersonal (e.g., knowledge, attitudes, behavior) factors, interpersonal/network factors (social networks, social support), community level factors (e.g., relationships among organizations/institutions), and larger social and cultural contexts (e.g., local, state, national laws). The present study focuses on the social ecological model of health promotion (McLeroy, Bibeau, Steckler, & Glanz, 1988). Social ecological models of health promotion have been used to explain the complex associations between social (e.g., social networks) and individual behavior, as well as the physical environment’s influences on health risk behavior (McLeroy et al., 1988; Poundstone, Strathdee, & Celentano, 2004). Ecological perspectives focus attention on documenting how multiple contextual levels affect behavior and development (McLeroy et al., 1988). The present study examines risk factors with the intrapersonal, interpersonal, and community context. Additionally, we are examining the interpersonal protective effect of protective social ties on individual sexual risk behavior. Guided by minority stress theory, we examine racial discrimination as a minority stressor impacting sexual risk behaviors (Meyer, 2003). Minority stress theory is often used to explain why minority stress is important for an understanding of health risk behaviors, such inconsistent condom use. This theory posits a social causation hypothesis, stating that social conditions do not lead directly to poor health among minorities. Rather, severe social conditions cause stress that accrues over time for minority individuals, resulting in long-term health disparities.
Social ecological theory complements minority stress theory by providing a way to model these risk factors through indirect pathways and protective processes. The protective processes investigated in this study include positive relationships with parents, intimate partners, peers, and mentors. Considering the intersection of minority stress and social–ecological theories, the protection from protective social ties that contextual risk factors induce is expected to result in prosocial attitudes which lead to decreased sexual risk behavior. The influence of risk factors will vary, however, depending on a young person’s attachment to protective social ties, those of which can be found in relationships with family, intimate partners, peers, and mentors.
Given this theoretical foundation, we hypothesized that men’s exposure to racial discrimination represents a stressful circumstance that signals to young men that their environment is hostile or isolating. Such environments are suggested to induce emotional distress, including symptoms of anger and depression (Liao, Kashubeck-West, Weng, & Deitz, 2015). Research suggests that emotional distress may be linked to sexual risk behaviors via two proximal factors, substance use and lack of self-regulation (DiClemente et al., 2001; Ethier et al., 2006; Kogan et al., 2010; Johnson, Cunningham-Williams, & Cottler, 2003; Tice, Bratslavsky, & Baumeister, 2018). Substance use is a proximal predictor of risky sexual behavior as young people demonstrate impaired judgement and reduced inhibitions while intoxicated. Emotional distress is a forceful antecedent of substance use and over use, providing a means to cope with negative affect (Shrier, Harris, Sternberg & Beardslee, 2001). Additionally, under stressful conditions, self-regulation can be undermined by negative emotions and individuals can lose control of their impulses (Johnson et al., 2003; Tice et al., 2018). Research that focuses specifically on young Black men, emotional distress, and self-regulation is rare; however, a study of multiethnic college students found that emotional distress undermined self-regulation and engendered a shift toward preferring immediate gratification (Tice, Bratslavsky, & Baumeister, 2001). Johnson et al. found that having difficulties in regulating emotional states, planning and controlling behavior in accordance with social norms, and coping adaptively with contextual stress is linked with sexual risk behavior among Black women. Black women who reported higher levels of depression also reported higher levels of sexual risk behaviors. The influence of self-regulation as a mediator of rural Black men’s sexual behavior is unknown. Therefore, we predict that emotional distress, a consequence of minority stress, will be linked to sexual risk behaviors via two mechanisms: increased substance use and decreases in self-regulation.
Despite exposure to racial discrimination, many young men will avoid engaging in HIV-related behavior. The factors that ameliorate the influence of discrimination on HIV-related behaviors are a critical target for investigation as they provide foci for preventive interventions. Little prospective research, however, has investigated protective processes for sexual risk behavior among Black men. Extant studies emphasize the role of protective social ties (close supportive relationships with family, peers, intimate partners, or mentors) in reducing risky behavior during the transition to adulthood (Kogan, Brody, & Chen, 2011a; Simons et al., 2006). Protective social ties encourage conventional behavior and reduce the influence of risk-taking peers (Umberson, Crosnoe, & Reczek, 2010). For example, men at risk of antisocial or other risky behavior who develop close romantic relationships with a prosocial partner experience a diminution in antisocial (Sampson, Raudenbush, & Earls, 2009) behavior and substance use (Cho & Kogan, 2016).
Research suggests that Blacks may depend on informal sources of social support, such family and peers, because financial and other social barriers often limit access to other types of resources (Mossakowski & Zhang, 2014.) Research has also shown that young people who evince close ties with family members and other adults in the community, romantic partners, and conventional peers are protected against substance misuse (Viner et al., 2012). Viner et al. found that social support from family, peers, and community members protects young people from sexual risk behaviors, teen pregnancy, and substance misuse. However, this study did not specifically focus on Black men. Brody, Yu, Chen, and Kogan (2012) found that among Black emerging adults, having protective parenting processes buffered young adults from engaging in substances. For young men experiencing contextual risk factors, a supportive network of social ties provides an outlet for coping with challenging emotions (Murry & Brody, 2004; Wills & Ainette, 2010). Stress models explain how social support protects mental health through moderation (Mossakowski & Zhang, 2014). Social support can be used to counteract the harmful effect of a stressor on mental health (Mossakowski & Zhang, 2014). Therefore, we predicted protective social ties would moderate the path between contextual risk and emotional distress.
We also predicted that protective social ties would moderate the relationship between emotional distress and substance use and self-regulation. For young men who are embedded in systems of conventional relationships, prosocial individuals reinforce and model appropriate or desired behaviors (Kogan, Wejnert, Chen, Brody, & Slater, 2011b). Thus, men with close, conventional social ties are likely to interact with significant others who discourage risk behavior (Murry, Heflinger, Suiter, & Brody, 2011). For young men experiencing the frustration of discriminatory treatment, a supportive network of social ties also may provide alternatives to substance use as a means of coping with emotional distress. In seeking relief from the discrimination-induced emotional distress, men can cope by seeking support rather than engaging in substance use or sexual risk behaviors. Studies also suggest that Black youth are strongly influenced by their families and peers regarding substance use behaviors. Conventional ties promote prosocial norms and attitudes and limit affiliations with risk-taking peers (Kogan et al., 2011a; Simons, Chao, Conger, & Elder, 2001; Simons-Morton, Chen, Abroms, & Haynie, 2004). Men with close, conventional ties are more likely to interact with others who discourage substance use. Therefore, strong relationships with family, peers, intimate partners, and prosocial adults in the community can buffer the effects of emotional distress and reduce substance use.
Strong relationships with conventional ties also foster the development of self-regulation (Murry & Brody, 2004; Wills & Ainette, 2010). Research has shown that as a response to emotional distress, Blacks strengthen social bonds which increases self-regulation (Mays, Cochran, & Barnes, 2007). Having supportive relationships with family, peers, intimate partners, and mentors make it easier for individuals to develop good self-regulatory processes (Cox & Paley, 1997). One-way supportive relationships develop self-regulation is through communication about problems. To cope with negative emotions, young men may communicate with their families, peers, and mentors who will recognize their feelings. This prevents emotional distress from undermining self-regulation.
Research that focuses specifically on Black young men is rare. Much of the research on self-regulation has also focused on the patterns of interactions within and across family subsystems (marital and parent–child, parent–child and sibling). Less research has focused on the impact of the interaction of multiple subsystems such as families, peers, intimate partners, and mentors together. Therefore, we predicted that protective social ties would moderate the association between emotional distress and self-regulation.
Recent data emphasize that among socioeconomically disadvantaged young men, the accumulation of multiple protective processes is critical for navigating high-risk environments (Beaver, Mancini, DeLisi, & Vaughn, 2011; Flouri, Tzavidis, & Kallis, 2010). Men with a wide array of protective social ties in multiple areas of their lives (peers, parents, mentors, etc.) are most likely to exhibit resilient outcomes. These studies suggest that rather than a specific relationship having significance, it is the number of protective relationships in a man’s life that is protective (Andershed, Gibson, & Andershed, 2016). Andershed et al. examined violent offending among young males and reported it is the cumulative effect that is more protective in reducing risk behaviors compared with any individual protective factors. We thus examined the accumulation of protective social ties in our analyses.
Summary and Hypotheses
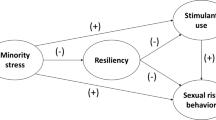
The present study investigated the proximal risk and protective mechanisms that link racial discrimination to risky sexual activity (unprotected intercourse and concurrent sexual partners) among young adult rural Black men. Figure 1 presents a summary of hypotheses regarding risk mechanisms. We predicted that exposure to racial discrimination would increase men’s involvement in risky sex by inducing emotional distress, which in turn encourages substance use and undermines self-regulation. Additionally, we investigated the protective effect of protective social ties with parents, informal mentor figures, romantic partners, and peers. We hypothesized that for men with greater numbers of protective social ties rather than fewer, the influence of racial discrimination on risky sexual behavior, and the hypothesized mediating mechanisms would be attenuated.

Summary of hypotheses
Method
Participants
Hypotheses were tested using data from the African-American Men’s Health Project, a longitudinal study of 505 Black men ages 19–22 at baseline from 11 counties in rural Georgia (Hicks, Kogan, Cho, & Oshri, 2017; Kogan, Allen, Gonzalez-Backen, Bae, & Cho, 2018; Kogan, Cho, Brody, & Beach, 2017; Oshri, Kogan, Liu, Sweet, & Mackillop, 2017). Participants were recruited using respondent-driven sampling, which combines a prescribed chain referral recruitment method with a mathematical model that allows for post-stratification sample weighting. Community liaisons recruited 45 initial “seed” participants from targeted counties to complete a baseline survey. Each participant was then asked to identify three other eligible Black men in their community from their personal network. Project staff contacted the referred participants, and the referring participant received $25 per person who completed the survey. After completing the survey, each referred participant, in turn, was asked to refer three men in his network. The RDS protocols and weighting system are designed to attenuate the influence of biases common in chain referral samples and to better approximate a random sample of the target population (Heckathorn, 1997, 2002) biases observed in chain referral samples including the characteristics of the initial seed participants, the recruitment efficacy of individual participants, and participants differing network sizes. Analyses of network data related to substance use and other risky behavior at T1 (Kogan et al., 2016a) indicated that the sample evinced negligible levels of common (Kogan, Cho, & Oshri, 2016b) biases observed in chain referral samples including the characteristics of the initial seed participants, the recruitment efficacy of individual participants, and participants differing network sizes.
African-American research staff visited participants at their home or a convenient community location and participants completed an audio computer-assisted self-interview on a laptop computer. This allowed participants to navigate the survey privately with the help of voice and video enhancements; literacy concerns were attenuated. Participants received $100 for completing the survey at each time point. Participants provided written informed consent at baseline; all study protocols were approved by the University Human Subjects Review Board.
Of the 505 men who participated at T1, 423 (83.8%) completed the T2 survey and 406 (75.2%) completed the T3 survey. In preliminary analysis (table not included here), the potential influence of attrition was investigated with a one-way ANOVA. Retention status was not associated with any study variables. Approximately 18.30 (SD = 4.19) months after the baseline survey (Time 1, T1), when men’s mean age was 21.85 years (SD = 1.27), a follow-up data collection visit (Time 2; T2) was conducted. A third visit (T3) occurred 19.68 months later when men’s mean age was 23.49 years (SD = 1.21).
Measures
Sexual Concurrency and Inconsistent Condom Use
Concurrent sexual partnerships were assessed at Time 1 and Time 3 with the question, “In the past year have you had sex with one woman, while being in a sexual relationship with another woman?” Men also reported how many times in the past 3 months they had vaginal sex. Men who reported more than zero times were asked a follow-up question, “Of those times you had vaginal sex in the past 3 months, how many times did you use a condom?” Responses ranged from 1 (never) to 6 (every time). This variable was dichotomized into 1 (inconsistent condom use) and 0 (consistent condom use). Participants who answered, “every time” were in the consistent condom use group.
Racial Discrimination
Men reported their perceptions of racial discrimination at T1 using a 9-item measure adapted from Williams’s research on everyday events of racial discrimination (Brody, Kogan, & Chen, 2012; Williams & Williams-Morris, 2000). Focus groups of community members identified most frequent events of racial discrimination and suggested wording changes to increase clarity of the measure (Murry & Brody, 2004). Participants reported the frequency during the past 6 months with which each of nine stressors occurred, ranging from 0 (never) to 3 (frequently). Example items included “Have you been ignored, overlooked, or not given service because of your race?” and “Have you been treated rudely or disrespectfully because of your race?” Cronbach’s α was .84.
Emotional Distress
Emotional Distress was assessed with two scales completed at T1 and T2. Men self-reported their anger/hostility on an eight-item subscale of the Client Evaluation of Self and Treatment (Joe, Broome, Rowan-Szal, & Simpson, 2002). Example items included “You feel a lot of anger inside of you” and “You have urges to fight or hurt others.” Responses ranged from 1 (strongly disagree) to 4 (strongly agree). Cronbach’s alpha was .88 at Time 1 and .91 at Time 2. Depressive symptoms were assessed using a 12-item short form of the Center for Epidemiologic Studies Depression Scale, a self-report measure of symptoms occurring during the previous week (CES-D; Carpenter et al., 1998; Radloff, 1977). The response set ranged from 0 (rarely or none of the time, less than 1 day) to 3 (most of the time, 6–7 days). The alpha for this measure was .73 at T1 and .78 at T2. Consistent with past research on negative emotionality (Martin, Neighbors, & Griffith, 2013; Troisi & D’Argenio, 2004), the measures were significantly correlated (r = .24 at T1 and .29 at T2); anger/hostility and depressive symptoms were standardized and summed at each wave to form an emotional distress index.
Self-Regulation
Self-regulation was assessed using a 10-item version of Self-Regulation Questionnaire (Brown, Miller, & Lawendowski, 1999). Items for the short version were selected for the AMP study based on factor analysis of questionnaire in a previous study (Kogan & Brody, 2010). Questions included “I set goals for myself and keep track of my progress,” “If I wanted to change, I am confident that I could do it,” and “If I make a resolution to change something, I pay a lot of attention to how I am doing.” Cronbach’s alpha was .89 for Time 1 and .95 at Time 2.
Substance Use
At Time 1 and Time 2, young men reported the number of times during the previous month that they drank alcohol, had 4 or more drinks of alcohol at one time, or smoked marijuana. Responses to these three items were standardized and summed to form a previous-month substance use index ranging from 0 to 81. Items were significantly intercorrelated; all ps < .01. This index has been used previous research with African-American youth and young adults (Brody & Ge, 2001; Brody et al., 2012).
Protective Social Ties
At T1, men self-reported their affiliations with prosocial versus antisocial peers; involvement in close, supportive relationships with romantic partners; and involvement in close, supportive relationships with a primary parenting figure.
Peer Affiliations
Peer affiliations were assessed using an 11-item scale that Elliott and Menard (1996) developed. Example items considering a 3-month time frame included “How many of your friends used tobacco regularly?” and “How many of your friends damaged or destroyed something that does not belong to them?” Participants’ responses ranged from 0 (none of them) to 3 (all of them). This scale was reverse coded to reflect affiliations with prosocial peers. Cronbach’s alpha was .89.
Relationships with a Romantic Partner
For men who reported that they had a “a woman or girl that you have a very special or committed romantic or sexual relationship with, such as a girlfriend or a spouse,” support from that partner was assessed using the four-item support scale from the Network of Relationship Inventory (NRI; Furman & Buhrmester, 1985). Example items included “How often do you turn to her for support with personal problems?” and “How often do you depend on her to cheer you up when you are feel down or upset?” Responses ranged from 0 (never) to 3 (very often). Cronbach’s alpha was .80.
Relationship with Parent
Support from a primary parent figure was assessed with a 6-item subscale from the NRI (Furman & Buhrmester, 1985). Example items included “How often do you depend on this parent for help, advice, or sympathy?” and “How often do you turn to this parent for support with personal problems?” Responses ranged from 0 (never) to 3 (very often). Cronbach’s alpha was .94. For each relationship measure (peers, romantic partners, parents), scores above the mean of the distribution were assigned a “1” and those below the mean were assigned a “0.” Scores were summed to form a protective social ties index that ranged from 0 to 3.
Control Variables
Past research has documented associations between racial discrimination, sexual risk behaviors and age, economic status and problems, and community disadvantage (Bowleg et al., 2014; Hudson, Puterman, Bibbins-Domingo, Matthews, & Adler, 2013). Therefore, to account for plausible rival explanations, all analyses controlled for T1 baseline outcomes (inconsistent condom use and sexual concurrency), age, education and/or employment status, economic distress, and community disadvantage.
During emerging adulthood, employment status and school status are particularly transitory and difficult to interpret. Thus, scholars studying emerging adults suggest that the most important demographic characterization for young men involves simultaneous consideration of employment and student status (Wald & Martinez, 2003). The goal is to differentiate young people who are employed or going to school from those involved in neither. In this study, participants who were currently enrolled in school or another educational program or who were employed were coded as “1” and participants who were not enrolled or employed were coded as “0.”
Economic distress was assessed with five items selected from the Adequate Necessities subscale of the Family Resources Scale (Dunst & Leet, 1987). Participants responded to items rated on a scale ranging from 1 (strongly disagree) to 4 (strongly agree) to indicate how well their resources met their needs. This scale has been used previously with African-American adults (Kogan, Brody, Crawley, Logan, & Murry, 2007). Cronbach’s alpha was .79 at Time 1.
Community social disorder was assessed at T1 with the nine-item Community Social Disorder Scale (Sampson et al., 2009). This scale assesses the frequency of community crime (i.e., Robbery, people selling drugs) and the extensiveness of community dilapidation (i.e., litter, graffiti, and vacant houses). This scale has been used previously with samples of rural Black men (Kogan et al., 2010, 2016a). Responses ranged from 1 (not a problem or never) to 3 (a big problem or often). Example items included “How big of a problem is vacant or deserted houses in the neighborhood in which you live?” and “How often has a fight in the neighborhood in which a weapon was used happened in the neighborhood in which you live?” Cronbach’s alpha was .90.
Analysis
Hypotheses were tested using structural equation modeling with MPlus 7 (Muthén & Muthén, 2010). Indirect effects were estimated for the mediation model using 95% bias-corrected confidence intervals obtained from bootstrapping (Preacher, Rucker, & Hayes, 2007). For the protective processes factor, we created two-way interaction terms (e.g., racial discrimination × protective social ties; emotional distress × protective social ties). To produce a common scale, standardized regression weights were used in which all study variables were standardized (a mean of 0 and a SD of 1) before the interaction terms were calculated. Per Bollen’s (1989) recommendations, we assessed goodness of fit with the root mean square error of approximation (RMSEA; Browne & Cudeck, 1992), comparative fit index (CFI; Bentler, 1990), and chi-square divided by its degrees of freedom.
In each analysis, baseline outcome variables (condom use, sexual concurrency) and mediator (emotional distress, substance use, and self-regulation) variables were controlled. As past research links discrimination and risky sexual behavior with age, economic status and problems, and community disadvantage, we controlled for T1 education/employment status, age, community social disorder, and economic distress in all models.
Results
Description of the Sample
On average, the men were 20 years old at baseline and most (74%) had completed high school or obtained a GED. Their average total monthly income was $693.79. Of those young men who were sexually active, on average, they had sex with three different women close in age to themselves within the past 3 months at Time 1 and Time 3. Additionally, 58.1% of sexually active young men reported inconsistent condom use at Time 1 and 66.5% at Time 3.
Correlation Analysis
Zero-order correlations are presented in Table 1. Significant associations emerged to support study predictions. Racial discrimination was significantly associated with emotional distress (r = .27, p < .01, df = 404). Emotional distress was significantly correlated with self-regulation (r = −.23, p < .01, df = 404) and substance use (r = .11, p < .05, df = 404). Substance use at T2 was significantly correlated with inconsistent condom use at T3 (r = .12, p < .05, df = 404) and sexual concurrency at T3 (r = .12, p < .05, df = 404). Self-regulation at T2 was significantly correlated with sexual concurrency at T3 (r = −.13, p < .05, df = 404); however, it was not significantly associated with inconsistent condom use at T3 (r = −.03, df = 404).
Indirect Effects Model
Figure 2 shows the test of the indirect effects model. The model fit the data as follows: CFI = .95; TLI = .94; RMSEA = .03; χ2 (13, N = 406) = 15.5, p = . 28. Racial discrimination at T1 had a significant positive effect on T2 emotional distress (β = .12, p < .01). T2 emotional distress had a significant positive effect on substance use (β = .20, p < .01) and a significant negative effect on self-regulation (β = −.18, p < .01). No direct effect between emotional distress and either inconsistent condom use or sexual concurrency was detected. T2 substance use predicted inconsistent condom use (β = .13, p < .05) and sexual concurrency (β = .15, p < .05). Self-regulation had a significant negative effect on inconsistent condom use (β = −.11, p < .05) and no effect on sexual concurrency.

Mediation model
The significance of indirect effects is reported in Table 2. There was a significant indirect effect from emotional distress to sexual concurrency, via substance use (β = .03, p < .05). Emotional distress indirectly predicted inconsistent condom use, via effects on substance use (β = .03, p < .05). A significant indirect effect was detected from racial discrimination to inconsistent condom use, via emotional distress and substance use (β = .02, p < . 05). Finally, there was a significant indirect effect from racial discrimination to sexual concurrency, via emotional distress and substance use (β = .02, p < .05).
Figure 3 shows the interactive effects of racial discrimination and protective social ties on emotional distress, self-regulation, and substance use. The model fit indices are as follows: CFI = .93; TLI = . 85; RMSEA = .04; χ2(17, N = 406) = 22.96, p = .18. The interaction term representing protective social ties x racial discrimination was not significantly associated with emotional distress. The protective social ties x emotional distress interaction term was significantly associated with substance use (β = .23, p < .01) and self-regulation (β = .15, p < .01). Figure 3 shows a graph of the interaction predicting substance use; a crossover interaction is in evidence. For those with more protective social ties, as emotional distress increases, substance use decreases. For those with few protective social ties, as emotional distress increased substance use decreased (Fig. 4). In contrast, for those with fewer protective social ties substance use increased with emotional distress. Figure 5 shows the graph for the interaction predicting self-regulation. In the context of many protective social ties, emotional distress had not influence on self-regulation. In contrast, for men with few social ties, emotional distress was associated with decreasing self-regulation.

Moderation model

Interactions of protective social ties and emotional distress on substance use

Interaction of protective social ties and emotional distress on self-regulation
Discussion
Rural African-American men experience elevated risk of HIV, and their risky sexual behavior can affect the spread of HIV via non HIV STIs. We predicted that racial discrimination would be associated with increases in emotional distress, which in turn would be associated with substance use and self-regulation, proximal predictors of inconsistent condom use, and multiple sexual partners. Studies reveal that racial discrimination forecasts risky sexual behavior among Black youth; however, the mechanisms through which discrimination influences behavior are unclear (Bowleg et al., 2014; Roberts et al., 2012). We further hypothesized that protective social ties would moderate the effect of racial discrimination on emotional distress, and protective social ties would moderate the effect of emotional distress on substance use and self-regulation. Results provide partial support for study predictions. We found that racial discrimination predicted emotional distress which affected increases in substance use and reduced levels of self-regulation; these were proximal predictors of concurrent sexual behavior and inconsistent condom use. Emotional distress, substance use, and self-regulation also partially mediated the influence of racial discrimination on inconsistent condom use and sexual concurrency. Finally, protective social ties moderated the association between emotional distress and substance use and the association between emotional distress and self-regulation.
Consistent with minority stress theory, our findings indicate that racial discrimination affects health risk behavior by inducing negative emotionality (Hayes, Chun-Kennedy, & Edens Locke, 2011). Our longitudinal design allowed us to investigate the influence of discrimination on changes in negative emotionality over an 18-month time period separating Waves 1 and 2. Effects were in evidence even with economic distress and community social disorder controlled, supporting the importance of the effect. This time period also coincides with the transition to the labor force; many young Black men may experience heightened exposure to discrimination as they seek jobs. Poor preparation for work and scarce opportunities likely combine with discriminatory practices, providing a uniquely demoralizing environment for many young men.
Consistent with our hypotheses, the emotional distress induced by discrimination affected substance use and self-regulation. These findings are consistent with recent research on young Black men’s escalation of substance use during this time period. Although rates are generally low in adolescence, as Black men experience increases in adult stressors in general, and racial discrimination in particular, substance use may become a more prevalent as a means of coping with frustration. We also replicated previously established links between emotional distress and self-regulation (Eisenberg et al., 2009; Smith & Cyders, 2016). Indirect effect analyses confirmed the role of substance use and emotional distress as mediating factors linking discrimination to risky sexual behavior. This suggests that the emotional distress induced by racial discrimination increases risk of substance use, a proximal factor in risky sexual behavior.
In contrast, indirect effects were not in evidence with self-regulation. Gibbons et al. (2012) found with a sample of Black adolescents, ages 10–18, that self-control mediated the influence of discrimination on substance use. Our findings with an older and exclusively male sample suggest that similar effects may not be relevant for men’s sexual behavior. Self-regulation yielded only modest predictions of condom use and was not a significant predictor of concurrency. It may be the case that while self-regulation is affected by emotional distress, risky sexual behaviors may not be a function of impulsive behavior. Rather concurrency and to a limited extend condom use may be intentional choices.
Consistent with social ecological theory of health promotion, protective social ties attenuated the effects of emotional distress on substance use and self-regulation (McLeroy et al., 1988). This is consistent with previous research that shows that protective social ties attenuate the influence of stressors on Black men’s substance use (Cho & Kogan, 2016). Studies of Black adolescents show that they are strongly influenced by their families and peers. (Schwinn & Schinke, 2014). For example, Schwinn and Schinke investigated Black and Latino youth and found that prosocial peers and family members reduced substance use and risk behaviors. For young men who are embedded in systems of supportive, conventional relationships, prosocial individuals reinforce and model appropriate behavior (Cho & Kogan, 2016; Schwinn & Schinke, 2014). Thus, men with protective social ties are more likely to interact with other who either discourage substance use or simply will not tolerate it.
Lastly, protective social ties buffered the effects of emotional distress on self-regulation. Past research has shown that parents, family, and friends socialize youth and provide them with invaluable relational support to promote healthy development (Anderson, Donlan, McDermott, & Zaff, 2015). Specifically, supportive relationships can lead to subsequent positive affect, self-regulation, and self-confidence (Anderson et al., 2015). Research also demonstrates that supportive relationships may provide young men with more adaptive coping strategies, such as accessing resources to solve immediate needs, particularly for young men with low self-regulation (Hamama & Ronen-Shenhav, 2013). Understanding the role of self-regulation and protective social ties for emotional stress and sexual risk behaviors, particularly among young Black men, may aid in prevention and intervention efforts.
These results have implications for prevention and intervention efforts. When tailoring programs for heterosexual young Black men, it is important to include content addressing racial discrimination and the emotions induced by unfair treatment. Interventions efforts could provide training for young Black men getting ready to enter the workplace. Job training that includes how to respond to racial discrimination in the workplace may be effective in increasing opportunities for young Black men during this crucial developmental time period in their lives. Racial discrimination reduction programs tailored for companies hiring young Black men may also be effective by making companies aware of the macroaggressions that exist in today’s society and how those macroaggressions and other forms of racial discrimination decrease opportunities for young Black men.
Study results suggest the importance of pairing substance use prevention and sexual risk prevention efforts. Documentation of protective social ties’ moderating influences suggests the importance of supporting prosocial relationships with parents, mentors, peers, and partners (Kogan et al., 2011a; Simons et al., 2006). Other research indicates that parents continue to exert protective influences on young adult children, and community mentors can assist young men in dealing with a challenging time without using substances to cope. Whereas antisocial peers and partners play an exacerbating role in risk behavior during this time period, the reverse also is true. Connecting young men to opportunities to affiliate with prosocial peers and to develop closer supportive relationships with romantic partners can have salubrious effects on health behavior.
Limitations
There are a few limitations that need to be acknowledged. Study findings focused on rural Black men during the years immediately following high school. Results may not generalize to men from other contexts (rural vs. urban neighborhoods, different age groups) or of other racial/ethnic backgrounds (Black/African-American vs. White, Hispanic, Caribbean, African). This study relies on self-report measures increasing the potential for social desirability bias and Type I errors. However, participants completed surveys on their own. This provides opportunities for participants to be more truthful with their answers without pressure of having an interviewer to respond to. The survey was also completed anonymously. Anonymity was communicated to the participants before beginning the survey; therefore, they were aware before answering questions that there was no identifiable information. Furthermore, the use of three waves of data controlling for baseline levels of the dependent variables as well as controlling for common confounds such as economic distress and community disorder increases confidence in study findings.
Conclusions
Overall, the present study underscores the pernicious influence of racial discrimination and pathways linking discrimination to sexual risk behavior via emotional distress and substance use. Additionally, this study identified protective social ties as a buffer of the negative consequences of discrimination on emotional distress, substance use, and self-regulation. Protective social ties may be an effective target for prevention and intervention efforts that focus on reducing the stress of racial discrimination on health outcomes.
References
Adimora, A. A., Schoenbach, V. J., & Doherty, I. A. (2007). Concurrent sexual partnerships among men in the United States. American Journal of Public Health, 97(12), 2230–2237.
Andershed, A. K., Gibson, C. L., & Andershed, H. (2016). The role of cumulative risk and protection for violent offending. Journal of Criminal Justice, 45(Suppl. C), 78–84. https://doi.org/10.1016/j.jcrimjus.2016.02.006.
Anderson, S., Donlan, A. E., McDermott, E. R., & Zaff, J. F. (2015). Ecology matters: Neighborhood differences in the protective role of self-control and social support for adolescent antisocial behavior. American Journal of Orthopsychiatry, 85(6), 536.
Ayala, G., Bingham, T., Kim, J., Wheeler, D. P., & Millett, G. A. (2012). Modeling the impact of social discrimination and financial hardship on the sexual risk of HIV among Latino and Black men who have sex with men. American Journal of Public Health, 102(S2), S242–S249.
Beaver, K. M., Mancini, C., DeLisi, M., & Vaughn, M. G. (2011). Resiliency to victimization: The role of genetic factors. Journal of Interpersonal Violence, 26(5), 874–898.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238.
Bollen, K. A. (1989). A new incremental fit index for general structural equation models. Sociological Methods & Research, 17(3), 303–316.
Bowleg, L., Fitz, C. C., Burkholder, G. J., Massie, J. S., Wahome, R., Teti, M., … Tschann, J. M. (2014). Racial discrimination and posttraumatic stress symptoms as pathways to sexual HIV risk behaviors among urban Black heterosexual men. AIDS Care, 26(8), 1050–1057.
Brody, G. H., & Ge, X. (2001). Linking parenting processes and self-regulation to psychological functioning and alcohol use during early adolescence. Journal of Family Psychology, 15(1), 82–94.
Brody, G. H., Kogan, S. M., & Chen, Y.-F. (2012). Perceived discrimination and longitudinal increases in adolescent substance use: Gender differences and mediational pathways. American Journal of Public Health, 102(5), 1006–1011. https://doi.org/10.2105/ajph.2011.300588.
Brown, J. M., Miller, W. R., & Lawendowski, L. A. (1999). The self-regulation questionnaire. In L. VandeCreek & T. L. Jackson (Eds.), Innovations in clinical practice: A sourcebook (Vol. 17, pp. 281–292). Sarasota, FL: Professional Resource Press/Professional Resource Exchange.
Browne, M. W., & Cudeck, R. (1992). Alternative ways of assessing model fit. Sociological Methods and Research, 21(2), 230–258.
Carpenter, J., Andrykowski, M., Wilson, J., Hall, L., Kay Rayens, M., Sachs, B., & Cunningham, L. (1998). Psychometrics for two short forms of the Center for Epidemiologic Studies-Depression Scale. Issues in Mental Health Nursing, 19(5), 481–494.
Centers for Disease Control and Prevention. (2017). HIV Surveillance Report 2016, 28. Retrieved March 1, 2018 from http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html.
Cho, J., & Kogan, S. M. (2016). Risk and protective processes predicting rural african american young men’s substance abuse. American Journal of Community Psychology, 58(3–4), 422–433.
Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N., … Godbole, S. V. (2011). Prevention of HIV-1 infection with early antiretroviral therapy. New England Journal of Medicine, 365(6), 493–505.
Cox, M. J., & Paley, B. (1997). Families as systems. Annual Review of Psychology, 48(1), 243–267.
DiClemente, R. J., Wingood, G. M., Crosby, R. A., Sionean, C., Brown, L. K., Rothbaum, B., … Davies, S. (2001). A prospective study of psychological distress and sexual risk behavior among Black adolescent females. Pediatrics, 108(5), e85–e85.
Dunst, C. J., & Leet, H. E. (1987). Measuring the adequacy of resources in households with young children. Child: Care, Health and Development, 13(2), 111–125.
Eisenberg, N., Valiente, C., Spinrad, T. L., Cumberland, A., Liew, J., Reiser, M., & Losoya, S. H. (2009). Longitudinal relations of children’s effortful control, impulsivity, and negative emotionality to their externalizing, internalizing, and co-occurring behavior problems. Developmental Psychology, 45(4), 988–1008. https://doi.org/10.1037/a0016213.
Elliott, D. S., & Menard, S. (1996). Delinquent friends and delinquent behavior: Temporal and developmental patterns. In J. D. Hawkins (Ed.), Delinquency and crime: Current theories (pp. 28–67). Cambridge: Cambridge University Press.
Ethier, K. A., Kershaw, T. S., Lewis, J. B., Milan, S., Niccolai, L. M., & Ickovics, J. R. (2006). Self-esteem, emotional distress and sexual behavior among adolescent females: Inter-relationships and temporal effects. Journal of Adolescent Health, 38(3), 268–274.
Fleming, P. L., Lansky, A., Lee, L. M., & Nakashima, A. K. (2006). The epidemiology of HIV/AIDS in women in the southern United States. Sexually Transmitted Diseases, 33(7), S32–S38.
Flouri, E., Tzavidis, N., & Kallis, C. (2010). Adverse life events, area socioeconomic disadvantage, and psychopathology and resilience in young children: The importance of risk factors’ accumulation and protective factors’ specificity. European Child and Adolescent Psychiatry, 19(6), 535–546. https://doi.org/10.1007/s00787-009-0068-x.
Furman, W., & Buhrmester, D. (1985). Children’s perceptions of the personal relationships in their social networks. Developmental Psychology, 21(6), 1016.
Gibbons, F. X., O’hara, R. E., Stock, M. L., Gerrard, M., Weng, C. Y., & Wills, T. A. (2012). The erosive effects of racism: Reduced self-control mediates the relation between perceived racial discrimination and substance use in African American adolescents. Journal of Personality and Social Psychology, 102(5), 1089.
Hall, H. I., Li, J., & McKenna, M. T. (2005). HIV in predominantly rural areas of the United States. Journal of Rural Health, 21(3), 245–253.
Hallfors, D. D., Iritani, B. J., Miller, W. C., & Bauer, D. J. (2007). Sexual and drug behavior patterns and HIV and STD racial disparities: The need for new directions. American Journal of Public Health, 97(1), 125–132. https://doi.org/10.2105/AJPH.2005.075747.
Hamama, L., & Ronen-Shenhav, A. (2013). The role of developmental features, environmental crises, and personal resources (self-control and social support) in adolescents’ aggressive behavior. Aggression and Violent Behavior, 18(1), 26–31.
Hayes, J. A., Chun-Kennedy, C., Edens, A., & Locke, B. D. (2011). Do double minority students face double jeopardy? Testing minority stress theory. Journal of College Counseling, 14(2), 117–126.
Heckathorn, D. D. (1997). Respondent-driven sampling: A new approach to the study of hidden populations. Social Problems, 44(2), 174–199.
Heckathorn, D. D. (2002). Respondent-driven sampling II: Deriving valid population estimates from chain-referral samples of hidden populations. Social Problems, 49(1), 11–34.
Hicks, M. R., Kogan, S. M., Cho, J., & Oshri, A. (2017). Condom use in the context of main and casual partner concurrency: Individual and relationship predictors in a sample of heterosexual African American men. American Journal of Men’s Health, 11(3), 585–591.
Hladik, F., & McElrath, M. J. (2008). Setting the stage–HIV host invasion. Nature Reviews Immunology, 8(6), 447–457.
Hudson, D. L., Puterman, E., Bibbins-Domingo, K., Matthews, K. A., & Adler, N. E. (2013). Race, life course socioeconomic position, racial discrimination, depressive symptoms and self-rated health. Social Science and Medicine, 97, 7–14.
Joe, G. W., Broome, K. M., Rowan-Szal, G. A., & Simpson, D. D. (2002). Measuring patient attributes and engagement in treatment. Journal of Substance Abuse Treatment, 22(4), 183–196.
Johnson, S. D., Cunningham-Williams, R. M., & Cottler, L. B. (2003). A tripartite of HIV-risk for African American women: the intersection of drug use, violence, and depression. Drug and Alcohol Dependence, 70(2), 169–175.
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Hawkins, J., … Zaza, S. (2016). Youth Risk Behavior Surveillance—United States, 2015. Morbidity and Mortality Weekly Report. Surveillance Summaries, 65(6), 1–174.
Kogan, S. M., Allen, K. A., Gonzales-Backen, M., Bae, D., & Cho, J. (2018). Romantic relationships among emerging adult African–American men: A latent profile analysis. Journal of Social and Personal Relationships, 0265407518776130.
Kogan, S. M., & Brody, G. H. (2010). Linking parenting and informal mentor processes to depressive symptoms among rural African American young adult men. Cultural Diversity and Ethnic Minority Psychology, 16(3), 299–306.
Kogan, S. M., Brody, G. H., & Chen, Y.-F. (2011a). Natural mentoring processes deter externalizing problems among rural African American emerging adults: A prospective analysis. American Journal of Community Psychology, 48(3–4), 272–283. https://doi.org/10.1007/s10464-011-9425-2.
Kogan, S. M., Brody, G. H., Chen, Y. F., Grange, C. M., Slater, L. M., & DiClemente, R. J. (2010). Risk and protective factors for unprotected intercourse among rural African American young adults. Public Health Reports, 125(5), 709–717.
Kogan, S. M., Brody, G. H., Crawley, C., Logan, P., & Murry, V. M. (2007). Correlates of elevated depressive symptoms among rural African American adults with type 2 diabetes. Ethnicity and Disease, 17(1), 106–112.
Kogan, S. M., Cho, J., Barton, A. W., Duprey, E. B., Hicks, M. R., & Brown, G. L. (2016a). The influence of community disadvantage and masculinity ideology on number of sexual partners: A prospective analysis of young adult, rural Black men. Journal of Sex Research, 54, 1–7. https://doi.org/10.1080/00224499.2016.1223798.
Kogan, S. M., Cho, J., Brody, G. H., & Beach, S. R. (2017). Pathways linking marijuana use to substance use problems among emerging adults: A prospective analysis of young Black men. Addictive Behaviors, 72, 86–92.
Kogan, S. M., Cho, J., & Oshri, A. (2016b). The influence of childhood adversity on rural Black men’s sexual risk behavior. Annals of Behavioral Medicine, 50, 1–10. https://doi.org/10.1007/s12160-016-9807-7.
Kogan, S. M., Wejnert, C., Chen, Y.-F., Brody, G. H., & Slater, L. M. (2011b). Respondent-driven sampling with hard-to-reach emerging adults: An introduction and case study with rural African Americans. Journal of Adolescent Research, 26(1), 30–60.
Liao, K. Y.-H., Kashubeck-West, S., Weng, C.-Y., & Deitz, C. (2015). Testing a mediation framework for the link between perceived discrimination and psychological distress among sexual minority individuals. Journal of Counseling Psychology, 62(2), 226–241.
Martin, L. A., Neighbors, H. W., & Griffith, D. M. (2013). The experience of symptoms of depression in men vs women: Analysis of the national comorbidity survey replication. JAMA Psychiatry, 70(10), 1100–1106. https://doi.org/10.1001/jamapsychiatry.2013.1985.
Mays, V. M., Cochran, S. D., & Barnes, N. W. (2007). Race, race-based discrimination, and health outcomes among African Americans. Annual Review of Psychology, 58, 201–225.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Education Quarterly, 15(4), 351–377.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697.
Mossakowski, K. N., & Zhang, W. (2014). Does social support buffer the stress of discrimination and reduce psychological distress among Asian Americans? Social Psychology Quarterly, 77(3), 273–295.
Murry, V. M., & Brody, G. H. (2004). Partnering with community stakeholders: Engaging rural African American families in basic research and the Strong African American Families preventive intervention program. Journal of Marital and Family Therapy, 30(3), 271–283.
Murry, V. M., Heflinger, C. A., Suiter, S. V., & Brody, G. H. (2011). Examining perceptions about mental health care and help-seeking among rural African American families of adolescents. Journal of Youth and Adolescence, 40(9), 1118–1131.
Muthén, L. K., & Muthén, B. O. (2010). 1998–2010 Mplus user‘s guide. Los Angeles, CA: Author.
Oshri, A., Kogan, S., Liu, S., Sweet, L., & Mackillop, J. (2017). Pathways linking adverse childhood experiences to cigarette smoking among young black men: A prospective analysis of the role of sleep problems and delayed reward discounting. Annals of Behavioral Medicine, 51(6), 890–898.
Poundstone, K. E., Strathdee, S. A., & Celentano, D. D. (2004). The social epidemiology of human immunodeficiency virus/acquired immunodeficiency syndrome. Epidemiologic Reviews, 26(1), 22–35.
Preacher, K. J., Rucker, D. D., & Hayes, A. F. (2007). Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research, 42(1), 185–227.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401.
Roberts, M. E., Gibbons, F. X., Gerrard, M., Weng, C. Y., Murry, V. M., Simons, L. G., & Lorenz, F. O. (2012). From racial discrimination to risky sex: Prospective relations involving peers and parents. Developmental Psychology, 48(1), 89–102.
Sampson, R. J., Raudenbush, S. W., & Earls, F. (2009). Neighborhoods and violent crime: A multilevel study of collective efficacy. In P. Hynes & P. Lopez (Eds.), Urban health: Readings in the social, built, and physical environments of US cities (pp. 79–97). Boston, MA: Jones and Bartlett.
Schwinn, T. M., & Schinke, S. P. (2014). Alcohol use and related behaviors among late-adolescent urban youths: Peer and parent influences. Journal of Child and Adolescent Substance Abuse, 23(1), 58–64.
Sharp, P. M., & Hahn, B. H. (2011). Origins of HIV and the AIDS pandemic. Cold Spring Harbor Perspectives in Medicine, 1(1), a006841.
Shrier, L. A., Harris, S. K., Sternberg, M., & Beardslee, W. R. (2001). Associations of depression, self-esteem, and substance use with sexual risk among adolescents. Preventive Medicine, 33(3), 179–189.
Simons, R. L., Chao, W., Conger, R. D., & Elder, G. H. (2001). Quality of parenting as mediator of the effect of childhood defiance on adolescent friendship choices and delinquency: A growth curve analysis. Journal of Marriage and Family, 63(1), 63–79.
Simons, R. L., Simons, L. G., Burt, C. H., Drummund, H., Stewart, E., Brody, G. H., & Cutrona, C. (2006). Supportive parenting moderates the effect of discrimination upon anger, hostile view of relationships, and violence among African American boys. Journal of Health and Social Behavior, 47(4), 373–389. https://doi.org/10.1177/002214650604700405.
Simons-Morton, B., Chen, R., Abroms, L., & Haynie, D. L. (2004). Latent growth curve analyses of peer and parent influences on smoking progression among early adolescents. Health Psychology, 23(6), 612–621.
Smith, G. T., & Cyders, M. A. (2016). Integrating affect and impulsivity: The role of positive and negative urgency in substance use risk. Drug and Alcohol Dependence, 163(Suppl. 1), S3–S12. https://doi.org/10.1016/j.drugalcdep.2015.08.038.
Sue, D. W., Capodilupo, C. M., Torino, G. C., Bucceri, J. M., Holder, A., Nadal, K. L., & Esquilin, M. (2007). Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist, 62(4), 271–286.
Sue, D. W., Nadal, K. L., Capodilupo, C. M., Lin, A. I., Torino, G. C., & Rivera, D. P. (2008). Racial microaggressions against Black Americans: Implications for counseling. Journal of Counseling and Development, 86(3), 330–338.
Tice, D. M., Bratslavsky, E., & Baumeister, R. F. (2001). Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! Journal of Personality and Social Psychology, 80, 53–67.
Tice, D. M., Bratslavsky, E., & Baumeister, R. F. (2018). Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! In R. F. Baumeister (Ed.), Self-regulation and self-control (pp. 275–306). United Kingdom: Routledge
Troisi, A., & D’Argenio, A. (2004). The relationship between anger and depression in a clinical sample of young men: the role of insecure attachment. Journal of Affective Disorders, 79(1), 269–272. https://doi.org/10.1016/S0165-0327(02)00406-8.
Umberson, D., Crosnoe, R., & Reczek, C. (2010). Social relationships and health behavior across life course. Annual Review of Sociology, 36, 139–157.
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., & Currie, C. (2012). Adolescence and the social determinants of health. The Lancet, 379(9826), 1641–1652.
Wald, M., & Martinez, T. (2003). Connected by 25: Improving the life chances of the country’s most vulnerable 14–24 year olds. William and Flora Hewlett Foundation Working Paper. Palo Alto, CA: Stanford University.
Williams, D. R., & Mohammed, S. A. (2009). Discrimination and racial disparities in health: evidence and needed research. Journal of Behavioral Medicine, 32(1), 20–47.
Williams, R. D., & Williams-Morris, R. (2000). Racism and mental health: the African American experience. Ethnicity and Health, 5(3–4), 243–268.
Wills, T. A., & Ainette, M. G. (2010). Temperament, self-control, and adolescent substance use: A two-factor model of etiological processes.
Acknowledgements
We would like to thank Eileen Neubaum-Carlan, M.S., for her helpful comments in the preparation of this article.
Funding
This research was supported by Award Number R01 DA029488 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse, or the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hicks, M.R., Kogan, S.M. Racial Discrimination, Protective Processes, and Sexual Risk Behaviors Among Black Young Males. Arch Sex Behav 48, 507–519 (2019). https://doi.org/10.1007/s10508-018-1341-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10508-018-1341-1